Embed Size (px)
Citation preview

Fall 2019 -‐ Spring 2020
1
Disorders of Adrenal Cortex
• Cushing Syndrome
(Adrenocortical Hyperfunction)
• Addison’s Disease (Adrenocortical Insufficiency)
Fall 2019 -‐ Spring 2020
Fluid & Electrolytes
Mobility
Perfusion
Stress & Coping
How will you know if your paBent has an adrenal gland disorder?
What nursing assessments are involved? 1
Changes in CorBsol RegulaBon Altera1on Descrip1on/Defini1on Manifesta1ons Interven1ons and
Therapies
Changes in corBsol regulaBon
Symptoms result from excess or deficient secreBon of corBsol from the adrenal glands. • Cushing Syndrome • Addison’s Disease
Excess corBsol results in Cushing syndrome, which is accompanied by a moon face and central obesity along with other symptoms. CorBsol deficiency results in Addison’s disease, which is accompanied by muscle weakness, faBgue, weight loss, and other symptoms.
Cushing syndrome is treated with either decreasing corBcosteroid dosage or surgery to remove a tumor, depending on the cause. Addison’s disease is treated with oral or injected corBcosteroids.
Fall 2019 -‐ Spring 2020 2
ADRENAL CORTEX
• GLUCOCORTICOIDS: Regulate metabolism, increase bood glucose levels, criBcal in physiological stress response
• MINERALOCORTICOIDS: Regulate sodium & potassium balance (Aldosterone)
• ANDROGENS: Growth & development, sexual development in women
Three classificaBons:
1. GlucocorBcoids 2. MineralocorBcoids 3. Androgens
Fall 2019 -‐ Spring 2020 3

Fall 2019 -‐ Spring 2020
2
GLAND: ADRENAL; HORMONE: CORTISOL
ETIOLOGY & PATHOPHYSIOLOGY: • Common causes: – Iatrogenic administration of exogenous corticosteroids (prednisone)
– ACTH-‐secreting pituitary adenoma
– Adrenal tumors – Ectopic ACTH production by tumors
Cushing Syndrome – Clinical condiBon that results form chronic exposure to excess corBcosteroids, parBcularly glucocorBcoids
Fall 2019 -‐ Spring 2020 4
Cushing Syndrome ñ Glucocorticoids • Excess glucocorticoids
dominate: – Hyperglycemia related to glucose intolerance and ↑ gluconeogenesis
– Muscle wasting → weakness – Loss of bone matrix → osteoporosis and back pain
– Loss of collagen → thin skin, easily bruises
– Delay in wound healing
DIAGNOSTIC STUDIES: • Confirmation of ↑ plasma
cortisol levels: (1) midnight or late night salivary cortisol, (2) low-‐dose dexamethasone suppression test, (3) 24-‐hour urine cortisol (Levels >80-‐120 mcg/24 hours)
• Plasma ACTH levels: • High or normal with
Cushing disease (pituitary etiology)
• Low or undetectable with Cushing syndrome –adrenal/medication etiology
• CT/MRI (brain/abdomen)
Fall 2019 -‐ Spring 2020 5
Cushing Syndrome ñ Glucocorticoids
CLINICAL MANIFESTATIONS: General appearance: truncal obesity, moon face, fat deposits back of neck & shoulders (buffalo hump) Integumentary: thin, fragile skin, purplish/red striae, petechial hemorrhages, bruises, rosey cheeks, acne, poor wound healing Cardiovascular: hypervolemia, HTN, lower extremity edema Gastrointes1nal: épepsin and HCL acid secreBon, PUD, anorexia Renal/urinary: glycosuria, hypercalciuria, renal stones
Fall 2019 -‐ Spring 2020 6
Fall 2019 -‐ Spring 2020
3
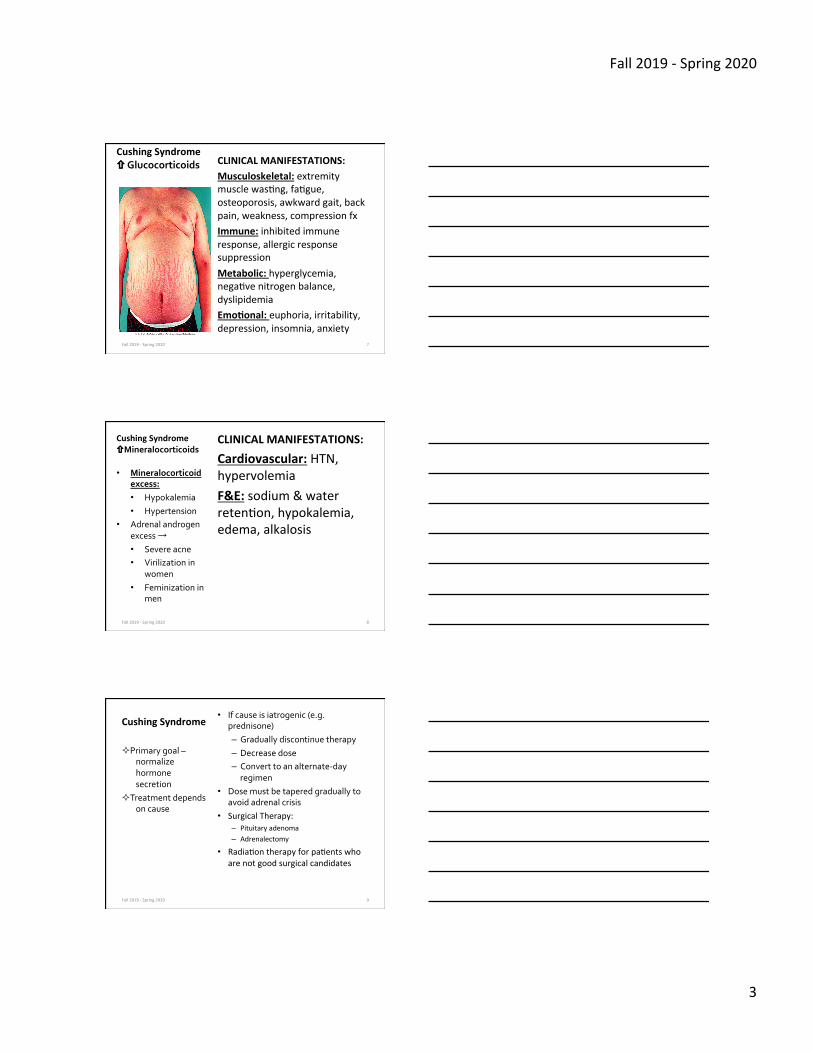
Cushing Syndrome ñ Glucocorticoids CLINICAL MANIFESTATIONS:
Musculoskeletal: extremity muscle wasBng, faBgue, osteoporosis, awkward gait, back pain, weakness, compression fx Immune: inhibited immune response, allergic response suppression Metabolic: hyperglycemia, negaBve nitrogen balance, dyslipidemia Emo1onal: euphoria, irritability, depression, insomnia, anxiety
Fall 2019 -‐ Spring 2020 7
Cushing Syndrome ñMineralocorticoids
CLINICAL MANIFESTATIONS:
Cardiovascular: HTN, hypervolemia F&E: sodium & water retenBon, hypokalemia, edema, alkalosis
• Mineralocorticoid excess: • Hypokalemia • Hypertension
• Adrenal androgen excess → • Severe acne • Virilization in
women • Feminization in
men
Fall 2019 -‐ Spring 2020 8
Cushing Syndrome • If cause is iatrogenic (e.g.
prednisone) – Gradually discontinue therapy – Decrease dose – Convert to an alternate-‐day regimen
• Dose must be tapered gradually to avoid adrenal crisis
• Surgical Therapy: – Pituitary adenoma – Adrenalectomy
• RadiaBon therapy for paBents who are not good surgical candidates
² Primary goal – normalize hormone secretion
² Treatment depends on cause
Fall 2019 -‐ Spring 2020 9

Fall 2019 -‐ Spring 2020
4
Nursing Implementation
ACUTE INTERVENTIONS: • Monitor VS, I&O, F&E, daily
weight, glucose + complicating conditions (e.g. CVD, DM, infection)
• Assess for S&S of inflammation/infection (which may be minimal or absent), pain, loss of function, thromboembolism, pulmonary emboli
• Provide emotional support – Patient may feel unattractive or unwanted
– Remain sensitive to patient’s feelings and be respectful
– Reassure patient that physical changes and emotional lability will resolve when hormone levels return to normal
Fall 2019 -‐ Spring 2020 10
Audience Response QuesBon An IV hydrocortisone infusion is started before a patient is taken to surgery for a bilateral adrenalectomy. Which explanation, if given by the nurse, is most appropriate? a. “The medication prevents sodium and water retention after surgery.” b. “The drug prevent clots from forming in the legs during your recovery from surgery.” c. “This medicine is given to help your body respond to stress after removal of the adrenal glands.” d. “This drug stimulates your immune system and promotes wound healing.”
Fall 2019 -‐ Spring 2020 11
Interprofessional Care –Surgical Therapy Cushing Syndrome
• Surgical removal of pituitary tumor using the transsphenoidal approach (see pg. 1158)
• Adrenalectomy –if caused by adrenal tumors or hyperplasia
INDICATIONS:
• Surgical removal or irradiation of pituitary adenoma
• Adrenalectomy for adrenal tumors or hyperplasia
• Removal of ACTH-‐secreting tumors
Fall 2019 -‐ Spring 2020 12

Fall 2019 -‐ Spring 2020
5
Interprofessional Care Surgical Therapy Cushing Syndrome
• Surgically opBmized – Cardiac clearance – F&E correcBons – Hyperglycemic control – NutriBonally adequate
SURGICAL THERAPY: Preoperative Care Ø Surgical/
Anesthesia consent Ø Pre-‐op labs Ø Medical clearance Ø Pre/Post-‐op
teaching Ø NPO Fall 2019 -‐ Spring 2020 13
SURGICAL THERAPY ADRENALECTOMY: Unilateral/Bilateral
• Laparoscopic • Open ² Compare & contrast
postop complicaBons between surgery of the adrenal vs. thyroid/parathyroid glands
Fall 2019 -‐ Spring 2020
Interprofessional Care Surgical Therapy Cushing Syndrome
14
• Monitor VS, ↑ Risk of hemorrhage • Large release of hormones into
circulation → instabilities in BP, F&E • Monitor for acute adrenal insufficiency:
– Vomiting, increased weakness, dehydration, hypotension, painful joints, pruritus, peeling skin, severe emotional disturbances
• Monitoring for subtle signs of infection
• Meticulous care to prevent infection • Increased risk for:
– Problems with glycemic control – Susceptibility to infection – Delayed wound healing
SURGICAL THERAPY: Postoperative Care Ø Surgical site Ø IVF,I&O,F&E balance Ø NGT, FC, JP drains Ø Diet Ø Activity Ø VTE prophylaxis Ø Pain management Ø High doses of
corticosteroids are given IV during and several days after surgery
Fall 2019 -‐ Spring 2020
Interprofessional Care Surgical Therapy Cushing Syndrome
15

Fall 2019 -‐ Spring 2020
6
Nursing Implementation
TEACHING NEEDS: (lack of endogenous corBcosteroids) • Home health nurse • Wear MedicAlert bracelet at all times • Avoid exposure to extremes of temperature,
infection, and stress • Teach patients about medication use and to monitor
for side effects • Teach how to adjust medication and when to call
health care provider • Lifetime corBcosteroid replacement therapy
Fall 2019 -‐ Spring 2020 16
Interprofessional Care Surgical Therapy Cushing Syndrome
Patient Goals/Outcomes: • Experience relief of
symptoms • Experience no S&S infection • Avoid serious complications • Maintain positive self-‐image • Verbalize acceptance of
appearance and actively participate in therapeutic plan
• Maintain weight appropriate for height
• Heal skin wounds and maintain intact skin
Nursing Diagnoses: • Risk for
infection • Risk for
overweight • Disturbed body
image • Impaired skin
integrity Fall 2019 -‐ Spring 2020 17
GLAND: ADRENAL; HORMONE: CORTISOL
ETIOLOGY & PATHOPHYSIOLOGY: • Primary: caused by lack of
glucocorticoids, mineralocorticoids, and androgens
• Secondary: lack of pituitary ACTH, lack of glucocorticoids and androgens, mineralcorticoids rarely deficient
Addison’s Disease – HypofuncBon of the adrenal cortex from a primary cause. All 3 classes of adrenal corBcosteroids are reduced
Fall 2019 -‐ Spring 2020 18
Fall 2019 -‐ Spring 2020
7
Addison’s Disease êGLUCOCORTICOIDS • Common causes:
– Autoimmune, antibodies destroy adrenal cortex
– Amyloidosis – Fungal infections – AIDS Metastatic cancer
• Iatrogenic Addison’s disease – Adrenal hemorrhage – Chemotherapy – Ketoconazole therapy for AIDS – Bilateral adrenalectomy
DIAGNOSTIC STUDIES: • ACTH SBmulaBon Test
• Baseline levels of cortisol and ACTH, IV injection of synthetic ACTH
• Levels rechecked after 30 and 60 minutes = ↑ Blood cortisol levels is normal
• Little or no ↑ in cortisol levels in Addison’s disease
• CRH SBmulaBon Test • Abnormal ACTH test
response • IV injection of synthetic CRH • Blood drawn after 30 and 60
minutes = High ACTH levels with no cortisol indicates Addison’s disease
• ↑ Potassium, ↑ BUN, ↓ Chloride, sodium, glucose
• Anemia • ECG changes • CT scan, MRI
Fall 2019 -‐ Spring 2020 19
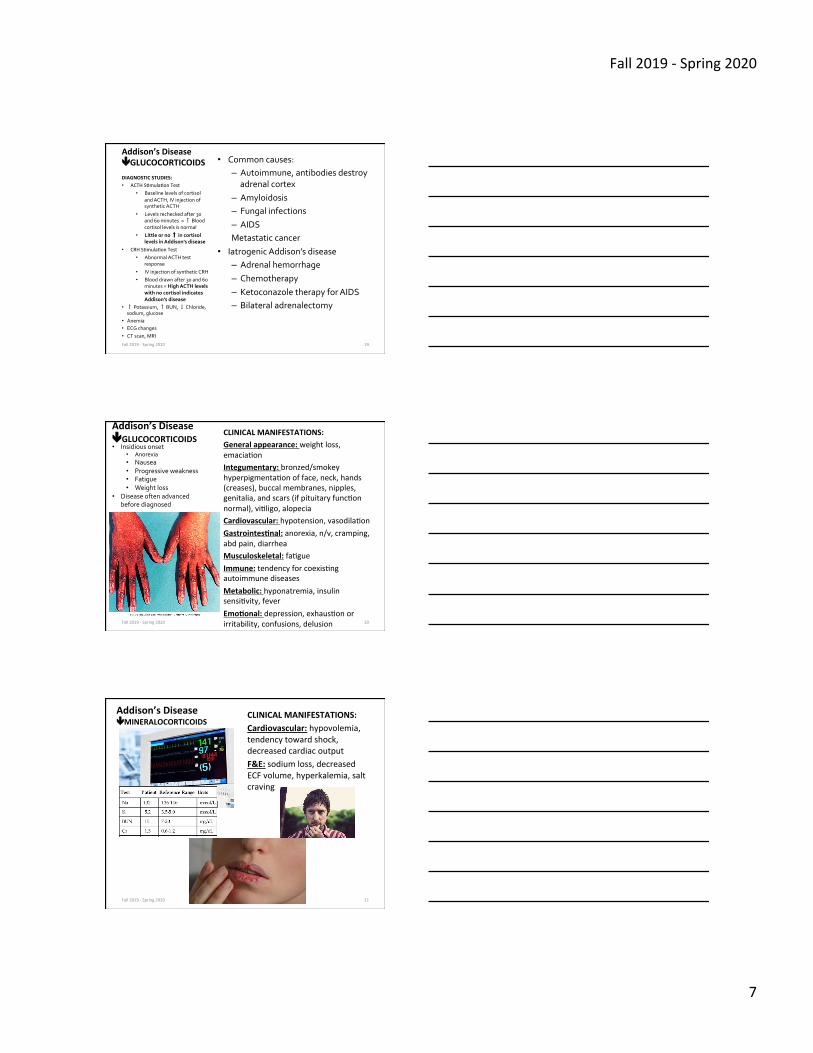
CLINICAL MANIFESTATIONS: General appearance: weight loss, emaciaBon Integumentary: bronzed/smokey hyperpigmentaBon of face, neck, hands (creases), buccal membranes, nipples, genitalia, and scars (if pituitary funcBon normal), viBligo, alopecia Cardiovascular: hypotension, vasodilaBon Gastrointes1nal: anorexia, n/v, cramping, abd pain, diarrhea Musculoskeletal: faBgue Immune: tendency for coexisBng autoimmune diseases Metabolic: hyponatremia, insulin sensiBvity, fever Emo1onal: depression, exhausBon or irritability, confusions, delusion
• Insidious onset • Anorexia • Nausea • Progressive weakness • Fatigue • Weight loss
• Disease often advanced before diagnosed
Fall 2019 -‐ Spring 2020
Addison’s Disease êGLUCOCORTICOIDS
20
Addison’s Disease êMINERALOCORTICOIDS
CLINICAL MANIFESTATIONS: Cardiovascular: hypovolemia, tendency toward shock, decreased cardiac output F&E: sodium loss, decreased ECF volume, hyperkalemia, salt craving
Fall 2019 -‐ Spring 2020 21

Fall 2019 -‐ Spring 2020
8
Addisonian Crisis MANIFESTATIONS OF GLUCOCORTICOID AND MINERALOCORTICOID DEFICIENCIES:
– Hypotension, tachycardia – Dehydration – ↓ Sodium, ↑ potassium, ↓ glucose
– Fever, weakness, confusion – Severe vomiting, diarrhea, pain
– Shock → circulatory collapse
• Acute adrenal insufficiency • Insufficient or
sudden, sharp decrease in hormones
• Various triggers: • stress (infection,
surgery, psychologic)
• Sudden withdrawal corticosteroids
• Adrenal surgery • Sudden pituitary
gland destruction
Fall 2019 -‐ Spring 2020 22
Addisonian Crisis • Shock management • High-‐dose
hydrocortisone replacement
• 0.9% saline solution and 5% dextrose
• Correct fluid and electrolyte imbalance
• Assess vital signs and neurologic status
• Daily weight • Accurate I&O (FC) • Calm environment • Watch for signs of
Cushing syndrome
Fall 2019 -‐ Spring 2020 23
Audience Response QuesBon
The nurse administers corticosteroids to a patient with acute adrenal insufficiency. The nurse determines that treatment is effective if what is observed? a. The patient is alert and oriented b. The patient’s lung sounds are clear c. The patient’s urinary output increases d. The patient’s potassium level is 5.0 mEq/L
Fall 2019 -‐ Spring 2020 24

Fall 2019 -‐ Spring 2020
9
Addison’s Disease Interprofessional Care
Patient teaching of dosing medications: • Glucocorticoids in divided doses • Mineralocorticoids once in the morning
– Reflects normal circadian rhythm – Decreases side effects of
corticosteroids • Need to increase corticosteroids during
times of stress Pa1ent Teaching: • Report signs and symptoms of
corticosteroid deficiency and excess to HCP
• Carry identification and wear medical ID bracelet
• Emergency kit • How to administer IM hydrocortisone • Written instructions
• Manage underlying cause
• Hormone therapy: • Hydrocortisone • Fludrocortisone
(Florinef)
• Increase dietary salt intake
Fall 2019 -‐ Spring 2020 25
Corticosteroid Therapy • Expected effects of
corticosteroid therapy – Antiinflammatory action – Immunosuppression – Maintenance of normal BP
• Effective in treating many diseases and disorders ² What are
examples?
• Complications and side effects with long-‐term use
• Potential benefits must be weighed against risks
Fall 2019 -‐ Spring 2020 26
Corticosteroid Therapy
Pa1ent Teaching: • Dietary needs • Rest and exercise* needs • Sodium restriction if edema
occurs • Need to monitor for
hyperglycemia * • Notify health care provider if
epigastric pain develops * • Need to prevent injury/
infection • Inform all health care providers
Side effects: • ↓ Potassium and calcium • ↑ Glucose and BP • Delayed healing • Susceptibility to infection • Suppressed immune
response • Peptic ulcer disease • Muscle atrophy/weakness • Mood and behavior
changes • Moon facies, truncal
obesity • Protein depletion • Risk for acute adrenal
crisis if therapy is stopped abruptly
Fall 2019 -‐ Spring 2020 27