Embed Size (px)
Citation preview

Additional Benefit of Montelukast in Patients Additional Benefit of Montelukast in Patients with Both Asthma and Allergic Rhinitis with Both Asthma and Allergic Rhinitis
Analysis from the COMPACT TrialAnalysis from the COMPACT Trial
Price DBPrice DB11, Swern AS, Swern AS22, Tozzi CA, Tozzi CA22, Philip G, Philip G22, Polos P, Polos P22, Yu Q, Yu Q22
Originally presented at the World Allergy Organization Congress (XVIII ICACI), Vancouver, BC, Canada - September 10, 2003
Abstract published in Allergy & Clinical Immunology International 2003, Suppl. 1:29 abstract O-15-1
1 General Practice and Primary Care, University of Aberdeen, Aberdeen, UK 2 Merck & Co., Inc., Rahway, New Jersey, USA

Clinical Observation of Montelukast as a Partner Agent
for Complementary Therapy
Price DB, Hernandez D, Magyar P et al. Thorax 2003;58:211-216

Asthma and allergic rhinitis frequently coexistAsthma and allergic rhinitis frequently coexist11
Rhinitis occurs in 75% of patients with allergic asthma and 80% of Rhinitis occurs in 75% of patients with allergic asthma and 80% of
patients with non-allergic asthmapatients with non-allergic asthma The same triggers (e.g., allergens) can cause rhinitis and asthmaThe same triggers (e.g., allergens) can cause rhinitis and asthma Actively treated rhinitis is a risk factor for asthma exacerbationsActively treated rhinitis is a risk factor for asthma exacerbations11
Upper and lower airways share a common & probably Upper and lower airways share a common & probably
interconnected inflammatory processinterconnected inflammatory process Common inflammatory cells: mast cells, eosinophils, T-cellsCommon inflammatory cells: mast cells, eosinophils, T-cells22
Common inflammatory mediators: histamine, leukotrienes, cytokinesCommon inflammatory mediators: histamine, leukotrienes, cytokines33
Bronchial challenge leads to nasal inflammation, and nasal challenge Bronchial challenge leads to nasal inflammation, and nasal challenge
leads to bronchial inflammationleads to bronchial inflammation33
1. Price D, Thomas M. ERS 20022. Bousquet J and the ARIA Workshop Group J Allergy Clin Immunol 2001;108(5):S147-S334 3. Management of Allergic Rhinitis and its Impact on Asthma (ARIA) Pocket Guide. A Pocket Guide for Physicians and Nurses. 2001
BackgroundBackground

Optimal management of rhinitis may improve Optimal management of rhinitis may improve
coexisting asthmacoexisting asthma11
Montelukast is approved to treat asthma and Montelukast is approved to treat asthma and
recently has gained approval for allergic rhinitis in recently has gained approval for allergic rhinitis in
several countriesseveral countries
Argentina, Czech Republic, Mexico, New Zealand, Argentina, Czech Republic, Mexico, New Zealand,
United States, etc.United States, etc.
1. Bousquet J and the ARIA Workshop Group J Allergy Clin Immunol 2001;108(5):S147-S334
BackgroundBackground

To determine the effect of:To determine the effect of:
Adding montelukast to inhaled budesonide 800 Adding montelukast to inhaled budesonide 800 g dailyg daily
versusversus
Doubling the dose of inhaled budesonide from 800 Doubling the dose of inhaled budesonide from 800 g g
daily to 1600 daily to 1600 g dailyg daily
COMPACT Study ObjectivesCOMPACT Study Objectives

Inclusion Criteria for COMPACTInclusion Criteria for COMPACT StudyStudy Adults (15 to 70 years) with chronic asthma for Adults (15 to 70 years) with chronic asthma for >>1 year1 year
Using inhaled corticosteroids for Using inhaled corticosteroids for >>12 weeks12 weeks
Dose Dose range: 600 to 1200 µg/day (of BDP or equivalent)range: 600 to 1200 µg/day (of BDP or equivalent)
Asthma not optimally controlled (judged by investigator)Asthma not optimally controlled (judged by investigator)
Baseline FEVBaseline FEV11 or PEF value or PEF value >>50% predicted 50% predicted
-agonist reversibility -agonist reversibility
>>12% in FEV12% in FEV11 or or >>15% in PEF at randomisation visit, or15% in PEF at randomisation visit, or
Predefined PEF variability Predefined PEF variability >>20%20%
Minimal level of daytime symptoms and Minimal level of daytime symptoms and -agonist use during -agonist use during
the 2 weeks pre-randomisationthe 2 weeks pre-randomisation

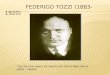
Study DesignStudy Design
Montelukast 10 mg once daily +
Budesonide 400 µg twice daily
Budesonide 800 µg twice daily
Budesonide 400 µg twice daily
Period IRun-in (4 weeks)
Single-blind
Period IIActive treatment (12 weeks)
Double-blind
0 4 16
Weeks
1
n=448
n=441
8 12

Objective of this AnalysisObjective of this Analysis
To determine if treatment with montelukast To determine if treatment with montelukast
added to budesonide (400 added to budesonide (400 g twice daily), g twice daily),
compared with budesonide (800 compared with budesonide (800 g twice g twice
daily), provides additional benefit to patients daily), provides additional benefit to patients
with co-existing asthma and allergic rhinitiswith co-existing asthma and allergic rhinitis

Statistical AnalysisStatistical Analysis All patients with a baseline and at least one on-treatment All patients with a baseline and at least one on-treatment
value were included in this intention-to-treat analysisvalue were included in this intention-to-treat analysis
Treatment comparisons were based on an analysis of Treatment comparisons were based on an analysis of
covariance (ANCOVA) model, with corresponding covariance (ANCOVA) model, with corresponding
baseline value included as a covariate and treatment baseline value included as a covariate and treatment
group as a factorgroup as a factor
All analyses of patient subgroups were post hoc All analyses of patient subgroups were post hoc

Definition of Groups in AnalysisDefinition of Groups in Analysis
Asthma+AR
Patients with asthma and allergic rhinitis, defined by both positive patient history and confirmed
physician diagnosis
Asthma–AR
Patients with asthma but without both a patient history and physician diagnosis of allergic rhinitis

Patient Demographic CharacteristicsPatient Demographic Characteristics
Asthma+AR Asthma–ARN=410 N=479
Age, years median (range) 43 (15-74) 45 (15-75)
Race, n (%) Caucasian 319 (77.8) 365 (76.2)Black 4 (1.0) 2 (0.4) Hispanic 46 (11.2) 82 (17.1) Other 41 (10.0) 30 (6.3)
Gender, n (%) Male 171 (41.7) 184 (38.4) Female 239 (58.3) 295 (61.6)

Patient HistoryPatient History
Asthma+AR N=410
Asthma–AR N=479
Age when asthma first treated, years
median (range)
23 (0.1-70) 28 (0- 71)
Duration of asthma, years
median (range)
15 (0-65) 13 (0-59)
History of exercise-induced asthma
n (%)
337 (82.6) 384 (80.2)
History of atopic dermatitis, n (%) 79 (19.3) 58 (12.1)
All year long without seasonal flares 25 (36.2) 18 (37.5)
Only during certain seasons 28 (40.6) 21 (43.8)
All year with seasonal flares 16 (23.2) 9 (18.8)
Skin tested for allergies, n (%) 305 (74.4) 275 (57.9)

Patient Baseline CharacteristicsPatient Baseline Characteristics
Asthma+AR Asthma–ARN=410 N=479
AM PEF median (range) 381 (89-870) 360 (62-875)
Eosinophils median (range) 0.24 (0-1.59) 0.23 (0-2.12)
Using Rhinitis Meds Prestudy n (%) n (%) Intranasal steroid (INS) 14 (3.4) 9 (1.9)Antihistamines (A) 41 (10.0) 15 (3.1)
Other treatments (O) 12 (2.9) 10 (2.1) INS or A or O 57 (13.9) 30 (6.3)

Change in AM PEF Change in AM PEF Total GroupTotal Group
p=0.36
0.0
10.0
20.0
30.0
40.0
50.0
4 8 12
Cha
nge
from
Bas
elin
e (L
/Min
, LS
Mea
n ±
SE
M)
Montelukast* (N=433)
Budesonide** (N=425)
Weeks
* Montelukast 10 mg once-daily along with budesonide 400 g twice-daily.** Budesonide 800 g twice-daily

Change in AM PEFChange in AM PEFTotal GroupTotal Group
AM PEF values
Montelukast*
N=433
Budesonide**
N=425
Baseline (L/min) 391.0 388.5
Absolute increase (L/min) 33.5 30.1
Percent increase (%) 8.6% 7.7%
Difference for
Montelukast–Budesonide
(L/min)
Least Squares Mean (95% CI)
4.2 (-4.7, 13.0)
P=0.357
* Montelukast 10 mg once-daily along with budesonide 400 g twice-daily.** Budesonide 800 g twice-daily

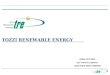
Change in AM PEFChange in AM PEFAsthma+AR Patient GroupAsthma+AR Patient Group
Post Hoc AnalysisPost Hoc Analysis
p<0.03
0.0
10.0
20.0
30.0
40.0
50.0
0 4 8 12
Ch
an
ge
s fr
om
Ba
selin
e
(L/M
in, L
S M
ea
n +
SE
M)
Montelukast* (N=216)
Budesonide** (N=184)
* Montelukast 10 mg once-daily with budesonide 400 g twice-daily.** Budesonide 800 g twice-daily
Weeks

Change in AM PEFChange in AM PEFAsthma+AR Patient GroupAsthma+AR Patient Group
AM PEF values
Montelukast*
N=216
Budesonide**
N=184
Baseline (L/min) 394.7 403.4
Absolute increase (L/min) 36.4 24.1
Percent increase (%) 9.2% 6.0%
Difference for
Montelukast–Budesonide
(L/min)
Least Squares Mean (95% CI)
14.2 (1.58, 26.84)
P=0.028
* Montelukast 10 mg once-daily along with budesonide 400 g twice-daily.** Budesonide 800 g twice-daily

-20.0
-10.0
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
4 8 12
Ch
an
ge
s fr
om
Ba
selin
e
(L/M
in, L
S M
ea
n +
SE
M)
Montelukast* (N=33)
Budesonide** (N=23)
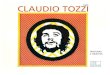
Change in AM PEFChange in AM PEFAsthma+AR Patients: Using Rhinitis MedsAsthma+AR Patients: Using Rhinitis Meds§§
Post Hoc AnalysisPost Hoc Analysis
§ Intranasal steroids or antihistamines or other treatments for rhinitis
p<0.02
Weeks
* Montelukast 10 mg once-daily along with budesonide 400 g twice-daily.** Budesonide 800 g twice-daily

Change in AM PEFChange in AM PEFAsthma+AR Patients: Using Rhinitis MedsAsthma+AR Patients: Using Rhinitis Meds§§
AM PEF values
Montelukast*
N=33
Budesonide**
N=23
Baseline (L/min) 431.1 411.9
Absolute increase (L/min) 52.1 7.8
Percent increase (%) 12.1% 1.9%
Difference for
Montelukast–Budesonide
(L/min)
Least Squares Mean (95% CI)
44.3 (8.35, 80.25)
P=0.017
§ Intranasal steroids or antihistamines or other treatments for rhinitis
* Montelukast 10 mg once-daily along with budesonide 400 g twice-daily.** Budesonide 800 g twice-daily

Montelukast* Budesonide**
N Percent N Percent
Total Patients 433 8.6% 425 7.7%
Asthma+AR Patients 216 9.2% 184 6.0%
Asthma+AR Patients Using
Rhinitis Meds §§ 33 12.1% 23 1.9%
Percent Increase in AM PEFPercent Increase in AM PEFin Different AR Subgroupsin Different AR Subgroups
Percentages calculated using LS mean for change and baseline mean
* Montelukast 10 mg once-daily along with budesonide 400 g twice-daily.** Budesonide 800 g twice-daily
§ Intranasal steroids or antihistamines or other treatments for rhinitis

ResultsResults Adding montelukast significantly improved AM PEF in Adding montelukast significantly improved AM PEF in
patients who had both asthma and allergic rhinitis patients who had both asthma and allergic rhinitis (defined by both patient history and physician diagnosis), (defined by both patient history and physician diagnosis), versus doubling the dose of inhaled budesonideversus doubling the dose of inhaled budesonide
Treatment effect was greatest in patients taking medications for Treatment effect was greatest in patients taking medications for rhinitis at randomizationrhinitis at randomization
Doubling the dose of budesonide was less effective for Doubling the dose of budesonide was less effective for asthma than adding montelukast in patients with both asthma than adding montelukast in patients with both allergic rhinitis and asthmaallergic rhinitis and asthma
Patients with both allergic rhinitis and asthma – who were Patients with both allergic rhinitis and asthma – who were alsoalso taking medications for rhinitis – showed minimal improvement in taking medications for rhinitis – showed minimal improvement in AM PEF with doubling the budesonide doseAM PEF with doubling the budesonide dose

ConclusionConclusion
In the subgroup of patients from the COMPACT study
who had both asthma and allergic rhinitis, adding
montelukast to budesonide provided greater benefit in
reducing airflow obstruction, compared with doubling the
dose of budesonide

Acknowledgment Acknowledgment The authors express gratitude to the study centers and investigators:The authors express gratitude to the study centers and investigators:
ArgentinaArgentina: Baena-Cagnani CE, Lopez AM, Nannini LJ, Neffen H, Callejas O, Rey CA, Rojas R, Taborda J: Baena-Cagnani CE, Lopez AM, Nannini LJ, Neffen H, Callejas O, Rey CA, Rojas R, Taborda J AustraliaAustralia: Bryant D, Dennis C, Holmes P: Bryant D, Dennis C, Holmes P AustriaAustria: Eckmayr J, Kummer F, Obermair H, Roger MG, Vetter N, Wanka W, Wild M, Wildner C, Zwick H: Eckmayr J, Kummer F, Obermair H, Roger MG, Vetter N, Wanka W, Wild M, Wildner C, Zwick H BelgiumBelgium: Dierickx H, Mestdagh J, Rombouts L, Schatteman E, Schoofs H: Dierickx H, Mestdagh J, Rombouts L, Schatteman E, Schoofs H BrazilBrazil: Fiterman J, Barreto SM: Fiterman J, Barreto SM CanadaCanada: Laviolette M: Laviolette M ChinaChina: Lin J, Luo W, Zhong NS, Zhou X: Lin J, Luo W, Zhong NS, Zhou X ColombiaColombia: Naranjo F: Naranjo F FinlandFinland: Rossi O, Toljamo T, Torkko M: Rossi O, Toljamo T, Torkko M GermanyGermany: Becker J, Beeh KM, Harnest U, Linnhoff A, Mikloweit P, Mitlehner W, Schmidtmann S, Schultebraucks R, Seevers C, Stutz P: Becker J, Beeh KM, Harnest U, Linnhoff A, Mikloweit P, Mitlehner W, Schmidtmann S, Schultebraucks R, Seevers C, Stutz P GreeceGreece: Christaki P, Gaga A, Galanis N, Gourgoulianis G, Cratsiou C, Konstantopoulos S, Papadakis NE, Papageoriou G, Siafakas N: Christaki P, Gaga A, Galanis N, Gourgoulianis G, Cratsiou C, Konstantopoulos S, Papadakis NE, Papageoriou G, Siafakas N HungaryHungary: Baliko Z, Berta G, Csontos Z, Herjavecz I, Kraszko P, Nekam K, Namenyi M, Magyar P, Szuks Z: Baliko Z, Berta G, Csontos Z, Herjavecz I, Kraszko P, Nekam K, Namenyi M, Magyar P, Szuks Z ItalyItaly: Centanni S, Di Maria GU, Fabbri LM, Schmid G: Centanni S, Di Maria GU, Fabbri LM, Schmid G MexicoMexico: Acuna M, Hernandez D, Perez R, Salazar R: Acuna M, Hernandez D, Perez R, Salazar R NetherlandsNetherlands: Aalbers R, Bantje T, Bax AJM, Creemers JPHM, Harreveld A, Van Kralingen K, Kuipers A, Luursema P, Van Noord J, : Aalbers R, Bantje T, Bax AJM, Creemers JPHM, Harreveld A, Van Kralingen K, Kuipers A, Luursema P, Van Noord J,
Rijssenbeek-Nouwens LHM, Sinninghe Damst HEJ, Van Weelden BM, Wever AMJRijssenbeek-Nouwens LHM, Sinninghe Damst HEJ, Van Weelden BM, Wever AMJ NorwayNorway: Bergmann A, Johansen B, Langaker KE: Bergmann A, Johansen B, Langaker KE PortugalPortugal: Almeida J, Arrobas AM, Miranda MS, Segorbe AL: Almeida J, Arrobas AM, Miranda MS, Segorbe AL RomaniaRomania: Radu JR, Stoicescu IP: Radu JR, Stoicescu IP SpainSpain: Ercoreca IA, Hernandez JC, Olaguibel-Rivera JM, Pelaez A, Prieto-Andres JL, Reques FG, Rodriguez JR, Sanz CC: Ercoreca IA, Hernandez JC, Olaguibel-Rivera JM, Pelaez A, Prieto-Andres JL, Reques FG, Rodriguez JR, Sanz CC SwedenSweden: Johansson G, Lind A, Lundback B, Spjuth A: Johansson G, Lind A, Lundback B, Spjuth A SwitzerlandSwitzerland: Graf HJ, Gumowski P, Pons M, Spertini F: Graf HJ, Gumowski P, Pons M, Spertini F TaiwanTaiwan: Chiang CD, Wang JH: Chiang CD, Wang JH UKUK: Barnes N, Corris P, O’Connor B, Dilworth P, Fahmy M, Fletcher P, James IB, Price DB: Barnes N, Corris P, O’Connor B, Dilworth P, Fahmy M, Fletcher P, James IB, Price DB VenezuelaVenezuela: Montes De Oca MDC: Montes De Oca MDC

This information is provided as a professional service by Merck & Co.,
Inc. The views expressed in this presentation reflect the experience and
opinions of the authors and not necessarily that of Merck & Co., Inc. or
any of its affiliates. For detailed prescribing information on any product
discussed in this presentation, please consult the physician circular or
instruction booklet issued by the manufacturer before initiating therapy
or procedures.
Used with author permission.