Embed Size (px)
Citation preview

PAIN MEDICINEVolume 4 • Number 1 • 2003
Adaptation to Chronic Pain in Systemic Lupus Erythematosus:Applicability of the Multidimensional Pain Inventory
Carol M. Greco, PhD,*† Thomas E. Rudy, PhD,*‡§ and Susan Manzi, MD, MPH¶
Departments of *Anesthesiology, †Rehabilitation Science and Technology, ‡Psychiatry, §Biostatistics, and ¶Medicine, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania
A B S T R A C T
Objectives. 1) Investigate psychosocial adaptation to chronic pain in patients with systemic lupuserythematosus; 2) Compare pain adaptation of lupus, chronic low back pain, and temporo-mandibular disorders patients; and 3) Evaluate the validity of Multidimensional Pain Inventory-based profiles of lupus patients.
Methods. Two hundred forty females with pain related to systemic lupus erythematosus (N = 80),chronic low back pain (N = 80), or pain related to temporomandibular disorders (N = 80) com-pleted the Multidimensional Pain Inventory, a 60-item psychosocial assessment instrument. Allpatients were classified into empirically derived profiles based on Multidimensional Pain Inventoryresponses. Systemic lupus erythematosus profile groups were compared on conceptually relatedvariables external to the classification, including indices of lupus disease activity, pain, distress, andphysical function.
Results. The scores of lupus patients resembled those of temporomandibular disorder patients,while chronic low back pain patients had higher pain and activity interference. 87.5% of lupuspatients could be classified into one of three profiles: Dysfunctional (14%), interpersonally dis-tressed (27.5%), or adaptive coper (46%). The Multidimensional Pain Inventory profiles for lupuspatients demonstrated validity, based on external measures.
Conclusions. Although many systemic lupus erythematosus patients cope well with their chronicpain, a substantial proportion exhibit pain-related distress, activity interference, or interpersonaldifficulties.
Key Words. Systemic Lupus Erythematosus; Psychosocial Subgroups; Pain; Low Back Pain; Temporomandibular Disorders
© American Academy of Pain Medicine 1526-2375/03/$15.00/39 39–50
Reprint requests to: Carol M. Greco, PhD, Pain Evaluation andTreatment Institute, University of Pittsburgh, 5750 CentreAvenue, Suite 400, Pittsburgh, PA 15209. Tel: (412) 665-8055; Fax: (412) 665-8067; E-mail: [email protected].
Introduction
Systemic lupus erythematosus (SLE) is achronic, unpredictable autoimmune disease
that predominantly affects women of childbearingage. Chronic pain is one of the most frequentlyreported problems among SLE patients, with 85%reporting arthralgia [1], and 32–66% reportingheadache of various etiologies [2–4]. Myalgia,
abdominal pain, and chest pain (esophageal pain,pleuritic-type pain, pericarditis, or costochondri-tis) are also common. SLE patients who reporthigh levels of pain incur substantially more days ofdiminished productivity in comparison with SLEpatients with less pain [5]. Lupus pain is also asso-ciated with perceptions of lowered physical func-tioning [6] and coping resources [7]. Despite the prevalence of pain in this population, SLEpatients’ psychosocial adaptations to chronic painare not well understood. Recent studies suggestthe need for psychosocial interventions to improvepain, distress, coping skills, and other aspects of health status in persons with SLE [8–10].

However, identifying which patients require inter-ventions and tailoring treatment components totheir unique psychosocial needs may be necessaryto insure the success and cost-effectiveness of suchinterventions.
The Multidimensional Pain Inventory (MPI) is a 60-item self-report questionnaire designed toassess chronic pain patients’ perceptions and inter-pretations of their symptoms. Three profiles ofpsychosocial adaptation to chronic pain have beenidentified empirically through cluster analyses ofpatients’ responses on the MPI [11–13]. TheseMPI profiles, or subgroups, are largely inde-pendent of physical disease severity [12,14].Approximately 90% of individuals with diversepain conditions, including low back pain [12,13],headache [15], temporomandibular disorders(TMD) [14], and fibromyalgia [16], can be classi-fied into one of three profiles. The first profileincludes patients who report high levels of pain,affective distress, and interference with activities.This group is labeled dysfunctional (DYS) becausepain broadly affects mood and activities. A secondgroup of pain patients is characterized by rela-tionship difficulties and a low sense of support andis labeled interpersonally distressed (ID). Lowerlevels of disability, distress, and perceived paincharacterize the third profile. This profile groupis labeled adaptive copers (AC).
The external validity of the MPI classificationis supported by studies [12,14,16] in which theprofile groups responded differently on depressioninventories [17,18], marital adjustment [19], andperceptions of control over health [20]. The MPIsubgroups have shown differential outcomes fol-lowing treatment programs [21–23]. For example,pain severity was reduced during multidisciplinarypain treatment in fibromyalgia patients classifiedas DYS or AC but not in those classified as ID [23],and depression improved in TMD patients in theDYS subgroup, but not in the ID or AC subgroupsfollowing dental and psychological treatments[21]. Thus, the information gained from the MPI-based classification system can be useful clinically for adapting treatment to the patient’srequirements.
Historically, the MPI has been used in popula-tions whose pain etiology is poorly understood or difficult to discern, such as headache, TMD,and low back pain. The MPI classification systemhas recently been applied to groups with knownorganic pathology, such as malignant pain, includ-ing metastatic and nonmetastatic cancer, in orderto identify individuals with problematic pain adap-
tation [24,25]. To date, the MPI classification hasnot been applied to individuals with pain relatedto SLE. In the past, psychosocial aspects of livingwith life-threatening diseases such as cancer andSLE have been relatively neglected. However, the psychological and behavioral impacts of SLEdisease are receiving increased attention in recentyears. For example, high psychological distress isassociated with poorer perceived physical andmental functions [9], and low self-esteem andinadequate social support have been linked tohigher disease activity and cumulative damage inSLE patients [26]. Identification of potential sub-groups of SLE patients whose relationships oractivity levels are affected by chronic pain couldlead to improved ability to successfully addresstheir unique needs.
The aims of this study were: 1) To evaluate SLEpatients’ psychosocial and behavioral adaptationsto chronic pain using the MPI; 2) To compare theproportions of SLE individuals in the three psy-chosocial profiles with the proportions in two dis-tinct chronic pain groups: Chronic low back pain(CLBP) and TMD; and 3) To evaluate the valid-ity of the MPI-based classification system for SLEby comparing the profiles on psychosocial vari-ables external to the MPI classification system.
Methods
ParticipantsA total of 240 females with pain related to SLE,TMD, or CLBP (80 per group) were included.The SLE sample consisted of patients enrolled in a treatment study at the Pain Evaluation andTreatment Institute (PETI) [27] who had beenrecruited from the Pittsburgh Lupus Registry andlupus support groups in the Western Pennsylvaniaand Eastern Ohio area. Of SLE patientsapproached, 24.6% indicated that they did notexperience substantial pain, and therefore, werenot interested in participating. Participants com-pleted written informed consent approved by theInstitutional Review Board prior to study entry.All SLE participants met 1982 revised AmericanCollege of Rheumatology criteria for SLE [28]and were females aged 18–70 years who reportedexperiencing pain at least three times each weekfor at least 3 months. SLE patients were excludedif medications and dosages had not been stable forat least 1 month, if they required greater than 15mg prednisone daily, or if they had currentactive kidney disease associated with SLE. BecauseSLE affects women and men at a ratio of approx-
40 Greco et al.

imately 10 :1, we included only females in thisstudy of SLE pain adaptation.
One aim of this study was to compare the psy-chosocial adaptation of SLE patients with chronicpain with adaptation in other pain conditions thatrepresent a broad spectrum of disability related topain. TMD and CLBP pain groups were chosenfor comparison with SLE because they representthe extremes in a continuum of pain-related dis-ability [13]. Individuals with TMD frequentlyhave only intermittent pain, and impaired func-tion is typically limited to masticatory activities. In contrast, CLBP patients are typically more disabled by their pain. Females with TMD and CLBP were randomly selected, using theSAMPLES program [29], from available researchrecords at the PETI. The TMD and CLBPpatients had completed informed consent proce-dures and completed the MPI prior to enteringtreatment studies at the same clinic as the SLEpatients. These patients were evaluated and diagnosed by a board-certified anesthesiologist(CLBP) or prosthodontist (TMD), were over 18years of age, did not carry an additional diagnosisof SLE, and had pain duration of 3 months orlonger.
ProceduresThe CLBP and TMD patients completed the MPIas part of medical or dental evaluation entry visitsfor research treatment programs at the PETI. TheSLE patients, who were entering another researchstudy at the PETI, underwent a medical evalua-tion with a rheumatologist (Dr. Manzi) to deter-mine current disease activity and cumulativedamage. During this medical evaluation visit, theSLE patients completed the MPI and additionalinstruments designed to assess perceived pain, dis-tress, and physical functioning.
MeasuresMPIAll participants completed the MPI [11], a 60-iteminstrument containing nine primary scales: Painseverity, interference with activities due to pain,sense of control over life, affective distress, per-ceived support, the frequencies of 1) punishingresponses, 2) solicitous responses, and 3) distract-ing responses from significant others to thepatients’ pain, and general activity levels. Scalescores range from 0 to 6, with 6 representing themost severe response. This instrument has beendemonstrated to have good reliability and validityin a variety of chronic pain conditions [13] and is
sensitive to change following multidisciplinarypain treatment [21,23]. Three profiles, DYS, ID,and AC, have been identified based on clusteranalysis of MPI responses and replicated acrossnumerous painful conditions [13,14,23–25].
Assessment of SLE Disease Activity and DamagePhysician-rated data on SLE activity includedthree validated and reliable measures. The Sys-temic Lupus Erythematosus Disease ActivityIndex (SLEDAI) [30] contains 24 weighteddescriptors of signs and symptoms present in thepast 10 days, and scores can range from 0 (noactivity) to 105. The Systemic Lupus ActivityMeasure–Revised (SLAM-R) [31] measuresdisease activity in 11 organ systems over the pre-vious month. Scores on the SLAM-R can rangefrom 0 to 81, and a score greater than 8 is consid-ered to represent a level of clinical activity thatindicates need for treatment [32]. In addition, thePhysician’s Global Assessment (PGA) [33] of SLEactivity was completed. The PGA is a 10-cm visualanalog scale that represents the clinician’s judg-ment of disease activity and has been used in thevalidation of other instruments.
SLE disease damage was measured by thephysician-rated Systemic Lupus InternationalCollaborating Clinics/American College ofRheumatology (SLICC/ACR) damage index [34],which reflects cumulative damage in 10 organsystems. Damage may be due to SLE disease,complications of treatment, or presence of dia-betes or cancer. Total scores range from 0 (nodamage) to 46 (maximum damage). The physi-cian’s examination and completion of SLE diseaseactivity and damage indices took place on the sameday that SLE participants completed the MPI andthe following psychosocial questionnaires.
Assessment of Pain, Distress, and PerceivedPhysical Function Limitations in SLETwo psychometrically validated self-report meas-ures of pain were included. The Arthritis ImpactMeasurement Scales–Revised (AIMS-2) pain scale[35] consists of five averaged items (range: 0–4)that assess frequency and severity of pain and stiff-ness. The McGill Pain Questionnaire–short form(MPQ-SF) total score [36] is designed to measurepain intensity using 15 verbal pain descriptors.Each descriptor is rated on severity from 0 to 3,yielding a possible range of 0 to 45 (highest intensity).
Distress was assessed by three well-validatedmeasures. The Center for Epidemiological
Pain Profiles in SLE 41

Studies–Depression (CES-D) scale [18] is a 20-item inventory that assesses presence and fre-quency of depressive symptoms over the pastweek, yielding a score range of 0 to 60. Cohen’sPerceived Stress Scale (STRESS) [37] (4-itemversion) assesses frequency of feeling out ofcontrol or overwhelmed with difficulties duringthe past week and can range from 0 (none) to 16 (high stress). The Arthritis Self-EfficacyScales–pain and other symptoms [38] consists of11 items designed to measure confidence in one’sability to manage the pain, fatigue, frustration, andother aspects of disease, reworded to reflect lupusrather than arthritis [8]. Confidence estimates for each item range from 0–100%, and items areaveraged, yielding a score range of 0–100.
Perceived physical function was assessed in twoways. The SF-36 Health Survey [39] includeseight reliable and valid subscales that assess variousaspects of perceived physical and mental health.This instrument is frequently included in quality-of-life studies of persons with lupus [40,41]. TheSF-36 Physical Function (SF36-PF) scale was usedin the present study. The SF36-PF consists of 10questions regarding perceived limitations in per-formance of various everyday activities. Scoresrange from 0–100, with higher scores indicatingbetter functioning. Additionally, participants’ per-ceptions of hours per day spent resting (HRS-REST) on the couch, bed, or a chair were used toassess physical function. This item can range from0 to 24. Although this has not been used previ-ously in lupus studies, similar measures (e.g., timespent in bed due to pain) are used in chronic painpopulations [12].
Data AnalysisThe data analyses were designed to assess theapplicability of the MPI scale scores and classifi-cation system to persons with pain related to SLE.The first objective was to determine whether therewere MPI scale score differences among individu-als with SLE, CLBP, and TMD. The MPI scalesfor SLE, TMD, and CLBP were compared usingMultivariate Analysis of Variance (MANOVA),with follow-up univariate ANOVAs to detect indi-vidual scale differences, since the MANOVA wassignificant. Tukey honestly significant difference(HSD) post hoc analyses were conducted on anyscales with significant ANOVA F values in orderto determine specific group differences.
The second objective of this study was to deter-mine whether the SLE, CLBP, and TMD samplescould be empirically classified into previously
identified subgroups of DYS, ID, and AC based onMPI responses. Multivariate generalized distancefunctions and Bayesian approaches to empiricalclassification [12] were used to classify SLE,CLBP, and TMD participants’ MPI scale scoresinto one of the three profiles (i.e., DYS, ID, orAC). This empirical approach to classificationevaluates the goodness of fit of each patient’s MPIresponses to each of the three profiles. The fre-quencies of the DYS, ID, and AC clusters or pro-files in the different pain groups were comparedusing chi-square analyses.
The third set of analyses was designed toprovide external validation of the classificationsystem by comparing MPI profile groups of SLEpatients on selected demographic, disease activity,and psychosocial variables. Statistically significantdifferences were expected on psychosocial vari-ables such as pain severity, distress, and perceivedfunction, whereas the groups were not expected todiffer from one another on demographic variablessuch as age and disease duration. The SLEpatients fitting the DYS, ID, and AC classifica-tions were compared using MANOVA, with univariate follow-up analyses and Tukey HSDpairwise post hoc comparisons for significant dif-ferences between groups. A P value of <0.05 wasused to indicate statistical significance.
Results
Participant DescriptionOnly persons who reported experiencing pain inthe past week were included in the study, andtherefore, results should not be interpreted as painprevalence rates for all individuals with SLE. Thepercentages of SLE patients reporting varioustypes of pain are provided in Table 1. The mediannumber of pain complaints was five (range: 2–9).Daily pain was reported by 85% of SLE partici-pants, and pain lasting throughout the day (12
42 Greco et al.
Table 1 Types of pain symptoms reported by SLEpatients with persistent pain (N = 80)
Pain type % of patients
Joint 96.2Muscle 72.0Headache 59.5Raynaud’s phenomenon 39.8Pleuritic-type 36.9Oral/nasal ulcers 35.7Abdominal 31.0Fibromyalgia 21.4Esophageal 20.2

hours or more) was reported by 56.5%. Cumula-tive damage due to SLE ranged from 0 to 8 withmedian of 1 on the SLICC/ACR damage index[34], and current SLE disease activity as measuredby the SLEDAI [30] ranged from 0 to 14 withmedian of 4. The length of time since SLE diag-nosis ranged from less than 1 year to over 36 years,with a median of 10.2 years. In this sample of SLEpatients, there were no statistically significant correlations between AIMS-2 pain severity andcumulative SLE damage (r = 0.197, P = 0.08), SLEdisease activity index (r = 0.175, P = 0.18), or SLEduration (r = 0.066, P = 0.56).
Demographic characteristics of the threechronic pain group samples are provided in Table2. The three groups were compared usingANOVA and chi-square analyses (computed withStatXact 4 [42] for exact probabilities under smallsample size conditions). The SLE, TMD, andCLBP patients did not differ significantly in age.Duration of pain in years differed among thegroups, with SLE mean pain duration of 10.0 yearssignificantly higher than CLBP at 6.3 years (TukeyHSD P = 0.011). Chi-square analyses indicatedsignificant ethnicity and marital status differences,with follow-up hierarchical analyses indicatingthat there were fewer African American and moreCaucasian individuals in the TMD sample than inthe SLE and CLBP samples (P = 0.001), and moreof the TMD patients were married compared withthe SLE and CLBP patients (P < 0.001). However,the proportions of SLE, CLBP, and TMD pa-tients reporting on the MPI the responses ofspouses/live-in partner versus other relatives orfriends to the patients’ expressions of pain werenot significantly different (c2 (2, N = 240) = 1.71,P = 0.424). Proportions of CLBP and SLE
patients receiving disability compensation werenot significantly different (37.5% and 36%,respectively), while no TMD patients receivedsuch compensation.
Before proceeding with comparative analysesamong patient groups, basic psychometric analy-ses were computed to determine whether the MPIperformed similarly in SLE and in other pain pop-ulations. Cronbach’s coefficient of internal consis-tency (alpha) is reported in Table 3 for each of thenine MPI scales for SLE patients. Internal consis-tency of the scales ranged from 0.69 to 0.93. Thisis comparable with the internal consistency ofMPI scales for the chronic pain norm group usedin the original MPI validation study, in whichCronbach’s alpha ranged from 0.72 to 0.90 [11].Table 3 also contains the correlations betweenscales. The correlations were similar in size anddirection to those originally reported in validationstudies of the MPI [11], thus suggesting the invari-ance of the instrument with SLE patients. Theseanalyses suggest that the MPI is psychometricallyappropriate for SLE patients, and therefore, theirMPI scale scores can be compared with those ofother pain populations.
Comparison of MPI Scale Scores in Three ChronicPain Conditions: SLE, CLBP, and TMDA MANOVA with pain condition as the inde-pendent variable and the nine MPI scale scores asdependent variables was performed to determinewhether the MPI was sensitive to differencesamong the SLE, CLBP, and TMD groups. ThisMANOVA was significant (F (18,458, N = 240) =12.26, P < 0.001). Means, standard deviations(SD), univariate F statistic significance levels, andresults of post hoc pairwise comparisons are pro-
Pain Profiles in SLE 43
Table 2 Demographic characteristics of chronic pain groups
Variable SLE (N = 80) CLBP (N = 80) TMD (N = 80) P value
Age in years mean (SD) 47.7 (9.8) 44.9 (13.4) 44.8 (7.9) 0.199Pain duration in years mean (SD) 10.0 (6.6) 6.3 (8.5) 7.9 (8.7) 0.016Ethnic group (%) 0.011
Caucasian 76.0 71.0 91.0African American 22.5 25.0 6.0Asian 1.5 1.5 0Hispanic 0 0 1.5Other 0 3.5 1.5
Marital status (%) <0.001Married 58.0 47.5 85.0Separated/divorced 21.0 26.0 11.0Single 17.5 17.5 4.0Widowed 2.5 9.0 0
Disability compensation (%) 36.0 37.5 0 <0.001

vided in Table 4. Significant differences among thethree chronic pain groups were found on all MPIscales, with the exception of Life Control. Allthree groups differed significantly on Pain Sever-ity and Interference with life activities due to pain.The CLBP patients reported significantly greaterPain Severity and pain-related Interference withlife activities than the other two groups. The meanInterference score of SLE patients was signifi-cantly higher than that of TMD patients, eventhough their ratings of overall Pain Severity weresignificantly lower. The observed differences inInterference with activities due to pain may be dueto the localized nature of TMD pain and the multiple locations and types of SLE pain. CLBPpatients reported less Support and General Activ-ity and greater Affective Distress than SLE andTMD patients. SLE patients, on average, reportedreceiving fewer Punishing Responses (such asanger, irritability, and blame) from significantothers regarding pain than did CLBP patients.Although SLE patients reported multiple paincomplaints, this symptom in general did notappear to be more disabling for them than forpersons with a single source of pain. In contrast,
the CLBP patients reported relatively greater psychosocial and behavioral disruption due to painthan patients in other pain groups.
MPI Classification of SLE, CLBP,and TMD PatientsThe majority of participants (87.5% of SLE andTMD patients and 99% of CLBP patients) couldbe accurately classified into one of the three MPIpain profiles. Ten patients (12.5%) in each of theSLE and TMD groups and one patient in theCLBP group had MPI responses that did not showan adequate fit statistically to any of the three profiles, and they were classified as “anomalous.”Anomalous profiles can be the result of randomresponding or unusual patterns of responding. Inthe present sample, the mean Pain Severity andInterference scores of the “anomalous” partici-pants were significantly lower than those of theAC group (F (1,110, N = 240) = 17.5, P < 0.001and F (1,110, N = 240) = 15.54, P < 0.001, respec-tively). Likewise, perceived Support from othersregarding pain was lower in the anomalous grouprelative to the AC group, perhaps indicating thatsupport regarding pain was not needed.
44 Greco et al.
Table 3 Internal consistency and intercorrelations of MPI scales in 80 females with SLE
Cronbach’s Pearson MPI scale alpha correlation1
PS 0.85 PS I LC AD S PR SR DRI 0.93 0.75LC 0.83 -0.34 -0.43AD 0.79 0.31 0.43 -0.61S 0.77 0.23 0.33 -0.03 0.09PR 0.87 0.14 0.29 -0.19 0.28 -0.30SR 0.87 0.15 0.13 0.06 0.01 0.70 -0.40DR 0.69 0.29 0.31 -0.08 0.08 0.54 -0.18 0.63GA 0.87 -0.31 -0.36 0.28 -0.14 0.04 -0.15 0.11 0.15
Abbreviations: PS = Pain Severity; I = Interference; LC = Life Control; AD = Affective Distress; S = Support; PR = Punishing Responses; SR = Solicitous Responses;DR = Distracting Responses; GA = General Activity.1r ≥ 0.22, P < 0.05; r ≥ 0.28, P < 0.01.
Table 4 Multidimensional Pain Inventory scale score means (SD) by chronic pain groups
MPI scale SLE (N = 80) CLBP (N = 80) TMD (N = 80) P value1 Tukey HSD2
Pain Severity 3.03 (1.45) 4.87 (0.94) 3.54 (1.28) <0.001 CLBP > TMD > SLEInterference 3.25 (1.53) 4.86 (0.94) 2.45 (1.66) <0.001 CLBP > SLE > TMDLife Control 3.30 (1.44) 2.99 (1.58) 3.33 (1.13) 0.208 —Affective Distress 3.21 (1.38) 4.05 (1.35) 3.26 (1.32) <0.001 CLBP > SLE&TMDSupport 3.99 (1.53) 4.75 (1.38) 3.56 (1.65) <0.001 CLBP > SLE&TMDPunishing Responses 1.26 (1.43) 1.93 (1.71) 1.74 (1.52) 0.020 CLBP > SLESolicitous Responses 3.26 (1.69) 3.86 (1.61) 2.93 (1.76) 0.002 CLBP > TMDDistracting Responses 2.28 (1.43) 2.59 (1.68) 1.78 (1.47) 0.004 CLBP > TMDGeneral Activity 2.95 (1.06) 1.99 (0.82) 3.03 (0.78) <0.001 SLE&TMD > CLBP
1ANOVA degrees of freedom are 2,237.2Tukey HSD comparison: P < 0.05.

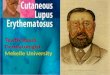
The distributions of the three MPI profiles inthe three pain groups are depicted in Figure 1.There were significant differences overall amongpain groups in the psychosocial profiles (c2 (4, N= 219) = 49.0, P < 0.001). Hierarchical follow-up chi-square analyses indicated the profile distribu-tions between SLE and TMD patients were notsignificantly different (P = 0.91), but that CLBPpatients had a significantly different distribution ofprofile proportions than SLE and TMD patients(P < 0.001). Compared with the TMD and SLEgroups, the CLBP group had a higher proportionof DYS profiles, while the TMD and SLE groupshad higher proportions of AC profiles.
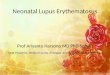
Construct Validation of the MPI in SLEThe MPI scale scores of the three SLE patientprofiles are displayed in Figure 2. In order tofurther examine the appropriateness of the MPI ina SLE sample, the three profiles were comparedon psychosocial variables conceptually related tothe MPI-based classification, including pain, dis-tress, and perceived physical function variables. Itwas expected that these related variables woulddifferentiate the profiles. In addition, the profilesof SLE patients were compared on categorical andcontinuous variables that are conceptually unre-lated to the psychosocial classification system,namely age, ethnicity, and disease and pain dura-tion, with the expectation that the profiles wouldnot differ on these variables.
Cluster Differences on Categorical Demographic VariablesA cluster by ethnicity chi-square test was signifi-cant (c2 (4, N = 70) = 14.04, P = 0.002). Post hocanalyses indicated that a significantly higher pro-portion of African Americans than Caucasianswere classed as DYS (P = 0.003), but no differenceswere found for ID and AC classifications (P =0.21). Further exploration of the role of ethnicityin the sample indicated that African Americans
Pain Profiles in SLE 45
Figure 1 MPI-based psychosocial subgroups in three chronic pain conditions.
Figure 2 MPI profiles of 70 SLE patients.

and Caucasians with SLE did not differ on currentdisease activity or severity of psychological dis-tress/self-efficacy, but in the area of pain, AfricanAmericans tended to report greater pain severityon the AIMS-2 pain scale and MPQ-SF than Cau-casians (F (1,67, N = 70) = 4.53, P = 0.014). Sig-nificant differences also were found betweencluster assignment and marital status (c2 (6, N =70) = 16.23, P = 0.013). Post hoc analyses indicatedthat married individuals were over-represented inthe AC profile, and unmarried participants wereover-represented in the DYS profile.
Profile Comparisons on Demographics and Disease HistoryThe mean scores on age, pain duration, diseasehistory variables, disease activity, pain, distress,and perceived function for each SLE pain profileare provided in Table 5. As expected, the threeprofile groups were not significantly different inage and pain duration or in disease history vari-ables, including the SLE damage index, years sincediagnosis, and length of time since symptomonset.
Comparing Profiles on Current Disease ActivityThe MANOVA on the set of three current diseaseactivity indicators (SLAM-R, SLEDAI, and PGA)among clusters was significant (F (6,130, N = 70)= 3.07, P = 0.008). Follow-up univariate analyses
indicated that this was primarily due to differencesin SLAM-R scores among clusters (Table 5).Tukey HSD post hoc pairwise comparisons indi-cated that the DYS group had higher SLAM-Rscores than the AC group. The SLAM-R reliesheavily on patient reports of pain, such as myalgia,joint pain, and headache, thus, it is not surprisingthat SLAM-R scores differentiated profiles. Thesethree pain report items were then omitted fromthe SLAM-R scores and the ANOVA wasrepeated. Nonetheless, the profiles remained sig-nificantly different from one another on theSLAM-R when pain items were omitted (F (2,67,N = 70) = 3.59, P = 0.033), which suggests that theSLAM-R differences were not simply due tohigher pain report among DYS patients.
Validation of Profiles Using External Psychosocial VariablesThe MANOVAs of pain, distress, and physicalfunction indicated significant differences amongthe three profiles, and all univariate analyses ofindividual variables were significant (Table 5). Forthe AIMS-2 pain scale, Tukey HSD post hoc pair-wise comparisons indicated significant differencesamong all three groups, with DYS having higherpain than ID, and ID reporting higher pain thanAC. The DYS patients’ SF36-PF and Self-Efficacyscores were lower than those of ID and AC
46 Greco et al.
Table 5 Comparison of means (SD) of MPI subgroups of SLE patients on demographic and disease variables andmeasures of pain, distress, and perceived physical function
DYS (N = 11) ID (N = 22) AC (N = 37) P value1
Demographics 0.505Age in years 48.55 (9.73) 49.64 (11.34) 45.73 (7.60) —Pain duration years 11.46 (7.73) 9.82 (4.49) 9.54 (7.01) —
Disease history 0.489Damage index 1.82 (2.40) 1.09 (1.44) 1.41 (1.50) —Years diagnosed 12.46 (6.46) 10.33 (5.59) 11.70 (8.29) —Symptom years 18.49 (7.24) 14.65 (8.97) 15.97 (9.62) —
SLE activity 0.008SLAM-R 11.27 (4.25)a2 8.50 (3.28)a,b 8.32 (3.37)b 0.048SLEDAI 3.09 (3.30) 2.64 (2.11) 4.41 (3.22) 0.071PGA (cm) 1.55 (0.84) 1.20 (0.49) 1.26 (0.71) 0.363
Pain 0.000AIMS-2 pain 3.19 (0.25)a 2.53 (0.66)b 2.11 (0.69)c <0.001MPQ-SF 25.39 (9.50)a 19.78 (7.94)a,b 14.96 (7.88)b <0.001
Distress 0.005CES-D 30.46 (12.64)a 22.00 (11.52)a,b 15.60 (10.43)b <0.001STRESS 9.18 (2.99)a 7.32 (3.37)a,b 5.46 (3.20)b 0.003Self-Efficacy 34.45 (8.97a 52.53 (17.85)b 59.32 (18.43)b 0.002
Physical function 0.003SF36-PF 24.09 (15.78)a 44.32 (20.43)b 53.24 (25.56)b 0.002Hours rest 7.36 (4.80)a 4.59 (3.71)a,b 3.30 (2.71)b 0.004
1Results of MANOVAs are presented for each of the six primary domains, with significance levels in bold face. Significant MANOVAs are followed by univariateANOVAs (df = 2,67).2Means with same letters (superscript a or b) for significant F tests are not significantly different from one another at the P < 0.05 level, based on Tukey HSDpost hoc tests.

patients. For all other variables, pairwise compar-isons revealed the DYS profile to be significantlyhigher in pain, distress, or perceived functionallimitation than AC, with ID between the othertwo profiles and not significantly different fromeither one.
Discussion
As medical advances improve mortality related to SLE, attention has broadened to include psy-chosocial factors associated with outcomes in thispopulation. Pain, coping skills, and psychologicaldistress have repeatedly been identified as impor-tant factors that are linked with disease activity.The current study is the first to focus specificallyon psychosocial adaptation to the chronic painthat is typically associated with SLE.
Among female SLE patients with pain, themajority can be classified into distinct groupsbased on their responses to the MPI. The sameempirically derived clusters, DYS, ID, and AC,apply to chronic pain samples of diverse etiologies,such as TMD, CLBP, fibromyalgia, and headache,as well as those whose pain is secondary to malig-nant process [13,16,25]. Like other individualswith chronic pain, persons with SLE-related painare not homogeneous, but can be categorized intodistinct groups based on psychosocial and behav-ioral responses.
In comparison with samples of CLBP andTMD patients from the same institution, SLEpatients appeared most similar to TMD patientsin terms of proportions classified as DYS, ID, andAC, with nearly half of these patients classified asAC. The similarity in profile distributions of SLEand TMD patients is surprising given that theSLE patients in the present study had averagepain duration of 10 years and a median of fivetypes of pain complaints. In contrast, TMDpatients’ pain, while chronic and potentially dis-abling, is limited to the head and neck region.Perhaps for many individuals in the SLE sample,particularly the AC group (46% of the sample),pain is not as debilitating as other aspects oflupus, such as fatigue. Future research is neededto assess the incremental psychosocial effects ofpain over and above other problems and symp-toms associated with SLE. Further investigationsinto the pain adaptation of SLE patients shouldinclude comparison groups that are also strug-gling with potentially life-threatening and dis-abling disease, such as persons with pain relatedto cancer.
The construct validity of the MPI in the SLEsample was supported. The clusters differed onpain and distress variables external to the classifi-cation and were not significantly different on conceptually unrelated variables of age, diseaseduration, and cumulative organ damage. However,there were differences among clusters on one ofthe measures of current disease activity. Partici-pants classified as DYS had higher scores on theSLAM-R, indicating that their disease was moreactive at the time of assessment. Previous validitystudies of the MPI have found profile group to beindependent of physical findings; for example,number of dental exam signs of TMD [14].However, the SLAM-R includes not only countsof clinical signs and symptoms, but also ratings ofthe current severity of each. Conceivably, the asso-ciation of profile group with SLE disease activitymay be due to good sensitivity of the measure tocurrent status. Our finding that greater diseaseactivity was associated with the DYS profile, whichis characterized by higher pain, distress, and dis-ruption in activities, is consistent with severalstudies linking psychological distress to currentSLE disease status [8–10,43].
Despite the serious and potentially life-threatening nature of SLE disease, many patientswith SLE appear to cope adaptively with their pain by maintaining activities and a positive moodand receiving adequate support from significantothers. Similarly high proportions of patientsfitting the AC profile (47.4%) have been identifiedin a study of patients with cancer-related pain [25].The high proportion of patients fitting the ACprofile in our sample may be due to the fact thatpain is only one of many problematic issues in SLEand other life-threatening conditions. Fatigue andphysical or social role changes are aspects of SLEthat may influence psychosocial adaptation inaddition to pain and are important to address infuture investigations.
Although many of the SLE patients in thisstudy appeared to cope well with chronic pain, asubstantial proportion of the classified patientsexhibited pain-related psychosocial disruption. Ofthe 87.5% who could be classified, 14% fit theDYS profile (higher perceived pain severity andaffective distress, lower activity level) and 27.5%were consistent with the ID profile, exhibitinglower support and perceiving negative reactionsfrom significant others. Other investigators reportthat SLE patients vary in levels of coping, socialsupport, and psychological distress [8,9,44]. Thissupports the idea that these patients are not a
Pain Profiles in SLE 47

homogenous group that responds to SLE and itssymptoms in exactly the same way. The currentstudy highlights the importance of comprehensiveassessments of psychosocial and behavioral adap-tations of SLE patients that include attention topain-related variability in psychological distress,relationship difficulties, and activity limitations.
Sampling issues may limit the generalizabilityof this study. The results of this study should bereplicated with larger samples that include maleswith SLE as well as persons with SLE who areattending routine rheumatology clinic visits rather than research-based medical evaluations.Although the SLE sample in the present study wasrepresentative of the geographic region and thePittsburgh Lupus Registry with regard to ethnicgroups, it included a high proportion of Cau-casians, only one Asian, and no Hispanic in-dividuals. In this study, African Americans wereover-represented in the DYS group, which wasdue to higher pain reports among African Ameri-cans. This is consistent with other reports of lowertolerance of African Americans to experimentallyinduced pain, and higher levels of pain related tomedical conditions in comparison with otherracial/ethnic groups [45]. However, future studiesof pain adaptation in SLE should include ethni-cally diverse samples in order to assess the impactof ethnicity on pain adaptation.
The range of disease damage, duration, andcurrent SLE activity in our sample was consistentwith other reports [9,26,41,46], with the majorityof patients characterized by mild to moderatedisease activity. It is possible that a sample includ-ing more individuals with severe disease activitycould result in a different distribution of MPI pro-files. The present study sample does not representall SLE cases, because some individuals with SLEdo not experience pain. Whether SLE patientswho do not have pain would report relationshipproblems and distress due to fatigue or unpre-dictable symptoms of lupus is unknown. As a firstinvestigation into the pain adaptation of SLEpatients, the current study highlights the multidi-mensional impact of pain in this population.
Conclusions
The majority of SLE patients could be classifiedinto MPI-based profiles of dysfunctional, inter-personally distressed, and adaptive coper, indicat-ing that persons with SLE are not homogeneousin terms of their psychosocial and behavioralresponses to pain. The profile groups differed
from one another on external measures of psy-chological distress, pain, and perceived physicalfunction, thus providing support for the constructvalidity of the MPI classification in a SLE popu-lation. Although all of the SLE patients in thissample reported multiple sources of pain, a sub-stantial proportion appeared to cope well withpain by maintaining activities and a positive mood.A comparison sample of CLBP patients tended toperceive their pain as more disabling than did SLEpatients and TMD patients. The MPI may beuseful for identifying individuals with SLE whoare in need of psychoeducational or behavioralpain management interventions.
Acknowledgments
Supported by the National Arthritis Foundation: RobertWood Johnson Clinical Science Grant, USPHS/NIDCRgrant R01 DE07514, NIH/NIAMD grant AR38698, andNIH/NCRR/GCRC grant 5-M01-RR-00056.
References
1 Gladman DD, Urowitz MB. Systemic lupus erythe-matosus: Clinical and laboratory features. In:Klippel J, Weyand C, Wortman R, editors. Primeron the rheumatic diseases. 11th edition. Atlanta,GA: Arthritis Foundation; 1997. p. 251–7.
2 Sfikakis PP, Mitsikostas DD, Manoussakis MN, etal. Headache in systemic lupus erythematosus: Acontrolled study. Br J Rheumatol 1998;37:300–3.
3 Glanz BI, Venkatesan A, Schur PH, et al. Prevalenceof migraine in patients with systemic lupus erythe-matosus. Headache 2001;41:285–9.
4 Omdal R, Waterloo K, Koldingsnes W, et al.Somatic and psychological features of headache insystemic lupus erythematosus. J Rheumatol 2001;28:772–9.
5 Clarke AE, Bloch DA, Danoff DS, et al. Decreas-ing costs and improving outcomes in systemic lupuserythematosus: using regression trees to develophealth policy. J Rheumatol 1994;21:2246–53.
6 Friedman AW, Alarcon GS, McGwin G Jr, et al.Systemic lupus erythematosus in three ethnicgroups. IV. Factors associated with self-reportedfunctional outcome in a large cohort study. Arthri-tis Care Res 1999;12:256–66.
7 Akkasilpa S, Minor M, Goldman D, et al. Associa-tion of coping responses with fibromyalgia tenderpoints in patients with systemic lupus erythemato-sus. J Rheumatol 2000;27:671–4.
8 Karlson EW, Daltroy LH, Lew RA, et al. The relationship of socioeconomic status, race, andmodifiable risk factors to outcomes in patients with systemic lupus erythematosus. Arthritis Rheum1997;40:47–56.
48 Greco et al.

9 Dobkin PL, Fortin PR, Joseph L, et al. Psychoso-cial contributors to mental and physical health in patients with systemic lupus erythematosus.Arthritis Care Res 1998;11:23–31.
10 Da Costa D, Dobkin PL, Pinard L, et al. The roleof stress in functional disability among women withsystemic lupus erythematosus: A prospective study.Arthritis Care Res 1999;12:112–9.
11 Kerns RD, Turk DC, Rudy TE. The West Haven-Yale Multidimensional Pain Inventory (WHYMPI).Pain 1985;23:345–56.
12 Turk DC, Rudy TE. Toward an empirically derivedtaxonomy of chronic pain patients: Integration ofpsychological assessment data. J Consult ClinPsychol 1988;56:233–8.
13 Turk DC, Rudy TE. The robustness of an empiri-cally derived taxonomy of chronic pain patients.Pain 1990;43:27–35.
14 Rudy TE, Turk DC, Zaki HS, et al. An empiricaltaxometric alternative to traditional classification oftemporomandibular disorders. Pain 1989;36:311–20.
15 Scharff L, Turk DC, Marcus DA. Psychosocial and behavioral characteristics in chronic headachepatients: Support for a continuum and dual-diagnostic approach. Cephalalgia 1995;15:216–23.
16 Turk DC, Okifuji A, Sinclair JD, et al. Pain, dis-ability, and physical functioning in subgroups ofpatients with fibromyalgia. J Rheumatol 1996;23:1255–62.
17 Beck AT, Ward CH, Mendelson M, et al. An inven-tory for measuring depression. Arch Gen Psychiat1961;4:461–71.
18 Radloff L. The CES-D scale: A self report depres-sion scale for research in the general population.Appl Psychol Meas 1977;1:385–401.
19 Locke HJ, Wallace KM. Short-term marital adjust-ment and prediction tests: Their reliability andvalidity. J Marriage Fam Liv 1959;21:251–5.
20 Wallston KA, Wallston BS, DeVellis R. Develop-ment of the Multidimensional Health Locus ofControl (MHLC) scales. Health Educ Monogr1978;6:160–70.
21 Rudy TE, Turk DC, Kubinski JA, et al. Differentialtreatment responses of TMD patients as a functionof psychological characteristics. Pain 1995;61:103–12.
22 Turk DC, Rudy TE, Kubinski JA, et al. Dysfunc-tional patients with temporomandibular disorders:Evaluating the efficacy of a tailored treatment pro-tocol. J Consult Clin Psychol 1996;64:139–46.
23 Turk DC, Okifuji A, Sinclair JD, et al. Differentialresponses by psychosocial subgroups of fibromyal-gia syndrome patients to an interdisciplinary treat-ment. Arthritis Care Res 1998;11:397–404.
24 Turk DC, Sist TC, Okifuji A, et al. Adaptation tometastatic cancer pain, regional/local cancer painand non-cancer pain: Role of psychological andbehavioral factors. Pain 1998;74:247–56.
25 Zaza C, Reyno L, Moulin DE. The Multidimen-sional Pain Inventory profiles in patients withchronic cancer-related pain: An examination of generalizability. Pain 2000;87:75–82.
26 Ward MM, Lotstein DS, Bush TM, et al. Psy-chosocial correlates of morbidity in women withsystemic lupus erythematosus. J Rheumatol 1999;26:2153–8.
27 Greco CM, Rudy TE, Manzi S. Stress reductionimproves lupus disease activity. Arthritis Rheum2001;44:382.
28 Tan EM, Cohen AS, Fries JF et al. The 1982 revisedcriteria for the classification of systemic lupus ery-thematosus. Arthritis Rheum 1982;25:1271–7.
29 Frankel MR, Spencer BD. SAMPLE: A supple-mentary module for SYSTAT. Evanston, IL:SYSTAT Inc., 1990.
30 Bombardier C, Gladman DD, Urowitz MB, et al.Derivation of the SLEDAI. A disease activity indexfor lupus patients. The Committee on PrognosisStudies in SLE. Arthritis Rheum 1992;35:630–40.
31 Liang MH, Socher SA, Larson MG, et al. Reli-ability and validity of six systems for the clinicalassessment of disease activity in systemic lupus ery-thematosus. Arthritis Rheum 1989;32:1107–18.
32 Abrahamowicz M, Fortin PR, du Berger R, et al.The relationship between disease activity and expertphysician’s decision to start major treatment inactive systemic lupus erythematosus: A decision aidfor development of entry criteria for clinical trials.J Rheumatol 1998;25:227–84.
33 Liang MH, Socher SA, Roberts WN, et al. Mea-surement of systemic lupus erythematosus activityin clinical research. Arthritis Rheum 1988;31:817–25.
34 Gladman D, Ginzler E, Goldsmith C, et al. Thedevelopment and initial validation of the SystemicLupus International Collaborating Clinics/American College of Rheumatology damage indexfor systemic lupus erythematosus. Arthritis Rheum1996;39:363–9.
35 Meenan RF, Gertman PM, Mason JH. Measuringhealth status in arthritis: The arthritis impact measurement scales. Arthritis Rheum 1980;23:146–52.
36 Melzack R. The short-form McGill pain question-naire. Pain 1987;30:191–7.
37 Cohen S, Williamson GM. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors. The social psychol-ogy of health. Newberry Park, CA: Sage Publica-tions; 1987. p. 31–67.
38 Lorig K, Chastain RL, Ung E, et al. Developmentand evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis Rheum1989;32:37–44.
39 Ware JE, Snow KK, Kosinski M. SF-36 HealthSurvey: Manual and interpretation guide. Lincoln,RI: QualityMetric Incorporated, 1993.
Pain Profiles in SLE 49

40 Strand V, Gladman D, Isenberg D, et al. Outcomemeasures to be used in clinical trials in systemiclupus erythematosus. J Rheumatol 1999;26:490–7.
41 Stoll T, Gordon C, Seifert B, et al. Consistency and validity of patient administered assessment ofquality of life by the MOS SF-36; its associationwith disease activity and damage in patients withsystemic lupus erythematosus. J Rheumatol 1997;24:1608–14.
42 Mehta C, Patel N. StatXact 4 for Windows: Statis-tical software for exact nonparametric inference.Cambridge, MA: CYTEL Software Corporation,1998.
43 Dobkin PL, Da Costa D, Dritsa M, et al. Qualityof life in systemic lupus erythematosus patientsduring more and less active disease states: Differen-tial contributors to mental and physical health.Arthritis Care Res 1999;12:401–10.
44 McCracken LM, Semenchuk EM, Goetsch VL.Cross-sectional and longitudinal analyses of copingresponses and health status in persons with systemiclupus erythematosus. Behav Med 1995;20:179–87.
45 Edwards CL, Fillingim RB, Keefe F. Race, ethnic-ity and pain. Pain 2001;94:133–7.
46 Bruce IN, Mak VC, Hallett DC, et al. Factors asso-ciated with fatigue in patients with systemic lupuserythematosus. Ann Rheum Dis 1999;58:379–81.
50 Greco et al.