Embed Size (px)
Citation preview

ADOLESCENT SUICIDE: AN ECOLOGICAL APPROACH
HUDA AYYASH-ABDO
Lebanese American University
Beirut, Lebanon
Adolescent suicide, which has been ranked among the top 10 causes of death in the world, is anissue of increasing concern to school psychologists, educators, and parents. Here an ecologicalapproach is proposed to enhance our understanding of how personal, interpersonal, and socio-cultural factors contribute to the increased risk for suicide among adolescents. The ecologicalapproach allows exploration of how adolescent suicide is determined by multiple factors relatedto the adolescent’s personal history or ontogenic development (e.g., depression), the influencesof those individuals with whom adolescents have immediate contact with, or the microsystems(e.g., family and school), the larger social units, or the exosystems, that indirectly influenceadolescents (e.g., media), and the larger culture or macrosystems (e.g., cultural differences inattitudes about suicide). In this article the interaction of several factors within and between thepermeable boundaries of each of the layers of the ecological paradigm is also highlighted. Finally,examples of intervention and prevention strategies at each level of the system are set forth.© 2002 Wiley Periodicals, Inc.
The number of adolescent deaths from suicide has increased dramatically over the last fivedecades to the extent that suicide has been described as “epidemic.” According to the Center forDisease Control and Prevention (CDC, 1995), the suicide rate in adolescents ages 15–19 increased28.3% from 1980 to 1992 in the United States. In fact, in 1998, more teenagers died from cancer,heart disease, AIDS, birth defect, stroke, pneumonia and influenza, and chronic lung diseasecombined; suicide was then ranked the third leading cause of death (CDC, 2001). In addition, thescope of this problem is even greater when suicidal attempts and other forms of risk taking behav-iors are considered. It is estimated that for every completed suicide there are as many as 50 to 150attempts (Dryfoos, 1990). Adolescent suicide is a major and universal problem; its prevalence,however, varies by race, nation, and culture. For example, relative to the United States, the suiciderates in Egypt, the Philippines, and Mexico are extremely low; at the opposite extreme, however,the rates in Germany, Austria, and Finland are exceptionally higher (Maris, Berman, & Silverman,2000).
The past decade has witnessed an extensive investigation into the underlying causes of sui-cidal behavior among adolescents. Nevertheless, despite researchers’ knowledge of certain riskfactors associated with adolescent suicidal behavior, little attempt has been made to integratefindings and to advance theoretical understanding of its etiology. To date, most research studiesfocus primarily on isolated or individualistic factors, and only few have examined interactionaldynamics; therefore, only limited progress has been made toward the goal of constructing a com-prehensive theory of life-threatening behavior (Berman, 1996).
Given this state of affairs, the purpose of this article is to present a framework to synthesizewhat is presently known about adolescent suicide, move beyond individualistic explanations, andtake into consideration the complex relationships between personal, interpersonal, and sociocul-tural factors influencing adolescent suicide. Accordingly, the ecological framework (Belsky, 1980;Bronfenbrenner, 1977; 1979) is used to examine the factors that have been mostly associated withadolescent suicidal behaviors at the ontogenic, microsystem, exosystem, and macrosystem levels.Ecological models have been proven useful in understanding a number of issues, such as sexual
Correspondence to: Huda Ayyash-Abdo, Lebanese American University, P.O. Box 13–15053, Chouran, Beirut 1102–2801. E-mail: [email protected]
Psychology in the Schools, Vol. 39(4), 2002 © 2002 Wiley Periodicals, Inc.Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pits.10042
459

revictimization (Grauerholz, 2000), stress in older adults (Weiss, 1995), child abuse and neglect(Tann & Ray, 1991), and alcoholism (Gacic, 1986). However, in the research to date, the ecolog-ical framework, with very few exceptions, has been rarely used to examine adolescent suicide(e.g., Henry & Stephenson, 1993). In addition, even when the ecological model was used tounderstand adolescent suicide, the focus was mainly on the family as a primary microsystem.
The Ecological Perspective
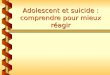
Bronfenbrenner’s (1977; 1979) developed an ecological model that places the individual atthe center of a series of complex systems: the microsystem, exosystem, and macrosystem, all inconcentric circles. The microsystem (e.g., family interactions) is the more immediate environmentand is embedded within the exosystem (e.g., the parental employment), which reflects indirectinfluences. The exosystem is in turn contained within a more distant layer, the macrosystem (e.g.,cultural norms). Belsky (1980) included the ontogenic system (Tinbergen, 1951) or person-oriented system, and consequently looked at the individual through the interaction of four systemsdepicted in four concentric circles: the ontogenic system, the microsystem, the exosystem, and themicrosystem, respectively (see Fig. 1).
Ontogenic development represents the demographic and psychological characteristics of ado-lescents that indicate increased risk for suicidal behaviors. The microsystem characterizes theimmediate forces of family, friends, religious group, and neighbors who influence adolescents’risk-taking behaviors. The exosytem refers to the “social structures (e.g., work places, neighbor-hood, residential setting) that do not themselves contain the developing person but impinge uponor encompass the immediate settings in which that person is found, and thereby influence, delimit,or even determine what goes on there” (Bronfenbrenner, 1977, p. 515). Finally, the macrosystem,the outer layer, involves the cultural and religious beliefs and values that increase the risk ofadolescent suicide through the influence they exert on ontogenic development, and the micro- andexosystems (Belsky, 1980).
Figure 1. Key suicide risk factors in an ecological paradigm.
460 Ayyash-Abdo

By applying this ecological model to the problem of adolescent suicide, the focus in thisarticle is on how factors at each of these four levels contribute to adolescent suicide and suicideattempt. The ecological approach, which integrates correlates of adolescent suicide in an inter-active and additive nature, is beneficial in a number of ways. First, the approach eschews from thetendency to focus on the adolescent’s personal history, such as depression, hopelessness, sub-stance abuse, etc. and depicts suicide as a result of an interaction among a number of factors(personal, interpersonal, and sociocultural) that are directly or indirectly related to adolescents. Itis beyond this scope of this article, however, to review all risk factors that have been found tocorrelate with adolescent suicide. Therefore, only key variables will be reviewed at each of thefour levels.
Factors Related to Adolescent Suicide
Ontogenic Factors
The ontogenic factors focus on the individuals’ psychological, historical, and medical char-acteristics that shape their response to the micro- and exosystems (Heise, 1998). Among the mostsignificant factors associated with adolescent suicidal behaviors are depression, hopelessness, andsubstance abuse.
Depression. Depression has been frequently reported as a correlate of suicide among ado-lescents who exhibit suicidal behavior (Brand, King, Olson, Ghaziuddin, & Naylor, 1996; Brent,Perper, Moritz, Baugher, et al., 1993; Marttunen, Aro, Henriksson, & Lonnqvist, 1991; Sadowski& Kelley, 1993). Research studies examining adolescents who make suicide attempts (e.g., Lewin-sohn, Rohde, & Seeley, 1994) as well as those who complete suicide (Brent et al., 1988; Shafferet al., 1996) report high proportion of youngsters suffering from depression. Adolescents withsuicide ideation also show symptoms of depression (Lewinsohn, Rohde, & Seeley, 1996). Mod-erate correlations, varying between .40 and .60, have been found in a number of research studiesexamining the relationship between depression and suicide ideation (e.g., Cole, 1989; Sadowski &Kelley, 1993). The relation, however, between depression and suicide is not as direct and simple asit seems. Not all youngsters who exhibit suicidal behaviors are depressed (Lewinsohn et al., 1996)nor are all depressed adolescents thinking of suicide.
Depression cannot be considered as an independent predictor of suicide for several reasons.First, because suicidal behavior is part of the symptomology for major depression in diagnosticsystems such as the Diagnostic and Statistical Manual of Mental Disorders IV (American Psychi-atric Association, 1994) and in the self-report and clinical interview measures of depression, asmall proportion of variance is added to the relationship between these two variables (Levy &Deykin, 1989). Second, the risk of suffering from a depressive disorder increases across the life-span, particularly between the ages of 9 and 19 (Maris, Berman, & Silverman, 2000). Accord-ingly, the high prevalence of depression among adolescents and young adults “limits the specificityof depressive disorders as a predictor of completed suicide” (Maris, Berman, & Silverman, 2000,p. 133). Depression in combination with other risk factors discussed below may increase the riskfor adolescent suicide behavior.
Hopelessness. Hopelessness, which refers to a negative attitude about future events, has beenthe subject of research by several investigators (e.g., Joiner & Rudd, 1996; Mazza & Reynolds,1998). Research has pointed to the association of hopelessness and suicidality in adults (e.g., Dyer& Kreitman, 1984), and a similar relationship has been inferred for adolescents (e.g., Beautrais,Joyce, & Mulder, 1999). Studies, however, of hopelessness, depression, and suicidal behaviorwithin clinical and nonclinical samples of adolescents have yielded inconsistent results (Cole,
Adolescent Suicide 461

1989; Lewinsohn, Rohde, & Seeley, 1994; Reifman & Windle, 1995; Rotheram-Borus & Traut-man, 1988). In a study of 281 high school students and 53 male juvenile delinquents, Cole (1989)found that hopelessness, especially among males, was not significantly related to suicidal ideationwhen depression was controlled for. Depression, however, remained an important predictor ofsuicidal ideation among males and females when hopelessness was controlled for. Similarly, Lewin-sohn, Rohde, and Seeley (1993) reported that hopelessness, along with other psychosocial vari-ables, were not related to previous suicide attempts when depression was statistically controlled.Somewhat different results were found by McLaughlin, Miller, and Warwick (1996) who reportedthat hopelessness is a more powerful predictor of adolescent suicidal behavior than depression.Hopelessness is associated with adolescent suicide, but more research is needed to investigatewhether hopelessness per se or depression accounts for this association.
Drug and Alcohol Abuse. There is considerable empirical evidence for the substantial sui-cidal risk associated with drug and alcohol abuse (e.g., Jones, 1997; Lyon et al., 2000). Psycho-logical autopsy studies of adolescents who completed suicide have reported the presence of ahistory of substance abuse as well as increased use at the time of the incident (e.g., Brent, Baugher,Bridge, Chen, Chiappetta, 1999; Shaffer et al., 1996). For example, Hawton, Fagg, and Mckeown(1989) found that 38% of adolescent suicide attempters had consumed alcohol within 6 hours priorto the attempt. Substance abuse, however, is more strongly associated with suicidal behavior thanwith suicidal ideation (Garrison, McKeown, Valois, & Vincent, 1993). Recently, Gould, Shaffer,Fisher, and Garfinkel (1998) noted the critical role of alcohol in even increasing the chances ofideators to make an actual suicide attempt.
Interaction of factors at the ontogenic level places the adolescent at a higher risk for attemptedand completed suicide. A number of research studies revealed that substance abuse comorbid withdepression illness increases the likelihood of occurrence of suicidal behavior and ideation (Brent,Baugher, et al., 1999; Brent, Perper, Moritz, Baugher, et al., 1993; Marttunen, Aro, Henriksson, &Lonnqvist, 1994) because alcohol impairs judgment, inhibits problem-solving ability, limits hopefor the future, and alters mood (Clark & Fawcett, 1992; Rogers, 1992). Thus, using alcohol torelieve depression and anxiety usually creates more depression and psychological distress, pro-ducing an effect labeled myopia (Steele & Joseph, 1990). Substance abuse comorbid with mooddisorder, particularly depression, allows for a 50-fold increased risk for suicide (Brent et al., 1999;Shaffer et al., 1996). The combination of alcohol and conduct disorder is also likely to representimportant suicide risk factor, especially for the males (Kelly & Lynch, 1999; Kelly, Lynch, Don-ovan, & Clark, 2001; Renaud, Brent, Birmaher, Chiappetta, & Bridge, 1999). In fact, Gould,Shaffer, Fisher, and Garfinkel (1998) found that substance abuse is correlated with suicide attemptsin adolescents and that the association of disruptive behavior disorders to suicide is mediated byan association with substance use disorders. Finally, although substance abuse is positively cor-related with suicide, it is not a leading contributor in and of itself.
Microsystem-Level Predictors
The above-mentioned ontogenic factors may interact with additional factors, and eventuallyplace adolescents at a higher risk to attempt suicide. The most immediate influences on adolescentsuicidal behaviors are within the microsystem and include those with whom adolescents haveimmediate contact, such as family, school, and peers. Accordingly, five key variables are reviewed:family history, loss, family dysfunction, peer, and schooling.
Family History. Among the risk factors that have been identified in the research studies ofadolescent suicidal behavior is a family history of suicide. Adolescents with one or more family
462 Ayyash-Abdo

members who have committed suicide are at a higher risk of attempting or completing suicide thanadolescents who do not have this family history (Brent et al., 1988; Brent, Perper, Moritz, Liotus,Schweers, et al., 1994; Bridge, Brent, Johnson, & Connolly, 1997; Gould, Fisher, Parides, Flory, &Shaffer, 1996; Gutierrez, King, & Ghaziuddin, 1996; Shaffi, Carrigan, Whittinghill, & Derick,1985). The reasons for multiple family suicides are still not known. These may be attributed to agenetic component (Schulsinger, 1980) rather than to a general index of family chaos and psycho-pathology because studies have shown that, after controlling for parental psychopathology andpoor parent–child relationships, a family history of suicidal behavior places adolescents at a higherrisk for suicide (Brent, 1996; Gould et al., 1996).
Parental psychopathology has also been implicated as a risk factor for suicidal behavior.Specifically, high rates of suicide, substance abuse, affective disorder, and antisocial disorders arecommonly found in the families of adolescent suicide completers, attempters and ideators (Brentet al., 1988; Brent et al., 1994; Fergusson & Lynskey, 1995; Fernquist, 2000; Lyon et al., 2000).In a case-control study, Brent and colleagues (1994) found that there was a higher incidence ofpsychiatric problems such as depression, substance abuse, and antisocial disorder among the par-ents of suicide attempters when compared with the parents of community controls. Results of thestudy also suggest a direct effect of parental psychopathology on increased suicidal behavioramong adolescents. The correlation between parental psychopathology and suicidal behavior wasstill high even after controlling for depression and substance abuse among suicidal adolescents.
Loss. Life stressors, particularly loss of someone who provides emotional, informationaland/or material support from death, separation, divorce or abandonment, have been associatedwith suicidal behavior among adolescents (Marttunen, Aro, & Lonnqvist, 1993; Brent, Perper,Moritz, Baugher et al., 1993; Gould, Shaffer et al., 1998; Wagner & Cole, 1995; Wichstrom,2000). In some studies, researchers have examined losses due to different causes (e.g. divorce,death, breaking up with a girlfriend or boyfriend) separately; others, however, have used a looserdefinition of “loss” variables and grouped adolescents who have experienced loss from any causetogether. Some psychological autopsy studies of representative samples of adolescents who havecommitted suicide have examined the relationship between loss, specifically divorce, and suicide(e.g., Brent et al., 1994; Brent, Perper, Moritz, Allan et al., 1993; Gould et al., 1996; Gould et al.,1998) and have yielded inconsistent results. While some studies have indicated that adolescentsuicide completers are more likely to come from a nonintact family of origin (e.g., Shaffi, Carri-gan, Whittinghill, & Derrick, 1985), others have found that separation or divorce do not signifi-cantly predict suicide attempts (Kovacs, Goldston, & Gatsonis, 1993; Reinherz et al., 1995).
There is emerging evidence, however, that divorce is much more likely to be a risk factor forsuicide if comorbid with other risk factors at the ontogenic level or with other microsystems.Some studies indicate that the additive effect of divorce and substance abuse places adolescents atan increased risk for suicide (e.g., Brent, Perper, Moritz, Baugher, et al., 1993). Others have alsofound that interaction of several microsystems such as divorce and parental psychopathology arestrongly associated with suicidal behavior (e.g., Gould et al., 1996). Finally, Wagner (1997) reportsthat parental separation or divorce, when considered apart from other losses, does not appear to bea significant risk factor for adolescent suicide. However, losses due to a number of causes—i.e.,loss to death, separation, divorce, and child placement outside home—may be a risk factor. Inaddition, early losses may play a significant role in the emergence of suicidal behavior.
Family Dysfunction. It is beyond doubt that family dysfunction has a negative effect on thechild’s personality and on the development of the adolescent’s ability to deal with problems. Ahigh frequency of family dysfunction in suicidal adolescents has been reported by a number of
Adolescent Suicide 463

researchers (Marttunen, Aro, & Lonnqvist, 1993; Marttunen, Aro, Henriksson, & Lonnqvist, 1994;Rozanes, Pearce, & Allison, 1995; Sokol-Katz, Dunham, & Zimmerman, 1997); however, thedefinition of family dysfunction has varied across studies. Some have considered family structure(Garfinkel, Froese, & Hood, 1982); others have examined communication patterns (Gould et al.,Shaffer, 1996), parent-child relationships (Brent, Perper, Moritz, Baugher et al., 1993), or levels offamily cohesion and conflict (Summerville, Kaslow, Abbate, & Cronan, 1994) as indicators offamily dysfunction. Among the most researched factors in areas of family dysfunction are nega-tive parent–child relationships and poor family communication patterns, both of which have beenassociated with suicidal behavior (Adams, Overholser, & Lehnert, 1994; Brent et al., 1994; Fer-gusson & Lynskey, 1995; Marttunen et al., 1994; Gould et al., 1996). Two large-scale studies withcommunity controls have provided information on parent-child relationships in families of suicidecompleters (Brent, Perper, Moritz, Baugher et al., 1993; Brent et al., 1994). In one of these studies,suicide victims, compared to community controls matched on demographics, showed higher ratesof parent–adolescent conflict beginning one year prior to the incident (Brent, Perper, Moritz,Baugher et al., 1993). Brent et al. (1994), however, found that parent–child conflict was not higheramong suicide victims after controlling for adolescent depression, conduct disorder, and substanceabuse. These findings may indicate that parent-adolescent relationship is associated with suicidal-ity indirectly through an association with psychopathology. Therefore, there is little evidence thatpoor parent–child relationship is a direct risk factor for completed suicide.
Studies that have examined parent–child relationships among suicide attempters and ideatorshave yielded somewhat different results. There is more consistent evidence that adolescent suicideattempters or ideators have more disturbed and conflictual relationships than community or clin-ical controls (Fergusson & Lynskey, 1995; Reinherz et al., 1995; Kelly et al., 2001; Summervilleet al., 1994). For example, in a 14-year longitudinal community study, Reinherz et al. (1995)examined the risk factors for adolescent suicidal ideation. Four hundred adolescents were fol-lowed between the ages of 5 and 18 years. Results revealed that female ideators were three timesmore likely than nonideators to report family violence between the ages 10 and 14. Both gendersperceived their family environment as poor, nonsupportive, and more volatile than those of non-ideators. Similarly, Mayhue and Kennedy (1990) reported that lower parental, both paternal andmaternal, closeness predicted suicidal ideation. Despite controlling for adolescent depression, theassociation between maternal closeness and suicidal ideation remained significant. Studies thathave also examined parent-child relationships as risk factors for suicide attempts have found thatlower levels of maternal emotional responsiveness are associated with higher risk for suicideattempts (Fergusson & Lynskey, 1995). In general, there is clear evidence that family functioningis important to consider in the assessment and treatment of suicidal behavior.
Peers. Adolescence is a period characterized by crucial needs for close friendships, emo-tional fulfillment, and emotional independence. During this developmental stage, adolescents turnto their peers for emotional support that was previously provided by their parents. They startsharing secrets, plans, and feelings and helping each other solve personal problems and interper-sonal conflicts. Loneliness, therefore, becomes one of the greatest problems during adolescence(Rice, 1999). A number of research studies have consistently reported that peer functioning is apredictor of depression (Aseltine, Gore, & Colten, 1998; Boivin, Poulin, & Vitaro, 1994; Panak &Garber, 1992), conduct problems, and substance abuse (Dishion, Capaldi, Spracklen, & Li, 1995),factors that have been previously cited as possible precursors to adolescent suicide. Other studieshave linked low levels of peer social support with suicidal ideation and behavior (Lewinsohnet al., 1993; Negron, Piacentini, Graae, Davies, & Shaffer, 1997; Prinstein, Boergers, Spirito,Little, & Grapentine, 2000; Wichstrom, 2000). Suicidal adolescents have been repeatedly profiled
464 Ayyash-Abdo

as more isolated than nonsuicidals; almost one third of adolescents who attempt suicide havereported being isolated from peers, breaking up with a boyfriend/girlfriend prior to the attempt,and/or lacking supportive friendships (e.g., Berman & Schwartz, 1990; Hawton, Fagg, & Simkin,1996). In a sample of 96 psychiatric inpatients, ages 12 to 17, Prinstein et al. (2000) examined theassociation between suicidal ideation and several dimensions of peer functioning, including closefriendship support, perceived peer acceptance and peer rejection, and deviant peer crowd affilia-tion. Results indicated that lack of friendship support and perceived peer rejection were directlyassociated with suicidal ideation while deviant peer affiliations were related to suicidal ideation,mediated by depression and substance abuse. In fact, several other studies support the associationof peer support with suicidal ideation or behavior via psychological impairment such as depres-sion (e.g., DiFilippo & Overholser, 2000; Reifman & Windle, 1995). Whether peer functioning isdirectly or indirectly related to suicide, problematic peer relations remain important risk factors tobe considered, especially when preventing suicidal behavior among at-risk youth.
Schooling. Poor school performance has been associated with adolescent suicidal behav-iors (e.g., Borowsky, Ireland, & Resnick, 2001; Lyon et al., 2000; McLaughlin, Miller, & War-wick, 1996; Querlat, 1993; Watt & Sharp, 2001). Borowsky et al. (2001) identified predictive aswell as protective factors against suicidal behavior among adolescents of different racial/ethnicgroups. Being held back a grade in school was among the predictive factors of suicide attempts.The authors also noted that academic achievement and perceived connectedness to school haveprotective effects against suicide, indicating that a sense of belonging and safety at school maydecrease the risk for suicide. Other scholars, however, reported finding no relationship betweenacademic achievement or school problems and suicidal behavior (DeMan & Leduc, 1993; Pfeffer,Zuckerman, Plutchik, & Mizruckhii, 1984). While research findings on the relation between schoolperformance and suicide are mixed, it appears that school performance in the presence of otherrisk factors at the ontogenic or within the microsystem level (e.g., family dysfunction, depression)place adolescents at a higher risk for suicide. For example, Lewinsohn, Rohde, and Seeley (1993)in a study of clinical populations found that suicide attempters had significantly lower level ofacademic achievement than nonattempters, suggesting a link between poor school performance,depression, and suicide attempts. On the other hand, a child’s belief that he or she is a failureincreases the risk of suicidal behavior. A child who is unable to develop healthy emotional secureattachment at home, failure at school may become a self-fulfilled prophecy; thus, validating lackof self-worth. Consequently, any drop of school grade when other warning signals coexist mayindicate a suicide risk (Orbach, 1988).
Exosystem-Level Predictors
Basic to an understanding of the ecological approach, is an appreciation of the embedednessof the individual and the family within larger social units. Therefore, the exosystem consists ofthose settings in which adolescents do not play a direct role but that nevertheless affects them. Oneof the most identified factors that may be of high risk factor for adolescents is the media.
Media. One of the examples of the indirect effect of exosystems on adolescents involvesthe media. Findings of several research studies indicate that media coverage on suicide, includingnewspaper articles (e.g., Ishii, 1991; Jonas, 1992; Stack, 1991; Wasserman, 1984), televisionreports (e.g., Bollen & Phillips, 1982; Phillips & Carstensen, 1986; Stack, 1993), and fictionalstories (Gould & Shaffer, 1986; Hawton et al., 1999), correlates with statistically significant increasein suicide rates. The increase becomes more pronounced when the amount of publicity given tothe suicide story is large (Bollen & Phillips, 1981; Phillips & Carstensen, 1986; Stack, 1987;
Adolescent Suicide 465

Wasserman, 1984). Furthermore, media coverage of a celebrity suicide has been found to have themost significant impact on adolescent suicidal behaviors, as it may inspire them to end their livesin a similar fashion (Berman, 1988; Stack, 1987; Wasserman, 1984). Cluster suicides may also bethe result of media coverage among adolescents because they are more sensitive than adults to theeffects of imitation (Bollen & Phillips, 1982; Phillips & Carstensen, 1986).
Even though many research studies indicate that media coverage of suicide stories is associ-ated with an increase in suicide rates, others have not found such an association (Jobes, Berman,O’Carroll, Eastgard, & Knickmeyer, 1996; Martin & Koo, 1996). For example, Jobes et al. (1996)did not find a significant increase in adolescent suicide following the media coverage of suicide ofKurt Cobain, a rock star. In fact, the authors suggested that Cobain’s death might have encouragedthe youth to seek help rather than to imitate his mortal behavior. Among the reasons that werefound to account for these results was the responsible job the news media did in reporting hisdeath. In general, there is more agreement that media coverage of suicide stories is more likely toaffect vulnerable adolescents who have a history of psychopathology, suicidal ideation, and/ortroubled home life (Graham, 1992; Wasserman, 1984). More research is needed to examine theeffect of recent media technology on adolescents’ suicidal behavior.
Macrosystem-Level Predictors
By exploring the larger culture in which the individual, the family, and the community areintermingled, the role of the macrosystem in adolescent suicide can be analyzed. Factors, such ascultural differences, ethnic differences, and adolescent population are examined.
Ethnic differences. Despite the substantial increase in suicides among African Americanadolescents from 1980–1995, research examining Black /White comparisons of suicidal behaviorhas consistently reported that African American youth have a suicide rate lower than most otherethnic groups (CDC, 1998; Maris et al., 2000). Black adolescents are definitely not protected fromspecific predictors of suicidal behavior; e.g., depression, substance abuse, hopelessness, and inter-personal conflict. In fact, Blacks in the United States have more social, economical, and psycho-logical frustration than Whites do; yet they have lower suicide rates. Few researchers have tried toexplain the reasons for the lower suicide rate among African Americans and the high suicide ratesamong Caucasians in a culturally relevant context. Most explanations are not of White suicides perse but, rather, of suicides of Blacks as contrasted with White suicides. Among the most commonlycited explanations for the low suicide rates of African Americans is the internal/external restrainttheory proposed by Henry and Short (1954). The theory suggests that African Americans are morelikely to blame others when personal frustration, depressive disorder, or social isolation occursand to externalize aggression in forms of homicides. Caucasians, however, are more likely toexperience guilt and to attribute adverse life situations to their personal inadequacies; as such,aggression is directed inwardly and takes the form of suicide. On the other hand, it was argued thatsuicide rates among African American are likely to increase as discrimination decreases (Kirk &Zucker, 1979); this view may explain the recent narrowing of the gap between suicide rates forBlack and White youths.
More recent research studies, however, have tried to identify the cultural values and world-views of African Americans that may act as protective factors for suicidal risk. One of the mostimportant protective factors that reduce suicidal risk for African Americans is religiosity (Early,1992; Gibbs, 1997; Stack & Wasserman, 1995). The church has long been a source of socialcohesion, social support, and stress reduction for the African American community (Billingsley,1992; Early, 1992; Gibbs, 1997) and, accordingly, has operated as a buffer against African Amer-icans opting for suicide. In addition, the extended family, which goes beyond blood relatives and
466 Ayyash-Abdo

includes friends and neighbors, has also provided African Americans with the emotional andsocial support they need to face adversities. Unlike Caucasians, a higher proportion of the elderlyin the African American community, for example, live with their extended family rather than innursing homes and take a major role as primary caretakers of children and adolescents (Gibbs,1997; Minkler & Roe, 1993). The presence of this strong social support system may be due tocommunalism, a cultural value which is prominent among African Americans and which empha-sizes the importance of interdependence and interconnectedness of people. Communalism dictatesthat the self is inherently connected with others, especially family members (Boykin & Ellison,1999). As a result, African Americans may share their problems and concerns with others and mayenjoy a sense of security knowing that they have others in their community to depend upon forsupport.
Cultural differences. Suicidal rates vary from one country to another. Countries with veryhigh suicide rates include Hungary, Austria, Denmark, and Finland while countries with low ratesinclude Egypt, the Philippines, Panama, Mexico, and Paraguay (Maris et al., 2000). The U.S.suicide rates are in the middle of international rankings. Research in the area of cross-culturalpsychology (Markus, Kitayama, & Heiman, 1996) suggests that cultural practices, beliefs, andvalues have a direct impact on suicidal behaviors as these practices may guide individuals incoping with difficult or stressful situations. A number of explanations have been posited to increaseunderstanding of the reasons for the present differential rates of suicidal behavior across cultures.
Among the most commonly cited explanations is that cultural differences in suicide comple-tions, attempts, and ideations may be a reflection of variations in the level of social support,belonging, and community support (Eckersley, 1993; Sanborn, 1990). Triandis, Kashima, Shimada,and Villareal (1986) have conceptualized societies along a spectrum that ranges from groups thathave an orientation toward individualism to those that have an orientation toward collectivism.Individualism has been defined as “the subordination of the goals of collectivities to individualgoals,” while collectivism involves the opposite, that is, “the subordination of the individual goalsto the goals of a collective.” (Hui & Triandis, 1986, p. 245). In collectivist cultures interdepen-dence, interconnectedness, and family integrity are emphasized; therefore, the self is viewed aspart of the group. In individualistic cultures, however, self-reliance, competition, and emotionaldetachment from in-groups are salient characteristics (Ayyash-Abdo, 2001). A number of researchstudies that have examined variation in suicidal ideation or attempts between Chinese (collectiv-ist) and American (individualist) college samples (Eshun, 2000; Zhang & Jin, 1996), and betweenGhanians (collectivist) and American samples (individualist) (Eshun, 1999, 2000); have consis-tently found that in collectivist cultures, Chinese and Ghanian, levels of suicidal behavior tend tobe lower than in the individualistic culture, American. Therefore, it was deduced that in collec-tivist cultures or cultures where there is de-emphasis on the individual as opposed to the group,with a corresponding emphasis on interdependence and interconnectedness suicide rates tend to below (e.g., Eckersley, 1993; Eshun, 2000; Sanborn, 1990; Shiang et al., 1997). Another explanationfor the differing suicide rates appears to be the different attitudes toward suicide each culture has.For example, in Africa there seems to be a general negative attitude toward suicide, that suicide innot acceptable regardless of life circumstances (Early & Akers, 1993), and that suicide victims areburied with less respect (Lester & Akande, 1994). In other countries, such as China, suicide isviewed as a disrespectful, harmful, as well as a shameful act to the victim’s family. Similarly, inSpanish-speaking countries individuals have a high regard for Catholicism and accordingly per-ceive suicide as an unacceptable act regardless of the circumstances. In addition, they believe thatdivine forces rather than personal control regulate the world; therefore, the person must acceptlife’s circumstances and not fight against them (Range et al., 1999).
Adolescent Suicide 467

Prevention and Interventions Within Ecological Systems
The ecological model has implications for prevention and treatment of the adolescent suicideproblem at each level. In this article, however, only few examples of intervention and preventionstrategies are set forth.
Organism-Level Interventions
Suicide is usually not spontaneous. Several behavioral and verbal warning signs can aidfamily members and school professionals such as teachers, principals, nurses, and psychologistsrecognize the potential for suicide among youth, and, accordingly, intervene before an actualattempt takes place. The American Academy of Child and Adolescent Psychiatry (1994) has iden-tified several behavioral clues that may indicate an increased risk for suicide. These are: changedeating habits; social withdrawal or isolation; unusual violent activity; running away; substanceabuse; unusual neglect of personal appearance; dramatic changes in personality; persistent bore-dom; difficulty concentrating and changes in school performance; frequent complaints about phys-ical symptoms that are often related to emotions, such as stomachaches, headaches, or fatigue;hopelessness; loss of interest in once-pleasurable activities; and inability to tolerate praise. Par-ents, caretakers, teachers, and all those who comprise the microsystems of youth can make refer-rals for therapy when adolescents express their wish to die, either through verbal hints or statementssuggesting despair or imminent departure or detailed plans about how to kill themselves, bydistributing or discarding cherished possessions, saying good-bye to family and friends, or byexpressing the feeling that others would be better off without them.
Upon the occurrence of a suicide attempt, intervention strategies can be planned by mentalhealth professionals to focus upon enhancing the coping and personal resources of youth. Researchhas revealed that hopelessness, problem-solving deficits, black-and-white thinking, cognitiverigidity, and the acceptance of suicide as a desirable solution are common cognitive characteristicsof suicidal adolescents. To this end, Cognitive Behavioral Therapy could be most effective withsuicidal adolescents (e.g., Berchick & Wright, 1992; Ellis & Newman, 1996; Trautman, 1995).Cognitive behavioral therapy is based on the idea that cognitive distortions, including selectiveabstraction, overgeneralization, dichotomous thinking, and magnification/minimization all of whichfound to be common cognitive characteristics of suicidal adolescents (e.g., Ellis & Newman,1996), can take place when people experience problems; these cognitions can maintain and exac-erbate difficulties (Beck, 1970; 1976; 1986). Therefore, increasing adolescents’ ability to generatealternative solutions to problems, identify positive consequences for solutions when confrontedwith problematic situations, and defuse black-and-white thinking become essential tools for cor-recting maladaptive thinking (Ellis & Newman, 1996; Maris et al., 2000). This can be accom-plished through engaging the adolescent in problem exploration, problem definition, generatingalternatives other than suicide to presenting problems, hypothesis testing, and conflict resolution.
Microsystem-Level Interventions
Prevention and intervention measures can also be taken through several microsystems. Sev-eral researchers have noted that family therapy is critical to the effective treatment of the suicidaladolescent (Catenaccio, 1995; Richman, 1992; Rotheram-Borus, Piacentini, Miller, Graae, & Castro-Blanco, 1994). ) because family problems often trigger suicidal behavior. One of the most crucialgoals of family therapy is the improvement of whole family functioning. This goal may be achievedin a number of ways designed to increase tolerance and flexibility, identify and resolve commu-nication problems, clarify dysfunctional alliances, reveal and accept previously held secrets, increasemutually rewarding behaviors among family members, and decrease punitive interactions among
468 Ayyash-Abdo

family members. In addition, parents may also be educated about the risk factors associated withadolescent suicide as well as the available resources to whom they can refer to in time of crisis(Maris et al., 2000).
Given the amount of time children and adolescents spend in school, it is logical that a numberof prevention programs are school-based. Among the most prominent suicide prevention programsthat have been implemented are curriculum programs presented to students. The major goals ofsuch programs are to (1) increase students’ awareness of suicidal behavior, (2) help studentsidentify warning signs of suicide, and (3) provide students with information about mental healthresources and how to access them (Kalafat & Elias, 1994; Shaffer, Garland, Gould, Fisher, &Trautman, 1990). Curriculum or education programs, when presented to students, have producedmixed results. Some research studies that have evaluated the effectiveness of such preventionstrategy have reported an increase in knowledge (Kalafat & Elias, 1994; Kalafat & Gagliano,1996; Overholser, Hemstreet, Spirito, & Vyse, 1989; Spirito, Overholser, Ashworth, Morgan &Benedict-Drew, 1988) and help-seeking behavior (Ciffone, 1993). For example, Hennig, Crabtree,and Baum (1998) have found that students who participated in a program about no-suicide con-tracting were better able to identify warning signs or symptoms of suicide in others and interveneappropriately with peers than the control group. In one study, however, suicidal students reactedmore negatively than nonsuicidals to a prevention program (Shaffer et al., 1990); the subjects ofthis study reported that they would not recommend the program to other students and that expo-sure to such programs may increase the risk of some students to actually try to kill themselves.Although suicide education programs appear, in general, to modify attitudes to suicidal behaviorseveral limitations should be noted.
First, such programs may be effective in increasing awareness or transmitting knowledge butinformation alone is not sufficient to modify behavior (Garland & Zigler, 1993). Second, thecontent of such programs may accidentally increase imitation (Velting & Gould, 1997). In addi-tion, most suicide prevention programs use a universal strategy, targeting all students rather thanat-risk students alone; however, most needy students are least likely to attend or be responsive tosuch programs (Westefeld et al., 2000). To this end, skills-training programs have been developedto help at-risk adolescents acquire the skills that unable them to manage depression, anger andaggression, or loneliness and improve their competencies such as decision making, social skills,and problem solving skills (Berman & Jobes, 1995). A number of research studies that haveevaluated the effectiveness of these programs have yielded positive results, encouraging the use ofsuch programs (e.g., Eggert, Thompson, Herring, & Nicholas, 1995; Zenere & Lazarus, 1997).
Exosystem-Level Interventions
Although direct intervention strategies are most commonly implemented at the ontogenic andmicrosystem levels, indirect intervention opportunities are available at the exosystem level. Forexample, news media professionals can also help in the adolescent suicide prevention process; asresearch indicates an association between media reports about suicide and suicidal behavior. TheCDC (1994) has developed a set of guidelines in an effort to minimize the negative and potentialcontagious impact of publicity about suicide. In general, these guidelines suggest that mediacoverage of a suicide should not be portrayed in such a way that the victim or the suicidal act isglorified; glorification could be minimized by revealing the negative as well as the positive qual-ities of the deceased person. Second, the suicidal act should be explicitly described as a result ofseveral events rather than of one simple precipitating factor. Third, detailed information regardingthe method used to commit suicide should be avoided. Fourth, sensationalizing the suicide byexcessive reporting of the suicidal act or the deceased may increase the occurrence of a copycat
Adolescent Suicide 469

attempt among at-risk individuals. Therefore, media professionals may take an active role in theprevention process if they adopt the CDC (1994) guidelines.
Macrosystem-Level Interventions
In most countries, guns are the primary suicide weapons. In the United States, for example,firearms are the most common method of suicide among males as well as females (Maris et al.,2000) and ownership has been only occasionally restricted. Research indicates that the suicide rateis positively correlated with the production, sales, and ownership of guns (Kellerman & Reay,1986) and negatively correlated with strict ownership laws (e.g., Leenaars et al., 2000). Accord-ingly, at the macro level, policymakers can have an important role in the prevention of adolescentsuicide when they set strict firearm control laws.
Conclusion
Previous research studies have placed strong emphasis on individualistic risk factors associ-ated with adolescent suicide; however, factors studied in isolation are usually not useful in pre-dicting suicidal risk. To this end, this study has tried to move from individualistic explanations ofsuicidal behaviors among adolescents because it is crucial to understand that any suicidal outcomeis a complex, multidomain, interactive effect of many factors over fairly long periods of time.Therefore, none of the commonly cited risk factors are definite signs of suicide. The model pro-posed in this article, based on the ecological perspective, specifically, the one refined by Belsky(1980), depicts four levels of analysis: the ontogenic development or personal history, the micro-systems, the exosystems, and the macrosystems. This model allowed greater understanding of theadolescent suicide problem as complex relationships between personal, interpersonal, and socio-cultural factors influencing adolescent suicidal behavior. As such, existing research from a varietyof areas has been integrated to allow understanding of the complexity of the suicide problem. Inaddition, examples of intervention and prevention strategies have also been proposed. These strat-egies encourage the active collaboration of parents, peers, teachers, school administrators, andmental health professionals in the helping process. In fact, as responsible members of society,school psychologists have the greatest capability in developing their knowledge about the extentof adolescent suicide, the risk factors associated with suicide, and the appropriate interventiontechniques. “Their overall knowledge regarding suicide may determine the school’s success inproviding assistance to at-risk students” (King, 2000, p. 260). In conclusion, the work presentedhere should be viewed as a step toward integrating findings on adolescent suicide that can guidefuture empirical work.
References
Adams, D.M., Overholser, J.C., & Lehnert, K.L. (1994). Perceived family functioning and adolescent suicidal behavior.Journal of the American Academy of Child and Adolescent Psychiatry, 33, 498–530.
American Academy of Child and Adolescent Psychiatry. (1994). Facts for teachers: Teen suicide. Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington,DC: Author.
Aseltine, R.H., Gore, S., & Colten, M.E. (1998). The co-occurrence of depression and substance abuse in late adolescence.Development and Psychopathology, 10, 549–570.
Ayyash-Abdo, H. (2001). Individualism and collectivism: The case of Lebanon. Social Behavior and Personality, 29,503–518.
Beautrais, A., Joyce, P., & Mulder, R. (1999). Personality traits and cognitive styles as risk factors for serious suicideattempts among young people. Suicide and Life-Threatening Behavior, 29, 37– 47.
Beck, A.T. (1970). Cognitive therapy. Cognitive Therapy, 1, 184–200.
Beck, A.T. (1976). Cognitive therapy and emotional disorders. New York: International Universities Press.
470 Ayyash-Abdo

Beck, A.T. (1986). Hopelessness as a predictor of eventual suicide. In J.J. Mann, & A. Stanley (Eds.), Psychobiology. NewYork: Academy of Sciences.
Belsky, J. (1980). Child maltreatment: An ecological integration. American Psychologist, 35, 320–335.Berchick, R.J., & Wright, F.D. (1992). Guidelines for handing the suicidal patient: A cognitive perspective. In B. Bongar
(Ed.), Suicide: Guidelines for assessment, management, and treatment. New York: Oxford University Press.Berman, A.L., (1988). Fictional depiction of suicide in television films and imitation effects. American Journal of Psychi-
atry, 145, 982–986.Berman, A.L. (1996). Dyadic death: A typology. Suicide and Life-Threatening Behavior, 26, 342–350.Berman, A.L., & Jobes, D.A. (1995). Suicide prevention in adolescents (age 12–18). Suicide and Life Threatening Behav-
ior, 25, 143–154.Berman, A.L., & Schwartz, R.H. (1990). Suicide attempts among adolescent drug users. American Journal of Diseases of
Children, 144, 310–314.Billingsley, A. (1992). Climbing Jacob’s ladder: The enduring legacy of African-American families. New York: Simon &
Schuster.Bollen, K.A., & Phillips, D.P. (1981). Suicidal motor vehicle fatalities in Detroit: A replication. American Journal of
Sociology, 87, 404– 412.Bollen, K.A., & Phillips, D.P. (1982). Imitative suicides: A national study of the effect of television news stories. American
Sociological Review, 47, 802–809.Boivin, M., Poulin, F., & Vitaro, F. (1994). Depressed mood and peer rejection in childhood. Development and Psycho-
pathology, 6, 483– 498.Borowsky, I.W., Ireland, M., & Resnick, M.D. (2001). Adolescent suicide attempts: Risk and protectors. Pediatrics, 107,
485– 496.Boykin, A.W., & Ellison, C.M. (1999). The multiple ecologies of black youth socialization: An Afigraphic analysis. In R.
Taylor (Ed.), African American youth: Their social and economic status in the United States. Westport CT: Green-wood Press.
Brand, E.F., King, C.A., Olson, E., Ghaziuddin, N., & Naylor, M. (1996). Depressed adolescents with a history of sexualabuse: Diagnostic comorbidity and suicidality. Journal of the American Academy of Child and Adolescent Psychiatry,35, 34– 41.
Brent, D.A. (1996). Familial factors in suicide and suicidal behavior. Lifesavers: The Quarterly Newsletter of the Amer-ican Suicide Foundation, 8, 2–3.
Brent, D.A., Baugher, M., Bridge, J., Chen, T., & Chiappetta, L. (1999). Age- and sex-related risk factors for adolescentsuicide. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 1497–1516.
Brent, D.A., Perper, J.A., Goldstein, C., Kolko, D., Alan, M., Allman, C., & Zelenak, J. (1988). Risk factors for adolescentsuicide: A comparison of adolescent suicide victims with suicidal inpatients. Archives of General Psychiatry, 45,581–588.
Brent, D.A., Perper, J.A., Moritz, G., Allan, C., Friend, A., Roth, B.S., Schweers, J., Balach, L., & Baugher, M. (1993).Psychiatric risk factors for adolescent suicide: A case control study. Journal of the American Academy of Child andAdolescent Psychiatry, 32, 521–529.
Brent, D.A., Perper, J.A., Moritz, G., Baugher, M., Roth, C., Balach, L., & Schweers, J. (1993). Stressful live events,psychopathology, and adolescent suicide: A case control study. Suicide and Life-Threatening Behavior, 23, 179–187.
Brent, D.A., Perper, J.A., Moritz, G., Liotus, L., Schweers, J., Balach, L., & Roth, C. (1994). Familial risk factors foradolescent suicide: A case control study. Acta Psychiatrica Scandinavica, 89, 52–58.
Bridge, J.A., Brent, D.A., Johnson, B.A., & Connolly, J. (1997). Familial aggregation of psychiatric disorders in a com-munity sample of adolescents. Journal of the American Academy of child and Adolescent Psychiatry, 36, 628– 637.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32, 513–531.
Bronfenbrenner, U. (1979). The ecology of human development. Cambridge, MA: Harvard University Press.
Catenaccio, R. (1995). Crisis intervention with suicidal adolescents: A view from the emergency room. In J.K. Zimmerman& G.M. Asnis (Eds.), Treatment-approaches with suicidal adolescents (pp. 71–90). New York: Wiley.
Center for Disease Control and Prevention. (1995, April). Suicide among children, adolescents, and young adults: UnitedStates, 1980–1992. Morbidity and Mortality Weekly Report, 44, 289–291.
Center for Disease Control and Prevention. (1994). Suicide contagion and the reporting of suicide: Recommendationsfrom a national workshop. Morbidity and Mortality Weekly Report, 42, 13–18.
Center for Disease Control and Prevention. (1998, April). Suicide among Black youths: United States, 1980–1995. Mor-bidity and Mortality Weekly Report, 47, 289–291.
Center for Disease Control and Prevention. (2001, August 3). Suicide in the United States. Retrieved September 12, 2001,from http://www.cdc.gov/ncip/factsheets/suifacts.htm
Ciffone, J. (1993). Suicide prevention: A classroom presentation to adolescents. Social Work, 98, 196–203.
Adolescent Suicide 471

Clark, D.C., & Fawcett, J. (1992). An empirically based model of suicide risk assessment for patients with affectivedisorder. In D. Jacobs (Ed.), Suicide and clinical practice (pp. 55–73). Washington, DC: American Psychiatric Press.
Cole, D.A. (1989). Psychopathology of adolescent suicide: Hopelessness, coping beliefs, and depression. Journal of Abnor-mal Psychology, 98, 248–255.
DeMan, A., & Leduc, C.P. (1993). Correlates of suicidal ideation in French-Canadian adolescents: Personal variables,stress, and social support. Adolescence, 28, 112–123.
DiFilippo, J.M., & Overholser, J.C. (2000). Suicidal ideation in adolescent psychiatric inpatients as associated with depres-sion and attachment relationships. Journal of Clinical Child Psychology, 29, 155–166.
Dishion, T.J., Capaldi, D., Spracklen, K.M., & Li, F. (1995). Peer ecology of male adolescent drug use. Development andPsychopathology, 7, 803–824.
Dryfoos, J.G. (1990). Adolescents at risk. New York: Oxford University Press.
Dyer, J.A.T., & Kreitman, A. (1984). Hopelessness, depression and suicidal intent in parasuicide. British Journal of Psy-chiatry, 144, 127–133.
Early, K.E. (1992). Religion and suicide in the African-American community. Westport, CT: Greenwood Press.
Early, K.E., & Akers, R.L. (1993). “It’s a White thing”: An exploration about beliefs about suicide in the African-Americancommunity. Deviant Behavior, 14, 227–296.
Eckersley, R. (1993). Failing a generation: The impact of culture on the health and well being of youth. Journal ofPediatrics & Child Health, 29, 516–519.
Eggert, L.L., Thompson, E.A., Herring, J.R., & Nicholas, L.J. (1995). Reducing suicide potential among high-risk youth:Tests of a school-based prevention program. Suicide and Life-Threatening Behavior, 25, 276–296.
Ellis, T.E., & Newman, C.F. (1996). Choosing to live: How to defeat suicidal behavior through cognitive therapy. Oakland,CA: New Harbinger.
Eshun, S. (1999). Cultural variations in hopelessness, optimism, and suicidal ideation: A study of Ghana and U.S. collegesamples. Cross-Cultural Research, 33, 227–238.
Eshun, S. (2000). Role of gender and rumination in suicide ideation. Cross-Cultural Research, 34, 250–264.
Fergusson, D.M., & Lynskey, M.T. (1995). Childhood circumstances, adolescent adjustment and suicide attempts in a NewZealand birth cohort. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 612– 622.
Fernquist, R.M. (2000). Problem drinking in the family and youth suicide. Adolescence, 35, 551–558.
Gacic, B. (1986). An ecosystem approach to alcoholism: Theory and practice. Contemporary Family Therapy, 8, 264–278.
Garfinkel, B.D., Froese, A., & Hood, J. (1982). Suicide attempts in children and adolescents. American Journal of Psychi-atry, 139, 1257–1261.
Garland, A., & Zigler, E. (1993). Adolescent suicide prevention: Recent research and social policy implications. AmericanPsychologist, 48, 169–182.
Garrison, C.Z., McKeown, R.E., Valois, R.F., & Vincent, M.L. (1993). Aggression, substance use, and suicidal behaviorsin high school students. American Journal of Public Health, 83, 179–184.
Gibbs, J.T. (1997). African American suicide: A cultural paradox. Suicide and Life-Threatening Behavior, 27, 68–79.
Gould, M.S., Fisher, P., Parides, M., Flory, M., & Shaffer, D. (1996). Psychosocial risk factors of child and adolescentcompleted suicide. Archives of General Psychiatry, 53, 1155–1162.
Gould, M.S., Shaffer, D., Fisher, P., & Garfinkel, R. (1998). Separation/divorce and child and adolescent completedsuicide. Journal of the American Academy of Child and Adolescent Psychiatry, 37, 155–163.
Gould, M.S., & Shaffer, D. (1986). The impact of suicide in television movies: Evidence of imitation. New EnglandJournal of Medicine, 315, 690– 694.
Graham, M. (1992). Adolescent suicide: Imitation and the clustering phenomenon. Youth Studies, 11, 28–32.
Grauerholz, L. (2000). An ecological approach to understanding sexual revictimization: Linking, personal, interpersonal,and sociocultural factors and processes. Child Maltreatment, 5, 5–28.
Gutierrez, P., King, C., & Ghaziuddin, N. (1996). Adolescent attitudes about death in relation to suicidality. Suicide &Life-Threatening Behavior, 26, 8–16.
Hawton, K., Fagg, J., & McKeown, S.P. (1989). Alcoholism, alcohol and attempted suicide. Alcohol and Alcoholism, 24,3–9.
Hawton, K., Fagg, J., & Simkin, S. (1996). Deliberate self-poisoning and self-injury in children and adolescents under 16years of age in Oxford 1976–1993. British Journal of Psychiatry, 169, 202–208.
Hawton, K., Simkin, S., Deeks, J.J., O’Connor, S., Keen, A., Altman, D.G., Philo, G., & Bulstrode, C. (1999). Effects of adrug overdose in a television drama on presentations to hospital for self poisoning: Times series and questionnairestudy. British Medical Journal, 318, 972–977.
Heise, L. (1998). Violence against women: An integrated ecological framework. Violence Against Women, 4, 262–290.
472 Ayyash-Abdo

Hennig, C.W., Crabtree, C.R., & Baum, T. (1998). Peer contracting as a response to potential suicide in adolescents.Archive of suicide research, 4, 169–187
Henry, A.F., & Short, J.F. (1954). Suicide and homicide. New York: Free Press.
Henry, C.S., & Stephenson, A. (1993). Adolescent suicide and families: An ecological approach. Adolescence, 28, 291–310.
Hui, C.H., & Triandis, H.C. (1986). Individualism-collectivism: A study of cross-cultural perspectives. Lincoln: NebraskaUniversity Press.
Ishii, K. (1991). Measuring mutual causation: Effect of suicide news on suicide in Japan. Social Science Research, 20,188–195.
Jobes, D.A., Berman, A.L., O’Carroll, P.W., Eastgard, S., & Knickmeyer, S. (1996). The Kurt Cobain suicide crisis.Suicide and Life-Threatening Behavior, 17, 310–325.
Joiner, T.E., & Rudd, M.D. (1996). Disentangling the interrelations between hopelessness, loneliness and suicidal ideation.Suicide and Life-Threatening Behavior, 26, 19–26.
Jonas, K. (1992). Modeling and suicide: A test of the Werther effect. British Journal of Social Psychology, 31, 295–306.
Jones, G.D. (1997). The role of drugs and alcohol in urban minority adolescent suicide attempts. Death Studies, 21,189–203.
Kalafat, J., & Elias, M. (1994). An evaluation of a school-based suicide awareness intervention. Suicide and Life-Threatening Behavior, 22, 315–321.
Kalafat, J., & Gagliano, C. (1996). The use of simulations to assess the impact of an adolescent suicide response curricu-lum. Suicide and Life-Threatening Behavior, 26, 359–364.
Kellerman, A.L., & Reay, D.T. (1986). Protection or peril? An analysis of firearm-related deaths in the home. New EnglandJournal of Medicine, 327, 467– 472.
Kelly, T.M., & Lynch, K.G. (1999). Suicidal behaviors in alcohol and conduct disordered adolescents. Alcoholism: Clin-ical and Experimental Research, 23, 125–137.
Kelly, T.M., Lynch, K.G., Donovan, J.E., & Clark, D.B. (2001). Alcohol use disorders and risk factor interaction foradolescent suicidal ideation and attempts. Suicide and Life-Threatening Behavior, 31, 181–193.
King, K.A. (2000). Preventing adolescent suicide: Do high school counselors know the risk factors? Professional SchoolCounseling, 3, 255–263.
Kirk, A., & Zucker, R. (1979). Some sociopsychological factors in attempted suicide among urban Black males. Suicideand Life-Threatening Behavior, 9, 76–86.
Kovacs, M., Goldston, D., & Gatsonis, C. (1993). Suicidal behaviors and childhood-onset depressive disorders: A longi-tudinal investigation. Journal of the American Academy of Child and Adolescent Psychiatry, 32, 8–20.
Leenaars, A., Cantor, C., Connolly, J., EchoHawk, M., Gailiene, D., Xiong He, Z., Kokorina, N., Lester, D., Lopatin, A.,Rodriguez, M., Schlebusch, L., Takahashi, Y., Vijayakumar, L., & Wenckstern, S. (2000). Controlling the environ-ment to prevent suicide: International perspectives. Canadian Journal of Psychiatry, 45, 639– 644.
Lester, D., & Akande, A. (1994). Attitudes about suicide among Yoruba of Nigeria. Journal of Social Psychology, 134,851–854.
Levy, J.C., & Deykin, E.Y. (1989). Suicidality, depression and substance abuse in adolescence. American Journal ofPsychiatry, 32, 60– 68.
Lewinsohn, P.M., Rohde, P., & Seeley, J.R. (1993). Psychosocial characteristics of adolescents with a history of suicideattempt. Journal of the American Academy of Child and Adolescent Psychiatry, 32, 60– 68.
Lewinsohn, P.M., Rohde, P., & Seeley, J.R. (1994). Psychosocial risk factors for future adolescent suicide attempts. Journalof Consulting and Clinical Psychology, 62, 297–305.
Lewinsohn, P.M., Rohde, P., & Seeley, J.R. (1996). Adolescent suicidal ideation and attempts: Prevalence, risk factors, andclinical implications. Clinical Psychology: Science and Practice, 3, 25–36.
Lyon, M.E., Benoit, M., O’Donnell, R.M., Getson, P.R., Silber, T., & Walsh, T. (2000). Assessing African Americanadolescents risk for suicide attempts: Attachment theory. Adolescence, 35, 121–134.
Maris, R.W., Berman, A.L., & Silverman, M.M. (2000). Comprehensive textbook of suicidology. New York: GuilfordPress.
Markus, H.R., Kitayama, S., & Heiman, R.J. (1996). Culture and “basic” psychological principles. In E.T. Higgins & A.W.Kruglanski (Eds.), Social psychology: Handbooks of basic principals (pp. 857–913). New York: Guilford Press.
Martin, G., & Koo, L. (1996). Celebrity suicide: Did the death of Kurt Cobain influence young suicides in Australia?Archives of Suicide Research, 3, 187–198.
Marttunen, M.J., Aro, H.M., & Lonnqvist, J.K. (1993). Precipitant stressors in adolescent suicide. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 32, 1178–1183.
Marttunen, M.J., Aro, H.M., Henriksson, M.M., & Lonnqvist, J.K. (1991). Mental disorders in adolescent suicide. Archivesof General Psychiatry, 48, 834–839.
Adolescent Suicide 473

Marttunen, M.J., Aro, H.M., Henriksson, M.H., & Lonnqvist, J.K. (1994). Psychosocial stressors more common in ado-lescent suicides with alcohol abuse compared with depressive adolescent suicides. Journal of the American Academyof Child and Adolescent Psychiatry, 33, 490– 497.
Mayhue, L.K., & Kennedy, R.E. (1990, March). Longitudinal changes in parent–child relations as precursors of suicidalideation in mid-adolescence. Paper presented at the biennial meetings of the Society for Research in Adolescence,Atlanta, GA.
Mazza, J., & Reynolds, W. (1998). A Longitudinal investigation of depression, hopelessness, social support, and major andminor life events and their relations to suicidal ideation in adolescents. Suicide and Life-Threatening Behavior, 28,358–374.
McLaughlin, J., Miller, R., & Warwick, H. (1996). Deliberate self-harm in adolescents: Hopelessness, depression, andproblem solving. Journal of Adolescence, 19, 523–532.
Minkler, M., & Roe, K.M. (1993). Grandmothers as caregivers: Raising children of the crack cocaine epidemic. NewburyPark, CA: Sage.
Negron, R., Piacentini, J., Graae, F., Davies, M., & Shaffer, D. (1997). Microanalysis of adolescent suicide attempters andideators during the acute suicidal episode. Journal of the American Academy of Child and Adolescent Psychiatry, 36,1512–1519.
Orbach, I. (1988). Children who don’t want to live: Understanding and treating the suicidal child. San Francisco: Jossey-Bass Publishers.
Overholser, J.C., Hemstreet, A.H., Spirito, A., & Vyse, S. (1989). Suicide awareness programs in the schools: Effects ofgender and personal experience. Journal of the American Academy of Child and Adolescent Psychiatry, 28, 925–930.
Panak, W.F., & Garber, J. (1992). Role of aggression, rejection, and attributions in the prediction of depression in children.Development and Psychopathology, 4, 145–165.
Pfeffer, C.R., Zuckerman, S., Plutchik, R., & Mizrucki, M. (1984). Suicidal behavior in normal school children: A com-parison with child psychiatric inpatients. American Academy of Child Psychiatry, 23, 416– 423.
Phillips, D., & Carstensen, L.L. (1986). Clustering of teenage suicide after television news stories about suicide. NewEngland Journal of Medicine, 315, 685– 689.
Prinstein, M.J., Boergers, J., Spirito, A., Little, T., & Grapentine, W.L. (2000). Peer functioning, family dysfunction, andpsychological symptoms in a risk factor model for adolescent inpatients’ suicidal ideation survey. Journal of ClinicalChild Psychology, 29, 392– 406.
Queralt, M. (1993). Risk factors associated with completed suicide in Latino adolescents. Adolescence, 28, 831–851.Range, L., Leach, M., MacIntyre, D., Posey-Deters, P., Marion, M., Kovac, S., Banos, H., & Vigil, J. (1999). Multicultural
perspectives on suicide. Aggression and Violent Behavior: A Review Journal, 4, 413– 430.Reifman, A., & Windle, M. (1995). Adolescent suicidal behavior as a function of depression, hopelessness, alcohol use,
and social support: A longitudinal investigation. American Journal of Community Psychology, 23, 329–354.Reinherz, H.Z., Giaconia, R.M., Silverman, A.B., Friedman, A., Pakiz, B., Frost, A.K., & Cohen, E.K. (1995). Early
psychosocial risks for adolescent suicidal ideation and attempts. Journal of the American Academy of Child andAdolescent Psychiatry, 34, 599– 611.
Renaud, J., Brent, D.A., Birmaher, B., Chiappetta, L., & Bridge, J. (1999). Suicide in adolescents with disruptive disorders.Journal of the American Academy of Child and Adolescent Psychiatry, 38, 846–851.
Rice, P. (1999). The adolescent: Development, relationships, and culture (9th ed.). Boston: Allyn and Bacon.Richman, J. (1992). The management of risk and the risk of management of the family in therapy with suicidal patients.
Unpublished manuscript.Rogers, J.R. (1992). Suicide and alcohol. Journal of Counseling and Development, 70, 540–543.Rotheram-Borus, M.J., Piacentini, J., Miller, S., Graae, F., & Castro-Blanco, D. (1994). Brief cognitive-behavioral treat-
ment for adolescent suicide attempters and their families. Journal of the American Academy of Child and AdolescentPsychiatry, 34, 81–90.
Rotheram-Borus, M.J., & Trautman, P.D. (1988). Hopelessness, depression, and suicide intent among adolescent suicideattempts. Journal of the American Academy of Child and Adolescent Psychiatry, 27, 700–704.
Rozanes, M.G., Pearce, C., & Allison, S. (1995). Adolescent suicide, depression and family dysfunction. Acta PsychiatricaScandinavica, 92, 336–344.
Sadowski, C., & Kelley, M.L. (1993). Social problem-solving in suicidal adolescents. Journal of Consulting and ClinicalPsychology, 61, 121–127.
Sanborn, C.J. (1990). Gender socialization and suicide: American Association of Suicidology presidential address, 1989.Suicide and Life Threatening Behavior, 20, 148–155.
Schulsinger, F. (1980). Biological psychopathology. Annual Review of Psychology, 31, 583– 606.Shaffer, D., Garland, A., Gould, M., Fisher, P., & Trautman, P. (1990). Preventing teenage suicide: A critical review. In S.
Chess, & M.E. Hertzig (Eds.), Annual progress in child psychiatry and child development, 1989. New York:Brunner/Mazel.
474 Ayyash-Abdo

Shaffer, D., Gould, M.A., Fisher, P., Trautman, P., Moreau, D., Kleinman, M., & Flory, M. (1996). Psychiatric diagnosis inchild and adolescent suicide. Archives of General Psychiatry, 53, 339–348.
Shaffi, M., Carrigan, S., Whittinghill, J.R., & Derrick, A.M. (1985). Psychological autopsy of completed suicide in childrenand adolescents. American Journal of Psychiatry, 142, 1061–1964.
Shiang, J., Blinn, R., Bongar, B., Stephens, B., Allison, D., & Schatzberg, A. (1997). Suicide in San Francisco, CA: Acomparison of Caucasians and Asian groups, 1987–1994. Suicide and Life-Threatening Behavior, 27, 80–91.
Sokol-Katz, J., Dunham, R., & Zimmerman, R. (1997). Family structure versus parental attachment in controlling adoles-cent deviant behavior: A social control model. Adolescence, 32, 199–215.
Spirito, A., Overholser, J., Ashworth, S., Morgan, J., & Benedict-Drew, R. (1988). Evaluation of a suicide awarenesscurriculum for high school students. Journal of the American Academy of Child and Adolescent Psychiatry, 27,705–711.
Stack, S.A. (1991). Social correlates of suicide by age: Media impacts. In A.A. Leenaars (Ed.), Life span perspectives ofsuicide: Time-lines in the suicide process (pp. 187–213). New York: Plenum press.
Stack, S.A. (1993). The media and suicide: A nonadditive model, 1968–1980. Suicide and Life Threatening Behavior, 23,63– 66.
Stack, S. (1987). Celebrities and suicide: A taxonomy and analysis, 1948–1983. American Sociological Review, 52,401– 412.
Stack, S., & Wasserman, I. (1995). Effect of marriage, family, and religious ties on African American suicide ideology.Journal of Marriage and the Family, 57, 215–222.
Steele, C.M., & Joseph, R.A. (1990). Alcohol myopia. American Psychologist, 45, 921–933.Summerville, M.B., Kaslow, N.J., Abbate, M.F., & Cronan, S. (1994). Psychopathology, family functioning, and cognitive
style in urban adolescents with suicide attempts. Journal of Abnormal Child Psychology, 22, 221–235.Tann, G.G., & Ray, M.P. (1991). Migrant farm child abuse and neglect within an ecosystem framework. Family Relations,
40, 84–90.Tinbergen, N. (1951). The study of instinct. Oxford, UK: Oxford University Press.Trautman, P.D. (1995). Cognitive behavior therapy of adolescent suicide attempters. In J.K. Zimmerman & G.M. Asnis
(Eds.), Treatment approaches with suicidal adolescents. New York: Wiley.Triandis, H., Kashima, Y., Shimada, E., & Villareal, M. (1986). Acculturation indices as a means of confirming cultural
differences. International Journal of Psychology, 21, 43–70.Velting, D.M., & Gould, M.S. (1997). Suicide contagion. In R.W. Maris, M.M. Silverman, & S. Canetto (Eds.), Review of
suicidology, 1997. New York: Guilford Press.Wagner, B.M. (1997). Family risk factors for child and adolescent suicidal behavior. Psychological Bulletin, 121, 246–298.Wagner, B.M., & Cole, R. (1995). Psychosocial correlates of suicide attempts among junior and senior high school youth.
Suicide and Life-Threatening Behavior, 25, 358–367.Wasserman, I.M. (1984). Imitation and suicide: A re-examination of the Werther effect. American Sociological Review, 49,
427– 436.Watt, T.T., & Sharp, S.F. (2001). Gender differences in strains associated with suicidal behavior among adolescents.
Journal of Youth and Adolescence, 30, 333–348.Weiss, J.C. (1995). Cognitive therapy and life review therapy: Theoretical and therapeutic implications for mental health
counselors. Journal of Mental Health Counseling, 17, 157–174.Westefeld, J.S., Range, L.M., Rogers, J.R., Maples, M.R., Bromley, J.L., & Alcorn, J. (2000). Suicide: An overview. The
Counseling Psychologist, 28, 445–510.Wichstrom, L. (2000). Predictors of adolescent suicide attempts: A nationally representative longitudinal study of Norwe-
gian adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 603– 608.Zenere, F.J., & Lazarus, P.J. (1997). The decline of youth suicidal behavior in an urban, multicultural public school system
following the introduction of a suicide prevention and intervention program. Suicide and Life-Threatening Behavior,27, 387– 403.
Zhang, J., & Jin, S. (1996). Determinants of suicide ideation: A comparison of Chinese and American college students.Cross-Cultural Studies, 31, 451– 467.
Adolescent Suicide 475