Embed Size (px)
Citation preview

DISEASES OF THE PANCREAS, SERIES #9
48� PRACTICAL�GASTROENTEROLOGY� •� DECEMBER�2014
Rad M. Agrawal, M.D., Series Editor
Satyanisth Agrawal, DO, Elie Aoun, MD West Penn Allegheny Health System, Division of Gastroenterology, Pittsburgh, PA
The Physiology of the Pancreas
Satyanisth Agrawal
INTRODUCTION
When originally studied, the pancreas was one of the last organs in the abdomen to catch critical attention of anatomists and physiologists.1 New
imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) have enhanced the understanding of pancreas anatomy and made possible the surgical, endoscopic and percutaneous manipulation of pancreas.2
AnatomyThe pancreas is a flat, long, and soft gland that is roughly 6 inches in length and weighs between 70 and 110 g. It lies obliquely in the retroperitoneal space of the upper abdomen and is covered by the stomach, transverse colon, and transverse mesocolon. The head of the pancreas lies next to the duodenal sweep at the level of the body of L2.3,4 The neck, body, and tail span leftward, with the tail extending close to the spleen.5
Functional AnatomyThe pancreas consists of ≥80% of acini that are arranged in clusters that form lobules separated by loose connective tissue. A circular shaped acinus and
its tubular draining ductule form the functional unit of exocrine pancreas.6 Many acini arranged like a bouquet secrete digestive enzymes into the ductule which drains into interlobular ducts and finally into the main pancreatic ductal system.
Pancreatic acinar cells are specialized exocrine secretory cells that synthesize, store, and secrete the digestive enzyme component of the pancreatic juice. An acinar cell is shaped like a triangle, with the basal membrane pointed outward for neurohormonal receptors and the apical membrane located inward forming the lumen of an acinus. The nucleus and rough endoplasmic reticulum (RER) are located near the basal membrane for protein synthesis.7 Zymogen granules that store digestive enzymes are located near the apical membrane and hence close to the lumen. Tight junctions between acinar cells form a barrier between the lumen and apical membrane to prevent inappropriate passage of enzymes but allow water and ions to go through.8,9 Secretagogues stimulate acinar cells causing the granules to fuse with each other and the apical membrane. Microvilli covering the apical surface of acinar cells facilitate exocytosis of enzymes into the lumen. Gap junctions between adjacent acinar cells allow coordinated chemical and electrical communication between cells for passage of small molecules such as calcium and other ions important for digestive enzyme secretion.
Elie Aoun

DISEASES OF THE PANCREAS, SERIES #9
The Physiology of the Pancreas
PRACTICAL�GASTROENTEROLOGY� •� DECEMBER�2014� 49
DISEASES OF THE PANCREAS, SERIES #9
The ducts collect pancreatic enzymes, and the activity of the ductular cells dilutes and alkalinizes pancreatic juice before it is washed out into the small intestine. The duct epithelium is made of cuboidal columnar cells held together by intercellular tight junctions. These ductular cells are packed with mitochondria to supply energy for ion transport. Once stimulated, these cells transport bicarbonate ions into the pancreatic juice as it passes along the duct, with water following in response to the resulting transepithelial osmotic gradient.10
Exocrine SecretionsPancreatic exocrine secretions, nearly 2.5L/day in volume, can be classified in two groups: organic and inorganic. Organic secretions are proteins such as digestive enzymes and inorganic secretions consist mostly of water and electrolytes. Acinar cells secrete digestive enzymes and ductal cells secrete bicarbonate rich electrolyte solution.11 Depending on the organic secretion, the enzyme component of pancreatic juice is mixed in various proportions with the aqueous component. Greater than 75% of proteins in organic secretions are enzymes and proenzymes; the rest are plasma proteins, trypsin inhibitors, and mucoproteins (Table 1).
Organic SecretionsOne of the major purposes of the pancreas is to synthesize digestive enzymes and deliver them to the intestine where they play a critical role in digestion. The four major enzyme groups are proteolytic (eg, chymotrypsin), amylolytic (eg, amylase), lipolytic (eg, lipase), and nuclease digestive enzymes. Some of the enzymes are present in more than one form (e.g., cationic trypsinogen, anionic trypsinogen, and mesotrypsinogen).12 To prevent auto digestion of the pancreas, and hence pancreatitis, enzymes are stored and secreted as inactive precursor forms. Enterokinase, secreted by duodenal mucosa, converts trypsinogen to its active form trypsin, which then catalyzes the activation of the other inactive proenzymes. The acinar cells also secrete a trypsin inhibitor, which inactivates trypsin by disabling this catalytic action.13
Inorganic SecretionsPancreatic electrolytes (sodium, potassium, chloride, and bicarbonate) mixed with water form an alkaline fluid that is isosmotic with extracellular fluid and
helps neutralize gastric acid entering the duodenum.14 Postprandial stimulation mediated mainly by secretin increases secretory flow rate from an average of 0.3 mL/minute in the resting (interdigestive) state to 4.0 mL/minute in the digestive state. The concentrations of bicarbonate and chloride in pancreatic juice change reciprocally as secretory flow rate increases making the osmolality of pancreatic juice independent of flow rate.15
Digestive Enzyme Functions
Amylase
The salivary glands and pancreas make amylases. Pancreatic amylase hydrolyzes the 1,4-glycoside linkages of complex carbohydrates and starches. This produces short dextrins, which can then be digested by brush border enzymes like maltose and maltotriose into glucose.
LipasesThe majority of dietary lipids in western diets are triglycerides, which cannot be digested by brush border enzymes. Pancreatic triglyceride lipase binds to the oil-water interface of the triglyceride oil droplet where it cleaves the majority of fatty acids from dietary triglycerides.
Bile acids and colipase are important for the full activity of lipases. Bile acids emulsify triglyceride molecules to expand surface area for lipase to act on.16 Colipase forms a complex with lipase and bile salts and anchors lipase to allow it to act in a more hydrophilic
Table 1. Pancreatic Acinar Cells Secretory ProductsProenzymes Enzymes
Cationic trypsinogen (PRSS1) Amylase
Anionic trypsinogen (PRSS2) Carboxylesterase
Mesotrypsinogen (PRSS3) Sterol esterase
Chymotrypsinogen B1, B2 Lipase
Kallireinogen DNase
Procarboxypepsidase A (1,2) RNase
Procarboxypepsidase B (1,2)
Proelastase

The Physiology of the Pancreas
DISEASES OF THE PANCREAS, SERIES #9
50� PRACTICAL�GASTROENTEROLOGY� •� DECEMBER�2014
will result in increased expression of amylase compared to other pancreatic enzymes. Zymogen granules then move towards the apical membrane of acinar cells via microtubules and await appropriate neurohormonal stimulus to trigger exocytosis.20
Facilitated by microvilli covering apical surface of acinar cells, exocytosis is a process where the zymogen granule fuses with the apical surface and allows its contents to be released in the ducts.21 This entire process takes less than 1 hour allowing the pancreas to be ready for the next meal by repeating synthesis and packaging of enzymes.
Cellular Regulation of Enzyme SecretionAt the cellular level, secretion of pancreatic juice can be divided into organic and inorganic secretions. Organic secretions containing pancreatic enzymes occurs by regulating acinar cells, and inorganic secretions containing bicarbonate and other electrolytes occurs by regulating ductal cells. Hormonal regulation of acinar and ductal cells is explained in this section and the integrated neurohormonal control of pancreatic secretion is discussed later.
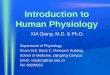
Acinar CellsAcinar cells express receptors on their basolateral membranes for the following hormones: cholecystokinin (CCK), acetylcholine (ACh), gastrin-releasing peptide (GRP), vasoactive intestinal peptide (VIP), and secretin.22,23 These receptors are divided into two groups based on their mode of stimulating acinar cells (Figure 1). VIP and secretin activate adenylate cyclase, which increases cellular cAMP and facilitates enzyme secretion through cAMP dependent protein kinase A. The other group consisting of acetylcholine, GRP, and CCK lead to an increase in intracellular free calcium concentrations via stimulating cellular metabolism of membrane phosphoinositides.24 This phospholipase C-dependent pathway is the primary stimulus for significant acinar secretion, with cAMP-dependent signaling playing a secondary role.
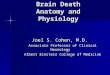
Ductular CellsDuctular cells contribute the fluid and bicarbonate components of pancreatic juice. Bicarboanate is predominantly derived from plasma rather than intracellular metabolism. Both the apical and basolateral membranes have polarized epithelial cells
(continued on page 52)
environment on the hydrophobic surface of the oil droplet. Carboxyl ester lipase can act on a variety of substrates and is important in digestion of cholesterol esters, lipid-soluble vitamins such as Vitamin A, and triglycerides.
ProteasesPancreatic proteases and gastric pepsin digest all of the complex dietary proteins into short peptides and amino acids for further digestion and absorption in the intestine. The most abundant enzyme is trypsin, which is present in three forms. Cationic trypsinogen, coded by PRSS1 gene, is present in a large proportion, and anionic trypsinogen and mesotrypsinogen, which are coded by PRSS2 and PRSS3 genes, respectively, are present in smaller proportions. All trypsinogens act similarly by attacking the exposed arginine and lysine residues within a peptide chain. Chymotrypsin and elastase are endopeptidases, just like trypsin, that cleave specific peptide bonds adjacent to specific amino acids. These amino acids eventually have greater effects on stimulating pancreatic secretion, inhibiting gastric emptying, regulating small bowel motility, and causing satiety.
Synthesis and Transport of Digestive EnzymesProtein synthesis occurs in the ribosomes close to the rough endoplasmic reticulum (RER) of acinar cells.17
The cell’s messenger RNA (mRNA) then translates these newly synthesized proteins into exportable proteins. A terminal peptide extension on pancreatic enzymes, known as signal protein, allows attachment and entry of the enzyme into the RER.18 The enzyme and signal protein interact with a membrane protein called a docking protein. This process permits the completion of the translocation, dissociation of the signal protein and mRNA from enzyme, and allows the enzyme to enter RER. Newly synthesized proteins can undergo modifications and conformational changes in the endoplasmic reticulum before being transported to the Golgi complex where further post-translational modification (glycosylation), sorting, and concentration occur.19
Digestive enzymes are then transported to the zymogen granules. A given zymogen granule has various pancreatic proteins mixed in relative proportions depending on their rates of synthesis. The rate of synthesis of a particular enzyme is related to the type of diet. For example, dietary increase in carbohydrates

52� PRACTICAL�GASTROENTEROLOGY� •� DECEMBER�2014
DISEASES OF THE PANCREAS, SERIES #9
The Physiology of the Pancreas
stimulation arises from cholinergic vagal input during the cephalic phase, and vago-vagal reflexes activated by gastric distension during the gastric phase. Gastric distention predominantly causes secretion of enzymes with little secretion of water and bicarbonate.28
The intestinal phase begins when chyme leaves stomach and enters the small intestine. During the intestinal phase, ductular secretion is strongly activated, resulting in the production of high volumes of pancreatic juice with decreased concentrations of protein, although the total quantity of enzymes secreted during this phase is actually also markedly increased. Ductular secretion during this phase is driven primarily by the endocrine action of secretin on receptors localized to
and membrane transport proteins that help with ion transportation (Figure 2). Ductal cells are very sensitive to secretin and VIP, both of which increase intracellular cAMP, which in turn leads to opening of CFTR chloride channels initiating secretion.14,15 Bicarbonate enters through the sodium-bicarbonate cotransporter on the basolateral membrane and exits through the CFTR channel on the apical membrane.25 Concomitantly, the sodium-potassium pump keeps the intracellular sodium low thus creating a continual electrochemical force and driving bicarbonate into the ductal cell through the sodium-bicarbonate cotransporter. Water and sodium ions follow paracellularly in response to the electrochemical gradient across the epithelium.
Organ Physiology Exocrine pancreatic secretion happens during two states: fasting (interdigestive) and after ingestion of a meal (digestive). The interdigestive pattern of secretion begins when the stomach is empty. Secretory activity related to eating (digestive state) occurs in phases: cephalic (20-25%), gastric (10%), and intestinal (approximately 60%-70%). Pancreatic secretion is activated by a combination of neural and hormonal effectors.
Interdigestive SecretionsThe interdigestive pancreatic secretions are governed by the cholinergic nervous system, motilin, and pancreatic polypeptide. Secretions follow the cyclical pattern of the migrating myoelectric complex (MMC) [26, 27]. Enzyme secretion occurs every 1 to 2 hours and is associated with the periods of increased motor activity in the stomach and duodenum. In addition to pancreatic enzyme secretion, there is increased secretion of bicarbonate and bile (secondary to partial gallbladder contraction) into the duodenum. The pancreatic secretion during the interdigestive phase is integral to the “housekeeping” function of the MMC to clear the stomach and small intestine of debris including bacteria between meals.26
Digestive SecretionsSecretion with ingestion of a meal is divided into three phases: cephalic, gastric, and intestinal. During the cephalic and gastric phases, secretions are low in volume with high concentrations of digestive enzymes, reflecting stimulation primarily of acinar cells. This
Figure 1.
Figure 2.
(continued from page 50)

DISEASES OF THE PANCREAS, SERIES #9
The Physiology of the Pancreas
PRACTICAL�GASTROENTEROLOGY� •� DECEMBER�2014� 53
Table 2. Pancreatic Function Tests
Indirect/Non-Invasive Tests:• Do not require IVS or tubes• Detection of severe exocrine pancreatic dysfunction• Insensitive for detecting mild or moderate pancreas dysfunction
Test Description Utility
Fecal fat Measure fat content in stool after ingesting meals with a known amount of fat
Provides quantitative measurement of steatorrhea
Fecal chymotrypsin or Elastase
Measure chymotrypsin or elastase in stool*no oral ingestion needed
Widely available testHigh clinical utility
NBT-PABA (N-benzoyl-l-tyrosyl-p-aminobenzoic acid) and Fluorescein dilaurate
Measure PABA or fluorescein in serum or urine after oral ingestion of NBT-PABA or fluorescein dilaurate with a meal
Easier to obtain than stool samplesUnreliable in patients with small bowel mucosal disease
Direct/Invasive tests:• Most sensitive and specific • Require duodenal intubation and IV administration of hormones• Not widely available
Test Description Utility
Secretin Measure volume of pancreas secretion andbicarbonate secretion into the duodenum after IV secretin
Detects mild, moderate,or severe exocrinepancreatic dysfunction
Cholecystokinin Measure duodenaloutput of amylase, trypsin,chymotrypsin, and lipase after IV cholecystokinin
Detects mild, moderate,or severe exocrinepancreatic dysfunction
Indirect/Invasive Tests:• No IV administration of hormones• Requires duodenal intubation, oral ingestion, and normal small bowel • Not widely available
Test Description Utility
Lundh test meal Measure duodenal trypsin concentration after ingestion of a test meal
Detects moderate or severe pancreatic dysfunction

The Physiology of the Pancreas
DISEASES OF THE PANCREAS, SERIES #9
54� PRACTICAL�GASTROENTEROLOGY� •� DECEMBER�2014
the basolateral pole of duct epithelial cells. The inputs to the acinar cells during the intestinal phase include CCK as well as neurotransmitters including acetylcholine (ACh), GRP, and VIP.29-31 The large magnitude of the intestinal phase is also attributable to amplification by so-called enteropancreatic reflexes transmitted via the enteric nervous system.
CCK is released from the upper small intestinal mucosa by digestion products of fat, protein, and starch. CCK is a potent stimulus of acinar secretion, acting both directly on CCK-B receptors localized to the basolateral membranes of acinar cells (Figure 1), and via stimulation of vagal afferents close to its site of release in the duodenum, thereby evoking vago-vagal reflexes that stimulate acinar cell secretion via cholinergic and noncholinergic neurotransmitters (the latter including both GRP and VIP).32 In addition to its effects on the pancreas, CCK coordinates the activity of other GI segments and draining organs, including contraction of the gallbladder, relaxation of the sphincter of Oddi, and the slowing of gastric motility to retard gastric emptying and thereby control the rate of delivery of partially digested nutrients to more distal segments of the gut.33 Finally, CCK modulates the activity of secretin in a synergistic fashion by markedly potentiating the effect of secretin as an agonist of pancreatic ductular secretion of bicarbonate.31
The other major regulator of pancreatic secretion is secretin, which is released from S cells in the duodenal mucosa by gastric acid, with a pH threshold of 4.5.34 When the meal enters the small intestine from the stomach, the volume of pancreatic secretions increases rapidly, shifting from a low-volume, protein-rich fluid to a high volume secretion in which enzymes are present at lower concentrations (although in greater absolute amounts, reflecting the effect of CCK and neural effectors on acinar cell secretion). As the secretory rate rises, the pH and bicarbonate concentration in the pancreatic juice rises, with a reciprocal fall in the concentration of chloride ions.34 These latter effects on the composition of the pancreatic juice are mediated predominantly by the endocrine mediator, secretin.35 After the meal, trypsin is free and inhibits intestinal CCK release and pancreatic enzyme secretion. This process is known as feedback inhibition and this effect of trypsin is mediated by intraluminal CCK-releasing factors (CCK-RF) present on the intestinal epithelium.36 In the presence of a meal the digestive proteases are occupied and CCK-RF promotes CCK release and more
digestive enzyme secretion. However, after digestion of a meal when there is an excess of digestive proteases in the intestinal lumen, CCK-RF is in turn digested and inactivated so that its ability to augment CCK release and stimulate further pancreatic enzyme secretion ceases (Table 2).
SUMMARYThe pancreas is a complex organ that plays a critical role in the digestion process. Understanding the cellular physiology of acinar and ductal cells lends to grasping the concepts of pancreatic exocrine secretions in various phases of digestion. Knowledge of normal pancreatic secretory functions can help clinicians order appropriate tests, which eventually assist in diagnosing specific pathologies. n
References
1. Clarke ES: History of gastroenterology. In: Paulson M, ed. Gastroenterologic Medicine, Philadelphia: Lea & Febiger; 1969.
2. Simeone DM. Mulholland MW. Pancreas: Anatomy and Structural Anomalies. In Yamada T. Atlas of Gastroenterology. 3rd ed. Hoboken. Wiley. 2003.
3. Mackie CR. Moosa AR. Surgical anatomy of the pancreas. In Moosa AR ed. Tumors of the Pancreas. Baltimore: Williams & Wilkins, 1980:1.
4. Clemente CD, ed. Gray’s Anatomy of the Human Body, 30th ed. Philadelphia: Lea & Febiger; 1985.
5. Barth BA. Burdick JS. Anatomy, Histology, Embryology, and Developmental Anomalies of the Pancreas. In Sleisenger and Fordtran’s Gastrointestinal and Liver Disease. 9th ed. Elsevier. 2010.
6. Motta PM, Macchiarelli G, Nottola SA, Correr S: Histology of the exocrine pancreas. Microsc Res Tech 1997; 37:384-398.
7. Williams JA: Intracellular signaling mechanisms activated by cholecystokinin-regulating synthesis and secretion of digestive enzymes in pancreatic acinar cells. Annu Rev Physiol 2001; 63:77-97.
8. Fallon MB, Gorelick FS, Anderson JM, et al: Effect of cerulein hyperstimulation on the paracellular barrier of rat exocrine pancreas. Gastroenterology 1995; 108:1863-1872.
9. Stauffer PL, Zhao H, Luby-Phelps K, et al: Gap junction communication modulates [Ca2+]i oscillations and enzyme secretion in pancreatic acini. J Biol Chem 1993; 268:19769-19775.
10. Steward MC, Ishiguro H, Case RM: Mechanisms of bicar-bonate secretion in the pancreatic duct. Annu Rev Physiol 2005; 67:377-409.
11. Owyang C, Williams JA. Pancreatic secretion. In: Yamada T. eds. Atlas of Gastroenterology. 3th ed. Philadelphia: Lippincott Williams and Wilkins; 2003:340-365.
(continued on page 56)

The Physiology of the Pancreas
DISEASES OF THE PANCREAS, SERIES #9
56� PRACTICAL�GASTROENTEROLOGY� •� DECEMBER�2014
12. Go V, Gardner J, DiMango E, et al ed. The exocrine pan-creas: Biology, pathobiology and disease, 2nd ed. New York: Raven; 1993:219-251.
13. Whitcomb DC, Lowe ME: Human pancreatic digestive enzymes. Dig Dis Sci 2007; 52:1-17.
14. Steward MC, Ishiguro H, Case RM: Mechanisms of bicar-bonate secretion in the pancreatic duct. Annu Rev Physiol 2005; 67:377-409.
15. Whitcomb DC, Ermentrout GB: A mathematical model of the pancreatic duct cell generating high bicarbonate concen-trations in pancreatic juice. Pancreas 2004; 29:e30-e40.
16. Tsujita T, Okuda H: Effect of bile salts on the interfacial inactivation of pancreatic carboxylester lipase. J Lipid Res 1990; 31:831-838.
17. Walter P, Gilmore K, Blobel G. Protein translocation across the endoplasmic reticulum. Cell 1984;38:5.
18. Schele G, Dobberstein B, Blobel G. Transfer of proteins across membranes: biosynthesis in vitro of pretypsinogen and typsinogen by cell fractions of canine pancreas. Eur J Biochem 1978; 82:593.
19. Jamieson JD, Palade GE. Intracellular transport of secretory proteins in the pancreatic exocrine cell. III. Dissociation of intracellular transport from protein synthesis. J Cell Bio 1968;39:580.
20. Reggio HA, Palade GE. Sulfated compounds in the zymogen granules of the guinea pig pancreas. J Cell Bio 1978; 77:288.
21. Nemoto T, Kojima T, Oshima A, et al: Stabilization of exo-cytosis by dynamic F-actin coating of zymogen granules in pancreatic acini. J Biol Chem 2004; 279:37544-37550.
22. Williams JA: Regulation of pancreatic acinar cell function. Curr Opin Gastroenterol 2006; 22:498-504.
23. Murphy JA, Criddle DN, Sherwood M, et al: Direct acti-vation of cytosolic Ca(2+) signaling and enzyme secre-tion by cholecystokinin in human pancreatic acinar cells. Gastroenterology 2008; 135:632-641.
24. Marino CR, Matovcik LM, Gorelick FS, Cohn JA: Localization of the cystic fibrosis transmembrane conduc-tance regulator in pancreas. J Clin Invest 1991; 88:712-716.
25. DiMagno EP, Hendricks JC, Go VL, Dozois RR: Relationships among canine fasting pancreatic and biliary secretions, pancreatic duct pressure, and duodenal phase III motor activity: Boldyreff revisited. Dig Dis Sci 1979; 24:689-693.
26. Zimmerman DW, Sarr MG, Smith CD, et al: Cyclic inter-digestive pancreatic exocrine secretion: Is it mediated by neural or hormonal mechanisms?. Gastroenterology 1992; 102:1378-1384.
27. Kreiss C, Schwizer W, Erlacher U, et al: Role of antrum in regulation of pancreaticobiliary secretion in humans. Am J Physiol 1996; 270:G844-G851.
28. Katschinski M, Dahmen G, Reinshagen M, et al: Cephalic stimulation of gastrointestinal secretory and motor responses in humans. Gastroenterology 1993; 103:383-391.
29. Holst JJ, Knuhtsen S, Skak-Nielsen T: The role of gastrin-releasing peptide in pancreatic exocrine secretion. Ann N Y Acad Sci 1988; 547:234-241.
30. Owyang C: Physiological mechanisms of cholecystokinin action on pancreatic secretion. Am J Physiol 1996; 271:G1-G7.
31. Li Y, Hao Y, Owyang C: High-affinity CCK-A receptors on the vagus nerve mediate CCK-stimulated pancreatic secre-tion in rats. Am J Physiol 1997; 273:G679-G685.
32. Liddle RA, Goldfine ID, Rosen MS, et al: Cholecystokinin bioactivity in human plasma: Molecular forms, responses to feeding, and relationship to gallbladder contraction. J Clin Invest 1985; 75:1144-1152.
33. Chey WY, Konturek SJ: Plasma secretion and pancreatic secretion in response to liver extract meal with varied pH and exogenous secretin in the dog. J Physiol 1982; 324:263-272.
34. Meyer JH, Way LW, Grossman MI: Pancreatic bicarbonate response to various acids in duodenum of the dog. Am J Physiol 1970; 219:964-970.
35. Chey WY, Kim MS, Lee KY, Chang TM: Effect of rabbit antisecretin serum on postprandial pancreatic secretion in dogs. Gastroenterology 1979; 77:1268-1275.
36. DiMagno M, DiMagno E: Chronic pancreatitis. Current Opin Gastroenterol 2006; 22:487-497.
37. Heiji HA, Obertop H, Schmitz PIM, et al: Evaluation of the secretin-cholecystokinin test for chronic pancreatitis by dis-criminant analysis. Scand J Gastroenterol 1986; 21:35-40.
38. Conwell DL, Zuccaro G, Morrow JB, et al: Analysis of duo-denal drainage fluid after cholecystokinin (CCK) stimulation in healthy volunteers. Pancreas 2002; 25:350-354.
39. Lundh G: Pancreatic exocrine function in neoplastic and inflammatory disease: A simple and reliable new test. Gastroenterology 1962; 42:275-280.
40. Lankisch PG: Function tests in the diagnosis of chronic pan-creatitis: Critical evaluation. Int J Pancreatol 1993; 14:9-20.
41. Hardt PD, Marzeion AM, Schnell-Kretschmer H, et al: Fecal elastase 1 measurement compared with endoscopic retro-grade cholangiopancreatography for the diagnosis of chronic pancreatitis. Pancreas 2002; 25:e6-e9.
42. Newcomer AD, Hofmann AF, DiMagno EP, et al: Triolein breath test: A sensitive and specific test for fat malabsorp-tion. Gastroenterology 1979; 76:6-13.
(continued from page 54)
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
This is an Adobe® Illustrator® File that wassaved without PDF Content.To Place or open this �le in otherapplications, it should be re-saved fromAdobe Illustrator with the "Create PDFCompatible File" option turned on. Thisoption is in the Illustrator Native FormatOptions dialog box, which appears whensaving an Adobe Illustrator �le using theSave As command.
A Token of Our APPreciation© for Our Loyal Readers
Add the App instantly to your iPad or iPhone:http://itunes.apple.com/us/app/practical-gastroenterology/id525788285?mt=8&ign-mpt=uo%3D4
Add the App instantly to your Android:https://market.android.com/details?id=com.texterity.android.PracticalGastroApphttp://www.amazon.com/gp/product/B00820QCSE
Download PRACTICAL GASTROENTEROLOGY to�your�Mobile�Device
Available�for�Free�on�iTunes,�Google�Play�and�AmazonA Peer Review Journal
PRACTICALGASTRO