Embed Size (px)
Citation preview

253
Adenoid cystic carcinoma presenting as an ulcer on the floor of the mouth: a rare case report
Saba Khan1, Khalid Agwani2, Puneet Bhargava1, Sreeja P. Kumar3
1Department of Oral Medicine and Radiology, NIMS Dental College and Hospital, NIMS University, Jaipur, 2Department of Oral and Maxillofacial Surgery, Darshan Dental College, Udaipur,
3Department of Oral Medicine and Radiology, Amrita School of Dentistry, Kochi, India
Abstract (J Korean Assoc Oral Maxillofac Surg 2014;40:253-257)
Adenoid cystic carcinoma is a rare epithelial tumour, and comprises about 1% of all malignant tumours of the oral and maxillofacial region. It is a malignant tumour which may develop in the trachea, bronchus, lungs or mammary glands, in addition to the head and neck region. Occurrences in the head and neck are mostly detected in the major salivary gland, oral cavity, pharynx and paranasal sinus where it presents as a slow growing firm nodu-lar swelling. The aim of the article is to highlight the unique presentation of adenoid cystic carcinoma as a solitary ulcer on the floor of the mouth.
Key words: Carcinoma, Adenoid cystic carcinoma, Oral cavity, Salivary gland neoplasms[paper submitted 2014. 4. 25 / revised 1st 2014. 6. 6, 2nd 2014. 7. 26 / accepted 2014. 7. 28]
bular,cribriformandsolidpatterns.Ithasarelentlessclinical
courseandusuallyafataloutcome”3.Thepresentcasereport
isuniqueasitshowspresentationofadenoidcysticcarci-
nomaasasolitaryulceronthefloorofthemouthratherthan
theclassicalnodularswelling.
II. Case Report
A56-year-oldmalepatientpresentedwithachiefcom-
plaintofanulcerintheleftfloorofthemouthforoneweek.
Hegaveahistoryofpainofrespectontheleftsideofthe
jawwhichwascontinuous,dull,throbbing,andradiatingto
theearofthesameside.Thepatienthadundergoneextrac-
tionfortooth#18butthepainstillpersisted.Thereafter,he
noticedanulcerontheleftfloorof themouthwhichwas
initiallysmallandincreasedtothepresentsize.Therewasno
relevanthistoryofinjury,traumaticsurgeryorbiopsy.There
wasnohistoryofbleedingordischarge,buthedidhavedif-
ficultyeatingandspeaking.Therewasnohistoryofsmoking,
quidchewingoralcoholconsumption.
Intraoralexaminationofthesofttissues,thebuccalmucosa,
labialmucosa,tongue,andpalateshowednoabnormalities,
buttherewasasolitaryulcerontheleftfloorofthemouth.
Examinationofgingivalstatusrevealedhisoralhygienesta-
tustobepoor,withseverestainsandcalculusdeposits.On
hardtissueexamination,healingsocketwaspresentinrespect
I. Introduction
AdenoidcysticcarcinomawasfirstdescribedbyBillroth
in1859andcalled“cylindroma”due to itscharacteristic
histologicappearance1.In1953,FooteandFrazell2renamed
thelesionasadenoidcysticcarcinoma.Adenoidcysticcar-
cinomaisamalignantsalivaryglandtumourcharacterized
byadeceptivehistologicpattern,indolent,locallyinvasive
growthwithhighpropensityforperineuralinvasion,localre-
currenceanddistantmetastasis.Theseuncommonneoplasms
accountforfewerthan1%ofallheadandneckmalignancies
andfewerthan10%ofallsalivaryneoplasms.Theymake
up15%-30%ofsubmandibularglandtumours,30%ofmi-
norsalivaryglandtumours,and2%-15%ofparotidgland
tumors1.It isdefinedbytheWorldHealthOrganizationas“abasaloidtumourconsistingofepithelialandmyoepithelial
cellsinvariousmorphologicalconfigurations,includingtu-
CASE REPORT
Saba KhanDepartment of Oral Medicine and Radiology, NIMS Dental College and Hospital, NIMS University, Shobha Nagar, Jaipur-Delhi highway, Jaipur 303121, Rajasthan, IndiaTEL: +91-1426-513102 FAX: +91-141-2605050E-mail: [email protected]
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
CC
Copyright Ⓒ 2014 The Korean Association of Oral and Maxillofacial Surgeons. All rights reserved.
http://dx.doi.org/10.5125/jkaoms.2014.40.5.253pISSN 2234-7550·eISSN 2234-5930

J Korean Assoc Oral Maxillofac Surg 2014;40:253-257
254
mostlysolitary,deep,andpainful,withsmoothmarginsanda
reddishhaloandmaypersistformonthswithhistoryofreoc-
currences.
Habitassociatedlesionsseeninquidchewersmayalso
formulcerationsattheregionofquidplacement.Odontogen-
icinfectionsmaybeassociatedwithanulcerthatmayserve
asacloacalopeningofasinusdrainingachronicalveolar
abscess.Theyaremostlyseeninthepalateandsublingualor
vestibularareas.Pusexudationwithregionallyinvolvedteeth
wouldhelpindifferentiation.Otherconditionssuchasacute
necroticulcerativegingivostomatitisorgangrenousstoma-
titisusuallypresentasnecroticsloughingulcerativelesions
diffuselyinvolvingthegingiva.Solitaryulcersarealsoseen
innonodontogenicsystemicdiseasessuchasuncontrolled
diabetesmellitus,blooddyscrasias(leukemia,sicklecellane-
mia),gastrointestinalandimmunocompromisedindividuals
andautoimmuneconditions(pemphigus,pemphigoid,ery-
themamultiforme,epidermolysisbullosa).Theulcersinsuch
conditionsarewelldemarcated,painful,andshallowwithan
erythematoushaloandagreynecroticfloor,usuallyinthe
marginalandinterdentalgingiva.Salivaryglanddisorders
suchasadenoidcysticcarcinoma,mucoepidermoidcarcino-
ma,mucousadenocarcinoma,Warthintumorandnecrotising
sialometaplasiaareseenassolitarypalatalulcers.
Anorthopantomogramandamandibularcrossectional
occlusalradiographweretakenandshowednoabnormality
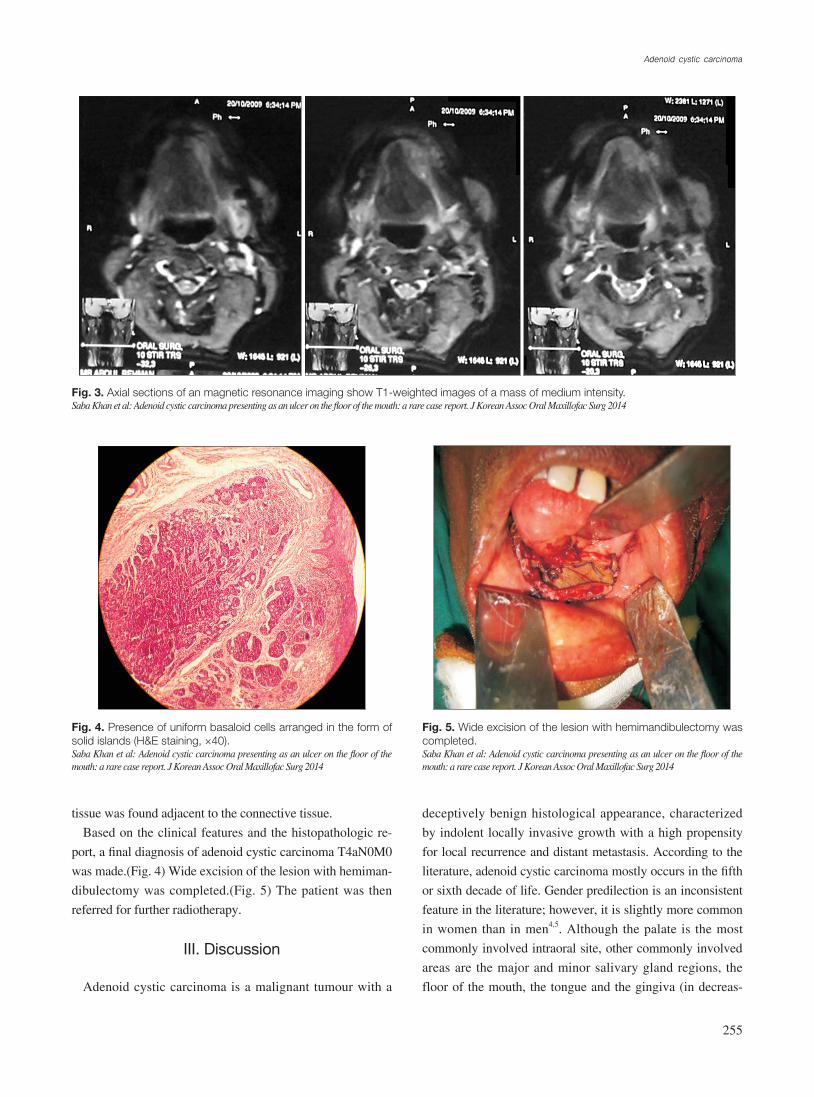
intheregionofinterest.(Fig.2)Amagneticresonanceim-
agewastaken,andtheaxialsectionsshowedaT1-weighted
imageofamassofmediumintensityextendingfromthe
midlineofthemandibletothepremolarregionontheleft
side.(Fig.3)Anincisionalbiopsywasperformedandthehis-
topathologicreportshowedthepresenceofuniformbasaloid
cellsarrangedintheformofsolidislands,alongwithacrib-
riformpatternatsomeplaces.Thetumourcellswerefound
tobeinfiltratingtheadjacenttissues.Normalsalivarygland
totooth#19.Onlocalexaminationofthelesion,inspectory
findingsrevealedasolitaryulcerpresentingasamucosaltear
involvingthemucosaandconnectivetissueextendingmesi-
allyfromleftsideofthelingualfrenumanddistallytoan
areacorrespondingtotheextractedtooth#19region.Theul-
cerwasseenincloseapproximationtotheleftalveolarridge.
Itwasovalinshape,3×2cmatitswidestpoint,and3cm
deep.Themarginswereeverted,theedgesoftheulcerwere
sloping,andthefloorwasnotevident.Thecolourwasthe
sameasthatoftheadjacentmucosa,buterythematousatthe
peripheryoftheulcer.Nobleedingordischargewasevident.
Photographsweretakenwithdueconsentfromthepatient.
(Fig.1)Onpalpationofthesite,thesizeandtheextentofthe
ulcerwereconfirmed.Theulcerwasmildlytenderonpalpa-
tion,withslopingedges.Themarginsandthebaseof the
ulcerweremildlyinduratedinaposterioraspect.Theulcer
restedonamuscularbase.
Basedonthehistorygivenbythepatientandtheclinical
features,aprovisionaldiagnosisofcarcinomaofthefloor
ofthemouthT4aN0M0,chronicgeneralizedperiodontitis,
partiallyedentulousinrespecttotooth#7,#5,#3,#13,#14,
#15,#24,#19,#25,and#31wasmade.Lesionspresenting
assolitaryulcersonthefloorofthemouthwereconsidered
inthedifferentialdiagnosis.Traumaticulcersaremostcom-
mononthetongue,lips,mucobuccalfold,gingivaandpalate.
Theypresentassolitaryulcerswithraisedreddishborders
andwhitenecroticfloorswithassociatedhistoryoftrauma.
Onthefloorofthemouth,theyareusuallyduetocalculus
orsharpdenturemargins.Majorrecurrentapthousulcersare
Fig. 2. Orthopantomogram does not reveal any changes in the region of interest.Saba Khan et al: Adenoid cystic carcinoma presenting as an ulcer on the floor of the mouth: a rare case report. J Korean Assoc Oral Maxillofac Surg 2014
Fig. 1. Solitary ulcer on the floor of the mouth.Saba Khan et al: Adenoid cystic carcinoma presenting as an ulcer on the floor of the mouth: a rare case report. J Korean Assoc Oral Maxillofac Surg 2014
Adenoid cystic carcinoma
255
deceptivelybenignhistologicalappearance,characterized
byindolentlocallyinvasivegrowthwithahighpropensity
forlocalrecurrenceanddistantmetastasis.Accordingtothe
literature,adenoidcysticcarcinomamostlyoccursinthefifth
orsixthdecadeoflife.Genderpredilectionisaninconsistent
featureintheliterature;however,itisslightlymorecommon
inwomenthaninmen4,5.Althoughthepalate is themost
commonlyinvolvedintraoralsite,othercommonlyinvolved
areasare themajorandminorsalivaryglandregions, the
floorofthemouth,thetongueandthegingiva(indecreas-
tissuewasfoundadjacenttotheconnectivetissue.
Basedontheclinicalfeaturesandthehistopathologicre-
port,afinaldiagnosisofadenoidcysticcarcinomaT4aN0M0
wasmade.(Fig.4)Wideexcisionofthelesionwithhemiman-
dibulectomywascompleted.(Fig.5)Thepatientwasthen
referredforfurtherradiotherapy.
III. Discussion
Adenoidcysticcarcinomaisamalignant tumourwitha
Fig. 3. Axial sections of an magnetic resonance imaging show T1-weighted images of a mass of medium intensity.Saba Khan et al: Adenoid cystic carcinoma presenting as an ulcer on the floor of the mouth: a rare case report. J Korean Assoc Oral Maxillofac Surg 2014
Fig. 4. Presence of uniform basaloid cells arranged in the form of solid islands (H&E staining, ×40).Saba Khan et al: Adenoid cystic carcinoma presenting as an ulcer on the floor of the mouth: a rare case report. J Korean Assoc Oral Maxillofac Surg 2014
Fig. 5. Wide excision of the lesion with hemimandibulectomy was completed.Saba Khan et al: Adenoid cystic carcinoma presenting as an ulcer on the floor of the mouth: a rare case report. J Korean Assoc Oral Maxillofac Surg 2014

J Korean Assoc Oral Maxillofac Surg 2014;40:253-257
256
adenoma8.
Possibletreatmentsofadenoidcysticcarcinomainclude
fourdifferentmodalities: surgical therapy, radiotherapy,
chemotherapyandcombinedtherapy.Surgicalexcisionwith
widemarginsis thetreatmentofchoice10.However, there
isstillcontroversyregardingtheadjuvanttreatmentofthis
tumour.Averyetal.11 recommendpostoperativeradiation
sinceradiationoftenproducestumourregressionandrelieves
symptoms.Postoperativeradiotherapyisalsoindicatedwhen
thetumourlocationisclosetothebaseofthecraniumwith
thepresenceofnecklymphnodemetastasisandperineural
invasion,withasolidhistologicalsubtype,andforrecur-
rent tumours11.Adenoidcysticcarcinomashowsalimited
responsetochemotherapy,anditisbelievedthatthislackof
aresponseisduetoitsslowgrowthrate.However,astudy
byAlcedoetal.12openedupanewpossibilityinthephar-
macological treatmentofthistumourbydemonstratingits
responsetoimatinibmesylate,apotentinhibitorofKITgenetyrosinekinase,whichisanenzymeinvolvedinthepatho-
genesisofthetumour.However,morestudiesareneededto
confirmitseffectiveness.Distantmetastasiscanoccureven
decadesaftertheprimarytumourhasbeentreatedandafter
havingachievedadequatelocoregionalcontrol.Thisleadsto
lowlong-termsurvivalrates.Someauthorsevenconsiderthis
tumourtobeanincurabledisease12.
Furthermore in thesettingof inoperable, incompletely
resectedorrecurrenttumours,outcomesafterconventional
therapyaredismalandremainatherapeuticchallenge.Some
authorshaveappliedotherformsofradiotherapy,particularly
neutronirradiation,aimingto improvetreatmentresults13.
However,adenoidcysticcarcinomaremainsincurablebe-
causefurtherimprovementsinlocal-regionalcontrolarenotlikelytoimpactsurvivalduetothehighnumberofdistant
failures.
Thepresentcasediffersfromusualcasesofadenoidcystic
carcniomawithrespecttositeandpresentation,makingita
rareentity.Thus,theaimofthisarticleistoemphasisethat
thoughtheliteraturestatesthatadenoidcysticcarcinomaul-
ceratesthesuperficiallesionalmucosa,itcanalsopresentas
anulcerativelesion.
Conflict of Interest
Nopotentialconflictofinterestrelevanttothisarticlewas
reported.
ingorder).Adenoidcysticcarcinomausuallypresentsasa
slowlygrowing,firm,unilobularmassintheglands.How-
ever,inourcaseitpresentedasasolitaryulceronthefloorof
themouth.Theclinicalcourseischaracterizedbyaninitial
periodofslowandindolentgrowththatisusuallyasymptom-
atic,althoughboneinvasionorperineuralspreadcancause
painorhypoesthesia5.Thetumourusuallyspreadsthrougha
haematogenousroutewithdistantmetastasis.Cervicalnode
metastasisisrare6.
Adenoidcysticcarcinomaofthesalivaryglandsisama-
lignantepithelial tumourwithbidirectionaldifferentiation
towardsluminal(ductal)andabluminal(myoepithelialand
basal)cells.Thetumouriscomposedofbasaloidcellswith
small,angulated,andhyperchromaticnucleiandscantcyto-
plasmarrangedintothreeprognosticallysignificantpatterns:
cribriform,tubular,andsolid.Thecombinationofsurgery
andpostoperativeradiationtherapyhasimprovedlocoregion-
alcontrolofthedisease.Despitethisachievement,latelocal
recurrenceanddistantmetastasisratesremainhighandmay
occurdecadesafterinitialdiagnosis5.
Initsmostfrequentlyseenhistologicalpattern,themajority
ofthecellsaresmallanddarklystainedwithscantcytoplasm.
Thecellsarearrangedinnestsorsheetsthatarefenestrated
byroundorovalspaces,creatingthecharacteristic“cribri-
form”design.Occasionally, the tumourshaveapredomi-
nantlysolidcellulargrowthwithabasaloidoranaplasticap-
pearancethathasfew,ifany,fenestrations.Thesolidvariant
oftendemonstratessmallareasofnecrosis.Tubularstructures
withminimalstratificationoftheliningepitheliumareoften
mixedwiththeclassiccribriformandsolidareas6.Several
authorshavesuggestedthatasolidhistologicalpatternindi-
catesamoreseriousprognosisthanacysticpattern.Stewart7
firstnotedtheincreasedaggressionsuggestedbythesolid
variant,althoughhecreditstheinitialobservationtoPatey
andThakray8.
Littleinformationexistsoncytogeneticabnormalitiesin
salivaryglandneoplasms,butinadenoidcysticcarcinoma,
anomaliesintheterminalpartofthe6qand9pchromosomes
havebeenreported.Recentstudieshavedemonstratedahigh
incidenceoflossofheterozygosityatchromosome6q23-359.
Thedifferentialdiagnosisofadenoidcysticcarcinomaincludes
tumoursthatalsoexhibittubularandcribriformstructures,
suchaspolymorphouslow-gradeadenocarcinoma,tumours
withbasaloidcellularmorphology,suchasbasalcelladenoma,
andbasalcelladenocarcinomaandtumourswithadualpopu-
lationofductalandmyoepithelialcells,suchaspleomorphic

Adenoid cystic carcinoma
257
lightofapathologicalstudyofparotidectomymaterial.BrJSurg1958;45:477-87.
9. RapidisAD,GivalosN,GakiopoulouH,FaratzisG,StavrianosSD,VilosGA,etal.Adenoidcysticcarcinomaoftheheadandneck.Clinicopathologicalanalysisof23patientsandreviewoftheliterature.OralOncol2005;41:328-35.
10. Norberg-SpaakL,DardickI,LedinT.Adenoidcysticcarcinoma:useofcellproliferation,BCL-2expression,histologicgrade,andclinicalstageaspredictorsofclinicaloutcome.HeadNeck2000;22:489-97.
11. AveryCM,MoodyAB,McKinnaFE,TaylorJ,HenkJM,Lang-donJD.Combinedtreatmentofadenoidcysticcarcinomaofthesalivaryglands.IntJOralMaxillofacSurg2000;29:277-9.
12. AlcedoJC,Fábrega JM,ArosemenaJR,UrrutiaA. Imatinibmesylateas treatmentforadenoidcysticcarcinomaof thesali-varyglands:reportoftwosuccessfullytreatedcases.HeadNeck2004;26:829-31.
13. HuberPE,DebusJ,LatzD,ZierhutD,BischofM,WannenmacherM,etal.Radiotherapyforadvancedadenoidcysticcarcinoma:neutrons,photonsormixedbeam?RadiotherOncol2001;59:161-7.
References
1. BillrothT.Beobachtungenübergeschwülstederspeicheldrüsen.ArchPathAnat1859;17:357-75.
2. FooteFWJr,FrazellEL.Tumorsof themajorsalivaryglands.Cancer1953;6:1065-133.
3. El-NaggarAK,HuvosAG.Adenoidcysticcarcinoma.In:BarnesL,EvesonJW,ReichartP,SidranskyD,eds.Pathologyandgeneticsofheadandnecktumors.WorldHealthOrganizationclassificationoftumors.Lyon:IARCPress;2005.
4. BianchiB,CopelliC,CocchiR,FerrariS,PederneschiN,SesennaE.Adenoidcysticcarcinomaofintraoralminorsalivaryglands.OralOncol2008;44:1026-31.
5. JasoJ,MalhotraR.Adenoidcysticcarcinoma.ArchPatholLabMed2011;135:511-5.
6. SpiroRH.Distantmetastasisinadenoidcysticcarcinomaofsali-varyorigin.AmJSurg1997;174:495-8.
7. StewartJ.Carcinomaofsalivaryglandsshowingthecylindromapattern.BrJSurg1961;49:241-5.
8. PateyDH,ThackrayAC.Thetreatmentofparotidtumoursinthe

















![Metastatic Adenoid Cystic Carcinoma with Signet Ring … · · 2016-02-02adenoid cystic carcinoma and was only first described in the literature in 2013 by Altemani et al [5]. They](https://img.pdfslide.net/doc/110x75/5adab81c7f8b9a6d7e8d1060/metastatic-adenoid-cystic-carcinoma-with-signet-ring-cystic-carcinoma-and-was.jpg)











