Embed Size (px)
Citation preview
4/13/17
1
Advancements in Therapeutic Surgical
Options for the CorneaMitch Ibach, OD
Vance Thompson Vision
no relevant financial disclosures
The cornea is assisted by a tear film and is composed of five layers.
Corneal conditions commonly corrected by surgery
Corneal Surgery Anatomical Timeline
• Penetrating Keratoplasty (PKP) • Deep
Anterior Lamellar Keratoplasty
• Descemet’s Stripping Endothelial Keratoplasty
• Descemet’s Membrane Endotheial Keratoplasty
Corneal Grafts are increasing in number
• Registry study of total # corneal grafts per year from 2000-2012
Coster, D. J., Lowe, M. T., Keane, M. C., & Williams, K. A. (2015, May). A Comparison of Lamellar and Penetrating Keratoplasty Outcomes. American Academy of Ophthalmology, 121(5), 979-987.
0
200
400
600
800
1000
1200
1400
1600
2000 2008 2012
Num
ber
of g
raft
s
Year
Anterior Lamellar grafts
Endothelial grafts
Penetrating grafts
Lambert, L. (Artist). Clienteles Cartoons 5 of 16. [Painting]. Cartoon Stock.

4/13/17
2
Here’s a patient who…
• Immigrated to the US, and today is his first eye exam
• Is best corrected to 20/80-1 OD and 20/125 OS
• On exam has advanced corneal scarring with corneal opacities and stromal haze
• Pentacam Tomography's look like this
• Pachymetry
• He wants new glasses.
Penetrating Keratoplasty (PK)/(PKP)
• Procedure
• A circular button-shaped full-thickness section of cornea is removed using a trephine or a laser.
• A matching button is removed from the donor cornea.
• The new donor cornea is sewn to the host cornea with sutures.
Post-Operative Course • Often high amount of irregular astigmatism post-operatively
• Incremental suture removal starting at 3-6 months post-op
• Vision and astigmatism fluctuations on every suture removal
• New glasses at 12-18 months post-op. Likely BCVA with specialty contact lenses
• Steroid Medication
Astigmatism becoming more regular.
Drawbacks of PK grafts-graft failure
• 10 years post-op 20 years Post-op 23 years post-op
11 % 51% 83%
Kelly, T., Williams, K., & Coster, D. (2011, June). Corneal Transplantation for Keratoconus. Archives of Ophthalmology, 129(6), 691-697.
Comparison of PK vs. DSEK
0.740.29
4
0.89
0.360.11
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Acuity >20/40 Endothelial Cell loss 1 year Astigmatism
PK
DSEK
Visual Acuity, ECD loss, and Astigmatism
Lee, B., Jacobs, D., Musch, D., Kaufman, S., Reinhart, W., & Shtein, R. (2009, September). Descemet's Stripping Endothelial Keratoplasty: Safety
and Outcomes. American Academy of Ophthalmology, 116(9).
Further Drawbacks of PK grafts-Post-Op visual acuity
• Australian registry study• most recent follow-up
Snellen acuity 20/40 or better in 74%
• AAO registry studyàAchieving 20/40 or better
• PK’s 39% vs. DALK’s 44%
Coster, D. J., Lowe, M. T., Keane, M. C., & Williams, K. A. (2015, May). A Comparison of Lamellar and Penetrating Keratoplasty Outcomes. American Academy of Ophthalmology, 121(5), 979-987.
Kelly, T., Williams, K., & Coster, D. (2011, June). Corneal Transplantation for Keratoconus. Archives of Ophthalmology, 129(6), 691-697.

4/13/17
3
Deep Anterior Lamellar Keratoplasty- DALK
• Here’s a patient who presents to your office..
1. He can’t see
2. His glasses prescription keeps changing
3. Doctors tell him “His eye is bulging forward.”
Deep Anterior Lamellar Keratoplasty-DALK
• Procedure
• Donor graft- Epithelium, Bowman’s, Stroma are dissected out.
• Host- Epithelium, Bowman’s, Stroma are cut out.
• Sutures bring the host and graft together.
VanDijk, K., Baydoun, L., Konder, R., & Melles, G. (2014, August 1). Contact Lenses After Keratoplasty. Contact Lens Spectrum.
DALK vs. PK
• Advantages of DALK1) No open globe
2) Unlikely immune rejection of endothelium
3) Minor loss of endo cells
4) Sutures can be removed earlier
5) Steroids can be stopped earlier
• Major review by AAO for BCVA and preservation of ECD for graft survival• 11 large comparative studies
• 6/11 = BCVA
• other non-determinant
• Graft survivalat 20 years
51% ?PK DALKReinhart, W. J., Musch, D. C., Jacobs, D. S., Lee, B., Kaufman, S. C., &
Shtein, R. M. (2011, January). Deep Anterior Lamellar Keratoplasty as an Alternative to Penetrating Keratoplasty. American Academy of Ophthalmology, 118(1), 209-218.
Amniotic Membrane Grafts
1. Anti-inflammatory
2. Anti-scarring
3. Anti-angiogenesis (new blood vessel growth)
4. Re-epithelialization
http://www.nature.com/eye/journal/v23/n10/fig_tab/eye2008410f2.html
What is amniotic membrane• Inner layer of the placenta
• Avascular connective tissue
• Epithelial cells on a basement membrane which resides over a stromal matrix
• Made of collagen, fibronectin, laminin
• Growth factors
• Anti-inflammatory components
Kenyon, K. R., & Lam, H. (2013, June 1). Amniotic Membrane: Themes and Variations. Ophthalmology Management, 1-6.
Amniotic Membrane Grafts (AMG)
Biotissue- Prokera, Amniograft, & Amnioguard
IOP Ophthalmics-Ambiodisk
http://www.iopinc.com/store/ambiodisk/http://www.biotissue.com/products/prokera.aspx

4/13/17
4
Clinical Usage1. Insertion Prokera vs. AmbioDisk
2. Time-frame to reabsorption = 10-21 days.Resorption will be faster in neovascularized or very inflammed eyes. More inflammatory cytokines will dissolve the graft faster.
3. Prokeraà remove ring in clinic. Ambiodiskà remove BCL
Kenyon, K. R., & Lam, H. (2013, June 1). Amniotic Membrane: Themes and Variations. Ophthalmology Management, 1-6.
AMG Actions
1. Reduces inflammation
2. Inhibits scarring
3. Inhibits angiogenesis
4. Promotes epithelialization
5. Possesses anti-microbial properties
6. Restoration of lost corneal thickness*
Indications/Conditions for use
• Acute corneal trauma
• Chemical or thermal burn
• Non-healing epithelial defects (herpes, diabetes)
• Neurotrophic corneal ulcers
• Filamentary Keratitis
• Severe Dry Eye Syndrome
• Recurring epithelial defects
• High risk keratoplastys
• Superficial keratectomy
• Tube shunt/bleb exposure
• Pterygium removal
Kenyon, K. R., & Lam, H. (2013, June 1). Amniotic Membrane: Themes and Variations. Ophthalmology Management, 1-6.
Here’s a patient who…
• Comes into your office because she can’t see
• 57 y/o female
• Complains of blurry vision worse in the morning.. Gets better
• Vision “Like looking through water”
• Do I have a cataract?
Kaiser, P., Friedman, N., & Pineda II, R. (n.d.). The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology: 2nd Edition (Vol. 2). N.p.: Elsevier Health Sciences.
Konan Endothelial Cell Count (ECC) (ECD-Density)
Cornea Fundamentals (2005). In Konan Medical . Retrieved May 23, 2015.Bonnell, A., & Cymbor, M. (2012, August 15). Under the specular microscope. Review of Optometry
Unfortunately- This patient’s ECC

4/13/17
5
Enter DSEK
• Descemet’s Stripping Endothelial Keratoplasty (DSEK/DSAEK)
Removes a. Descemet’sb. Endothelium
Inserta. Posterior Stromab. Descemet’sc. Endothelium
VanDijk, K., Baydoun, L., Konder, R., & Melles, G. (2014, August 1). Contact Lenses After Keratoplasty. Contact Lens Spectrum.
Gas/Air bubble tamponades the graft into place
Post-Operative Course
• Post-Op 1 Day à Patient positioning 1st 24-48 hrs• Vision 20/200-HM, air/gas bubble covering pupil, IOP normal
(ALERT), edematous graft, suture
• Post Op 1 week• Vision 20/30-20/100, air/gas bubble gone or nearly, IOP normal, able
to visualize graft, mild to no edema, suture
• Post-Op 1 month• Vision 20/25-20/50, no bubble, IOP stable, +/--- suture, clear graft
• Post-Op 3 months• Vision stable =1 month, ready for new glasses, IOP stable, clear graft.
ALERT
• If bubble is blocking the PI, the PI is non-patent, or bubble behind Irisè patient will be in pupillary block with elevated IOP• IOP ranges 30-75
• Nausea, headache, vomiting.
• Burping the paracentesis or wound will help.
• If these patients call youàAsk them to sit UP.
A Patient with Fuch’s Dystrophy
• Number 1 concern= Glare
• Vision 20/25 è 20/400
• “I can’t do the things I need to”
• “Scared and nervous”
• Pseudophakic
• His description
The Decision
A. Monitor
B. Muro 128 ointment BID
C. Refer:Endothelial Keratoplasty
D. Look harder for PCO

4/13/17
6
Introducing DMEK
• Descemet’s Membrane Endothelial Keratoplasty
Removes a. Descemet’sb. EndotheliumInserta. Descemet’sb. Endothelium
Gas/Air bubble tamponades the graft into place
Post-Operative Course: Similar to DSEK
• Post-Op 1 Day à Patient positioning 1st 24-48 hrs• 20/200-HM, air/gas bubble covering
pupil, IOP normal (ALERT), edematous graft, suture
• Post Op 1 week• 20/20-20/100, bubble gone or nearly, IOP
normal, able to visualize graft, mild to no edema, suture
• Post-Op 1 month• 20/20-20/50, IOP stable, +/- suture
• Post-Op 3 months• VA stable, ready 4 new glasses, IOP stable
DMEK +/- Cataract Surgery (Triple Procedure)
3.1%
26%30%
0.1
3.5%
26%29%
00.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
early graft failure
median ECD @ 6 months
Air re-injection rate
logMAR bcva
DMEK alone
DMEK+CEX
Chaurasia, S., Price, Jr., F., Gunderson, L., & Price, M. (2014, February). Descemet's Membrane Endothelial Keratoplasty-Clinical Results
of Single Versus Triple Procedures. American Academy of Ophthalmology, 121(2), 454-458.
DMEK vs. DSEK
DMEK vs. DSEK-Acuity
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
pre-op bcva 3-month bcva 6-month bcva
logM
AR
DMEK
DSEK
logMAR 0.6=20/80
logMAR 0.3=20/40
logMAR 0=20/20
Tourtas, T., Laaser, K., Bachmann, B., Cursiefen, C., & Kruse, F. (2012, June). Descemet Membrane Endothelial Keratoplasty Versus Descemet Stripping Automated Endothelial Keratoplasty. American Journal of Ophthalmology, 153(6), 1082-1089.
20/100
20/32
20/60
20/25-
20/40-
DMEK vs. DSEK- Pachymetry
0
100
200
300
400
500
600
700
pre-op pach 3-month pach
6-month pach
652
552517
698638 618
DMEK
DSEK
Tourtas, T., Laaser, K., Bachmann, B., Cursiefen, C., & Kruse, F. (2012, June). Descemet Membrane Endothelial Keratoplasty Versus DescemetStripping Automated Endothelial Keratoplasty. American Journal of Ophthalmology, 153(6), 1082-1089.
4/13/17
7
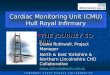
DMEK vs. DSEK- ECD
0
500
1000
1500
2000
2500
3000
ECD pre-op ECD 3 months PO
ECD 6 months PO
2575
1498 1520
2502
17781532
DMEK
DSEK
Tourtas, T., Laaser, K., Bachmann, B., Cursiefen, C., & Kruse, F. (2012, June). Descemet Membrane Endothelial Keratoplasty Versus Descemet Stripping Automated Endothelial Keratoplasty. American Journal of Ophthalmology, 153(6), 1082-1089.
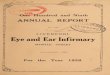
0.7% 1%
9%
12%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
13 month F-U Probability at 2 years
Risk of Transplant Rejection at 1 Year and Probability at 2 Years
DMEK DSEK
Risk of Transplant Rejection
Anshu, A., Price, M., & Price, F. (2012, March). Risk of Corneal Transplant Rejection Significantly Reduced with Descemet's Membrane Endothelial Keratoplasty. Ophthalmology, 119(3), 536-539.
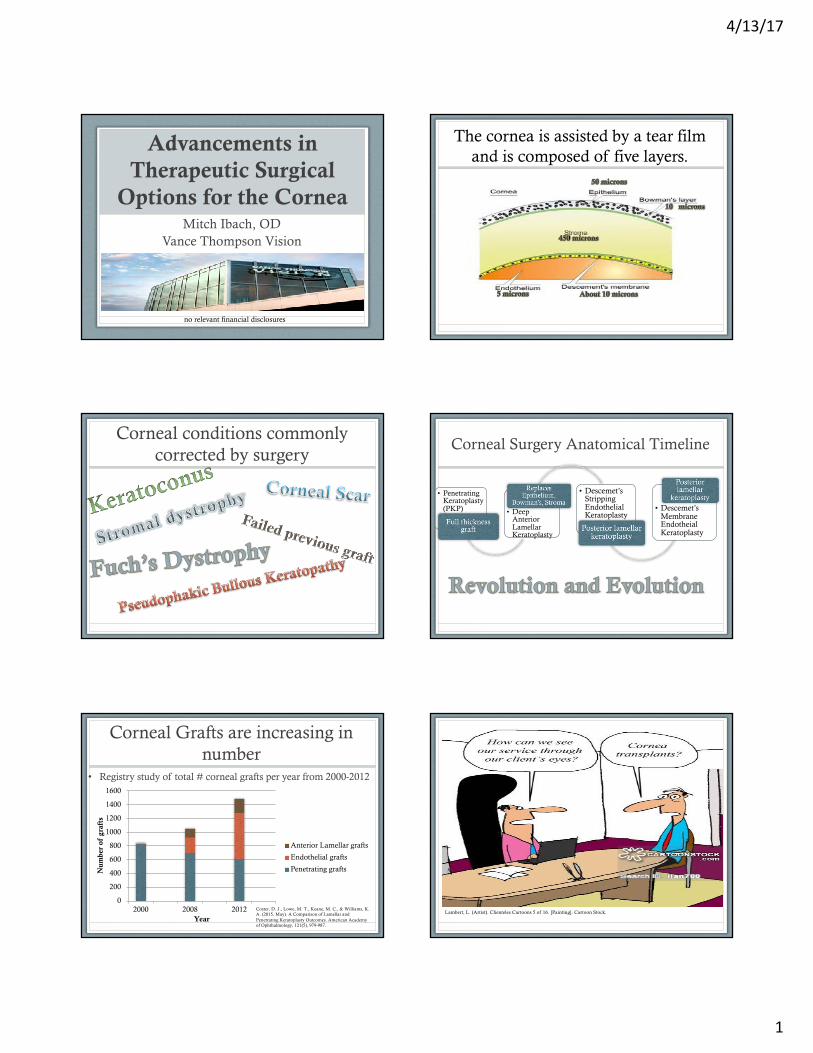
DMEK vs. DSEK- re-bubbling rate
0
5
10
15
20
25
30
35
re-bubbled grafts
DMEK
DSEK
Discussion: “Although a higher re-bubbling rate for DMEK– no effect on visual outcome or endothelial cell survival rate, but was associated with increased post-operative effort”
Tourtas, T., Laaser, K., Bachmann, B., Cursiefen, C., & Kruse, F. (2012, June). Descemet Membrane Endothelial Keratoplasty Versus DescemetStripping Automated Endothelial Keratoplasty. American Journal of Ophthalmology, 153(6), 1082-1089.
27%
44%
0%
39%
0%5%10%15%20%25%30%35%40%45%50%
Re-bubbles needed
Percent decrease in
ECD
Graft Adhesion > Sulfur Hexafluoride (SF6) Gas bubbles for
lower re-bubble rates
Purple = AIRYellow = GAS
Acar, B., Muftuoglu, O., & Acar, S. (2014, March). Comparison of Sulfur Hexafluoride and Air for Donor Attachment in DescemetStripping Endothelial Keratoplasty in Patients with Pseudophakic Bullous Keratopathy. Cornea, 33(3).
Patients Care About Vision.

4/13/17
8
• DMEK
v Maintains corneal anatomy
v Thinner pachymetry
v Equal endothelial cell loss
v With SF6 gas re-bubble rates are lowering, and process is safe for patient
v Less graft rejection
v Better VISION
• DSEK
vAdds thickness to corneal anatomy
vEqual endothelial cell loss
vRe-bubble rates are lowervLess TravelvLess Visits
vWorks well for patients with poor visual potential