Embed Size (px)
Citation preview
Acute Pulmonary Hypertension
and the Right Ventricle
24th Postgraduate Refresher Course
Brussels, December 5, 2018

Acute right heart failure
▪ Clinical presentation: systemic hypoperfusion (pale and clammy skin, confusion, chest pain, arrythmia, ileus, oliguria, lactic acidosis) and systemic congestion (turgescent jugular veins, hepatomegaly, edema, ascites)
▪ Right atrial pressure > left atrial pressure
▪ Echocardiography: dilated right heart chambers and septal shift, increased velocity of tricuspid regurgitation, shortened acceleration time of PA flow waves, with eventually pericardial effusion

CVP 15 mmHg, clinical right heart failure

Causes of the ARHF
- Cardiac surgery: transplantation, congenital, mitral valve, left ventricular assist, cardiopulmonary bypass, protamine, postoperative pulmonary hypertension crisis
- ARDS
- Acute-on-chronic respiratory insufficiency
- High volume/pressure mechanical ventilation
- Pulmonary embolism
- End-stage pulmonary arterial hypertension (idiopathic, cardiac shunts, scleroderma, HIV, liver disease)
- ARHF is associated with a poor prognosis

ARHF
The cause of ARHF is (almost) always an
increase in pulmonary artery pressure
ARHF is a right ventricular failure on an
abnormal increase in afterload

Male, 25 yrs
mPAP = 56 mmHg
Female, 24 yrs
mPAP = 53 mmHg
SV = 90 ml SV = 30 ml
Right ventricular responses to load :
2 different patterns
V Noordegraaf, VUMC

The laws of the heart
• Starling’s law: the heart adapts to increased
afterload (maintained SV) or preload
(increased SV) through increased
dimensions (heterometric adaptation)
• Anrep’s law: the heart adapts to increased
loading through an increased contractility
(homeometric adaptation)
Starling: for beat-to-beat changes or homeometric
failure in case of too rapid increase in PAP – or
endstage PH

Preseved RV-arterial
coupling by increased
homeometric
adaptation (Anrep)
Failing RV-arterial
coupling with
heterometric adaptation
(Starling)
RV failure in PH
V Noordegraaf, VUMC

The Right Ventricle and its Load in Pulmonary
Hypertension Vonk Noordegraaf, Westerhof BE,
Westerhof N. JACC 2017; 69: 236-241
From increased contractility and preserved RV-PA coupling to increased
dimensions and negative ventricular interaction

Coupling RV function to the pulmonary circulation
Volume
Pre
ssu
re
Isometric
Contraction
Ejection
Isometric
Relaxation
Diastolic filling End-diastole
End-systole Pulmonary Valve
Opening
Tricuspid
Valve
Opening
Ees = ESP/ESV
Ea = ESP/SV
After M Pinsky, without
permission

The PV loop allows for the definition of
systolic function and afterload, and thus
of RV-arterial coupling
Systolic function: end-systolic elastance Ees = ESP/ESV
Afterload: arterial elastance Ea = ESP/SV
Optimal RV-arterial coupling: Ees/Ea ratio of 1.5-2
Sagawa et al. Cardiac contraction and the PV relationship,
Oxford University Press, 1988.

The importance of systolic function adaptation to afterload
From M Overbeek
Optimal RV-
arterial
coupling:
Ees/Ea = 1.5-2
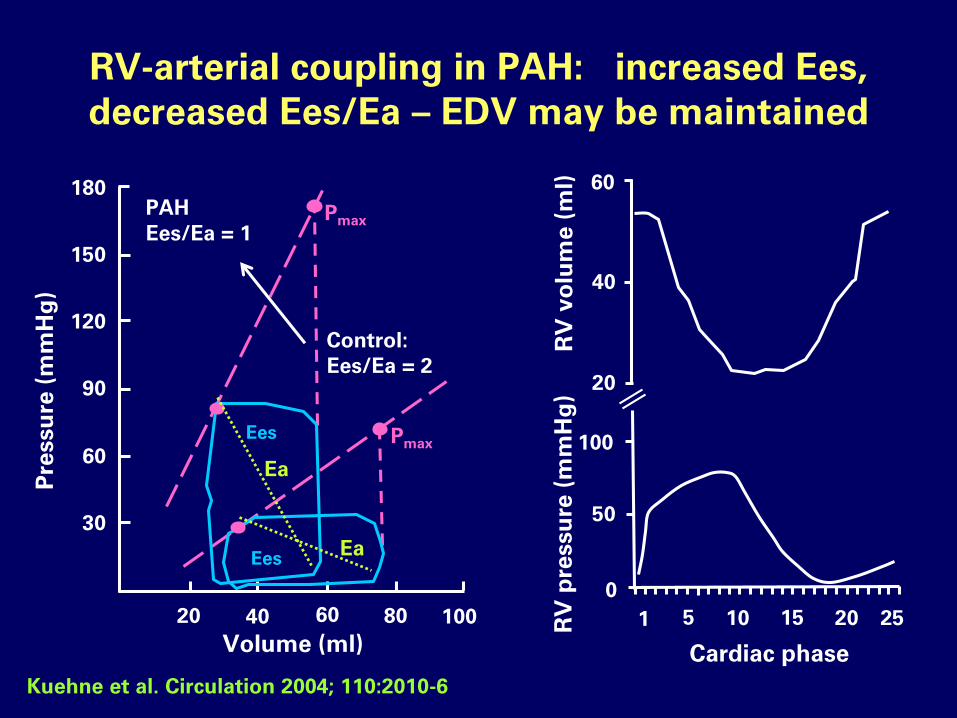
RV-arterial coupling in PAH: increased Ees,
decreased Ees/Ea – EDV may be maintained
Ea
Ea
180
150
120
90
60
30
20 40 60 80 100
Volume (ml)
Pre
ssu
re (
mm
Hg
)
Pmax
PmaxEes
Ees
Control:
Ees/Ea = 2
PAH
Ees/Ea = 1
Cardiac phase
60
40
20
100
50
0
1 5 10 15 20 25RV
pre
ssu
re (
mm
Hg
)R
V v
olu
me (
ml)
Kuehne et al. Circulation 2004; 110:2010-6

PV loops in PH: clinical studies
Diagnosis n Ees Ea Ees/Ea
IPAH 42 ↑ ↑ - or ↓, ex ↓
CCTGA 1 ↑ ↑ ↓
SSc-PAH 22 - ↑ - or ↓, ex ↓
CTEPH 13 ↑ ↑ - , ex ↓
1. Kuehne Circulation 2004;110:2010, 2. Wauthy Cardiol Young 2005;15:647,
3. Tedford Circ Heart Fail 2013, 4. McCabe J Appl Physiol 2014; 116: 355-63,
5. Spruijt AJRCCM 2015; 191: 1050-7 , 6. Hsu et al Circulation 2016; 133:
2413-22; Naeije et al Heart Fail Clin 2018; 14: 237-245
Pattern: Increased Ea (PVR), increased Ees, Ees/Ea maintained or
decreased, Ees/Ea decreased during exercise (5,6), EDV increases when
Ees/Ea decreases during exercise (6) - Ees and Ea measured by single
beat or family of PV loops ar decreasing venous return

RV-arterial coupling in experimental PHNaeije et al, Pulm Circ 2014; 4:395-406
Model Animal Ees Ea Ees/Ea EDV
Hypoxia Dog,goat,pig ↑ ↑ - -
Monocrotaline Rat ↑ ↑ ↓ ↑
Sepsis, early Pig ↑ ↑ - -
Sepsis, late Pig - ↑ ↓ ↑
Embolism Dog,goat,pig ↑ ↑ - -
PA banding Dog,goat,pig ↑ ↑ - -
AP shunting 3 mo Pig ↑ ↑ - -
AP shunting 6 mo Pig ↓ ↑ ↓ ↑
RVF on PH crisis Dog,pig ↓ ↑ ↓
↑
Chronic heart failure Dog - ↑ ↓ ↑Brimioulle AJP 2003;284:H1625, Wauthy 2004;286:H1441, Fesler AJP 2006;101:1085,
Rex ICM 2008;34:179, de Man Circ HeartFail 2012;5:97, Lambermont Cardiovasc Res
2003;59:412, de Vroomen AJP2000;278:H100, Leeuwenburgh AJP 2001;281:H2697,
Faber AJP 2006;291:H1580, Kerbaul CCM 2004;32:2814, Rondelet Circulation
2003;107:1329, Rondelet Eur Heart J 2012;33:1017, Pagnamenta JAP 2010;109:1080

RV-arterial coupling in experimental PH
• Contractility is almost always increased to
preserve RV-arterial coupling
• Insufficient increase in Ees in septic or
inflammatory models of PH (monocrotaline),
PH crisis, prolonged aorta-pulmonary
shunting or left heart failure
- Results in increased RV volumes

Pharmacological interventions Naeije et al, Pulm Circ 2014; 4:395-406
Model Drug Ees Ea Ees/Ea
Hypoxia Dobutamine ↑ - ↑
Norepinephrine ↑ - ↑
Sildenafil - ↓ ↑
Isoflurane ↓ ↑ ↓ ↓
Desflurane ↓ ↑ ↓ ↓
Propranolol ↓ ↑ ↓ ↓
RVF on PAB Levosimendan ↑ ↓ ↑ ↑
Dobutamine ↑ - ↑
CHF Milrinone ↑ - ↑
Nitroprusside - - -
Brimioulle AJP 2003;284:H1625, Fesler AJP 2006;101:1085, Rex ICM 2008;34:179,, Kerbaul
CCM 2004;32:2814, Pagnamenta JAP 2010;109:1080, Kerbaul Anesthesiology 2004;101:1357-
1361

Effects of inhaled iloprost on RV contractility,RV-
vascular coupling and ventricular interdependence in
an experimental model of acute pulmonary
hypertension Rex et al, Crit Care 2008, 12:R113
26 pigs, hypoxic pulmonary hypertension, 5 µg inhaled iloprost
Emax/Ea ratio stable at 1

Pharmacological interventions
• Low-dose dobutamine and norepinephrine are
inotropes with no effect on the pulmonary circulation
• Inhaled anesthetics deteriorate RV-arterial coupling
by a combination of negative inotropy and increased
PVR
• Levosimendan improves RV-arterial coupling by a
combination of positive inotropy and pulmonary
vasodilation

Pathophysiology of RV failure in PH
Pulmonary hypertension Increased afterload
Increased contractlity Homeometric adaptation (Anrep) to preserve
RV-arterial coupling
Increased EDV Heterometric adaptation (Starling) to preserve flow output, causes altered ventricular interaction

Pathophysiology of RV failure in PH
Pulmonary hypertension Increased afterload: targeted therapies: iNO, epoprostenol, ERA’s, PDE5i’s, blood gases, lung volumes
Increased contractlity Homeometric adaptation (Anrep) to preserve RV-
arterial coupling: dobutamine,
norepinephrine, levosimendan (?)
Increased EDV Heterometric adaptation (Starling) to preserve flow output diuretics

PAP 62 mmHg
RAP 18 mmHg
PAWP 24 mmHg
CI 1.6 L/min/m2
Case report
Patient admitted for
decompensated
IPAH
Echo: RHF, LVEF
normal

Before diuretics, PAWP 24 mmHg After diuretics, PAWP 13 mmHg
Treatment with iv dobutamine and furosemide

What happened?
• Diastolic left ventricular failure caused by leftward
bowing of the septum during diastole, decreased LV
chamber size, compliance and contractility
• This is called a « reverse Bernheim effect » after the
report by Bernheim et al in 1910 of RV failure in a
patient with aortic stenosis
Bernheim P De l’asystolie veineuse dans l’hypertrophie
du cœur gauche par sténose concomitante du
ventricule droit Rev Med 1910;39:785-801
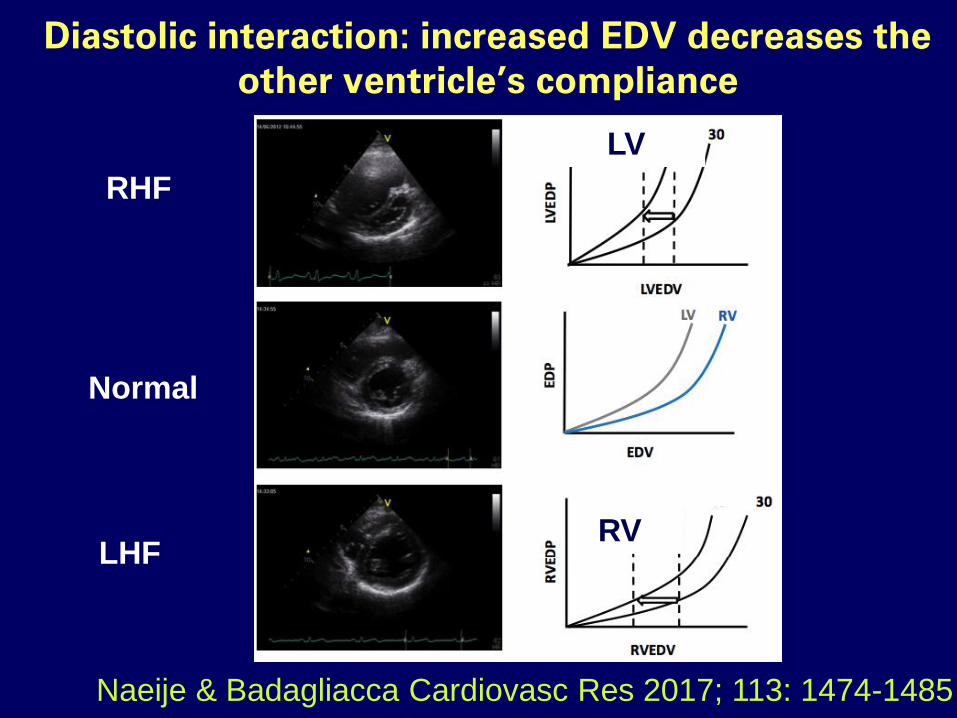
Diastolic interaction: increased EDV decreases the
other ventricle’s compliance
Naeije & Badagliacca Cardiovasc Res 2017; 113: 1474-1485
LV0
0
RV0
Normal
LHF
RHF

Ventricular interdependence
Right and left ventricles have the
septum and free wall
myocardial fibers in common,
and are constrained within a
non-distensible pericardial
envelope
There is thus ventricular
interdependence, defined as
the forces that are transmitted
from one ventricle to the
other ventricle through the
myocardium and pericardiumSantamore and Dell’Italia, Progr Cardiovasc Dis 1998;40:289
Naeije and Badagliacca, Cardiovasc Res 2017; ; 113: 1474-1485 ,
Friedberg and Redington Circulation 2014;129:1033-1044

Systolic interaction; RV pressure–segment length and pressure-diameter loops during severe pulmonary artery
(PAC) and aortic constriction (AOC)
Belenkie I et al. Circulation 1995;92:546-554
Copyright © American Heart Association

Comparative significance in systolic
ventricular interaction Yamaguchi et al
Cardiovasc Res 1991 ; 25 : 774-783
Systolic ventricular interdependence was quantified by
measurements of instantaneous cross-talk gains during
ventricular pressure changes caused by sudden release of
aortic or pulmonary arterial constriction
20-40 % of RV systolic pressure results from LV
contraction 4-10 % of LV systolic pressure results from
RV contraction
Naeije R, Badagliacca R. The overloaded RV and
ventricular interdependence. Cardiovasc Res 2017; 113:
1474-1485

Pathophysiologic rationale of treatment of
of (after)load-induced RV failure
Pulmonary hypertension
Increased contractlity
Increased EDV diastolic interaction stroke volume
systolic interaction hypotension
ischemia

Treatment of afterload-induced RV failure
Pulmonary hypertension
Increased contractlity
Increased EDV diastolic interaction stroke volume
systolic interaction hypotension
ischemia
Thrombolytic therapy, iNO, iILO,
- PDE5i, ERA, PGI2, FRC, pH,
hypoxemia
Dobutamine, norepinephrine,
levosimendan

Treatment of afterload-induced RV failure
Pulmonary hypertension
Increased contractlity
Increased EDV diastolic interaction stroke volume
systolic interaction hypotension
ischemia
Thrombolytic therapy, iNO, iILO,
- PDE5i, ERA, PGI2, FRC, pH,
hypoxemia
Dobutamine, norepinephrine,
levosimendan
Diuretics

Treatment of afterload-induced RV failure
Pulmonary hypertension
Increased contractlity
Increased EDV diastolic interaction stroke volume
systolic interaction hypotension
ischemia
Thrombolytic therapy, iNO, iILO,
- PDE5i, ERA, PGI2, FRC, pH,
hypoxemia
Dobutamine, norepinephrine,
levosimendan
Norepinephrine
Diuretics

Conclusions
• As there is currently no evidence from randomized
controlled trials, treatment of RV failure in the ICU has
to rely on sound pathophysiological principles
• Interventions include targeted therapies, and
normalisation of blood gases and FRC to decrease
afterload, inotropic drugs to improve systolic function,
correction of hypotension (systolic interaction) and
optimization of RV filling (diastolic interaction)

« La maladie n’est
qu’une altération
de la faculté
physiologique »
C Bernard 1813-1878





























