Embed Size (px)
Citation preview
• PATA is a network of healthcare providers operating programmes in partnership with 289 facilities in 24 African countries.
• From July 2014 – August 2017, PATA conducted a situational analysis of adolescent HIV treatment and care in 218 facilities in 23 countries. Narrative responses from health facility surveys (n=218) and programme reports by healthcare providers (n=289) constitute the primary research base for this study.
• Inductive analysis of Mzantsi Wakho and PATA data identified multiple, divergent understandings of ART non-adherence and defaulting among HIV-positive teenagers, caregivers, and healthcare providers. Combined deductive analysis explored these discrepancies in further detail.
Adherence misfits: Divergent perspectives on ART-defaulting among HIV-positive adolescents, caregivers and healthcare workersRebecca Hodes1,2, Luanne Hatane3, Lesley Gittings1,4, Agnes Ronan2, Samantha Malunga3, Lucie Cluver2,5, Daniella Mark3, Elona Toska6, Kim Bloch3 and Roxanna Haghighat2
1 AIDS and Society Research Unit, University of Cape Town, South Africa, 2 Department of Social Policy and Intervention, Oxford University, United Kingdom, 3 Paediatric Adolescent Treatment for Africa, 4 Department of Public Health and Family Medicine, University of Cape Town, South Africa, 5 Department of Psychiatry and Mental Health, University of Cape Town, 6 Department of Sociology, University of Cape Town, South Africa
ResultsHealthcare workers’ perspectives: ‘We don’t know how to stop this defaulting business’
• Within the combined PATA and Mzantsi Wakho datasets, many healthcare workers were frustrated by non-adherence among adolescent patients, which they perceived as a behavioural phenomenon beyond their control, but for which they would bear the negative consequences in the form of a heavier case-burden of HIV-related morbidity and mortality.
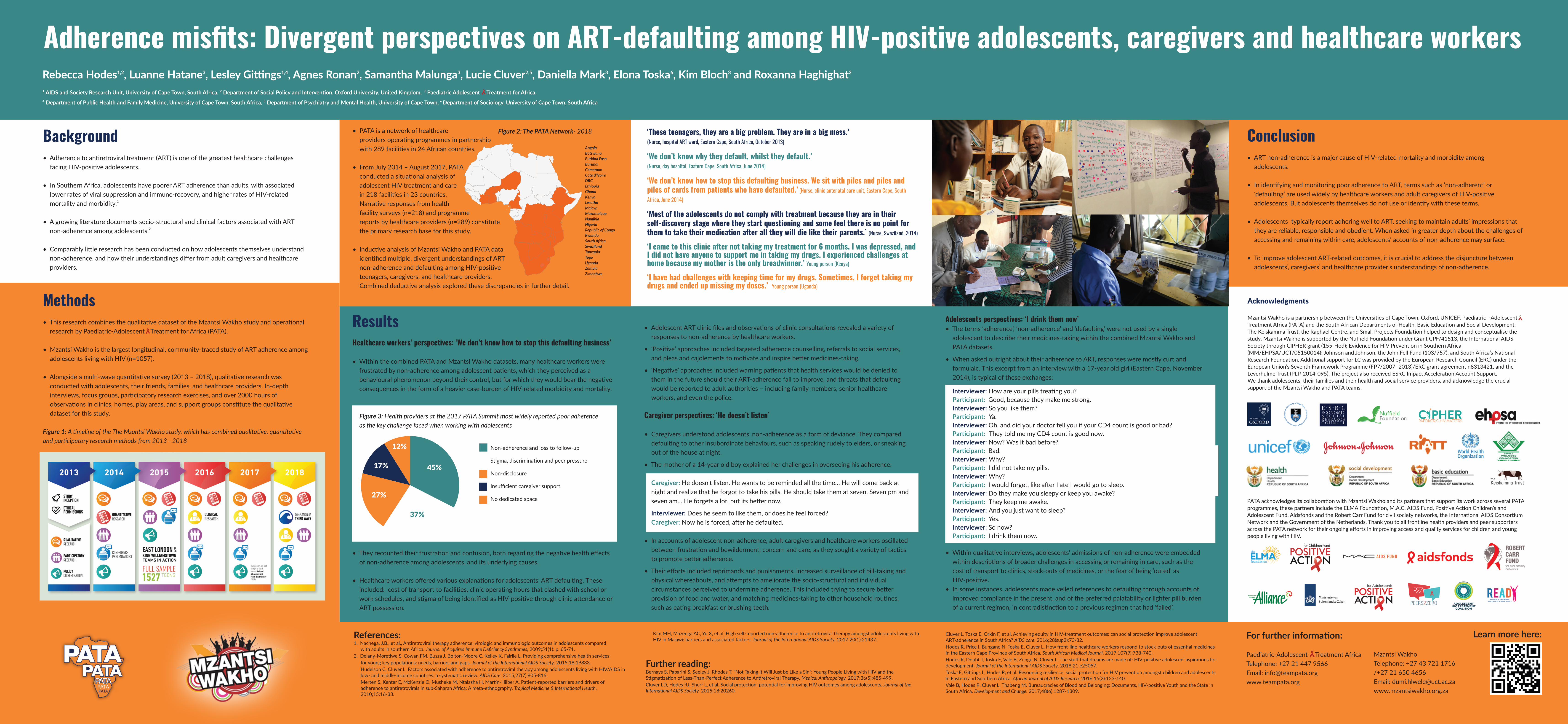
Figure 3: Health providers at the 2017 PATA Summit most widely reported poor adherence as the key challenge faced when working with adolescents
• They recounted their frustration and confusion, both regarding the negative health effects of non-adherence among adolescents, and its underlying causes.
• Healthcare workers offered various explanations for adolescents’ ART defaulting. These included: cost of transport to facilities, clinic operating hours that clashed with school or work schedules, and stigma of being identified as HIV-positive through clinic attendance or ART possession.
‘These teenagers, they are a big problem. They are in a big mess.’ (Nurse, hospital ART ward, Eastern Cape, South Africa, October 2013)
‘We don’t know why they default, whilst they default.’ (Nurse, day hospital, Eastern Cape, South Africa, June 2014)
‘We don’t know how to stop this defaulting business. We sit with piles and piles and piles of cards from patients who have defaulted.’ (Nurse, clinic antenatal care unit, Eastern Cape, South Africa, June 2014)
‘Most of the adolescents do not comply with treatment because they are in their self-discovery stage where they start questioning and some feel there is no point for them to take their medication after all they will die like their parents.’ (Nurse, Swaziland, 2014)
‘I came to this clinic after not taking my treatment for 6 months. I was depressed, and I did not have anyone to support me in taking my drugs. I experienced challenges at home because my mother is the only breadwinner.’ Young person (Kenya)
‘I have had challenges with keeping time for my drugs. Sometimes, I forget taking my drugs and ended up missing my doses.’ Young person (Uganda)
Acknowledgments
Mzantsi Wakho is a partnership between the Universities of Cape Town, Oxford, UNICEF, Paediatric - Adolescent Treatment Africa (PATA) and the South African Departments of Health, Basic Education and Social Development. The Keiskamma Trust, the Raphael Centre, and Small Projects Foundation helped to design and conceptualise the study. Mzantsi Wakho is supported by the Nuffield Foundation under Grant CPF/41513, the International AIDS Society through CIPHER grant (155-Hod); Evidence for HIV Prevention in Southern Africa (MM/EHPSA/UCT/05150014); Johnson and Johnson, the John Fell Fund (103/757), and South Africa’s National Research Foundation. Additional support for LC was provided by the European Research Council (ERC) under the European Union’s Seventh Framework Programme (FP7/2007–2013)/ERC grant agreement n8313421, and the Leverhulme Trust (PLP-2014-095). The project also received ESRC Impact Acceleration Account Support. We thank adolescents, their families and their health and social service providers, and acknowledge the crucial support of the Mzantsi Wakho and PATA teams.
References: 1. Nachega, J.B., et al., Antiretroviral therapy adherence, virologic and immunologic outcomes in adolescents compared
with adults in southern Africa. Journal of Acquired Immune Deficiency Syndromes, 2009;51(1): p. 65-71.2. Delany-Moretlwe S, Cowan FM, Busza J, Bolton-Moore C, Kelley K, Fairlie L. Providing comprehensive health services
for young key populations: needs, barriers and gaps. Journal of the International AIDS Society. 2015;18:19833.Hudelson C, Cluver L. Factors associated with adherence to antiretroviral therapy among adolescents living with HIV/AIDS in low- and middle-income countries: a systematic review. AIDS Care. 2015;27(7):805-816. Merten S, Kenter E, McKenzie O, Musheke M, Ntalasha H, Martin-Hilber A. Patient-reported barriers and drivers of adherence to antiretrovirals in sub-Saharan Africa: A meta-ethnography. Tropical Medicine & International Health. 2010;15:16-33.
Kim MH, Mazenga AC, Yu X, et al. High self-reported non-adherence to antiretroviral therapy amongst adolescents living with HIV in Malawi: barriers and associated factors. Journal of the International AIDS Society. 2017;20(1):21437. For further information:
Paediatric-Adolescent Treatment AfricaTelephone: +27 21 447 9566Email: [email protected]
Learn more here:
Background• Adherence to antiretroviral treatment (ART) is one of the greatest healthcare challenges
facing HIV-positive adolescents.
• In Southern Africa, adolescents have poorer ART adherence than adults, with associated lower rates of viral suppression and immune-recovery, and higher rates of HIV-related mortality and morbidity.1
• A growing literature documents socio-structural and clinical factors associated with ART non-adherence among adolescents.2
• Comparably little research has been conducted on how adolescents themselves understand non-adherence, and how their understandings differ from adult caregivers and healthcare providers.
Methods• This research combines the qualitative dataset of the Mzantsi Wakho study and operational
research by Paediatric-Adolescent Treatment for Africa (PATA).
• Mzantsi Wakho is the largest longitudinal, community-traced study of ART adherence among adolescents living with HIV (n=1057).
• Alongside a multi-wave quantitative survey (2013 – 2018), qualitative research was conducted with adolescents, their friends, families, and healthcare providers. In-depth interviews, focus groups, participatory research exercises, and over 2000 hours of observations in clinics, homes, play areas, and support groups constitute the qualitative dataset for this study.
Figure 1: A timeline of the The Mzantsi Wakho study, which has combined qualitative, quantitative and participatory research methods from 2013 - 2018
Mzantsi WakhoTelephone: +27 43 721 1716/+27 21 650 4656Email: [email protected]
AngolaBotswanaBurkina FasoBurundiCameroonCote d'IvoireDRCEthiopiaGhanaKenyaLesothoMalawiMozambiqueNamibiaNigeriaRepublic of CongoRwandaSouth AfricaSwazilandTanzaniaTogoUgandaZambiaZimbabwe
Figure 2: The PATA Network- 2018
45%
37%
27%
17%
12% Non-adherence and loss to follow-up
Stigma, discrimination and peer pressure
Non-disclosure
Insufficient caregiver support
No dedicated space
Conclusion• ART non-adherence is a major cause of HIV-related mortality and morbidity among
adolescents.
• In identifying and monitoring poor adherence to ART, terms such as ‘non-adherent’ or ‘defaulting’ are used widely by healthcare workers and adult caregivers of HIV-positive adolescents. But adolescents themselves do not use or identify with these terms.
• Adolescents typically report adhering well to ART, seeking to maintain adults’ impressions that they are reliable, responsible and obedient. When asked in greater depth about the challenges of accessing and remaining within care, adolescents’ accounts of non-adherence may surface.
• To improve adolescent ART-related outcomes, it is crucial to address the disjuncture between adolescents’, caregivers’ and healthcare provider’s understandings of non-adherence.
Further reading:Bernays S, Paparini S, Seeley J, Rhodes T. “Not Taking it Will Just be Like a Sin”: Young People Living with HIV and the Stigmatization of Less-Than-Perfect Adherence to Antiretroviral Therapy. Medical Anthropology. 2017;36(5):485-499.Cluver LD, Hodes RJ, Sherr L, et al. Social protection: potential for improving HIV outcomes among adolescents. Journal of the International AIDS Society. 2015;18:20260.
PATA acknowledges its collaboration with Mzantsi Wakho and its partners that support its work across several PATA programmes, these partners include the ELMA Foundation, M.A.C. AIDS Fund, Positive Action Children’s and Adolescent Fund, Aidsfonds and the Robert Carr Fund for civil society networks, the International AIDS Consortium Network and the Government of the Netherlands. Thank you to all frontline health providers and peer supporters across the PATA network for their ongoing efforts in improving access and quality services for children and young people living with HIV.
Cluver L, Toska E, Orkin F, et al. Achieving equity in HIV-treatment outcomes: can social protection improve adolescent ART-adherence in South Africa? AIDS care. 2016;28(sup2):73-82.Hodes R, Price I, Bungane N, Toska E, Cluver L. How front-line healthcare workers respond to stock-outs of essential medicines in the Eastern Cape Province of South Africa. South African Medical Journal. 2017;107(9):738-740.Hodes R, Doubt J, Toska E, Vale B, Zungu N, Cluver L. The stuff that dreams are made of: HIV-positive adolescen’ aspirations for development. Journal of the International AIDS Society. 2018;21:e25057.Toska E, Gittings L, Hodes R, et al. Resourcing resilience: social protection for HIV prevention amongst children and adolescents in Eastern and Southern Africa. African Journal of AIDS Research. 2016;15(2):123-140.Vale B, Hodes R, Cluver L, Thabeng M. Bureaucracies of Blood and Belonging: Documents, HIV-positive Youth and the State in South Africa. Development and Change. 2017;48(6):1287-1309.
• Adolescent ART clinic files and observations of clinic consultations revealed a variety of responses to non-adherence by healthcare workers.
• ‘Positive’ approaches included targeted adherence counselling, referrals to social services, and pleas and cajolements to motivate and inspire better medicines-taking.
• ‘Negative’ approaches included warning patients that health services would be denied to them in the future should their ART-adherence fail to improve, and threats that defaulting would be reported to adult authorities – including family members, senior healthcare workers, and even the police.
Caregiver perspectives: ‘He doesn’t listen’
• Caregivers understood adolescents’ non-adherence as a form of deviance. They compared defaulting to other insubordinate behaviours, such as speaking rudely to elders, or sneaking out of the house at night.
• The mother of a 14-year old boy explained her challenges in overseeing his adherence:
Caregiver: He doesn’t listen. He wants to be reminded all the time… He will come back at night and realize that he forgot to take his pills. He should take them at seven. Seven pm and seven am… He forgets a lot, but its better now.
Interviewer: Does he seem to like them, or does he feel forced?Caregiver: Now he is forced, after he defaulted.
• In accounts of adolescent non-adherence, adult caregivers and healthcare workers oscillated between frustration and bewilderment, concern and care, as they sought a variety of tactics to promote better adherence.
• Their efforts included reprimands and punishments, increased surveillance of pill-taking and physical whereabouts, and attempts to ameliorate the socio-structural and individual circumstances perceived to undermine adherence. This included trying to secure better provision of food and water, and matching medicines-taking to other household routines, such as eating breakfast or brushing teeth.
Adolescents perspectives: ‘I drink them now’• The terms ‘adherence’, ‘non-adherence’ and ‘defaulting’ were not used by a single
adolescent to describe their medicines-taking within the combined Mzantsi Wakho and PATA datasets.
• When asked outright about their adherence to ART, responses were mostly curt and formulaic. This excerpt from an interview with a 17-year old girl (Eastern Cape, November 2014), is typical of these exchanges:
Interviewer: How are your pills treating you?Participant: Good, because they make me strong.Interviewer: So you like them?Participant: Ya.Interviewer: Oh, and did your doctor tell you if your CD4 count is good or bad?Participant: They told me my CD4 count is good now.Interviewer: Now? Was it bad before?Participant: Bad.Interviewer: Why?Participant: I did not take my pills.Interviewer: Why?Participant: I would forget, like after I ate I would go to sleep.Interviewer: Do they make you sleepy or keep you awake?Participant: They keep me awake.Interviewer: And you just want to sleep?Participant: Yes.Interviewer: So now?Participant: I drink them now.
• Within qualitative interviews, adolescents’ admissions of non-adherence were embedded within descriptions of broader challenges in accessing or remaining in care, such as the cost of transport to clinics, stock-outs of medicines, or the fear of being ‘outed’ as HIV-positive.
• In some instances, adolescents made veiled references to defaulting through accounts of improved compliance in the present, and of the preferred palatability or lighter pill burden of a current regimen, in contradistinction to a previous regimen that had ‘failed’.