Embed Size (px)
DESCRIPTION
ACUTE RESPIRATORY DISTRESS SYNDROME ( ARDS ). Oea Khairsyaf. Acute Respiratory Distress Syndrome. Defenisi. “Non-cardiogenic Pulmonary Oedema” Ashbaugh, Bigelow et al, 1967 “Adult Respiratory Distress Syndrome” Petty and Ashbaugh, 1971 “Shock Lung” Staub, 1974 - PowerPoint PPT Presentation
Citation preview

ACUTE RESPIRATORY DISTRESS ACUTE RESPIRATORY DISTRESS SYNDROME ( ARDS )SYNDROME ( ARDS )
Oea Khairsyaf

Acute Respiratory Distress Acute Respiratory Distress SyndromeSyndrome
Acute Respiratory Distress Acute Respiratory Distress SyndromeSyndrome
• ““Non-cardiogenic Pulmonary Oedema”Non-cardiogenic Pulmonary Oedema”– Ashbaugh, Bigelow et al, 1967Ashbaugh, Bigelow et al, 1967
• ““Adult Respiratory Distress Syndrome”Adult Respiratory Distress Syndrome”– Petty and Ashbaugh, 1971Petty and Ashbaugh, 1971
• ““Shock Lung”Shock Lung”– Staub, 1974Staub, 1974
• ““Acute Respiratory Distress Syndrome”Acute Respiratory Distress Syndrome”– American-European Consensus Committee, American-European Consensus Committee,
19921992
Defenisi

Consensus Conference Definitions for Acute Lung Injury (ALI) and Acute Respiratory Distress Syndrome (ARDS)Consensus Conference Definitions for Acute Lung Injury (ALI) and Acute Respiratory Distress Syndrome (ARDS)
waktwaktuu
OxsigenasiOxsigenasi
(astrup)(astrup)X-rayX-ray
Tekanan Tekanan arteri arteri
pulmonalepulmonale
ALI ALI KriteriKriteriaa
AkutAkut PaOPaO2 2 / FIO/ FIO22 ≤ ≤ 300 mmHg300 mmHg
(fraksi oksigen (fraksi oksigen 21%)21%)
InfiltratInfiltrat
bilateralbilateral≤ ≤ 18 mmHg18 mmHg
ARDS ARDS KriteriKriteriaa
AkutAkut PaOPaO2 2 / FIO/ FIO22 ≤ ≤ 200 mmHg 200 mmHg (fraksi oksigen (fraksi oksigen 21%)21%)
InfiltratInfiltrat
BilateralBilateral≤ ≤ 18 mmHg18 mmHg

ETIOLOGI ARDSETIOLOGI ARDS
• Asma bronkial • PPOK• Pneumonia• Aspirasi makanan• Pulmonary
contusion• Near-drowning• Inhalational injury• DLL
• Sepsis• Severe trauma
with shock • Drug overdose• Acute pancreatitis• Transfusion of
blood products
SECARA LANGSUNG TIDAK LANGSUNG

Acute Respiratory Distress SyndromeAcute Respiratory Distress Syndrome
Gambaran klinis:Gambaran klinis: Awal “shock” responsif terhadap resusitasi.Awal “shock” responsif terhadap resusitasi. Periode latent : beberapa jam, biasanya Periode latent : beberapa jam, biasanya
beberapa hari (12-48 jam).beberapa hari (12-48 jam). Insidious tachypnoea, pasien jadi gelisah .Insidious tachypnoea, pasien jadi gelisah . Paru Paru tidal volume kecil, napas cepat, tidal volume kecil, napas cepat,
hipoksemia refrakter.hipoksemia refrakter. Mula-mula alkalosis respiratorik Mula-mula alkalosis respiratorik asidosis asidosis
respiratorikrespiratorik Ventilasi mekanis Ventilasi mekanis

PatogenesisPatogenesisPatogenesisPatogenesis
3 fase dari lung injury:3 fase dari lung injury:1.1. Fase exudatif ( edema and Fase exudatif ( edema and
perdarahan )perdarahan )
2.2. Fase inflammatory and repairFase inflammatory and repair
3.3. Fase fibrotic Fase fibrotic

Acute Respiratory Distress SyndromeAcute Respiratory Distress Syndrome
Exudative Phase, 0-5 hari.Exudative Phase, 0-5 hari. Ruang alveoli terisi cairan, protein dan inflammatory Ruang alveoli terisi cairan, protein dan inflammatory
cells.cells. Necrosis sel-sel pneumocyte type 1, fibrin, platelet Necrosis sel-sel pneumocyte type 1, fibrin, platelet
thrombi.thrombi.
Inflammatory Phase, 5-10 hari.Inflammatory Phase, 5-10 hari. Proliferasi fibroblasts dan sel-sel pneumocyte type 2.Proliferasi fibroblasts dan sel-sel pneumocyte type 2. Squamous metaplasia dan pembentukan hyaline Squamous metaplasia dan pembentukan hyaline
membranes.membranes.
Fibroproliferative Phase, 10 hari sampai sembuh Fibroproliferative Phase, 10 hari sampai sembuh atau mati.atau mati. Fibrosis interstital dan intra-alveolar.Fibrosis interstital dan intra-alveolar. Thrombosis dan obliterasi vaskuler.Thrombosis dan obliterasi vaskuler. Collagen paru meningkat.Collagen paru meningkat.

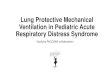
Alveolar / capillaryAlveolar / capillarypermeabilitypermeability
Pulmonary OedemaPulmonary Oedema
ARDS / ALIARDS / ALI
Precipitating EventPrecipitating Event
Inflammatory ResponseInflammatory ResponseNeutrophil activationNeutrophil activation
Neutrophils in BALNeutrophils in BALHistology appearancesHistology appearances
Protein levels in BALProtein levels in BAL
ROSROSReactive Oxygen SpeciesReactive Oxygen Species
Superoxide / HydroxylSuperoxide / Hydroxyl
Lung Water Lung Water
Pathogenesis ARDS / ALIPathogenesis ARDS / ALI

Patogenesis ARDS / ALIPatogenesis ARDS / ALI
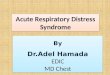
REDOX BalanceREDOX Balance
Generation ofGeneration ofOxidantOxidantspeciesspecies
AntioxidantAntioxidant ProtectionProtection
ROSROSHH22OO22
Superoxide (O2Superoxide (O2.-.-))Hydroxyl radical (OHHydroxyl radical (OH--))RNSRNSNitric oxide (NO)Nitric oxide (NO)Peroxynitrite (ONOOPeroxynitrite (ONOO--))
Superoxide dismutaseSuperoxide dismutaseCatalaseCatalaseGlutathioneGlutathioneTransferrinTransferrinCeruloplasminCeruloplasminVit EVit EVit CVit CBeta-caroteneBeta-carotene
NormalNormal

Patogenesis ARDS / ALIPatogenesis ARDS / ALI
Oxidative StressOxidative Stress
ROS formation &ROS formation &Oxidative damageOxidative damage
Depletion ofDepletion ofantioxidantsantioxidants

The Pathogenesis of ARDS / ALIThe Pathogenesis of ARDS / ALIThe Pathogenesis of ARDS / ALIThe Pathogenesis of ARDS / ALI
ROSROSRNSRNS
Molecular DamageMolecular Damageand Dysfunctionand Dysfunction
Alveolar / capillaryAlveolar / capillarypermeabilitypermeability
Pulmonary OedemaPulmonary Oedema
ARDS/ALIARDS/ALI
Ventilatory supportVentilatory supportInhaled NOInhaled NO
signallingsignalling
InflammatoryInflammatorymediatorsmediators
InflammatoryInflammatorymediatorsmediators
Precipitating EventPrecipitating Event
Inflammatory ResponseInflammatory Response(Respiratory Burst)(Respiratory Burst)
Predisposition?Predisposition?

Faktor-faktos seluler dan humoral pada ALI/ARDS
Faktor-faktos seluler dan humoral pada ALI/ARDS
• Neutrophils.Neutrophils.– ROS dan proteases.ROS dan proteases.– Resting, activated, primed and unresponsive.Resting, activated, primed and unresponsive.
• Cytokines (polypeptides).Cytokines (polypeptides).– TNF-TNF-, macrophages, monocytes, neutrophils., macrophages, monocytes, neutrophils.– IL-1IL-1, macrophages, endothelial cells, macrophages, endothelial cells– GM-CSF, monocytes, macrophages, fibroblasts GM-CSF, monocytes, macrophages, fibroblasts
epithelial, endothelial dan smooth muscle cells.epithelial, endothelial dan smooth muscle cells.• Chemokines (chemotactic cytokines).Chemokines (chemotactic cytokines).
– IL-8.IL-8.• Eicosanoids (prostaglandin, leucotrienes, Eicosanoids (prostaglandin, leucotrienes,
thromboxanes), complement, endotoxins, thromboxanes), complement, endotoxins, adhesion molecules, PAF, endothelins, NO.adhesion molecules, PAF, endothelins, NO.

PathogenesisPathogenesis
• Influx cairan edema kaya protein Influx cairan edema kaya protein alveoli alveoli (permeabilitas alveolar-capillary barrier (permeabilitas alveolar-capillary barrier ))
• Kerusakan Kerusakan Type 2 cellsType 2 cells gangguan epithelial gangguan epithelial fluid transport fluid transport gangguan pengeluaran gangguan pengeluaran cairan dan cairan dan produksi surfactant abnormalproduksi surfactant abnormal
• Bila kerusakan hebat Bila kerusakan hebat gangguan epithelial gangguan epithelial repair repair fibrosis fibrosis
• Neutrophils merupakan sel yang dominantNeutrophils merupakan sel yang dominant• Cytokines dan proinflammatory compounds Cytokines dan proinflammatory compounds
mengawali dan memperkuat respons mengawali dan memperkuat respons inflammatoryinflammatory

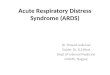
Ware LB, Matthay MA. Ware LB, Matthay MA. N Engl J MedN Engl J Med 2000;342:1334-1349 2000;342:1334-1349

Ware LB, Matthay MA. Ware LB, Matthay MA. N Engl J MedN Engl J Med 2000;342:1334-1349 2000;342:1334-1349
Exudative phaseExudative phase(A & D)(A & D)
Fibrosing-alveolitis phaseFibrosing-alveolitis phase(B, C & E)(B, C & E)
Hyaline membr Collagen

Ware LB, Matthay MA. Ware LB, Matthay MA. N Engl J MedN Engl J Med 2000;342:1334-1349 2000;342:1334-1349
Exudative phaseExudative phase Fibrosing-alveolitis phaseFibrosing-alveolitis phase

ARDSARDS

PENATALAKSANAAN
Obati penyakit dasar
Antibiotika
Kortikosteroid
oksigenasi
Anti oksidan

Keluaran (outcome)Keluaran (outcome)
• Tahun 1967 - 1979Tahun 1967 - 1979– Asbaugh (1967) : survival 42%Asbaugh (1967) : survival 42%– Survival : 18 – 38%Survival : 18 – 38%
• Tahun 1980 - 1989Tahun 1980 - 1989– Survival (< 1985) : 32 – 36%Survival (< 1985) : 32 – 36%– Survival (> 1985) : 41 - 52% (European Collaborative Survival (> 1985) : 41 - 52% (European Collaborative
Study 41%)Study 41%)
• Tahun 1990 – 2000Tahun 1990 – 2000– Survival : 41 – 60%Survival : 41 – 60%– NIH ARDS study : mortality 40% vs 30% (penurunan NIH ARDS study : mortality 40% vs 30% (penurunan
25%, antara VT 12 mL/kg vs 6 mL/kg)25%, antara VT 12 mL/kg vs 6 mL/kg)

Outcome Jangka Panjang pada Survivors
(1-1,5 tahun pasca ARDS)
Outcome Jangka Panjang pada Survivors
(1-1,5 tahun pasca ARDS)
Sequelae pulmonerSequelae pulmoner
Majoritas, fungsi paru kembali hampir normalMajoritas, fungsi paru kembali hampir normal
Gangguan residual:Gangguan residual:• restrictive ventilatory defect (biasanya ringan),restrictive ventilatory defect (biasanya ringan),• Hipertensi pulmoner (ringan),Hipertensi pulmoner (ringan),• airflow limitation (airflow limitation ( bronchial hyperactivity) bronchial hyperactivity)
Gangguan pada exercise testing lebih Gangguan pada exercise testing lebih bermakna (setara pasien COPD berat)bermakna (setara pasien COPD berat)
Derajat gangguan ~ umur, riwayat merokok, Derajat gangguan ~ umur, riwayat merokok, ventlasi mekanis berkepanjanganventlasi mekanis berkepanjangan

SurvivalSurvival• 10 tahun terakhir, mortalitas turun 10 tahun terakhir, mortalitas turun 20% 20%• Mortalitas:Mortalitas:
– Umur : 75% (≥ 60 th) vs 37% (< 60 th)Umur : 75% (≥ 60 th) vs 37% (< 60 th)– Faktor resiko : 64% (sepsis) vs 42% Faktor resiko : 64% (sepsis) vs 42%
(trauma)(trauma)– Penyulit : 86% (sepsis) vs 38% (tanpa Penyulit : 86% (sepsis) vs 38% (tanpa
sepsis)sepsis)
– Response thd PEEP : PaOResponse thd PEEP : PaO22/FiO/FiO2 2 > 150 > 150 mmHg mortalitas 23% mmHg mortalitas 23%