Embed Size (px)
Citation preview

Acute myeloid leukemia
Myelodysplastic
syndromes
Internal Medicine V.20.Febr.2019.
Ilona Tárkányi

Acute leukemia in adults
70% myeloid, 30% lymphoid
Average age at presentation is 60 years.
60% of the patients is older than 55-60 years.
Clinical presentation: deficiency of functional blood cells( anaemia, thrombocytopenia, neutropenia) or infiltration of the organs by immature leukemic blasts
>20% blasts on the bone marrow (BM is usually hypercellular, rarely hypoplastic).
Flow cytometry/ citochemistry is required for further classification (ALL/AML)- therapy is different!!!
Survival is just weeks or months without treatment

Clinical presentation ♦ Pancytopenia:
fever, infection, anaemia, bleeding
♦ Signs og malignant proliferation:
pain in the bones, lymphadenomegaly, meningeal signs
♦ Compression signs
(MYELOID SARCOMA!)

AML
M0
M2
M1
M4-M5b
M5a
FAB subtype NameAdult AML patients
(%)
M0Undifferentiated acute
myeloblastic leukemia5%
M1
Acute myeloblastic
leukemia with minimal
maturation
15%
M2
Acute myeloblastic
leukemia with
maturation
25%
M3Acute promyelocytic
leukemia10%
M4Acute myelomonocytic
leukemia20%
M4eos
Acute myelomonocytic
leukemia with
eosinophilia
5%
M5Acute monocytic
leukemia10%
M6Acute erythroid
leukemia5%
M7Acute megakaryocytic
leukemia5%

AML WHO classification
AML with recurrent genetic abnormalities:
• t(8;21), inv(16) or t(16;16), t(15;17), t(9;11), t(6;9), inv(3)or t(3;3), t(1;22)
AML with myelodysplasia-related change
Therapy-related myeloid neoplasms
AML, not otherwise specified: M0-M7
Myeloid sarcoma
Myeloid proliferations related to Down syndrome:
• Transient abnormal myelopoiesis
• Myeloid leukemia associated with Down syndrome (50x incidence !!!)


Therapy
High dose therapy with the aim of cure
Palliative- to decrease malignant cell burden
Best supportive care

Favorable
t(8;21) (q22;q22); RUNX1-RUNX1T1
inv(16) (p13.1q22) or t(16;16)(p13.1;q22); CBFB-MYH11
Mutated NPM1 without FLT3-ITD (normal karyotype)
Mutated CEBPA (normal karyotype)
Intermediate-I
Mutated NPM1 and FLT3-ITD (normal karyotype)
Wild type NPM1 and FLT3-ITD (normal karyotype)
Wild type NPM1 without FLT3-ITD (normal karyotype)
Intermediate-II t(9;11)(p22;q23); MLLT3-MLL
Adverse
inv(3) (q21q26.2) or t(3;3) (q21;q26.2); RPN1-EVI1
t(6;9) (p23;q34); DEK-NUP214
t(v;11) (v;q23); MLL rearranged
-5 or del(5q);
-7;
del17p;
complex karyotype; monosomal karyotype
AML ELN risk classification

High dose therapy in non-M3 AML
Induction: aim is complete remission (CR):
<5% blasts in BM, no blast and normal cell
count in PB (10E8 leukemic cells left!)
„7+3” protocol: AraC+anthracyclin
Postremission treatment: aim is elimination of
residual cells

High dose therapy in non-APL AML
Postremission treatment
HiDAC
AlloPBSCT
The incidence of CNS leukemia appears to have decreased since the
INCORPORATION OF HIGH DOSES OF CYTARABINE, during both initial induction
and post-remission therapy. PRIOR to the use of cytarabine, MENINGEAL
DISEASE developed in up to 20 percent of children and 16 PERCENT OF
ADULTS with AML. An estimate of the current incidence, based upon
patients treated at the author's center or in large clinical trials, IS LESS THAN
5 PERCENT of patients with AML overall.

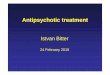
Graft sources

HLA class II HLA class I
antigens
DP DQ DR B C A
6 9 19 46 10 21
MHC (224 genes)
6
Human Major Histocompatibility Complex
B1 A1 B1 A1 B3
B4
B5
A1B1
alleles(DNA) 126 81 559 851 276 506
(2400)

HLA genotypically
identical sib
DP ACwDQ DR B
related
A/B/C
DR/DQ/DP
A/B/C
DR/DQ
12/12
10/10
A/B/DR 6/6
unrelated
A/B/C/DR 8/8

HLA matching
Donor age
CMV (-) for CMV(-) patients
Gender (male)
Pregnancy
ABO
Body mass

Much of the benefit of alloSCT is
due to immune GVL effect

Transplant related mortality
Early effects: – Infection, sepsis
– Mucositis (etoposid, MTX)
– Haemorrhagic cystitis (cyclophosphamid, adenovirus, BK virus)
– GVHD
– Graft failure
– Transplant related lung injury, interstitial pneumonitis (CMV)
– Venoocclusive disease (damage of sinosoidal endothelium-jaundice,
fluid retention)
– Transplantation associated thrombotic microangiopathy

Graft Versus Host Disease
Acute (<100 days)
skin-mucosa
gut
liver
Chronic
skin, eye, mouth, lung, liver, etc. oral ulcerations (lichen planus), keratoconjunctivitis sicca, xerostomia, polyserositis, esophagitis and stricture, intrahepatic obstructive liver disease, obstructive pulmonary disease, scleroderma, morphea,
fasciitis and myositis

Acut Promyelocytic Leukemia
FAB M3
Distinct entity: t(15;17) PML-RARa
RARa keeps DNA and ligand binding properties:
Co-repressors dissociate with farmacologic
doses of retinoids

APL
Clinical:
• BM infiltration with promyelocytes
• first signs are DIC/hyperfibrinolysis
Therapy:
„urgency leukemia”
All-trans retinoic acid (ATRA) in case of APL suspicion

APL therapyInduction + consolidation + maintenance
Protocol:
AIDA (ATRA+Idarubicin)+ risk-adapted consolidation therapy
ATRA+ATO (arsenic trioxide)
(first chemo free regimen!!)
Results: 90-95% Complete remission
CAVE: differentiation sy (fever, hypertension, oedema, pulmonal
infiltrate, pseudotumor cerebri)
Prevention of differentiation sy: Steroid

Treatment in patients over 60
Comorbidities: OH-Urea, haemosupportation
Low intensity chemotherapy:
hypomethylating agents: AzaC, Decitabin
sc low dose AraC
7+3 with doese reduction:
100-200 mg/m2 AraC + 45-60 mg/m2 daunorubicin
new agents: venetoclax

Cancer. 2013 Sep 15;119(18):3326-33..The demarcation between younger and older acute myeloid
leukemia patients: a pooled analysis of 3 prospective studies.Yanada M, Japan Adult Leukemia
Study Group.

Immunetherapy
Gemtuzumab Ozogamycin
FDA: 2017 September, first line and relapse

FLT3-ITD and FLT3-TKD

FLT3-ITD
Gale et al, 2005

FLT3-ITD
Gale et al, 2005


Treatment of adults with relapsed or refractory acute myeloid
leukemia (AML) with an isocitrate dehydrogenase-2
(IDH2) mutation
100 mg once daily until disease progression or unacceptable toxicity;
treat for a minimum of 6 months for response
Risk of differentiation syndrome (may be fatal if not treated)
Enasidenib

Ivosidenib
FDA approved ivosidenib (Tibsovo) for the treatment of adult
patients with relapsed or refractory AML with a susceptible
IDH1 mutation

ABT-199/ Venetoclax

On November 21, 2018, the FDA granted accelerated approval to
venetoclax in combination with azacitidine or
decitabine or low-dose cytarabine for the treatment of
newly-diagnosed acute myeloid leukemia (AML) in adults who are
age 75 years or older, or who have comorbidities
that preclude use of intensive induction
chemotherapy.

Glasdegib (Daurismo)
Glasdegib is approved for use in
combination with low-dose
cytarabine (LDAC) to treat
adults with newly diagnosed
AML who are age 75 and older
or who are ineligible for
intensive chemotherapy.

Glasdegib

Myelodysplasia
Clonal disease of haematopoietic stem cells: insufficient
haemopoiesis and dysplasia in one or more cell lines
Clinical:
-ineffective haematopoiesis (increased apoptosis)- cytopenia
and progressive BM insufficiency
-leukemic transformation is possible

Epidemiology:
Average age around 70 years
3/100000/year
Can be due to previous radio- or chemotherapy
30% leukemic transformation
Diagnosis:
♦Peripheral blood count
♦BM biopsy and aspiration
♦Cytogenetic evaluation
Other CAUSES HAVE TO BE EXCLUDED:
♦Vitamin (B12,folic acid) deficiency
♦Chr. Liver diseases
♦Malignant diseases
♦HIV
♦Autoimmune diseases
♦Ring sideroblasts: alcoholism, As or Pb exposition,
drugs, congenital haematopoietic diseases

Etiology
Familiar: rare
Therapy related (t-MDS)
CAUSE IS USUALLY UNKNOWN

Peripheral blood
Heterogenous disease
Sine qua non: Quantitative deficiency in one or more cell lines
Anaemia:
– Isolated cytopenia without anaemia is rare(<5%)
Leukopenia: ~50%
Trombocytopenia: ~25%
Pancytopenia: 50% at diagnosis

Morphology in PB:
RBC: anisocytosis
macro-ovalocytosis
basophilic punctation
Granulocyte:
deficient granulation
hypo- or hyperlobulated nuclei
Thrombocytopenia (except 5q-)
Blasts

RBC
Anaemia
Retikulocyte count is low
Normocytic or macrocytic
Elliptocytes, dacrocytes
2 different RBC poplutation could be observedNucleated RBCs

MDS:
WBCGranulocytopenia: ~50% at dg
Nuclei:– Decreased
segmentation(“pseudo-Pelger-Huët” anomaly)
– Ring form
Cytoplasm: decreased or absent granulation

Platelets
Thrombocytopenia: ~25% at diagnosis
– Isolated thrombocytopenia rare as first
presentation sign
Giant thrombocytes
5q- sy: thrombocytosis could be seen.

WHO classification
Refractory anaemia (RA): cytopenia in one or two cell lines,
blasts <5%, ring sideroblasts<15%
RA with ring sideroblast (RARS): ring sideroblasts >15%
Refractory cytopenia with dysplasia in two or more cell lines (RCMD):
>10% dysplastic cells, <5% blasts,
RAEB-1: 5-9% blasts
RAEB-2: 10-19% blasts
MDS/MPDS
Del(5q): Anaemia, blasts <5%, normal or elevated platelet count
(female predominance, transformation is rare)
>20% blasts =ACUTE LEUKEMIA

IPSS-R calculator: http://www.ipss-r.com


Pathogenesis of ring
sideroblasts
Cazzola M et al. Blood. 121(2):260-9

Treatment
♦ Supportive care: RBC and THR transfusion
Iron chelators: decreased organ damage and improved
hematological response
♦ Biologic response modifiers:
♦ Immune modulating agents (lenalidomide)
♦ Growth factors (Epo, G-CSF) TPO receptor antagonists???
♦ Immunosuppressive agents (cyclosporine, ATG)
♦ Hypomethylating agents (decitabin, azacitidin)
♦ High-dose chemotherapy
♦ AlloPBSCT

Therapeutic choices
Del5q: lenalidomide
Transfusion dependent, seEpo<500 U/l: Epo +/- G-CSF
Hypoplastic variant: ATG (anti-thymocyte globulin)/cyclosporin
Thr-penia/neutropenia, high risk: demethylating agents- Azacitidine, decitabin
High risk, suitable for high dose chemotherapy: chemotherapy -
alloPBSCT

Lenalidomide in del5q MDS