Embed Size (px)
Citation preview

Adult Congenital Hydrocephalus
RamanaRamana YedavalliYedavalli, , University of Illinois College of Medicine, Year IVUniversity of Illinois College of Medicine, Year IV
Gillian Lieberman, MDGillian Lieberman, MD
September 12, 2002September 12, 2002

Ramana Yedavalli
Gillian Lieberman, MD
2
ObjectivesObjectives
Discuss normal CSF flow mechanicsDiscuss normal CSF flow mechanics
Discuss normal radiographic findingsDiscuss normal radiographic findings
Discuss epidemiology of hydrocephalusDiscuss epidemiology of hydrocephalus
Discuss briefly the etiologies of hydrocephalusDiscuss briefly the etiologies of hydrocephalus
Discuss pathology and pathophysiology associated with Discuss pathology and pathophysiology associated with hydrocephalus with emphasis on adult clinical hydrocephalus with emphasis on adult clinical presentationpresentation
Discuss clinical case and radiographic findingsDiscuss clinical case and radiographic findings

Ramana Yedavalli
Gillian Lieberman, MD
3
Introduction
““Water on the BrainWater on the Brain””
Abnormal accumulation of CSF in the cranial Abnormal accumulation of CSF in the cranial vaultvault
CSF generally produced at an average rate of CSF generally produced at an average rate of ~0.3mL/min. To maintain steady state, rate of ~0.3mL/min. To maintain steady state, rate of CSF production must necessarily equal rate of CSF production must necessarily equal rate of CSF outflowCSF outflow

Ramana Yedavalli
Gillian Lieberman, MD
4
Two general causes:Two general causes:
Obstruction of outflow of CSF (common)Obstruction of outflow of CSF (common)
Overproduction of CSF (usually due to choroid Overproduction of CSF (usually due to choroid plexus plexus papillomapapilloma –– rare rare -- less than 0.5% of cases)less than 0.5% of cases)
Two categories of obstructive hydrocephalusTwo categories of obstructive hydrocephalus
CommunicatingCommunicating
NoncommunicatingNoncommunicating
Etiologies can be congenital or acquiredEtiologies can be congenital or acquired
Introduction

Ramana Yedavalli
Gillian Lieberman, MD
5
Communicating hydrocephalus Communicating hydrocephalus –– results when the results when the obstruction to outflow is distal to the foramina of obstruction to outflow is distal to the foramina of MagendieMagendie and and LuschkaLuschka
All ventricles are enlargedAll ventricles are enlarged
Obstruction is usually at the level of the Obstruction is usually at the level of the arachnoidarachnoid granulationsgranulations
Causes can include Causes can include intraventricularintraventricular hemorrhage, hemorrhage, meningealmeningeal scarring, among others.scarring, among others.
NoncommunicatingNoncommunicating hydrocephalus hydrocephalus –– results when the results when the obstruction to outflow is proximal to the fourth ventricle obstruction to outflow is proximal to the fourth ventricle foraminaforamina
Ventricle(sVentricle(s) proximal to the obstruction are enlarged) proximal to the obstruction are enlarged
Ventricle(sVentricle(s) distal to the obstruction are generally normal in ) distal to the obstruction are generally normal in sizesize
Obstruction can be congenital or acquiredObstruction can be congenital or acquired
Introduction

Ramana Yedavalli
Gillian Lieberman, MD
6
Ventricular System
Adapted from: Netter, F.H.: Netter, F.H.: Atlas of Human Anatomy, 2Atlas of Human Anatomy, 2ndnd ed.ed. East Hanover, New Jersey: East Hanover, New Jersey: Novartis, 1997Novartis, 1997

Ramana Yedavalli
Gillian Lieberman, MD
7
CSF Circulation Pathways
Adapted from: Netter, F.H.: Netter, F.H.: Atlas of Human Anatomy, 2Atlas of Human Anatomy, 2ndnd ed.ed. East Hanover, New Jersey: East Hanover, New Jersey: Novartis, 1997Novartis, 1997

Ramana Yedavalli
Gillian Lieberman, MD
8
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
Source: http://www.cid.ch/
Saggital T1-weighted image

Ramana Yedavalli
Gillian Lieberman, MD
9
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
Saggital T1-weighted image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
10
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
Saggital T1-weighted image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
11
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted axial image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
12
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted axial image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
13
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted axial image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
14
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted axial image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
15
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted axial image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
16
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted axial image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
17
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted coronal image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
18
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted coronal image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
19
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted coronal image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
20
Normal MRI Findings in the BrainNormal MRI Findings in the Brain
T2-weighted coronal image
Source: http://www.cid.ch/

Ramana Yedavalli
Gillian Lieberman, MD
21
Hydrocephalus Epidemiology
Cannot be accurately calculatedCannot be accurately calculated
In US there are >125,000 patients with CSF shunts and In US there are >125,000 patients with CSF shunts and 50,000 shunt operations performed annually50,000 shunt operations performed annually
The accepted rate of incidence of hydrocephalus is 3 to 4 The accepted rate of incidence of hydrocephalus is 3 to 4 per 1,000 births; however, even this is considered to be per 1,000 births; however, even this is considered to be underreporting the actual rate.underreporting the actual rate.
Adult hydrocephalus accounts for greater than 50% of the Adult hydrocephalus accounts for greater than 50% of the total diagnoses of hydrocephalus.total diagnoses of hydrocephalus.
Actual numbers of adults who suffer from congenital Actual numbers of adults who suffer from congenital hydrocephalus is unknown.hydrocephalus is unknown.

Ramana Yedavalli
Gillian Lieberman, MD
22
Hydrocephalus Etiology
Maternal malnutrition (e.g.Maternal malnutrition (e.g.-- folic acid deficiency leading to neural tube folic acid deficiency leading to neural tube defects).defects).
Infectious causes:Infectious causes:
Bacterial Bacterial –– in rare cases can lead to in rare cases can lead to leptomeningealleptomeningeal scarring scarring and permanent fibrosis of CSF absorptive surfaces:and permanent fibrosis of CSF absorptive surfaces:
–– E. coliE. coli–– H. H. influenzaeinfluenzae–– S. S. pneumoniaepneumoniae–– S. S. agalactiaeagalactiae

Ramana Yedavalli
Gillian Lieberman, MD
23
ViralViral –– can lead to can lead to aqueductalaqueductal atresiaatresia or or
stenosisstenosis
CMVCMV
MumpsMumps
VaricellaVaricella
RubellaRubella
Hydrocephalus Etiology

Ramana Yedavalli
Gillian Lieberman, MD
24
TraumaTrauma
NeoplasmsNeoplasms or cystsor cysts
IntraventricularIntraventricular hemorrhagehemorrhage
Subarachnoid hemorrhageSubarachnoid hemorrhage
CongenitalCongenital
ArnoldArnold--ChiariChiari malformationsmalformations
DandyDandy--Walker malformationsWalker malformations
SpinaSpina bifida (bifida (myelocelesmyeloceles and and meningomyelocelesmeningomyeloceles))
Hydrocephalus Etiology

Ramana Yedavalli
Gillian Lieberman, MD
25
Congenital Congenital aqueductalaqueductal stenosisstenosis
IdiopathicIdiopathic
Congenital malformationCongenital malformation•• ArnoldArnold--ChiariChiari I & III & II•• DandyDandy--Walker Walker •• KlippelKlippel--FeilFeil syndromesyndrome•• Agenesis of foramen of Agenesis of foramen of MonroMonro
XX--linked recessive or neurofibromatosis linked recessive or neurofibromatosis mutationmutation
PeriaqueductalPeriaqueductal tumortumor
AbnormalAbnormal bloodblood vesselvessel
ArachnoidArachnoid cystcyst
SecondarySecondary membranousmembranous occlusionocclusion
Hydrocephalus Etiology

Ramana Yedavalli
Gillian Lieberman, MD
26
Pathophysiologic Findings
Dilated ventriclesDilated ventricles
PeriventricularPeriventricular gliosisgliosis
Thinning of corpus Thinning of corpus callosumcallosum and atrophy of the and atrophy of the periventricularperiventricular white matter white matter –– hemispheric disconnection hemispheric disconnection can resultcan result
Severe hydrocephalus can cause gross thinning of the Severe hydrocephalus can cause gross thinning of the cortexcortex
Basal ganglia atrophy has also been reported in several Basal ganglia atrophy has also been reported in several cases with associated resultant motor pathologycases with associated resultant motor pathology

Ramana Yedavalli
Gillian Lieberman, MD
27
Mechanisms of Injury
Physical/mechanical distortion and Physical/mechanical distortion and parenchymalparenchymal injury injury –– compressioncompression
Altered extracellular environment Altered extracellular environment –– which can which can lead to altered neuronal functionlead to altered neuronal function
Impaired diffusionImpaired diffusion
Areas of stagnationAreas of stagnation
Improper accumulation and clearance of potentially Improper accumulation and clearance of potentially toxic metabolites, neurotransmitters, and other toxic metabolites, neurotransmitters, and other substances.substances.
Blood brain barrier is mildly altered Blood brain barrier is mildly altered

Ramana Yedavalli
Gillian Lieberman, MD
28
Mechanisms of Injury
Vascular Vascular –– postulated mechanismspostulated mechanisms
Doppler blood flow studies, SPECT, MRI and CT have all been Doppler blood flow studies, SPECT, MRI and CT have all been used to show decrements in blood flow in white matter used to show decrements in blood flow in white matter –– ischemic ischemic changes (various animal models have also shown this)changes (various animal models have also shown this)
Changes in cerebral blood flow and oxidative metabolismChanges in cerebral blood flow and oxidative metabolism
Consequence of diminished blood flow is injury to Consequence of diminished blood flow is injury to oligodendrocytesoligodendrocytes and axons in the white matterand axons in the white matter
Mechanisms and morphological characteristics of axonal damage Mechanisms and morphological characteristics of axonal damage in rats have similarities to those detected after ischemic insulin rats have similarities to those detected after ischemic insultt
HTN and atherosclerosis may aggravate situation in adult humansHTN and atherosclerosis may aggravate situation in adult humans

Ramana Yedavalli
Gillian Lieberman, MD
29
Adult Onset Hydrocephalus
Includes hydrocephalus caused by Includes hydrocephalus caused by
Tumor, hemorrhage, trauma, infection, or other Tumor, hemorrhage, trauma, infection, or other brain pathologybrain pathology
Congenital hydrocephalusCongenital hydrocephalus
Primary hydrocephalus occurring in older Primary hydrocephalus occurring in older adults such as that seen with idiopathic normal adults such as that seen with idiopathic normal pressure hydrocephalus (NPH)pressure hydrocephalus (NPH)

Ramana Yedavalli
Gillian Lieberman, MD
30
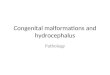
Adult-onset Hydrocephalus
Almost always caused by a CSF outflow tract obstructionAlmost always caused by a CSF outflow tract obstruction
Etiology of adult onset hydrocephalus. Shown here are percent diEtiology of adult onset hydrocephalus. Shown here are percent distribution of stribution of 468 cases tried at the Cleveland Clinic between 1994 and 2000. 468 cases tried at the Cleveland Clinic between 1994 and 2000. SxSx = surgery; = surgery; ICH = intracranial hemorrhage; NPH = normal pressure hydrocephalICH = intracranial hemorrhage; NPH = normal pressure hydrocephalus; SAH us; SAH = subarachnoid hemorrhage.= subarachnoid hemorrhage.
Taken from: Taken from: ChahlaviChahlavi, A., El, A., El--BabaaBabaa, S.K., , S.K., LucianoLuciano, M.G.: , M.G.: ““AdultAdult--Onset Hydrocephalus.Onset Hydrocephalus.”” Neurosurgery Neurosurgery Clinics of North Clinics of North AmericaAmerica 36(4):75336(4):753--760, 2001760, 2001

Ramana Yedavalli
Gillian Lieberman, MD
31
Adult-onset Hydrocephalus
Little understanding of the adaptive brain response to hydrocephLittle understanding of the adaptive brain response to hydrocephalus. alus. It may be that this adaptive response is what makes the brain toIt may be that this adaptive response is what makes the brain tolerant lerant of a slowly evolving of a slowly evolving ventriculomegalyventriculomegaly when similar when similar ventriculomegalyventriculomegaly is devastating, and often fatal, when it is more acute.is devastating, and often fatal, when it is more acute.
Adaptive responses may includeAdaptive responses may include
Hydrodynamic responsesHydrodynamic responses
Brain compliance changesBrain compliance changes
Vascular adaptationsVascular adaptations
Etc?Etc?
While the exact process is unknown, the above might explain why While the exact process is unknown, the above might explain why patients with severe patients with severe ventriculomegalyventriculomegaly (congenital or otherwise) may (congenital or otherwise) may do well for decades and then present in adulthood with symptoms do well for decades and then present in adulthood with symptoms of of hydrocephaly.hydrocephaly.

Ramana Yedavalli
Gillian Lieberman, MD
32
Clinical Presentation – Adult Onset
May be acute, May be acute, subacutesubacute, or chronic and insidious, or chronic and insidious
Acute and Acute and subacutesubacute forms present with symptoms of forms present with symptoms of increased ICP:increased ICP:
Acute Acute –– stupor and coma stupor and coma –– most often seen with SAH, most often seen with SAH, exudativeexudative meningitis, meningitis, meningealmeningeal neoplasticneoplastic infiltration and fourth ventricle infiltration and fourth ventricle tumors.tumors.
SubacuteSubacute –– develops over a few days or weeks and causes develops over a few days or weeks and causes progressive drowsiness or progressive drowsiness or abuliaabulia with incontinencewith incontinence
Symptoms of a more gradually evolving case include Symptoms of a more gradually evolving case include (patient needn(patient needn’’t have all symptoms)t have all symptoms)
HeadacheHeadache
Nausea (position independent)Nausea (position independent)
VomitingVomiting
AtaxiaAtaxia
Visual disturbancesVisual disturbances

Ramana Yedavalli
Gillian Lieberman, MD
33
Clinical Presentation cont.
Symptoms often evolve over years in a patient with Symptoms often evolve over years in a patient with aqueductalaqueductal stenosisstenosis. Symptoms include. Symptoms include
Ataxia (generally Ataxia (generally truncaltruncal))
Slowed Slowed mentationmentation
SeizuresSeizures
Urinary incontinenceUrinary incontinence
Symptoms resulting from Symptoms resulting from aqueductalaqueductal stenosisstenosis in adults are somewhat in adults are somewhat dependent on age and the degree of dependent on age and the degree of ventriculomegalyventriculomegaly. . FukuharaFukuhara et al. et al. reviewed features of late onset idiopathic reviewed features of late onset idiopathic stenosisstenosis and concludedand concluded
Younger adults present with symptoms of increased ICP such Younger adults present with symptoms of increased ICP such as headaches and nauseaas headaches and nausea
Older adults with larger ventricles present with symptoms Older adults with larger ventricles present with symptoms similar to NPHsimilar to NPH

Ramana Yedavalli
Gillian Lieberman, MD
34
Clinical Presentation cont.
Hydrocephalus evolves after SAH, meningitis, and severe Hydrocephalus evolves after SAH, meningitis, and severe trauma frequently enough that it should be suspected with trauma frequently enough that it should be suspected with any delayed deterioration over weeks or months after the any delayed deterioration over weeks or months after the original insult. Symptoms of congenital hydrocephalous original insult. Symptoms of congenital hydrocephalous can evolve insidiously over years (as in the case of this can evolve insidiously over years (as in the case of this patient)patient)
MR is the diagnostic tool of choice as it is better able to MR is the diagnostic tool of choice as it is better able to identify areas of obstruction than CT, ultrasound, or plain identify areas of obstruction than CT, ultrasound, or plain films. MR can also allows direct measurement of CSF films. MR can also allows direct measurement of CSF flow.flow.

Ramana Yedavalli
Gillian Lieberman, MD
35
Clinical Case
69 year old Caucasian man69 year old Caucasian man
PMHxPMHx::(1) Complex partial seizures(1) Complex partial seizures(2) Chronic (2) Chronic atrialatrial fibrillationfibrillation(3) S/P surgery for melanoma on scalp(3) S/P surgery for melanoma on scalp(4) HTN(4) HTN(5) CHF(5) CHF(7) Obesity(7) Obesity(8) S/P bilateral total knee (8) S/P bilateral total knee arthroplastiesarthroplasties(9) Benign prostatic hyperplasia(9) Benign prostatic hyperplasia(10) Urinary incontinence(10) Urinary incontinence(11) Questionable dementia(11) Questionable dementia(12) Congenital hydrocephalus(12) Congenital hydrocephalus

Ramana Yedavalli
Gillian Lieberman, MD
36
Medication listMedication list
LanoxinLanoxin
AtenololAtenolol
ParoxetineParoxetine
ASAASA
PhenytoinPhenytoin
DitropanDitropan
PlendilPlendil
Clinical Case cont.

Ramana Yedavalli
Gillian Lieberman, MD
37
Physical exam is remarkable for no neurologic Physical exam is remarkable for no neurologic abnormalities except for slightly ataxic gait, abnormalities except for slightly ataxic gait, inability to perform fingerinability to perform finger--nosenose--finger test finger test satisfactorily, and inability to touch heel to shin.satisfactorily, and inability to touch heel to shin.
Patient is slightly Patient is slightly macrocephalicmacrocephalic
Patient has never had a craniotomy (i.e. Patient has never had a craniotomy (i.e. –– ventriculoperitonealventriculoperitoneal or or ventriculoatrialventriculoatrial shunt never shunt never placed)placed)
Clinical Case

Ramana Yedavalli
Gillian Lieberman, MD
38
Clinical Case cont.
No complaints of No complaints of diplopiadiplopia, blurred vision, or tinnitus, blurred vision, or tinnitus
Serial MRISerial MRI’’s of brain were done between 1998 and 2002 s of brain were done between 1998 and 2002 show marked, but stable, enlargement of lateral and third show marked, but stable, enlargement of lateral and third ventricles with a normal fourth ventricle, likely due to ventricles with a normal fourth ventricle, likely due to chronic congenital chronic congenital aqueductalaqueductal stenosisstenosis, however, the , however, the aqueduct of aqueduct of SylviusSylvius appears patent on imaging studies. appears patent on imaging studies. There is compression of the cortices along the occipital, There is compression of the cortices along the occipital, temporal, and parietal regions. There is a small amount of temporal, and parietal regions. There is a small amount of preserved cortex within bilateral frontal lobes.preserved cortex within bilateral frontal lobes.

Ramana Yedavalli
Gillian Lieberman, MD
39
Clinical Case MRIClinical Case MRI
T1T1--weighted weighted saggitalsaggital imageimageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
40
Clinical Case MRIClinical Case MRI
T1T1--weighted weighted saggitalsaggital imageimageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
41
Clinical Case MRIClinical Case MRI
T1T1--weighted weighted saggitalsaggital imageimageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
42
Clinical Case MRIClinical Case MRI
T1T1--weighted weighted saggitalsaggital imageimageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
43
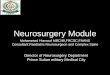
Clinical Case MRIClinical Case MRI
T1T1--weighted weighted saggitalsaggital imageimage
Cerebral aqueduct of Cerebral aqueduct of SylviusSylvius
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
44
Clinical Case MRIClinical Case MRI
T2T2--weighted axial imageweighted axial imageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
45
Clinical Case MRIClinical Case MRI
T2T2--weighted axial imageweighted axial imageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
46
Clinical Case MRIClinical Case MRI
T2T2--weighted axial imageweighted axial image
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
47
Clinical Case MRIClinical Case MRI
T2T2--weighted axial imageweighted axial image
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
48
Clinical Case MRIClinical Case MRI
T2T2--weighted axial imageweighted axial image
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
49
Clinical Case MRIClinical Case MRI
T2T2--weighted axial imageweighted axial imageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
50
Clinical Case MRIClinical Case MRI
T2T2--weighted axial imagesweighted axial imagesSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
51
Clinical Case MRIClinical Case MRI
T1T1--weighted coronal imageweighted coronal imageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
52
Clinical Case MRIClinical Case MRI
T1T1--weighted coronal imageweighted coronal imageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
53
Clinical Case MRIClinical Case MRI
T1T1--weighted coronal imageweighted coronal imageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
54T1T1--weighted coronal imageweighted coronal image
Clinical Case MRIClinical Case MRI
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
55
Clinical Case MRIClinical Case MRI
T1T1--weighted coronal imageweighted coronal imageSource: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
56T1T1--weighted coronal imagesweighted coronal images
Clinical Case MRIClinical Case MRI
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
57T1T1--weighted coronal imagesweighted coronal images
Clinical Case MRIClinical Case MRI
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
58
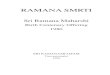
Clinical Case MRI Clinical Case MRI -- 20002000
T1 T1 sagittalsagittal, T2 axial, and T1 coronal images respectively from , T2 axial, and T1 coronal images respectively from 5/2000 demonstrating stability of patient5/2000 demonstrating stability of patient’’s hydrocephaluss hydrocephalus
Source: University of Illinois Hospital PACS

Ramana Yedavalli
Gillian Lieberman, MD
59
Unique features of this case includeUnique features of this case include
Patient has never had a shunting procedure done to remove the Patient has never had a shunting procedure done to remove the excess CSFexcess CSF
Patient has apparently been relatively stable for many years Patient has apparently been relatively stable for many years with little or no neurological degradationwith little or no neurological degradation
Some of patientSome of patient’’s symptoms fit the s symptoms fit the symptomatologysymptomatology associated with associated with Normal Pressure Hydrocephalus (NPH)Normal Pressure Hydrocephalus (NPH)
Urinary incontinence (wet)Urinary incontinence (wet)
Ataxia (wobbly)Ataxia (wobbly)
Decreased Decreased mentationmentation (weird)(weird)
Clinical Case Clinical Case -- DiscussionDiscussion

Ramana Yedavalli
Gillian Lieberman, MD
60
Reasons NPH is not a likely diagnosisReasons NPH is not a likely diagnosis
ChronicityChronicity of hydrocephalus (patient has studies dating back of hydrocephalus (patient has studies dating back to 1998 but apparently had been followed at an outside hospital to 1998 but apparently had been followed at an outside hospital for many years). Is much more likely that patient has for many years). Is much more likely that patient has hydrocephalus associated with increased intracranial pressure.hydrocephalus associated with increased intracranial pressure.
Decreased Decreased mentationmentation of NPH is qualitatively different from the of NPH is qualitatively different from the dementia this patient suffers from.dementia this patient suffers from.
Please see handout for a more complete discussion of NPHPlease see handout for a more complete discussion of NPH
Further imaging studies might involve performing MR Further imaging studies might involve performing MR quantification of CSF flow through the aqueduct of quantification of CSF flow through the aqueduct of SylviusSylvius..
Clinical Case Clinical Case -- DiscussionDiscussion

Ramana Yedavalli
Gillian Lieberman, MD
61
Treatment
Generally involves diversionary shunting procedure to Generally involves diversionary shunting procedure to relieve the pressure caused by the excess CSF in the relieve the pressure caused by the excess CSF in the calvariumcalvarium..
It is not a perfect solutionIt is not a perfect solution
EpendymalEpendymal lining is generally not restoredlining is generally not restored
Large blood vessels can resume their normal configuration Large blood vessels can resume their normal configuration but capillaries do not , or at least not quickly.but capillaries do not , or at least not quickly.
Once axons have been destroyed it is unlikely that they can Once axons have been destroyed it is unlikely that they can be restored be restored
Early shunting is better than late shunting.Early shunting is better than late shunting.
In this patient since he has been hydrocephalic for many In this patient since he has been hydrocephalic for many years (perhaps his whole life) it is unlikely shunting will years (perhaps his whole life) it is unlikely shunting will prove efficacious. Observation is probably best.prove efficacious. Observation is probably best.

ReferencesOiOi, S., , S., ShimodaShimoda, M., Shibata, M., Honda, Y., Togo, K., , M., Shibata, M., Honda, Y., Togo, K., ShinodaShinoda, M., , M., TsuganeTsugane, R., Sato, O.: , R., Sato, O.: ““Pathophysiology of LongPathophysiology of Long--Standing Overt Standing Overt VentriculomegalyVentriculomegaly in Adults.in Adults.”” J. J. NeurosurgNeurosurg.. 92:93392:933--940, 2000940, 2000
PattisapuPattisapu, J.V.: , J.V.: ““Etiology and Clinical Course of Hydrocephalus.Etiology and Clinical Course of Hydrocephalus.”” Neurosurgery Clinics of Neurosurgery Clinics of North AmericaNorth America 36(4):65136(4):651--659, 2001659, 2001
Del Del BigioBigio, M.R.: , M.R.: ““PathophysiologicPathophysiologic Consequences of Hydrocephalus.Consequences of Hydrocephalus.”” Neurosurgery Neurosurgery Clinics of North AmericaClinics of North America 36(4):63936(4):639--649, 2001649, 2001
PartingtonPartington, M.D.: , M.D.: ““Congenital Hydrocephalus.Congenital Hydrocephalus.”” Neurosurgery Clinics of North AmericaNeurosurgery Clinics of North America36(4):73736(4):737--742, 2001742, 2001
ChahlaviChahlavi, A., El, A., El--BabaaBabaa, S.K., , S.K., LucianoLuciano, M.G.: , M.G.: ““AdultAdult--Onset Hydrocephalus.Onset Hydrocephalus.”” Neurosurgery Neurosurgery Clinics of North AmericaClinics of North America 36(4):75336(4):753--760, 2001760, 2001
Bradley, W.G.: Bradley, W.G.: ““Diagnostic Tools in Hydrocephalus.Diagnostic Tools in Hydrocephalus.”” Neurosurgery Clinics of North Neurosurgery Clinics of North AmericaAmerica 36(4):66136(4):661--684, 2001684, 2001
Hakim, C.A., Hakim, R., Hakim, S.: Hakim, C.A., Hakim, R., Hakim, S.: ““NormalNormal--Pressure Hydrocephalus.Pressure Hydrocephalus.”” Neurosurgery Neurosurgery Clinics of North AmericaClinics of North America 36(4):76136(4):761--773, 2001773, 2001
Netter, F.H.: Netter, F.H.: Atlas of Human Anatomy, 2Atlas of Human Anatomy, 2ndnd ed.ed. East Hanover, New Jersey: Novartis, 1997East Hanover, New Jersey: Novartis, 1997
http://http://www.cid.chwww.cid.ch
Ramana Yedavalli
Gillian Lieberman, MD

Ramana Yedavalli
Gillian Lieberman, MD
63
Glen Glen DobbenDobben, , MDMD(Department(Department of Radiology, University of Illinois Hospital)of Radiology, University of Illinois Hospital)
Gillian Lieberman, MDGillian Lieberman, MD
Ms. Pamela Ms. Pamela LepkowskiLepkowski
BIDMC Department of RadiologyBIDMC Department of Radiology
Acknowledgements

Thank You Very MuchThank You Very Much
Ramana Yedavalli
Gillian Lieberman, MD