Embed Size (px)
Citation preview

Adams-Oliver syndrome associated with bilateralanterior polar cataracts and optic disk drusenGerassimos Lascaratos, MRCSEd(Ophth), MSc(Oxon),a Wayne W. Lam, MD, FRCP,b
William D. Newman, FRCS(Glasg), FRCOphth,c and Mary MacRae, FRCOphtha
Adams-Oliver syndrome (AOS) (MIM 100300) was first described in1945 as a condition of terminal transverse limb defects and aplasiacutis congenita. Since then, its clinical features have been found tobe highly variable and include cardiac defects, abdominal walldefects, vascular malformations, brain abnormalities, and ocularanomalies. We report the case of a 3-year-old girl with AOS whowas also found to have bilateral anterior polar cataracts and pseu-dopapilledema secondary to optic disk drusen. To the best of ourknowledge, this is the first case of bilateral anterior polar cataractsand pseudopapilledema secondary to optic disk drusen to bereported in association with the AOS.
Case Report
A3-year-old girl was referred to the Paediatric Oph-thalmology Service at the Princess Alexandra EyePavilion in Edinburgh, United Kingdom, for rou-
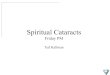
tine follow-up and continuation of care as the result ofa change in her parents’ permanent residence. Our patientwas asymptomatic and was the only child of healthy, non-consanguineous parents, with no family history of congen-ital abnormalities. Medical history was notable for 3 scalpdefects (cutis aplasia congenita) at birth (Figure 1), contrib-uting to a diagnosis of Adams-Oliver syndrome (AOS).1
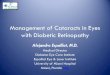
The scalp defects extended to the skull and dura. The bio-membrane that was initially used to cover the defectscaused overgranulation and had to be removed. No furthersurgery was necessary, and the defect healed by secondaryintention with no grafting. A residual defect in the calvar-ium was present after healing. There was no underlyingdefect, and magnetic resonance imaging scan of the brainwas normal. In infancy, during her regular follow-up atthe Alder Hey Children’s Hospital in Liverpool, bilateralanterior polar cataracts had been noted (Figure 2). Agood view of the fundus was possible, and no interventionhad been considered necessary.On routine ophthalmology examination at our institu-
tion, the patient was found to have bilateral optic diskswelling. There were no disk hemorrhages or exudates,
Author affiliations: aPrincess Alexandra Eye Pavilion, Lothian NHS Trust, ChalmersStreet, Edinburgh, UK; bDepartment of Clinical Genetics, Western General Hospital,Edinburgh, UK; and cDepartment of Paediatric Ophthalmology, AlderHey Children’s NHSFoundation Trust, Eaton Road, Liverpool, UKSubmitted October 13, 2010.Revision accepted February 23, 2011.Published online June 6, 2011.Reprint requests:GerassimosLascaratos,MRCSEd(Ophth),MSc(Oxon),PrincessAlexandra
Eye Pavilion, Chalmers Street, Edinburgh, EH3 9HA (email: [email protected]).J AAPOS 2011;15:299-301.Copyright � 2011 by the American Association for Pediatric Ophthalmology and
Strabismus.1091-8531/$36.00doi:10.1016/j.jaapos.2011.02.012
Journal of AAPOS
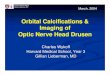
and funduscopic examination was otherwise unremarkable.The anterior polar cataracts were unchanged, and her vi-sionmeasured 6/12 in both eyes with Cardiff cards. On pal-pation of the scalp defect, no tension was felt that wouldsuggest high intracranial pressure. She was hypermetropic(16.50 in the right eye, and 15.50 in the left eye) and hadno evidence of strabismus. Ultrasonography confirmed thepresence of bilateral optic disk drusen (Figure 3). Sixmonths later, she remained asymptomatic with stable ocu-lar features and unremarkable neurological examination.
Parental examination for subtle systemic and ocularfeatures of AOS was unremarkable. Genetic studies inour patient showed a normal 135K microarray (Nimble-Gen 135K whole genome oligonucleotide array; Roche ,Nutley, NJ; HG18 genome assembly).
Discussion
AOS is a rare syndrome, typically autosomal dominant,with an estimated incidence of 0.44 per 100,000 livebirths.2
Amore severe autosomal-recessive variant of AOS has beenreported3 in association with neurological abnormalities.The systemic features of AOS have been found to be highlyvariable and include congenital heart disease, cutis
FIG 1. One of three scalp and skull defects identified at birth on thevertex area in a patient with Adams-Oliver syndrome.
299

FIG 3. B-scan ultrasound of the right eye of a 3-year-old girl withAdams-Oliver syndrome showing optic disk drusen (white arrow).
FIG 2. Bilateral anterior polar cataracts in a 3-year-old girl withAdams-Oliver syndrome.
300 Lascaratos et al Volume 15 Number 3 / June 2011
marmorata telangiectatica congenita, and brain abnormal-ities. Other associated anomalies include cardiovascularand bowel malformations, cryptorchidism, accessory nip-ples, spina bifida, and cleft lip.4 None of the above featureswas present in our case, and there was no family history ofsimilar lesions. Given that she was the only affected mem-ber of her family, we cannot state with confidence themodeof inheritance in this case.
AOS is thought to result from ischemia, necrosis, andresorption of structures after an intrauterine vascularevent affecting the brachial artery.5 The role of earlyembryonic vascular disruption, as one of the underlyingcauses of AOS, is further supported by the occurrenceof vascular malformations in this syndrome, includingcutis marmorata telangiectatica congenita and abnormalpulmonary and portal vasculature.6 Postmortem examina-tion of an AOS patient with pulmonary hypertension re-vealed abnormalities in the vascular smooth muscle cellsand pericyte coverage of the vasculature associated withvessel dilatation (pericyte absence) or stenosis (pericytehyperproliferation).2
Vascular disruption associated with AOS may cause de-velopmental abnormalities with an early arrest in the lenscell differentiation, leading to the formation of cataracts.In 1977 Sacks and colleagues7 suggested that a congeni-tally abnormal disk vasculature may allow transudationof plasma proteins that in turn serve as a nidus for the de-position of extracellular materials and supports the evolu-tion of disk drusen. Many of the angiograms of eyes withoptic disk drusen were also found to have an abnormalbranching pattern on the disk, relatively large blood ves-sels connecting the superficial and deep disk circulations,and increased disk capillarity.7 Moreover, optic disk dru-sen are known to be associated with various vascular ab-normalities in the eye, including optociliary shunts andanterior ischemic optic neuropathy. Nevertheless, it re-mains possible that the described association in our casemay be coincidental, since most of the previously de-scribed ocular findings appear to be related to the retinaor choroid.
Congenital cataracts have been previously reported ina single case of AOS8; however, these were nuclear cat-aracts and not, as in our case, anterior polar cataracts.Other reported ocular features of AOS include esotropia,microphthalmia,9 bilateral retinal detachment,9 bilateralfalciform retinal folds involving the macula,10 and un-usual choroidal architecture with possible staphyloma.Hypertelorism, epicanthal folds, and blue sclerae havealso been described in two sisters with AOS3; our patientmay have demonstrated the first 2 features (Figure 2). Inconclusion, this case is unique in that it identifies for thefirst time additional ocular features of AOS and increasesour understanding of the ocular manifestations of thisrare condition.
Literature Search
PubMedwas searched through September 2010 for the fol-lowing terms:Adams-Oliver syndrome, anterior polar cataract,and disc drusen.
Acknowledgments
We thank S. Gairns and M. Brannan for their help in the preparationof the images.
References
1. Adams FH, Oliver CP. Hereditary deformities in man due to arresteddevelopment. J Hered 1945;36:3-7.
2. Patel MS, Taylor GP, Bharya S, Al-Sanna’a N, Adatia I, Chitayat D,et al. Abnormal pericyte recruitment as a cause for pulmonary hyper-tension in Adams-Oliver syndrome. Am J Med Genet A 2004;129A:294-9.
3. McGoey RR, Lacassie Y. Adams-Oliver syndrome in siblings withcentral nervous system findings, epilepsy, and developmental delay:Refining the features of a severe autosomal recessive variant. Am JMed Genet 2008;146A:488-91.
4. Snape KM, Ruddy D, Zenker M, Wuyts W, Whiteford M,Johnson D, et al. The spectra of clinical phenotypes in aplasia cutiscongenita and terminal transverse limb defects. Am J Med Genet A2009;149A:1860-81.
Journal of AAPOS

Volume 15 Number 3 / June 2011 Lascaratos et al 301
5. Hoyme HE, Der Kaloustian VM, Hogg H, Entin MA,Guttmacher AE. Possible common pathogenetic mechanisms for Po-land sequence and Adams-Oliver syndrome: An additional clinical ob-servation. Am J Med Genet 1992;42:398-9.
6. Maniscalco M, Zedda A, Faraone S, de Laurentiis G, Verde R,Molese V, et al. Association of Adams-Oliver syndrome with pulmo-nary arterio-venous malformation in the same family: A furthersupport to the vascular hypothesis. Am J Med Genet A 2005;136:269-74.
7. Sacks JG, O’Grady RB, Choromokos E, Leestma J. The pathogenesisof optic nerve drusen. A hypothesis. ArchOphthalmol 1977;95:425-8.
Journal of AAPOS
8. Fayol L, Garcia P, Denis D, Philip N, Simeoni U. Adams-Oliver syn-drome associated with cutis marmorata telangiectatica congenita andcongenital cataract: A case report. Am J Perinatol 2006;23:197-200.
9. Orstavik KH, Stromme P, Spetalen S, Flage T, Westvik J,Vesterhus P, et al. Aplasia cutis congenita associated with limb, eye,and brain anomalies in sibs: A variant of the Adams-Oliver syndrome?Am J Med Genet 1995;59:92-5.
10. Prothero J, Nicholl R,Wilson J,Wakeling E. Aplasia cutis congenita,terminal limb defects, and falciform retinal folds: Confirmation ofa distinct syndrome of vascular disruption. Clin Dysmorphol 2007;16:39-41.





![Case Report Surgical Correction of Hallermann-Streiff Syndrome: … · 2017. 3. 23. · nose), congenital cataracts, bilateral microphthalmia, and proportionate dwarfism [3]. Ocular](https://img.pdfslide.net/doc/110x75/60fa652a8b23401a032c5859/case-report-surgical-correction-of-hallermann-streiff-syndrome-2017-3-23-nose.jpg)