-
8/13/2019 Adrenal Glands and Addison's
1/6
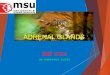
ADRENAL GLANDS Adrenal glands have
a)Cortexcortex has two functional parts:
1)Zona fascicular/reticularissecretes glucocorticoids and
androgens
2)Zona Glomerulosasecretes mineralocorticoidsb) Medullasecrets
adrenaline and noradrenalin
Control of the adrenal glands is gien the !ox"
S#nthesis of adrenal hormones
-
8/13/2019 Adrenal Glands and Addison's
2/6
Glucocorticoids$
Cortisol is the major glucocorticoids in the humans.
Cortisol levels are highest in the morning and lowest in the
night.
Glucocorticoids increase or stimulate follo%ing
luconeogenesis
l!cogen deposition
"rotein catabolism
#at deposition
-
8/13/2019 Adrenal Glands and Addison's
3/6
Mineralocorticoids$
Aldosterone is the predominant mineralocorticoid.
Aldosterone increases the $a%reabsorbtion and increases
&%and ' %excretion.
Aldosterone is important is blood pressure regulation( and is
controlled b! the AA*
s!stem
Androgens$ Androgens are important for pubert!.
Androgens are regulated b! the same '"A axis.
Catecholamines$
+nl! small portions of catecholamines are secreted b! the
adrenal medulla( the! are
mainl! secreted b! the nerve endings.
ADD&S'N(S D&SEASE
Etiolog#
Clinical features$
Asthenia is the cardinal s!mptom. wea,ness( anorexia ma! be
other features.
-nexplained weight losss
$ausea( vomiting( chronic diarrhea
'!perpigmentation .
/t commonl! appears as a diffuse brown( tan( or bron0e dar,ening
of parts such as
the elbows or creases of the hand and of areas that normall! are
pigmented suchas the areola about the nipples.
luishblac, patches ma! appear on the mucous membranes.
'!per pigmentation is due to AC' excess( so h!per pigmentation
is not feature
of secondar! adrenal in sufficienc!
3itiligo ma! paradoxicall! be present in patient with autoimmune
Addison4s disease
)rimar# *+AC,-.
Autoimmune *poradic(
"ol!glandular s!ndromes
uberculosis
'/35A/6*
7etastatic carcinoma
ilateral adrenalectom!
Rare causes 8!mphoma
/ntraadrenal haemorrhage
Corticosteroid !ios#nthetic en#me defects
Congenital adrenal h!perplasias
6rugs met!rapone( ,etocona0ole (etc
Secondar# *0AC,-.
ithdrawal of suppressive glucocorticoids
therap!
'!pothalamic or pituitar! disease
-
8/13/2019 Adrenal Glands and Addison's
4/6
Arterial h!potension with postural accentuation is fre;uent .
"ostural h!potension is
usuall! ver! earl! sign
Axillar! and pubic hair ma! be decreased esp. in women.
Clinical features of acute Addison(s disease are:
1. unconsciousness2. Circulator! shoc, with h!potension.
3. 3omiting and diarrhoea.
&nestigations$
1. AC,- stimulation test:
his test is done to confirmadrenal insufficienc!
2
-
8/13/2019 Adrenal Glands and Addison's
5/6
'/3 I8/*A.
/maging of the adrenals b! C or 7/ to identif! metastatic
malignanc!
Management$
reatment of adiisons disesease is life long replacement of
glucocorticoids.
eplacement doses and advice to patient of Addison4s disease
are
"rednisolone B.< mg dail! 9< mg on wa,ing( 2.
-
8/13/2019 Adrenal Glands and Addison's
6/6
+ral replacement medication is then started( unless unable to
ta,e oral medication(
initiall! h!drocortisone 2= mg( Fhourl!( reducing to 2=>= mg
in divided doses
over a few da!s.
C'NGEN&,AL ADRENAL ->)ER)LAS&A*CA-. +ne of the
important cause of h!poadrenalism.
CA' is autosomal recessive disorder( deficienc! of en0!mes of
cortisol s!nthesis.
Commonest deficienc! is 21h!drox!lase resulting in reduced
levels of cortisol and
increased of AC'.
Clinical features
1. ;emales: ambiguous genitalia( clitoromegal! and
h!poadrenalism.
2. Males$ enlarged penis and increased pubic hair and
h!poadrenalism.
3. 6eficiencies of 11 h!drox!lase and 1B h!drox!lase present
with h!pertension.
&nestigations$ educed levels cortisol and increased levels
of 1B h!drox!progesterone and AC'.
+ther investigations are same as Addison4s disease.
Management$
eplacement of glucocorticoids is the main sta! therap!. aim is
to suppress the
AC'.
6oses of steroids are same as addisons but higher dose is
re;uired in the night and
lower in the morning