Embed Size (px)
Citation preview

• Ali, Muhammad, Yair Safriel, Jaideep Sohi, Alfred Llave, and Susan Weathers. "West Nile Virus Infection: MR Imaging Findings in the Nervous System." American Journal of Neuroradiology 26, no. 2 (February 2005): 289-97. • Hart, John, Gail Tillman, Michael A. Kraut, Hsueh-Sheng Chiang, Jeremy F. Strain, Yufeng Li, Amy G. Agrawal, Penny Jester, John W. Gnann, and Richard J. Whitley. "West Nile Virus Neuroinvasive Disease: Neurological Manifestations and
Prospective Longitudinal Outcomes." BMC Infectious Diseases 14, no. 1 (2014). doi:10.1186/1471-2334-14-248. • Hughes, J. M., M. E. Wilson, and J. J. Sejvar. "The Long-Term Outcomes of Human West Nile Virus Infection." Clinical Infectious Diseases 44, no. 12 (2007): 1617-624. doi:10.1086/518281.
• Iro, Mildred. "IgNiTE: Immunoglobulin in the Treatment of Encephalitis." Http://isrctn.com/, 2015. doi:10.1186/isrctn15791925.
• Kennard, Christopher, and Michael Swash. "Acute Viral Encephalitis Its Diagnosis And Outcome." Brain 104, no. 1 (1981): 129-48. doi:10.1093/brain/104.1.129. • Klee, Anne L., and Beth Maldin. "Long-Term Prognosis for Clinical West Nile Virus Infection." Emerging Infectious Diseases 10, no. 8 (August 2004): 1405-411.
• Ledermann, Jeremy P., Maria A. Lorono-Pino, Christine Ellis, Kali D. Saxton-Shaw, Bradley J. Blitvich, Barry J. Beaty, Richard A. Bowen, and Ann M. Powers. "Evaluation of Widely Used Diagnostic Tests To Detect West Nile Virus Infections in Horses Previously Infected with St. Louis Encephalitis Virus or Dengue Virus Type 2." Clinical and Vaccine Immunology 18, no. 4 (2011): 580-87. doi:10.1128/cvi.00201-10.
• Malan, A. K., T. B. Martins, H. R. Hill, and C. M. Litwin. "Evaluations of Commercial West Nile Virus Immunoglobulin G (IgG) and IgM Enzyme Immunoassays Show the Value of Continuous Validation." Journal of Clinical Microbiology 42, no. 2 (2004): 727-33. doi:10.1128/jcm.42.2.727-733.2004.
• Murray, Kristy O., Melissa S. Nolan, Shannon E. Ronca, Sushmita Datta, Koushik Govindarajan, Ponnada A. Narayana, Lucrecia Salazar, Steven P. Woods, and Rodrigo Hasbun. "The Neurocognitive and MRI Outcomes of West Nile Virus Infection: Preliminary Analysis Using an External Control Group." Frontiers in Neurology 9 (2018). doi:10.3389/fneur.2018.00111.
• Rosas, Humberto, and Franz Wippold. "West Nile Virus: Case Report with MR Imaging Findings." American Journal of Neuroradiology 24, no. 7 (August 2003): 1376-378.
• Solomon, T., NM Dung, and B. Wills. "Interferon Alfa-2a in Japanese Encephalitis: A Randomised Double-blind Placebo-controlled Trial." The Lancet 9360 (March 8, 2003): 821-26.
• Thakur, K. T., M. Motta, A. O. Asemota, H. L. Kirsch, D. R. Benavides, E. B. Schneider, J. C. Mcarthur, R. G. Geocadin, and A. Venkatesan. "Predictors of Outcome in Acute Encephalitis." Neurology 81, no. 9 (2013): 793-800. doi:10.1212/wnl.0b013e3182a2cc6d.
• Tyler, Kenneth L., M.D. "Acute Viral Encephalitis." N Engl J Med 379 (August 9, 2018): 557-66. • Vector Disease Control International. "West Nile Virus: Education, Public Health, Mosquito Management." Yellow Fever: Education, Public Health, Integrated Mosquito Management. Accessed September 06, 2018.
http://www.vdci.net/vector-borne-diseases/west-nile-virus-education-and-mosquito-management-to-protect-public-health.
• "West Nile Virus." Centers for Disease Control and Prevention. August 15, 2017. Accessed September 06, 2018. https://www.cdc.gov/westnile/healthcareproviders/index.html
Introduction
Acute Viral Encephalitis due to West Nile Virus Jarrod Tembreull, MD
Internal Medicine - Pediatrics Residency, Maine Medical Center, Portland, ME
- Started on antibiotics including levoquin & doxycycline on admission (received vancomycin & cefepime in ED) - MRI Brain with global volume loss & non-specific white matter changes that may reflect small vessel disease. There is no mass, hydrocephalus or acute infarction. - Deterioration in exam with increasing lethargy & new tremor on hospital day #5 – broadened to vancomycin and cefepime - Unable to obtain LP given treatment with plavix & considered likely low yield given antibiotics – Discussed with Infectious Disease & Neurology, consults pending.
Cefepime discontinued due to concern of drug fever and potential for cefepime neurotoxicity - Patient noted to have decreased responsiveness with whole body myoclonus on HD #7. Intubated for respiratory protection - Continuous EEG with no evidence of seizure activity – started on fosphenytoin for seizure prophylaxis - STAT Head CT with no acute intracranial process. - LP obtained on HD#7 – notable for pleocytosis, multiple labs ordered - Continued on broad spectrum antibiotics including acyclovir, ampicillin, doxycycline, meropenem, & vancomycin - Sedative medications discontinued on HD#9 with no improvement in mental status for >36 hours – started on amantadine - Positive confirmatory results for West Nile Virus Ab, IgG, and IgM resulted on HD#13 - Patient extubated with daily improvement in mental status on HD#13. - Discharged to acute rehab on HD#17 with plan to complete month long course of amantadine in addition to two week course of fosphenytoin
History of Present Illness: Patient is an 86 year old man with past medical history as noted below who presents with fever, weakness, and episodes of confusion for two days. Patient had been working outdoors on his yard in Baton Rouge, LA for several hours in 97°F+ heat prior to the onset of his symptoms. That evening he seemed to be overheated and had decreased ability to ambulate with reported fever. Family cooled him and provided rehydration before patient insisted on traveling to Portland. He continued to feel ill with generalized weakness while traveling and developed one episode of diarrhea and one episode of emesis. Upon arrival his family noted him to be very weak and dehydrated, requiring a wheelchair to transport from the airport. Patient normally is fully independent in all activities. On the morning prior to presentation to the ED patient was noted by family to be confused while only intermittently responding to questions in addition to decreased intake. He was noted to have a oral temperature of 104°F the morning prior to presentation. In the ED patient was responding appropriately. He denied any focal complaints other than diarrhea & emesis including no dyspnea, cough, abdominal pain, rashes, headache, or neck pain. He denied any recent sick contacts. PMH: CKDIII, Diabetes, Hypertrygliceridemia, GERD, peripheral vascular disease SH: Lives in Baton Rouge, LA with wife. Retired geology professor. No smoking, alcohol, or illicit drug use FH:No significant family history of stroke, heart disease, or cancer Medications: atenolol 100mg QD, clopidogrel 75mg QD, darbepoitin 25mcg q30d, fenofibrate 145mg QD, latanoprost 0.005% 1 drop each eye QHS, omeprazole 20mg QD, rosuvasatin 20mg QD, vitamin B complex 1 tab QD Allergies: None known Physical Exam: Vitals: Temp 38.1 °C, BP 89/50, Pulse 85, RR 17, SpO2 100% on Room Air GEN: Alert, elderly male lying on bed comfortably in no acute distress HEENT: Normocephalic, atraumatic; PERRL, EOMs intact. Oropharynx clear, moist mucus membranes Neck: Supple, No lymphadenopathy, no carotid bruit and no JVD CV: Regular rate & rhythm, S1, S2 normal, no murmur Pulm: Clear to auscultation bilaterally. Abd: Soft, nontender. Bowel sounds normal. No masses no organomegaly. Back: Symmetric, ROM normal. No CVA tenderness Extremites: No cyanosis or edema Pulses: 2+ and symmetric all extremities Skin: Normal turgor, no rashes or lesions Neurologic: CNII-XII intact. Normal strength, sensation, and reflexes throughout
Case Description
Laboratory Findings Epidemiology and Clinical Presentation • 20-50% of cases of encephalitis with a known cause are attributed to a viral etiology • Incidence of West Nile Virus neuroinvasive disease varies drastically based mostly on
age, region, and seasonality but is the most commonly diagnosed arbovirus in the U.S. • 1 in 150 people who are infected with WNV develop neuroinvasive disease (encephalitis
or meningitis) • West Nile Virus was first introduced to the United States in 1999, since this time there
have been >46,000 cases of WNV reported and >21,000 cases of neuroinvasive disease have been reported
• The Culex species of mosquito is the main vector for WNV and is active in all 48 contiguous states
• There have been only 2 cases of WNV reported in Maine since 1999 • Louisiana has one of the highest reported incidence rates of WNV infection in the U.S. • The most common symptoms include fever, headaches, generalized weakness, vomiting,
diarrhea, and rash Diagnosis • NEJM suggests a tiered approach to diagnosis of viral encephalitis. Tier 1 includes HSV,
VZV, enterovirus PCR, & arbovirus serum testing based on geographic region • West Nile Virus Antibody Testing is commonly available for both CSF and serum • There can be cross reactivity of IgM antibodies with other flaviviruses however a
positive WNV IgM is still >95% specific for WNV infection • IgM antibodies are present within 3-8 days of infection. • Both sensitivity & specificity of IgG testing is >98% • PRNT, RT-PCR & viral cultures are also available for confirmation generally through
state public health laboratories or the CDC
Therapy & Outcomes • Mainstay of treatment for WNV neuroinvasive disease remains supportive care • IDSA guidelines recommend the use of acyclovir for HSV encephalitis (A-level recommendation; I
level quality of evidence) but there are no recommendations or evidence for antiviral treatment of WNV encephalitis
• Randomized, placebo controlled have found no benefit of interferon alfa or IVIG treatment for WNV or other flaviviruses
• There is an active multicenter trial assessing use of early IVIG in children with acute encephalitis
• >40% of patients hospitalized for WNV continued to experience deficits (i.e. weakness, fatigue, insomnia, etc) at 18 months post-hospitalization
• Poor prognostic indicators for recovery include age >65, female sex, need for ICU admission, GCS score of <8, cerebral edema, and development of status epilepticus
129
2.9
94 29 20
135 2.34
11.6 10.7
32.1 270
93% PMNs
MCV: 89.1 AST: 80 ALT: 39 Alk Phos: 34 Albumin: 4.1 Bili: 0.7
CSF Cell Count
Positive Tests
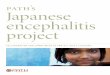
Figure 1. A) FLAIR imaging of patient obtained on HD#1 B) FLAIR showing increased signal in thalami and lentiform nucleus in patient with WNV C) FLAIR image from patient with known WNV with bilateral hyperintensity in basal ganglia and thalami
References
Acute encephalitis is a common presenting symptom to the hospital and carries a broad differential diagnosis. Viral etiologies account for up to half of the known causes of acute encephalitis. Arboviruses such as West Nile virus are a commonly considered yet overall rarely diagnosed (0.45 cases per 100,000 population nationally for West Nile Virus) cause of acute encephalitis. The CDC monitors incidence and prevalence of West Nile Virus neuroinvasive disease through ArboNET. It is important to take a step-wise approach in diagnosis of etiology of encephalitis and consider the patients full travel history for exposure risks.
Imaging A
Graphs. A) Average Annual Incidence of WNV Neuroinvasive Disease reported to CDC by Age Group, 1999-2016, B: WNV Disease cases reported to CDC by Week of Illness Onset, 1999-2016
C C
Discussion
Glucose: 68 Protein: 116 Leukocytes: 259 Erythrocytes: 386
CSF Arbovirus Panel: Positive WNV IgM *Includes EEE IgM, St. Louis Encephalitis IgM, Powassan RT-PCR, Deer Tick Virus RT-PCR
Serum WNV Ab IgG, IgM: Positive for IgM & IgG
Serum - Negative/normal Tick Panel (Anaplasma/Babesia/Ehrlichia)
Blood Parasite Smear x2 Legionella Ag (Urine) HIV 1+2 Ab+Ag Treponema Pallidum IgG/IgM C. difficile Toxin
CSF - Negative/normal HSV 1+2 QL PCR VDRL VZV PCR + Ab IgG/IgM Lyme Western Blot MTB complex PCR
Culture Data Urine Cultures: Negative Blood Cultures: Negative Stool Culture: Negative CSF Cultures plus Acid Fast &Fungal: Negative
Image A: Average Annual Incidence of WNV Neuroinvasive Disease Reported to CDC, 1999-2016
Image B: 2018 WNV Neuroinvasive Disease Incidence by State (as of 8/21/18) Image C: 2018 WNV Activity by State (as of 8/21/18)
B
BA
Hospital Course and Treatment
Incidence of WNV Neuroinvasive Disease



![Clinical characteristics and long-term prognosis of ... · other possible causes, such as viral encephalitis and herpes simplex encephalitis. Relapsing anti-NMDAR encephalitis [5]](https://img.pdfslide.net/doc/110x75/5f5cb978af3eab35a02f3630/clinical-characteristics-and-long-term-prognosis-of-other-possible-causes-such.jpg)





![Challenges in viral CNS infections [encephalitis] · Challenges in viral CNS infections [encephalitis] Definition Encephalitis is defined as a syndrome of neurological dysfunction](https://img.pdfslide.net/doc/110x75/5e220e3e60d1c1105809daf5/challenges-in-viral-cns-infections-encephalitis-challenges-in-viral-cns-infections.jpg)