Embed Size (px)
DESCRIPTION
Citation preview

Adherence to HIV Medications: An Evidence-Based Review
Christopher Behrens, MD
Northwest AIDS Education & Training Center
University of Washington

Adherence
”[physicians] should keep aware of the fact that patients often lie when they state that they have
taken certain medicines." - Hippocrates
“Drugs don’t work if people don’t take them.” - C. Everett Koop

Adherence and Antiretroviral Therapy
• Measuring Adherence
• Why Adherence Matters– antiretroviral efficacy– development of resistance
• Factors associated with adherence
• Interventions to improve adherence

How do we Measure Adherence?
• Provider Estimates
• Patient self-report
• Diaries
• Pill Count
• Laboratory Markers
• Electronic Devices

Current DHHS guidelines on Initiation of Antiretroviral Therapy
– “The likelihood of patient adherence should be discussed and determined by the individual patient and clinician before therapy is initiated.”
– “Before the first prescription is written, patient ‘readiness’ to take medication should be clearly established”
August 2001 Guidelines for the Use of Antiretroviral Agents in HIV-Infected Adults and Adolescents

Clinicians’ Estimates of Adherence Not Much Better Than Random
Bangsberg 2001 JAIDS HAARTPaterson 2000 Annals Int Med HAARTHaubrich1999 AIDS HAARTSteiner 1995 Arch Int Med AZTBosely 1995 Eur Resp J Inhaled terbutalineCharney 1967 Pediatrics PenicillinCaron 1978 Clin Pharmacol AnatacidsGilbert 1980 Can Med Assoc J DigoxinBlowey 1997 Ped Nephrology CyclosporinMushlin 1977 Arch Int Med Hypertensive

Provider Estimate vs.Three 3-Day Patient Report Compared to Pill Count
Three 3-day Self Report and Pill Count Adherence
Pill Count
100806040200
Pat
ient
Rep
ort
100
80
60
40
20
0
Provider Estimate and Pill Count Adherence
Pill Count
100806040200
Pro
vide
r E
stim
ate
100
80
60
40
20
0
Provider EstimateR sq = 0.26
Patient ReportR sq = 0.72
Bangsberg et al JAIDS 2001:26:435
n=45

Measuring Adherence: Patient Self-Report
• patients tend to report what they think the provider wants to hear1
• patients are unlikely to misrepresent high levels of adherence3 - hence, patient-reported poor adherence is specific but not sensitive
• patient-reported adherence tends to exceed adherence by more objective measurements, such as pill count or electronic monitoring2
1. DiMatteo MR, DiNicola DD, eds. Achieving Patient Compliance. New York: Pergamon Press; 1982:1-28.
2. Golin C et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago. Abstract 95.
3. Bond W, Hussar DA, Am J Public Health 1991;81:1978-1988.

How Do Adherence Measurement Techniques Compare to One Another?
0102030405060708090
100
Self-Report ClinicianEstimate
Pill Count Electronicbottle cap
ADEPT Study; N=81 patients
Adapted from Golin C et al. 1999; Miller L et al. 1999.
Adh
eren
ce, %

Measuring Adherence: Patient Self-Report
• Nevertheless, studies have documented an association between patient-reported adherence and viral outcome1-3
• patient-reported adherence may be a useful tool to evaluate adherence at a group level but not so much on an individual level
1. Bangsberg DR, et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago. Abstract 93.2. Duong M, et al. 39th ICAAC; 1999; San Francisco. Abstract 20693. Demasi R, et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago. Abstract 94.

Measuring Adherence: Diaries
• In theory, better than relying on memory
• in practice, not very useful– many patients do not fill them in1
– those that do may do so immediately before office visit
1. Golin C, et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago. Abstract 95.

Measuring Adherence: Pill Counts
• Advantages:– more objective than
patient report
– correlates better with electronic bottle caps than does self-reported adherence1
1. Golin C, et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago. Abstract 95
• Drawbacks:– many patients forget to
bring their bottles
– patients can still exaggerate adherence
– time consuming
– patients may find it too paternalistic
– does not reveal patterns of missed doses

Measuring Adherence: Laboratory Markers
• many antiretroviral agents associated with changes in laboratory parameters– AZT, d4T produce macrocytosis– indinavir associated with hyperbilirubinemia– didanosine changes urinary uric acid levels
• drug levels could also potentially be used to monitor adherence

Laboratory Markers to Assess Adherence: Drawbacks
• lab markers not highly sensitive nor specific
• do not give any information regarding the pattern of non-adherence
• patients who take their medications immediately before having blood levels drawn could exaggerate their adherence
• measurement of drug levels has not been standardized
• other factors besides adherence can affect drug levels

Measuring Adherence: Electronic Bottle Caps
• caps harbor chips that register each time a bottle is opened or closed
MEMScaps, Aardex Corp.

QuickRead software, for use with MEMScaps system
http://www.aardex.ch/QRCalendar.htm

http://www.aardex.ch/QRChronology.htm
QuickRead software, for use with MEMScaps system

Measuring Adherence: Electronic Bottle Caps
• Advantages– more difficult for
patients to exaggerate their adherence
– reveals patterns of non-adherence
– studies using these devices have documented relationship between adherence & dosing
• Disadvantages– too expensive for
routine use outside of research studies
– cannot be used for patients who use pillboxes

The Future of Adherence Assessment? Computer-Assisted Self-Interviewing (CASI)
• Advantages of CASI– Privacy may improve disclosure
– Visual ARV recognition
– Standardizes adherence assessment
– Not personnel intensive
– Could be administered in waiting room or at home via the webBangsberg D et al. AIDS Care, 2002 (in press)
• Purposes of CASI– Determine patient’s understanding of medication regimen– Determine patient’s adherence over 3-day period
http://www.edermpda.com/hivadhere/

Printed with permission from West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Printed with permission from
West Portal Software Corp.

Pilot CASI Adherence Measurement
• 111 patients, 11 providers in study
• over 50% of patients made at least one error in describing their regimen
• providers missed 76% of non-adherent patients• patients’ reports of adherence significantly
associated with viral load counts• 65% of patients reported that CASI made them
think more about how they take their medications
Bangsberg, Bronstone & Hoffman AIDS Care 2002 (in press)

Why is Adherence so Important for Antiretroviral Therapy?
I. Efficacy
II. Resistance

Virologic Control falls sharply with diminished adherence
0
10
20
30
40
50
60
70
80
90
95-100% 90-95% 80-90% 70-80% < 70%
Adherence, by prescription refill
% A
chie
ving
<50
0 co
pies
/mL
N = 504 pts on HAART
Montessori, V, et al. XII International Conference on AIDS, Durban, South Africa, 2000. Abstract MoPpD1056.

0
20
40
60
80
100
>95 90-95 80–90 70-80 <70
Pat
ient
s w
ith
HIV
RN
A<
400
cop
ies/
mL
, %
PI adherence, % (electronic bottle caps)
Paterson, et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago, IL. Abstract 92.
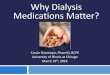
Virologic Control falls sharply with diminished adherence

10% Adherence difference = 21% reduction in risk of AIDSAdherence and AIDS-Free Survival
Bangsberg D, et al. AIDS. 2001:15:1181
Pro
port
ion
AID
S-F
ree
Months from entry
P = .0012
0 5 10 15 20 25 30
0.00
0.25
0.50
0.75
1.00
AdherenceO 90–100%O 50–89%O 0–49%

Adherence & Drug Resistance
• HIV Reverse Transcriptase (RT) is error-prone
• on average, HIV RT generates one mutation in each copy of HIV produced
• billions of HIV virions produced daily in untreated patients
• some HIV mutations associated with drug resistance

Sub-Optimal Adherence Predisposes to Resistance
• Sub-optimal adherence ==> sub-therapeutic drug levels ==> incomplete viral suppression ==> generation of resistant HIV strains by selection for mutant viruses
• association between poor adherence and antiretroviral resistance well-documented1,2
1. Vanhove G, et al. JAMA. 1996;276:1955-1956.2. Montaner JS, et al. JAMA. 1998;279:930-937.

What Contributes to Sub-Optimal Adherence?

Reasons for Non-Adherence: Clinician vs Patient Views
0
10
20
30
40
50
60
valu
e, %
No. of doses orpills
Side Effects Meal Instructions Schedulecomplexity
Other
ClinicanPatient
Chesney M. Adherence to antiretroviral therapy. 12th World AIDS Conference, 1998; Geneva. Lecture 281

Predictors of Poor Adherence
• active alcohol1 or substance2 abuse
• work outside the home for pay1
• depressed mood1
• lack of perceived efficacy of HAART3
• lack of advanced disease4
• concern over side effects4
1. Chesney MA. 37th ICAAC, 1997; Toronto. Abstract 281. 2. Cheever LW, Curr Infect Dis Rep 1999 Oct;1(4):401-407.3. Horne R, et al. 39th ICAAC, 1999; San Francisco. Abstract 588. 4. Wenger N, et al. 6th Conference on Retroviruses and Opportunistic Infections, 1999; Chicago. Abstract 98.

Predictors of Poor Adherence, continued
• non-caucasian race documented in some studies1-
3 but not others5
– association of race with adherence not found in other disease states
– lower literacy rate a confounder?4
1. Paterson, et al. 6th Conference on Retroviruses and Opportunistic Infections, 1999; Chicago, IL. Abstract 92.2. Wenger N, et al. 6th Conference on Retroviruses and Opportunistic Infections, 1999; Chicago, IL. Abstract 98.3. Mar-Tang M, et al. J Gen Intern Med. 1999;14(suppl 2):53. 4. Kalichman SC, et al. J Gen Intern Med. 1999;14:267-273.5. Stone VE, et al. JAIDS 2001; 28:124-131

Predictors of Poor Adherence, continued
• inability to fit medications into daily schedule
• tid dosing, food requirements1
1. Stone VE, et al. JAIDS 2001; 28:124-131

Other Considerations
• a large proportion of patients incorrectly recall their medication schedules1,2
• Virologic control does not necessarily imply high levels of adherence3
– patients with virologic control despite poor adherence may not maintain durable viral suppression without improved adherence
1. Chesney MA, International AIDS Society USA Meeting, 1998; Los Angeles.
2. Kravitz RL, et al. Arch Intern Med. 1993;153:1869-1878.
3. Kaplan A, et al. 6th Conference on Retro-viruses and Opportunistic Infections; 1999; Chicago. Abstract 96.

Factors Associated with Higher Levels of Adherence
• twice-daily or once-daily regimens1,4
• belief in own ability to adhere to regimen1
• not living alone2
• dependent on a significant other for support2
• history of Opportunistic Infection or Advanced HIV disease3
1. Eldred L, et al, J Acquir Immune Defic Syndr Hum Retrovirol 1998;18:117-125.
2. Morse EV et al, Soc Sci Med 1991;32:1161-1167. 3. Singh N, et al, AIDS Care 1996;8:261-269. 4. Stone VE, et al. JAIDS 2001; 28:124-131

Factors Associated with Higher Levels of Adherence
• Belief in efficacy of antiretroviral therapy
• Belief that non-adherence will lead to viral resistance
Wenger N, et al. 6th Conference on Retroviruses and Opportunistic Infections, 1999; Chicago. Abstract 98.

Interventions Shown to Improve Adherence to Antiretrovirals
• medication alarms1
• education & counseling sessions2,3
• Directly Observed Therapy (DOT)4,5
1. Samet JH, et al. Am J Med. 1992;92:495-502. 2. Malow RW, et al. Alcohol Drug Abuse 1998;49:1021-4.3. Tuldra A, et al. 39th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1999; Abstract 595.4. Sorensen JL, et al. AIDS Care. 1998;10:297-312. 5. Wall TL, et al. Drug Alcohol Depend. 1995;37:261-269.

Self-Adminstered vs Directly Observed Therapy During Incarceration
0
102030405060708090
100
% w
ith
VL
< 5
0 co
pies
/mL
w4 w8 w16 w24 w48 w64 w72 w80 w88
DOT <50
SAT <50
Fischl et al 8th CROI, 2001 abstract 528
p < 0.01
N = 50 in each group

Interventions to Improve Adherence: Lessons from Other Disease States
• addressing multiple factors most effective
• education
• behavioral support from other members of the health care team
Miller et al., The AIDS Reader 10(3):177-185, 2000.

Putting it all Together
Practical Strategies to Improve Adherence

Improving Adherence: before Initiation of Therapy
Assess how medications fit into patient's lifestyle
Consider adherence trial with jelly beans to mesh pill taking with daily schedule
Make contingency plans for pill taking during weekends, holidays, or other changes in routine
Assess adherence and barriers to adherence in a nonjudgmental manner
Adapted from: Miller et al., The AIDS Reader 10(3):177-185, 2000.

Improving Adherence: before Initiation of Therapy
Assess patient's understanding and acceptance of the regimens
Determine other medical barriers to adherence
Manage or refer for management of adherence-limiting co-morbid conditions
Adapted from: Miller et al., The AIDS Reader 10(3):177-185, 2000.

Improving Adherence: before Initiation of Therapy
• Try to use simple regimens– bid or better– avoid food requirements if possible
• Clear & simple instructions
• Negotiated treatment plan

Improving Adherence: After Initiation of Therapy
• Close follow-up
• Ask patient to verbalize treatment regimen
• Education about adherence– re-emphasize importance of adherence at each
visit, even in patients with good virologic control
– review incidence & management of adverse effects often

Improving Adherence: After Initiation of Therapy
• consider cues to remind patients of dosing
• other reminders: alarms, watches, pagers
• consider recruiting family/friends as support
• referral to community support groups
• involve other members of the health care team
• formal recognition of adherence as a job responsibility
Adapted from: Miller et al., The AIDS Reader 10(3):177-185, 2000.

Should Public Health Concerns about HIV Resistance Influence
Prescribing Practices?


DHS/HIV/Resistance /PP
Are Non-Adherent Patients Responsible for Rising Levels of Antiretroviral Resistance?
2
1
7
2
6
0
2
4
6
8
10
Res
ista
nt
Iso
late
s %
NRTI NNRTI PI
1996-1998
1999-2000
3
From: Little SJ. JAMA 1999;282:1142-9.Little SJ. 8th Conf Retrovirus. Abstract 756
N = 108 PatientsNewly HIV-Infected Phenotypic Data: 10-fold Resistance

Adherence and Viral Load Suppression10% adherence difference : 0.33 log VL difference
Pill count percent adherence
Bangsberg D, et al. AIDS. 2000:14:357
Log
10 H
IV R
NA
cop
y nu
mbe
rs7
0
1
2
3
4
5
6
0 10 20 30 40 50 60 70 80 90 100

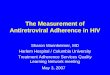
High Levels of Adherence are Required to Generate Antiretroviral Resistance
Pill count percent adherence
Log
10 H
IV R
NA
cop
y nu
mbe
rs7
0
1
2
3
4
5
6
0 10 20 30 40 50 60 70 80 90 100
Resistant*Sensitive
*Primary Drug Resistant Mutation IAS-USA
Bangsberg D, et al. AIDS. 2000:14:357

Discontinuation of HAART Leads to Rapid Decline in Resistant Strains of HIV
SG Deeks et al NEJM 344:472-480

Adherence, Antiviral Activity & Risk of Resistance Mutations
Incr
easi
ng p
roba
bili
tyof
sel
ecti
ng m
utat
ion
Increasing Adherence
Low Risk of Resistance:Inadequate Drug Pressureto Sustain Poorly Fit Virus
Low
Risk
of Resistan
ce:C
omp
lete Viral
Su
pp
ressionHigh Risk of
Resistance:Drug
PressureSustains
Replication of Poorly Fit Virus

Hypothesis
• Prescribing HIV antiretroviral therapy to patients with marginal adherence will not accelerate the rise in population levels of drug resistance
– Nonadherence is associated with insufficient drug pressure to select or sustain resistant virus
– It is the patients with higher levels of adherence that may be generating resistant strains

Counseling Your Patients about Adherence
An Illustrative Cartoon

How Resistance Develops to HIV
This is the virus known as HIV.
The only thing that matters to him
in his short, nasty life is to destroy
T-Cells. To do this, he must
somehow get over this wall.
The wall is created by taking anti-
HIV medications. When the
medicines are taken correctly, the
virus is unable to climb over the
wall to get to your T-cells

Sometimes the Wall Comes Down
When you forget to take your evening dose, or only take 2 of your anti-HIV medicines, the strong wall comes down
The virus breaks free and is able to get over the wall.
When he gets to the other side, he discovers a way to get over the wall in the future. This is called resistance. He finds a spring that will give him a little more bounce.

The Wall Goes Back Up
When you start taking the
medicine regularly again, the
wall goes back up.
Sometimes,it’s too late and the
virus uses the spring to jump
over the wall. At this point, it is
a resistant virus The drugs may
not be able to keep the wall
high enough to stop the
springing virus.

Lessons to Be Learned
It is better to not take anti-HIV drugs at all than to
take them only some of the time.
If you think you may be missing doses often,
please tell your health care provider or
pharmacist! We promise not to tell your mother.