Embed Size (px)
Citation preview
Adjuvant and NeoadjuvantChemotherapy
2014 Situation
Dr Alexandre BodmerCentre du SeinHUG Genève
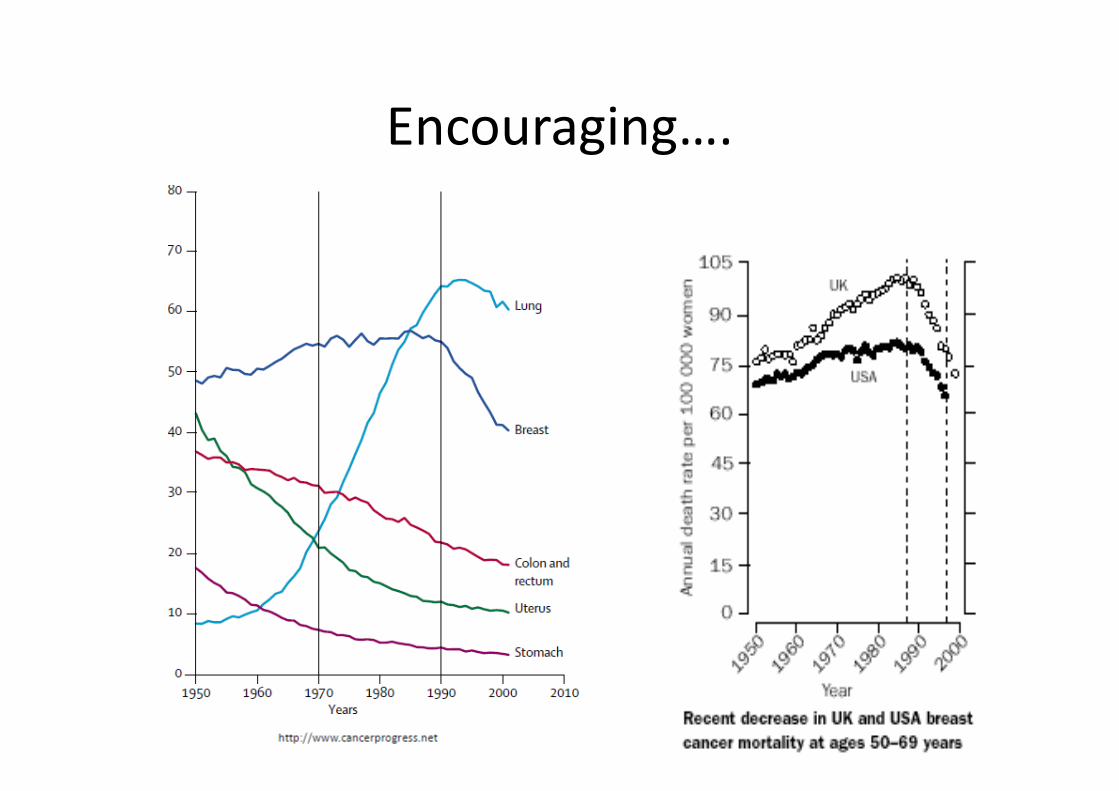
Encouraging….
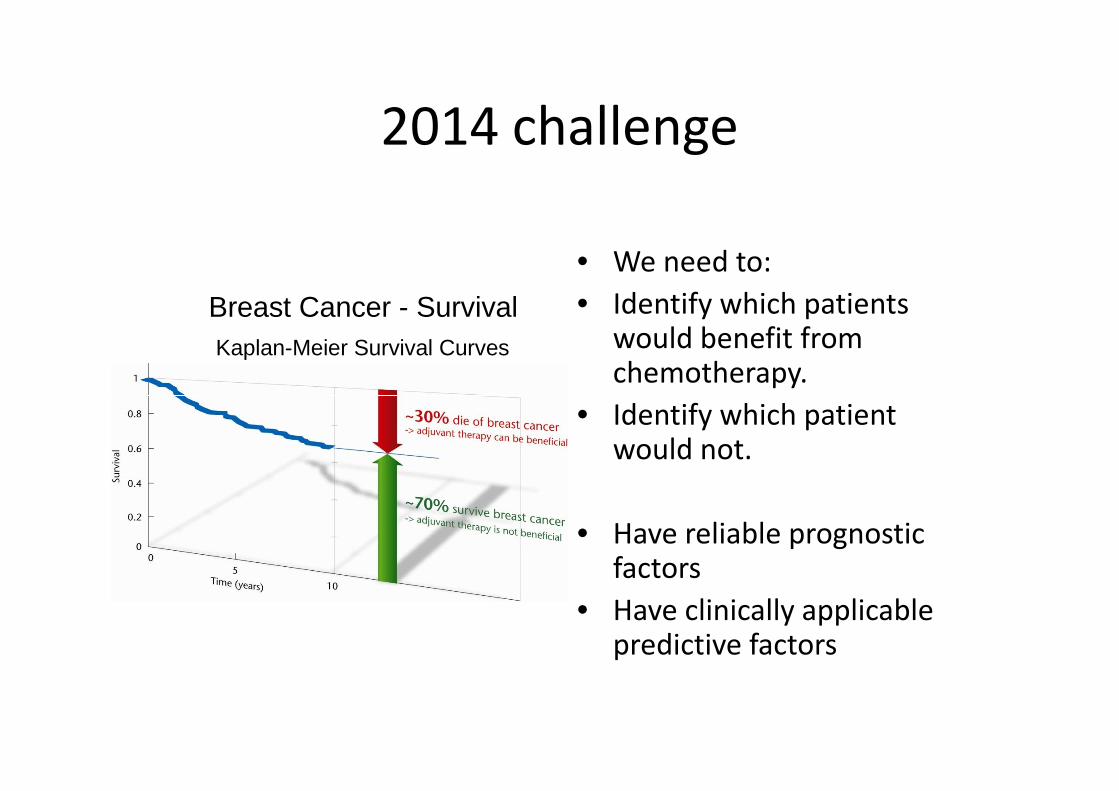
Kaplan-Meier Survival Curves
Breast Cancer - Survival
2014 challenge
• We need to:
• Identify which patientswould benefit fromchemotherapy.
Identify which patient
Which Breast Cancers Return?
• Identify which patientwould not.
• Have reliable prognosticfactors
• Have clinically applicablepredictive factors
Risk assessmentPrognostic and predictive factors
• Tumor size
• Lymph node involvement
• Grade
• Proliferation Markers : Ki 67• Proliferation Markers : Ki 67
• Hormone receptors
• HER2 status
• Gene expression profiles

91% at5 years
80 %at5 years
98% at 5years
84% at 5years
Stage : prognostic factor
63% at5 years
5 years years
58% at 5years
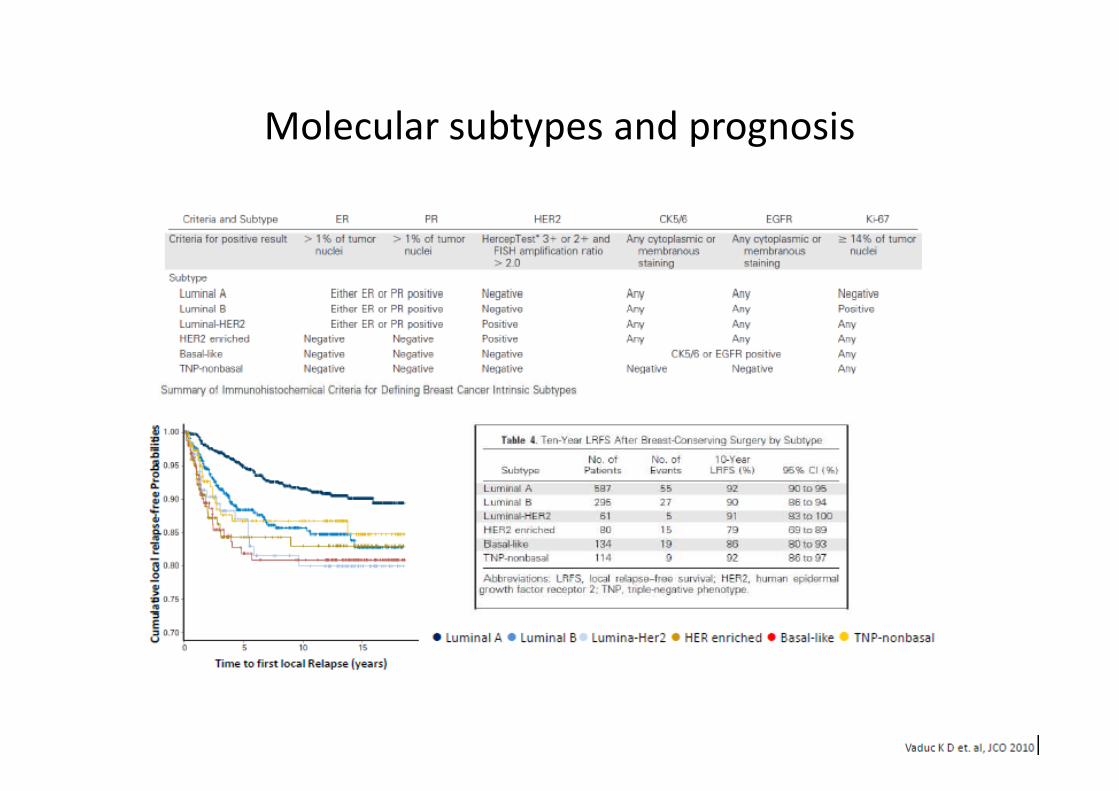
Molecular subtypes and prognosis
How can we do better?
• Better selection of patients for adjuvantchemotherapy
• Treat only those patients who are most likely to recur• Treat only those patients who are most likely to recurand who will therefore benefit most from theaddition of chemotherapy
• Take advantage of genomics
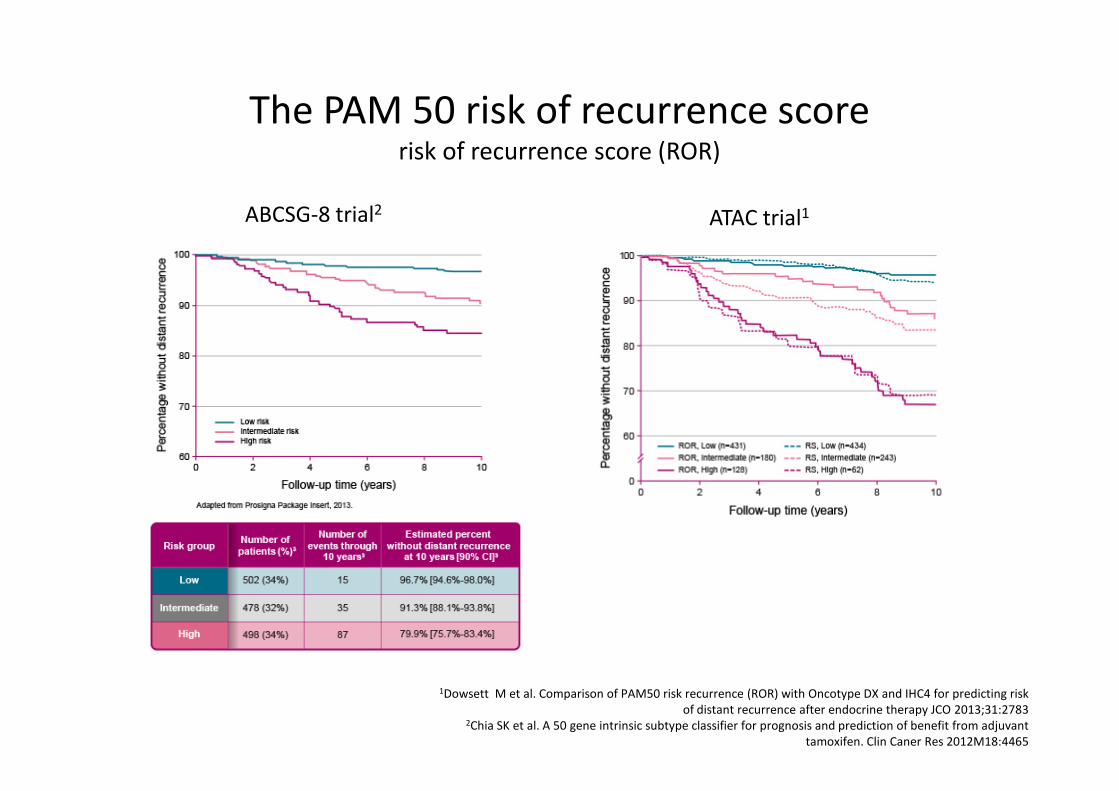
ATAC trial1ABCSG-8 trial2
The PAM 50 risk of recurrence scorerisk of recurrence score (ROR)
1Dowsett M et al. Comparison of PAM50 risk recurrence (ROR) with Oncotype DX and IHC4 for predicting riskof distant recurrence after endocrine therapy JCO 2013;31:2783
2Chia SK et al. A 50 gene intrinsic subtype classifier for prognosis and prediction of benefit from adjuvanttamoxifen. Clin Caner Res 2012M18:4465
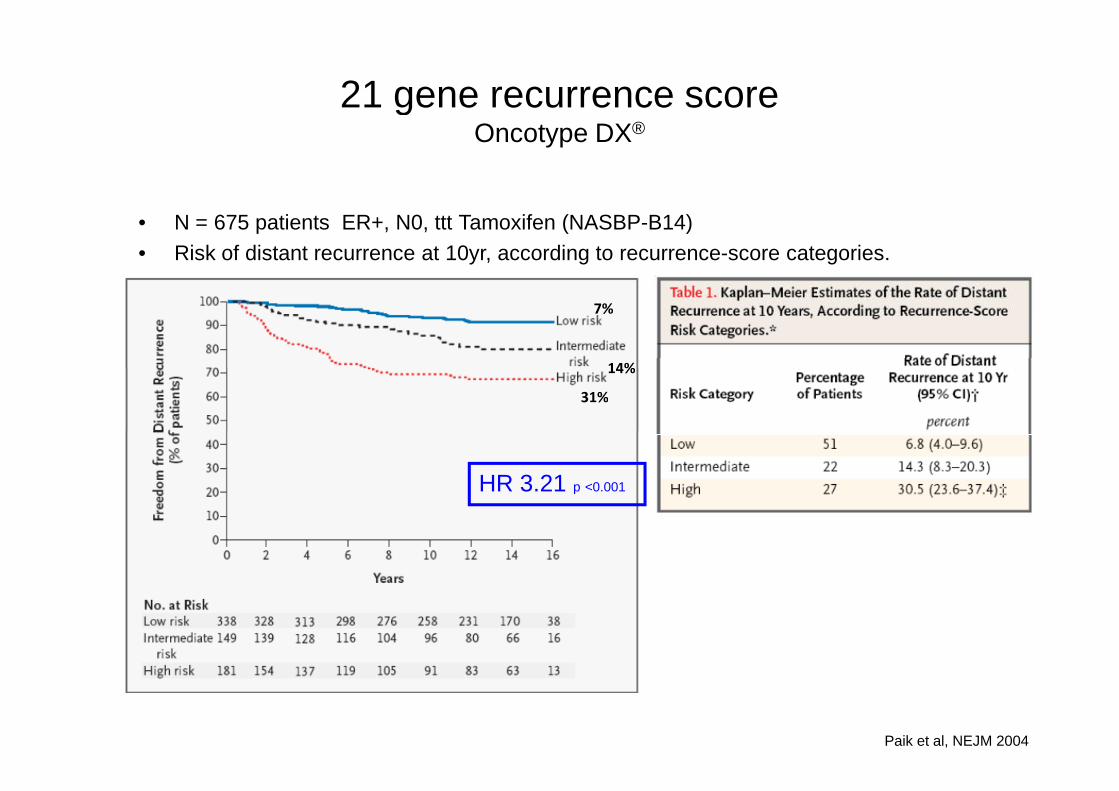
21 gene recurrence scoreOncotype DX®
• N = 675 patients ER+, N0, ttt Tamoxifen (NASBP-B14)
• Risk of distant recurrence at 10yr, according to recurrence-score categories.
7%
14%
31%
HR 3.21 p <0.001
Paik et al, NEJM 2004
31%
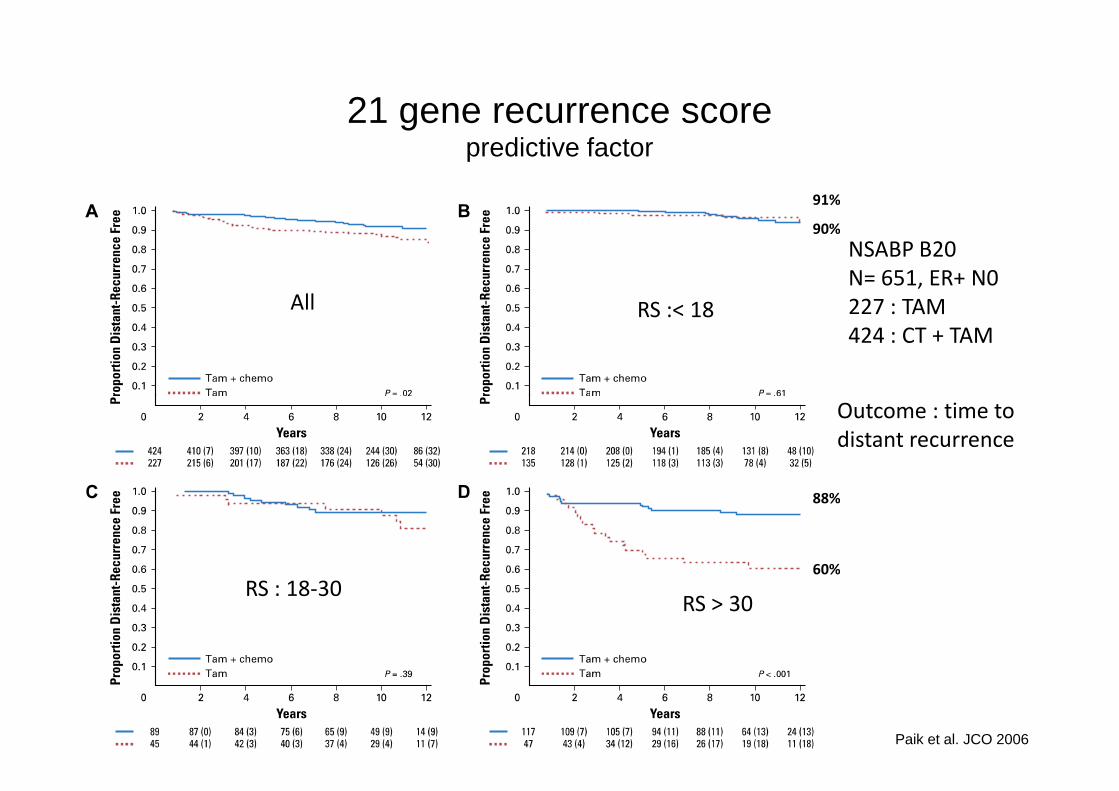
21 gene recurrence scorepredictive factor
NSABP B20N= 651, ER+ N0227 : TAM424 : CT + TAM
All RS :< 18
Outcome : time to
91%
90%
RS : 18-30RS > 30
Outcome : time todistant recurrence
Paik et al. JCO 2006
88%
60%
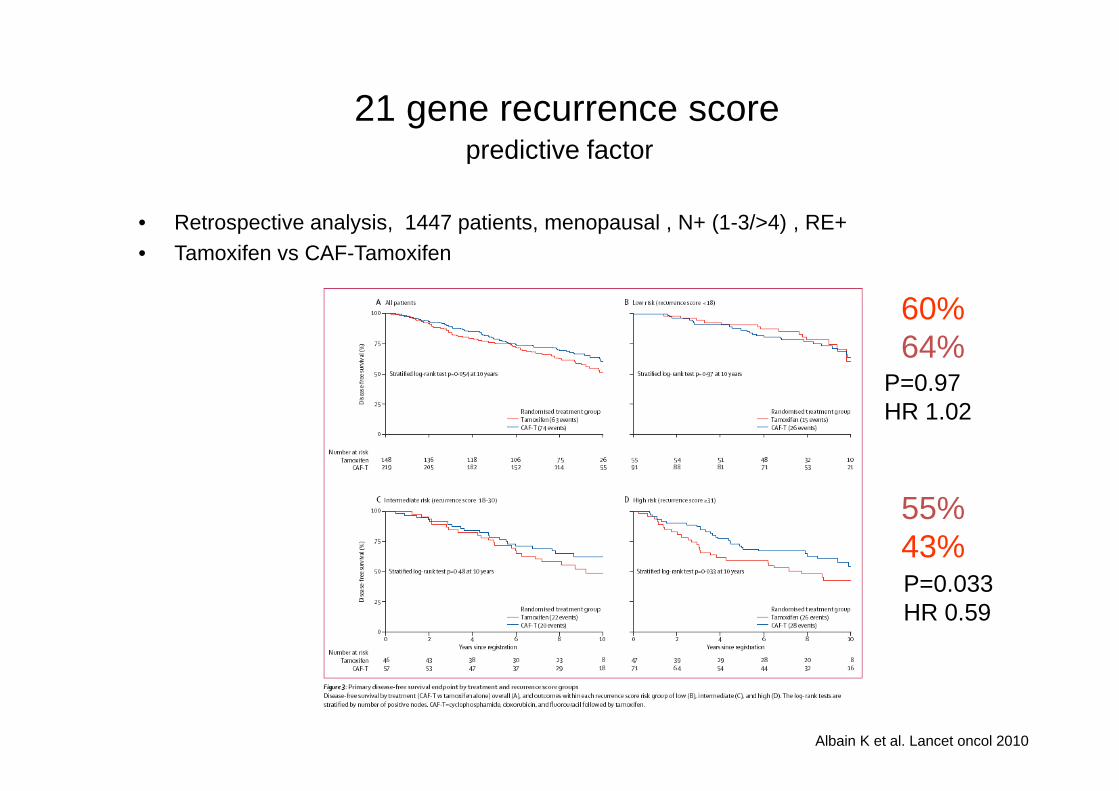
21 gene recurrence scorepredictive factor
• Retrospective analysis, 1447 patients, menopausal , N+ (1-3/>4) , RE+
• Tamoxifen vs CAF-Tamoxifen
60%64%
P=0.97P=0.97HR 1.02
55%43%P=0.033HR 0.59
Albain K et al. Lancet oncol 2010
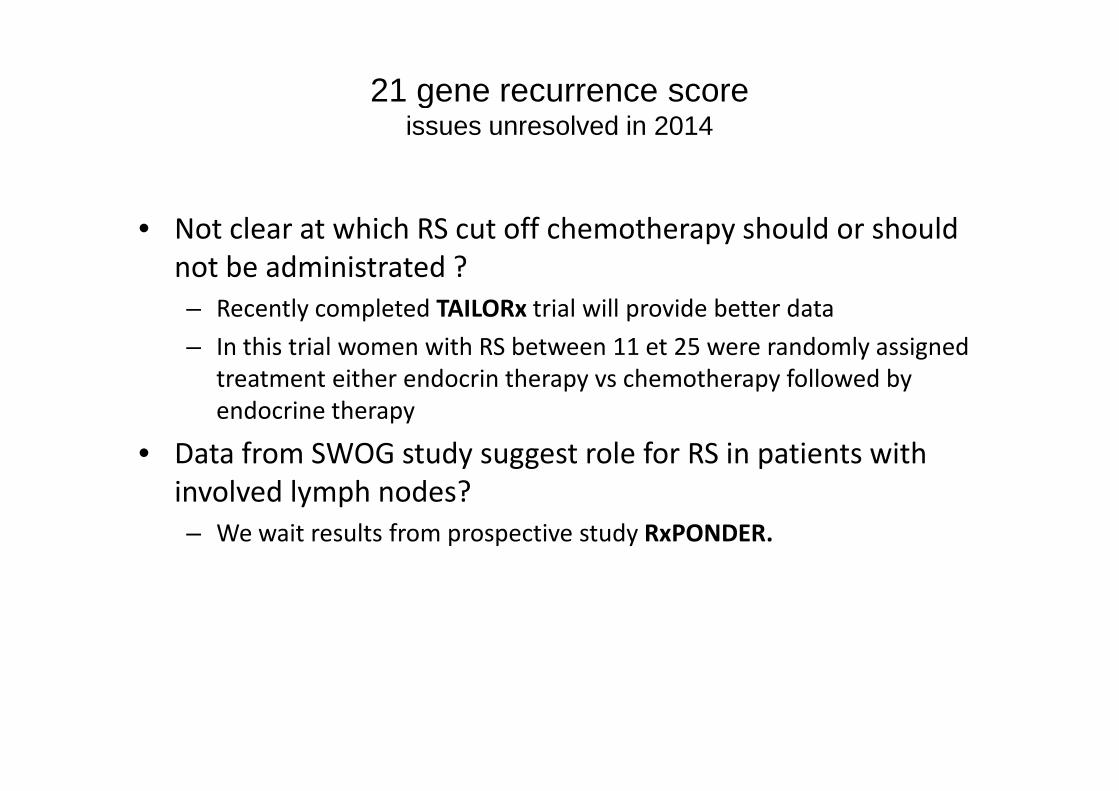
21 gene recurrence scoreissues unresolved in 2014
• Not clear at which RS cut off chemotherapy should or shouldnot be administrated ?– Recently completed TAILORx trial will provide better data
– In this trial women with RS between 11 et 25 were randomly assignedtreatment either endocrin therapy vs chemotherapy followed byendocrine therapyendocrine therapy
• Data from SWOG study suggest role for RS in patients withinvolved lymph nodes?– We wait results from prospective study RxPONDER.
Adjvuant chemotherapy for HR+/- & HER2- BC
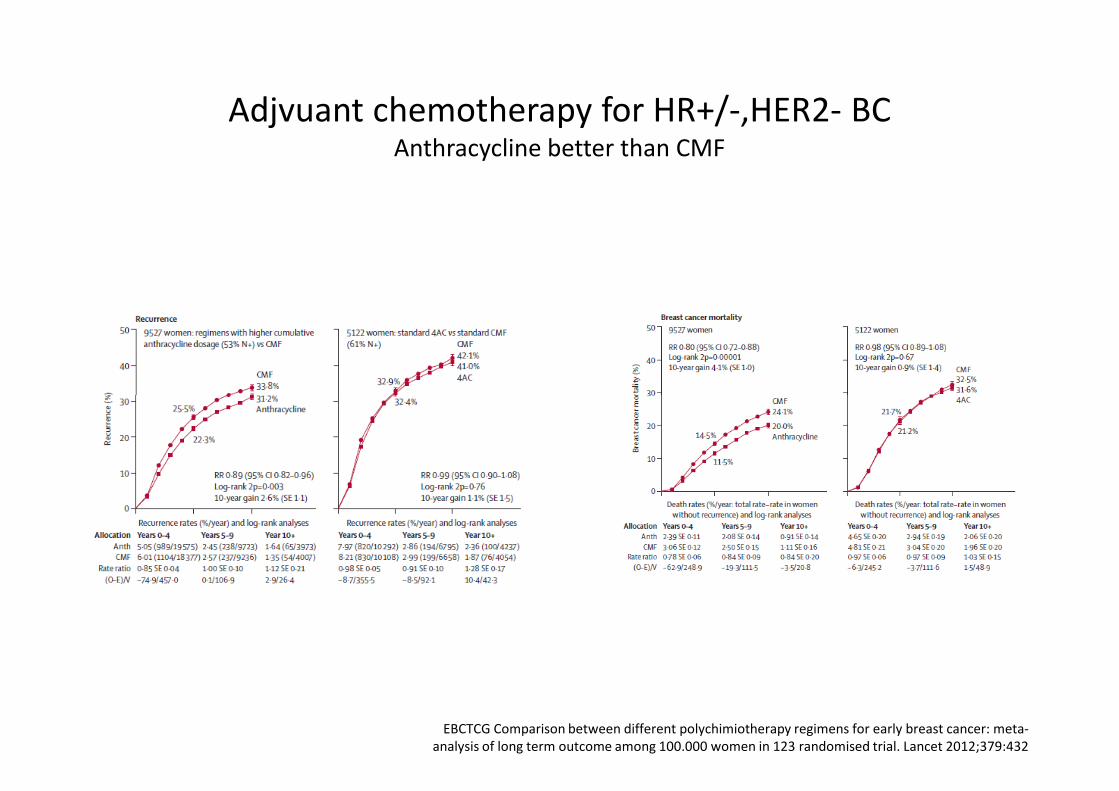
Adjvuant chemotherapy for HR+/-,HER2- BCAnthracycline better than CMF
EBCTCG Comparison between different polychimiotherapy regimens for early breast cancer: meta-analysis of long term outcome among 100.000 women in 123 randomised trial. Lancet 2012;379:432
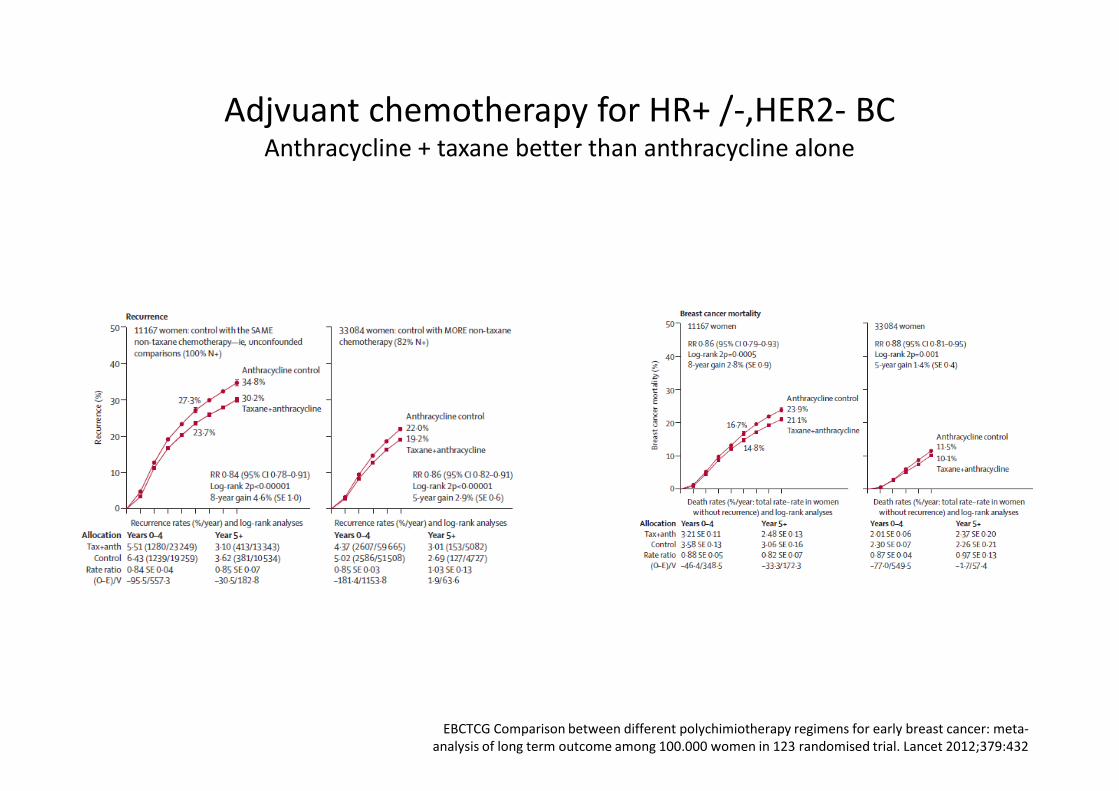
Adjvuant chemotherapy for HR+ /-,HER2- BCAnthracycline + taxane better than anthracycline alone
EBCTCG Comparison between different polychimiotherapy regimens for early breast cancer: meta-analysis of long term outcome among 100.000 women in 123 randomised trial. Lancet 2012;379:432
Adjvuant chemotherapy for HR+/-, HER2- BCNo single standard regimen
• Intermediate risk– ER+/PR- or low ER/PR or T>2cm or Grade 2-3 orKi67% >20%– TC x 4 ( docetaxel 75mg/2 + Cyclophosphamide 600mg/m2)
• High risk– N+– 3xFEC – 3x docetaxel– 3xFEC – 3x docetaxel
• Alternative chemotherapy– AC /EC x 4– AC/EC x 4 –docetaxel x 4– AC / EC x 4-paclitaxel weekly x 12 weeks– 4x AC( every 14 days) -paclitaxel dose dense– FEC 100 x 6– CMF x6
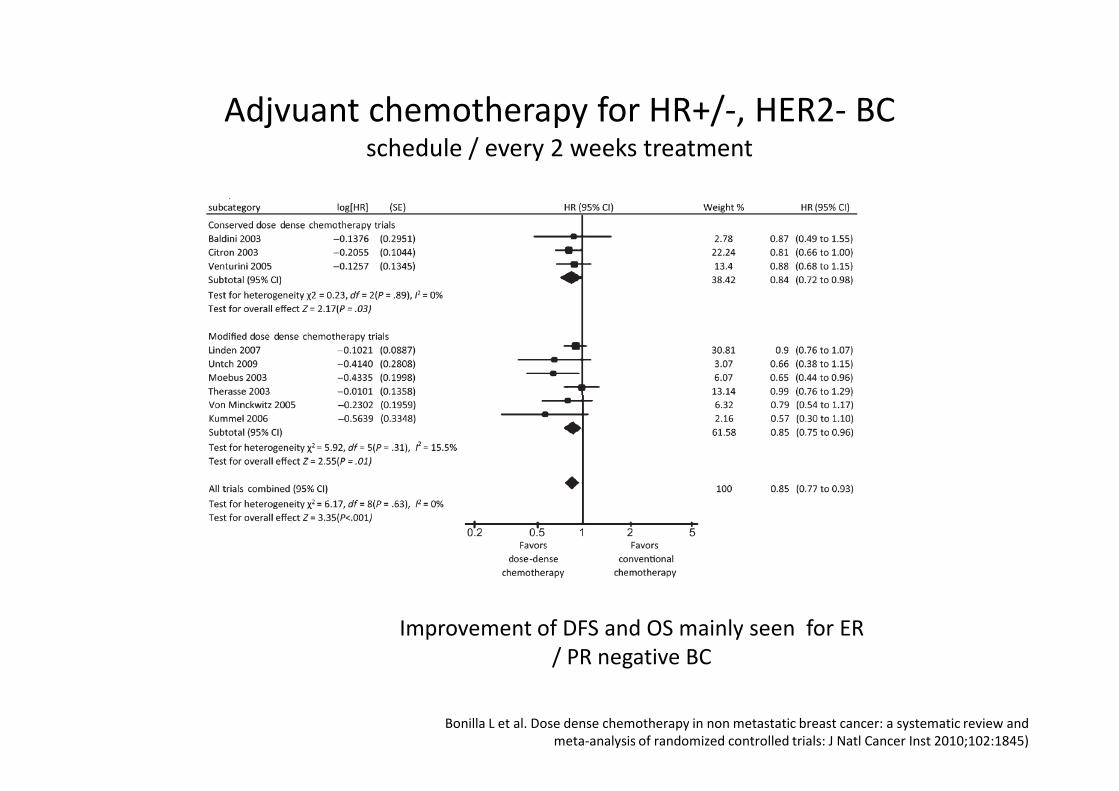
Adjvuant chemotherapy for HR+/-, HER2- BCschedule / every 2 weeks treatment
Bonilla L et al. Dose dense chemotherapy in non metastatic breast cancer: a systematic review andmeta-analysis of randomized controlled trials: J Natl Cancer Inst 2010;102:1845)
Improvement of DFS and OS mainly seen for ER/ PR negative BC
Adjvuant therapy for HR+/- & HER2+ BC
Adjvuant chemotherapy for HER2+ BCbenefit of adjuvant trastuzumab
• All trials establishing the benefit (DFS and OS) of adjuvant trastuzumab1
• pT1a ?
• Trastuzumab is, still in 2014, the only HER2 directed agent to result insurvival benefit when administered with chemotherapy in the adjuvantsetting
• Subcutaneous formulation?• Subcutaneous formulation?
• On the basis of pertuzumab in neoadjuvant and metastatic setting, NCCNguidelines added: pertuzumab can be incorporated into adjuvanttreatment of HER2+, alongside trastuzumab and chemotherapy.
• However the benefit of this strategy for overall survival is not known
• Randomized trial evaluating th role of pertuzumab are ongoing.
• Other HER directed agent including trastuzumab-emtansine and lapatinibremain area of clinical investigation.
1Moja L et al. Trastuzumab containing regimens for early breastcancer Cochrane Database Syst Rev 2012;4:CD006243
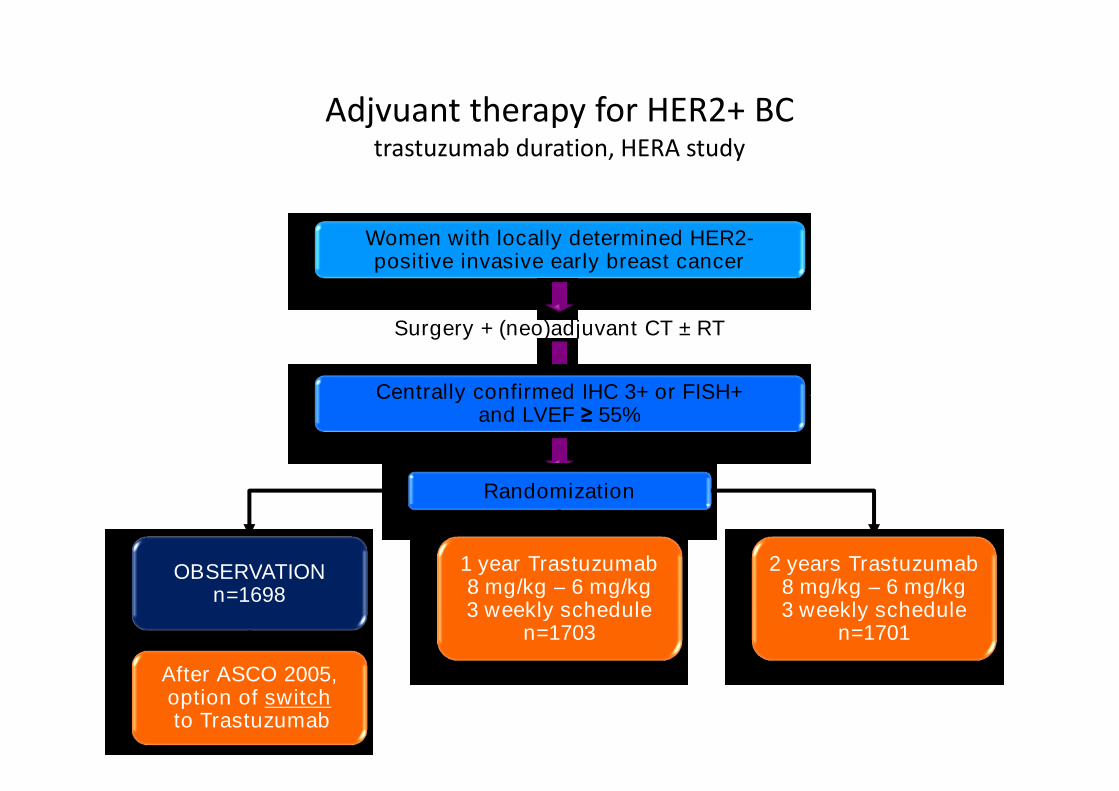
Adjvuant therapy for HER2+ BCtrastuzumab duration, HERA study
Women with locally determined HER2-positive invasive early breast cancer
Surgery + (neo)adjuvant CT ± RT
Centrally confirmed IHC 3+ or FISH+
OBSERVATIONn=1698
Centrally confirmed IHC 3+ or FISH+and LVEF ≥ 55%
Randomization
1 year Trastuzumab8 mg/kg – 6 mg/kg3 weekly schedule
n=1703
2 years Trastuzumab8 mg/kg – 6 mg/kg3 weekly schedule
n=1701
After ASCO 2005,option of switchto Trastuzumab
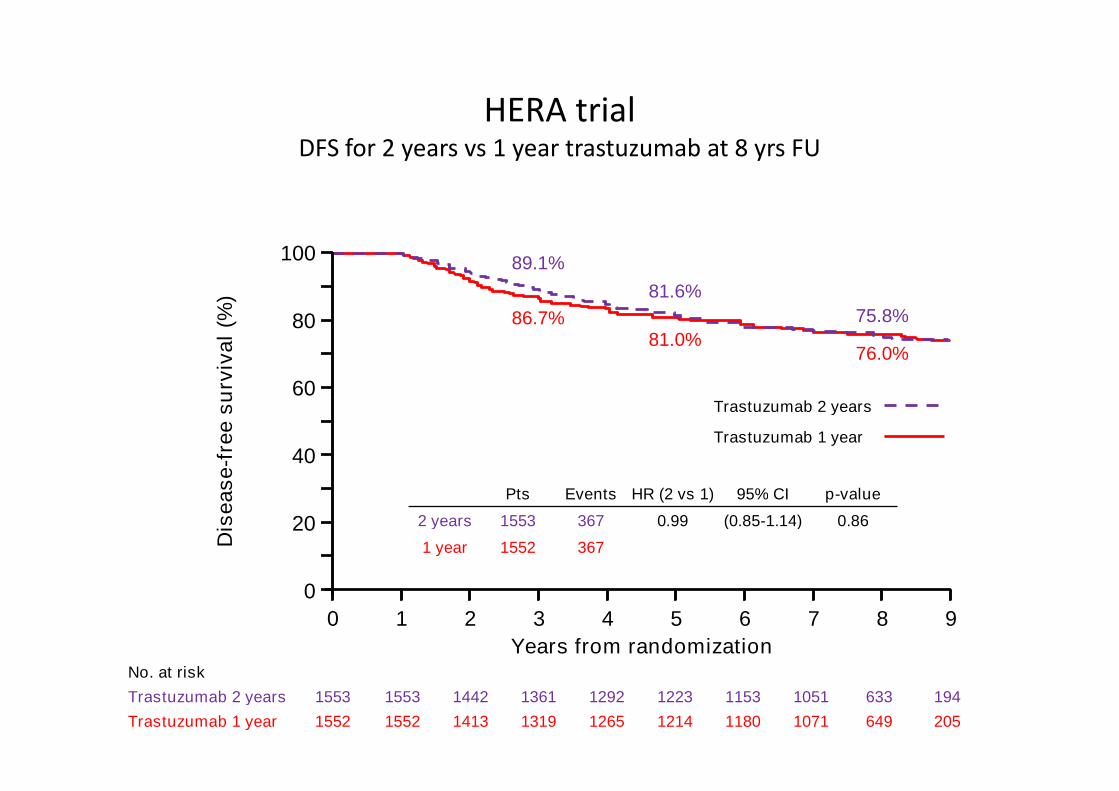
HERA trialDFS for 2 years vs 1 year trastuzumab at 8 yrs FU
urv
iva
l(%
)
89.1%
86.7%81.0%
81.6%
75.8%
76.0%
100
80
60
Dis
ea
se
-fre
es
u
Years from randomization
60
40
20
0
0 1 2 3 4 5 6 7 8 9
No. at risk
Trastuzumab 2 years 1553 1553 1442 1361 1292 1223 1153 1051 633 194
Trastuzumab 1 year 1552 1552 1413 1319 1265 1214 1180 1071 649 205
Trastuzumab 1 year
Trastuzumab 2 years
Pts Events HR (2 vs 1) 95% CI p-value
2 years 1553 367 0.99 (0.85-1.14) 0.86
1 year 1552 367
DFS
Adjuvant therapy for HER2+ BCChoice of chemotherapy
• Several chimiotherapy regimens have been evaluated withtrastuzumab
• Anthracycline followd by taxane&trastuzumab regimen isprefered: greater experience and limited data to suggestgreater efficacy for non-anthracycline based regimengreater efficacy for non-anthracycline based regimen
• No anthracycline based regimen: docetaxel+ carboplatine+trastuzumab (TCH)(D. Slamon) = appropriate and effectivealternative
• Lower congestive heart failure (0.4% vs 2%)
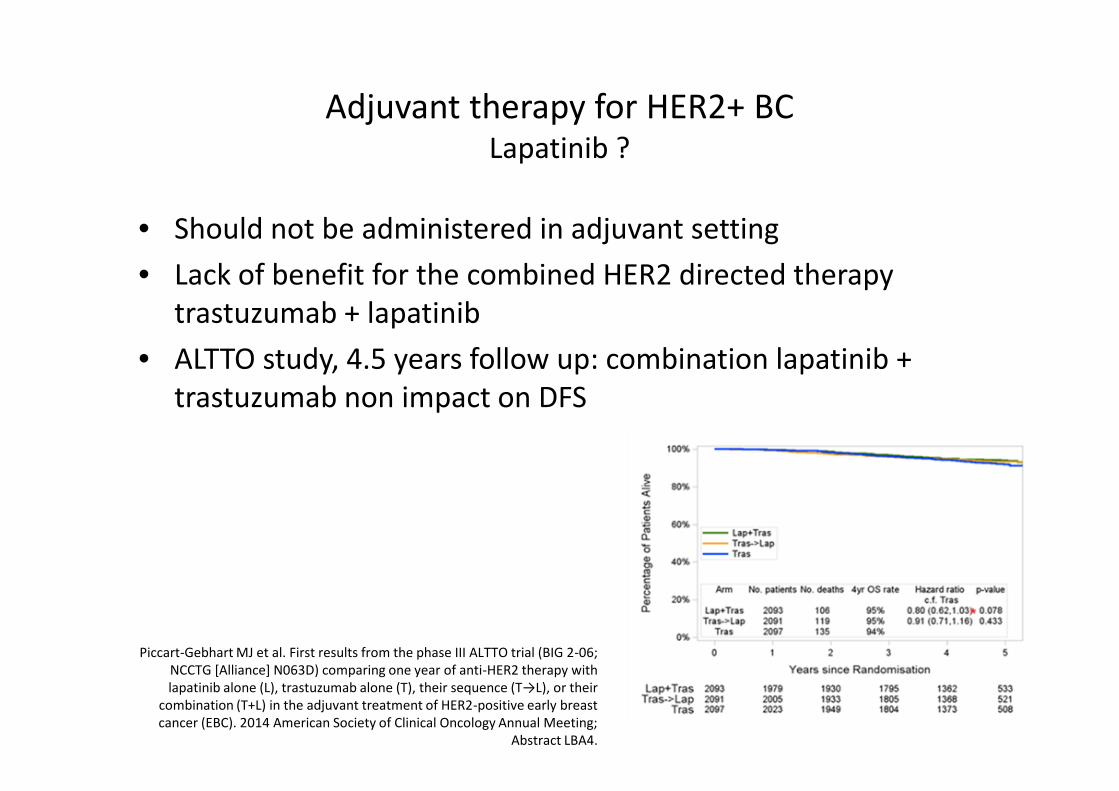
Adjuvant therapy for HER2+ BCLapatinib ?
• Should not be administered in adjuvant setting
• Lack of benefit for the combined HER2 directed therapytrastuzumab + lapatinib
• ALTTO study, 4.5 years follow up: combination lapatinib +trastuzumab non impact on DFStrastuzumab non impact on DFS
Piccart-Gebhart MJ et al. First results from the phase III ALTTO trial (BIG 2-06;NCCTG [Alliance] N063D) comparing one year of anti-HER2 therapy withlapatinib alone (L), trastuzumab alone (T), their sequence (T→L), or their
combination (T+L) in the adjuvant treatment of HER2-positive early breastcancer (EBC). 2014 American Society of Clinical Oncology Annual Meeting;
Abstract LBA4.
Role of Neoadjuvant chemotherapy
Role of Neoadjuvant Chemotherapy
• Originally neoadjuvant chemotherapy was considered forwomen with large toumors or inflammatory disease
• Actually commonly used for high risk (ER-/PR-) (HER2+),operable, stage II and III, primary breast cancer.
• Associated with identical DFS and OS compared to same• Associated with identical DFS and OS compared to sametreatment in the adjuvant setting1
• Additionnal benefit:– Improvement surgical options
– Enhancement of breast conservation
• Attractive model for new drug investigation
1Mauri D et al. Neoadjuvant verus adjuvant systemic treatment inbreast cancer: meta-analysis. J Natl Cancer Inst 2005;97:188-94
Role of Neoadjuvant ChemotherapyImpact of pCR
• Assess clinical response of the primary tumor.
• Minimal response to pathological complet response (pCR)
• Definition of pCR/FDA1
– Absence of any residual invasive cancer– Absence of any residual invasive cancer
– Absence of invasive and non invasive cancer on hematoxylin and eosinevaluation on the resected breast specimen, and all sampledipsilateral lymph nodes following completion of Neoadjuvantchemotherapy
• pCR correlated with improved survival2
1Cortazar P et al. Pathological complete response and long term clinical benefit in breastcancer : the CTNeoBC pooled analysis. Lancet 2014, feb 13
2Von Minckwitz G et al. Impact of treatment charachterisitcs on response of different breastcancer phenotypes:pooled analysis of the German neoadjuvant chemotherapy trials Breast
cencer Treat 2011;125: 145-56
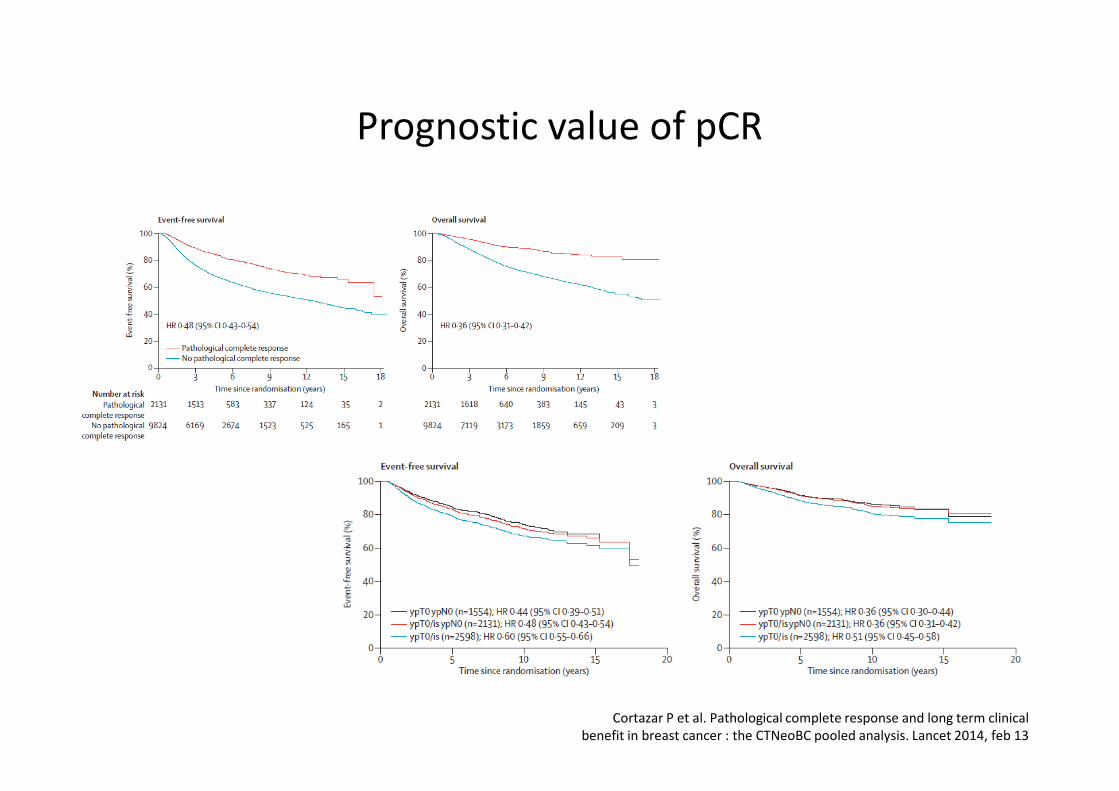
Prognostic value of pCR
Cortazar P et al. Pathological complete response and long term clinicalbenefit in breast cancer : the CTNeoBC pooled analysis. Lancet 2014, feb 13

Prognostic value of pCRby breast subtypes
Cortazar P et al. Pathological complete response and long term clinicalbenefit in breast cancer : the CTNeoBC pooled analysis. Lancet 2014, feb 13
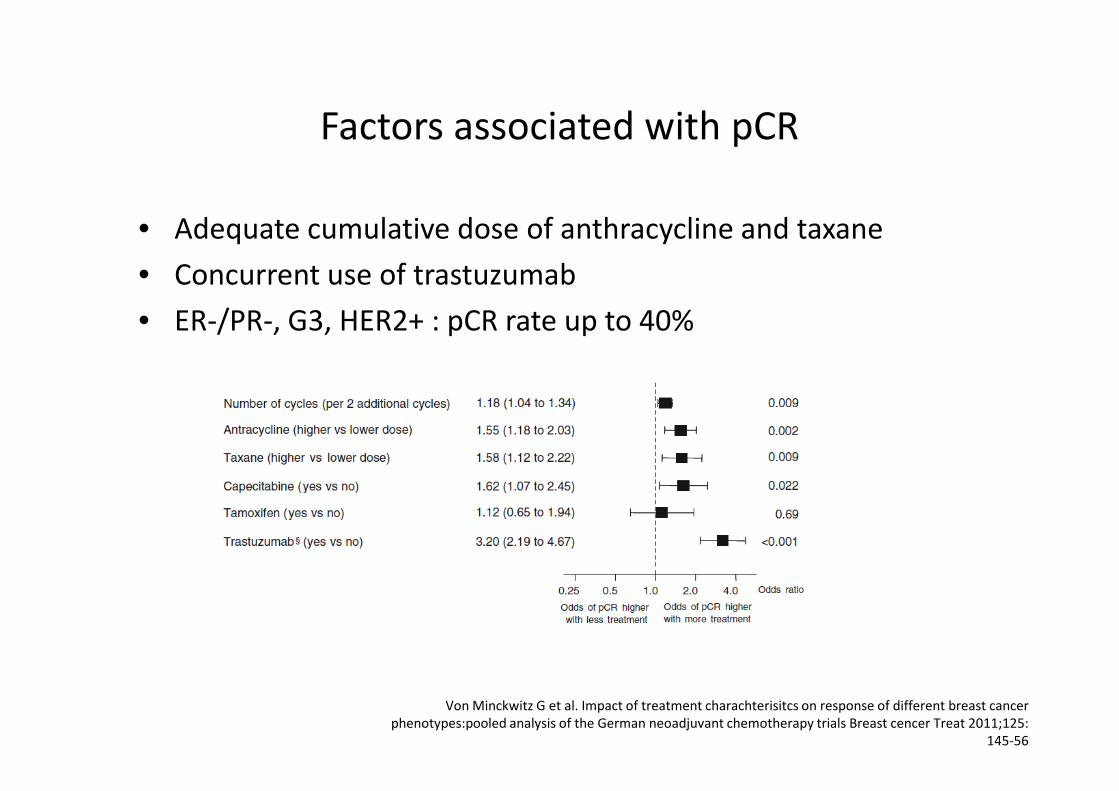
Factors associated with pCR
• Adequate cumulative dose of anthracycline and taxane
• Concurrent use of trastuzumab
• ER-/PR-, G3, HER2+ : pCR rate up to 40%
Von Minckwitz G et al. Impact of treatment charachterisitcs on response of different breast cancerphenotypes:pooled analysis of the German neoadjuvant chemotherapy trials Breast cencer Treat 2011;125:
145-56
Patients selection
• Locally advanced breast cancer, stage 2-3
• Inflammatory breast cancer
• Large operable tumor (> 5cm)1
• According tumor biology, likelihood of achieving a pCR• According tumor biology, likelihood of achieving a pCR– HER2+/non luminal
– TNBC
– Luminal B
1Fisher B et al. Effect of preoperative chemotherapy on loco-regional disease in women with operable breast cancer:
findings from the NSABP B18. JCO 1997:15:2483
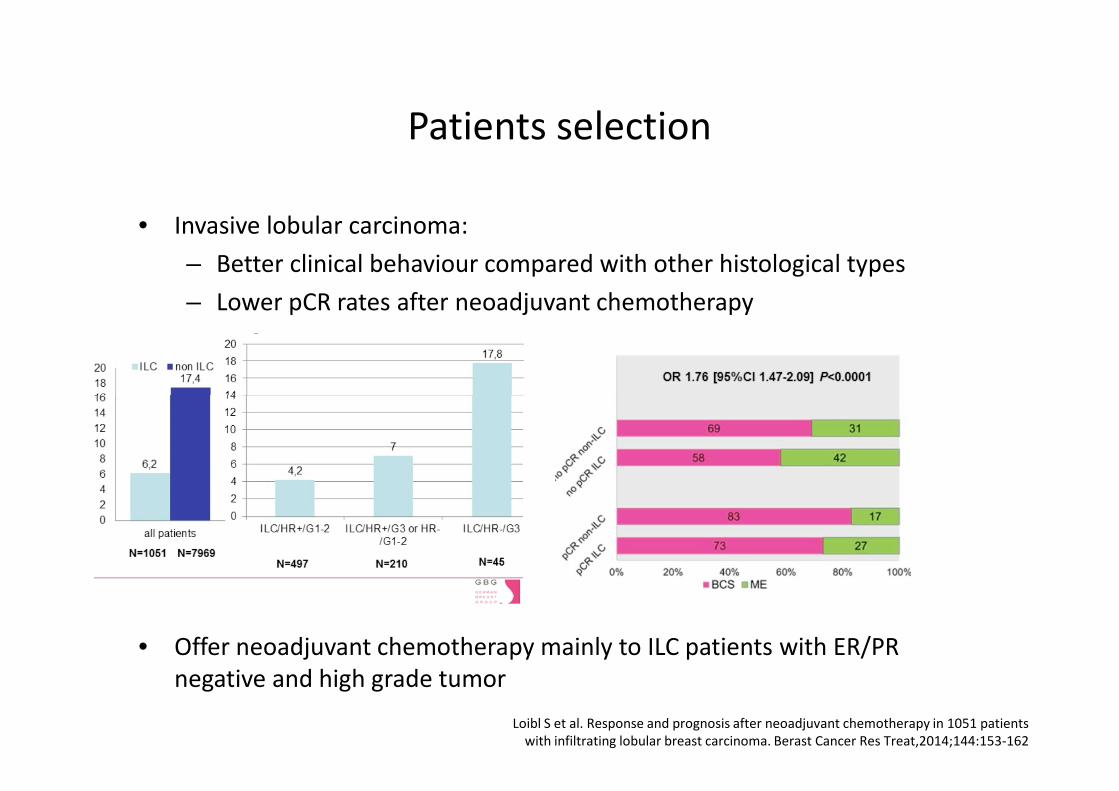
Patients selection
• Invasive lobular carcinoma:
– Better clinical behaviour compared with other histological types
– Lower pCR rates after neoadjuvant chemotherapy
• Offer neoadjuvant chemotherapy mainly to ILC patients with ER/PRnegative and high grade tumor
Loibl S et al. Response and prognosis after neoadjuvant chemotherapy in 1051 patientswith infiltrating lobular breast carcinoma. Berast Cancer Res Treat,2014;144:153-162
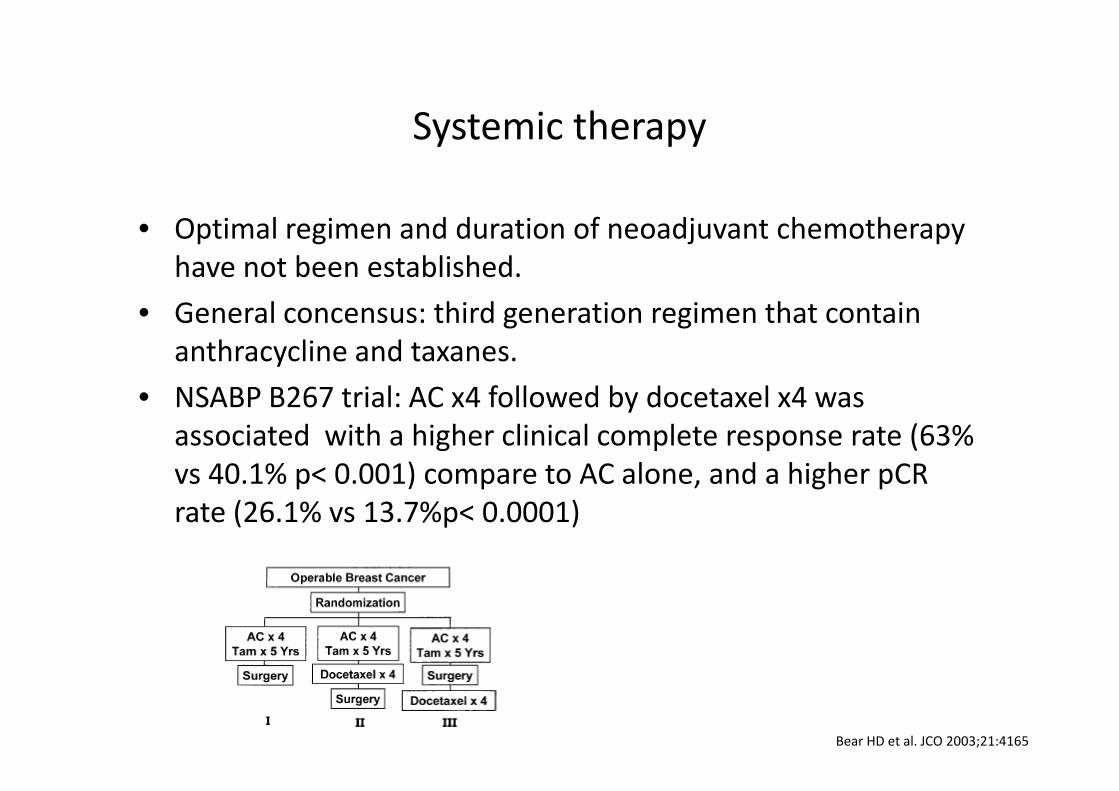
Systemic therapy
• Optimal regimen and duration of neoadjuvant chemotherapyhave not been established.
• General concensus: third generation regimen that containanthracycline and taxanes.
• NSABP B267 trial: AC x4 followed by docetaxel x4 was• NSABP B267 trial: AC x4 followed by docetaxel x4 wasassociated with a higher clinical complete response rate (63%vs 40.1% p< 0.001) compare to AC alone, and a higher pCRrate (26.1% vs 13.7%p< 0.0001)
Bear HD et al. JCO 2003;21:4165
What we have learned?
• Early switch to a non-cross resistant regimen: GeparTrio study
– Specific treatment strategies for patients with or without response to2 cycles of TAC ( docetaxel, doxorubicine, cyclophosphamide)
– Response guided ( switch to another chemotherapy in case of no earlyresponse)response)
– Patient with response guided chemotherapy had a signigificant longerDFS and OS.
– Regimen: TAC x 6 vs TAC x 8 /responder vs TAC-NX ( navelbine, xeloda)
Von Minckwitz G et al. Neoadjuvant chemotherapy adapted by interim response improvesoverall survival of primary breast cancer patients: result of the Gepar Trio trial. Cancer Res
2011;72 (24suppl)53-2
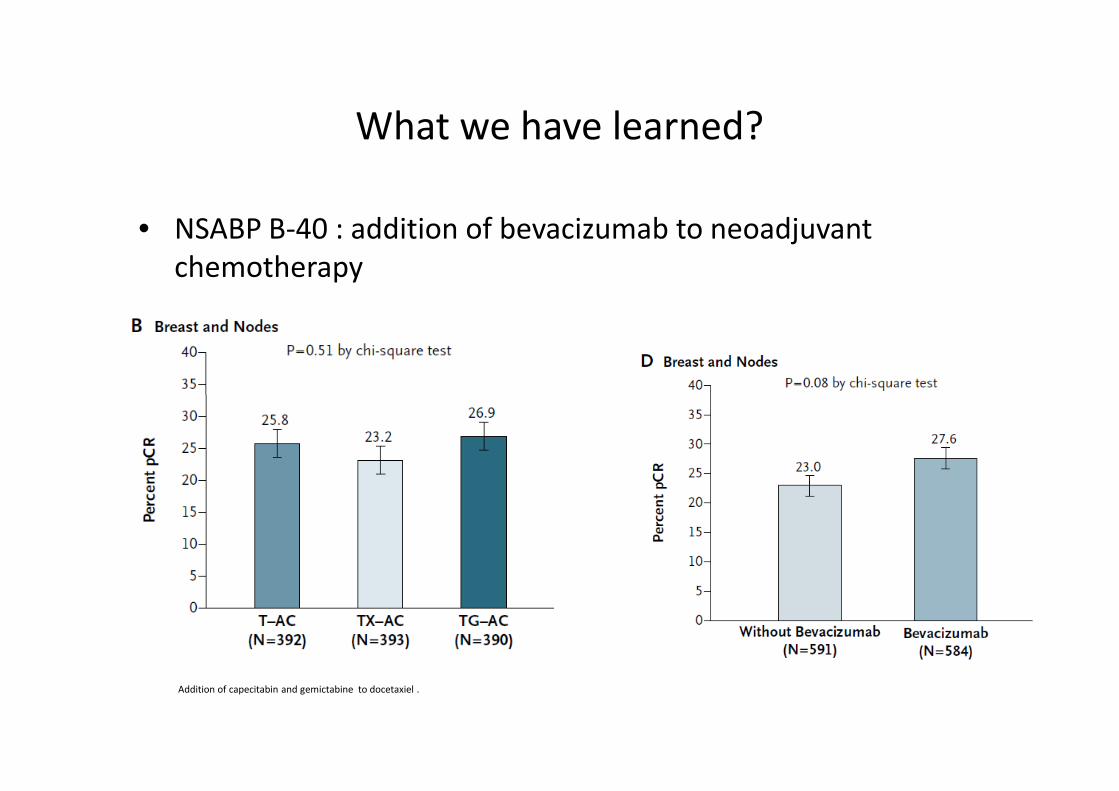
What we have learned?
• NSABP B-40 : addition of bevacizumab to neoadjuvantchemotherapy
Addition of capecitabin and gemictabine to docetaxiel .
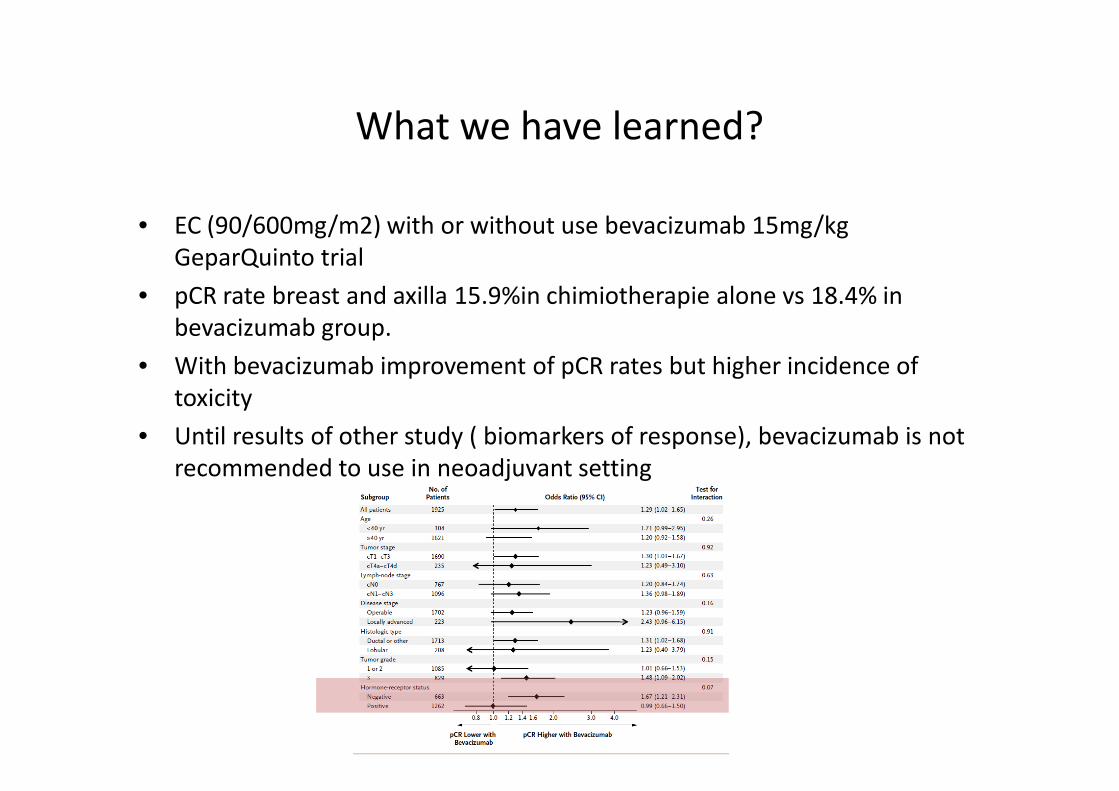
What we have learned?
• EC (90/600mg/m2) with or without use bevacizumab 15mg/kgGeparQuinto trial
• pCR rate breast and axilla 15.9%in chimiotherapie alone vs 18.4% inbevacizumab group.
• With bevacizumab improvement of pCR rates but higher incidence oftoxicitytoxicity
• Until results of other study ( biomarkers of response), bevacizumab is notrecommended to use in neoadjuvant setting
• Incorporation of additional cytotoxic agent or anti-angiogenic agent to anthracycline-taxane basedregimens:
What we have learned?Conclusion-I
– Has not offered significant additional benefit to breastconservation or pCR rate
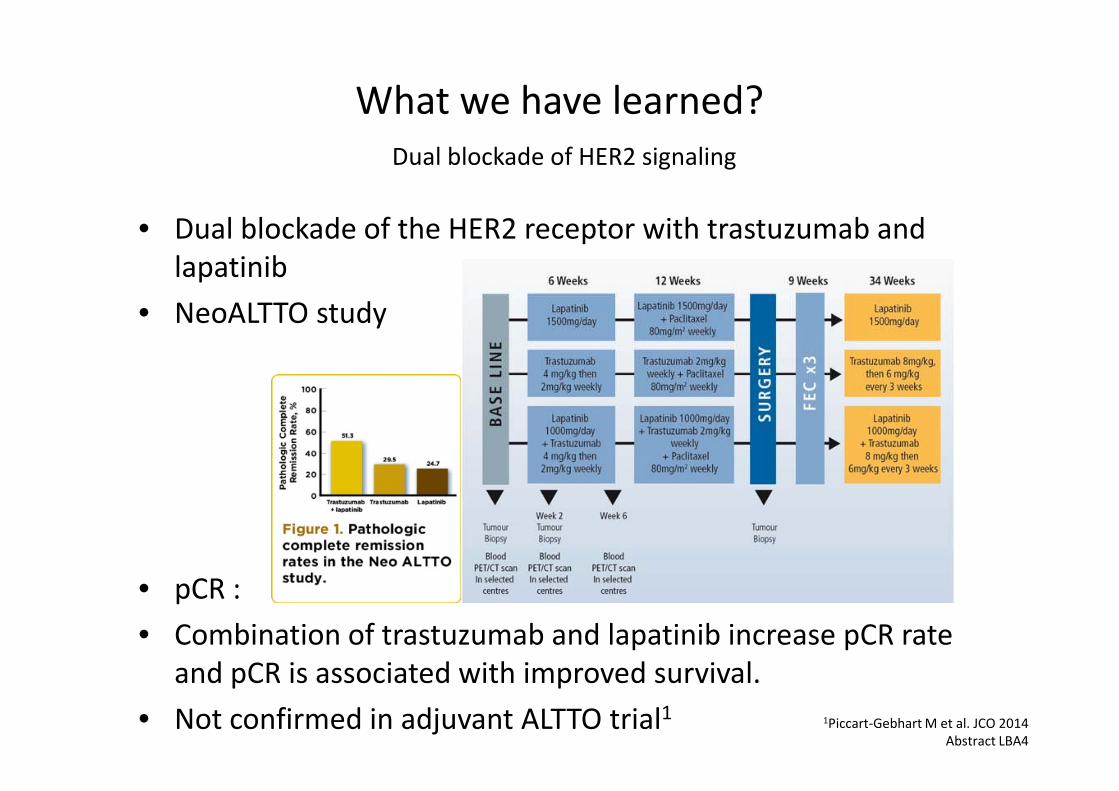
• Dual blockade of the HER2 receptor with trastuzumab andlapatinib
• NeoALTTO study
What we have learned?Dual blockade of HER2 signaling
• pCR :
• Combination of trastuzumab and lapatinib increase pCR rateand pCR is associated with improved survival.
• Not confirmed in adjuvant ALTTO trial1 1Piccart-Gebhart M et al. JCO 2014Abstract LBA4
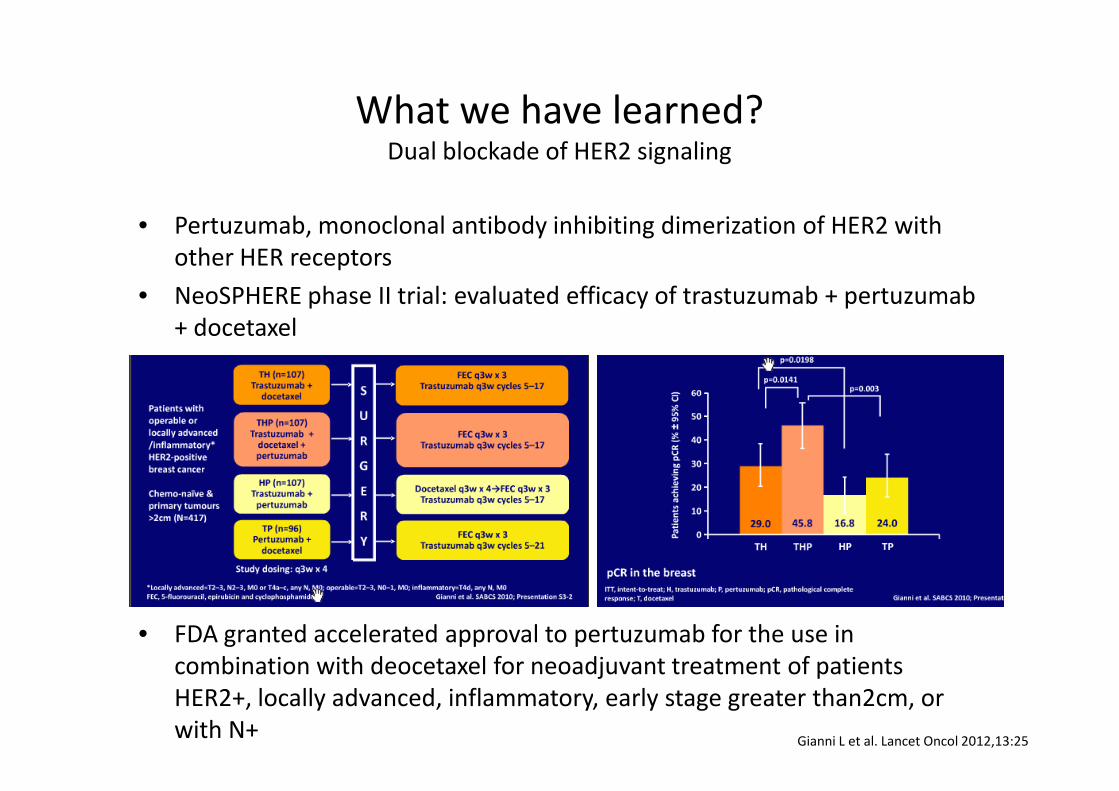
• Pertuzumab, monoclonal antibody inhibiting dimerization of HER2 withother HER receptors
• NeoSPHERE phase II trial: evaluated efficacy of trastuzumab + pertuzumab+ docetaxel
What we have learned?Dual blockade of HER2 signaling
• FDA granted accelerated approval to pertuzumab for the use incombination with deocetaxel for neoadjuvant treatment of patientsHER2+, locally advanced, inflammatory, early stage greater than2cm, orwith N+
Gianni L et al. Lancet Oncol 2012,13:25
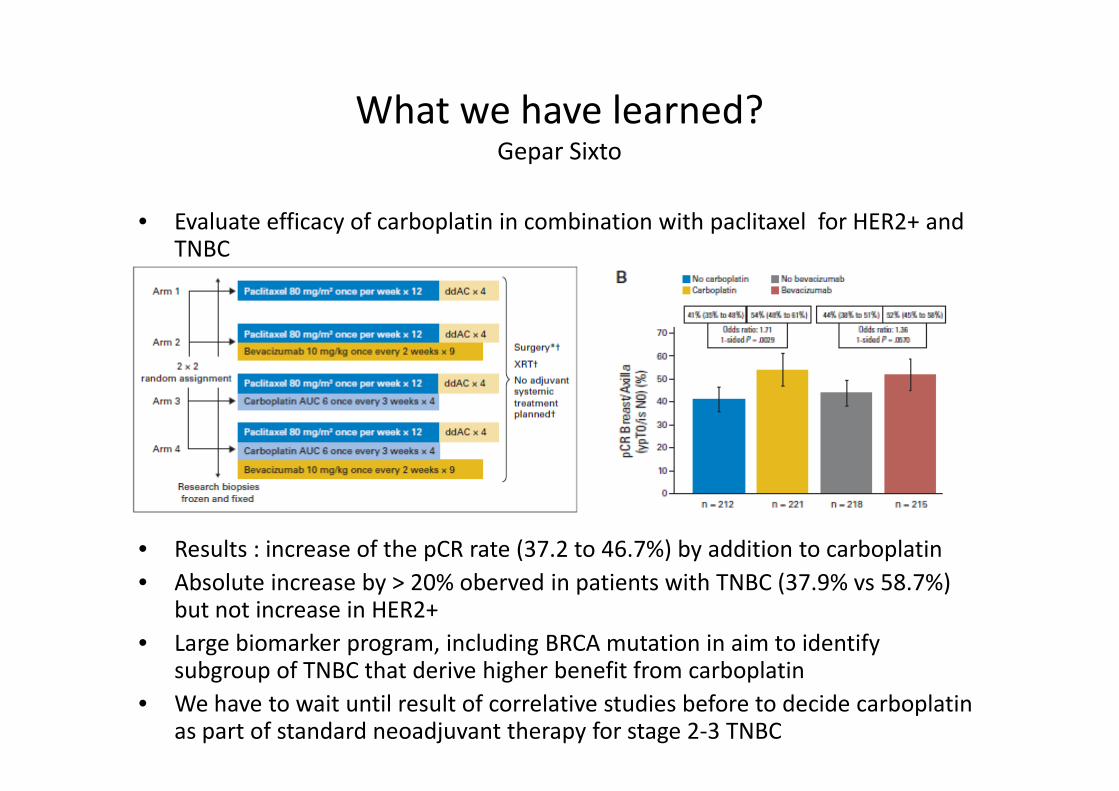
• Evaluate efficacy of carboplatin in combination with paclitaxel for HER2+ andTNBC
What we have learned?Gepar Sixto
• Results : increase of the pCR rate (37.2 to 46.7%) by addition to carboplatin
• Absolute increase by > 20% oberved in patients with TNBC (37.9% vs 58.7%)but not increase in HER2+
• Large biomarker program, including BRCA mutation in aim to identifysubgroup of TNBC that derive higher benefit from carboplatin
• We have to wait until result of correlative studies before to decide carboplatinas part of standard neoadjuvant therapy for stage 2-3 TNBC
Future perspective
• Patients who have no achieving pCR, currently no clear rolefor adjuvant chemotherapy.
• Novel compounds are being investigated in post neoadjuvant
Future perspective
• Trastuzumab-emtansine (T-DM1)– Post neoadjuvant without pCR: treatment with T-DM1 compared with
continuation of trastuzumab in HER2+ patients (Katherine Study)
• Novel cyclin D kinase 4/6 inhibitor: palbociclib– Cyclin D kinase inhibitor explored in addition to endocrine therapy in– Cyclin D kinase inhibitor explored in addition to endocrine therapy in
patients without pCR after neoadjuvant treatment (PENELOPE study)
• Olaparib:– Phase III evaluating efficacy and safety of PARP ihibitors as adjuvant
treatment in patients with germline BRCA1/2 mutations and high riskHER2- primary breast cancer.Have completed surgery and(neo)adjuvant chemotherapy
CONCLUSIONS
• Current consensus opinion for use of neoadjuvant chemotherapyrecommends anthracycline and taxane based therapy
• Several data suggest that neoadjuvant anthracycline and taxane basedtherapy is associated with the highest response rate.
• As similar survival benefits have been demonstrated for the administrationof chemotherapy before or after surgery. More frequently recommendedof chemotherapy before or after surgery. More frequently recommendedfor women with primary operable stage 2-3 disease
• Neoadjuvant chemotherapy is an attractive area for research byidentifying new effective treatment strategies
• As we enter in an era of « personalized » therapy, the identification ofsurrogate predictive and prognostic biomarkers are essential in order toaid treatment decisions.
Thank you for your attention