Embed Size (px)
Citation preview

www.mghcme.org
Adolescent Substance AbuseTimothy E. Wilens, M.D.
Chief, Division of Child & Adolescent Psychiatry, (Co) Director of Center for Addiction Medicine,
Massachusetts General HospitalMassachusetts General Hospital for Children
Harvard Medical School

www.mghcme.org
0
5
10
15
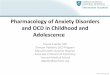
Alcoholabuse/dependence
Drugabuse/dependence
Any substance usedisorder
Merikangas et al. J.Am.Acad.Child Adolesc.Psychiatry, 2010;49(10):980-989
Lifetime Prevalence of DSM-IV Substance Use
Disorders Disorders in the National Comorbidity
Survey-Adolescent (NCS-A)

www.mghcme.org
56%
5%
9%4% 18%
8%
Free from a Friend or Relative Taken from a friend or relative without asking
Bought from a friend or relative Drug dealer
From one doctor Other source
SAMHSA, 2008 National Survey on Drug Use and Health (September 2009)
70%
From
friends
and
family
family
Sources of Pain Relievers for Most Recent
Nonmedical Use Among Past Users

www.mghcme.org
Age at Onset of DSM-IV Drug
Abuse and Dependence
Compton et al. Arch Gen Psychiatry/ Vol 64, May 2007; 45(11): 1294 - 1303

www.mghcme.org
Juvenile SUD: Overview
• Definitions
– Use - at least once [often stratified in reports as past 30d, past year]
– Misuse - emergence of pattern of use
– Substance Use Disorder (DSM V) - pattern of misuse with impairment and/or consequences, inability to control use, use despite consequences, physiological symptoms
• Graded mild-severe
• No differentiation between abuse vs dependence

www.mghcme.org
Photo courtesy of the NIDA Web site. From
A Slide Teaching Packet: The Brain and the
Actions of Cocaine, Opiates, and Marijuana.
Inhibitions
Major Brain Circuits Involved in Addiction

www.mghcme.org
Substance Mechanism of Action
Alcohol GABA, opioid agonist; NMDA antagonist
Cocaine Blocks re-uptake of dopamine
Amphetamines Stimulate dopamine release
PCP, ketamine NMDA antagonist
Opioids Mu, delta, and kappa agonism
Cannabis CB1 agonist
MDMA (“ecstasy”) 5HT release and re-uptake inhibition; mild DA and NE reuptake inhibition
LSD (“Acid”) 5HT2a agonism leading to increased glutamate?
(Adapted from Textbook of SUD Tx: Galanter; APA Press 2013)

www.mghcme.org
Juvenile SUD: Risk and Protective Factors
Familial - runs in families
Genetic – 50% accounted for by “genes”
Environmental – Values, patterns, availability
Self medication – Symptoms, affect intolerance
(Wilens et al., 2000; 2002, 2005, 2013; Nunes et al. 2003; Rhee et al. 2003; Yule et al. AJA 2013)

www.mghcme.org
Wong SS, Wilens TE..
Pediatrics.
2017;140(5):e20171818
Medical Cannabinoids in Children and Adolescents: A Systematic Review

www.mghcme.org
Note: Boldface figures indicate significant results. Dashes indicate analyses were not performed because
of a limited number of data points.
Groenman AP et al. J Am Acad Child Adolesc Psychiatry. 2017
Jul;56(7):556-569
Child Psychopathology Increases Risk for Later SUD

www.mghcme.org
Life
tim
e P
reva
len
ce
Persistent BPD vs. Control: p=0.001;
Persistent BPD vs. Non-Persistent BPD: p=0.2;
Non-Persistent BPD vs. Controls: p=0.2
Development of SUD in Adolescent Bipolar Disorder
Wilens et al. J Clin Psych 2016
Bipolar
Control

www.mghcme.org
Juvenile SUD: Diagnostics
– Evaluate medical condition including complications (LFT, STDs)
– Generate differential diagnosis for psychiatric/medical symptoms
– Utilize urine, saliva, or hair toxicology screens
(Jackson, Yule, Wilens; Adolescent SUD in Handbook of
Adolescent Medicine, 2nd Edition, 2017)

www.mghcme.org
Screening Adolescents for Drugs and Alcohol:S2BI (Levy et al, Pediatrics 2016)
In the past year, how many times have you used:
• Tobacco?
• Alcohol?
• Marijuana?
STOP if all “Never.”
Otherwise, CONTINUE.
• Prescription drugs that were not prescribed for you (such as pain medication or Adderall)?
• Illegal Drugs (such as cocaine or Ecstasy)?
• Inhalants (such as nitrous oxide)?
• Herbs or synthetic drugs (such as salvia, “K2”, or bath salts)?
https://www.drugabuse.gov/ast/s2bi/#/

www.mghcme.org
Screening Adolescents for Drugs and Alcohol
C Have you ever ridden in a CAR driven by someone who was “high” or had been using alcohol or drugs?
R Do you ever use alcohol or drugs to RELAX, feel better about yourself, or fit in?
A Do you ever use alcohol or drugs while you are by yourself, ALONE?
F Do you ever FORGET thins you did while using alcohol or drugs?F Do your family or FRIENDS ever tell you that you should cut
down on your drinking or drug use/T Have you ever gotten into TROUBLE while you were using
alcohol or drugs?
• Two or more yes answers on the CRAFFT suggest a serious problem and a need for further assessment
(Knight et al., Arch Pediatr Adolesc Med 1999: 153: 591-6)

www.mghcme.org
Documentation
According to Group Health’s standards for substance use disorder
documentation, clinical staff may and should document the following
information related to substance use:
• Patient disclosures about substance use, abuse, or dependence.
• Patient disclosures about current or past chemical dependency
treatment.
• Completed screening tools including:
- Adolescent substance use screening tool (CRAFFT) and CRAFFT results.
- Others
- A DSM diagnosis of substance abuse or dependence and the pertinent
clinical information that supports the diagnosis.
- Referrals for a chemical dependency evaluation (includes all levels of
care, behavioral, medical, inpatient, partial, outpatient).
Protection of chemical dependency information begins at the start of a
treatment program, not at the time of screening, identification, or referral
(as outlined in confidentiality regulation 42 CFR Part 2).
Adapted from Group Health Guidelines
www.ghc.org/all-sites/guidelines/drug-adolescent.pdf

www.mghcme.org
Juvenile SUD: Treatment
Stabilization of alcohol / drug abuse
– Harm Reduction: Lowering use
– Absolute sobriety: None
– Basic self-help philosophy
• Give multiple referrals
• Alcoholics Anonymous/Narcotics Anonymous for teens
• Rational Recovery
• Avoid “tough love” as initial step
(Jackson, Yule, Wilens; Adolescent SUD in Handbook of Adolescent Medicine, 2nd Edition, Springer, 2017)

www.mghcme.org
Juvenile SUD: Treatment
Psychotherapy– Groups: for youth and for their parents
– Motivational interviewing• Engage/collaborative connection with patient• Discuss issues that are problematic (don’t focus on SUD)
– Cognitive Behavioral modification• Reduction in impairing behaviors
• Coping skills
• Reduce SUD “cues”
• Relapse prevention (eg reducing cues, balance in life)
(Wilens, McKowen & Kane Contemp Peds 2013)

www.mghcme.org
Psychopharmacologic Strategies with Juvenile Substance Abuse
• Aversive treatment (antimetabolism)
• Reduce urge or craving
• Substitution therapy
• Treat underlying psychiatric comorbidity
• Preventive therapy
(Gignac et al. 2010; Yule and Wilens, Curr Psych. 2015; 14(4): 36-39, 47-51.Jackson, Yule, Wilens;
Adolescent SUD in Handbook of Adolescent Medicine, 2nd Edition, Springer, 2017)

www.mghcme.org
Pharmacotherapies to Reduce Urge or Cravings
• Nicotine– Nicotine patch (most effective in teens), inhaled
nicotine, nicotine gum, nicotine lozenges– Bupropion (Wellbutrin, Zyban)– Varenicline (nicotinic modulator)– Cytisine (acacia seed extract, nicotinic partial
agonist)-used in Europe– Experimental: Riminobant (Cannabinoid type I
receptor antagonist); nicotinic partial/full agonists-various nicotinic subunits
– E-cigs not recommended (e.g. may encourage cig use)
(Lerman et al. J Clin Oncol 2005:23-311-323; Basil et al. Psychiatry 12:2005:49-52; West et al. NEJM
2011:365: 1193-200; Dutra and Glants, JAMA Pediatrics, 2014: 168: 610-617).

www.mghcme.org
Pharmacotherapies to Reduce Urge or Cravings
• Alcohol– Naltrexone (Rivea) -reduces alcoholic drinking: dosing 25-50 mg
BID to TID– Acamprosate (Campral) -helps with abstinence: dosing 333 mg 1-
2 TID– Topirimate (Topamax) -helps reduce alcoholic drinking, maintain
abstinence: dosing <300 mg /day– Odansetron (Zofran) -helps reduce urges and drinking in early
onset alcohol use disorders; 2-8 mg/day– Baclofen -GABA derivative, anecdotally reported to reduce
drinking urges and edginess; 10-20 mg/day– Dilsufiram (Antabuse)- reaction to alcohol (use for passes, highly
motivated youth); blocks aldehyde dehydrogenase
(Lerman et al. J Clin Oncol 2005:23-311-323; Basil et al. Psychiatry 12:2005:49-52; Johnson et al. JAMA 2007; 298:1641-
1651; Niederhofer &Staffen: Eur Child Adolesc Psychiatry:12:144148 2003; Deas D. et al., JAACAP 2005. 15:723-728; ADD
RECENT REFERENCE)

www.mghcme.org
Pharmacotherapy for Marijuana Use Disorders
• N-Acetyl Cysteine (NAC)-natraceutical-dosing 1200 mg BID (RCT; Grey et al. Am J Psych 2012)
• Buspirone (pilot RCT; McRae-Clark et al., 2009)
• Gabapentin (pilot RCT; Mason et al., 2012)
• Topirimate (adult addiction studies)
• Rimonabant- experimental (CB-1 receptor blocker; EU approval and withdrawal: mood/SI) (Huestis MA, et al.
Psychopharm 2007)

www.mghcme.org
Young people SUD- Comorbidity
• ADHD – Consider addressing both conditions– Low level substance use–> continue to treat ADHD– More severe SUD –> address SUD first, if possible– Can treat ADHD through SUD (nonstim, XR stims only)
• Depression – Co-treat Depression and SUD– May need to improve SUD to see residual mood symptoms
• Anxiety– Address SUD initially, then anxiety– Can treat anxiety through SUD (use SSRI/SNRI, buspirone)
• Severe Mood Dysregulation– Treat mood dysregulation and SUD simultaneously– Use safer agents (e.g. SGAs for mood)
For review, see (Gignac et al. 2010; Yule and Wilens, Curr Psych. 2015; 14(4): 36-39,
47-51.Jackson, Yule, Wilens; Adolescent SUD in Handbook of Adolescent Medicine, 2nd
Edition, Springer, 2017)

www.mghcme.org
Juvenile SUD: Confidentiality
• Need to discuss SUD with patient & parent
1) Adolescent discussion with parent
2) Practitioner + adolescent discussion with parent(s)
• Need for immediate disclosure
– Dangerousness or severe SUD (eg. IV)
– Incompetent adolescent
(Gignac, Waxmonsky and Wilens, Adol SA, in Child Adoles Psychopharm, 2010; Jackson, Yule,
Wilens; Adolescent SUD in Handbook of Adolescent Medicine, 2nd Edition, Springer, 2017)

www.mghcme.org
Juvenile SUD: Summary
• Juvenile SUD is commonly comorbid with psychopathology
• Screening, discussion, and documentation constitute components of care of these youth
• Treatment of psych may reduce ultimate SUD
• Treatment of comorbid youth requires both SUD and psych intervention
• Pharmacotherapy can be effective in youth with SUD problems


























![Principles of psychopharm[1]](https://img.pdfslide.net/doc/110x75/55498fedb4c905c26a8b5446/principles-of-psychopharm1.jpg)
