-
8/10/2019 Adolescent Oral Health
1/45
1 www.aap.org/oralhealth/pact
Protecting All Childrens Teeth
Oral Health inAdolescence
-
8/10/2019 Adolescent Oral Health
2/45
2 www.aap.org/oralhealth/pact
Introduction
Continued focus on oral health during the adolescent period
is
important.
Many childhood risk factors persist and new oral health risk
factors
may emerge during adolescence. Opportunities exist to
prepare,
educate, and empower adolescents to take control of their
oral
health as they move toward adulthood.
Because adolescents often have an increased focus on
personal
aesthetics, this can provide an opening to discuss oral
health
knowledge and behaviors during office visits.
-
8/10/2019 Adolescent Oral Health
3/45
3 www.aap.org/oralhealth/pact
Learner Objectives
Upon completion of this presentation, participants will be able
to:
List common risk factors for dental caries during
adolescence.
Define periodontitis and gingivitis and state clinical signs,
riskfactors, and anticipatory guidance regarding periodontal
disease.
Discuss the prevalence of tobacco use among US adolescentsand
oral effects of tobacco.
Recall the adverse oral effects of methamphetamines
andmarijuana.
List common signs of oral cancer.
Cite the AAP and AAPD stand on oral piercings and counsel
apatient on the risks associated with oral piercings.
-
8/10/2019 Adolescent Oral Health
4/45
4 www.aap.org/oralhealth/pact
Dental Caries
52% of 12- to 19 year olds have experienced tooth decay in
at
least 1 tooth and13% of adolescents have untreated caries.
The pit and fissure surfaces of the molars are the most
common
site of caries.
The dynamic caries balance continues throughout adolescence,and
the same factors that influence caries risk in children still
exist
in adolescence.
-
8/10/2019 Adolescent Oral Health
5/45
-
8/10/2019 Adolescent Oral Health
6/45
6 www.aap.org/oralhealth/pact
Dental Caries, continued
Special health care needs
Infrequent professional dental care
Risk factors that may first be noted in the adolescent,
include
eating disorders and orthodontic appliances that make
performing
oral hygiene more difficult
-
8/10/2019 Adolescent Oral Health
7/457 www.aap.org/oralhealth/pact
Anticipatory Guidance
Anticipatory guidance in caries prevention for adolescents is
similar
to that of young children:
Encourage fluoridated water intake.
Recommend fluoride supplementation for high risk teens not
having access to fluoridated water (up to age 16).
Encourage fluoridated toothpaste use twice a day.Encourage daily
flossing.
-
8/10/2019 Adolescent Oral Health
8/458 www.aap.org/oralhealth/pact
Anticipatory Guidance, continued
Encourage and assist in referrals for dental visits that can
provide
preventive strategies such as dental sealants, topical fluoride,
plaque
andcalculusremoval, and restorative measures.
Promote a healthy diet with rare snacking on sugary or acidic
foods
and liquids. Counsel on risk of vending machine options as these
are
often placed in locations that teens frequent.
Encourage and empower parental assistance in oral hygiene
for
adolescents with special health care needs.
-
8/10/2019 Adolescent Oral Health
9/459 www.aap.org/oralhealth/pact
Gingivitis
Gingivitis is gingival (gum) inflammation
due to the build-up of plaque on
tooth surfaces.
Symptoms of gingivitis include red and
swollen gums that easily bleed with
brushing or flossing.
Gingivitis is usually the result of suboptimal oral hygiene,
both
inadequate brushing and flossing.
Antonio Moretti, DDS, MS Associate Professor, Department
ofPeriodontology. UNC School of Dentistry
-
8/10/2019 Adolescent Oral Health
10/4510
www.aap.org/oralhealth/pact
Periodontitis
Periodontitis is usually accompanied by gingivitis but is a
distinct
disease process that involves irreversible destruction of the
supporting
tissues surrounding the tooth, including the alveolar bone.
Plaque and tartar accumulate at the gum line and the
resultant
inflammation leads to formation of a periodontal pocket between
the
gums and the teeth.
The infection and inflammation spread from the gingiva to
the
periodontal ligament and alveolar bone that support the teeth.
The
destruction of support causes the teeth to become mobile and, if
left
untreated, can lead to tooth loss.
-
8/10/2019 Adolescent Oral Health
11/45
11 www.aap.org/oralhealth/pact
Signs and Symptoms of Periodontal
Disease
Gums that are swollen, bright red,
and tender to touch
Gums that bleed easily
Gingival recession
Tooth Loss
Loose/mobile permanent teeth
Both hormonal changes and externalfactors can affect the
periodontal
tissues of the adolescent
Gingival Recession
(affecting the mandibular anterior teeth)
Antonio Moretti, DDS, MS Associate Professor, Department
ofPeriodontology. UNC School of Dentistry
-
8/10/2019 Adolescent Oral Health
12/45
Localized Aggressive Periodontitis
Usually begins at onset of puberty
Alveolar bone loss usually affects incisors and 1stmolars
Destruction of supporting tissues = high risk for tooth loss
Signs can include tooth mobility and migration (increased
spacingbetween teeth)
Can occur without obvious inflammation (gingivitis) or other
signs/symptomsDisease typically progresses very quickly
Clinical and radiographic exam by a dental team is very
important
-
8/10/2019 Adolescent Oral Health
13/45
Localized Aggressive Periodontitis
Intra-oral condition is not necessarily linked to any
systemic
disease
Genetic predisposition (family dental history should be
evaluated; siblings should be examined)
Destruction can either arrest or progress and affect more
teeth
and become Generalized Aggressive Periodontitis (can affect
the entire dentition)A specific group of bacteria have been
associated with this
disease, so dental treatment typically includes
antimicrobial
therapy
-
8/10/2019 Adolescent Oral Health
14/45
www.aap.org/oralhealth/pact
14
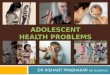
Localized Aggressive Periodontitis
Photos courtesy of:Antonio Moretti, DDS, MS Associate Professor,
Department of
Periodontology. UNC School of Dentistry
Arrows indicate sites with significant alveolar bone loss
-
8/10/2019 Adolescent Oral Health
15/45
15 www.aap.org/oralhealth/pact
Risk Factors for Periodontal Disease
Poor oral hygiene resulting in plaque and calculus formation
Gingivitis or gingival recession Can be triggered by abrasions
from oral piercings
Systemic conditions: Down syndrome
Immunodeficiency (e.g., cyclic neutopenia, leukocyte
adhesiondeficiency)
Metabolic diseases (e.g., diabetes, hypophosphatasia) Oncologic
(e.g., leukemia, Langerhans cell histiocytosis)
Tobacco or marijuana use
Pregnancy and hormonal contraceptives
Oral trauma
-
8/10/2019 Adolescent Oral Health
16/45
16
Periodontal Link to Systemic Disease
Periodontitis may be an independent risk factor for:
Cardiovascular disease (stroke and coronary heart disease)
Diabetes (glycemic control, diabetes complications, and
development
of type 2 diabetes)
Adverse pregnancy outcomes (i.e., low-birth weight, premature
birth)
Association with multiple other systemic diseases (cancer,
arthritis,
obesity, metabolic syndrome, chronic kidney disease) has
been
studied, but study size, limitations, and confounders
prohibit
statement of causal connection at this time.
Additional studies are warranted to investigate these
associations.
www.aap.org/oralhealth/pact
-
8/10/2019 Adolescent Oral Health
17/45
-
8/10/2019 Adolescent Oral Health
18/45
18 www.aap.org/oralhealth/pact
Trauma
Adolescents are at increased risk for trauma to the mouth
and
teeth because of their active lifestyle and increased
risk-takingbehaviors.
Oral and facial trauma can occur secondary to falls,
violence,
athletics, or motor vehicle and other accidents.
-
8/10/2019 Adolescent Oral Health
19/45
-
8/10/2019 Adolescent Oral Health
20/45
20 www.aap.org/oralhealth/pact
Tobacco
Consider the prevalence of tobacco use among teenagers in
the
United States (2009 study):
26% of high school students report some tobacco use
(cigarettes,
smokeless tobacco, cigars).
19.5% of high school students were current cigarette
smokers.
14% of high school students reported cigar use.8.9% of all high
school students used smokeless tobacco.
-
8/10/2019 Adolescent Oral Health
21/45
21 www.aap.org/oralhealth/pact
Oral Effects of Tobacco
Tobacco has a direct carcinogenic effect on the epithelial cells
of theoral mucous membranes and may cause oral cancer.
Tobacco can also have the following oral effects:
Tooth stains and discoloration
Halitosis
Calculus formation
Encouraging patients to quit smoking or using chewing tobacco
canhave positive effects on both their general and oral health.
-
8/10/2019 Adolescent Oral Health
22/45
22 www.aap.org/oralhealth/pact
Illicit Drugs
Illicit drug use can have negative effects on oral health by
affecting salivary flow, changing the acidity of the mouth, and
bypromoting poor dietary habits and laxity in oral hygiene.
-
8/10/2019 Adolescent Oral Health
23/45
23 www.aap.org/oralhealth/pact
Methamphetamines
Street names: Crystal meth, meth, speed, ice, crank.
Potent central nervous system stimulant that stimulates
releaseand blocks re-uptake of monoamines in the brain.
Can be smoked, snorted, injected, or taken orally.
Rampant caries progression, termed meth mouth, may result
from
a combination of drug-induced xerostomia, increased
consumption
of high calorie, sugared, carbonated beverages, tooth grinding
and
clenching, and poor oral hygiene.
-
8/10/2019 Adolescent Oral Health
24/45
24 www.aap.org/oralhealth/pact
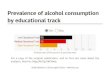
Meth Mouth
Signs of meth mouth include:
1. Accelerated tooth decay in teensand young adults.
2. Distinctive pattern of decay on
buccal smooth surface of teeth and
interproximal surfaces of anteriorteeth.
3. Malnourished appearance of user. Used with permission from
the American Dental Association
-
8/10/2019 Adolescent Oral Health
25/45
25 www.aap.org/oralhealth/pact
Meth Mouth, continued
If meth mouth is discovered:
1. Encourage the patient to stop using the drug, ask if they
would
like help quitting, and assist them in finding help.
2. Encourage good oral hygiene.
3. Refer to a dentist for evaluation and management.
-
8/10/2019 Adolescent Oral Health
26/45
26 www.aap.org/oralhealth/pact
Cannabis
The oral health effects of cannabis are similar to tobacco and
include:
Gingivitis and periodontal disease
Oral cancer
Xerostomia
-
8/10/2019 Adolescent Oral Health
27/45
27 www.aap.org/oralhealth/pact
Oral Cancer
Approximately 30,000 Americans are diagnosed annually with
oral
cancer. In the 15-24 age group, there are 30 deaths per
year.
Approximately 75% of oral cancers are related to tobacco
use,
alcohol use, or both.
Tobacco use in any form (cigarettes, cigars, chewing tobacco)
can
cause oral cancer.
-
8/10/2019 Adolescent Oral Health
28/45
28 www.aap.org/oralhealth/pact
Signs and Symptoms of Oral Cancer
1.Oral tenderness, burning, or a sore that does not heal
2. Pain, tenderness, or numbness in the mouth
3. Lump in the mouth4. Color changes in the mouth
5. Difficulty chewing, swallowing, or speaking
6. Change in the way the teeth fit together
7. Leukoplakia
Providers should encourage and assist in tobacco cessation, as
well as
examine the oral mucosa for abnormalities, especially in
tobacco-using
patients.
-
8/10/2019 Adolescent Oral Health
29/45
29 www.aap.org/oralhealth/pact
Oral Piercings and Grills
The American Dental Association and the American Academy
of Pediatric Dentistry have officially recommended against
intraoral/perioral piercing and tongue splitting because of
the
potential for numerous negative sequelae.
-
8/10/2019 Adolescent Oral Health
30/45
-
8/10/2019 Adolescent Oral Health
31/45
31 www.aap.org/oralhealth/pact
Jewelry-Related Complications
Injury to the gums.
Chipped (fractured) teeth
Interference with normal oral function.
Allergic reaction/hypersensitivity tometal (eg, nickel).
Interference with oral health evaluation.
Aspiration or ingestion possible ifjewelry becomes loose.Used
with permission from the Martha Ann Keels, DDS, PhD; Division Head
ofDuke Pediatric Dentistry, Duke Children's Hospital
-
8/10/2019 Adolescent Oral Health
32/45
32 www.aap.org/oralhealth/pact
Grills
No studies show that grills are harmful
to the mouth. However, there is at least
one case report of a grill acceleratingthe caries process in an
adolescent.
Grill wearers should be counseled to:
Remove the grill when eating.Limit the amount of time the grill
is worn.
Brush and floss carefully.
Watch for symptoms of allergy to the grill's metal.
Used with permission from the American Academy of Pediatric
Dentistry (AAPD);Reproduced with AAPD permission
-
8/10/2019 Adolescent Oral Health
33/45
33 www.aap.org/oralhealth/pact
Question #1
Which of the following is a risk factor for caries
inadolescents?
A. Poor oral hygiene
B. Inadequate access to topical fluoride
C. Previous caries experience
D. Frequent access to sugars
E. All of the above
-
8/10/2019 Adolescent Oral Health
34/45
34 www.aap.org/oralhealth/pact
Answer
Which of the following is a risk factor for caries
inadolescents?
A. Poor oral hygiene
B. Inadequate access to topical fluoride
C. Previous caries experience
D. Frequent access to sugars
E. All of the above
-
8/10/2019 Adolescent Oral Health
35/45
35 www.aap.org/oralhealth/pact
Question #2
Which of the following is not a sign or symptom ofperiodontal
disease?
A. Loose teeth
B. Leukoplakia
C. Halitosis
D. Swollen gums
E. Gums that bleed easily
-
8/10/2019 Adolescent Oral Health
36/45
36 www.aap.org/oralhealth/pact
Answer
Which of the following is not a sign or symptom ofperiodontal
disease?
A. Loose teeth
B. Leukoplakia
C. Halitosis
D. Swollen gums
E. Gums that bleed easily
-
8/10/2019 Adolescent Oral Health
37/45
-
8/10/2019 Adolescent Oral Health
38/45
38 www.aap.org/oralhealth/pact
Answer
Which of the following behaviors can affect salivary flow
and
change the acidity of the mouth?
A. Oral piercings
B. Using tobacco
C. Using illicit drugs
D. Wearing a grill
E. All of the above
-
8/10/2019 Adolescent Oral Health
39/45
39 www.aap.org/oralhealth/pact
Question #4
True or False? Approximately 30% of high school studentsare
smokers.
A. True
B. False
-
8/10/2019 Adolescent Oral Health
40/45
-
8/10/2019 Adolescent Oral Health
41/45
41 www.aap.org/oralhealth/pact
Question #5
Which of the following can cause gingivitis?
A. PregnancyB. Smoking
C. Certain medications
D. All of the above
E. None of the above
-
8/10/2019 Adolescent Oral Health
42/45
42 www.aap.org/oralhealth/pact
Question #5
Which of the following can cause gingivitis?
A. PregnancyB. Smoking
C. Certain medications
D. All of the above
E. None of the above
-
8/10/2019 Adolescent Oral Health
43/45
43
www.aap.org/oralhealth/pact
References
1. American Academy of Pediatric Dentistry. Guideline on
Adolescent Oral Health Care. AAPD
Reference Manual. 2005-2006. P. 72-79.
2. American Academy of Pediatric Dentistry. Policy on
Intraoral/Perioral Piercing and Oral
Jewelry/Accessories. Revised 2011. Reference Manual. 35 (6):
65-66. Accessed December 20, 2013.
3. American Academy of Pediatric Dentistry. Periodontal Diseases
of Children and Adolescents.
Reference Manual. 2004; 35(6): 338-345.
3. American Dental Association. Grills, grillz, and fronts.
JADA. 2006; 137:1192.
4. American Dental Association. Oral piercing and health. JADA.
2001; 132:127.
5. Borgnakke W, Ylostalo P, Taylor G. et al. Effect of
periodontal disease on diabetes: Systematic
review of epidemiologic observational evidence. J Periodontol.
2013; 84(4 Suppl): 135152.6. Brown LJ, Brunelle JA, Kingman A.
Periodontal status in the United States, 1988-1991:
prevalence, extent and demographic variations [special issue]. J
Dent Res. 1996; 75:672-83
7. Campbell A, Moore A, Williams E, Stephens J, Tatakis DN.
Tongue piercing: impact of time and
barbell stem length on lingual gingival recession and tooth
chipping. J Periodontology.2002;
73(3):289-297.
-
8/10/2019 Adolescent Oral Health
44/45
References
8. Casamassimo P. Bright futures in practice: Oral health.
Arlington, VA. National Center for
Education in Maternal and Child Health. 1996.
9. CDC. Youth Risk Behavior Surveillance, United States2009,
Surveillance Summaries, June 4.
MMWR 2010; 59(No. SS-5).10. Dietrich T, Sharma, P, Walter, C et
al. The epidemiological evidence behind the association
between periodontitis and incident atherosclerotic
cardiovascular disease. J Periodontol. 2013; 84
(Suppl 4), 7084.
11. Hollowell WH, Childers NK. A New Threat to Adolescent Oral
Health: The Grill. Pediatr Dent.2007; 29(4): 320-2.
12. Howe AM. Methamphetamine and childhood and adolescent
caries.Aust Dent J. 1995;
40(5):340.13. Ide M, Papapanou PN. Epidemiology of association
between maternal periodontal disease andadverse pregnancy outcomes
- systematic review. J Periodontol. 2013. 84(4 Suppl): 181194.
14. Kapferer I, Beier US, Persson RG. Tongue Piercing: The
Effect of Material on MicrobiologicalFindings. Journal of
Adolescent Health. 2011; 49(1):76-83.
-
8/10/2019 Adolescent Oral Health
45/45
www.aap.org/oralhealth/pact
References, continued
15. Linden GJ, Lyons A, Scannapieco FA. Periodontal systemic
associations: review of the evidence.J Periodontol. 2013; 84(Suppl
4):S8-S19.
16. Ludwig DS, Peterson KE, Gormaker SL. Relation between
consumption of sugar-sweeteneddrinks and childhood obesity: A
prospective, observational analysis. Lancet. 2001;
357(9255):505-8.
17. Oh TJ, Eber R, Wang HL. Periodontal diseases in the child
and adolescent. J Clin Periodontol.2002; 29(5):400-10.
18. The Society of Teachers of Family Medicine. Smiles for Life:
A national oral health curriculum.Available online at:
wwwsmilesforlifeoralhealth.org. Accessed May 25, 2013.
19. US Department of Health and Human Services. Oral health in
America: A Report of the SurgeonGeneral. Rockville MD: US
Department of Health and Human Services, National Institute of
Dental and Craniofacial Research, National Institutes of Health;
2000. Available online
atwww.nidcr.nih.gov/DataStatistics/SurgeonGeneral. Accessed January
18, 2013.
20. Wyshak G. Teenaged girls, carbonated beverage consumption,
and bone fractures.ArchPediatr Adolesc Med. 2000; 154(6):610-3.