Embed Size (px)
Citation preview
187
International Journal of
HEMATOLOGY
Case Report
1. Introduction
The incidence of myelodysplastic syndrome (MDS) oracute myelogenous leukemia (AML) in patients with a pre-vious diagnosis of chronic lymphocytic leukemia (CLL) israre (less than 1%) [1]. In the majority of reported cases,AML is diagnosed following treatment of CLL and isthought to be a secondary or therapy-related leukemia [2].However, there are reports of cases of AML arising inpatients with untreated CLL and of cases of AML and CLLdiagnosed simultaneously [3-5].
In this article, we report the clinical, immunophenotypic,and genetic features of a quite rare case of AML concurrentwith untreated CLL.
2. Case Report
The patient, an 84-year-old Japanese man, had been welluntil August 24, 2000, when general fatigue and fever devel-oped. He was admitted to the Chihaya Hospital on Septem-
Acute Myelogenous Leukemia Concurrent WithUntreated Chronic Lymphocytic Leukemia
Tsuyoshi Muta,a Takashi Okamura,b Yoshiyuki Nihoa
aDepartment of Internal Medicine, Chihaya Hospital, Fukuoka City; bMedicine and Biosystemic Science,Kyushu University Graduate School of Medical Sciences, Fukuoka City, Japan
Received February 23, 2001; received in revised form October 5, 2001; accepted October 12, 2001
AbstractWe report a case of acute myelogenous leukemia (AML) concurrent with untreated chronic lymphocytic leukemia (CLL).
An 84-year-old Japanese man was admitted to the Chihaya Hospital with persistent high-grade fever. Morphologic observa-tion of peripheral blood and bone marrow smears revealed a proliferation of blasts and lymphocytosis with small and maturephenotypes. Immunophenotyping of the blast cells revealed CD13+, CD33+, CD34+, and HLA-DR+, and that of the lympho-cytes revealed CD5+, CD19+, CD20+, and �+ on the cell surface. The peripheral lymphocytes revealed an IgH gene rearrange-ment. Chromosome analysis of 20 metaphase cells from bone marrow showed numerous abnormalities, containing +8,+11,+21.The patient’s disease was diagnosed as AML with trilineage dysplasia concurrent with CLL. The simultaneous occurrence ofAML and CLL is extremely rare but should not be overlooked as a possible underlying cause of lymphocyte abnormalities inAML patients. Int J Hematol. 2002;75:187-190.©2002 The Japanese Society of Hematology
Key words: Chronic lymphocytic leukemia; Acute myeloid leukemia; Flow cytometry
Correspondence and reprint requests: Tsuyoshi Muta, MD,Department of Internal Medicine, Kyushu-Koseinenkin Hospital,Kishinoura 2-1-1, Yahatanishi-ku, Kitakyushu City 806-0034,Japan; 81-93-641-5111; fax: 81-93-642-1868.
ber 1. Physical examination on admission revealed neitherlymphadenopathy nor hepatosplenomegaly. The palpebralconjunctiva was anemic, but palpebral bulbi were not icteric.Chest auscultation indicated a slight ale on the right lung.Blood analysis on admission showed hemoglobin 10.7 g/dL,red blood cell count 2.99 � 106/mL, hematocrit 32.5%,platelet count 96 � 103/mL, and white blood cell count 6540/mL, with 1% banded neutrophils, 11% segmented neu-trophils, 76% lymphocytes, and 12% blasts. The blasts hadlarge nuclei, fine chromatin, prominent nucleoli, and abun-dant pale blue cytoplasm, some of which had dysplastic fea-tures (Figure 1A).The increased lymphocytes were small andmature and did not demonstrate cytoplasmic granulation(Figure 1A). Biochemical data showed a total bilirubin levelof 1.3 mg/dL, glutamic oxaloacetic transaminase (GOT)65 IU/L, glutamic pyruvic transaminase (GPT) 39 IU/L, lac-tic dehydrogenase (LDH) 971 IU/L, alkaline phosphatase327 IU/L, blood urea nitrogen 15.8 mg/dL, serum creatinine1.0 mg/dL, total protein 7.6 mg/dL, immunoglobulin (Ig)G2290 mg/dL, IgA 202 mg/dL, IgM 54 mg/dL, serum iron43 mg/dL, ferritin 750 ng/mL, haptoglobin 543 mg/dL, ery-thropoietin 154 mU, C-reactive protein 14.9 mg/dL, and sol-uble interleukin 2 receptor level 1440 U/mL. Human T-cellleukemia virus type 1 was serologically negative. The chestx-ray and the chest computed tomography revealed pneu-monia in the right lung. Ultrasonographic study of the

188 Muta et al / International Journal of Hematology 75 (2002) 187-190
Figure 1. A, May-Giemsa–stained film of peripheral blood. The blast cell and the small lymphocytes are indicated (original magnification �1000).B, May-Giemsa–stained film of bone marrow aspiration. The dysplastic features of myeloid cells are indicated (original magnification �1000). C, Themultinucleated erythroblast can be seen (original magnification �1000). D, The blast cells showed a diffuse peroxidase reaction but the small lympho-cytes did not (original magnification �1000).
abdomen revealed mild splenomegaly. Bone marrow aspira-tion revealed that 56.6% of nucleated cells were morpholog-ically small and mature lymphocytes and 49% of all nucle-ated cells without lymphocytes were blast cells. The subtypeof leukemia by the French-American-British (FAB) classifi-cation [6] was diagnosed as AML-M2. Myeloid and erythroiddysplastic features were noted (Figures 1B and C). The bonemarrow clot sections showed trilineage dysplasia. The blastcells were positive for myeloperoxidase (Figure 1D) and neg-ative for esterase stain. Using flow cytometric analysis, wewere able to distinguish and characterize the 2 malignant cellpopulations seen in this patient.
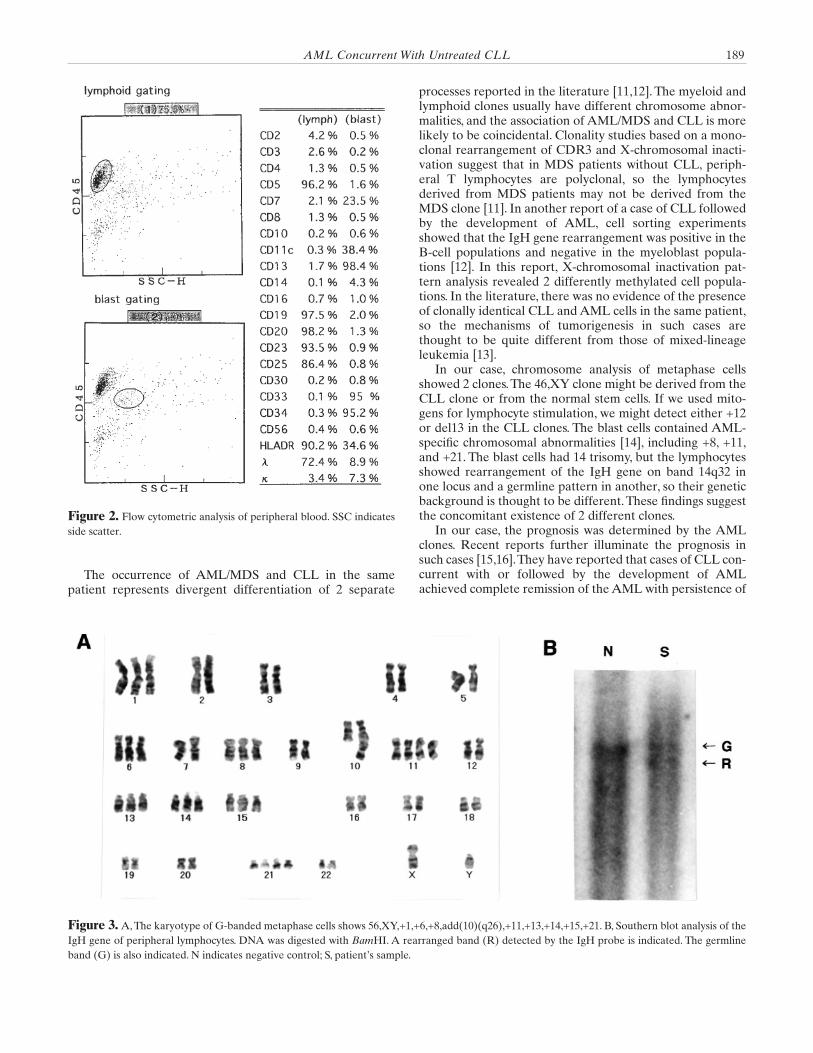
The blast cells of peripheral blood expressed CD13,CD33, and CD34 but not CD2, CD3, CD5, CD7, CD10, orCD19 (Figure 2). Some of the blast cells also expressedCD7, which is often detected in AML cells with frequentmonocytic differentiation and unfavorable prognosis [7].The increased peripheral lymphoid cells expressed CD5,CD19, CD20, CD23, CD25, and � chain but not CD2, CD3,CD7, CD10, CD13, CD33, or CD34. The cell surface pheno-type of bone marrow blasts and lymphocytes was the sameas the phenotype of peripheral blood. Southern blottinganalysis of peripheral lymphocytes revealed that IgH generearrangement was present (Figure 3B). Chromosomeanalysis of metaphase cells from the bone marrow showed
56,XY,+1,+6,+8,add(10)(q26),+11,+11,+13,+14,+15,+21,+21in 19 of 20 cells (Figure 3A) and 46,XY in 1 of 20 cells. Thepatient’s disease was diagnosed as AML (FAB M2) with tri-lineage dysplasia concurrent with CLL. The patient’speripheral lymphocyte counts were less than 10 � 103/mL,but the findings of bone marrow involvement and a mono-clonal CD5+ B-cell phenotype fulfill the B-CLL diagnosticcriteria [8].
The patient received antibiotics intravenously and recov-ered from the pneumonia. He refused a transfusion andchemotherapy because of his religious faith. The number ofperipheral blast cells increased more than 1 � 105/mL,whereas the lymphocyte counts did not change. He died of abrain hemorrhage on November 3, 2000.
3. Discussion
The incidence of AML/MDS in patients with previouslyuntreated CLL is quite rare. Robertson et al reported that,among 1374 CLL cases, only 3 patients who had received noprior alkylating agents presented with AML/MDS [9]. Flo-rensa et al reported that only 6 of 1198 primary untreatedMDS cases presented with B-CLL [10]. In Japan, ours is thefirst case of AML concurrent with untreated CLL reportedin the literature.
AML Concurrent With Untreated CLL 189
Figure 2. Flow cytometric analysis of peripheral blood. SSC indicatesside scatter.
Figure 3. A, The karyotype of G-banded metaphase cells shows 56,XY,+1,+6,+8,add(10)(q26),+11,+13,+14,+15,+21. B, Southern blot analysis of theIgH gene of peripheral lymphocytes. DNA was digested with BamHI. A rearranged band (R) detected by the IgH probe is indicated. The germlineband (G) is also indicated. N indicates negative control; S, patient’s sample.
The occurrence of AML/MDS and CLL in the samepatient represents divergent differentiation of 2 separate
processes reported in the literature [11,12]. The myeloid andlymphoid clones usually have different chromosome abnor-malities, and the association of AML/MDS and CLL is morelikely to be coincidental. Clonality studies based on a mono-clonal rearrangement of CDR3 and X-chromosomal inacti-vation suggest that in MDS patients without CLL, periph-eral T lymphocytes are polyclonal, so the lymphocytesderived from MDS patients may not be derived from theMDS clone [11]. In another report of a case of CLL followedby the development of AML, cell sorting experimentsshowed that the IgH gene rearrangement was positive in theB-cell populations and negative in the myeloblast popula-tions [12]. In this report, X-chromosomal inactivation pat-tern analysis revealed 2 differently methylated cell popula-tions. In the literature, there was no evidence of the presenceof clonally identical CLL and AML cells in the same patient,so the mechanisms of tumorigenesis in such cases arethought to be quite different from those of mixed-lineageleukemia [13].
In our case, chromosome analysis of metaphase cellsshowed 2 clones.The 46,XY clone might be derived from theCLL clone or from the normal stem cells. If we used mito-gens for lymphocyte stimulation, we might detect either +12or del13 in the CLL clones. The blast cells contained AML-specific chromosomal abnormalities [14], including +8, +11,and +21. The blast cells had 14 trisomy, but the lymphocytesshowed rearrangement of the IgH gene on band 14q32 inone locus and a germline pattern in another, so their geneticbackground is thought to be different. These findings suggestthe concomitant existence of 2 different clones.
In our case, the prognosis was determined by the AMLclones. Recent reports further illuminate the prognosis insuch cases [15,16].They have reported that cases of CLL con-current with or followed by the development of AMLachieved complete remission of the AML with persistence of

190 Muta et al / International Journal of Hematology 75 (2002) 187-190
the CLL population. In another report, it was also suggestedthat patients with CLL in whom AML/MDS develops had aprognosis similar to that other patients with AML/MDS [17].
In conclusion, we report a case of CLL concurrent withAML. The flow cytometry strategy, as reported in the litera-ture [18], was useful in evaluating the complex disease in thelymphocytes in our case. The immunodeficiency state associ-ated with CLL may have played a role in the subsequentdevelopment of AML, but further study is required to iden-tify the pathogenesis of such a case.
Acknowledgment
We thank Dr. Koichi Oshima, First Department of Pathol-ogy, School of Medicine, Fukuoka University, for clonalanalysis.
References
1. Foucar K. B Cell Chronic Lymphocytic Leukemia (CLL) and Pro-lymphocytic Leukemia. Baltimore, Md: Williams and Wilkins; 1991.
2. McPhedran P, Heath C.W. Acute leukemia occurring duringchronic lymphocytic leukemia. Blood. 1970;35:7-11.
3. Roberts PD, Forester PM. Chronic lymphocytic leukemia associ-ated with acute myelomonocytic leukemia. Br J Haematol. 1973;25:203-206.
4. Lawlor E, McCann SR, Whelan A, Greally J, Temperley J. Acutemyeloid leukemia occurring in untreated chronic lymphocyticleukemia. Br J Haematol. 1979;43:369-373.
5. Stern N, Shemesh J, Ramot B. Chronic lymphocytic leukemia ter-minating in acute myeloid leukemia. Cancer. 1981;47:1849-1851.
6. Bennet JM, Catovsky D, Daniel MT, et al. Chronic lymphocyticleukemia: proposal for the classification of the acute leukemias. BrJ Haematol. 1976;33:451-458.
7. Poeta GD, Stasi R, Venditti A, et al. CD7 expression in acutemyeloid leukemia. Leukemia Lymphoma. 1995;17:111-119.
8. Binnet JL, Catovsky D, Dighiero G, et al. Chronic lymphocyticleukemia: recommendations for diagnosis, staging, and responsecriteria. Ann Intern Med. 1989;110:236-238.
9. Robertson LE, Estey E, Kantarjian H, et al. Therapy-relatedleukemia and myelodysplastic syndrome in chronic lymphocyticleukemia. Leukemia. 1994;8(12):2047-2051.
10. Florensa L, Vallespi T, Woessner S, et al. Incidence and characteris-tics of lymphoid malignancies in untreated myelodysplastic syn-dromes. Leukemia Lymphoma. 1996;23:609-612.
11. Culligan DJ, Cachia P, Whittaker J, Jacobs A, Padua RA. Clonallymphocytes are detectable in only some cases of MDS. Br JHaematol. 1992;81:346-352.
12. Mitterbauer G, Schwarzmeier J, Mitterbauer M, et al. Myelodys-plastic syndrome/acute leukemia supervening previously untreatedchronic B-lymphocytic leukemia: demonstration of the concomi-tant presence of two different malignant clones by immunoligic andmolecular analysis. Ann Haematol. 1997;74:193-197.
13. Killick S, Matute E, Powles RL, et al. Outcome of biphenotypicacute leukemia. Haematologica. 1999;84:699-706.
14. Harrison CJ. The management of patients with leukemia: the roleof cytogenetics in this molecular era. Br J Haematol. 2000;108:19-30.
15. Barresi GM, Albitar M, Obrien SM. Acute myeloid leukemia,inversion 16, occurring in a patient with chronic lymphocyticleukemia. Leukemia Lymphoma. 2000;38(506):621-625.
16. Mateu R, Bellido M, Sureda A, et al. Concomitant chronic lym-phocytic leukemia and acute myeloid leukemia with an uncommonimmunophenotype. Am J Haematol. 1997;56281-56287.
17. Robertson LE, Estey E, Kantarjian H, et al. Therapy-relatedleukemia and myelodysplastic syndrome in chronic lymphocyticleukemia. Leukemia. 1994;8(12):2047-2051.
18. Gomez-Arbones J, Gallart MA, Mellado A, Marco V, Pandes MJ,Macia JM. Concomitant diagnosis of acute myeloid leukemia(AML) and chronic lymphocytic leukemia (CLL). Importance offlow cytometry in the diagnosis of CLL without lymphocytosisaccompanying AML. Eur J Haematol. 1997;59:335-337.