Embed Size (px)
Citation preview

ADHDADHDTreatmentTreatment

CONTINUITY CLINIC
ObjectivesObjectives
Be familiar with the evidence Be familiar with the evidence supporting particular forms of supporting particular forms of management for ADHD, including management for ADHD, including medicationmedication
Know the different classes of Know the different classes of stimulant medications and their stimulant medications and their potential side effectspotential side effects
Be familiar with Atomoxetine and its Be familiar with Atomoxetine and its potential side effectspotential side effects

CONTINUITY CLINIC
Recommendation 1:Recommendation 1:Management ProgramManagement Program
Primary care clinicians should Primary care clinicians should establish a management program establish a management program that recognizes ADHD as a that recognizes ADHD as a chronic conditionchronic condition
Strong evidenceStrong evidence Strong recommendationStrong recommendation

CONTINUITY CLINIC
Recommendation 1:Recommendation 1:Management ProgramManagement Program
Prevalence 4-12% of school-age Prevalence 4-12% of school-age childrenchildren
60-80% persist into adolescence60-80% persist into adolescence
Inform, educate, counsel, demystifyInform, educate, counsel, demystify family, childfamily, child
ResourcesResources local, national (CHADD, ADDA)local, national (CHADD, ADDA)

CONTINUITY CLINIC
Recommendation 1:Recommendation 1:Management ProgramManagement Program
What distinguishes this condition What distinguishes this condition from most other conditions from most other conditions managed by primary care managed by primary care clinicians is the important role clinicians is the important role that the that the educational systemeducational system plays plays in the treatment and monitoring of in the treatment and monitoring of children with ADHD.children with ADHD.

CONTINUITY CLINIC
Recommendation 2:Recommendation 2:Target Outcomes by TeamTarget Outcomes by Team The treating clinician, parents, The treating clinician, parents,
and the child, in collaboration with and the child, in collaboration with school personnel, should specify school personnel, should specify appropriate target outcomes to appropriate target outcomes to guide management.guide management.
Strong evidenceStrong evidence Strong recommendationStrong recommendation

CONTINUITY CLINIC
Recommendation 2:Recommendation 2:Outcomes- maximize Outcomes- maximize
functionfunction RelationshipsRelationships parents, siblings, peersparents, siblings, peers
Disruptive behaviorsDisruptive behaviors Academic performanceAcademic performance
work volume, efficiency, completion, work volume, efficiency, completion, accuracyaccuracy
IndividualIndividual self-care, self-esteemself-care, self-esteem
Safety in the community Safety in the community

CONTINUITY CLINIC
Objectives of the Literature Objectives of the Literature ReviewReview
EffectivenessEffectiveness (short and long-term) (short and long-term) and and safetysafety of therapies of therapies
Medication and non-medication Medication and non-medication therapiestherapies
Single therapy vs combinationSingle therapy vs combination 6-12 year olds6-12 year olds

CONTINUITY CLINIC
Sources for ReviewSources for Review
Agency for Healthcare Research & QualityAgency for Healthcare Research & Quality McMaster Univ. Evidence-based Practice CenterMcMaster Univ. Evidence-based Practice Center
Canadian Office for Health Technology Canadian Office for Health Technology Assessment Study (CCOHTA)Assessment Study (CCOHTA)
Multimodal Treatment Study (MTA Study)Multimodal Treatment Study (MTA Study) Pelham et al. review of psychosocial therapiesPelham et al. review of psychosocial therapies

CONTINUITY CLINIC
Recommendation 2:Recommendation 2:developing target outcomesdeveloping target outcomes
InputInput parents, children (patient), teachersparents, children (patient), teachers
3-6 key targets3-6 key targets realistic, attainable, measurablerealistic, attainable, measurable methods will change over time methods will change over time

CONTINUITY CLINIC
School InterventionsSchool InterventionsIndividual Education Plan Individual Education Plan
504 Plan504 Plan IDEA = Individuals IDEA = Individuals
with Disabilities with Disabilities Education ActEducation Act
ADHD under “Other ADHD under “Other Health Impaired”Health Impaired”
Educational DisabilityEducational Disability ServicesServices
Section 504 of the Section 504 of the Rehabilitation ActRehabilitation Act
ADHD medical ADHD medical diagnosisdiagnosis
Medical Disability Medical Disability with educational with educational impactimpact
AccommodationsAccommodations

CONTINUITY CLINIC
Recommendation 3:Recommendation 3:make some make some
recommendationsrecommendations The clinician should recommend The clinician should recommend
stimulant medication and/or behavior stimulant medication and/or behavior therapy as appropriate, to improve therapy as appropriate, to improve target outcomes in children with target outcomes in children with ADHDADHD
StrongStrong evidence (medication), evidence (medication), FairFair evidence (behavior evidence (behavior therapy) therapy)
Strong recommendationStrong recommendation

CONTINUITY CLINIC
Recommendation 3:Recommendation 3:Efficacy of StimulantsEfficacy of Stimulants
Short-term benefits well establishedShort-term benefits well established
Core symptoms: attention, Core symptoms: attention, hyperactivity, and impulsivityhyperactivity, and impulsivity
observable social and classroom observable social and classroom behaviorsbehaviors
IQ and achievement testing- less IQ and achievement testing- less effect effect

CONTINUITY CLINIC
Recommendation 3:Recommendation 3:MTA StudyMTA Study
Effects over 14 monthsEffects over 14 months 579 children 7-9.9 years old579 children 7-9.9 years old 4 randomized groups4 randomized groups
medication alonemedication alone medication and behavior medication and behavior
managementmanagement behavior managementbehavior management standard community care standard community care

CONTINUITY CLINIC
Recommendation 3:Recommendation 3:MTA StudyMTA Study
Medication management alone Medication management alone Medication + behavior therapy Medication + behavior therapy
> Community management> Community management > Behavior management alone> Behavior management alone

CONTINUITY CLINIC
The StimulantsThe StimulantsNobody does it betterNobody does it better
Short, intermediate (the “old” long-Short, intermediate (the “old” long-lasting), truly long actinglasting), truly long acting
22 studies show 22 studies show NONO difference between difference between methylphenidate, dextroamphetamine, methylphenidate, dextroamphetamine, or mixed amphetamine salts (Adderall)or mixed amphetamine salts (Adderall)
Individual’s response may varyIndividual’s response may vary NONO serologic, hematologic tests needed serologic, hematologic tests needed**EKG – based on history and risk**EKG – based on history and risk

CONTINUITY CLINIC
Non-stimulantsNon-stimulantsSecond rate-only 2Second rate-only 2
Tricyclic antidepressantsTricyclic antidepressants 9 studies alone9 studies alone 4 studies =/< methylphenidate4 studies =/< methylphenidate
Bupropion (Wellbutrin, Zyban)Bupropion (Wellbutrin, Zyban) Clonidine Clonidine
limited studieslimited studies > placebo> placebo

CONTINUITY CLINIC
StimulantsStimulantsDose determinationDose determination
NOTNOT weight dependent weight dependent Optimal effects with minimal side Optimal effects with minimal side
effectseffects nothing ventured, nothing gainednothing ventured, nothing gained
Match target outcomes and timingMatch target outcomes and timing crucial step prior to startingcrucial step prior to starting

CONTINUITY CLINIC
StimulantsStimulantsSide effectsSide effects
appetite suppressionappetite suppression stomachache, headachestomachache, headache delayed sleep onsetdelayed sleep onset jitterinessjitteriness overfocused, dull demeanoroverfocused, dull demeanor mood disturbancesmood disturbances

CONTINUITY CLINIC
StimulantsStimulantsSide effects- NOTSide effects- NOT
seizures- seizures- NONO increased frequency with increased frequency with mphmph
growth delay- at least one negative studygrowth delay- at least one negative study Tourette syndromeTourette syndrome
15-20% of patients have motor tics15-20% of patients have motor tics 50% of TS have ADHD50% of TS have ADHD 7 studies comparing stimulants vs 7 studies comparing stimulants vs
placebo/other show placebo/other show NONO increase in tics with increase in tics with stimulantsstimulants

CONTINUITY CLINIC
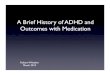
Short Intermediate Short Intermediate ExtendedExtended
Methylphenidate Ritalin Focalin
Ritalin 20 SR Metadate ER
Concerta Metadate CD Ritalin LA
Dextroamphetamine Dexedrine Dextrostat
Dexedrine spansule
Adderall
Adderall XR
3-4 hours 5-6 hours 8-10 (12)hours

CONTINUITY CLINIC

CONTINUITY CLINIC
AtomoxetineAtomoxetineStratteraStrattera
Selective norepinephrine uptake Selective norepinephrine uptake inhibitorinhibitor
Little effect on dopamine or Little effect on dopamine or serotonin uptakeserotonin uptake
Little effect on Ach, H1, alpha-2, DA Little effect on Ach, H1, alpha-2, DA receptorsreceptors
Well-tolerated in adult and pediatric Well-tolerated in adult and pediatric studiesstudies

CONTINUITY CLINIC
Atomoxetine...Atomoxetine...Randomized, Randomized, Placebo-Controlled, Dose-Placebo-Controlled, Dose-
Response...Response... 297 children and adolescents297 children and adolescents 8-18 years old; 71 % male8-18 years old; 71 % male 70% had prior stimulant therapy70% had prior stimulant therapy Combined/Inattentive/Hyper-impulsiveCombined/Inattentive/Hyper-impulsive 63/33/2 %63/33/2 % 37 % Oppositional-defiant disorder37 % Oppositional-defiant disorder 1 depression, 1 anxiety disorder1 depression, 1 anxiety disorder
Atomoxetine…AD/HD…Study. Pediatrics 108:e83, 2001

CONTINUITY CLINIC
Side EffectsSide Effects Small samples:Small samples:
dizziness 9% vs 1% placebodizziness 9% vs 1% placebo vomiting 6% vs 7% vomiting 6% vs 7%
Weight loss dose dependentWeight loss dose dependent mean 0.4kg at 1.2 mg/kg/dmean 0.4kg at 1.2 mg/kg/d
small pulse, BP changessmall pulse, BP changes no EKG changesno EKG changes <5% dropout rate atmx and placebo<5% dropout rate atmx and placebo
Atomoxetine…AD/HD…Study. Pediatrics 108:e83, 2001

CONTINUITY CLINIC
Efficacy of Atomoxetine vs Efficacy of Atomoxetine vs Placebo in School-Age Girls Placebo in School-Age Girls
with AD/HDwith AD/HD 52 children and adolescents52 children and adolescents 7-13 years old7-13 years old Combined/Inattentive/Hyper-Combined/Inattentive/Hyper-
impulsiveimpulsive 79/21/0 %79/21/0 % 38.5 % Oppositional-defiant disorder38.5 % Oppositional-defiant disorder 13.5% phobias13.5% phobias
Efficacy…Girls...AD/HD. Pediatrics 110:e75, 2002

CONTINUITY CLINIC
MeasuresMeasures
ADHD Rating Scale- ParentADHD Rating Scale- Parent Conners’ Parent RS-RevisedConners’ Parent RS-Revised
No Teacher ratingsNo Teacher ratings
Clinical Global Impressions of ADHD Clinical Global Impressions of ADHD Severity- ClinicianSeverity- Clinician
Efficacy…Girls...AD/HD. Pediatrics 110:e75, 2002

CONTINUITY CLINIC
Side EffectsSide Effects Small sample size subset here Small sample size subset here
(279 total); so no significant (279 total); so no significant differencesdifferences
Vomiting 19% vs 0%Vomiting 19% vs 0% Abdominal pain 29% vs 14%Abdominal pain 29% vs 14% Nausea 6.5% vs 14%Nausea 6.5% vs 14% ?Weight, cardiac...?Weight, cardiac... Increased cough 16% vs 4.8%Increased cough 16% vs 4.8%Efficacy…Girls...AD/HD. Pediatrics 110:e75, 2002

CONTINUITY CLINIC
Atomoxetine and Atomoxetine and Methylphenidate... Methylphenidate... Prospective Prospective
Randomized, Open-Label TrialRandomized, Open-Label Trial 228 children and adolescents228 children and adolescents 184 atomoxetine, 44 mph; 10 weeks184 atomoxetine, 44 mph; 10 weeks 7-15 year old boys; 7-9 year old girls7-15 year old boys; 7-9 year old girls Most/all had prior stimulant therapyMost/all had prior stimulant therapy Combined/Inattentive/Hyper-Combined/Inattentive/Hyper-
impulsiveimpulsive 76/23/1 %76/23/1 % 53% ODD, 7% major depression 53% ODD, 7% major depression
Atomoxetine and Methylphenidate... Prospective Randomized, Open-Label Trial JAACAP 41:7, 2002

CONTINUITY CLINIC
MeasuresMeasures
ADHD Rating Scale- Parent ADHD Rating Scale- Parent CompletedCompleted
ADHD Rating Scale- Parent InterviewADHD Rating Scale- Parent Interview Conners’ Parent RS-RevisedConners’ Parent RS-Revised
No Teacher ratingsNo Teacher ratings Clinical Global Impressions of ADHD Clinical Global Impressions of ADHD
Severity- ClinicianSeverity- Clinician Atomoxetine and Methylphenidate... Prospective Randomized, Open-Label Trial JAACAP 41:7, 2002

CONTINUITY CLINIC
FindingsFindings
Comparable improvement between the Comparable improvement between the twotwo
mean dose 1.4 mg/kg/d extensive mtb, mean dose 1.4 mg/kg/d extensive mtb, 0.5mg/kg/d slow mtb 0.5mg/kg/d slow mtb
mph mph 0.85 mg/kg/d, (31mg/d) 0.85 mg/kg/d, (31mg/d)
High rate of dropoutsHigh rate of dropouts
Atomoxetine and Methylphenidate... Prospective Randomized, Open-Label Trial JAACAP 41:7, 2002

CONTINUITY CLINIC
FindingsFindings 43% of mph, 36 % atmx dropped out!43% of mph, 36 % atmx dropped out! 11%; 5 % because of adverse effects 11%; 5 % because of adverse effects
comparablecomparable
atomoxetine wt loss avg 0.6 kg; (mph 0.1)atomoxetine wt loss avg 0.6 kg; (mph 0.1) small changes both in pulse, BPsmall changes both in pulse, BP EKG, labs no problems, no differencesEKG, labs no problems, no differences
Atomoxetine and Methylphenidate... Prospective Randomized, Open-Label Trial JAACAP 41:7, 2002

CONTINUITY CLINIC
Side EffectsSide Effects Generally comparableGenerally comparable Vomiting 12% vs 0%Vomiting 12% vs 0% Abdominal pain 23% vs 17.5% (NS)Abdominal pain 23% vs 17.5% (NS) Nausea 10% vs 5% (NS)Nausea 10% vs 5% (NS) ?Weight, cardiac...?Weight, cardiac... Cough 5% sameCough 5% same ““Thinking abnormal” 0% vs 5% (N=2)Thinking abnormal” 0% vs 5% (N=2)
Atomoxetine and Methylphenidate... Prospective Randomized, Open-Label Trial JAACAP 41:7, 2002

CONTINUITY CLINIC
Pros and Pros and Cons Cons
No abuse potentialNo abuse potential adolescent usageadolescent usage adult usageadult usage
24/7 coverage24/7 coverage No tic relationshipNo tic relationship Novel class of medNovel class of med
use use withwith stimulants, toostimulants, too
Little data head to Little data head to head vs stimulantshead vs stimulants
Weight loss/vomitingWeight loss/vomiting Takes week(s) to Takes week(s) to
effectseffects Tolerance Tolerance
““starter kit” issuestarter kit” issue adjust if SSRI added adjust if SSRI added
CostCost

CONTINUITY CLINIC
Behavior TherapyBehavior Therapyaccept no substitutesaccept no substitutes
Behavior therapyBehavior therapy Emotions-based therapy Emotions-based therapy
e.g. play therapy-e.g. play therapy-NOTNOT efficacious in efficacious in ADHDADHD
Thought patterns directedThought patterns directed cognitive, cognitive-behavioral therapycognitive, cognitive-behavioral therapy NOTNOT efficacious in ADHD efficacious in ADHD

CONTINUITY CLINIC
Behavior TherapyBehavior TherapyParent TrainingParent Training
8-12 weeks with trained therapist8-12 weeks with trained therapist teaches parent teaches parent skillsskills incorporates maintenance and incorporates maintenance and
relapsesrelapses improves child’s functioning and improves child’s functioning and
behaviorbehavior not necessarily achieves normal not necessarily achieves normal
behaviorbehavior

CONTINUITY CLINIC
Behavior TherapyBehavior Therapy Examples of Techniques Examples of Techniques
Positive reinforcementPositive reinforcement reward for performancereward for performance
Time-outTime-out removing positive reinforcementremoving positive reinforcement
Response costResponse cost losing advance rewards losing advance rewards
Token economyToken economy combinationcombination

CONTINUITY CLINIC
Behavior TherapyBehavior Therapy Meta-analyses difficult and Meta-analyses difficult and
fewfew Must be maintained to be effectiveMust be maintained to be effective Stimulant effects much > behavioral Stimulant effects much > behavioral
therapytherapy MTA study: combination > med alone, but MTA study: combination > med alone, but notnot
a statistically significant differencea statistically significant difference However, parents and teachers However, parents and teachers more satisfiedmore satisfied
Schools can implementSchools can implement 504 Plan504 Plan IEPIEP

CONTINUITY CLINIC
Recommendation 4:Recommendation 4:When to re-evaluateWhen to re-evaluate
When the selected management for a When the selected management for a child with ADHD has child with ADHD has not met target not met target outcomesoutcomes, clinicians should evaluate , clinicians should evaluate the the original diagnosisoriginal diagnosis, , use use of all of all appropriate treatments, adherence to appropriate treatments, adherence to the treatment plan, and presence of the treatment plan, and presence of coexistingcoexisting conditions conditions
Weak evidenceWeak evidence Strong recommendation Strong recommendation

CONTINUITY CLINIC
Recommendation 4:Recommendation 4:Ddx in re-evaluationDdx in re-evaluation
unrealistic target symptomsunrealistic target symptoms poor information regarding child’s poor information regarding child’s
behaviorbehavior incorrect diagnosis and/orincorrect diagnosis and/or coexisting condition interferingcoexisting condition interfering
ODD, conduct disorder, mood, anxiety, LDODD, conduct disorder, mood, anxiety, LD poor adherence/compliancepoor adherence/compliance treatment failure treatment failure

CONTINUITY CLINIC
Recommendation 4:Recommendation 4:Steps in re-evaluationSteps in re-evaluation
Re-establish target symptomsRe-establish target symptoms ““team” communicationteam” communication
Gather further information, other Gather further information, other sourcessources
Consider consultationConsider consultation Consider psycho-educational testingConsider psycho-educational testing

CONTINUITY CLINIC
Recommendation 4:Recommendation 4:True treatment failureTrue treatment failure
Lack of response to 2-3 stimulantsLack of response to 2-3 stimulants maximum dosemaximum dose without side effects without side effects any dose with intolerable side effectsany dose with intolerable side effects
Inability to control child’s behaviorInability to control child’s behavior Interference of coexisting conditionInterference of coexisting condition
Refer to mental healthRefer to mental health

CONTINUITY CLINIC
Recommendation 5:Recommendation 5:follow-up guidelinesfollow-up guidelines
The clinician should periodically The clinician should periodically provide a systematic follow-up for provide a systematic follow-up for the child with ADHD. Monitoring the child with ADHD. Monitoring should be directed to should be directed to target target outcomesoutcomes and and adverse effectsadverse effects by by obtaining specific information from obtaining specific information from parents, teachers, and the child.parents, teachers, and the child.
Fair evidenceFair evidence Strong recommendationStrong recommendation

CONTINUITY CLINIC
Recommendation 5:Recommendation 5:follow-up guidelinesfollow-up guidelines
TeamTeam management plan management plan not just : “What does the doctor not just : “What does the doctor
recommend?”recommend?” Recording clinical dataRecording clinical data
flow sheet, progress noteflow sheet, progress note Interview, T-Con, teacher reports, Interview, T-Con, teacher reports,
report cards, checklistsreport cards, checklists

CONTINUITY CLINIC
Recommendation 5:Recommendation 5:frequency of follow-upfrequency of follow-up
NONO controlled trials document the controlled trials document the appropriate frequencyappropriate frequency
MTA study: more frequent did MTA study: more frequent did better, BUTbetter, BUT
Once stable, visit every 3-6 monthsOnce stable, visit every 3-6 months

CONTINUITY CLINIC
Conclusion nuggetsConclusion nuggets ADHD is a ADHD is a chronicchronic condition condition
Explicit negotiations regarding Explicit negotiations regarding targettarget outcomes are key outcomes are key
Stimulant and behavior therapy Stimulant and behavior therapy use are the mainstay of therapyuse are the mainstay of therapy