Embed Size (px)
Citation preview
Addressing ADHD Naturally
Kathi Kemper, MD, MPH
Disclaimer
I have no relevant financial relationships with the manufacturers of any commercial product(s) or provider(s) of commercial services discussed in this CME activity.
I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.
I am an AUTHOR of :HarperQuill, “ The Holistic Pediatrician”
AAP, “Mental Health Naturally”XLibris, “Addressing ADD Naturally”
Two Harbors, “Authentic Healing”
Rationale ADHD is the 2nd most common
pediatric mental health diagnosis (after anxiety) Over 1/3 families use natural products
or mind-body approaches to ADHD and fewer than half mention this to their physician. Moreover, few pediatricians are
trained to answer families’ questions about these therapies. Don’t ask, don’t tell is common. Impaired relationship, misattribution of
benefits/side effects, lack of attention to healthy lifestyle?
3
Road2Hana

Objectives
By the end of this session, participants will be able to Counsel patients on dietary modifications and
supplements to improve attentiveness Use effective behavioral strategies and provide
advice about behavior management and neurofeedback
Use and recommend evidence-based resources(See AAP Section on Integrative Medicine, SOIM; join the listserv – [email protected])
CaseYou are referred an 11 year old boy by a
family nurse practitioner for management of ADHD because he did not respond to methylphenidate.
The mother says she stopped giving the medication after two weeks, because she didn’t like the idea of “drugging him up.” Instead, she has been giving him ginseng and ginkgo.
She doesn’t know if he’s any better, but “at least it’s natural”.
Attention Deficit Hyperactivity Disorder AD(H)D: criteria
Core symptoms of: Impulsivity (or Hyperactivity) Inattention
Impairing home, school, social and self-concept (at least 2 settings)
By age 6 years Chronic condition (at least 6 months) NOT due to another condition Use standard screen, Vanderbilt
www.brightfutures.org/mentalhealth/pdf/professionals/.../adhd.pdf
Epidemiology: Prevalence: 4-11% in US Boys: Girls, 3:1 Etiology: multifactorial
Genetic – family history of ADHD, alcoholism, sociopathy, LD, mood and anxiety disorders
Medical (maternal smoking and alcohol use during pregnancy; gestational diabetes; head injury; seizures; CNS infection; OSAS), and
Environmental risks (lead, CO, Cd, TV) and protective factors (high IQ, supportive, structured family environment)
Cultural – much lower prevalence estimates in Europe and Japan than US; most restless Europeans moved to North America
many unknowns
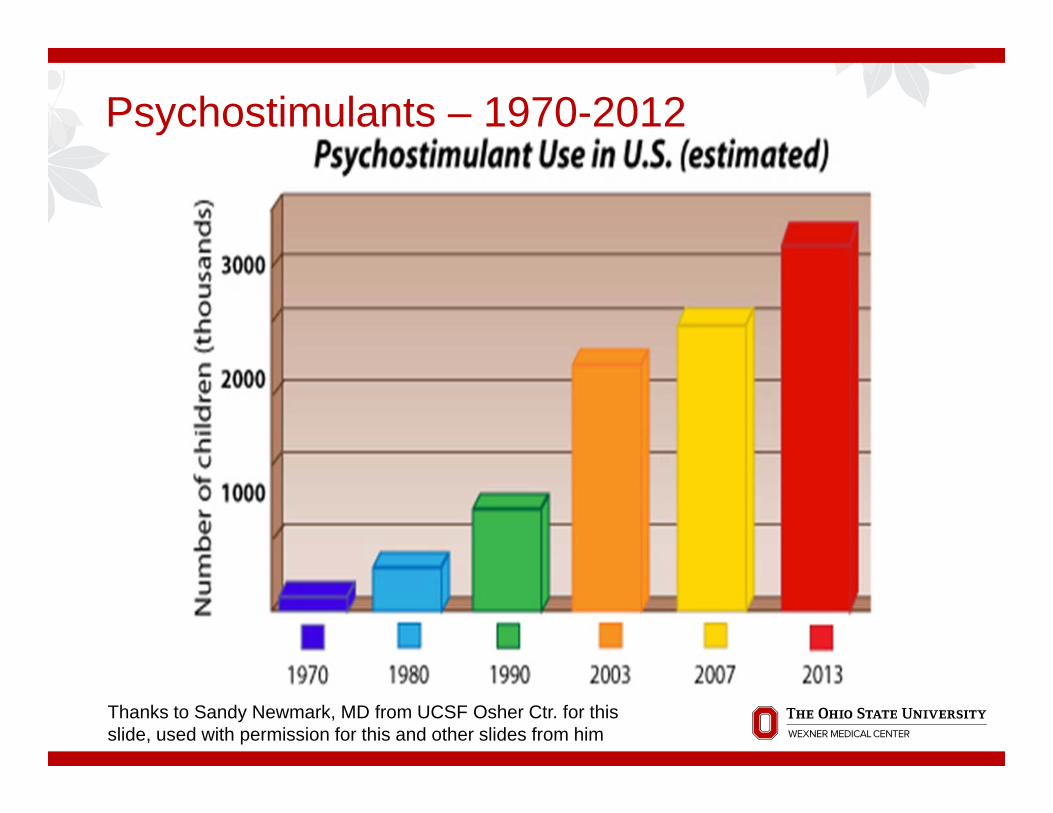
Psychostimulants – 1970-2012
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide, used with permission for this and other slides from him

Why the Explosion in the Diagnosis of ADHD?
Possible Explanations1. There are the same number of children with ADHD
but we are better at finding and helping them.2.We have loosened the definition so more people are
being diagnosed and treated.3. We are actually misdiagnosing and treating many
people who don’t have ADHD, even by a loosened definition.
4.There are now more people who actually have ADHD
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Born in the Wrong Month?
Diagnosed with ADHD -10% of Kindergarteners born in August (youngest in class) 4.5% born in September (oldest in class) Treated with Psychostimulants - 8.3% of
those born in August, as 3.5% born in September
900,000 Incorrect Diagnoses?
Journal of Health Economics 2010
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Age in Class and ADHD - Iceland
Younger Children in each class had higher likelihood ADHD diagnosisYoungest third of class 50% more likely than those in the oldest third to be prescribed stimulants between 7 and 14
Pediatrics 2012
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Delayed development?
446 kids with and without ADHD scanned repeatedly over years ADHD kids lag 3 yrs in cortical growth ADHD: motor cortex matures earlier; executive
function in frontal cortex; coordination and other cerebellar functions, delayed Functional connectivity differences in ACC, caudate Brain imaging not clinical tool No evidence of abnormality, only delay
Shaw P. National Academy of Science. 2007
Toxins in Umbilical Cord Blood
10 newborns –an average 200 industrial chemicals and pollutants 287 chemicals detected, 217 are
toxic to the brain and nervous system, 208 cause birth defects or
abnormal development in animal tests
Environmental Working Group 2005Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Neurotoxicants
Neurotoxicant chemicals: Lead, methylmercury, PCB, arsenic, toluene (2006) Mn, fluoride; chlorpyrifos and DDT (pesticides),
tetrachloroethylene (solvents), polybrominateddiphenyl esters (2014)
Grandjean and Landrigan, Lancet Neurology, 2014
Maternal use of acetaminophen! (Odds ratio 1.4); dose response found, after controlling for maternal infection, inflammation, mental health
Liew Z, et al. JAMA Pediatrics, 2014
14

Organochlorines and Child Development
Dichlorodiphenyl dichloroethylene (p,p'DDE)umbilical cord blood. High levels = worse mental and
psychomotor development. The higher the level, the worse the child's
development at 13 months old. PEDIATRICS Vol. 111 No. 5 May 2003
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Pesticides and ADHD Trichlorophenols. TCP. Children with any
detectable urinary 2,4,6-TCP had a higher risk of ADHD compared to children with undetectable levels (OR 1.77, 95% CI 1.18 to 2.66) (Xu X. Occupational Environmental Med, 2010)
Organophosphate exposure measured by DAP in urine. “In utero DAPs and, to a lesser extent, postnatal DAPs were associated adversely with attention as assessed by maternal report, psychometrician observation, and direct assessment. These associations were somewhat stronger at 5 years than at 3.5 years and were stronger in boys.” (Marks AR. Environ Health Perspect 2010)
Pesticides and ADHD
1139 children 8 to 15 years “children with higher urinary levels of organophosphatemetabolites were more likely to meet the diagnostic criteria for ADHD” For the most-commonly detected DMAP
metabolite, dimethyl thiophosphate, children with levels higher than the median of detectable concentrations had twice the odds of ADHD
Pediatrics, June 2010
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide

Pesticides, continued
Cross-sectional NHANES data from for 1139 children, 119 with ADHD by diagnostic interview. Measured urinary dimethyl alkylphosphate(DMAP) concentrations
A 10-fold increase in DMAP concentration was associated with an adjusted odds ratio of 1.55 (95% confidence interval: 1.14-2.10). For, dimethyl thiophosphate, children with levels higher than the median of detectable concentrations had twice the odds of ADHD (adjusted odds ratio: 1.93 [95% confidence interval: 1.23-3.02]), compared with children with undetectable levels.
Bouchard MF. Pediatrics, 2010
MANY MORE STUDIES EMERGING ON THIS!
Does Eating Organic Help? Children who ate organic fruits
and vegetables had 1/5th the level of organophosphate pesticide metabolites in their urine Children can “reduce exposure
levels from ‘uncertain’ to ‘negligible’ risk”
Environmental Heath Perspectives 2003
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Electronics and ADHD - 6 Hours/Day!
TV – 4 hours 29 minutes Computer – 1 hour 13 minutes Video games – 49 minutes
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
TV and Attention
TV viewing accounted for significant portion of the variation in ratings of ADHD s/s (Miller CJ, 2007)
Frequent television viewing associated with subsequent attention and school problems (Johnson JG, 2007)
Japanese cohort study: “Daily TV exposure at age 18 months was associated with hyperactivity-inattention and prosocial behavior at age 30 months” (Cheng S. J Epidemiol, 2010)

Treatment
Placebo
Placebo effects well documented in psychiatry Parents and teachers tend to
evaluate kids more positively if they think they are medicated Parents and teachers tend to attribute
positive changes to medications even when no meds are given Ethical issues
Waschbusch, DA J Dev Behav Pediatr2009
Usual vs. Integrative Approach
Treatment as Usual (TAU) Diagnose, using standard
scale Rule out anemia, vision,
hearing probs. Start stimulants Monitor sleep and growth Revise or refill as needed
Integrative Care Identify goals, strengths,
resources, lifestyle Assess of attention,
impulsivity, hyperactivity with standard scale
Identify specific target behavior (SMART plan)
Brainstorm behavioral, lifestyle, natural and medical treatment options; focus on fundamentals
Prioritize plan, anticipate difficulties
Monitor Revise, follow-up Advocate for policy changes
Assessment History (age of onset); other conditions Family History Diet: allergies, sensitivities, artificial
colors/flavors/sweeteners? Activity (sports), sleep; TV, nature Stress management; Social and Organizational
skills; Managing Misbehaviors Interview: mood, trauma, anxiety Standardized: Vanderbilt; vision, hearing, PE
(allergies, rashes, heart murmurs, neurologic) Lab studies: freeT4, ferritin, Vit D; consider lead
level ALL CURRENT TREATMENTS and others tried
Standard (TAU) challenges
• Making a diagnosis; what if they don’t meet criteria?
• Mastering medications, side effects etc.
• Managing resistance to treatment/referral
Wissow and Gadomski, 2008

Medication Challenges Poor response
Poor response in 35% (no behavioral improvement) to 1st drug; 2/3 of non-responders can respond to subsequent tries
Side effects >50%: nausea, weight loss, insomnia, tics, irritability, “not himself”; arryhthmias (rare), liver dysfunction
Increase in calls to Poison Control Centers Failure to take them; stigma; dependence Lack of attention to other aspects of lifestyle that improve overall
health and esteem Long-term, no impact!
Parents seek other options (30% - 40%) Mis-use? (increasing use in college students before
exams)Chan E. J Dev Beh Ped, 2003
Psychopharm Bull 2008; 41:37-47Setlick, J Pediatrics 2009; 124: 875-80
Jensen, J Am Acad Child Adolesc Psychiatry, 2007, 2013

An Integrative Approach to ADHD
It is important to see the whole child, with his or her unique combination of strengths and weaknesses, in the context of family, friends, school, and community, and not just a set of symptoms to fix. Sometimes a change in the home environment, school or teacher is more important than any medicine, nutritional supplement or herb.
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide

Strengths-based approach
Build on strengths: great for sales, entertainment, the arts Creativity, imagination, innovation Energy, exuberance, enthusiasm Desire to please; Sociability Flexible; notices subtle details in environment
NOT a character flaw or willfully bad Improvement in specific skills (attention,
diligence, self-discipline) is possible
Healthy Habits, Healthy Habitat
5 Fundamentals: 5Fs1. Fitness and Sleep: more exercise, more sleep
(sleep hygiene)2. Food – “Eat food. Mostly plants. Not too
much.” Consider supplements to avoid deficiencies (iron, zn, D, folate) and meet unique metabolic or drug-induced needs.
3. Friendship with self: emotional, mental, spiritual attention, frustration, and stress management
4. Fellowship with others –participate; develop social skills; taking turns
5. Fields/Environment: More nature; mindful music; Less TV and toxins
52 Adolescents had High or Low Glycemic Index breakfast, or No breakfast 30 and 120 Minutes Cognitive testing Low GI Breakfast: Better Executive function Better Working memory Better Attention
British Journal of Nutrition, 2012
Glycemic Index – eat LOW
Food, not “edible food-like substances”
Eat breakfast; keep the brain supplied with fuel
Avoid artificial colors, flavors, sweeteners , preservatives, e.g., benzoate(Stevens LJ. Clinical Pediatrics, 2011; McCann D. Lancet, 2007; Bateman B. Arch Dis Child, 2004; Boris M. Ann Allergy, 1994)
It’s not the sugar, it’s the other stuff See Center for Science in the
Public Interesthttp://www.cspinet.org/new/20080602
2.html

Dietary Controversies
12 negative RCTs of sugar Food allergies/sensitivities?
Next…. Supplements – megavitamins
bad; magnesium, zinc, iron may be helpful. Follows…
Effect of a Restricted Elimination Diet on the Behavior of Children with ADHD: (INCA Study) a Randomized Controlled Trial – Lancet, Feb 2011
• 100 children – 50 on restrictive diet – 50 controls 5 weeks
• Restricted diet (few foods) Rice, meat, vegetables, pears, water as basic diet
• After 5 weeks 64% of children had 40% improvement on ADHD rating Scales
• Assessor blinded, but parents and teachers not
INCA Study – Phase 2
Double Blind Placebo Controlled Trial of those who responded to elimination diet in Phase I Children were given challenge
foods and relapse of ADHD sx occurred in 19 of 30 children. Evaluators, patients and family
were blinded as to which foods were being challenged.
Appleton Central HS
Charter School for kids “struggling in conventional settings Removed vending machines selling candy, soda,
and chips. “Natural Ovens” began a healthful meal program
for breakfast and lunch Serving salad bars, fresh fruits, whole grain
breads and cereals, vegetables, meats, etc.
Appleton Central HS
Very Striking Improvements Better academic performance Fewer Behavior problems Less fighting Less drug use
www.totalhealthandwellness.net/news/docs/AppletonStudy.pdf
ADHD and Food Sensitivity
19 children responded favorably to a multiple food elimination diet. 16 completed a DBPC Food Challenge. Symptoms improved significantly on days given
placebo rather than foods they were sensitive to (P=0.003)
Boris M. Annals of Allergy, 1994
ADHD and Food Allergy Egger 62/76 children treated with an
Oligoantigenic diet improved. 28/62 who improved completed a DBPCFT
-foods thought to provoke symptoms were reintroduced. Symptoms worse on active foods than placebo. 48 foods were incriminated.
Artificial colors and preservatives were the most common provoking substances.
Pelsser (Impact of Nutrition on Children with ADHD – Netherlands, Belgium) RCT of elimination diet X 5 weeks, followed
by DBX-food challenge in 100 4-8 yo with ADHD
78% responded to elimination diet P<0.0001; relapse in 63% of responders with DB challenge
Egger J. Lancet. 1985Pelsser LM. Lancet, 2011

Artificial Colors, Flavors, and Preservatives
153 3 year olds & 144 8/9 year olds Given Sodium Benzoate and an artificial
color and additive mixture or placebo Artificial colours or a sodium
benzoate preservative (or both) in the diet result in increased hyperactivity in 3-year-old and 8/9-year-old children in the general population.
Lancet 2007

In Europe, Dyed Foods Get Warning Label
Products with Yellow 5, Red 40, Other Dyes “May Have an Adverse Effect on Activity and Attention in Children”July 20, 2010
Dietary Trial1. Avoid artificials2. Eat regular meals and
snacks3. Remove potentially
sensitive food(s) for 2 weeks; NOT FOREVER
4. Challenge eliminated foods one at a time
5. Keep diary6. Must be highly motivated
and nutrition educated7. Consider NUTRITION
CONSULT.
ADHD Supplements?
Correct deficits Iron Zinc Magnesium
Omega 3 fatty acids
NOTE: Most MV contain very little of these three. Diet is best source.

Iron in ADHD Iron plays a key role in dopamine metabolism; Ferritin levels inversely related to ADHD
hyperactivity scores (Calarge C. J Child Adolesc Psychopharm,
2010;Oner, 2008); 84% of ADHD pts had abnormally low ferritin levels (Konofal et al, Arch. Pediatr. Adolesc. Med. 2004)
Iron improved Connor’s ratings even if initial Hgband Hct are normal (Sever, 1997; Pediatric Neurology, 2008)
Iron treatment for ADHD reduced ADHD rating scale and CGI at 12 weeks (Konofal, 2008)
CHECK FERRITIN AND CORRECT!
Zinc in ADHD
Zinc levels predict stimulant response (Arnold, 1990)
Serum zinc levels low in ADHD (Bekaroglu, 1996)
Zinc effective as supplement to stimulant (Akhondzadeh, 2004)
Zinc effective in reducing hyperactive and impulsive behavior (Bilici, 2005)
MOST EFFECTIVE IN DEFICIENT POPULATIONS, ie. NOT most US kids; worth trying in picky eaters who are non-respondents to stimulants; MAY Help decrease necessary dose of stimulants.
Zinc in ADHD
RCT of Zinc supplements for 209 7th graders
Dose: 0, 10 or 20 mg Zinc 5x/wk for 10 Weeks
Statistical improvement in 20mg group (no improvement with lower doses)
Study presented at Experimental Biology meeting April 4, 2005 at San Diego, CA by J Penland.
RCT of zinc + amphetamine treatment. Zinc alone ineffective, but supplements reduced dose of amphnecessary to benefit kids behavior by 37%
Arnold LD. J Child Adolesc Psychopharm, 2011
CONSIDER based on dietary history (beef, pork, lamb, dark meat of poultry, nuts, whole grains, legumes, fish; get handout from Medline Plus)
Magnesium for ADHD
French study evaluated Mg and B6 30 / 52 hyperactive children had low ERC-Mg values Open label supplementation with 100 mg daily of Mg and B6 for
3-24 weeks “In all patients, symptoms of hyperexcitability (physical
aggressivity, instability, scholar attention, hypertony, spasm, myoclony) were reduced after 1 to 6 months treatment. Other family members shared similar symptoms, had low ERC-Mg values, and also responded clinically to increased Mg(2+)/vitamin B6 intakes. “
MORE STUDIES NEEDED; May help anxiety, constipationMousain-Bosc M, Am J Clin Nutr, 2004
Mousain-Bosc, Magnes Res, 2006Huss M. Lipids Health Dis, 2010 (also used PUFA)
Treating adults with MVMM
RCT study by Rucklidge and colleagues (2014 ProgNeuropsychopharm Biol Psychiatry) 80 adults with ADHD 8 weeks treatment with MVMM Baseline deficiencies only in vitamin D (27%); lab
values not associated with symptom levels Yet, 61% improved symptoms with supplements
49

50
Supplement Facts
Serving Size ½ Tablet 1 Tablet
%DV for Children2 and 3 years
%DV for Children4 years and older
Amount Per Tablet (½ Tablet) (1 Tablet)
Calories 5
Total Carbohydrate 1 g * <1%†
Sugars <1 g * *
Vitamin A 3,500 IU (29% as Beta-Carotene) 70% 70%
Vitamin C 60 mg 75% 100%
Vitamin D 400 IU 50% 100%
Vitamin E 30 IU 150% 100%
Vitamin K 10 mcg * 13%
Thiamin 1.5 mg 107% 100%
Riboflavin 1.7 mg 106% 100%
Niacin 20 mg 111% 100%
Vitamin B6 2 mg 143% 100%
Folic Acid 400 mcg 100% 100%
Vitamin B12 6 mcg 100% 100%
Biotin 45 mcg 15% 15%
Pantothenic Acid 10 mg 100% 100%
Calcium 108 mg 7% 11%
Iron 18 mg 90% 100%
Phosphorus 50 mg 3% 5%
Iodine 150 mcg 107% 100%
Magnesium 40 mg 10% 10%
Zinc 15 mg 94% 100%
Copper 2 mg 100% 100%
Manganese 1 mg * 50%
Chromium 20 mcg * 17%
Molybdenum 20 mcg * 27%
Centrum Kids®
No omega-3s
Contains dairy, corn, soy, and wheat; BHTBlue 2Red 40Yellow 6AspartameCarageenanGuar gum
Read labels!
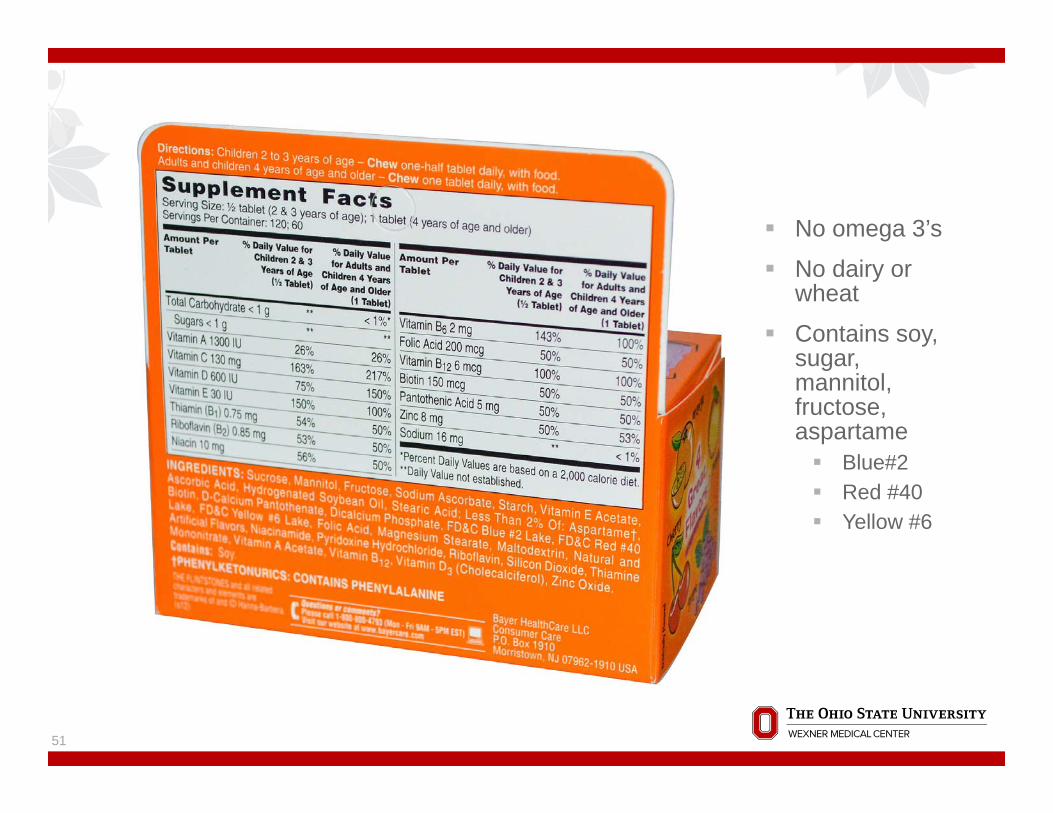
No omega 3’s
No dairy or wheat
Contains soy, sugar, mannitol, fructose, aspartame Blue#2 Red #40 Yellow #6
51
Center for Science in the Public Interest“In general, it's best to avoid the following ingredients. Aspartame, Acesulfame-K, Saccharin, Sucralose Food dyes Mycoprotein (Quorn-brand meat substitutes) Partially hydrogenated oils (trans fat)” “A recent review of all of the evidence by the
scientists who conducted the three positive animal studies urges governments to re-examine their positions on aspartame, and recommends that pregnant women and children not consume aspartame.”
https://www.cspinet.org/reports/chemcuisine.htm?gclid=Cj0KEQiAl5u2BRC6yszC1_75v5wBEiQAD-
hdzxWe0aPx4pZr6YXVeq6f4ps8YueVB_1BFEvEJsqMo2gaAjfs8P8HAQ
52
Omega-3’s, ADHD, and LD
Lower omega-3 FA levels in children with ADHD
Omega 3’s are important in brain development
RCT: 92 Swedish children with ADHD; 500 mg daily EPA Supplements “two ADHD subgroups (oppositional and less hyperactive/impulsive children) improved after 15-week EPA treatment”
Gustaffson PA. Acta Paediatr, 2010
RCT: 41 Children with ADHD and LD given a Omega-3’s vs. placebo for 12 weeks. Significant improvement in ADHD scores for active vs. placebo.
Progress in Neuro-Psychopharmacology
& Biological Psychiatry, 2002
Essential fatty acids for ADHD
41 kids, RCT to EPA 186 mg + DHA 480 mg + GLA 96 mg + cis-linoleic acid 864 vs. placebo mg daily for 12 weeks; EFA lowered Connors scores.
Richardson. 2002. Oxford-Durham RCT of fatty acids for 117
children with developmental coordination disorder: “significant improvements for active treatment vs placebo were found in reading, spelling, and behavior over 3 months of treatment in parallel groups. After the crossover, similar changes were seen in the placebo-active group.”
High dose EPA is 40% as effective as stimulants. SAFE
Richardson. Pediatrics, 2005J Am Acad Child Adolesc Psychiatry, 2011
Flax oil and vitamin C supplements improve ADHD 30 kids with ADHD, compared with 30 normal kids in
clinic in India Supplement with 200 mg ALA + 25 mg Vitamin C twice a
day, for 3 months All kids had more EFA in RBC cell membranes after 3
months ADHD kids had (P<0.01) improvements in total
hyperactivity score, self-control, psychosomatic, restlessness, inattention, impulsivity, social problems, learning problems
Joshi K. Prostaglandins Leukot Essent Fatty Acids. 2006
PUFA+Mg+Zn
German observational study of 812 children with ADHD given omega-3 + Omega-6 + Mg + Zn (ESPRICO™) X 12 weeks. Better sleep; fewer emotional problems Reduced ADHD on standard scales No serious adverse effects; 5% had mild
effects/dislike that led to stopping supplementHuss M. Lipids, Health, Dis, 2010
Vitamin D and ADHD? Three datasets including 49
states in 2003 and 2007 + 9 non US countries Inverse relationship between
solar intensity and ADHD, with solar intensity explaining 34% -57% of variance in ADHD rates, even after controlling for LBW, income, and infant mortality
Arns, M. Biol Psychiatry, 2013
57
Carnitine (Inattentive type only)
Amino acid used to ferry fatty acids into mitochondria Semi-essential amino acid Two positive European studies Two negative American studies
EXCEPT in inattentive type ADD
Arnold LE. Child Adolesc Psychiatr Clin N Am, 2013
58
Coffee, (green) tea?
Caffeine (adenosine receptor agonist) is a mild stimulant Less potent than MPH, but has
some benefits (Pires VA. Behav Brain Res, 2010; Garfinkel BD, Can Med Assoc J, 1975; Garfinkel BD, Can J Psychiatry, 1981; Schechter MD. J Clin Pharmacol, 1985)
Well-known side effects Ability to titrate with home trials
on weekend
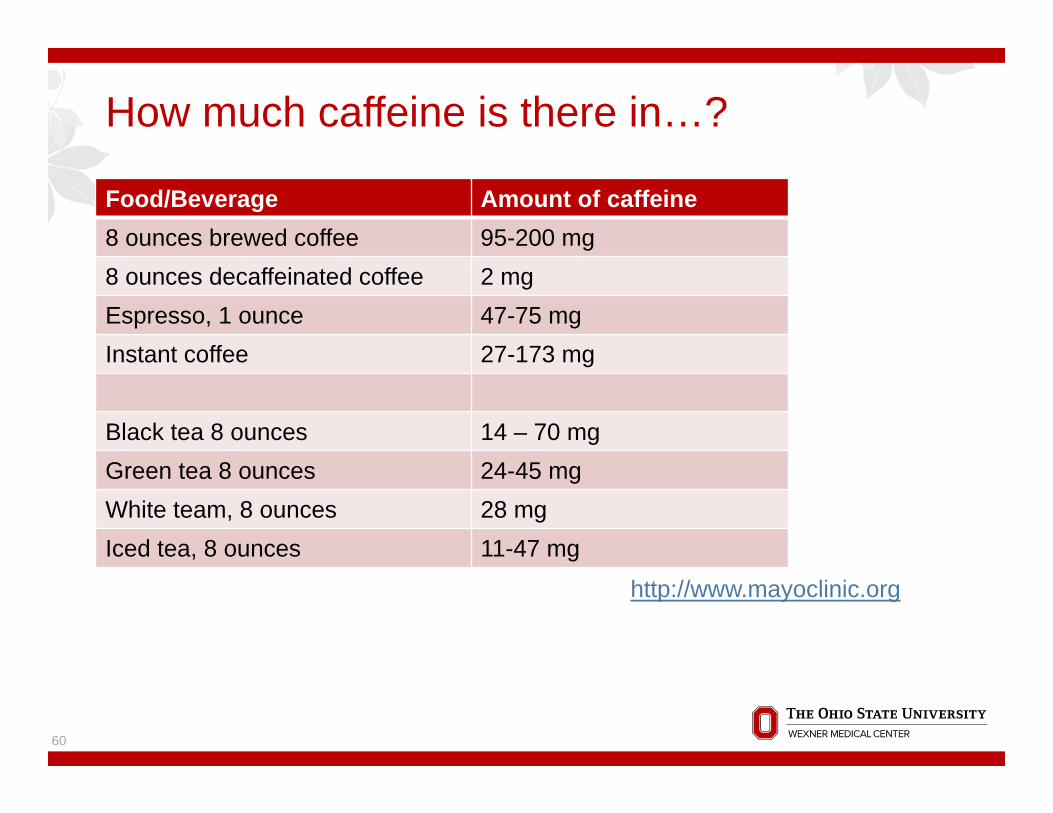
How much caffeine is there in…?
Food/Beverage Amount of caffeine8 ounces brewed coffee 95-200 mg8 ounces decaffeinated coffee 2 mgEspresso, 1 ounce 47-75 mgInstant coffee 27-173 mg
Black tea 8 ounces 14 – 70 mgGreen tea 8 ounces 24-45 mgWhite team, 8 ounces 28 mgIced tea, 8 ounces 11-47 mg
60
http://www.mayoclinic.org
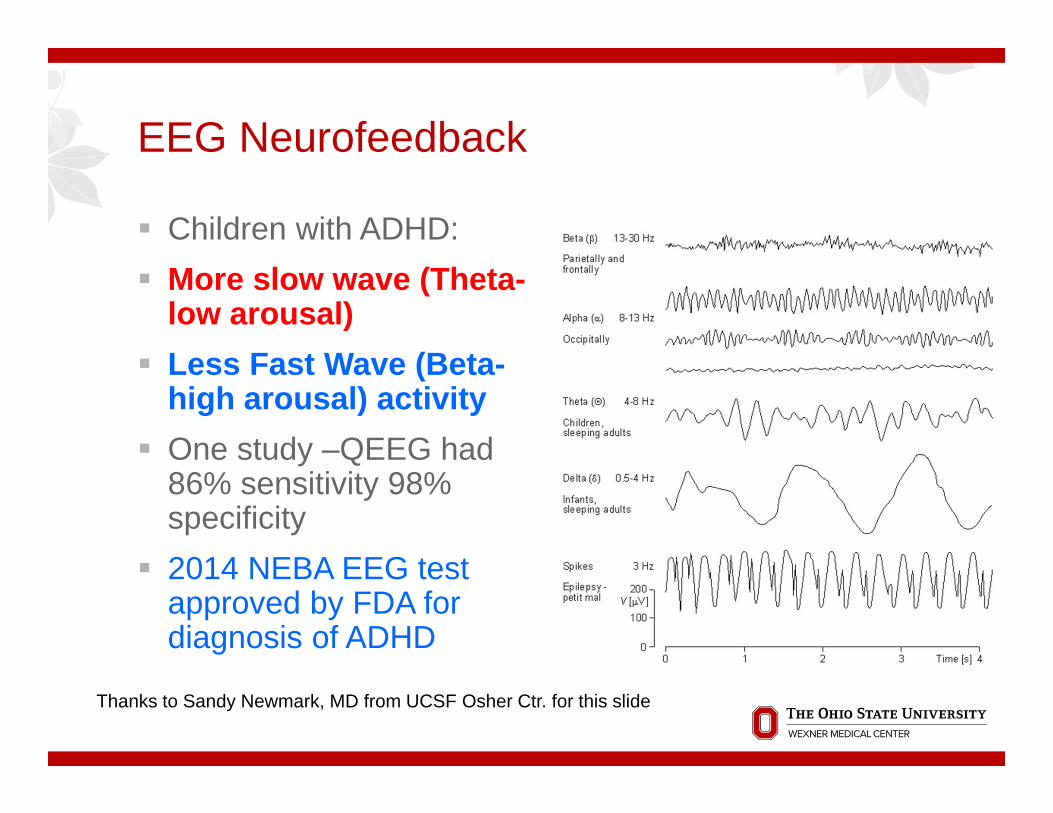
EEG Neurofeedback
Children with ADHD: More slow wave (Theta-
low arousal) Less Fast Wave (Beta-
high arousal) activity One study –QEEG had
86% sensitivity 98% specificity
2014 NEBA EEG test approved by FDA for diagnosis of ADHD
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Neurofeedback
RCT comparing school-based neurofeedback to cognitive training (CT) for 104 7-11 year olds with ADHD treated for 40 sessions Six month follow up showed faster and more
sustained significant improvements on Connor scales for neurofeedback than CT or control; also, had fewer increases in medication dosage than CT or controls Expensive, time-consuming
Steiner N, et al. Pediatrics, 2014
Steiner N, et al. J Dev Behav Pediatr, 2013
62
School Interventions
The right school and the right teacher can make all the difference
Sometimes 1st grade awful, 2nd grade fine, 3d grade terrible, etc. etc.
504 plan –reasonable classroom modifications Set of books for home Modified homework More time or quiet place for test
taking Direct communication of homework
assignments
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Tolson School-the Nurtured Heart Tolson School, Tucson. “Failing School”75% of
children from low income families. Entire school began to apply the Nurtured
Heart approach (Transforming the Difficult Child) Behavioral management system based on
highly increased positive feedback clear rules well defined consequences, given without ‘energy’
Thanks to Sandy Newmark, MD from UCSF Osher Ctr. for this slide
Suggested Practice Changes Test for ferritin in at least 50% of ADHD evaluations
Take a dietary history from at least 80% of your ADHD patients
Recommend breakfast for at least three patients in the first week home
Recommend avoiding processed food with artificials
Do a trial of coffee on the weekend
Check EWG website for Clean 15 and Dirty Dozen
Ask your staff to print out handouts on commonly used dietary supplements from Medline Plus for your patients
Encourage parents to note the positives about their child
Read Transforming the Difficult Child by Howard Glaser
Join the AAP SOCIM ([email protected] or www.aap.org/sections within the next month
Resources On-line course on Herbs and Dietary Supplementshttp://herbs-supplements.osu.edu Web
www.aap.org/sections/CHIM http://www.cspinet.org/ (Ctr Science Public Interest) http://www.nlm.nih.gov/medlineplus/druginformation.html
(Medline Plus -- good summaries of supplements) Natural Medicines (fee) ConsumerLabs.com (fee)
Books Newmark S. ADHD Without Drugs Culbert and Olness (ed). Integrative Pediatrics


Extra slides
68

Melatonin in ADHD
RCT in 25 children with ADHD and chronic sleep onset insomnia; melatonin 5 mg daily at 6pm vs. placebo Melatonin significantly improved sleep onset;
decreased sleep latency and increased total sleep time No change in ADHD behavior over 4 weeks, but all
kids kept using it for one yearSmits. J Neurology, Neurosurg, Psychiatry, 1999
American ginseng and Ginkgo for ADHD
Open trial among 36 children, 3-17 yo Panax quinquefolium (200 mg) + Ginkgo biloba
(50 mg) BID X 4 weeks Connors parents scale 2 weeks: 31% improved on anxious/shy; 67%
improved on psychosomatic 4 weeks: 74% improved on Conners’ ADHD Index
Lyon, et al. J Psychiatry Neurosci, 2001