Embed Size (px)
Citation preview

Aging Clin Exp Res, Vol. 24, No. 5 555
Key words: Acute lymphoblastic leukemia, Eosinophilia, Hypereosinophilic syndrome.Correspondence: Shukui Wang, Central Laboratory of Nanjing First Hospital, Nanjing Medical University, 68 Changle Rd, Nanjing 210006,China.E-mail: [email protected] July 15, 2011; accepted in revised form March 30, 2012.First published ahead of print April 5, 2012 as DOI: 10.3275/8337
Acute lymphocytic leukemia with eosinophilia:a case report and review of the literature
Aging Clinical and Experimental Research
Guoqi Song1, Hong Liu1, Feng Sun1, Ling Gu2 and Shukui Wang2
1Department of Hematology, Affiliated Hospital of Nantong University, Nantong,2Central Laboratory of Nanjing First Hospital, Nanjing Medical University, Nanjing, China
ABSTRACT. We present a 61-year-old man withmarked peripheral blood eosinophilia, feature of hy-pereosinophilic syndrome, that later evolved into acutelymphocytic leukemia (ALL-L2). Initially the patient suf-fered from significant complications related toeosinophilic toxicity, including large urticarial hyper-pigmented plaques, myocardial infarction, andeosinophilic pneumonia. He was treated with highdose of steroids resulting in a rapid suppression of theeosinophilia. Two weeks later, the eosinophilia had re-lapsed, so a bone marrow aspiration was performed.Cytomorphological examination of the bone marrowshowed typical ALL features, while flow cytometricanalysis revealed an My+pre-B-ALL immunopheno-type, and chromosome analysis of bone marrowshowed a normal karyotype. He received chemotherapyaccording to the standard protocol for ALL and diedfrom refractory respiratory failure and congestiveheart failure immediately after antileukemic therapy.We review the literature and compare the demo-graphics, clinical features, and outcomes of several cas-es and reported studies.(Aging Clin Exp Res 2012; 24: 555-558)©2012, Editrice Kurtis
median age of 15.3 years and an age range of 2-58years; however no patient over 60 years old has been re-ported. As to patients, the characteristic feature of ALLwith eosinophilia is absence of blasts in the peripheralblood film. They always have common symptoms in-cluding urticarial plaques, sweats, arthralgia, fever, myal-gia, and dyspnea. If bone marrow aspiration was notperformed and the patient started on steroid therapy, thiscould lead to delay in the diagnosis. The most commoncytogenetic abnormality encountered in acute lym-phoblastic leukemia with eosinophilia is t(5;14)(q31;q32)(2-6), characterized by overproduction of interleukin-3.Here we present a case of My+pre-B ALL associated withmarked peripheral eosinophilia. The patient was a 61-year-old man, having a normal karyotype, presentingwith large urticarial hyperpigmented plaques, myocardialinfarction, and eosinophilic pneumonia, and subsequentlydiagnosed with My+pre-B-ALL.
CASE REPORTA male patient, 61-year-old, was admitted with a history
of fatigue and diffuse muscle pain especially marked in thelower legs and both hip joints for one month. He was afarmer occasionally smoking and drinking alcohol. Hewas not worried and no medication was performed before.Three weeks later, he was suffering from fever, large ur-ticarial hyperpigmented plaques, cough, shortness ofbreath, vomiting, arthralgia, and cardiopalmus. Therewas no history of worm infestations and allergy. Family his-tory was also not significant.
He was referred to a dermatologist, where he under-went a physical examination and blood tests. His tem-perature was 100.9°F, with a pulse of 134/min, respi-
INTRODUCTIONEosinophilia can be seen in helminthic infections, al-
lergic disorders, lymphoproliferative disorders, skin dis-eases and malignancy, but the association of acute lym-phocytic leukemia (ALL) with symptomatic eosinophilia israre. Since Spitzer and Garson (1) first described thedisease in 1973, 54 other patient cases have been re-ported. Many case reports involve male children with a
CASE REPORT

ration of 31/min, and blood pressure of 139/86. He haderythematous and hyperpigmented urticarial plaques at theknees, dorsa of his feet and his abdomen. There was nolymphadenopathy, but the tip of his spleen was palpableat that time.
An initial laboratory examination revealed an elevatedwhite blood cell (WBC) count of 44000/μL with a dif-ferentiation of 36080/μL mature eosinophils (82%).The hemoglobin concentration was 12.2 g/dL and theplatelet count 121000/μL. The erythrocyte sedimentationrate was elevated, 23 mm/hr (ref. <15 mm/hr). Toxocaratiters, toxoplasmosis titers and isohemagglutinin titerswere unremarkable. Multiple stool samples were negativefor ova and parasites. Antinuclear antibody, rheumatoidfactor, CEA test, prostatic carcinoma laboratory test,venereal disease research laboratory test and hepatitis Bsurface antigen were all negative. An electrocardiogramshowed ST segment depressions with an elevation ofcardiac isoenzymes. A chest computed tomography (CT)showed bilateral interstitial pneumonia and a small rightpleural effusion. Then a diagnosis of hypereosinophilicsyndrome was made by a dermatologist. They gave himhigh dose steroids with 200 mg of methylprednisolone for14 days, with good symptomatic relief, a rapid suppres-sion of eosinophilia, and resolution of his radiological find-ings.
Two weeks later, as the steroids were tapered, theeosinophilia recurred and those symptoms relapsed. Hiswhite count was 18000/μL with 63% eosinophils(11340/μL), hemoglobin was 8.9 g/dL and plateletswere decreased to 36000/μL. Then he was referred to thedepartment of hematology. Three days later, the patientdeveloped worsening shortness of breath and hypoxia. Achest CT revealed diffuse bilateral infiltrate and bilateral in-terstitial pneumonia. An abdominal ultrasound revealed hisspleen was larger than before, 1.8 cm below the costalmargin. ECG showed signs of ischaemia.
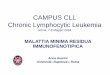
For correct diagnosis, further in-depth diagnostic tests,bone marrow aspiration (BMA), immunophenotype, bonemarrow biopsy (BMB), and cytogenetic study were carriedout. The BMA and BMB (Fig. 1) showed a hypercellularmarrow with markedly increased numbers of eosinophilsand a diffuse infiltration of blasts. Immunophenotyping byflow cytometry on the bone marrow aspirate showedlymphoblast positivity for HLA-DR, CD10, CD19, CD33,CD22, and CD79α, but CD5, CD7, CD11b, CD34,CD13, CD14, CD117, CD56, CD20 and MPO werenegative. Bone marrow chromosomal analysis showed anormal male karyotype (46 XY) in 20 out of 20 studiedmetaphases. Fluorescence in situ hybridization (FISH)studies using a dual-color probe demonstrated that all ofthe most common rearrangements associated with acutelymphoid leukemia including ALL/Eo, such as BCR/ABL,TEL/AML1, MYC, E2A, MLL, P16 (ID Labs, Canada),DNA probes of chromosome 5 and 14 (Cytocell, England)
were negative. These outcomes of BMA, BMB and theimmunophenotyping confirmed the type of pre-B-cellacute lymphoblastic leukemia (ALL) with eosinophilia.Before taking the outcomes of those aforesaid tests, thepatients were given small doses of steroid and antibi-otics with intention to decrease eosinophils and delay theprogress of interstitial pneumonia. Unfortunately at thistime interstitial pneumonia had developed. He also suf-fered from hemoptysis.
A decision was made to begin induction chemothera-py with daunomycin, vincristine, prednisolone and L-as-paraginase, along with supportive treatment. During thesecond week, the patient had an aggressive clinical coursewith congestive cardiac failure as well as intractable neu-tropenia and developed staphylococcal pneumonia. Thepatient was digitalized and diuretic treatment started.Three days later, the patient became acutely dyspneic andexpired in refractory congestive heart and respiratoryfailure.
DISCUSSION AND REVIEWOF THE LITERATUREEosinophilia is encountered mostly often as a reactive
(non-clonal) proliferation associated with infections, par-asitic infestations, asthma and allergies, respiratory dis-eases, cytokine infusions, vasculitides, non-haematologi-cal malignant diseases, drug reactions and connectivetissue diseases etc. (7). Neoplasm-associated eosinophilicproliferation may be seen in chronic myelogenousleukemia and acute myelomonocytic leukemia witheosinophilia and acute lymphoblastic leukemia, Hodgkinand non-Hodgkin lymphoma and others (1). Hypere-osinophilic syndrome (HES) is characterized by bloodeosinophilia of >1500/μL eosinophilic granulocytes.
G. Song, H. Liu, F. Sun et al.
556 Aging Clin Exp Res, Vol. 24, No. 5
Fig. 1 - A bone marrow trephine biopsy showing hypercellular mar-row with markedly increased numbers of eosinophils and diffuse in-filtration of blasts (Hematoxylin, Giemsa and acid fuchsin, ×400).

Multiple organs such as the heart, lungs, skin, joints andnervous system are frequently infiltrated by matureeosinophils, eventually leading to severe dysfunction (8).But the term HES is used in the absence of any clonal ab-normality or reactive cause. As we all know, the early dis-crimination between HES and acute lymphocytic leukemiawith eosinophilia (ALL-Eo) confined to a reactive processand HES capable of progressing towards a lympho- ormyeloproliferative disease is still uncertain and repre-sents the subject of intensive investigation. The eosinophil-ia associated with ALL is believed to be a nonneoplasticreaction to the malignant lymphoblasts because onlymature eosinophils with no cytogenetic abnormalitieswere found in these cases (1, 9). Indeed, at present thereare no specific markers that may help predict the disease’sprogressive evolution. These patients are liable to bemisdiagnosed and mistreated before primary disease clin-ical features are found to be taking place.
Since its first description in 1973 by Spitzer and Gar-son (1), ALL with eosinophilia is very rare, given as lessthan 1% (10-12). However, clearly defined as a clinico-pathological entity, approximately 54 cases have been re-ported. ALL-Eo has generally been reported in a youngage group, the mean and median age of these patientswas 15 years with a range from 2 to 58 with a strikingmale predominance (73%). To our knowledge, patientsover 60 years old have not been reported in the PubMedliterature.
The differentiation of ALL-Eo from HES is not al-ways straightforward, which is one cause of misdiagnosis.Some common features of the patients are presented withnon-specific symptoms: fever, cough and/or shortness ofbreath plaques, vomiting, arthralgia, cardiopalmus andfinding of lung infiltrates, which are evident in one-third totwo-thirds of the patients. These organs functional dis-turbances are caused possibly by eosinophilic infiltrationand proteins found in the cytoplasm of eosinophilic gran-ulocytes (7). The eosinophilia usually precedes or is con-comitant with the initial diagnosis of ALL, disappears inremission and usually appears at the time of leukaemia re-lapse (13). In the present case, eosinophilia and accom-panying respiratory symptoms, cutaneous rashes etc.had antedated the diagnosis. So the hypereosinophilia inALL-Eo may serve as a sensitive marker for leukemic dis-ease activity.
The relation between eosinophilia and ALL is of in-terest and remains controversial. The etiology appears tobe reactive in nature. Some have hypothesized that thelymphoblasts may secrete factors that stimulateeosinophilopoiesis or the immune response initiated bylymphocytes may induce increased production ofeosinophils by the bone marrow (1). In some patients, thechromosomal translocation t(5;14)(q31;q32) (3-7), joiningthe IL3 gene from chromosome 5 to the IgH gene fromchromosome 14, has been detected, cloned and studied
at a molecular level. The t(5;14) translocation rearrangedthe IL-3, IL-5 and GM-CSF genes affecting the differen-tiation and production of eosinophils (10, 14). Overex-pression in some or all of these three growth factorscould explain a secondary rise in eosinophils throughtriggering of the production maturation and survival of thecells. Meeker et al. (10) also measured elevated levels ofIL-3 in one of these patients and found that elevations inserum IL-3 levels correlated with the occurrence of the dis-ease. Our patient had a normal karyotype, observed in45% of ALL/Eo patients. However, there were other cy-togenetic abnormalities found in ALL-Eo: 5q-,t(5;9)(q31;p24) and t(7;12)(q22;p13) (15-17), suggestingthe heterogeneity in the underlying pathophysiology.
ALL/Eo is an aggressive rare subtype of ALL. Theprognosis is also significantly worse than standard ALL,with a median survival time of 7.5 months showing a neg-ative outcome in most reported cases (18). Congestiveheart failure and dyspnoea are the main causes of in-creased mortality in ALL/Eo, compared to standard-riskALL as our patient presents. The eosinophilic infiltrationof lung and heart tissue presents additional challenges oftherapy. In the face of possible end organ damage sec-ondary to eosinophilia which releases specific granules, de-position of eosinophil proteins, activation of eosinophilsand thrombotic events that may lead to the functional im-pairment of normal tissues (1), making the choice of atreatment plan is very difficult. At early stage of ALL/Eo,the disease shares similar clinical and laboratory featureswith HES, so the rate of misdiagnosis and mistreatmentis high. This results in patients not receiving promptand perfect treatment as was the case with our patient.
Although our patient succumbed from respiration fail-ure and congestive heart failure attributed to theeosinophilia and ALL in a very short time, we can learnmuch from the patient. It is very important for cliniciansto be aware of this specific and rare subtype of ALL.When facing those patients with a persistent peripheraleosinophilia, particularly if there are no lymphoblasts inthe peripheral blood, we suggest that regularly checkingand early bone marrow aspiration is necessary to providean opportunity for accurate diagnosis and enhance thesurvival time for these patients.
REFERENCES1. Spitzer G, Garson OM. Lymphoblastic leukemia with marked
eosinophilia: a report of two cases. Blood 1973; 42: 377-84.
2. Troxell ML, Mills GM, Allen RC. The hypereosinophilic syn-drome in acute lymphoblastic leukemia. Cancer 1984; 54:1058-61.
3. Fishel RS, Farnen JP, Hanson CA et al. Acute lymphoblasticleukemia with eosinophilia. Medicine (Baltimore) 1990; 69:232-43.
4. Meeker TC, Hardy D, Willman C et al. Activation of the inter-leukin-3 gene by chromosome translocation in acute lymphocyticleukemia with eosinophilia. Blood 1990; 76: 285-9.
Acute lymphocytic leukemia with eosinophilia
Aging Clin Exp Res, Vol. 24, No. 5 557

5. Grimaldi JC, Meeker TC. The t(5;14) chromosomal translocationin a case of acute lymphocytic leukemia joins the interleukin-3gene to the immunoglobulin heavy chain gene. Blood 1989; 73:2081-5.
6. Hogan HF, Koss W, Murgo AJ et al. Acute lymphoblasticleukemia with chromosomal 5;14 translocation and hypere-osinophilia: case report and literature review. J Clin Oncol 1987;5: 382-90.
7. Brito-Babapulle F. The eosinophilias, including the idiopathichypereosinophilic syndrome. Br J Haematol 2003; 121: 203-23.
8. Aractingi S, Janin A, Zini JM et al. Specific mucosal erosions inhypereosinophilic syndrome. Evidence for eosinophil proteindeposition. Arch Dermatol 1996; 132: 535-41.
9. Knuutila S, Alitalo R, Ruutu T. Power of the MAC (morphology-antibody-chromosomes) method in distinguishing reactive and clon-al cells: report of a patient with acute lymphatic leukemia,eosinophilia, and t(5; 14). Gene Chromosome Canc 1993; 8:219-23.
10. Grimaldi JC, Meeker TC. The t(5;14) chromosomal translocationin a case of acute lymphocytic leukemia joins the interleukin-3gene to the immunoglobulin heavy chain gene. Blood 1989; 73:2081-25.
11. Wilson F, Tefferi A. Acute lymphocytic leukemia with eosinophil-ia: two case reports and a literature review. Leukemia Lymphoma2005; 46: 1045-50.
12. Jain P, Kumar R, Gujral S et al. Granular acute lymphoblasticleukemia with hypereosinophilic syndrome. Ann Hematol 2000;79: 272-4.
13. Narayanaa G, Hussain BM, Chandralekha B et al. Hypere-osinophilic syndrome in acute lymphoblastic leukaemia - case re-port and literature review. Acta Oncol 2000; 39: 241-3
14. Girodon F, Bergoin E, Favre B et al. Hypereosinophilia inacute B-lineage lymphoblastic leukaemia. Br J Haematol 2005;129: 568.
15. Wyun TT, Heerema NA, Hammond S et al. Acute lymphoblasticleukemia with hypereosinophilia: report of a case with 5q deletionand review of the literature. Pediatr Dev Pathol 2003; 6: 558-63.
16. Nunez CA, Zipf TF, Roberts WM et al. Molecular monitoring ofcerebrospinal fluid can predict clinical relapse in acute lym-phoblastic leukemia with eosinophilia. Arch Pathol Lab Med2003; 127: 601-5.
17. Abbas Bhatti F, Hussain I, Zafar Ali M. Adult B lymphoblasticleukaemia/lymphoma with hypodiploidy(-9) and a novel chro-mosomal translocation t(7;12)(q22;p13) presenting with severeeosinophilia – case report and review of literature. J HematolOncol 2009; 2: 26.
18. Files MD, Zenel JA, Armsby LB et al. A child with eosinophilia,Loeffler endocarditis, and acute lymphoblastic leukemia. PediatrCardiol 2009; 30: 530-2.
G. Song, H. Liu, F. Sun et al.
558 Aging Clin Exp Res, Vol. 24, No. 5