-
8/8/2019 Acute Respiratory Failure 2010
1/87
Arterial Blood GasesArterial Blood GasesRespiratory
FailureRespiratory Failure
Michael Lippmann, MD
Division of Pulmonary and Critical Care Medicine
Department of Internal Medicine
-
8/8/2019 Acute Respiratory Failure 2010
2/87
Respiratory SystemRespiratory System
LungParenchyma
Airways
BellowsRespiratory control centers
Peripheral nerves
Muscles
Chest wall
-
8/8/2019 Acute Respiratory Failure 2010
3/87
Role of Respiratory SystemRole of Respiratory System
Maintain optimal levels of oxygen and pH in theblood despite
variations in ambient conditions and
demand
pH maintained via control of arterial PCO2
Measurement of arterial blood gases evaluates
effectiveness of respiratory system in fulfilling its
role
-
8/8/2019 Acute Respiratory Failure 2010
4/87
Alveolar Gas PressuresAlveolar Gas Pressures
Determined by balance between delivery ofoxygen and carbon
dioxide to the lung and theirremovalAtmospheric air passes through
airways where it is
fully saturated with water vapor and delivered to thealveoli
Oxygen is delivered to the alveoli by ventilation andtaken up by
the hemoglobin in the blood perfusing thelung
Carbon dioxide is delivered to the alveoli by the bloodperfusing
the lung and removed by ventilation
-
8/8/2019 Acute Respiratory Failure 2010
5/87
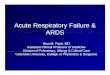
Effect of V/Q Ratio on Alveolar GasEffect of V/Q Ratio on
Alveolar Gas. .
Normal
range of
V/Q
ratios
.1 .2 .4 .6 .8 1 2 4 6 810
POPO22 in alveolusin alveolus
and capillary
and capillary
PCO2 in alveolus
and capillary
20
40
60
80
100
120
140
160
20
40
60
80
100
120
140
160
Log V/Q ratios. .
PO
2orP
CO
2
-
8/8/2019 Acute Respiratory Failure 2010
6/87
Alveolar PCOAlveolar PCO22
PaCO2 = VCO2/(VE-VD)Where:
PaCO2 = Arterial carbon dioxide tension
VCO2 = CO2 production by the bodyVE= Minute ventilation
VD = Dead space ventilation
Therefore, arterial carbon dioxide tension will increase if:
there is an absolute decrease in bellows function
the bellows are unable to increase ventilation in proportion
to
increased CO2 production or increased dead space
.
.
.
. . .
-
8/8/2019 Acute Respiratory Failure 2010
7/87
Alveolar Gas Equation for OxygenAlveolar Gas Equation for
Oxygen
PPAAOO22 = F= FIIOO22(P(PBB - P- PHH22OO) - P) -
PaaCOCO22/R/R
Where:
FIO2= Fraction inspired oxygen tensionP
B= Barometric pressure (747 mm Hg)
PH2O
= Partial pressure of water vapor (47 mm Hg)
PaCO
2= Arterial carbon dioxide tension
R = Respiratory equivalent (0.8)
-
8/8/2019 Acute Respiratory Failure 2010
8/87
Alveolar Gas Equation for OxygenAlveolar Gas Equation for
Oxygen
Balance between removal of oxygen from the alveolus byperfusion,
and the addition of oxygen to the alveolus by
ventilation determines alveolar O2 Calculates the PO2 of an
alveolus with a specific ratio of
ventilation to perfusion The first part calculates the alveolar
PO2 in the absence of any
perfusion
The second component corrects for effect of perfusion,
whichremoves oxygen and adds CO2 to the alveolus
PPAAOO22 = FIO= FIO22(P(PBB - P- PHH22OO) - P) -
PaaCOCO22/R/R
-
8/8/2019 Acute Respiratory Failure 2010
9/87
Arterial Gas PressuresArterial Gas Pressures
Determined by the average of gas contents ofblood leaving
alveolo-capillary units
Gas pressure gas content
Pressure index of the tendency of a gas
molecule to moveGas molecules move from areas of higher pressure
to
those of lower pressure
Flow stops when pressure (not content) equilibrates
Content number of gas molecules contained in agiven volume
-
8/8/2019 Acute Respiratory Failure 2010
10/87
Ideal Gas LawIdeal Gas Law
P = pressure
V = volume of vessel = number of moles of gas
R = universal gas constant
T = absolute temperature
Pressure will increase with
Increase in amount of gas Decrease in volume of
container
Increase in temperature
PV =PV = RTRT
-
8/8/2019 Acute Respiratory Failure 2010
11/87
Henrys LawHenrys Law
P = kCP = kC The solubility of a gas in a liquid is directly
proportional
to the partial pressure of that gas above the liquid
kis a temperature-dependent constant (769.2 Latm/mol for
oxygen in water at 298K)Pis the partial pressure (atm)
Cis the concentration of the dissolved gas in the liquid
(mol/L)
The less soluble the gas (higher k) the lower the content for
any
pressure
-
8/8/2019 Acute Respiratory Failure 2010
12/87
Oxygen ContentOxygen Content
Oxygen is poorly soluble in plasma and is carriedby
hemoglobin
Oxygen capacity = 1.34 (ml O2/g Hgb) x
hemoglobin (g/dl)Oxygen content = (oxygen carrying capacity)
x
(% oxygen saturation) + 0.003 ml/dl (PaO
2)
-
8/8/2019 Acute Respiratory Failure 2010
13/87
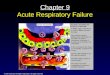
Oxyhemoglobin Dissociation CurveOxyhemoglobin Dissociation
Curve
Oxygen content = (1.34 ml x Hgb) SaO2 Curve also represents
relationship between
PO2 and oxygen content
0
20
40
60
80
100
20 40 60 80 100 120
SO
2%
PO2
Left-shifted (Increased affinity) decreased temp decreased 2-3
DPG increased pH carbon monoxide
Right-shifted (Decreased affinity) increased temp
increased 2-3 DPG
decreased pH
-
8/8/2019 Acute Respiratory Failure 2010
14/87
Oxygen ContentOxygen Content P PaaOO22 = 100= 100
1.34 ml O2
x (16 g/dl Hgb) x 98% = 21 ml O2
+
0.003 ml O2 (100) = .03 ml O2
1.31 ml
O2
1.31 mlO
2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 mlO
2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2 1.31 ml
O21.31 mlO
2
.03 ml
O2
O2 Content = 21.03 ml/dl blood
-
8/8/2019 Acute Respiratory Failure 2010
15/87
Oxygen ContentOxygen Content P PaaOO22 = 40= 40
1.34 ml O2
x (16 g/dl Hgb) x 75% = 16 ml O2
+
0.003 ml O2 (40) = .012 ml O2
1.00 ml
O2
1.00 mlO
2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 mlO
2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2 1.00 ml
O21.00 mlO
2
.012 ml
O2
O2 Content = 16.012 ml/dl blood
-
8/8/2019 Acute Respiratory Failure 2010
16/87
Oxygen ContentOxygen Content P PaaOO22 = 600= 600
1.34 ml O2
x (16 g/dl Hgb) x 100% = 21.4 ml O2
+
0.003 ml O2 (600) = .18 ml O2
1.34 ml
O2
1.34 mlO
2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 mlO2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2 1.34 ml
O21.34 mlO
2
.18 ml
O2
O2 Content = 21.58 ml/dl blood
-
8/8/2019 Acute Respiratory Failure 2010
17/87
MixingMixingEqual volumes (100 cc) of blood mixed together
each with equal amounts of hemoglobin (16g/dl)
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2
1.31 ml
O2 1.31 ml
O21.31 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2 1.00 ml
O21.00 ml
O2
PO2 = 100
SO2 = 98%
Content = 21 ml O2/100cc
PO2 = 40
SO2 = 75%
Content = 16 ml O2/100cc
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
PO2 = 54
SO2 = 86.5%
Content = 18.5 ml O2/100cc
1.16 ml
O2
1.16 ml
O21.16 ml
O2
1.16 ml
O2
1.16 mlO2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
1.16 ml
O2
+ =
-
8/8/2019 Acute Respiratory Failure 2010
18/87
MixingMixingEqual volumes (100 cc) of blood mixed together
each with equal amounts of hemoglobin (16g/dl)
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2
1.34 ml
O2 1.34 ml
O21.34 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2
1.00 ml
O2 1.00 ml
O21.00 ml
O2
PO2 = 600
SO2 = 100%
Content = 21.4 ml O2/100cc
PO2 = 40
SO2 = 75%
Content = 16 ml O2/100cc
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
PO2 = 57
SO2 = 87.5%
Content = 18.7 ml O2/100cc
1.17 ml
O2
1.17 ml
O21.17 ml
O2
1.17 ml
O2
1.17 mlO2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
1.17 ml
O2
+ =
-
8/8/2019 Acute Respiratory Failure 2010
19/87
West Two-Compartment Model -West Two-Compartment Model -
OxygenOxygen
Bloodflow
2.4 l/min
2.4 l/min
VA2 l/min
PO2 99
VA2 l/min
PO2 99VAQ
= .83VAQ
= .83
P
O299SO
297.5
PO299
SO297.5
PO299 SO2 97.5
. .
. .
-
8/8/2019 Acute Respiratory Failure 2010
20/87
V/Q Mismatch - OxygenV/Q Mismatch - Oxygen
Blood
flow
2.4 l/min
2.4 l/min
VA3.6 l/min
PO2 117
VA0.4 l/min
PO2 51.5VAQ
= 1.5VAQ
= .167
PO2117
SO298.2
PO251
.5 SO286
PO264 SO2 92.1
. .
..
-
8/8/2019 Acute Respiratory Failure 2010
21/87
Alveolar-arterial GradientAlveolar-arterial Gradient
Calculated alveolar O2(P
AO
2) -
measured arterial O2 (PaO2)
-
8/8/2019 Acute Respiratory Failure 2010
22/87
A-a GradientA-a Gradient
Measures dispersion of V/Q ratios within thelung
Normal lung has narrow range of V/Q ratios
The greater the variability, the higher the A-agradient
. .
. .
-
8/8/2019 Acute Respiratory Failure 2010
23/87
A-a GradientA-a Gradient
Clinically, can be used to assess underlying lungfunction in
patients with decreased P
aCO
2or
receiving supplemental oxygen
Arterial PO2may be normal or elevated despite the
presence of significant V/Q mismatch
In these situations the increased A-a gradient can
indicate significant underlying lung dysfunction
. .
-
8/8/2019 Acute Respiratory Failure 2010
24/87
PCOPCO22 versus COversus CO22 ContentContent
50
55
60
40 50 60
Deoygenated
bloodOxygenated
blood
0
20
40
60
20 40 60 80
CO
2con
ten
t
PCO2
-
8/8/2019 Acute Respiratory Failure 2010
25/87
V/Q Mismatch - Carbon DioxideV/Q Mismatch - Carbon Dioxide
CO2 production
200 ml/min
PCO2 46
50%flow
PCO2 40
100 ml/minCO2
50%flow
PCO2 40
100 ml/minCO2
PCO240
PCO24
0
PCO2 40
. .
-
8/8/2019 Acute Respiratory Failure 2010
26/87
V/Q Mismatch - Carbon DioxideV/Q Mismatch - Carbon Dioxide
CO2 production
200 ml/min
PCO2 46
50%flow
100 ml/min
CO2
50%flow
0 ml/min
CO2
PCO246
PCO240
PCO2 43
. .
-
8/8/2019 Acute Respiratory Failure 2010
27/87
OptionsOptions
Increase blood flow to normal V/Q regions
Increase ventilation of normal V/Q regions (normal
ventilatory drive)
Increase arterial and mixed venous PCO2 (blunted
ventilatory drive)
. .
. .
COCO22 Elimination Must Equal COElimination Must Equal
CO22ProductionProduction
-
8/8/2019 Acute Respiratory Failure 2010
28/87
Bicarbonate Buffer SystemBicarbonate Buffer System
H2CO3H+
+ HCO3-
weak acid conjugate
base
Equilibrium is far to the left - there are 600 parts
of CO2 in solution for every part carbonic acid
Thus, carbonic acid component is equal todissolved CO2.
Dissolved CO2 in mmole =
0.03 x PCO2
CO2 + H2OH2CO3H+ + HCO3-
-
8/8/2019 Acute Respiratory Failure 2010
29/87
Henderson-Hasselbach EquationHenderson-Hasselbach Equation
Effectiveness of a buffer depends on its pK (pH at
which the buffer exists half as the weak acid and
half as the conjugate base). Buffering is optimal at
its pKAlso depends on the amount of buffer present
-
8/8/2019 Acute Respiratory Failure 2010
30/87
Henderson-Hasselbach EquationHenderson-Hasselbach Equation
pH pKconjugate base
weak acid= + log
[ ]
[ ]
For the bicarbonate system:
p H= 6.1 l o g [H C O3 ] m e t a b o l i c0. 0 3xP C O
2
r e s p i r a t
-
8/8/2019 Acute Respiratory Failure 2010
31/87
The bicarbonate generated by the buffer pair does not
effectively buffer the change in H+ when PCO2rises
CO2+ H
2OH
2CO
3H+ + HCO
3
-
doubling the CO2doubles [H+]
for every mole rise in [H+] there will be an identical rise
in
[HCO3
-]
Thus [HCO3
-] will rise only 40 nanoequivalents, an
insignificant increase compared to usual concentration
Bicarbonate Buffer SystemBicarbonate Buffer System
-
8/8/2019 Acute Respiratory Failure 2010
32/87
Bicarbonate Buffer SystemBicarbonate Buffer System
PCO2 40
[HCO3-] = 24 mmole
0.03 x PCO2 = 1.2 mmole
pH = 6.1 + log (24/1.2)
ph = 7.4
Lung
PCO2 40
[HCO3-] = 19 mmole
0.03 x PCO2 = 1.2 mmole
pH = 6.1 + log (19/1.2)
ph = 7.3
Lung
CO2 CO2
+ 5 meq H+
Open
(Ventilating)
System
-
8/8/2019 Acute Respiratory Failure 2010
33/87
PCO2 40
[HCO3-] = 24 mmole
0.03 x PCO2 = 1.2 mmole
pH = 6.1 + log (24/1.2)
ph = 7.4
Lung
PCO2 207
[HCO3-] = 19 mmole
0.03 x PCO2 = 6.2 mmole
pH = 6.1 + log (19/6.2)
ph = 6.59
Lung
CO2
+ 5 meq H+
Bicarbonate Buffer SystemBicarbonate Buffer System
Closed
(Non ventilating)
System
-
8/8/2019 Acute Respiratory Failure 2010
34/87
Acid-Base TerminologyAcid-Base Terminology
Acidemia blood pH < 7.36Alkalemia blood pH > 7.44
Hypocapnia PaCO2< 36 mmHg
Hypercapnea PaCO2 > 44 mmHgHyperventilation associated with
hypocapnia
Hypoventilation associated with hypercapnea
Tachypnia high breathing rate
-
8/8/2019 Acute Respiratory Failure 2010
35/87
Acid-Base TerminologyAcid-Base Terminology
Respiratory acidosisA primary process associated with an
increase in P
aCO
2
Decreases pH
Compensation through renal retention of bicarbonate
Respiratory alkalosis
A primary process associated with a decrease in PaCO
2
Increases pH
Compensation through renal excretion of bicarbonate
-
8/8/2019 Acute Respiratory Failure 2010
36/87
Acid-Base TerminologyAcid-Base Terminology
Metabolic acidosis
A primary process associated with a decrease in
serumbicarbonate
Decreases pH
Compensation through hyperventilation
Metabolic alkalosis
A primary process associated with an increase in
serumbicarbonate
Increases pHCompensation through hypoventilation
-
8/8/2019 Acute Respiratory Failure 2010
37/87
Blood Gas InterpretationBlood Gas Interpretation
Normal valuespH between 7.36 and 7.44
PCO2between 36 and 44 mmHg
PO2between 80 and 100 mmHg
-
8/8/2019 Acute Respiratory Failure 2010
38/87
Blood Gas InterpretationBlood Gas Interpretation
Establish relationship between pH and PCO2Primary respiratory
disorder
Inverse relationship between changes in pH and PCO2
In acute disorders reciprocal change of 0.08 in pH for every
change of 10 mmHg PCO2
Primary metabolic disorder
Changes in pH and PCO2discordant or change in pH is of a
greater magnitude than expected by change in PCO2
-
8/8/2019 Acute Respiratory Failure 2010
39/87
-
8/8/2019 Acute Respiratory Failure 2010
40/87
Blood Gas InterpretationBlood Gas Interpretation
pH 7.24, PCO2 40Low pH with normal PCO2
Metabolic acidosis
pH 7.32, PCO2 30
PCO2 and pH both low
Metabolic acidosis with partial respiratory
compensation (respiratory alkalosis)
-
8/8/2019 Acute Respiratory Failure 2010
41/87
Acute Respiratory FailureAcute Respiratory Failure
Arterial carbon dioxide tension (PaCO2) greaterthan 50 mm Hg
concomitant with an arterial pH
less than 7.3
and/or
Arterial oxygen tension (PaO2) less than 50 mm
Hg when breathing room air at sea level
-
8/8/2019 Acute Respiratory Failure 2010
42/87
Bellows Failure - EtiologiesBellows Failure - Etiologies
Respiratory control centersdrugs, infections, bleeding,
trauma
Peripheral nerves
Guillain Barre syndrome, polio
Muscles
myotonic dystrophy, fatigue
Chest wall
kyphoscoliosis
-
8/8/2019 Acute Respiratory Failure 2010
43/87
Bellows Failure - EtiologiesBellows Failure - Etiologies
Respiratory control centersdrugs, infections, bleeding,
trauma
Peripheral nerves
Guillain Barre syndrome, polio
Muscles
myotonic dystrophy, fatigue
Chest wall
kyphoscoliosis
-
8/8/2019 Acute Respiratory Failure 2010
44/87
Ventilation vs. COVentilation vs. CO22
21 3 4 5 6 7 8 9 10
20
40
60
80
100
120
Alveolar ventilation
PaC
O2
-
8/8/2019 Acute Respiratory Failure 2010
45/87
Effects ofEffects ofHypercapneaHypercapnea
Decreased PaO2 proportional to rise in PaCO2 (A-agradient
normal)
Acidemia (compensated by metabolic changes if
the increase is gradual)
-
8/8/2019 Acute Respiratory Failure 2010
46/87
Lung FailureLung Failure
Characterized by hypoxemia with widened A-agradient
Hypercapnea not seen until later stages when
bellows failure supervenes
V/Q mismatch most common cause
easily corrected by supplemental oxygen
Intrapulmonary right-to-left shunting is refractory
to supplemental oxygen
. .
-
8/8/2019 Acute Respiratory Failure 2010
47/87
Lung InfectionsLung Infections
Among the most common causes of V/Qmismatch
Upper airway or bronchial infections decreaseairflow to the
distal alveoli
Infections of the distal airways and alveoli(pneumonia) disrupt
or totally obstruct airflow toan area of the lung
Release of inflammatory mediators mayparadoxically increase the
perfusion to these areasfurther lowering V/Q ratios
. .
. .
-
8/8/2019 Acute Respiratory Failure 2010
48/87
Supplemental Oxygen in V/Q MismatchSupplemental Oxygen in V/Q
Mismatch
Increasing the concentration of oxygen in inspiredair (FIO
2) increases P
AO
2
Increased PAO
2equilibrates with capillary blood
increasing PO2 and O2 content of blood leaving
thealveolo-capillary unit
Blood with higher O2content mixes with blood
from other units and increases Pa
O2
A-a gradient remains elevated
. .
-
8/8/2019 Acute Respiratory Failure 2010
49/87
ShuntShunt
Defined as areas of the lung where there isperfusion but no
ventilation (V/Q ratio = 0)
Refractory to supplemental oxygen
Arterial oxygen tension dependant upon mixed
venous oxygen tension
. .
-
8/8/2019 Acute Respiratory Failure 2010
50/87
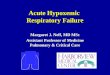
Shunt and Mixed Venous OxygenShunt and Mixed Venous Oxygen
PO2
0
20
40
60
80
100
20 40 60 80 100 120
SO
2%
140 200 300 400 500 6000
20
40
60
80
100
20 40 60 80 100 120
SO
2%
140 200 300 400 500 600
PO2
Oxygenated Shunt Mixed
-
8/8/2019 Acute Respiratory Failure 2010
51/87
ARDSARDS
A specific form of lung injury with diverse causescharacterized
pathologically by diffuse alveolar
damage and pathophysiologically by a breakdown
in both the barrier and gas exchange function of
the lung, resulting in proteinaceous alveolaredema and
hypoxemia
-
8/8/2019 Acute Respiratory Failure 2010
52/87
Adult Respiratory DistressAdult Respiratory Distress
Syndrome (ARDS)Syndrome (ARDS)
Characterized physiologically by stiff, non-compliant lungs
and refractory hypoxemia due to shunt
Multiple possible etiologies cause diffuse damage to the
alveolo-capillary membrane resulting in increased
vascularpermeability
Fluid accumulation in the alveolar and interstitial space
makes the lungs stiffer and inactivates surfactant causing
alveolar instability and collapse further reducing
lungcompliance
-
8/8/2019 Acute Respiratory Failure 2010
53/87
ARDS: Diagnostic CriteriaARDS: Diagnostic Criteria
Definitive
Diffuse bilateral alveolar edema
Increased lung vascular permeability
Diffuse alveolar damage at pathologic examination
OperationalDyspnea usually severe
Hypoxemia with PaO2 / FIO2 < 200
Bilateral radiographic infiltrates
Reduced respiratory system compliance
No evidence of cardiac etiology
-
8/8/2019 Acute Respiratory Failure 2010
54/87
ARDS: CausesARDS: Causes
Direct Lung InjuryDirect Lung Injury
Common causes
Pneumonia
Aspiration of gastric contents
Less common causes Pulmonary contusion
Fat emboli
Near-drowning
Inhalational injury Reperfusion injury
Indirect Lung InjuryIndirect Lung Injury
Common causes
Sepsis
Severe trauma with shock
and multiple transfusions
Less common causes
Cardiopulmonary bypass
Drug overdose
Acute pancreatitis Transfusion of blood
products
-
8/8/2019 Acute Respiratory Failure 2010
55/87
Pathophysiologic FeaturesPathophysiologic Features
Increased permeabilty of pulmonary vasculature
Loss of hypoxic vasoconstriction
Intrapulmonary right-to-left shunt
Increased pulmonary vascular resistance
-
8/8/2019 Acute Respiratory Failure 2010
56/87
Consequences of IncreasedConsequences of Increased
PermeabilityPermeability
Formation of shunt
Increase in ventilation to non-flooded alveoli
Loss of complianceOverdistension of ventilated alveoli
-
8/8/2019 Acute Respiratory Failure 2010
57/87
Lung ComplianceLung Compliance
Change in lung volume for any given change intranspulmonary
pressure
Normally about 80-100 ml/cm H2O
Early in ARDS, compliance decreases because of
reduced volume of aeratable lung
-
8/8/2019 Acute Respiratory Failure 2010
58/87
Lung Heterogeneity in ARDSLung Heterogeneity in ARDS
The lung in ARDS includes
Healthy tissue
Recruitable tissue
Diseased tissue
PEEP is used to open recruitable tissue and
maintain its patency throughout the inspiratory-
expiratory cycle
-
8/8/2019 Acute Respiratory Failure 2010
59/87
ARDSARDS
-
8/8/2019 Acute Respiratory Failure 2010
60/87
PEEP in ARDSPEEP in ARDS
Hypoxemia reversed through the use of positive
end expiratory pressure (PEEP)Prevents collapse of unstable
alveoli allowing
them to participate in gas exchangeOpened alveoli positioned on
a more compliant
portion of their pressure-volume curveDelivered tidal volume can
be distributed to more
alveoli reducing over-distention of the previouslyventilated
alveoli
-
8/8/2019 Acute Respiratory Failure 2010
61/87
Lung RecruitmentLung Recruitment
Gattinoni et al. NEJM, 2006
-
8/8/2019 Acute Respiratory Failure 2010
62/87
Effects of PEEP on ComplianceEffects of PEEP on Compliance
Pressure
Volume
{
{normal
ARDS
Alveolar
compliance
curve
-
8/8/2019 Acute Respiratory Failure 2010
63/87
Protective VentilationProtective Ventilation
NEJM 2001;344:1986
-
8/8/2019 Acute Respiratory Failure 2010
64/87
PEEP The Double Edged SwordPEEP The Double Edged Sword
Potential protective effects of PEEP
Reduction of shear stresses by preventing collapse of
alveoli
Reduction of high levels of FIO
2
Detrimental effects of PEEP
Decreased cardiac output
Overdistension of normal alveoli
-
8/8/2019 Acute Respiratory Failure 2010
65/87
Oxygen TransportOxygen Transport
Danger ofhypoxemia (low arterial oxygentension) is that it will
lead to insufficient
delivery of oxygen to the tissues (hypoxia)
leading to cellular dysfunction, lacticacidosis, and potential
cell death
-
8/8/2019 Acute Respiratory Failure 2010
66/87
Causes of HypoxiaCauses of Hypoxia
Reduced O2Delivery
Low cardiac output (heart failure, tamponade)
Low hemoglobin concentration (anemia)
Low arterial oxygen tension
Reduced O2 unloading in tissues High oxygen-hemoglobin affinity
(alkalosis, reduced 2,3 DPG,
abnormal hemoglobin)
Impaired O2utilization in mitochondrion
Enzyme poisons (cyanide)
-
8/8/2019 Acute Respiratory Failure 2010
67/87
Lung and Bellows FailureLung and Bellows Failure
Fatigue - the inability of a muscle to continue to
develop or maintain a predetermined force
When energy demands become excessive, fatigue
results and inspiratory muscles fail to generate or
sustain minute ventilation required to maintainnormal arterial
carbon dioxide tension
Characteristics - elevated arterial PCO2, hypoxemia
with an increased A-a gradient
-
8/8/2019 Acute Respiratory Failure 2010
68/87
Respiratory MusclesRespiratory Muscles
-
8/8/2019 Acute Respiratory Failure 2010
69/87
Diaphragmatic InsertionsDiaphragmatic Insertions
Di h ti O i t tiDi h ti O i t ti
-
8/8/2019 Acute Respiratory Failure 2010
70/87
Diaphragmatic OrientationDiaphragmatic Orientation
Di h ti O i t tiDi h ti O i t ti
-
8/8/2019 Acute Respiratory Failure 2010
71/87
Diaphragmatic OrientationDiaphragmatic Orientation
fW k f B thi
-
8/8/2019 Acute Respiratory Failure 2010
72/87
Work of BreathingWork of Breathing
Force required to move air into and out of alveoli
per unit time
Determinants
Compliance of the lung
Resistance of the airways
Minute ventilation
Frequency and tidal volume
I i t M l St thI i t M l St th
-
8/8/2019 Acute Respiratory Failure 2010
73/87
Inspiratory Muscle StrengthInspiratory Muscle Strength
AtrophyNeuromuscular disease
Nutritional status
Oxygen deliveryLung volume
M h i l I di t i COPDM h i l I di t i COPD
-
8/8/2019 Acute Respiratory Failure 2010
74/87
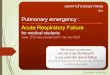
Mechanical Impediments in COPDMechanical Impediments in COPD
Thoracic cage
elastic recoil
directed inwards
Shortened
muscle fibers
Decreased
diaphragmatic
curvature
Medial orientation
of diaphragmatic fibers
Decreased zone
of apposition
Horizontal ribs
L Pl LL Pl L
-
8/8/2019 Acute Respiratory Failure 2010
75/87
LaPlaces LawLaPlaces Law
P=2Tr
Where:
P = pressure
T = tension
r = radius of curvature
P ti I dP ti I d
-
8/8/2019 Acute Respiratory Failure 2010
76/87
Pressure-time IndexPressure-time Index
0
0.5
1
0 10.5
Fatigue
Criticalzone
Duratio
n
(TI
/T
tot
)
Force (Pdi / Pdi max )
TI = Inspiratory time
Ttot = Inspiratory + expiratory timePdi = Pressure generated by
diaphragm
Pdimax = Maximum pressure diaphragm can generate
DD
-
8/8/2019 Acute Respiratory Failure 2010
77/87
DyspneaDyspnea
An uncomfortable awareness of breathing
Corresponds to several factors
increased ventilatory drive
length-tension inappropriateness
pulmonary arterial or venous hypertension
hypoxemia and hypercapnea
cortical influences including depression and anxiety
fF t I fl i D
-
8/8/2019 Acute Respiratory Failure 2010
78/87
DYSPNEA
Cortical influences
(depression, anxiety)
Length-tension
inappropriateness
Respiratory
drive
Vagal
reflexes
Pulmonary edema
Pulmonary
hypertension
Ventilatorydrive
PaO2
PaCO2 pH
Respiratory muscle
weakness or fatigue
Neuromuscular
disease
Malnutrition
Impediment to
breathing
Hyperinflation
Airway
obstruction
COPDAsthma
Factors Influencing DyspneaFactors Influencing Dyspnea
Chronic COChronic CO RetentionRetention
-
8/8/2019 Acute Respiratory Failure 2010
79/87
Chronic COChronic CO22 RetentionRetention
Seen most commonly in patients with high
inspiratory work loads (chronic bronchitis or
obesity)
May help reduce the work of breathing and
prevent acute diaphragmatic fatigue
Chronic COChronic CO RetentionRetention
-
8/8/2019 Acute Respiratory Failure 2010
80/87
Chronic COChronic CO22 RetentionRetention
In order to maintain a constant level of arterial PCO2, a
person must excrete the same amount of carbon dioxide
as the body produces each minute
The amount of carbon dioxide excreted is determined by
the amount delivered to the alveolus by the blood vs.
thealveolar ventilation
Blood with elevated PCO2delivers more CO
2to the
alveolus so each breath can excrete more at the same
alveolar ventilation
Chronic COChronic CO RetentionRetention
-
8/8/2019 Acute Respiratory Failure 2010
81/87
Chronic COChronic CO22 RetentionRetention
Drawbacks
worsening hypoxemia through decrease in alveolar
oxygen tensions
acidosis (will have renal compensation)
Response of Respiratory Drive to COResponse of Respiratory Drive
to CO
-
8/8/2019 Acute Respiratory Failure 2010
82/87
Response of Respiratory Drive to COResponse of Respiratory Drive
to CO22
40 50 60 70 80 90
10
20
PaCO2
P0.1
(mm
Hg
)
Normocapnic COPD
Normal
Hypercapnic COPD
Ch i H d OCh i H d O
-
8/8/2019 Acute Respiratory Failure 2010
83/87
Chronic Hypercapnea and OxygenChronic Hypercapnea and Oxygen
TherapyTherapy Patients with chronic hypercapnea and hypoxemia
will
often have further increases in arterial PCO2when given
supplemental oxygen
Etiologies decreased minute ventilation
increased V/Q mismatch
Haldane effect
. .
D d Mi t V til tiDecreased Minute Ventilation
-
8/8/2019 Acute Respiratory Failure 2010
84/87
Decreased Minute VentilationDecreased Minute Ventilation
Long postulated that patients are dependent onhypoxic drive to
maintain ventilation
Supplemental oxygen felt to improve hypoxemia,
decreasing driveStudies have not confirmed this to be a
factor
.. ..V/Q Mi t h
-
8/8/2019 Acute Respiratory Failure 2010
85/87
Increases in alveolar PO2from the supplemental
oxygen decrease hypoxic vasoconstriction of
vessels supplying poorly ventilated alveoli
Increases in perfusion to alveolus are initially not
matched by increases in ventilation causingworsening V/Q
ratios
V/Q MismatchV/Q Mismatch
..
/QV/Q Mi t h. .
-
8/8/2019 Acute Respiratory Failure 2010
86/87
V/Q MismatchV/Q Mismatch
Decreasing V/Q ratio increases the PCO2of the
blood leaving the alveolocapillary unit
Normal individuals compensate for this increase
by increasing minute ventilation
Patients with preexisting hypercapnea do not
increase their ventilation to compensate
. .
-
8/8/2019 Acute Respiratory Failure 2010
87/87