Embed Size (px)
Citation preview
Adamantinoma
Ted Scriven
Sept 15th, 2008
• Adamantinoma is a malignant bone tumour
Definition
• Rare• < 1% of primary bone tumours• Patents mostly 2nd and 3rd decade of life, but
wide range overall• Predilection for tibia - ~ 80% of cases• Usually occurs in diaphysis• Slight male predominance 1.25:1
Epidemiology
• Theory:
– Adamantinoma arises from aberrant nests of epithelial cells – this would explain why the high occurrence in the subcutaneous proximal tibia
• Theory:
– Osteofibrous dysplasia is benign precursor to adamantinoma
– ? 2 types – classic (>20yo) and differentiated (<20yo – transformed from OFD)
Etiology
• Slow growing therefore symptoms may be present for years
• Most common symptom: Pain• Occasionally palpable mass (due to
subcutaneous location)• 20% present with pathologic fracture
Clinical
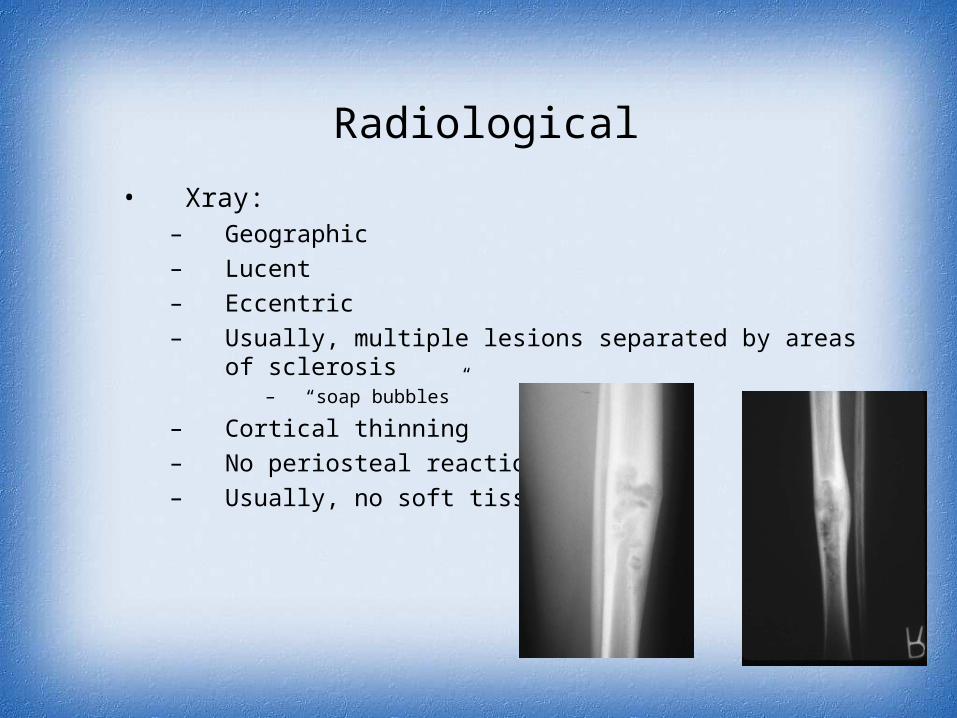
• Xray:– Geographic
– Lucent
– Eccentric
– Usually, multiple lesions separated by areas of sclerosis– “soap bubbles”
– Cortical thinning
– No periosteal reaction
– Usually, no soft tissue mass
Radiological
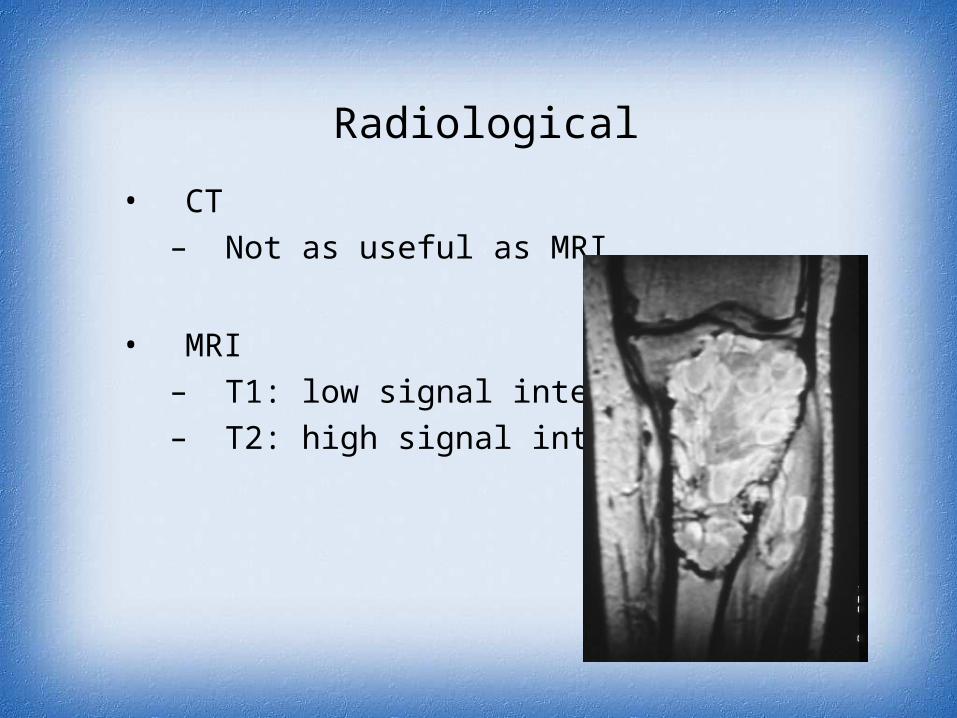
• CT
– Not as useful as MRI
• MRI
– T1: low signal intensity
– T2: high signal intensity
Radiological
• osteofibrous dysplasia• fibrous dysplasia• ABC• chondromyxoid fibroma• chondrosarcoma
DDx
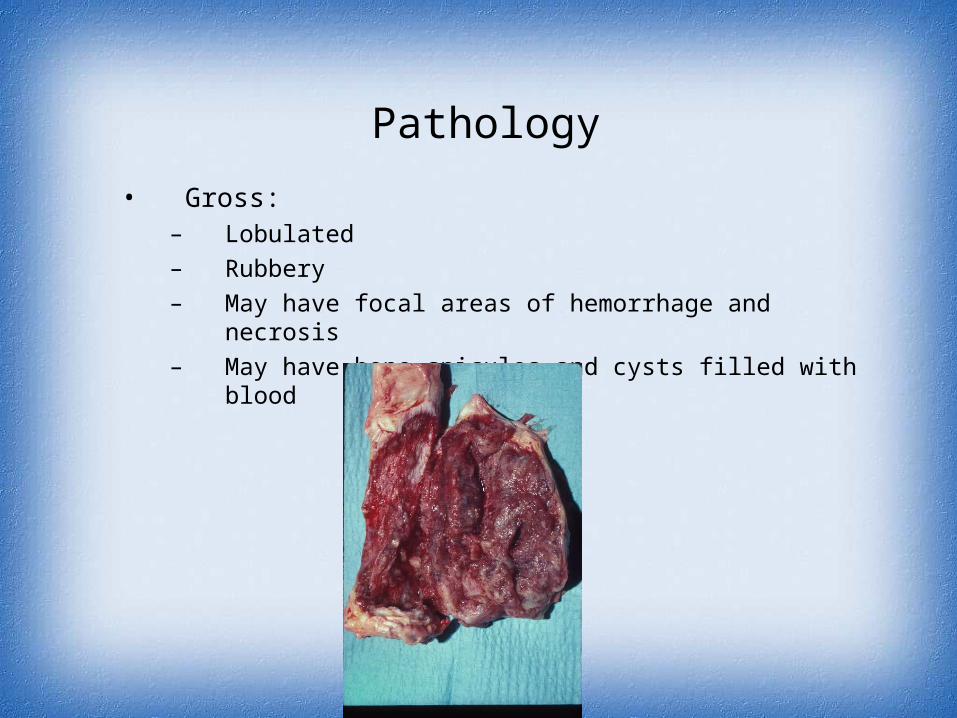
• Gross:– Lobulated
– Rubbery
– May have focal areas of hemorrhage and necrosis
– May have bone spicules and cysts filled with blood
Pathology
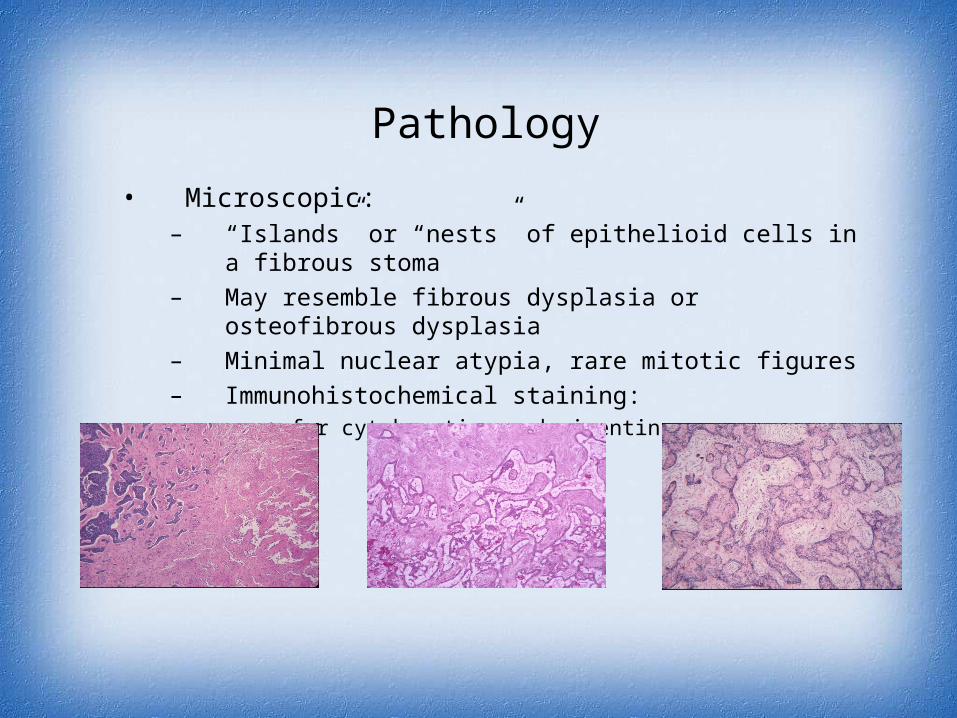
• Microscopic:– “Islands” or “nests” of epithelioid cells in a fibrous stoma
– May resemble fibrous dysplasia or osteofibrous dysplasia
– Minimal nuclear atypia, rare mitotic figures
– Immunohistochemical staining:• + for cytokeratins and vimentin
Pathology
• Wide resection or amputation• Radio-resistant• Chemo not shown to be effective
Treatment
• Prognosis depends on surgical margins
• Recurrence in 25 - 32% who do not undergo wide resection or amputation (< 10% by wide excision)
• Mets occur in up to 30%
• Mets usually in lungs or lymph nodes
• 85% survival at 10 yrs?
• Long term follow up very important as tumour is slow-growing
Prognosis
THANK YOU