Embed Size (px)
Citation preview

Review
Addressing the Need to Tailor Treatment to the Spectrumof Type 2 Diabetes: New Perspectives
Arturo R. Rolla, M.D.
Abstract
Type 2 diabetes mellitus is characterized by the progressive loss of beta cell function, which occurs after manyyears of insulin resistance. Within this definition, clinicians may see a diverse array of presentations, suggestingdifferent proportions of these two pathogenic factors and a complex etiology. There are also differences in the rateof type 2 diabetes progression in each patient, so treatments must be reviewed frequently to respond to changingseverity of pathophysiologies. This article first considers some of the heritable factors and the pathogenic het-erogeneity of type 2 diabetes. Relevant socioeconomic and demographic factors influencing disease developmentare reviewed after that, while emphasizing how a patient’s treatment requires changes over time.
Introduction
Type 2 diabetes mellitus (T2DM) is a progressive diseasewith changing clinical features set against a background
of hereditary and acquired factors. The molecular causes arestill poorly understood, but they result in a complex interac-tion between genetics and the environment. If human geneshave not changed that much over the centuries, the rapidincrease in prevalence of type 2 diabetes can be explained byenvironmental factors very much related to excessive nutri-tion and decreased physical activity leading to the explosionof obesity worldwide in the last hundred years. The diseaseis characterized by a progressive loss of beta cell function,that appears in certain individuals after decades of insulinresistance.1
Genetic factors
Epidemiological research (linkage and twin studies andpatterns of familial inheritance) has clearly indicated a heri-table predisposition to type 2 diabetes. More recent datasuggest a complex genetic component to the disorder.2 Newtechnologies, such as microarrays and genome-wide analysis,are suggesting three distinct genetic subgroups of diabetes:monogenic, polygenic, and mitochondrial.
Monogenic diabetes is more commonly known as maturi-ty-onset diabetes of the young (MODY), in which impairedinsulin secretion is not accompanied by pre-existent insulin
resistance. This condition is characterized by autosomaldominant inheritance and an early onset of hyperglycemia.3
MODY is currently known to be associated with mutations insix genes (named MODY1–6), and some of these variantscharacteristic of MODY may also be associated with the morecommon polygenic forms of diabetes.4 Several types ofMODY may also have other complications; MODY5, for in-stance, is associated with renal cysts.3
In contrast to monogenic diabetes, polygenic diabetes (90%of all T2DM cases) results, by definition, from several con-current genetic alterations. The additive effect of these conferssusceptibility, and diabetes may then develop if environ-mental triggers are also present. For example, gene sequenc-ing data from obese and non-obese individuals have revealedthat a combination of three polymorphisms increases the riskof obesity when coupled with a high caloric diet and seden-tary lifestyle.2 This gene–environment interaction explains therecent epidemic rise in obesity and type 2 diabetes seen inmany populations. Genes related to obesity are going to berelated also to type 2 diabetes because of the pathogenic in-teractions between these two conditions. Candidate genesinvolved in insulin synthesis and secretion are also being in-vestigated as likely sites for genetic changes associated withT2DM.3 Notably, mutations in the genes controlling insulineffect (insulin receptors, insulin cascade proteins, glucosetransporters, peroxisome proliferator-activated receptor g) areassociated with insulin resistance and are likely candidates tocontribute to these gene–gene interactions.2 Ongoing research
Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts.
DIABETES TECHNOLOGY & THERAPEUTICSVolume 11, Number 5, 2009ª Mary Ann Liebert, Inc.DOI: 10.1089=dia.2008.0075
267

into the genetic diversity of type 2 diabetes can be followed onthe Online Mendelian Inheritance in Man database.4
Mitochondrial diabetes, the rarest form of the disease, in-volves an alteration in organelle DNA that causes dysfunctionin oxidative phosphorylation. The primary resultant defectis impaired insulin secretion, and, when associated withother symptoms, manifests as maternally inherited early-onsetdiabetes.3
Ethnicity
Mass population genotyping is impractical, and so, instead,vulnerable patient groups are often identified by epidemio-logical associations between ethnicity and risk. The assump-tion behind this approach is that ethnicity acts as a proxy forgenetic difference. The DECODE–DECODA study groupstratified the prevalence of diabetes by country and found thatpopulations from Malta and India had higher frequencies ofdiabetes than those in Japan, China, and the rest of Europe.5
Even within the same country, the risk may differ betweendifferent ethnic groups. African-Americans and HispanicAmericans, for instance, show a higher frequency of diabetesthan their European-American counterparts.6
To investigate the association between ethnicity, risk, andoutcomes in diabetes, Lanting et al.7 analyzed 51 studies ofpatients with diabetes throughout the United States and theUnited Kingdom. After adjusting for confounding risk factorssuch as smoking, income, years of education, socioeconomicstatus, and body mass index (BMI), they concluded thatAfrican-Americans and Hispanics in the United States andAsians in the United Kingdom had an increased risk of dia-betic end-stage renal disease. The authors also reported thatAfrican-Americans and Hispanics in the United States had acomparatively high risk of diabetes-related retinopathycompared with Caucasians.7
To treat patients with type 2 diabetes with consideration oftheir ethnic identity must, however, be undertaken with thecaveat that ethnicity itself is a problematic term, and the exactgenetic variations of different races are still poorly understood.Ethnic categorizations can be vague or poorly informed, andthere is also a danger of overestimating differences betweenpopulation groups and underestimating the individuality of apatient’s particular disease history.8
Gender
Differences in both disease prevalence and patient out-comes have been observed between men and women.9,10
Among children without diabetes, girls may be up to 35%more insulin-resistant than boys.11 Supporting research sug-gests that this difference in insulin response is observablefrom birth, with higher concentrations of serum insulin foundin female infants.9 This could suggest an additional sex-linkedgenetic component modifying the development of T2DM.9,11
Gender-specific medical problems may also be relevant here:polycystic ovary syndrome and gestational diabetes areknown risk factors for T2DM.10
There are also gender differences in the rate of diabeticcomplications. The risk of cardiovascular disease (CVD) inT2DM is greater for women than for men: their likelihood ofdeath from CVD is increased, and prognosis following myo-cardial infarction is worse.10 Among patients with T2DM,women have a four- to sixfold increased risk of developing
coronary artery disease (CAD) compared with a two- tothreefold risk in men.10 This may be explained by the higherprevalence of risk factors for CAD in women with diabetes(compared with men with diabetes). Such risk factors in-clude hypertension, obesity, severe dyslipidemia, and oxida-tive stress.10 The same study also reported that, perhapscounterintuitively, women are frequently treated less ag-gressively for CAD.10
Characteristics and Complications of T2DM
Progression and treatment challenges
T2DM is a multifactorial disease with two main pathogeniccauses: insulin resistance and beta cell dysfunction. In-dividuals who develop insulin resistance (through either diet,genetic disposition, or a combination of these factors) do notnecessarily develop diabetes; most are able to increase insulinsecretion through beta cell compensation (hyperplasia andhypersecretion), which can usually be sustained to maintaineuglycemia for many years.12 Although incompletely under-stood, this compensation of the beta cell relies on the appro-priate responses of multiple biochemical pathways. In somepeople, failure of these processes can lead to impaired beta cellfunction, diminished insulin secretion, and hyperglycemia.12
Early intervention may have some success in preventing ordelaying the onset of T2DM in these insulin-resistant indi-viduals. Lifestyle interventions focusing on weight loss havebeen proven effective,13 as has the early use of metformin1 andinsulin sensitizers such as thiazolidinediones and biguanides,which decrease insulin resistance and facilitate beta cell rest.14
Unfortunately, many patients arrive at our clinics too late todelay or reverse the development of diabetes. The importanceof early recognition of the tendency towards T2DM cannot beoveremphasized.
In some, but not all, individuals with long-term insulinresistance a progressive dysfunction of the beta cell appears.Initially it is characterized by three abnormalities: increasedpro-insulin to insulin secretion ratio, disruption of insulinsecretory pulses, and loss of the first phase of prandial insulinsecretion.1 The initial beta cell dysfunction is progressive be-cause of a continuous loss of beta cells due to increased apo-ptosis not matched by new beta cell formation. T2DM appearsclinically when approximately 50% of beta cell mass has beenlost. The causes of the initial beta cell dysfunction are notknown, but they appear to be genetically determined in in-dividuals who are going to develop T2DM. Once hypergly-cemia ensues, glucotoxicity increases the progressive loss ofbeta cell function and mass.
In T2DM, the daily challenge is to maintain optimal gly-cemic control in the context of the progressive loss of endog-enous insulin secretion. Despite our best efforts, patients withT2DM are at increased risk of developing chronic micro- andmacrovascular complications. For example, a cohort of theUnited Kingdom Prospective Diabetes Study initially withouteye manifestations (n¼ 1,216) was followed over a period of 6years, during which 22% developed retinopathy, and its in-cidence was strongly associated with the severity of hyper-glycemia.15 In the United States and around the world, theproportion of patients with T2DM who are within the gly-cemic goals of glycohemoglobin A1c (HbA1c) is still quitelow, indicating that the rate of chronic complications amongour patients nowadays remains quite high.
268 ROLLA

Macrovascular complications occur independently of gly-cemic levels because of other potent risk factors (dyslipide-mia, hypertension, smoking, etc.). A completely euglycemicindividual may have an acute myocardial infarction or a ce-rebrovascular accident. On the other hand, patients withT2DM may live with more or less controlled glycemic levels,but the large majority are going to die of a macrovascularevent due to a clot formation in one of their arteries. The risk ofCVD, for example, reduces life expectancy for people withT2DM by up to 10 years, and evidence suggests that patientswith diabetes have a poorer prognosis after suffering amyocardial infarction.16 A follow-up study investigatingoutcomes in Japanese-Americans (n¼ 927) found that, whenage- and coronary-adjusted risk factors were taken into ac-count, cases of coronary heart disease (CHD) and CVD mor-tality were significantly more frequent patients with diabetes(Table 1).17 T2DM attracts and potentiates the risk factors ofCVD, and for that reason when the diagnosis of T2DM ismade on a patient, a ‘‘multi-control’’ therapeutic programshould be started trying to control not only blood glucoselevels but also blood pressure, lipids, and other risk factorseven more aggressively than in the population withoutdiabetes.
The importance and risks of intensive glycemic control toreduce the rate of cardiovascular complications in high-riskpatients as studied in the Action to Control CardiovascularRisk in Diabetes (ACCORD) Study, which sought HbA1ctargets close to euglycemia in the ‘‘intensive therapy group.’’18
The results were an increased mortality without significantlylowering the risk of CVD. This study emphasizes the ‘‘multi-control’’ that is necessary in patients with T2DM addressingall the CVD risk factors and the risks of intensive glycemiccontrol in an older population with known and subclinicalchronic complications. Greater benefit and lower risk of in-tensive glycemic control seem to be obtained in earlier stagesof T2DM.
Metabolic syndrome
Patients with T2DM often have other metabolic irregular-ities that predispose them to CVD (usually more frequentlyand more severely), making prevention of macrovascularcomplications of diabetes more difficult. These are, com-monly, obesity, hyperlipidemia, and hypertension.19 The term‘‘metabolic syndrome’’ was first used in 197720 to refer to thecommon association of diabetes, obesity, dyslipidemia, hy-pertension, hyperuricemia, and fatty liver to explore theircombined and additive risk factor on atherosclerosis.20
Metabolic syndrome has since been characterized furtheras a combination of cardiovascular risk factors in the contextof abdominal obesity, impaired insulin response, and=orT2DM. There is no consensus definition for metabolic syn-drome (Table 2),12–24 as its causes and the importance of eachof its components are still being debated.25 Increased waistcircumference and BMI are still being debated as definingcriteria for the metabolic syndrome in terms of their predict-ing value for cardiovascular outcomes.26 What is generallyagreed upon is that metabolic syndrome potentiates thedevelopment of diabetes-related cardiovascular complica-tions.25 Data from 6,255 individuals who had participated inthe Second National Health and Nutrition examination sur-vey were analyzed to determine how metabolic abnormalitiesaffect patient outcomes.27 Patients with both diabetes andmetabolic syndrome (n¼ 520) had significantly increasedhazard ratios for overall mortality compared with controls(P< 0.001) 1.97 (95% confidence intervals: 1.59, 2.43).27 As therelationship between the elements of metabolic syndrome isnot completely understood, therapy should aim at ‘‘multi-control’’ and must achieve a balance between the control ofone component without compromising others.
Obesity
It is generally recognized that obesity plays a key role in thedevelopment of T2DM; in particular, a high BMI and ab-dominal obesity are associated with insulin resistance,28 al-though the threshold at which BMI is sufficiently elevated todisrupt metabolic processes may differ regionally. In Indiaand Malta, for example, an increase in the prevalence of dia-betes is associated with BMI >15 kg=m2, whereas in Europe,this value is >25 kg=m2.5 Increased visceral (abdominal) fatdistribution confers an increased risk of vascular complica-tions relative to other patterns of weight distribution. Onestudy of visceral obesity and hemostatic profiles in patientswith T2DM found that this subgroup had both impaired fi-brinolysis and thrombogenesis.28 Reduction of obesity, par-ticularly visceral obesity, should therefore be one of the mostimportant goals in the treatment of patients with T2DM.Paradoxically, although advice to most overweight patientswith T2DM rightly emphasizes the importance of weight loss,pharmacological therapy against diabetes often has the un-desirable side effect of weight gain. Agents that have aweight-neutral or weight-sparing effect (for example, met-formin, exenatide, and detemir insulin) should be consideredin obese patients to achieve glycemic control without exac-erbating obesity.
Table 1. Association Between Type 2 Diabetes and Death from CHD=CVD
Men Women
No type 2 diabetes (n¼ 322) Type 2 diabetes (n¼ 78) No type 2 diabetes (n¼ 426) Type 2 diabetes (n¼ 91)
CHD (n) 17 12 5 9Risk ratioa 1 1.54 (1.03–2.25) 1 3.29 (1.79–6.55)
CVD (n) 31 19 18 13Risk ratioa 1 1.50 (1.11–2.00) 1 1.93 (1.29–2.85)
Values in parentheses are 95% confidence intervals. ª Elsevier and reproduced with permission from Imazu et al.17
aRisk ratio has been adjusted for age, BMI, serum uric acid, total cholesterol, triglyceride levels, hypertension, electrocardiograminformation, and smoking.
TREATMENT TAILORED TO TYPE 2 SPECTRUM 269

Ta
bl
e2.
AS
um
ma
ry
of
Cu
rr
en
tl
yU
se
dD
efi
nit
io
ns
fo
rM
et
ab
ol
ic
Sy
nd
ro
me
NC
EP
(20
01
)21
IDF
(20
05
)22
WH
O(1
99
9)2
3E
GIR
(19
99
)24
Pre
req
uis
ite
Incr
ease
dw
eig
ht
circ
um
fere
nce
(as
det
erm
ined
usi
ng
eth
nic
-sp
ecifi
ccr
iter
ia)
Dia
bet
esm
elli
tus,
imp
aire
dfa
stin
gg
luco
seo
rin
suli
nre
sist
ance
Insu
lin
resi
stan
ce
At
leas
tth
ree
of
the
foll
ow
ing
:P
lus
two
of
the
foll
ow
ing
:P
lus
two
of
the
foll
ow
ing
:B
loo
dp
ress
ure
�13
0=85
mm
Hg
or
dru
gtr
eatm
ent
�13
0=85
mm
Hg
or
dru
gtr
eatm
ent
�14
0=90
mm
Hg
or
dru
gtr
eatm
ent
�14
0=90
mm
Hg
or
anti
hy
per
ten
siv
em
edic
atio
nD
ysl
ipid
emia
TG�
150
mg=d
Lan
d=o
rH
DL
-C<
40m
g=
dL
(mal
e)an
d<
50m
g=d
L(f
emal
e)
TG�
150
mg=d
Lan
d=
or
HD
L-C
<40
mg=d
L(m
ale)
and<
50m
g=d
L(f
emal
e)
TG�
150
mg=d
Lan
d=o
rH
DL
-C�
35m
g=d
L(m
ale)
and�
40m
g=d
L(f
emal
e)
TG�
177
mg=d
Lan
d=o
rH
DL
-C<
40m
g=d
Lan
d=o
rtr
eate
dfo
rd
ysl
ipid
emia
Ob
esit
yC
entr
alo
bes
ity
:w
aist
circ
um
fere
nce
�10
2cm
(mal
e),�
88cm
(fem
ale)
Geo
gra
ph
y-s
pec
ific
thre
sho
lds
use
dW
aist
:hip
rati
o>
0.9
(mal
e),
>0.
85(f
emal
e)an
d=o
rB
MI>
30k
g=m
2
Cen
tral
ob
esit
y:
wai
stci
rcu
mfe
ren
ce�
94cm
(mal
e),�
80cm
(fem
ale)
Mic
roal
bu
min
uir
iaU
rin
ary
alb
um
inex
cret
ion
rati
o�
20m
g=m
ino
ral
bu
min
:cre
atin
era
tio
�30
mg=g
Fas
tin
gp
lasm
ag
luco
se�
110.
8m
g=d
L�
110
mg=d
L�
110
mg=d
L
EG
IR,
Eu
rop
ean
Gro
up
for
the
Stu
dy
of
Insu
lin
Res
ista
nce
;H
DL
-C,
hig
h-d
ensi
tyli
po
pro
tein
cho
lest
ero
l;ID
F,
Inte
rnat
ion
alD
iab
etes
Fed
erat
ion
;N
CE
P,
Th
eN
atio
nal
Ch
ole
ster
ol
Ed
uca
tio
nP
rog
ram
Ad
ult
Tre
atm
ent
Pan
elII
I;T
G,
trig
lyce
rid
es;
WH
O,
Wo
rld
Hea
lth
Org
aniz
atio
n.
270

Dyslipidemia
In people with T2DM, dyslipidemia typically manifestsas moderate hypertriglyceridemia with low levels of high-density lipoprotein cholesterol. This condition is likely to be aconsequence of the obesity and increased insulin resistanceseen in T2DM.29 Clinical evidence suggests that loweringcholesterol levels with statins reduces the risk of CHD in pa-tients with T2DM.29 Lowering triglyceride levels in personswith T2DM to reduce CVD mortality is still debatable. On theother hand, extreme hypertriglyceridemia increases the riskof eruptive xanthomas, lipemia retinalis, and pancreatitis.30
Although treatment is always necessary, conventional lipid-lowering agents are unlikely to be effective when blood glu-cose levels are poorly controlled.30 In such cases, intensivetherapy to normalize blood glucose levels should begin beforeregular monitoring of fasting triglyceride levels and lipid-lowering medication are introduced.
Hypertension
Hypertension is a risk factor for CVD commonly found inT2DM; here again, treatment has to complement existingtherapy, taking into account the fact that some antihyper-tensive medications may increase glycemic levels. Overall,clinical trials focusing on hypertensive patients with diabetessuggest that either an angiotensin-converting enzyme inhib-itor or an angiotensin receptor blocker should be consideredas a first-line drug, with beta-blockers as an alternative whenpatients also have CAD.31 However, most hypertensive pa-tients will require more than one agent to adequately controltheir blood pressure, and three or four drugs may be neces-sary to meet blood pressure targets. Achieving a blood pres-sure <130=80 mm Hg (<125=75 mm Hg, where patients alsohave renal insufficiency) significantly improves patientoutcomes.31
Psychosocial Factors
Depression
T2DM is known to act as a risk factor for depression, al-though there is a controversy over the likely prevalence; re-ported figures range from 9% to 60%.32 A concomitantdepression lowers the quality of life and also makes the con-
trol of diabetes more difficult. Increased HbA1c levels seem tobe associated with the severity of depression in some pa-tients.33 Whether this association reflects patients’ concernover their blood sugar levels or whether depression has acausative role in undermining glycemic control is unclear;further research is needed.
The treatment of depression in diabetes is complicated bypharmacological interactions. Classical tricyclic antidepres-sants increase sugar craving and worsen symptoms of auto-nomic neuropathy (postural hypotension, impotence, bladderdysfunction, etc.). Long-term treatment with different types ofantidepressants is associated with weight gain. Some selectiveserotonin reuptake inhibitors affect the metabolism of oralantidiabetes drugs such as some thiazolidinediones and me-glitinides and so may increase the likelihood of hyperglyce-mia.32 Pharmacological treatment of depression is oftennecessary but should be done with caution looking for pos-sible side effects, and we don’t have to forget that psycho-therapy may have the added benefit of supporting patientswith their diabetes and overall life management.
Patients’ ability to manage their diabetes mellitus plays acrucial part in any regimen; in the course of a year, an indi-vidual with an intensive insulin management regimen islikely to have self-injected more than 1,400 times, undertakenapproximately 2,190 blood glucose checks, and will have beenexpected both to monitor daily caloric intake and to adhere toa physically active lifestyle. If a patient fails to maintain anappropriate regimen, glycemic control is affected, which in-creases the risk of developing diabetes complications. It isperhaps not surprising that many patients become stressed bytheir diabetes, especially if they find self-injecting difficult.34
Socioeconomic factors
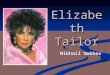
Socioeconomic factors play a role in outcomes for all pa-tients (Fig. 1). In some cases, poorer outcomes, definedbroadly as an increase in frequency and severity of diabetescomplications, can be linked to insufficient access to care. Inthe United States, as in many countries, reimbursement playsa substantial role in how patients receive treatment, and it hasbeen shown that, even in the same hospital, increased wealthsignificantly is associated with better quality of care.35 Thisrelationship between wealth and outcomes in diabetes mayresult directly from patients’ ability to contribute to the cost of
Socioeconomic position• Education• Employment• Occupational prestige• Income• Community
Health behaviors• Blood glucose monitoring• Adherence to diet and exercise program• Adherence to medication(s) prescribed• Smoking cessation
Health outcomesLife expectancy
Risk and severity of complicationsQuality of Life
Healthcare• HbA1c measurement• Cholesterol measurement• Nephropathy assessment• Foot examination• Dilated eye examination
FIG. 1. Conceptual framework for the relation between socioeconomic position and health among persons with diabetesmellitus.
TREATMENT TAILORED TO TYPE 2 SPECTRUM 271

treatment, or it may reflect a more subtle bias in how patientsare perceived by caregivers. Even where health care is, intheory, equal for all, socioeconomic status is a factor in diseaseoutcomes. A U.K. study correlated hospital admission ratesfor patients with diabetes with patients’ residence, suggest-ing that hospitalization was more frequent among poorerpatients.36
Age
The elderly are another vulnerable patient group.37,38
Poorer outcomes experienced by older patients with diabe-tes37,38 may be explained by confounding factors associatedwith age: increased frailty and impairment of manual dex-terity and=or cognitive function may all increase a patient’sdependence on others. Furthermore, these factors may con-tribute to an increased hypoglycemia unawareness, assymptoms of low blood sugar can be confused with a generalimpairment of cognitive function. A study comparing olderpatients (60–70 years) with younger patients (22–26 years)found that the elderly group were more vulnerable to severecognitive impairment and were less likely to be aware ofhypoglycemic events.39
Concerns over an elderly patient’s ability to withstandtreatment side effects, such as hypoglycemia, may promptphysicians to titrate doses less aggressively, particularly in thecase of patients living alone.40 Treating older patients there-fore requires adaptation of a regimen to account for a lower
threshold of tolerability. Certain oral antidiabetes drugs andmodern insulin analogs may help here by providing an im-proved balance between glycemic control and treatment sideeffects. For example, a recent study pooled data from threeclinical trials, conducted in older patients, and found a sig-nificantly lower level of hypoglycemia in patients taking in-sulin detemir compared with neutral protamine Hagedorninsulin at equivalent levels of glycemic control.40
Implications for Diabetes Therapy
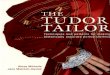
T2DM is a disease of substantial diversity: the developmentand magnitude of symptoms differ between patients, as doestheir ability to manage a prescribed regimen following diag-nosis. However, irrespective of the characteristics of the in-dividual patient, achieving good glycemic control is a clearand universal priority. An American Diabetes Association-approved algorithm has been proposed by Nathan et al.41 as abasis for addressing glycemic control (Fig. 2), with separatealgorithms proposed for introducing and intensifying anti-diabetes medication and=or insulin therapy. To successfullyimplement the algorithms, a review process every 3 months isrecommended, during which HbA1c levels are checked andtherapy adjusted accordingly until patients reach the Ameri-can Diabetes Association target of <7%. Then, a review every6 months is recommended to ensure that good glycemiccontrol is maintained. Another useful tool for physicians is theAmerican Association of Clinical Endocrinologists Roadmap
Yes*
No
NoNo
No No
Diagnosis
Lifestyle intervention + metformin
A1c ≥7% Yes*
Add basal insulin– most effective
Add sulfonylurea– least expensive
Add glitazone– no hypoglycemia
No A1c ≥7% A1c ≥7%
Intensify insulin Add glitazone+ Add basal insulin Add sulfonylurea+
A1c ≥7% Yes* A1c ≥7%
Add basal or intensify insulin
Intensive insulin + metformin ± glitazone
Yes* Yes*Yes*A1c ≥7%
FIG. 2. Algorithm for the metabolic management of type 2 diabetes. Lifestyle intervention should be reinforced at everyvisit, while reviewing treatment for existing and emergent co-morbidities. *HbA1c should be checked every 3 months until<7% and then at least every 6 months.{Although three oral agents can be used, initiation and intensification of insulintherapy are preferred based on effectiveness and expense. This algorithm has taken into account the relative costs of varioustreatments. ª American Diabetes Association and reproduced with permission from Nathan et al.41
272 ROLLA

and recently amended guidelines,42 which detail strategicapproaches for managing each stage of the patient’s changingcondition.
Regular appraisal of blood glucose offers physicians anopportunity for broader consideration of their patients’ treat-ment; as discussed, genetic or non-modifiable factors, stage ofdisease, concurrent morbidities, and associated risk factorsshould all be considered in the course of this process. Mod-ifiable risk factors such as obesity, dyslipidemia, and hyper-tension should also be addressed, such that a treatment reviewmay incorporate a wider spectrum of medication than is re-quired just to control blood glucose levels (‘‘multi-control’’).
Conclusions
The dynamic nature of T2DM means that therapy must bereviewed regularly, and a need for intensification should beanticipated. Intensification, which will include a change toinsulin therapy in patients initially treated with diet and oralantidiabetes drugs, must be appropriate to the underlyingfeatures of the disease in the individual, must take into ac-count changes in disease status and clinical presentation, andmust be simple and feasible for the individual. This includesthe need to address postprandial glucose as well as basalglucose in many patients, consideration of injection frequency,the desirability of minimizing weight gain, and the path tofuture intensification. As the regimen becomes more complex,through either co-morbidity or the progression of the diabe-tes, physicians may need to introduce elements of educationor psychological intervention to support adherence.
Acknowledgments
The author would like to acknowledge Dr. C. Mulcare,Watermeadow Medical, for medical writing assistance withthe manuscript, the support for which was provided by NovoNordisk Inc.
Author Disclosure Statement
A.R. is a member of the Speakers’ Bureaus for NovoNordisk A=S, Eli Lilly and Company, Takeda Pharmaceu-ticals North America, Inc., Roche Laboratories, and Glaxo-SmithKline.
References
1. Buchanan TA: Pancreatic beta-cell loss and preservation intype 2 diabetes. Clin Ther 2003;25(Suppl B2):B32–B46.
2. Freeman H, Cox RD: Type-2 diabetes: a cocktail of geneticdiscovery. Hum Mol Genet 2006;15:R202–R209.
3. Tusie Luna MT: Genes and type 2 diabetes mellitus. ArchMed Res 2005;36:210–222.
4. OMIM (Online Mendelian Inheritance in Man): http:==www.ncbi.nlm.nih.gov=sites=entrez?db¼omim (accessedJanuary 14, 2008).
5. The DECODE-DECODE Study Group on behalf of the Eu-ropean Diabetes Epidemiology Group and the InternationalDiabetes Epidemiology Group: Age, body mass index andtype 2 diabetes–-associations modified by ethnicity. Diabe-tologia 2003;46:1063–1070.
6. Egede LE, Dagogo-Jack S: Epidemiology of type 2 diabetes:focus on ethnic minorities. Med Clin North Am 2005;89:949–975.
7. Lanting LC, Joung IM, Mackenbach JP, Lamberts SW,Bootsma AH: Ethnic differences in mortality, end-stagecomplications, and quality of care among diabetic patients: areview. Diabetes Care 2005;28:2280–2288.
8. Barr DA: The practitioner’s dilemma: can we use a patient’srace to predict genetics, ancestry and the expected outcomesof treatment? Ann Intern Med 2005;143:809–815.
9. Wilkin TJ, Murphy MJ: The gender insulin hypothesis: whygirls are born lighter than boys, and the implications forinsulin resistance. Int J Obes 2006;30:1056–1061.
10. Legato MJ, Gelzer A, Goland R, Ebner SA, Rajan S, VillagraV, Kosowski M: Gender-specific care of the patient withdiabetes: review and recommendations. Gend Med 2006;3:131–158.
11. Murphy MJ, Metcalf BS, Voss LD, Jeffery AN, Kirkby J,Mallam KM, Wilkin TJ; The EarlyBird Study (EarlyBird 6):Girls at five are intrinsically more insulin resistant than boys:the programming hypotheses revisited–-the EarlyBird Study(EarlyBird 6). Pediatrics 2004;113:82–86.
12. Prentki M, Nolan CJ: Islet beta cell failure in type 2 diabetes.J Clin Invest 2006;116:1802–1812.
13. Chaturvedi N: The burden of diabetes and its complications:trends and implications for intervention. Diabetes Res ClinPract 2007;76(Suppl 1):S3–S12.
14. Tjokroprawiro A: New insights into oral agents in thetreatment of T2DM (the roles of fixed dose oral agentscombinations). Fol Med Indones 2005;41:159–168.
15. Stratton IM, Kohner EM, Aldington SJ, Turner RC, HolmanRR, Manley SE, Matthews DR: UKPDS 50: risk factorsfor incidence and progression of retinopathy in Type II di-abetes over 6 years from diagnosis. Diabetologia 2001;44:156–163.
16. Cubbon R, Kahn M, Kearney MT: Secondary prevention ofcardiovascular disease in type 2 diabetes and prediabetes: acardiologist’s perspective. Int J Clin Pract 2007;62:287–289.
17. Imazu M, Sumii K, Yamamoto H, Toyofuku M, Tadehara F,Okubo M, Yamakido M, Kohno N, Onaka AT: Influence oftype 2 diabetes mellitus on cardiovascular disease mortality:findings from the Hawaii-Los Angeles-Hiroshima study.Diabetes Res Clin Pract 2002;57:61–69.
18. Action to Control Cardiovascular Risk in Diabetes StudyGroup: Effects of intensive glucose lowering in type 2 dia-betes. N Engl J Med 2008;358:2545–2559.
19. Zimmet P, Boyko EJ, Collier GR, de Courten M: Etiology ofthe metabolic syndrome: potential role of insulin resistance,leptin resistance, and other players. Ann N Y Acad Sci1999;892:25–44.
20. Haller H: [Epidemiology and associated risk factors of hy-perlipoproteinemia]. Z Gesamte Inn Med 1977;32:124–128.
21. Executive Summary of the Third Report of the NationalCholesterol Education Program (NCEP) Expert Panel onDetection, Evaluation, and Treatment of High Blood Cho-lesterol in Adults (Adult Treatment Panel III). JAMA2001;285:2486–2497.
22. Alberti KG, Zimmet P, Shaw J: The metabolic syndrome–-anew worldwide definition. Lancet 2005;366:1059–1062.
23. World Health Organization: Definition, Diagnosis andClassification of Diabetes Mellitus and Its ComplicationsReport of a WHO Consultation. Part 1: Diagnosis andClassification of Diabetes and Mellitus. Publication NumberWHO=NCD=NCS=99.2. Geneva: World Health Organi-zation, 1999. http:==www.who.int=diabetes=publications=Definition%20and%20diagnosis%20of%20diabetes_new.pdf(accessed July 11, 2008).
TREATMENT TAILORED TO TYPE 2 SPECTRUM 273

24. Balkau B, Charles MA: Comment on the provisional reportfrom the WHO consultation. European Group for the Studyof Insulin Resistance (EGIR). Diabet Med 1999;16:442–443.
25. Wang J, Ruotsalainen S, Moilanen L, Lepisto P, Laakso M,Kuusisto J: The metabolic syndrome predicts cardiovascularmortality: a 13-year follow-up study in elderly non-diabeticFinns. Eur Heart J 2007;28:857–864.
26. Ryan MC, Farin HMF, Abbasi F, Reaven GM: Comparisonof waist circumference versus body mass index in diagnos-ing metabolic syndrome and identifying apparently healthysubjects at increased risk of cardiovascular disease. AmJ Cardiol 2008;102:40–46.
27. Malik S, Wong ND, Franklin SS, Kamath TV, L’Italien GJ,Pio JR, Williams GR: Impact of the metabolic syndrome onmortality from coronary heart disease, cardiovascular dis-ease, and all causes in United States adults. Circulation2004;110:1245–1250.
28. Kozek E, Katra B, Malecki M, Sieradzki J: Visceral obesityand hemostatic profile in patients with type 2 diabetes: theeffect of gender and metabolic compensation. Rev DiabetStud 2004;1:122–128.
29. Betteridge DJ: Diabetic dyslipidaemia. Diabetes Obes Metab2000;2(Suppl 1):S31–S36.
30. Smellie WS: Hypertriglyceridaemia in diabetes. BMJ2006;333:1257–1260.
31. Deedwania PC: Diabetes and hypertension, the deadly duet:importance, therapeutic strategy, and selection of drugtherapy. Cardiol Clin 2005;23:139–152.
32. Musselman DL, Betan E, Larsen H, Phillips LS: Relationshipof depression to diabetes types 1 and 2: epidemiology, bi-ology and treatment. Biol Psychiatry 2003;54:317–329.
33. Lustman PJ, Anderson RJ, Freedland KE, de Groot M,Carney RM, Clouse RE: Depression and poor glycemic con-trol: a meta-analytic review of the literature. Diabetes 2000;23:934–942.
34. Mollema ED, Snoek FJ, Ader HJ, Heine RJ, van der PloegHM: Insulin-treated diabetes patients with fear of self-injecting or fear of self-testing. Psychological comorbidityand general well-being. J Psychosom Res 2001;51:665–672.
35. Brown AF, Ettner SL, Piette J, Weinberger M, Gregg E,Shapiro MF, Karter AJ, Safford M, Waitzfelder B, Prata PA,Beckles GL: Socioeconomic position and health among per-
sons with diabetes mellitus: a conceptual framework andreview of the literature. Epidemiol Rev 2004;26:63–77.
36. Caddick SL, McKinnon M, Payne N, Ward TJ, Thornton-Jones H, Kells J, Ward JD: Hospital admissions and socialdeprivation of patients with diabetes mellitus. Diabet Med1994;11:981–983.
37. Kronmal RA, Barzilay JI, Smith NL, Psaty BM, Kuller LH,Burke GL, Furberg C: Mortality in pharmacologically treatedolder adults with diabetes: the Cardiovascular Health Study,1989–2001. PLoS Med 2006;3(10):e400.
38. Smith NL, Savage PJ, Heckbert SR, Barzilay JI, Bittner VA,Kuller LH, Psaty BM: Glucose, blood pressure, and lipidcontrol in older people with and without diabetes mellitus:the Cardiovascular Health Study. J Am Geriatr Soc2002;50:416–423.
39. Matyka K, Evans M, Lomas J, Cranston I, Macdonald I,Amiel SA: Altered hierarchy of protective responses againstsevere hypoglycemia in normal aging in healthy men. Dia-betes Care 1997;20:135–141.
40. Garber AJ, Clauson P, Pedersen CB, Kolendorf K: Lower riskof hypoglycemia with insulin detemir than with neutralprotamine Hagedorn insulin in older persons with type 2diabetes: a pooled analysis of Phase 3 trials. J Am Geriatr Soc2007;55:1735–1740.
41. Nathan DM, Buse JB, Davidson MB, Heine RJ, Holman RR,Sherwin R, Zinman B: Management of hyperglycemia intype 2 diabetes: a consensus algorithm for the initiationand adjustment of therapy. Diabetes Care 2006;9:1963–1972.
42. AACE Diabetes Mellitus Clinical Practice Guidelines TaskForce: American Association of Clinical Endocrinologistsmedical guidelines for clinical practice for the managementof diabetes mellitus. Endocr Pract 2007;13(Suppl 1):1–66.
Address reprint requests to:Arturo Rolla, M.D.
Beth Israel Deaconess Medical CenterHarvard Medical School
110 Francis Street, Suite 2FBoston, MA 02215
E-mail: [email protected]
274 ROLLA