Embed Size (px)
Citation preview

Acute Myeloid Leukemia
ByAhmed Refaat Abd Elzaher
Assistant lecturer of Medical Oncology South Egypt Cancer Institute
Assuit University

HeterogeneousHeterogeneous clonal stem cell malignancy
Immature hematopoietic cells proliferate and accumulate in
BM, PB & other tissues features of BM failure.
Recently, certain CyG abnormalities classified as Recently, certain CyG abnormalities classified as
AML AML irrespective of blast count irrespective of blast count : : t(8;21)t(8;21), , inv(16)inv(16) and and t(15;17)t(15;17)
Definition & epidemiology
PB and/or BM blasts > 20 % of nucleated cell (NC) count
If the blasts in the BM are > 5% & < 20% MDS
Roboz G & Sung L. ASH-SAP 2010; PP 475Roboz G & Sung L. ASH-SAP 2010; PP 475

Acute myeloid leukemia
• Incidence – 2.7 per 100,000– median age of presentation : 65 yo
• AML comprises 90% of all acute leukemias in adults
• More prevalent:– Males– European – Hispanic (promyelocytic leukemia (AML M3)

AML - Etiology• Primary AML
– Increased incidence• Genetic fragility
– Faconi anemia– Down syndrome
• tobacco use?• herbicides?, pesticides?• benzene exposure
• Secondary AML– XRT – Topoisomerase II inhibitors (e.g etopisode), alkylating agents– MDS– other cell proliferation disorders
• CML, polycythemia vera, primary thrombocytosis, PNH


ACUTE LEUKEMIA
Diagnosis Clinical
Morphological
Immunophenotyping
Molecular genetics
Cytogenetics

Clinical presentation Sign or symptoms related to pancytopenia:
WBCinfection.Hb anemia.platelets bleeding
Approximately 25% of AML patients present with white blood cell (WBC) counts > 50,000/mm³
Monocytic variants (M4 or M5)
commonly display infiltration of gingivae,
skin, soft tissues or meninges
DIC is a common presentation in AML M3
M2 : Chloroma:-presents as a mass lesion ‘tumor of leukemic cells’

Leukostasis• Leukostasis – predominantly in those with WBC counts > 100,000 (10% of patients); can also be seen in patients with WBC > 50,000
– Most common in those with M4 or M5 leukemia
• Common symptoms
– Pulmonary: dyspnea, chest pain
– CNS: headaches, altered mentation, CN palsies, ocular symptoms
– Priapism
– Myocardial Infarction

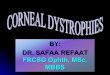
Gingival Infiltration in Gingival Infiltration in Monocytic AML (M4)Monocytic AML (M4)
After tt !After tt !

Diagnosis
Previously >30% blasts on BM aspirate (per FAB criteria)¹
Recently changed to > 20% blasts in the peripheral blood or BM (per WHO criteria)²
Patients with certain cytogenic abnormalities are considered to have AML regardless of blast percentage²
• t(8;21) (q22;q22), inversion (16) (p13q22)• t(16;16) (p13;q22), and t(15;17) (q22;q12)
1- Bennett et al, Br J Haematol 1976 2-Vardiman et al, blood 2002

FAB Classification of AML (1976)
M0: minimally differentiated M1: without maturation
M2: with maturation M3: hypergranular promyelocytic
30%
5%

M4: myelomonocytic M5a: Monoblastic
M6: erythroleukemia M7: megakaryoblastic
20%
30%
2-4%
M5b: monocytic
FAB Classification of AML (1976)

AML AML (WHO 2008)(WHO 2008)
Cytogenetics Cytogenetics & &
MolecularsMoleculars
FAB !FAB !ExcludingExcludingAPL (M3)APL (M3)
EXTREMELYEXTREMELYIMPORTANTIMPORTANT

(eg alklating agents, topoisom. II inhib., RT…) (eg alklating agents, topoisom. II inhib., RT…)
Therapy-related AML ….Therapy-related AML ….
WHO classificationWHO classification(2008) (2008)
((FAB excludingFAB excludingAPLAPL))
Poor prognosis… Poor prognosis… BAD cytogenetics BAD cytogenetics
AML with MDSAML with MDS

“Therapy-related AML:
Alkylating agents and radiotherapy
Topoisomerase II inhibitors
Onset 5-6 years post-exposure
1-5 years post-exposure
Ch abn. Of MDS Rearrangements of ch 11
MMAML

______________________ALL____________AML__________
• Myeloperoxidase - +
• Suddan black - +
• Non-specific esterase - + in M4, M5
• Periodic acid Schiff (PAS) + in B-ALL + in M6
• Acid phosphatase + in T-ALL + in M6
Bennett et al, Br J Haematol 1976
Cytochemistry

Immunophenotype• Based on blast surface
antigen expression • CD34
– Stem cell marker
• CD117, CD33, CD13, MPO
– Myeloid markers
• CD14, CD64
– Monocytic marker
• Glycophorin A
– Erythroid marker
• CD41, CD61
– Megakaryocytic markers

Qadir et al, Cytometry Part B: Clinical Cytometry,2006

Normal / Normal / t(9;11)t(9;11) Normal / Normal / t(9;11)t(9;11)
Roboz G & Sung L. ASH-SAP 2010; 475-487Roboz G & Sung L. ASH-SAP 2010; 475-487 Jabbour E et al. Mayo Clin Proc. 2006; 81:247Jabbour E et al. Mayo Clin Proc. 2006; 81:247
Others:Others: Complex (≥3 abnorm.), Complex (≥3 abnorm.), monosomal karyotype monosomal karyotype 5 or 7 5 or 7 (MK (MK 5 / 7 seems to be of the worst !) 5 / 7 seems to be of the worst !) t(9;22), t(6;11), abn(17). t(9;22), t(6;11), abn(17).
(Trisomy 8)(Trisomy 8)
(CBF)(CBF)

Rowe JM et al. Blood 2010;116:3147Rowe JM et al. Blood 2010;116:3147
AML in pts AML in pts less than 60 years less than 60 years of age:of age: Survival, by karyotype, of de novo and therapy-related (t-AMLSurvival, by karyotype, of de novo and therapy-related (t-AML) )
Grimwade D & Hills RK. Hematology ASH Educ Program 2009; 385–395Grimwade D & Hills RK. Hematology ASH Educ Program 2009; 385–395. .

Molecular genetics:Molecular genetics:
The field of biology that studies the structure and function ofThe field of biology that studies the structure and function of
genes at a moleculargenes at a molecular (atomic)(atomic) levellevel

““The most important prognostic indicators The most important prognostic indicators
in AML are age, cytogenetics, and in AML are age, cytogenetics, and
molecular genetics….”molecular genetics….”

& inv1620-30% of t(8;21)& 30-40% of inv16
The WORSTThe WORST
GOODGOOD
GOODGOOD
(BAD)(BAD)
(Intermediate risk)(Intermediate risk)

Frohling S et al. JCO 2004; 22:624Frohling S et al. JCO 2004; 22:624Preudhomme C et al. Blood 2002; Preudhomme C et al. Blood 2002; 100:2717100:2717
OS for AML patients with NC according to OS for AML patients with NC according to CEBPA mutation statusCEBPA mutation status
(similar results in two studies)(similar results in two studies)

cytogenetic markers revolutionized therapeutic decisions
favorable, intermediate & unfavorable.
However, patients tend to respond differentlyrespond differently to a specific
therapeutic approach within the same cytogenetic risk group`.
Molecular markers of AMLMolecular markers of AML. .
Remember…Remember…
Both the Both the NCCN and the ELN guidelines NCCN and the ELN guidelines recommend: recommend:
molecular genetics (mainly molecular genetics (mainly FLT3FLT3, , NPM1NPM1, C-Kit and , C-Kit and CEBPA)CEBPA) to to
further categorizefurther categorize cytogenetically normal patientscytogenetically normal patients…. More …. More
individualized decision making !individualized decision making !

Cytogenetics and Molecular Abnormalities


DNMT3A Mutations Common in Intermediate-Risk AML
• Mutations in the DNA methyltransferase gene, DNMT3A, are also associated with poor prognosis and are highly recurrent in patients with intermediate-risk AML. Presence of any DNMT3A mutation, either alone or in combination with the FLT3 internal tandem duplication (ITD) mutation, is associated with significantly shorter overall survival
Ley TJ, et al. ASH 2010. Abstract 99.

Isocitrate dehydrogenase (IDH ) :IDH1 and IDH2 mutations occur in 25–30% of patients with CN-AML, and in general predict for worse outcome in certain molecular (NPM1 wild-type) and clinical (older age) subsets of patients
Molecular markers of AMLMolecular markers of AML

Evaluation
● Cytogenetics are critical.
● Molecular diagnostics mandatory for all patients including the elderly: at least FLT3-ITD, NPM1, CEBPA; also consider C-KIT in patients with core-binding factor AML.
● Post-remission monitoring of minimal residual disease using cytogenetics, PCR, and multicolor flow cytometry.
● Send HLA typing of patient and siblings at time of initial diagnosis.


Assessment of response to treatment
CALGB Criteria Detection of minimal residual disease (MRD)
•Karyotyping
•FISH
•PCR
•Immunophenotyping
CR PR
•Clinical
•PB
•BM
MRD- MRD+

Criteria of response to treatment (CALGB)
Definition of CR
Clinical Peripheral blood Bone marrow
•TLC= 2-10 X 109/L– ANC > 1000
– No blasts
•HB > 11 (females)
> 12 (males)
•PLT > 100 000/m3
•P.S. = 100%
•No organomegaly
•Normocelluar•Blasts <5%
The presence of Auer rods is not allowed in CR marrow
NCCN Guidelines Version 2.2011

Essentially, routine practice nowadaysEssentially, routine practice nowadays for all AML pts !for all AML pts !
…previously !!previously !!

Treatment of AMLTreatment of AML
5) Special considerations5) Special considerations Elderly AMLElderly AML Concept of targeted therapy in AMLConcept of targeted therapy in AML
1) Supportive treatment (for all pts)1) Supportive treatment (for all pts)
2) Induction therapy2) Induction therapy
3) Post-remission (consolidation) therapy3) Post-remission (consolidation) therapy
4)4) Treatment of Relapsed AMLTreatment of Relapsed AML

Supportive treatmentSupportive treatment Hydration and allopurinol to prevent tumor lysis syndrome… esp Hydration and allopurinol to prevent tumor lysis syndrome… esp
initial cyto-reduction with HU (if TLC) initial cyto-reduction with HU (if TLC)
Availability of “full” neutropenic precautions Availability of “full” neutropenic precautions
Insertion of a central line to deliver chemotherapy . Insertion of a central line to deliver chemotherapy .
Blood and platelets transfusion Blood and platelets transfusion
Oral care and nutritional adviceOral care and nutritional advice
Antimicrobials (prophylactic / therapeutic) Antimicrobials (prophylactic / therapeutic)
Sperm bankingSperm banking
Hormonal therapy to control menses during time of Hormonal therapy to control menses during time of
thrombocytopenia.thrombocytopenia.

To begin with, till this very To begin with, till this very moment…. It is still themoment…. It is still the: :
““3 + 7” regimen (from the 1970s …..!!)3 + 7” regimen (from the 1970s …..!!)
Anthracycline X 3d Anthracycline X 3d (usually Daunorubicin) (usually Daunorubicin)
AraC (Cytarabine) X 7dAraC (Cytarabine) X 7d
Although AML…heterogeneous Same tt Although AML…heterogeneous Same tt
approach (except APL)… ! approach (except APL)… !

Induction Treatment Of AMLInduction Treatment Of AML
• Dauno 45mg/m2 D 1-3 I.V
• AraC 100 / 200100 / 200 mg/m2 D 1-7 C.I
Standard DA (3+7)
Initially Initially
No Difference No Difference in OSin OS
BUT …BUT …

(Fernandez HF et al. NEJM 2009; 361:1249)(Fernandez HF et al. NEJM 2009; 361:1249)

IdarubicinIdarubicin (10 or 12mg/m2 X 3d) OROR
MitoxantroneMitoxantrone 12mg/m2 X 3d
Which anthracycline ?Which anthracycline ?
NO advantage over the higher doses of DaunoNO advantage over the higher doses of Dauno
(i.e 60 or 90)(i.e 60 or 90)


Day 14 BMDay 14 BM Blasts <5% wait till CBC recovery
Blasts >5% & < 50% of initial blasts initial blasts 2nd 3+7 (if tolerable & NO active infection)(if tolerable & NO active infection)
Blasts > 50% of initial blasts initial blasts Salvage (eg HAM / FLAG-M)
Upon CBC recoveryUpon CBC recovery BM BM
Day 14 BMDay 14 BM Blasts <5% wait till CBC recovery
Blasts >5% & < 50% of initial blasts initial blasts 2nd 3+7 (if tolerable & NO active infection)(if tolerable & NO active infection)
Blasts > 50% of initial blasts initial blasts Salvage (eg HAM / FLAG-M)
Upon CBC recoveryUpon CBC recovery BM BM
Still with remission inductionStill with remission inductionStill with remission inductionStill with remission induction
((NadirNadir) )

Treatment of AMLTreatment of AML
5) Special considerations5) Special considerations Elderly AMLElderly AML Concept of targeted therapy in AMLConcept of targeted therapy in AML
1) Supportive treatment (for all pts)1) Supportive treatment (for all pts)
2) Induction therapy2) Induction therapy
3) Post-remission (consolidation) therapy3) Post-remission (consolidation) therapy
4) Treatment of Relapsed AML4) Treatment of Relapsed AML

• Rational: eradicate residual Leukemic clone
Consolidation therapy: Consolidation therapy: “EXTREMELY” crucial…..“EXTREMELY” crucial…..

Consolidation after CRConsolidation after CR(exclusively… (exclusively… cytogeneticscytogenetics) )
AML (1AML (1stst CR) CR)
Good riskGood risk HiDAC x 3-4HiDAC x 3-4
Intermed. Intermed. riskrisk
Allo-HSCT Allo-HSCT OROR HiDACHiDAC
Poor riskPoor risk Allo-HSCT Allo-HSCT OROR clinical trialclinical trial
Two meta analyses superiority of Allo in these risk groups: Two meta analyses superiority of Allo in these risk groups: 1)1)Cornelissen J et al. Blood 2007; 109:3658Cornelissen J et al. Blood 2007; 109:36582)2)Koreth A. et al. JAMA 2009; 301:2349Koreth A. et al. JAMA 2009; 301:2349

Current factsCurrent facts
The new era of The new era of molecular incorporationmolecular incorporation…. ….
therapeutic map is changingtherapeutic map is changing
(Few grey zones...!)(Few grey zones...!)

FavorableFavorableNo role for HSCT,No role for HSCT,
EXCEPT:EXCEPT:
Those with a Those with a mutation inmutation in c-c-
KIT KIT ((eg with CBF eg with CBF t t 8;218;21) ) or FLT3or FLT3
45% of AML, mostly 45% of AML, mostly cytogenetically cytogenetically
normal (CN)normal (CN)
IntermediateIntermediate
Allo-HSCT for allAllo-HSCT for all EXCEPTEXCEPT mutant mutant NPM1 NPM1 but but FLT3FLT3--
ITD -veITD -ve OROR CEBPA+veCEBPA+ve
Allo-HSCT Allo-HSCT for allfor all
UnfavorableUnfavorable

Post-remission therapy for adults with newly diagnosed AML (except APL)
Induction by (3+7) irrespective of risk group
CR
Favorable risk Intermediate/unfavorable risk
HD ARA-C containing regimen X 3 cycles
Relapse
2nd induction
Donor present
No donor
Allo BMT in CR2
ABMT in CR2
Donor present
No donor
Allo BMT in CR1 as soon as possible
HD ARA-C containing
regimen X 3
ABMT in CR1
Relapse
Palliative therapy


Treatment of special forms of AML
AML M5
High Risk Of CNS DiseaseAfter reaching CR by induction chemotherapy, give triple intrathecal prophylaxis:
• MTX 15 mg
• ARA-c 40 mg
• Dexamethazone 4 mg
• MTX 15 mg
• ARA-c 40 mg
• Dexamethazone 4 mg
Every 8 weeks for a total of 6 injections.

Treatment of AML in Eldery

Treatment of AML in Eldery

HAM
Treatment of relapsed AML
Mitoxantrone
ARA-c 1 gm/m2 (3hrs infusion) /12 hrs.
12 mg/m2 I.V. short infusion.
Days
3-5
1-3

HAM
Treatment of relapsed AML
- High dose ARA-c should not be given over a period shorter than 3 hours :
- Prophylaxis ARA-C induced chemical conjunctivitis (excreted in tears) :
Dexamethazone eye drops (e.g. Isoptodex): 2 drops in each eye qid day 1-7.
Due to enteritis problem
- Antiemetic ttt
Zofran 16-32 mg C.I. or I.V. (2-4 amp.).

Treatment of relapsed AML
AVVV
VP 16
ARA-c 100 mg/m2 C.I.
100 mg/m2 I.V.
Days
12
1-7
Vincristine 2 mg ...……I.V.
1-5
10
Velbe 10 mg …… I.V.

Treatment of relapsed AML
FLAG Days
ARA-c*
Fludarabine 25 mg/m2
1gm/m2/12 hrs
1-5
G-CSF** 200 gm /m2
1-5
D0 ANC >1000
1 hr inf.
3 hrs inf.
S.C.
*ARA-c should be given at least 4 hrs after Fludarabine to modulate pharmacokinetics of ARA-c (++ level of ARA-CTP in blast cells).
** Our experience is either to drop G-CSF or to start it on day +6

Epigenetic changesEpigenetic changes (Heritable modifications in gene function or activity without (Heritable modifications in gene function or activity without
changes in DNAchanges in DNA sequence)sequence)
• DNA hypermethylationDNA hypermethylation
• Histone deacetylationHistone deacetylation
Gene silencing…”switching off”Gene silencing…”switching off”
(tumor suppressor genes) (tumor suppressor genes)
Carcinogenesis Carcinogenesis
REVERSIBLE ! REVERSIBLE !
HistoneHistoneDeacetylationDeacetylation
Inhibitors Inhibitors (HDACi)(HDACi)
Hypomethylating Hypomethylating agents… agents… AZA / AZA /
DECDEC

It is easy to kill cancer It is easy to kill cancer cells, but the challenge is cells, but the challenge is
keeping the patient alive at keeping the patient alive at the same time…..!the same time…..!

Thank You