Embed Size (px)
Citation preview
Acute Ophthalmology
F DeanConsultant Ophthalmologist
Aims of the session
• Anatomy of the eye and orbit• Ophthalmic history, examination and
assessment• Ophthalmic triage• Conditions –true emergencies• Using an ophthalmoscope
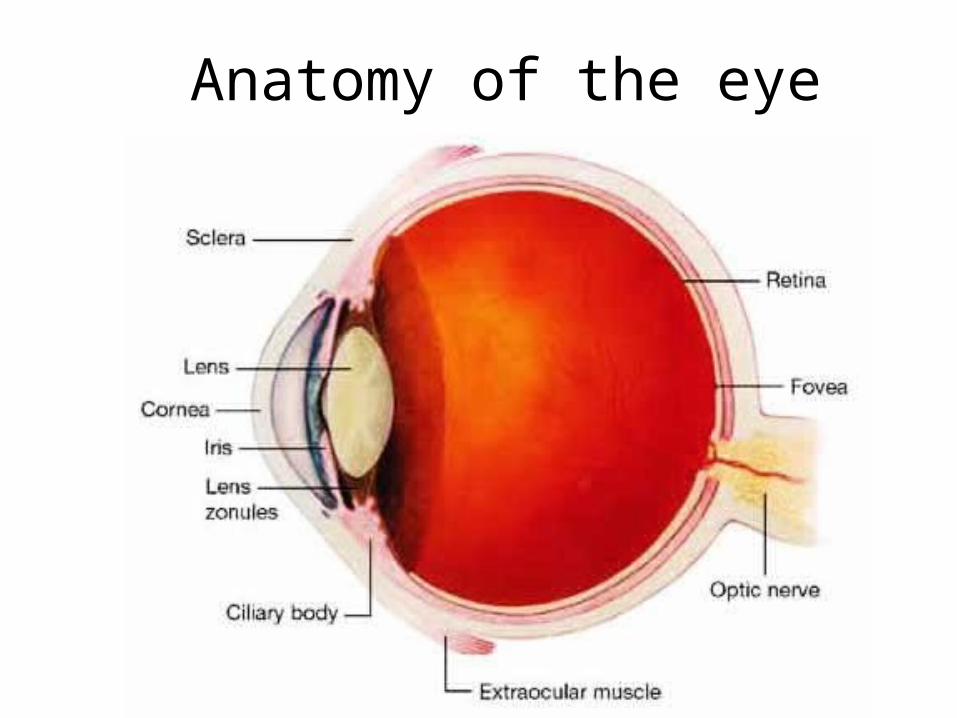
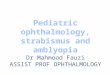
Anatomy of the eye
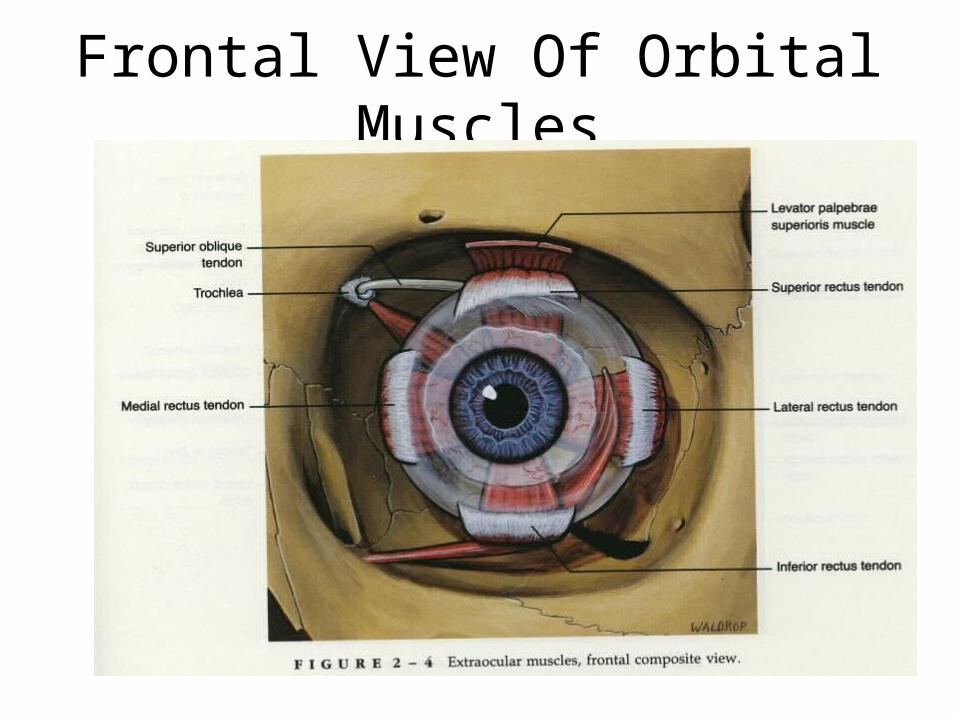
Frontal View Of Orbital Muscles
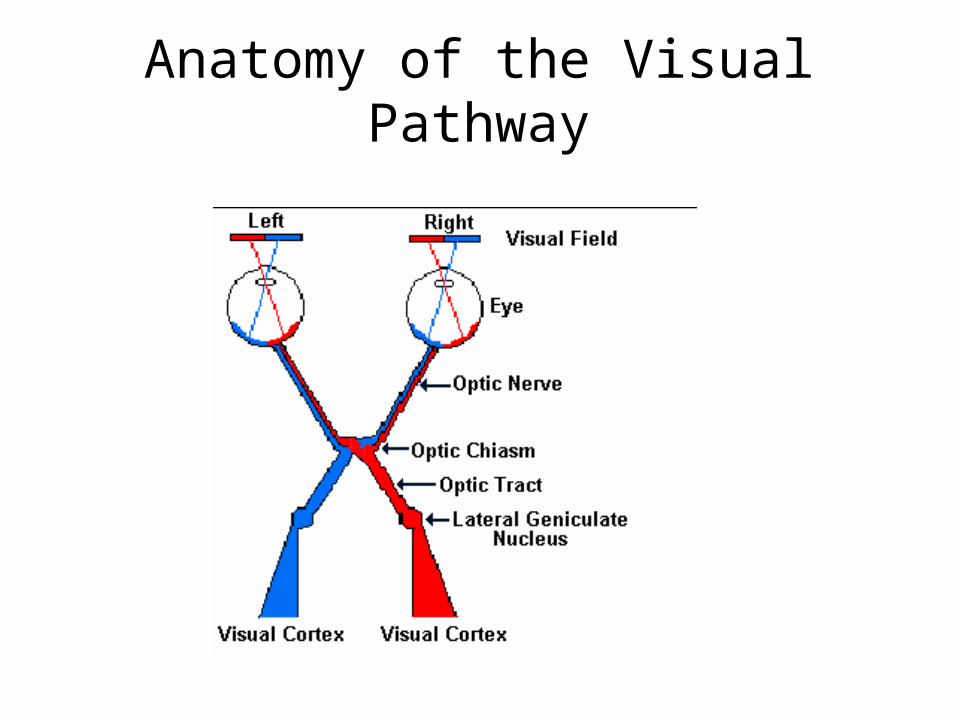
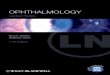
Anatomy of the Visual Pathway
Taking the history
What symptoms may be specific to the eye?
• Red/sore/watering/itchy/burning/hot• Aching
• Can’t see– Intermittent– Complete or partial
• Double vision • Funny vision- flashes/floaters/distortion
Ophthalmic History
Loss of Vision• rate of loss• near or distance• total blurr or part blurr
– general loss = loss of acuity– part loss = loss of visual field
• associated features e.g distortion, floaters, flashing lights, pain etc
Ophthalmic Symptoms from different structures
• Eyelid-itchy, burning,dry• Conjunctiva- watery,sticky, burn, sore• Eye ball- aching, visual disturbance,
floaters• Orbit- watery, ache• Brain- headache, visual disturbance,
photopsia, diplopia
Pain
Pain• Type of pain
– Gritty sandy feeling = ocular surface– Ache within the eye = deeper tissue involvement
e.g. uveal tissues
• duration• precipitating or relieving factors• Location/radiation
History
• Past medical history• Social history• Drug history• Family history
General History
• Diseases with known ocular associations– Diabetes, atherosclerosis, collagen vascular
disease, – Hypertension– Meningitis– Raised intracranial pressure
Eye Examination
• Visual acuity.• Examination of the
– Lids– Cornea and conjunctiva– Pupils– Red reflex/lens– Fundus
• Examination of the eye movements• Examination of the fields
Visual Acuity
• Logmar acuity Newspaper for near vision
• With spectacle correction as required
• With and without a pinhole
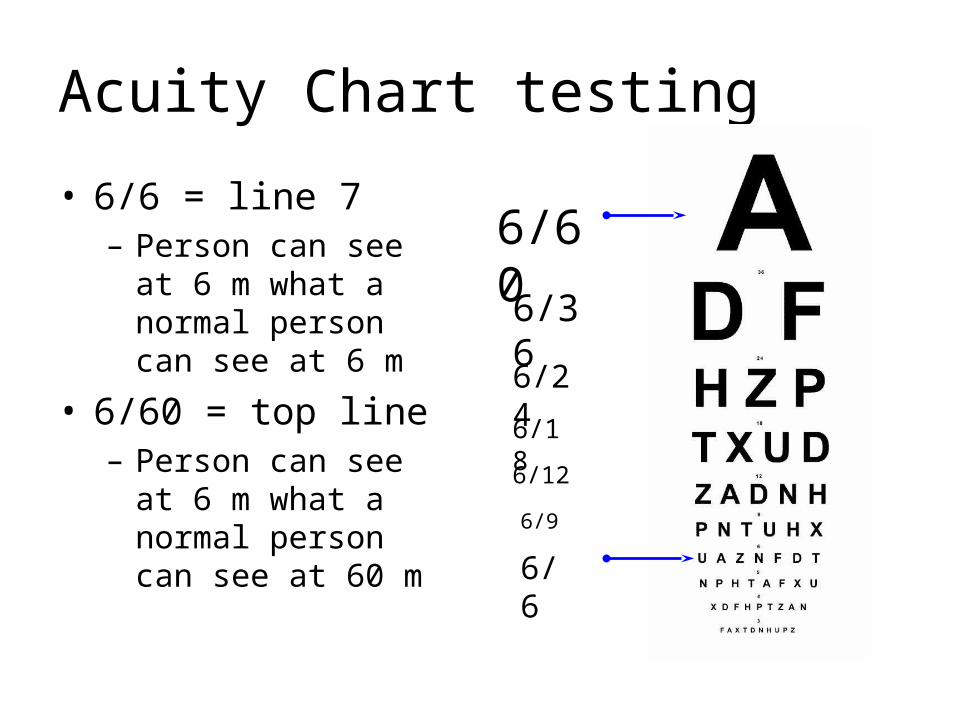
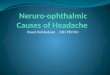
Acuity Chart testing
• 6/6 = line 7– Person can see at 6 m
what a normal person can see at 6 m
• 6/60 = top line– Person can see at 6 m
what a normal person can see at 60 m
6/60
6/6
6/36
6/24
6/18
6/12
6/9
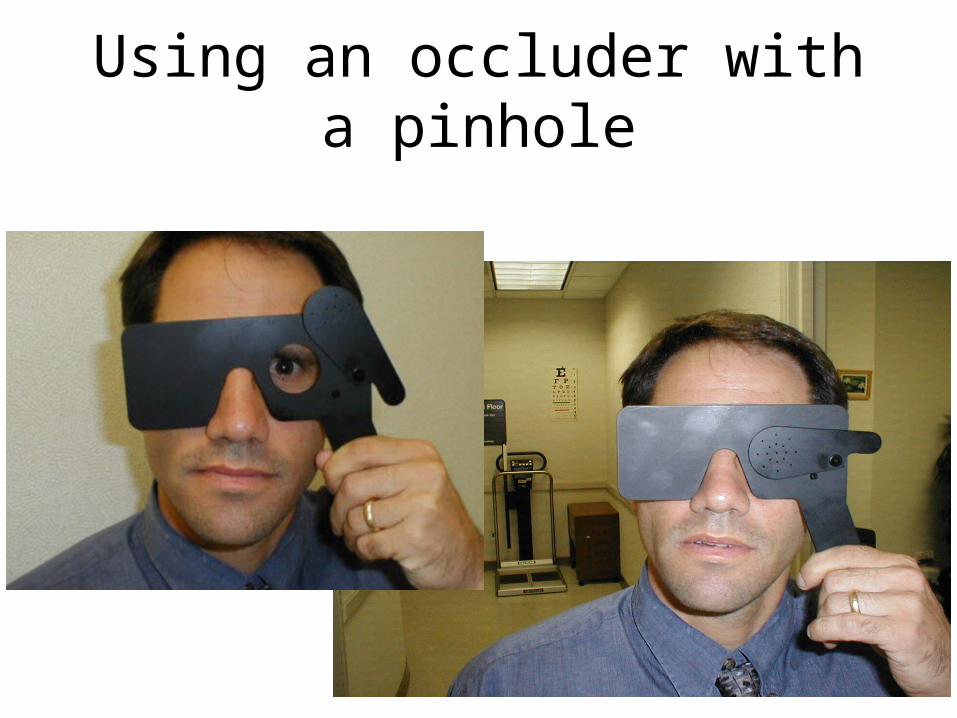
Using an occluder with a pinhole
Ophthalmic examination
• Visual acuity.– With and without
glasses
• Examination of the – Lids– Cornea and conjunctiva– Pupils– Red reflex/lens– Fundus
• eye movements• Visual fields
Topical Medication for Examination
• To check for break in epithelium– Fluorescein
• Local anaesthetic – Benoxinate 0.4%
• For pupil dilation – Tropicamide 0.5%– Phenylephrine 2.5%
External Eye
• Use good general illumination e.g angle poised lamp• Pen torch pencil beam for tangent illumination +
fluorescein stain• Use topical anaesthetic when required for patient
comfort• Start with eyelids, then conjunctiva, cornea and pupil
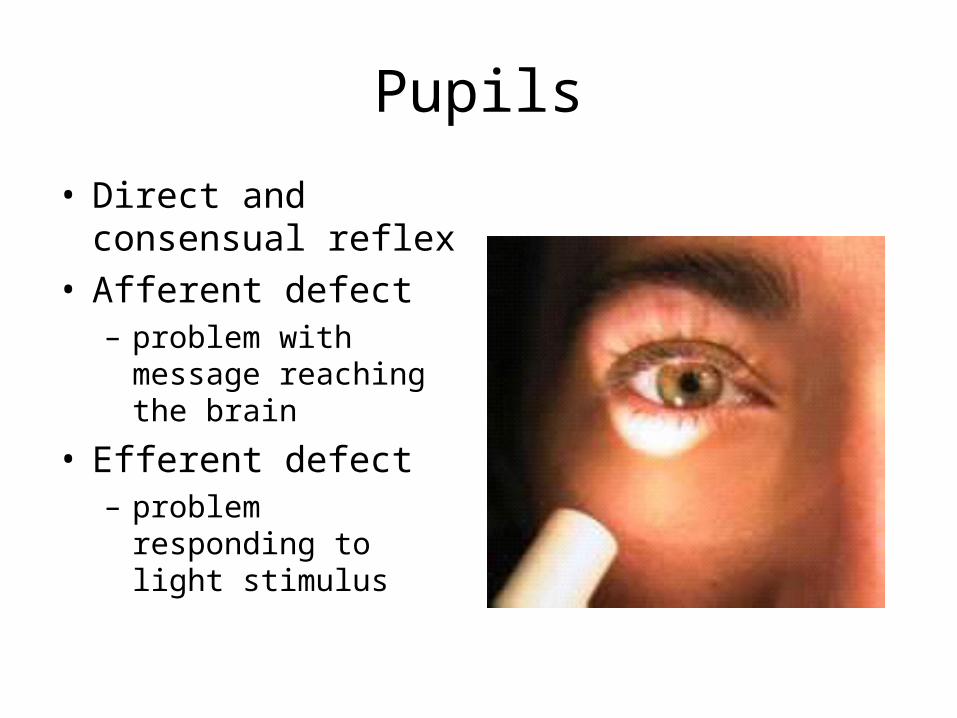
Pupils
• Direct and consensual reflex
• Afferent defect– problem with message
reaching the brain
• Efferent defect– problem responding to
light stimulus
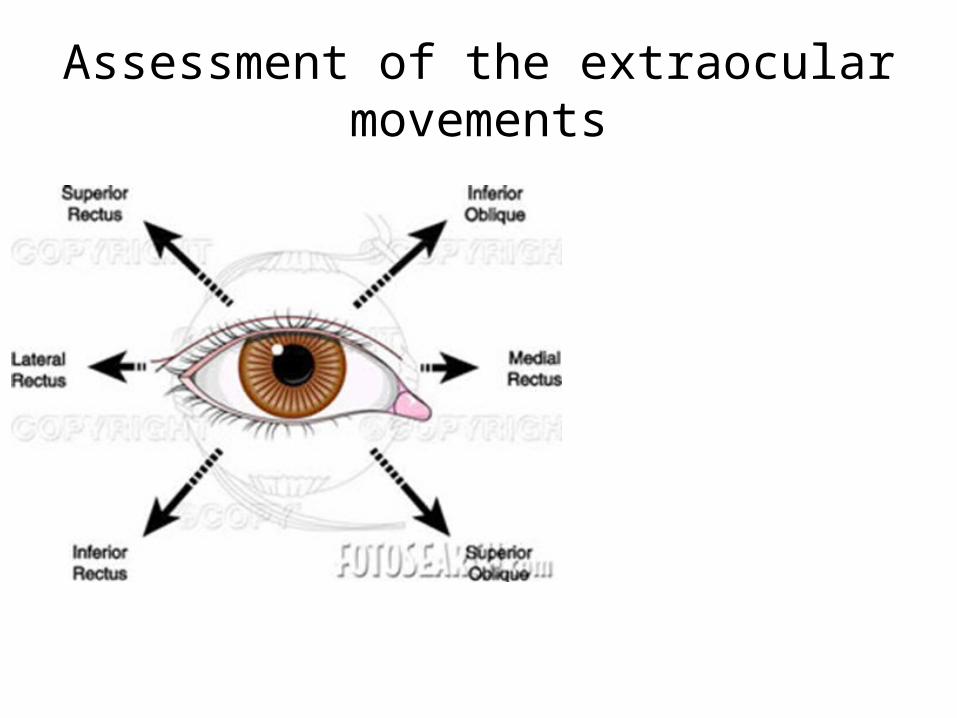
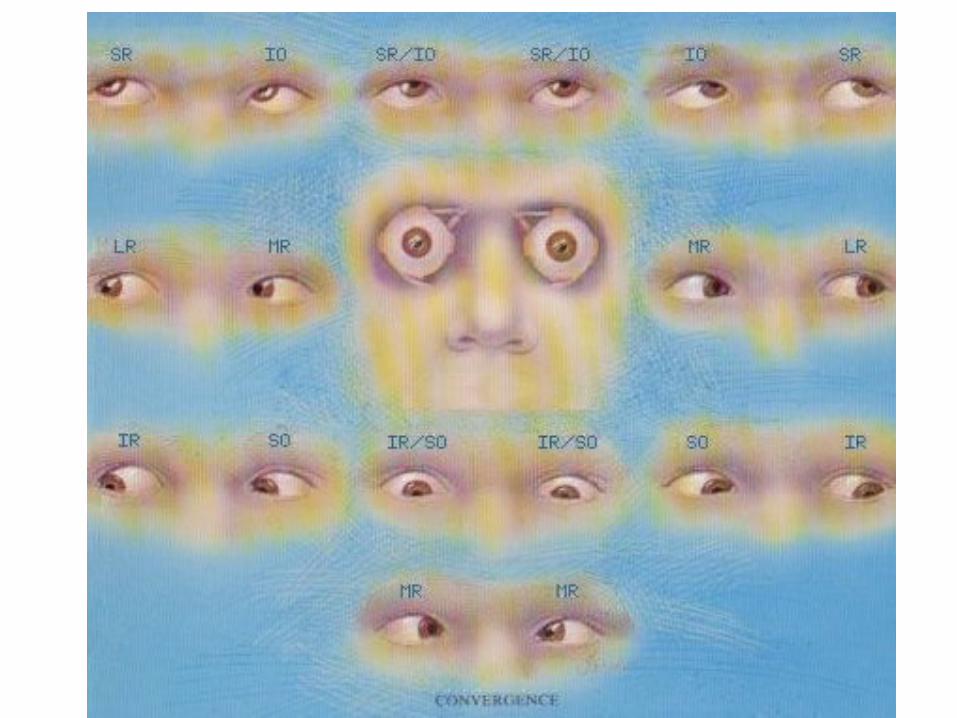
Assessment of the extraocular movements
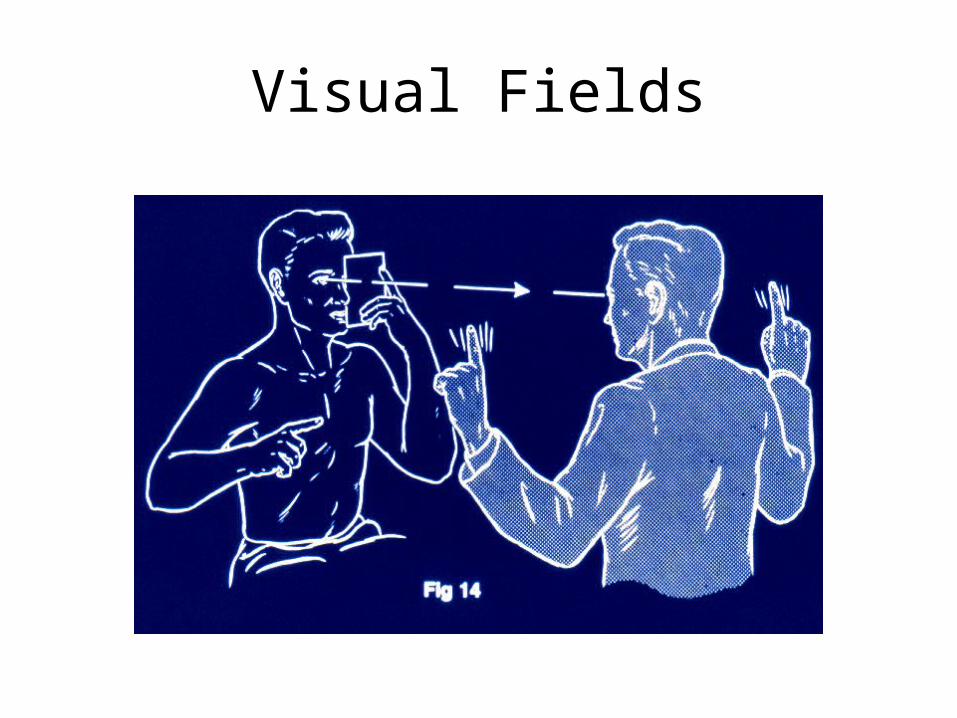
Visual Fields
Assessment of Squint
• Monocular vision – may have amblyopia (lazy eye)
• Eye movements– is there any restriction of movement– is there any double vision
• Cover Test– check for ocular deviation
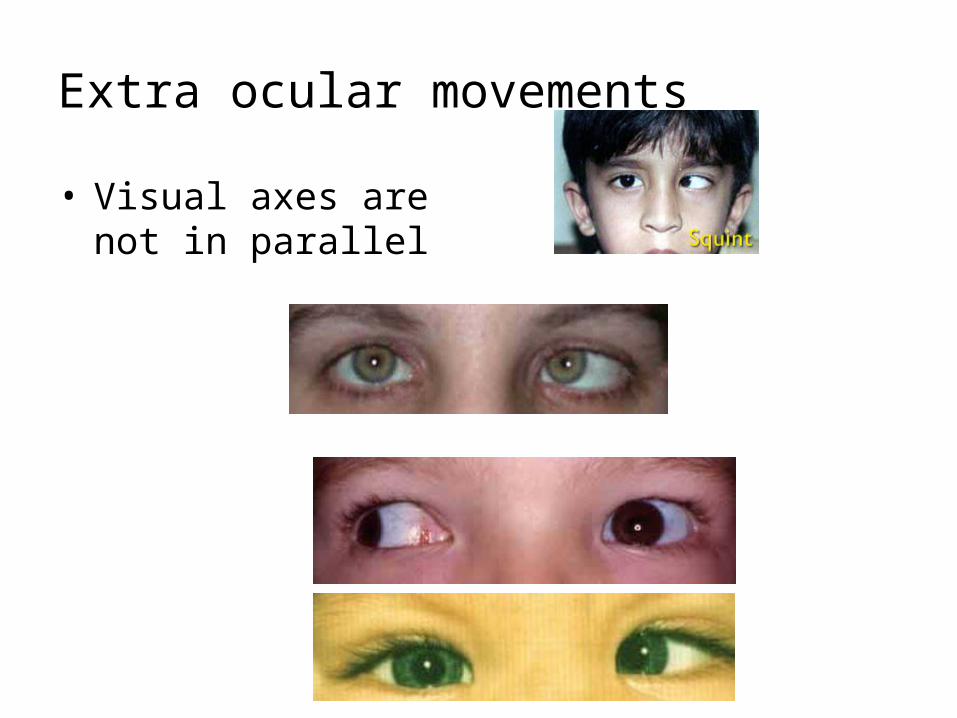
Extra ocular movements
• Visual axes are not in parallel
Ophthalmoscopy
• Don’t be afraid to DILATE the pupil
• Correct for refractive errors
• Use the optic disc as a landmark and follow the arcades
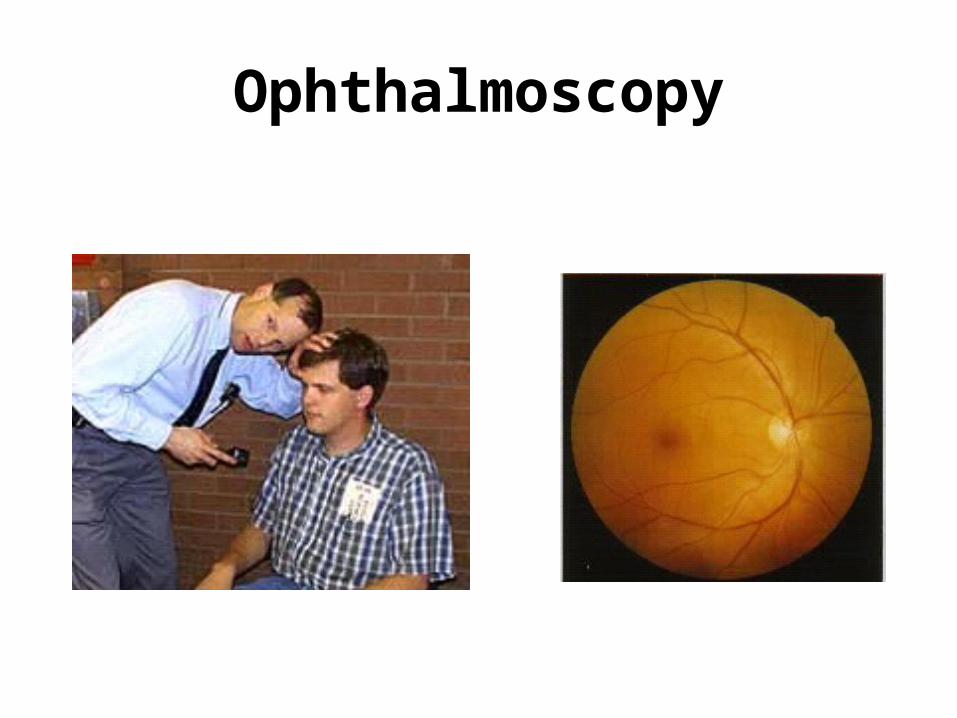
Ophthalmoscopy
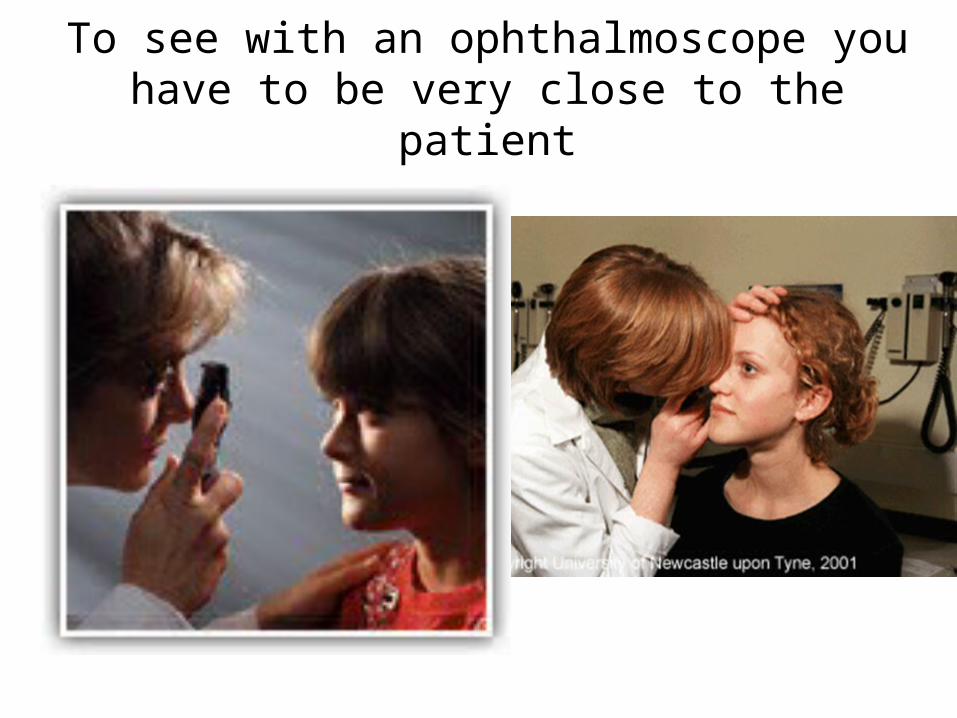
To see with an ophthalmoscope you have to be very close to the patient
What is Triage?
A process by which a patient is assessed upon arrival to determine the urgency of the problem and to
designate the appropriate healthcare resources to care for the identified
problem
Aim of Triage System
• Realistic priorities of care are determined which result in appropriate, efficient and effective service delivery
Discriminators
• General • Specific
General Discriminators
• Life Threat• Pain• Haemorrhage• Conscious level• Temperature• Acuteness
General Discriminator
• Ophthalmic patients with pain in pain in conjunction with specific discriminators.conjunction with specific discriminators.
Specific Discriminators
• Chemical eye injury• Penetrating eye trauma• Sudden loss of vision• Reduced visual acuity• Inappropriate history• Red eye with abnormal pupil reaction
Specific discriminators
• Chemical eye injury– Acid– Alkali– molten metal– CS gas
Specific discriminators
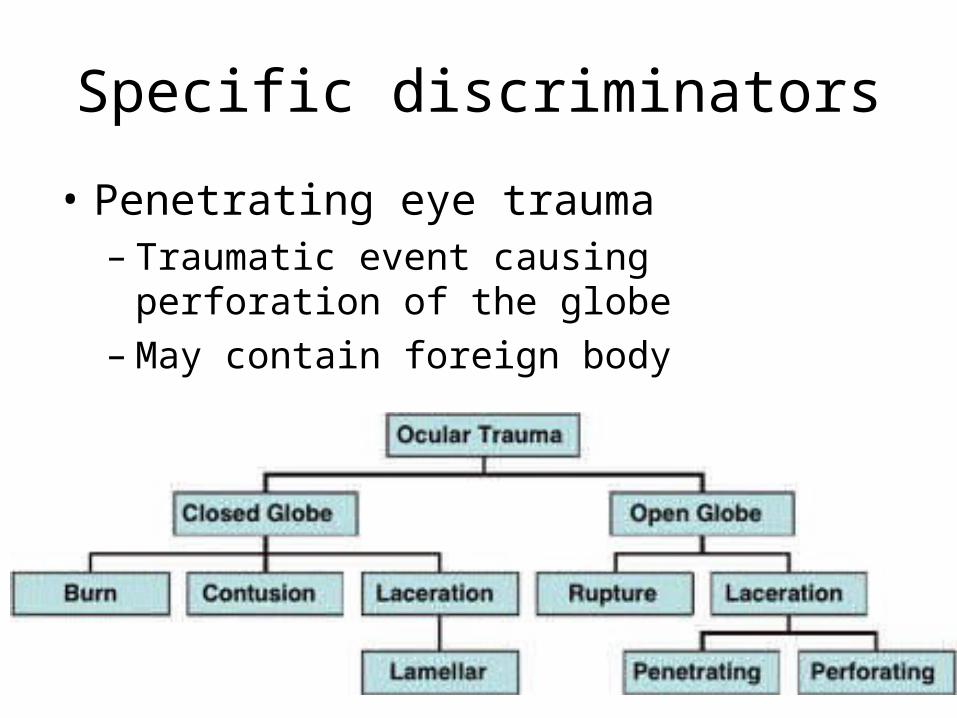
• Penetrating eye trauma– Traumatic event causing perforation of the globe– May contain foreign body
Specific discriminators
• Sudden complete loss of vision– loss of vision in one or both eyes within the
preceding 24 hours
– Normally vascular
Specific discriminators
• Reduced Visual acuity– corrected visual acuity loss.
Specific discriminators
• Inappropriate history– alleged mechanism of injury does not fit the injury

Specific discriminators
• Red eye– with or without pain– complete or partially red
Discriminators
• In addition to specific discriminators add• Pupil reaction• Shape• Size
Specific discriminators
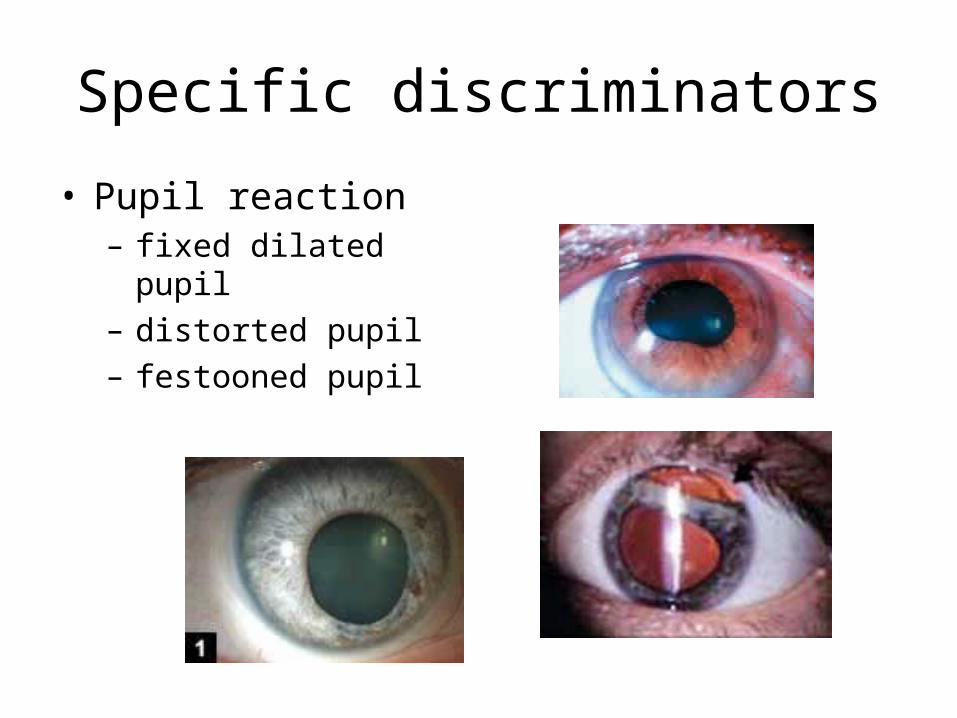
• Pupil reaction– fixed dilated pupil– distorted pupil– festooned pupil
Red Flags
• Ocular pain- particularly deep ache• Visual loss• Bleeding
• Always refer when pain and visual loss are present simultaneously.

MANCHESTER TRIAGE DISCRIMINATORS
(OPHTHALMIC)
Categories
• Red• Orange• Yellow• Green• Blue
RED CATEGORY
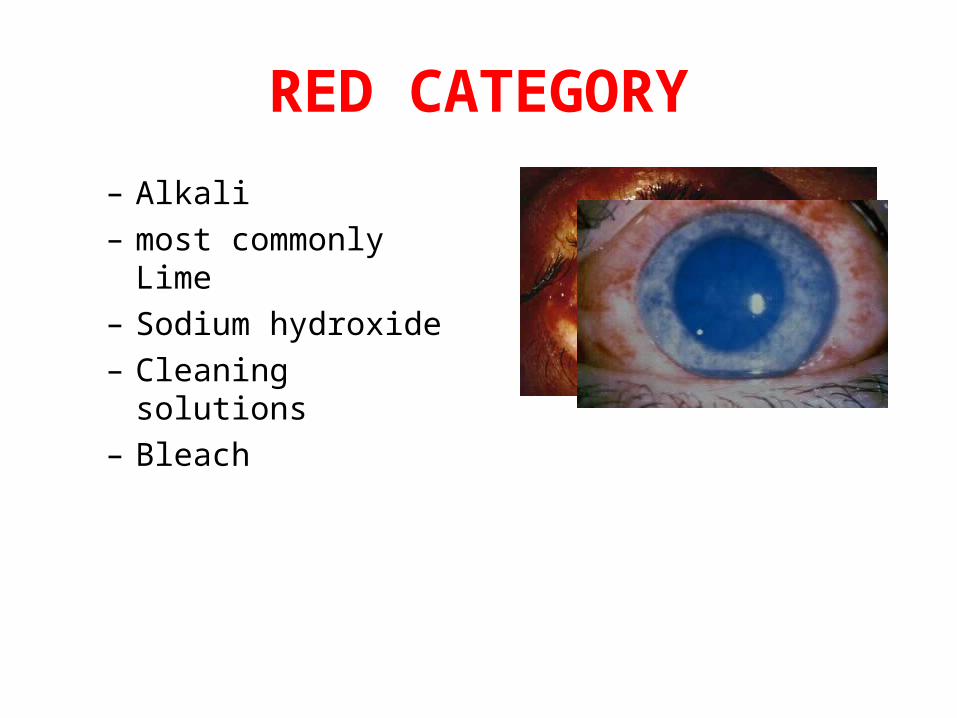
– Alkali– most commonly Lime– Sodium hydroxide– Cleaning solutions– Bleach

Chemical Injury
• Alakali injury• Other chemical injury.
RED CATEGORY
– Acid eg battery– molten metal– CS gas
ORANGE CATEGORY
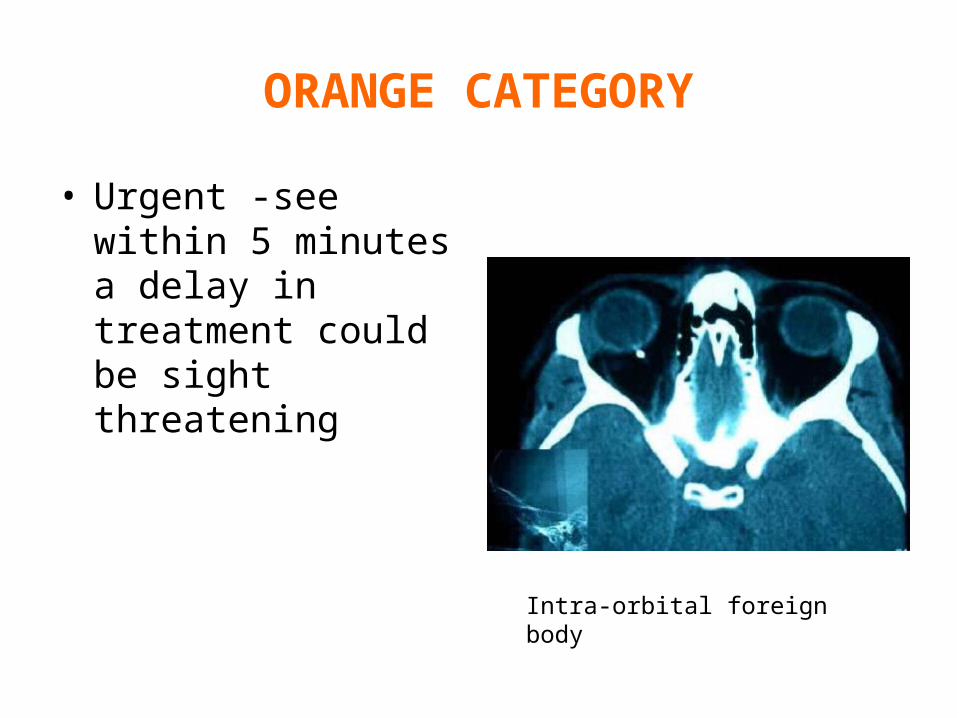
• Urgent -see within 5 minutes a delay in treatment could be sight threatening
Intra-orbital foreign body
ORANGE CATEGORY
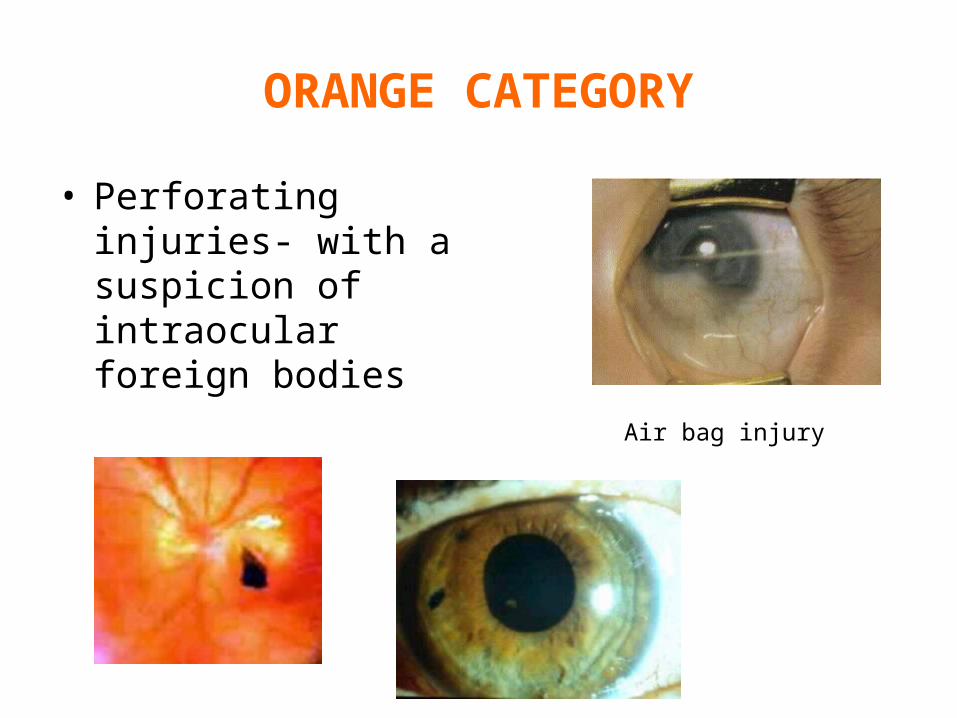
• Perforating injuries- with a suspicion of intraocular foreign bodies
Air bag injury
ORANGE CATEGORY
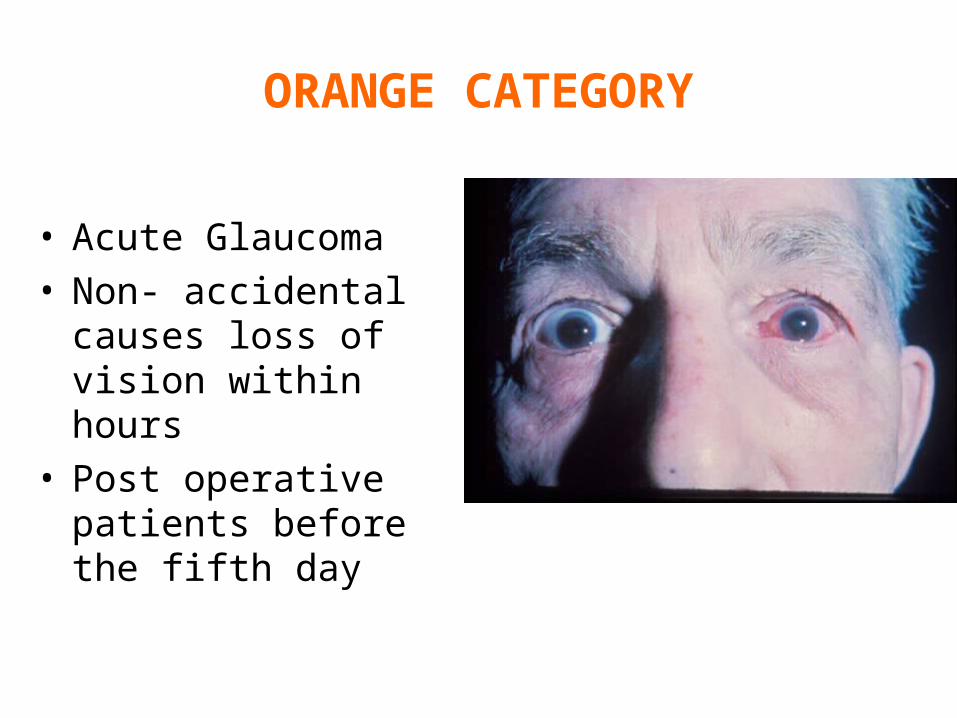
• Acute Glaucoma• Non- accidental
causes loss of vision within hours
• Post operative patients before the fifth day
ORANGE CATEGORY
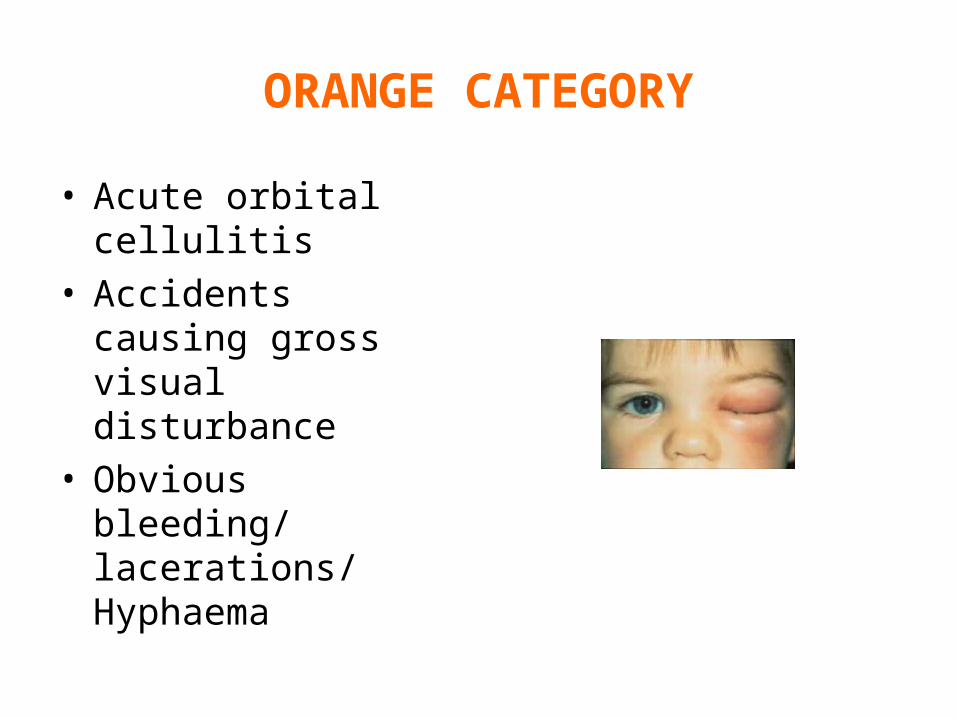
• Acute orbital cellulitis• Accidents causing gross
visual disturbance• Obvious bleeding/
lacerations/ Hyphaema
ORANGE CATEGORY
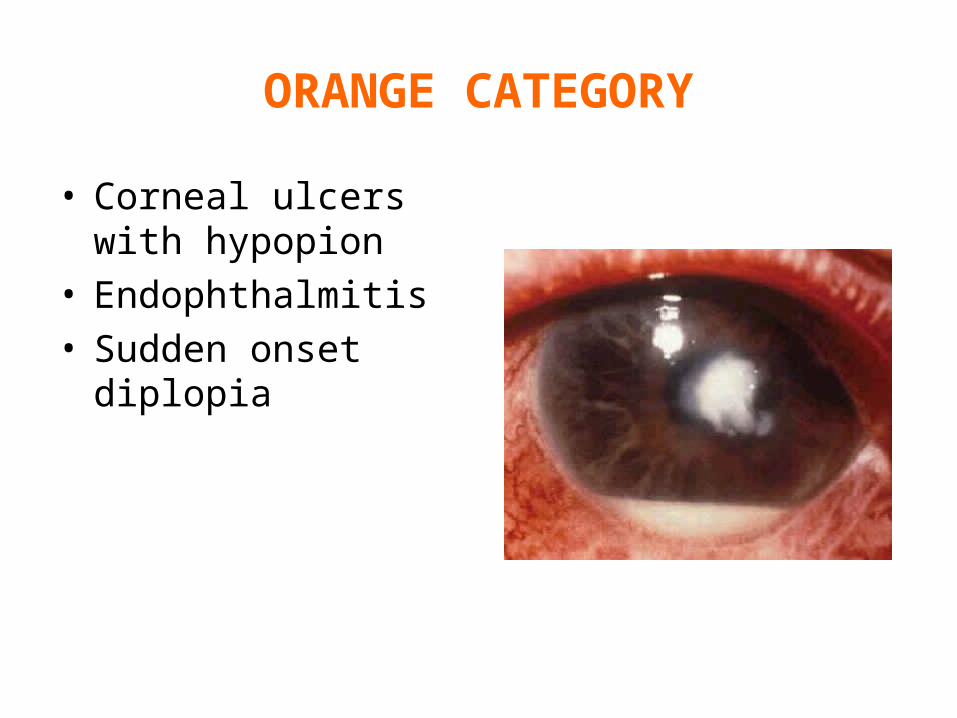
• Corneal ulcers with hypopion
• Endophthalmitis• Sudden onset diplopia
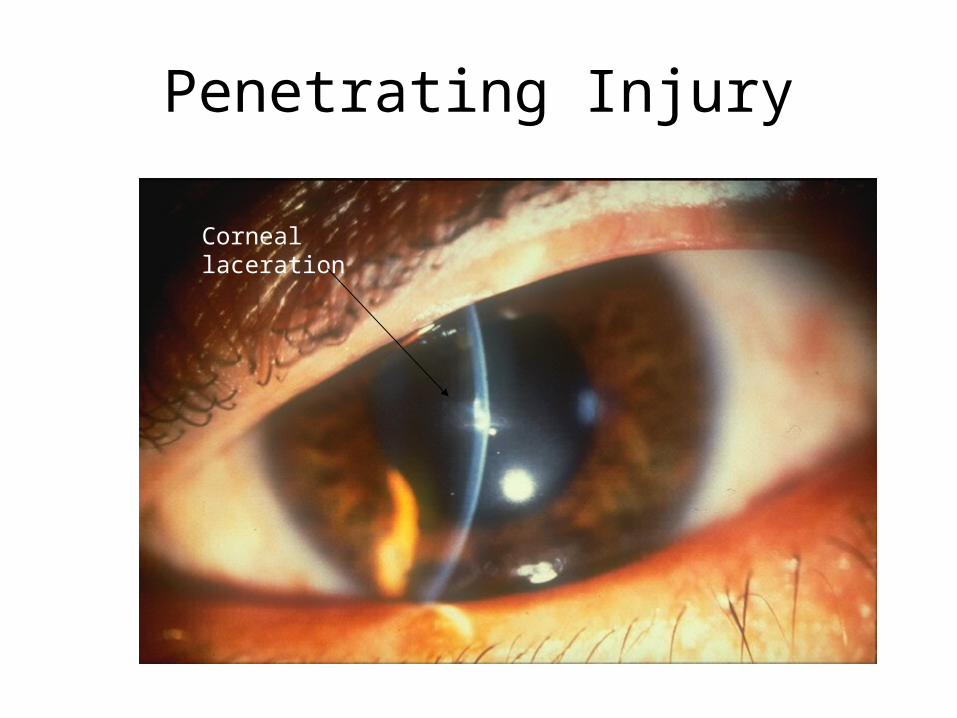
Penetrating Injury
Corneal laceration

Perforating injury

Shot Gun Injury

Blunt Injury, Contusion
• Bruising to eye lids
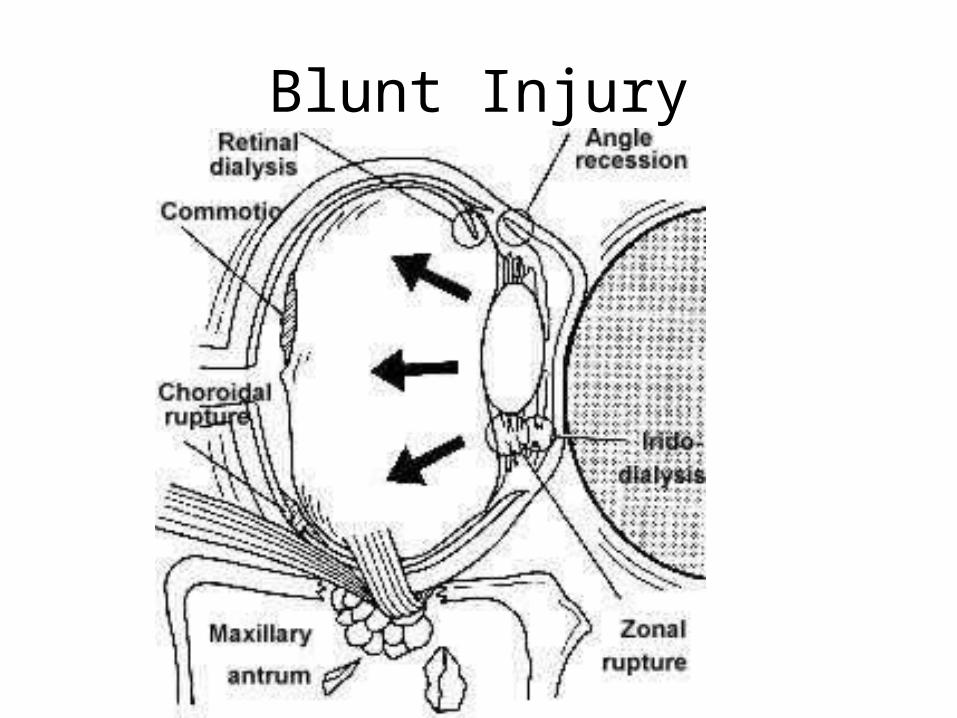
Blunt Injury
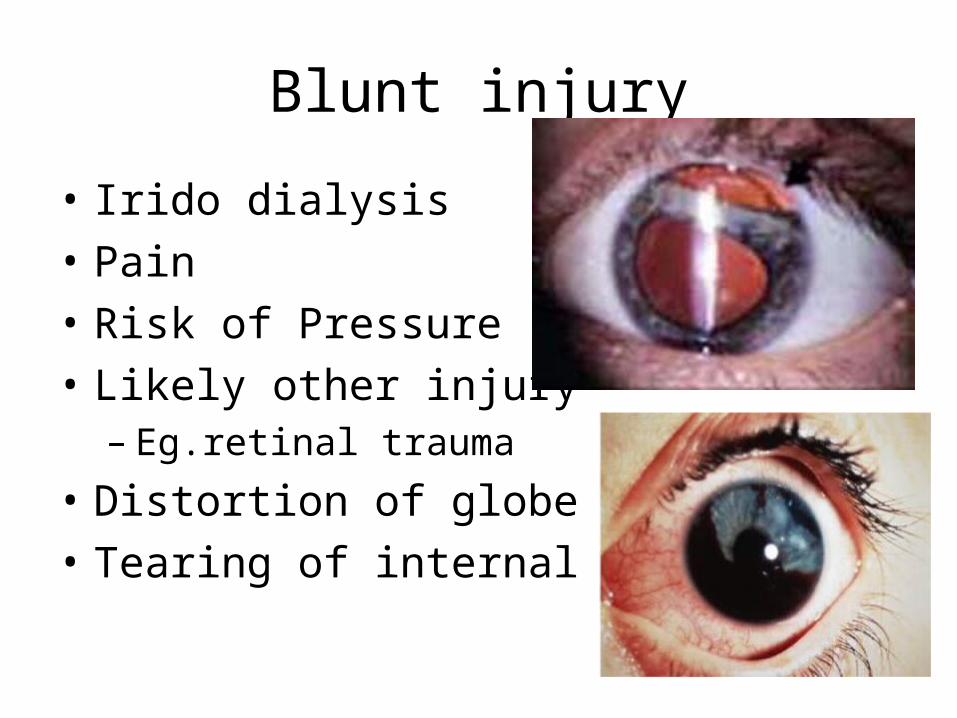
Blunt injury
• Irido dialysis• Pain• Risk of Pressure• Likely other injury
– Eg.retinal trauma
• Distortion of globe• Tearing of internal structures
Blunt Injury
• Hyphaema- blood in anterior chamber• Microscopic or Macroscopic
– Blood in the anterior chamber– Pressure problems, esp. re-bleed
• Must ask if FH of sickle cell in relevant ethnic gp– Other injury– Children require admission– Must ask if FH of sickle cell in relevant ethnic
group
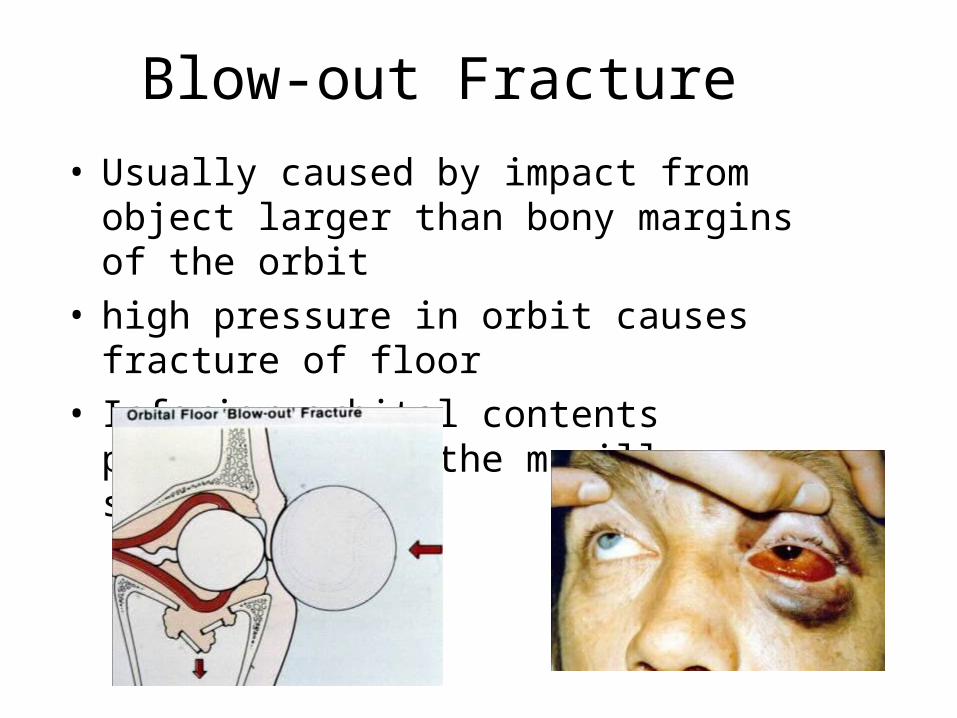
Blow-out Fracture• Usually caused by impact from object larger than
bony margins of the orbit• high pressure in orbit causes fracture of floor• Inferior orbital contents prolapsed into the
maxillary sinus
Blow-out fracture-symptoms
• Black Eye• Double Vision• Blurred Vision• Small eye (enopthalmos)• Pulling sensation on up gaze
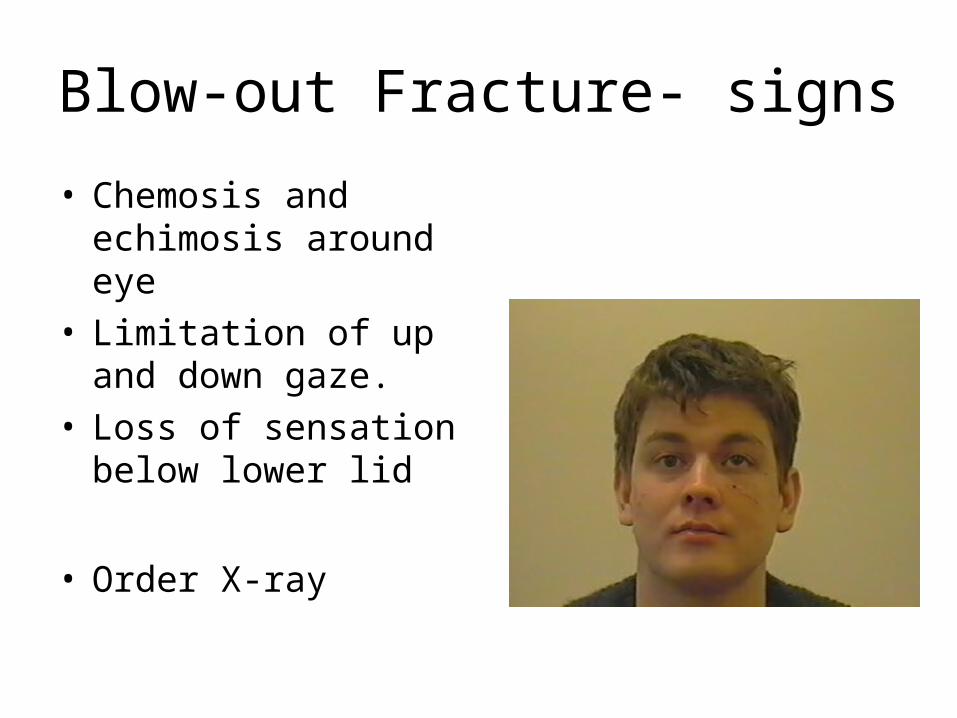
Blow-out Fracture- signs
• Chemosis and echimosis around eye
• Limitation of up and down gaze.
• Loss of sensation below lower lid
• Order X-ray
Facial Bone Fractures
• In a facial injury involving a fracture there is a 30% chance of maxillary involvement
• Chance of ocular injury – 10-23% in Le Fort II and III– 2-10% blinded
– 89% frontal sinus and supra orbital


Le Fort 3
All red and orange conditions need referral to an ophthalmologist
• All conditions classified as Blue/green can wait
What Ophthalmic conditions require fundoscopy?
• Anything with Visual loss
• What systemic conditions require ophthalmoscopy?
Systemic diseases requiring ophthalmoscopy
• Head injury?• Suspicious of raised ICP• Meningitis• Neurological- MS• Vascular presentations- CVA, Hypertension
What does the fundus tell you?
• Papilloedema- raised ICP• Pale disc- previous optic neuritis• Haemorrhagic disc• Hypertensive changes• Diabetic retinopathy- control/ renal function