Embed Size (px)
Citation preview

Eur J Haematoll998: 60: 310-312 Printed in UK - all rights reserved
Copyright 0 Munksgaard 1998 EUROPEAN
JOURNAL OF HAEMATOLOGY ISSN 0902-4441
Letters to the Editor
Acute meizakarvocvtic leukaemia (AML-MY) with mielofibrosis terminating in AML-MO with concurrent liver fibrosis To the Editor: Acute myelofibrosis is distinct from classical idio- pathic myelofibrosis (IMF) and is associated with haematopoietic disorders including myelodysplastic syndrome (MDS) and acute myelogenous leukae- mia (AML). In particular, acute megakaryocytic leukaemia (AMgKL), M7, is closely linked to bone marrow fibrosis (1). We present a case of AML- M7 with acute myelofibrosis progressing to AML- MO and with massive ascites resulting from obscure hepatic fibrosis.
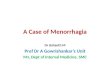
A 55-yr-old man was referred to our hospital because of pancytopenia. Physical examination revealed scattered petechiae on his legs in addition to anaemic palpebrae. Neither hepatomegaly nor splenomegaly were found, and there were no enlarged surface lymph nodes. His peripheral blood showed leucoerythroblastic anaemia including a haemoglobin of 3.4g/dl, a platelet count of 28x109/l, and a leucocyte count of 2.9x109/1 with a differ- ential of 1 YO promyelocytes, 0.5% myelocytes, 0.5% metamyelocytes, 55% neutrophils, 7.5% mono- cytes, 0.5 YO eosinophils, 0.5% basophils and 33.5% lymphocytes, in addition to erythroblasts with a ratio of 4 erythroblasts per 100 leucocytes. Neutro- phi1 alkaline phosphatase (NAP) activity was com- parable to that of a normal control. Serum concentrations of transaminases, bilirubin, lactate dehydrogenase (LDH) and haptoglobin were all in the normal range, and there were no chemical findings suggesting haemolytic anaemia or hepatic disease. Serum concentrations of platelet factor 4 (PF4) and P thromboglobulin (PTG) were both elevated despite a decreased platelet count (PF4 76 ng/ml (normal value: less than 20), PTG 200 ng/ml (normal value: less than 50)). An attempted bone marrow aspiration resulted in a dry tap, and a trephine biopsy specimen displayed intense colla- gen fibrosis and increased numbers of megakaryo- cytes together with proliferation of large blastic cells (Fig. 1). Blastic cells had large nuclei with dense chromatin and were immunohistochemically positive for PLTl monoclonal antibodies against GPIIb/IIIa (CD41, Coulter Immunology, Hialeah,
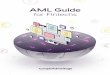
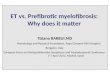
FL, USA). A diagnosis of AMgKL with myelo- fibrosis was made; steroid pulse therapy in addition to frequent platelet and red cell transfusions did not produce haematologic improvement. Two months later, he noted increased abdominal girth due to ascites. The ascitic fluid was found to be transudative and contain erythroblasts, granulo- cytes and megakaryocyte-like large cells (Fig. 2). One month before death, the leucocyte count rose suddenly to 28.8x109/1 with 88.0% leukaemic cells; these were both cytochemically and immuno- phenotypically consistent with AML-MO at this time. Chromosome analysis using peripheral blood leukaemic cells did not demonstrate Philadelphia chromosome (Ph’). Ascites progressed despite fre- quent drainage; the patient died 7 months following his initial presentation. Postmortem examination revealed massive infiltration of leukaemic cells into the bone marrow, liver, spleen, kidneys, adrenals and diaphragm. There was massive bloody ascites (12,000 ml), but extramedullary haematopoietic foci were not found in the peritoneal cavity. In addition to intense bone marrow fibrosis, sinu- soidal fibrosis of the liver was noted in the areas between Glisson’s capsules (Fig. 3), and this was associated with oesophageal and gastric varices. Of interest, liver fibrosis was not accompanied by nodular regeneration of hepatic cells, which is commonly seen in liver cirrhosis.
IMF is a myeloproliferative disorder charac- terized by extramedullary haematopoiesis and intense bone marrow fibrosis. Similar conditions are known to occur in MDS and AML, and these are designated “acute myelodysplasia with myelofibrosis (AMMF)”, “acute myelosclerosis” or “acute mega- karyoblastic leukaemia with myelofibrosis”. These disorders are characterized by acute onset, older age, severe pancytopenia reflecting bone marrow insufficiency, no associated organomegaly, and rapid progression to acute leukaemia; the incidence of fibrosis is reported to vary from 30 to 72% in AML and MDS (1). Although classical IMF is known to transform into acute leukaemia (2, 3), our patient initially presented with severe pancytopenia without
31 0

Letters to the Editor
Fig. 1. A bone marrow biopsy specimen at initial presentation. Collagen fibrosis is noted, and megakaryocytes are increased in number. In addition, blastic cells with large nuclei and dense chromatins are recognized (haematoxylin & eosin stain, ~400).
an apparent myeloproliferative phase, and he rap- idly progressed to overt leukaemia within a short period. Furthermore, there was neither spleno- megaly nor other extramedullary haematopoietic foci. Thus, our findings appear to differ from those of typical IMF, suggesting the diagnosis of AMMF evolving into AMgKL (AML-M7).
One interesting finding is ascites of unknown origin. Two major mechanisms have been con- sidered in the occurrence of ascites in myelo- fibrosis. First, peritoneal and/or mesenteric extramedullary haematopoiesis may cause fluid retention in serous cavities, and these contain various haematopoietic cells such as erythroblasts, megakaryocytes and immature granulocytes (4). In fact, some megakaryocyte-like large cells were detected in this patient’s ascitic fluid. Secondly, portal hypertension is an alternative explanation for ascites in myelofibrosis. Portal hypertension is thought to result from several conditions, including
hepatic or portal vein thrombosis, increased blood flow due to splenomegaly, nodular hyperplasia of the liver and intrahepatic sinusoidal obstruction (5 , 6). The liver fibrosis in our case showed one unique feature distinct from ordinary liver cir- rhosis: there was no nodular regenerative hyper- plasia with pseudolobular transformation of hepatocytes. Similar findings have been previously reported. Tsao (7) reported 2 patients with agno- genic myeloid metaplasia (AMM) and noted lack of nodular regeneration despite extensive sinu- soidal fibrosis of the liver. He suggested the pres- ence of haematopoietic elements in the sinusoids and linked a pathogenesis of liver fibrosis to fibro- sis of the bone marrow. Moreover, Tsao linked hepatic sinusoidal fibrosis pathologically with extramedullary haematopoiesis in patients with myelofibrosis for the first time. Recently, Miyauchi and colleagues (8) presented 4 autopsy cases of transient myeloproliferative disorder (TMD) with intralobular diffuse liver fibrosis, which is distinct from typical cirrhosis because of the absence of pseudolobular nodular transformation of hepato- cytes. They histochemically demonstrated haemato- poietic cells of three lineages in liver tissue and suggested that liver fibrosis was the result of haemato- poietic cytokines. Detection of megakaryocyte-like large cells in the ascites of our patient supports these hypotheses.
Cytokines such as platelet-derived growth factor (PDGF), transforming growth factor+ (TGF-P) and platelet factor 4 (PF4) will stimulate the growth of fibroblasts and therefore, could cause bone marrow fibrosis (9). In addition, PTG has been reported to be elevated in the serum of patients with AMgKL with myelofibrosis (10). In our patient, PF4 and/or PTG may play a role in both marrow and liver fibrosis. Blastic cells of mega- karyocytic origin, which secrete fibroblast growth
Fig. 2. Cytology of ascitic fluid. A megakaryocyte-like large cell is surrounded by erythroblasts, granulocytes, and lymphocytes (Papanicolaou stain, x400).
Fig. 3. An autopsy specimen of the liver. Diffuse sinusoidal fibrosis is noted, but nodular regenerative hyperplasia of hepatocytes is not observed (haematoxylin & eosin stain, x80).
31 1

Letters to the Editor
factors and induce fibrosis in the bone marrow, may also aberrantly migrate to the liver, generate sub- clinical haematopoietic foci, and cause unusual fibrosis in a fashion similar to myelofibrosis. In conclusion, our case critically suggests an associ- ation between acute myelofibrosis and unique fibrosis in extramedullary tissues.
References
1.
2.
3.
4.
5.
6.
IMBERT M, NGUYEN D, SULTAN C. Myelodysplastic syn- dromes (MDS) and acute myeloid leukemias (AML) with myelofibrosis. Leuk Res 1992: 16: 51-54. EMILIA G, SACCHI S, TEMPERANI P, LONGO R, VECCHI A. Progression of essential thrombocythemia to blastic crisis via idiopathic myelofibrosis. Leuk Lymph 1993: 9: 423-426. NAKAHATA J, TAKAHASHI M, FUSE I, et al. Paroxysmal noc- turnal hemoglobinuria with myelofibrosis: progression to acute myeloblastic leukemia. Leuk Lymph 1993: 12 137-142. SILVERMAN JE Extramedullary hematopoietic ascitic fluid cytology in myelofibrosis. Am J Clin Pathol 1985: 84: 125- 128. Roux D, MERLIO JP, QUINTON A, LAMOULIATTE H, BALABAUD C, BIOULAC-SAGE l? Agnogenic myeloid meta- plasia, portal hypertension, and sinusoidal abnormalities. Gastroenterology 1987: 92: 1067-1072. LIOTE F, YENI P, TEILLET-THIEBAUD F, et al. Ascites revealing peritoneal and hepatic extramedullary hematopoiesis with peliosis in agnogenic myeloid metaplasia: case report and review of the literature. Am J Med 1991: 90: 111-117.
7.
8.
9.
10.
TSAO M-S. Hepatic sinusoidal fibrosis in agnogenic myeloid metaplasia. Am J Clin Pathol 1989: 91: 302-305. MIYAUCHI J, ITO Y, KAWANO T, TSUNEMATSU Y, SHIMIZU K. Unusual diffuse liver fibrosis accompanying transient myeloproliferative disorder in Down's syndrome: a case report of four autopsy cases and proposal of a hypothesis.
REILLY JT. Pathogenesis of idiopathic myelofibrosis: present status and future directions. Br J Haematol 1994 88: 1-8. GAREL D, MIELOT F, GAULARD J, QUILLARD J, DOMMERGUES JP, TCHERNIA G. Acute megakaryocytic leukemia (AMKL) with major myelofibrosis in an infant. Diagnosis by liver biopsy and response to treatment. Nouv Rev Fr Hematol
Blood 1992: 80: 1521-1527.
1991: 33: 5-8.
Keisuke Shibata, Shigeo Nakano', Masayuki Watanabe, Hiromi Yano, Miwako Matsuzaki and Masayuki Sano Division of Haematology, Department of Internal Medicine and 'Department of Pathology, Saga Medical School, Saga, Japan
Correspondence: Keisuke Shibata MD, Division of Haematology, Department of Internal Medicine, Saga Medical School, 5-1-1 Nabeshima, Saga 849- 8501, Japan Tel: 81-952-6511 ext. 2360 Fax: 81 -952-34-2017
31 2