Embed Size (px)
Citation preview

Rapid Assessment and Treatment of Patients with Acute Decompensated Heart Failure (ADHF)
Nani Hersunarti
Department of Cardiology and Vascular Medicine
Faculty of Medicine, University of Indonesia
Harapan Kita National Cardiac Center

Improve patient hemodynamic status in order to relief symptoms and stabilize organ function– Reduce fluid volume and filling
pressures of the heart– Reduce systemic vascular resistance
(SVR)– Increase cardiac output (CO) – Reduce neurohormones
Therapeutic Goals in ADHF

Therapeutic Goal Parameters
in ADHF
SBP > 80 mm HgNo orthopneaNo peripheral
edemaNo hepatomegaly
or ascitesJVP < 8 cmWarm extremities
SBP > 80 mm Hg PCWP < 15 mm HgRAP < 8 mm HgSVRI < 1200 dyne-
s-cm-5
ClinicalHemodynamic

Oxygenation and ventilatory assist.
– The first priority in ADHF treatment is adequate cellular oxygenation to prevent organ target dysfunction.
– Oxygen saturation is maintained 95-98%.• Airway Patency• Oksigen supply ; Nasal or Mask or CPAP or
non-invasive positive pressure ventilation (NIPPV).
• Ventilator support in case of respiratory failure
ESC guidelines Acute Heart Failure, 2005

Pharmacologic option in ADHF
Diuretics Vasodilators Inotropes
Reducefluid
volume
Decreasepreload
andafterload
Augmentcontractility
Vasodilate; reduce fluid
volume;counteract RAAS/SNS
Natriuretic peptides
RAAS = renin-angiotensin-aldosterone system; SNS = sympathetic nervous system

Ideal Agent for ADHF
• Vasodilator (venous and arterial)• Rapidly decreases ventricular filling
pressures• Rapidly decreases symptoms of
congestion • Does not increase heart rate or directly
increase contractility (decreases myocardial oxygen demand)
• Not proarrhythmic
Fonarow GC. Rev Cardiovasc Med. 2001;2(suppl 2):S7

• Does not induce tachyphylaxis (tolerance)
• Provides neurohormonal suppression
• Promotes diuresis / natriuresis
• Conveniently dosed (can be used with or without pulmonary artery catheterization)
• Able to give in a less monitored setting
Ideal Agent for ADHF
Fonarow GC. Rev Cardiovasc Med. 2001;2(suppl 2):S7

A
L C
B
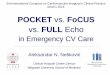
Congestion at rest
Yes
Yes
No
NoWarm & dry
Cold & WetCold & dry
Warm & wet
Low
perf
usi
on a
t re
st
Sign of low perfusion:
Narrow pulse pressure,cool extremities,sleepy, suspect from ACEI hypotension, low Na, renal worsening
Sign of congestion:
Orthopnea,elevated JVP,edema,pulsatile hepatomegaly, asites, rales,louder S3,P2 radiation left ward, abdomino-jugular reflex, valsava square wave
European Heart Journal of Heart Failure,2005; 7:323-331
Two Minutes Assessment of Two Minutes Assessment of Haemodynamic ProfileHaemodynamic Profile

Patient Treatment Selection
Fonarow GC. Rev Cardiovasc Med. 2001;2(suppl 2):S7–S12.
Congestion at Rest
Lowperfusi
onat Rest
YesNo
Warm & DryPCWP normal
CI normal (compensated)
Cold & WetPCWP elevatedCI decreased
Cold & DryPCWP low/normal
CI decreased
Inotropic DrugsDobutamine
Milrinone
Normal SVR High SVR
No
Yes
Warm & WetPCWP elevated
CI normal MOST PATIENTS
VasodilatorsNitroprussideNitroglycerin
or
Natriuretic Peptides

Acute Heart Failure with Systolic Dysfunction
Oxygen/CPAPFurosemide + vasodilator
Clinical evaluation (leading to mechanistic therapy)
SBP > 100 mmHg SBP 85-100 mmHg SBP <85 mmHg
Vasodilator(NTG, nitroprusside, BNP)
Vasodilator and/orInotropic (dobutamin
PDEI or Levosimendan)
Volume loading ?Inotrope and/or
Dopamin > 5mcg/kg/mntAnd/or norepinephrine
Good responseOral therapy
Furosemide, ACE-I
No respon :Reconside mechanistic
therapyInotropic agent ESC, Acute Heart Failure, 2005

Morphine and its analogues
In patient present with restlessness and dyspnoea
Morphine induces • Venodilatalion • Mild arterial dilatation• Reduce heart rate
Dose : 3 mg IV bolus Repeated if required
ESC guidelines Acute Heart Failure, 2005

Diuretics
•For achieving optimal volume status eliminate or minimize congestion•High doses of i.v diuretics 2-3 times daily •More effective with continous i.v.•Combination diuretics•“Resistent diuretics” is a common problem

Inotropes:Dopamine, Dobutamine, Milrinone
• Improve cardiac output by directly increasing cardiac contractility
• Significant proarrhythmic effects• May precipitate ischemia• Not recommended for routine use in
ADHF, but clearly have a role in specific patients

Felker GM. Am Heart J. 2001;142:393–401.
The use of inotropes as a treatment of :
• cardiogenic shock
• diuretic/ACE inhibitor– refractory heart failure decompensations
• a short-term bridge to definitive treatment, such as revascularization or cardiac transplantation, is potentially appropriate
Role of Inotropic Therapy in Patients With Heart Failure

Inotropic AgentIndication :
Peripheral hypoperfusion (hypotension, decrease renal function) with or without congestion
ESC guidelines, Acute Heart Failure, 2005
There is increasing prevalence of i.v. inotropes infusion that Cannot be Cannot be weaned without symptomaticweaned without symptomatic hypotension, recurrent renal dysfunction
!
Dependence on i.v. inotropeDependence on i.v. inotrope can be avoidedcan be avoided with wean infusion in 1-2 weekswean infusion in 1-2 weeks and reduce or discontinuation other medication that decrease discontinuation other medication that decrease blood pressure and renal functionblood pressure and renal function ( Nitrate, Ca++ Channel blocker, NSAID)

Inotropic AgentsDopamine• Is dose dependent and they involve in
three different receptors.
• In low dose (< 2 In low dose (< 2 g/kgBW/min), g/kgBW/min), vasodilatationvasodilatation occurs predominantly in renal, coronary, and cerebral vascular beds.
• However if no response is seen in diuresis the therapy should be terminated (Level of evidence C, class IIb)ESC, Acute Heart Failure, 2005

Inotropic Agents
Dopamine (cont.)• At higher doses (> 2 g/kgBW/min)
stimulates adrenergic and increase in myocardial contractility and cardiac output.
• At doses > 5 g/kgBW/min dopamine will increase peripheral vascular resistance via adrenergic receptors
ESC, Acute Heart Failure, 2005

DobutamineDobutamine
• Clinical action is dose dependent positive inotropic and chronotropic effects.
• In low dose induce arterial vasodilatation and in higher induce arterial vasoconstriction
Inotropic Agents
ESC, Acute Heart Failure, 2005

Phosphodiesterase inhibitors
• Block the breakdown of cyclic AMP into AMP (milrinone, enoximone)
• In advance HF, associated with inotropic, lusitropic, vasodilating effects
• Intermediate between vasodilator and predominant inotrope
Inotropic Agents
ESC, Acute Heart Failure, 2005

Treat the rhythm disturbance
AF or Atrial Flutter;
Cardiovert if possible, or digoxin 0.125-0.25 mg IV or B blocker or amiodarone
ST or SVT;
B bloker when clinically and hemodimanically tolerated - metoprolol 5 mg iv as slow bolus
VF or pulseless VT; Defibrilate 200J
ESC, Acute Heart Failure, 2005

VasodilatorsNitroprusside, Nitroglycerin, Nitrate family
• Work by cGMP mediated smooth muscle relaxation -> vasodilation
• Decrease myocardial work by afterload and preload reduction
• May cause hypotension• May cause headache

• NitratesNitrates
– Not evaluated by large scale studies– Many studies shown their favorable effectLimitationLimitation– Side effect– Nitrate ResistanceNitrate Resistance– Nitrate ToleranceNitrate Tolerance
Prevention• Intermittent dosing : 12 hour nitrate free
interval• Escalating dose• Concomitant use of hydralazine
Elkayam, The American Journal of Cardiology

DR I
MKRG
S SS
SGLG
FC CS SG
SGQVMK V L R
RH
KPS
Cardiac3
Vetricular relaxation (lusitropy) Antifibrotic ( TGF) Antiremodeling
Hemodynamic1,2
(balanced vasodilation) Veins Arteries Coronary arteries
Neurohumoral2
aldosterone4
endothelin2
norepinephrine5
Renal1,5
Diuresis Natriuresis
1Marcus LS et al. Circulation. 1996;94:3184; 2Zellner C et al. Am J Physiol. 1999;276(3 pt 2):H1049;3Tamura N et al. Proc Natl Acad Sci U S A. 2000;97:4239; 4Abraham WT et al. J Card Fail. 1998;4:37;5Clemens LE et al. J Pharmacol Exp Ther. 1998;287:67
Pharmacologic Actions of hBNP

Nesiritide Dosing and Administration
• IV bolus of 2 mcg/kg followed by a continuous infusion of 0.01 mcg/kg/min.
• Natrecor should not be initiated at a dose above the recommended dose.
• The infusion dose can be increased by 0.005 mcg/kg/min no more frequently than every 3 hours up to a maximum dose of 0.03 mcg/kg/min.
Natrecor Prescribing Information (PI), 2004Natrecor Prescribing Information (PI), 2004

IV Agents for ADHF
Nitroprusside
Nesiritide
Nitroglycerin
Milrinone
Dobutamine
??
Dopamine (ng/kg/min)Low (<3)Mod (3-7)High (7-15)
DiuresisArrhythmiaHRBPPCWPCOTherapy
BP = blood pressure; CO = cardiac output; HR = heart rate; PCWP = pulmonary capillary wedge pressureAdapted from Young JB. Rev Cardiovasc Med. 2001;2(suppl 2):S19-S24.
P0415400

Conclusion
• Rapid assessment and treatment of ADHF could decreased mortality and morbidity rate
• Management strategies including – Ensure oxygenation– Reduce pain– Reduce fluid volume– Reduce preload and or afterload – Increase cardiac output– Identify and treat the cause of CHF

Rapid assessment and prompt treatment result in a good outcome for ADHF patients