Embed Size (px)
Citation preview

Addressing the Developmental Needs of Children in Child Welfare
Presenters:Mimi Graham, EdD
FSU CENTER FOR PREVENTION & EARLY INTERVENTION POLICY

Trajectory of DevelopmentPoverty Maltreatment Lack of Health
Services Toxic Stress
Nurturing Family
PreK & Quality Child Care
Targeted Supports Health Services Intensive
Intervention
Healthy
At-Risk
Delayedor Disordered
Read
y to
Lea
rn

3
Most Maltreated Children Have Developmental Problems
• 23 – 65%Cognitive Problems
• 14 – 64%Speech Delays
• 22 – 80%Health Problems
• 4 – 47%Motor Delays
• 10 – 61% Mental Problems

4
Nurturing & Responsive Relationships
IntensiveInterventionTargeted
Social Emotional Supports
High Quality EnvironmentsNurturing & Responsive
Relationships
Uni
vers
al
Prom
otio
n
Prev
enti
on
Trea
tmen
t
80%
15%
5%
Pyramid for Promoting Social Emotional Competence in Infants & Young Children
The Center on the Social and Emotional Foundations for Early Learning

5
Enriched Environments Can Improve Development
Early Head Start
Accredited childcare – National Assoc.for the Education of Young Children
80
85
90
95
100
105
110
115
0 1 2 3 5 8 18
Age of children in years
Sta
nd
ard
ize
d T
es
t S
co
res
TreatedControl
IntensiveIntervention
Targeted Social Emotional Supports
High Quality Environments
Nurturing & Responsive Relationships


Left Behind By Kindergarten:Children living in poverty average 15 IQ points below their peers.
Vocabulary at Age 3Poor children: 525 wordsWorking class: 749 wordsProfessional: 1,116 words
By age 4, the average child in a poor family might have been exposed to 13 million fewer words than child in a working class family and
30 million fewer words than a child in a professional family. 7

8
• Developmental screening
• Early Intervention
• Early childhood mental health consultants to childcare
• Specific counseling
• Support to siblings, biological and foster families
Targeted Supports
IntensiveIntervention
Targeted Social Emotional Supports
High Quality Environments
Nurturing & Responsive Relationships

Opportunities for Developmental Screening for Child Welfare
1. Childcare Screening2. CAPTA3. Comprehensive Health Assessment4. Comprehensive Behavioral Health
Assessment

1. Developmental screening required for All children in subsidized childcare
10

Signs of Trauma in Toddlers
• Biting, kicking, tantrums, unprovoked aggression
• Lack of verbal skills toexpress emotions
• Disengagement with others
• Indiscriminate preferencesof caregivers
• Skill regression
IntensiveIntervention
Targeted Social Emotional Supports
High Quality Environments
Nurturing & Responsive Relationships
Understand Children’s Underlying Emotional Needs in
Challenging Behaviors

12
2. Federal Mandate for Developmental Screening of Maltreated Children
CAPTA: 108-36 2003 Child Abuse Prevention & Treatment & Adoption Reform
Requires states to have procedures for the referral of children under 3 involved in substantiated cases of child abuse or neglect to early intervention services
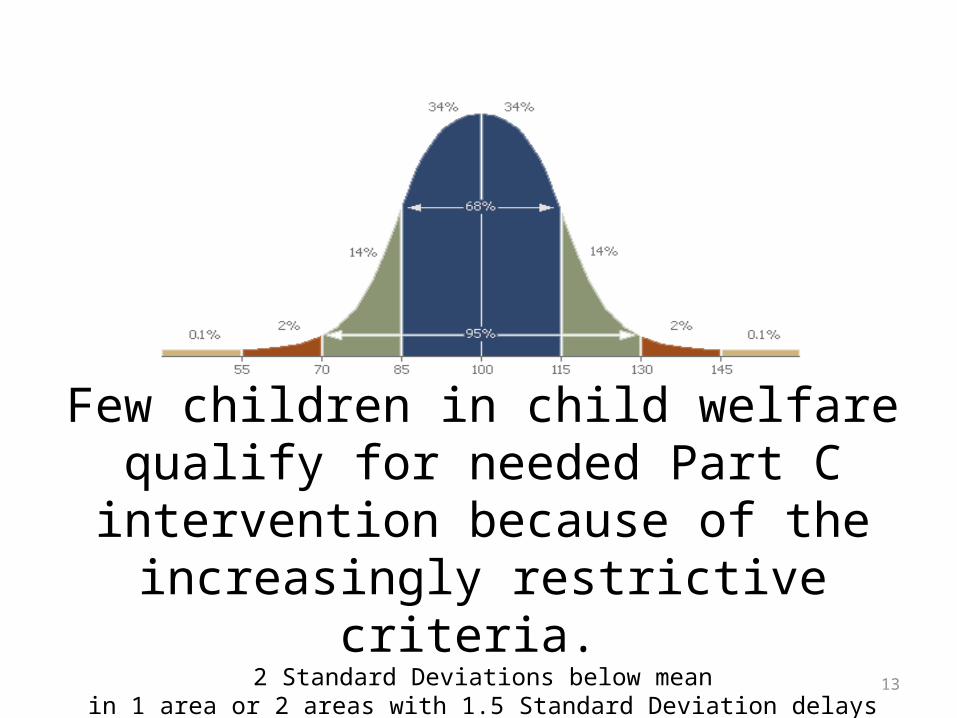
Few children in child welfare qualify for needed Part C intervention because of the
increasingly restrictive criteria. 2 Standard Deviations below mean
in 1 area or 2 areas with 1.5 Standard Deviation delays13

14
• NSCAW I: 1990-2000: 35% of children birth to 3 years need Part C early intervention services at time of contact with CWS
• Only 12% had an IFSP by age 3 indicating services
Source: NSCAW I and II
A national study found that…
Unmet Developmental Needs Of Children Investigated For Maltreatment

Mental Health Needs of Children Investigated for Maltreatment: NSCAW 1
15
• 26% of children birth to 2and 32% of children 3-5 years have emotional or behavioral problems
• Almost 80% do not receive timely intervention/treatment or primary care services
• 30% of infants in care show behavioral problems at school entry
Source: Casanueva, C., Smith, K., Dolan, M., & Ringeisen, H. (2011). NSCAW II Baseline Report: Maltreatment.OPRE Report #2011-27c, Washington, DC: Office of Planning, Research and Evaluation, Administration for Children and Families,
U.S. Department of Health and Human Services.

National Longitudinal Studyof the Developmental Needs of
Children Encountering Child Welfare with a Measured Delay
– 65% of children not receiving any services– 51% of children receiving services at home– 38% of children in foster homes – 22% of children in kinship care
16
Source: Casanueva, C., Ringeisen, H., Wilson, E., Smith, K., & Dolan, M. (2011). NSCAW II Baseline Report: Child Well-Being.OPRE Report #2011-27b, Washington, DC: Office of Planning, Research and Evaluation, Administration for Children and Families,
U.S. Department of Health and Human Services.

Estimated Children Encountering Florida Child Welfare System With Delay(s)
& Not Receiving Part C ServicesType of Child Welfare
InvolvementChildren 0-3 in
Florida Child Welfare,SFY 2009-2010
National Study Percentages of Children with Measured Delays
Estimated No. of Florida Children in Child Welfare
with Delay
Investigations with “No Findings” 19,247 65% 12,511
Children Not Served or Referred to Prevention Programs* 8,476 65% 5,509
Children Served at Home 9,015 51% 4,598
Children Served Out of Home 14,680 38% 5,578
Total # Children in all Situations 51,418 28,196
Total Estimated # Child Welfare Children Served by Part C** 2,652
Estimated # of children with delays not getting Part C 25,544Source: Radigan, Hogan & Graham, (2011). Helping the Child Welfare Population in Early Intervention:
Implications for Practice. Available at www.cpeip.fsu.edu. 17

18
3. American Academy of PediatricsRecommendations for Health Care of Young
Children in Foster Care• Initial health screening
(within 72 hours)
• Comprehensive healthassessment (within 30 days of removal) and must address the physical, behavioral, dental and developmental
• Well Child Check-ups completed with EPSDT periodicity schedule.(1, 2, 4, 6, 9, 12, 15, 18 months; then annually from age 2)American Academy of Pediatrics, Committee on Early Childhood, Adoption, and Dependent Care. (2002). Health care of young children in foster care. Pediatrics, 109(3), 536-541

19
DCF/CBC Requirements
• Initial Health Screening
(within 72 hours)
• Comprehensive Health Assessment (within 30 days of removal) and must address the physical, behavioral, dental and developmental
• Comprehensive Health Plan

4. Comprehensive Behavioral Health Assessment 0-5
Medicaid Handbook, (page 2-2-6) The assessment must include, at a minimum, the following information related to the child and the child’s family:• Reason for referral;• Personal and family history;• Placement history, including adjustment to a new care giver and home;• Sources of information (i.e., counselor, hospital, law enforcement);• Interviews and interventions;• Cognitive functioning. Screening for emotional-social development, problem solving, communication, response of the child and family to the assessment and ability to collaborate with the assessor;• Previous and current medications including psychotropics;• Last physical examination, and any known medical problems including pre-natal, pregnancy and delivery history which may affect the child’s mental health status, such as prenatal exposure, accidents, injuries, etc.;• History of mental health treatment of parents and child’s siblings. The mother’s history, including a depression screen;• History of current or past alcohol or chemical dependency of parents and child;• Legal involvement and status of child and family;• Resources including income, entitlements, health care benefits, subsidized housing, social services, etc.;• Emotional status – hands on interactive assessment of the infant regardingsensory and regulatory functioning, attention, engagement, constitutionalcharacteristics, and organization and integration of behavior;• Educational analysis – daycare issues concerning behavioral and developmental concerns;• Functional analysis – presenting strengths and problems of both child and family;

21
Unhealed Trauma
National Survey for Child and Adolescent Well-Being II (NSCAW)White, Havalchak, Jackson, O’Brien & Pecora, 2007.
63% of Foster Children Have Mental Health ProblemsAt least one diagnosis in lifetime

Observations
Need for trauma based mental health interventions.• 15 month old KH was drug exposed during pregnancy. No
recommendations in CBHA to address development nor future assessments.
• 3.5 year old DL. Foster parent has concerns re: his nightmares/ does not sleep at childcare/no assessment
• 2.5 year old EJ. Described in chart as “very hyper”
• 4 year-old has behavioral problems in childcare---bites and kicks, defecates in his pants
• 2 year old CH “cries a lot”.
• 5.5 year old CP. Foster parent reports that behavior is “problematic- doesn’t listen, doesn’t want to be told what to do.”

Untreated Adverse Early Childhood Events Only Exacerbate Over Time
Childhood• Developmental
Delays• Expulsion
Adolescence• Delinquency• Mental Health• Sexual Activity• Drugs & Alcohol• Violence
Adulthood• Psychiatric Problems• Drug Abuse• Alcohol• Crime
23Source: Adverse Childhood Experiences (ACE) Study. Available at www.cdc.gov/ace/index.htm

• Nurturing responsive emotionally available caregiver
• Enriched environment with early childhood mental health consultation to address his trauma & needs
• Medical evaluation to address failure to thrive, nutrition, physical issues.
• Developmental assessment with appropriate early intervention services
• Frequent contact with mom• IMH evaluation of parent/child
relationship and dyadic therapy to improve repair and enhance
24
What Does Children Like Billy Need to Thrive?

Florida Association for Infant Mental Health12th Annual Conference
June 12, 2013 Tampa FL
Infusing Infant Mental Health into Early Childhood Systems: • How to Screen, • How to Intervene & • How to Fund IMH Services
Early Steps Child Welfare & Baby Courts Home Visiting Childcare





























