Embed Size (px)
Citation preview
ADVANCES IN INTEGRATED
TREATMENT OF CO-OCCURRING
DISORDERS: WHAT DOES RESEARCH
SAY?
Paula Riggs MD
Professor of Psychiatry
Director Division of Substance Dependence
University of Colorado School of Medicine

LEARNING OBJECTIVES
At the conclusion of this presentation, participants
should be able to:
1) Understand developmental risk
factors substance abuse and mental health
problems in young people
2) Have a working knowledge of evidence-
based substance treatment modalities for adolescents and young
adults
3) Understand research–based principles of
integrated treatment for co-occurring mental
health and substance use disorders
4) The impact of health care reform (ACA) on behavioral health and integrated systems of
care

• The BEST TREATMENT for co-occurring
disorders is an integrated approach, where both
the substance abuse problem and the mental
disorder are treated simultaneously.
• RECOVERY depends on treating both disorders.
• COMBINED TREATMENT IS BEST---ideally,
combined mental health and addiction treatment
from the same treatment provider or team.
SAMHSA, NIDA


Age
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
5 10 15 20 25 30 35 40 45 50 55 60
% i
n E
ach
Age G
rou
p t
o D
evelo
p
Fir
st-
tim
e D
ep
en
den
ce
THCALCOHOL
TOBACCO
70
Mental Illness and Addiction are Developmental Disorders
• Childhood onset mental
health problems increase
risk for adolescent-onset
SUD
• Adolescent-onset
substance abuse
exacerbates existing
and/or increase increases
risk for developing
mental health problems
• Comorbidity is the rule,
not the exception
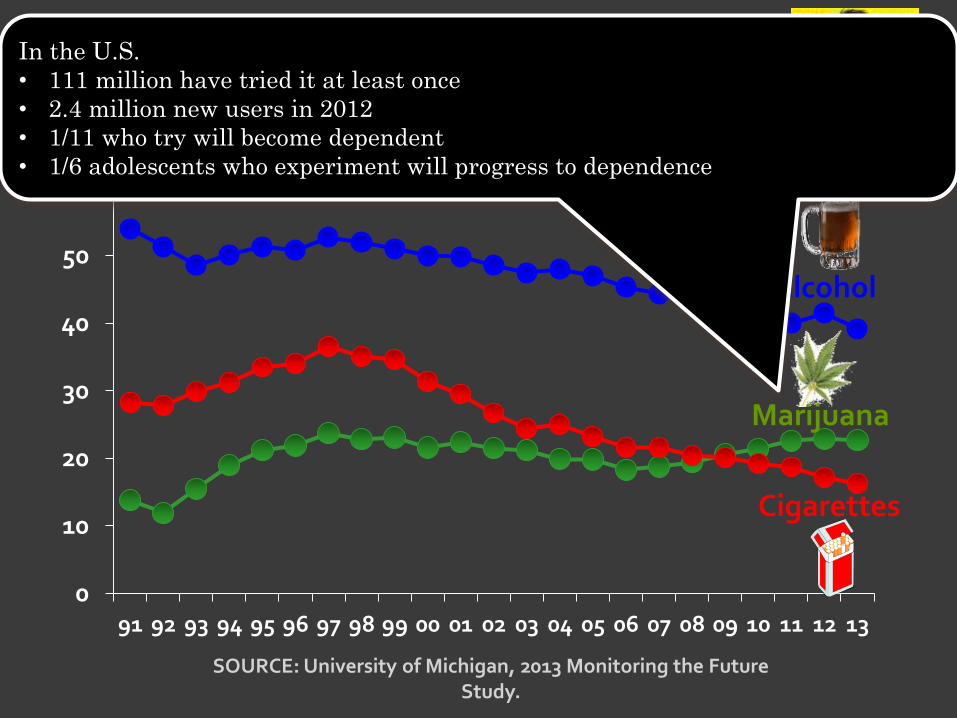
0
10
20
30
40
50
60
91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11 12 13
Percentage of U.S. 12th Grade Students Reporting Past Month Use of Alcohol, Cigarettes, Marijuana
SOURCE: University of Michigan, 2013 Monitoring the Future Study.
Cigarettes
Alcohol
Marijuana
In the U.S.
• 111 million have tried it at least once
• 2.4 million new users in 2012
• 1/11 who try will become dependent
• 1/6 adolescents who experiment will progress to dependence

Pre-natal
MJ
exposure
Birth
poor sleep
continuity
organization
DEFICITS
short
term
memory &
verbal
reasoning
Age 3 Age 6
DEFICITS IN
• impulse control,
reading, visual
analysis,
hypothesis testing
• short-term
memory; attention;
quantitative and
verbal reasoning
Age
14
Age
10
Inattention,
hyperactivity
Depression
onset age
10
DEFICITS IN
• attention, verbal and
abstract reasoning;
INCREASED RISK
• conduct problems and
delinquent behavior
• early–onset cannabis
use prior to age 14
Goldschmidt et al 2012 –Longitudinal Study of pre-natal MJ exposure < 1 joint per day vs > 1 joint per day . Most
findings associated with first trimester MJ use (heavy users smoked 2.4, 2.1,2.4 joints per day 1st, 2nd, 3rd trimesters,
respectively)
Poorer academic achievement
Interferes
with immune
system
development
Pre-natal Cannabis Exposure Increases Risk for Depression, Conduct, SUD, Learning Problems,
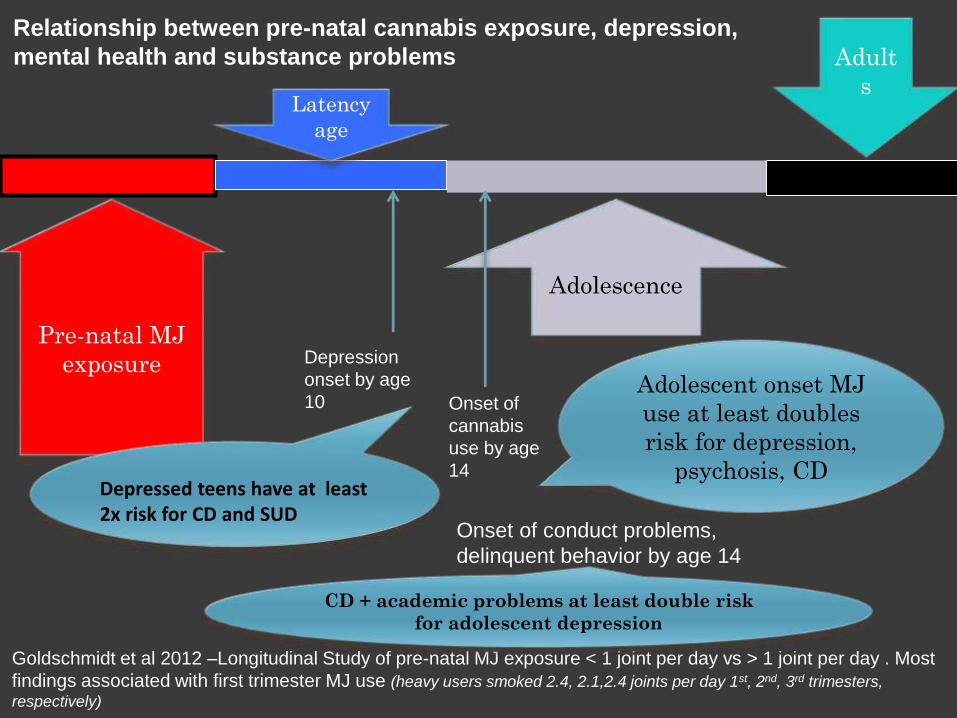
Pre-natal MJ
exposure
Latency
age
Adolescence
Adult
s
Depression
onset by age
10
Goldschmidt et al 2012 –Longitudinal Study of pre-natal MJ exposure < 1 joint per day vs > 1 joint per day . Most
findings associated with first trimester MJ use (heavy users smoked 2.4, 2.1,2.4 joints per day 1st, 2nd, 3rd trimesters,
respectively)
Onset of
cannabis
use by age
14
Onset of conduct problems,
delinquent behavior by age 14
Depressed teens have at least 2x risk for CD and SUD
Adolescent onset MJ
use at least doubles
risk for depression,
psychosis, CD
CD + academic problems at least double risk
for adolescent depression
Relationship between pre-natal cannabis exposure, depression,
mental health and substance problems
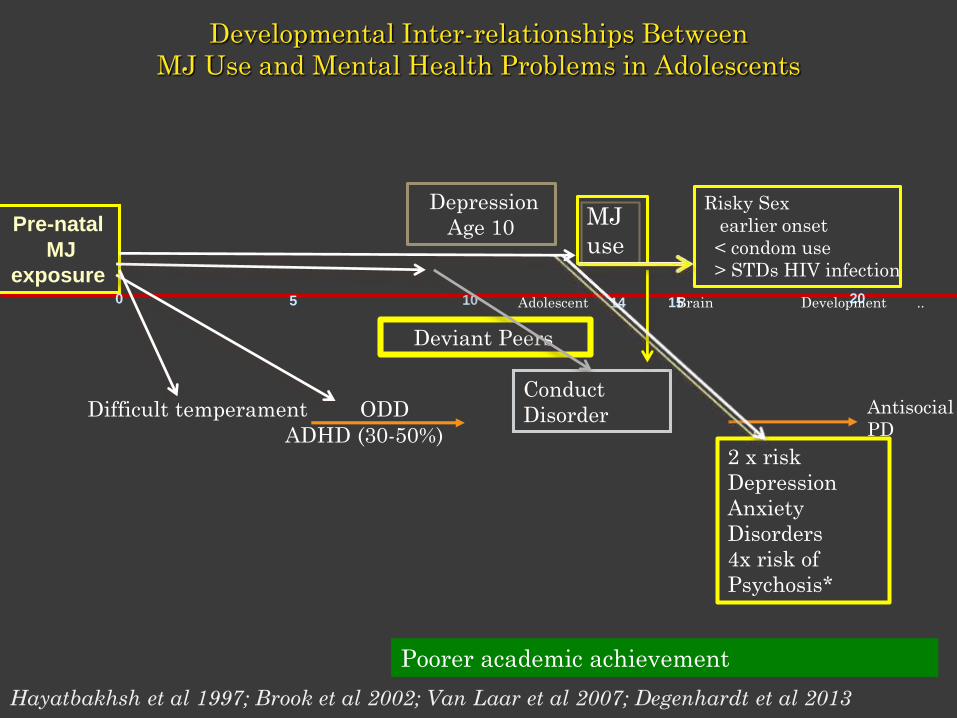
0 10 205 15
Pre-natal
MJ
exposure
Difficult temperament ODD
ADHD (30-50%)
Conduct
Disorder Antisocial
PD
Developmental Inter-relationships Between
MJ Use and Mental Health Problems in Adolescents
Depression
Age 10
Deviant Peers
MJ
use
14
Risky Sex
earlier onset
< condom use
> STDs HIV infection
2 x risk
Depression
Anxiety
Disorders
4x risk of
Psychosis*
Adolescent Brain Development ..
Poorer academic achievement
Hayatbakhsh et al 1997; Brook et al 2002; Van Laar et al 2007; Degenhardt et al 2013

Predominant environment and activities during teenage years
guides selective synapse “pruning” (elimination) during critical
period of adolescent development Giedd et al; Casey et al. 2010

+EVIDENCE-BASED SUBSTANCE AND PSYCHIATRIC TREATMENTS
FOR ADOLESCENTS
Substance Use Disorders
Family-based (MDFT, FFT, MST,
BSFT, ACRA-with MET/CBT)
Behavioral/Contingency
Management (CM) /incentives
Cognitive Behavioral Therapy
(CBT)+ MET
Psychiatric Disorders
Conduct Disorder (60-80%)
Family-Based
CBT
Depression, Anxiety(30-40%)
CBT
Pharmacotherapy
ADHD (30-50%)
CBT
Pharmacotherapy
MET/CBT + CM
(< 20% abstinence)
(30% abstinence)
50% abstinence
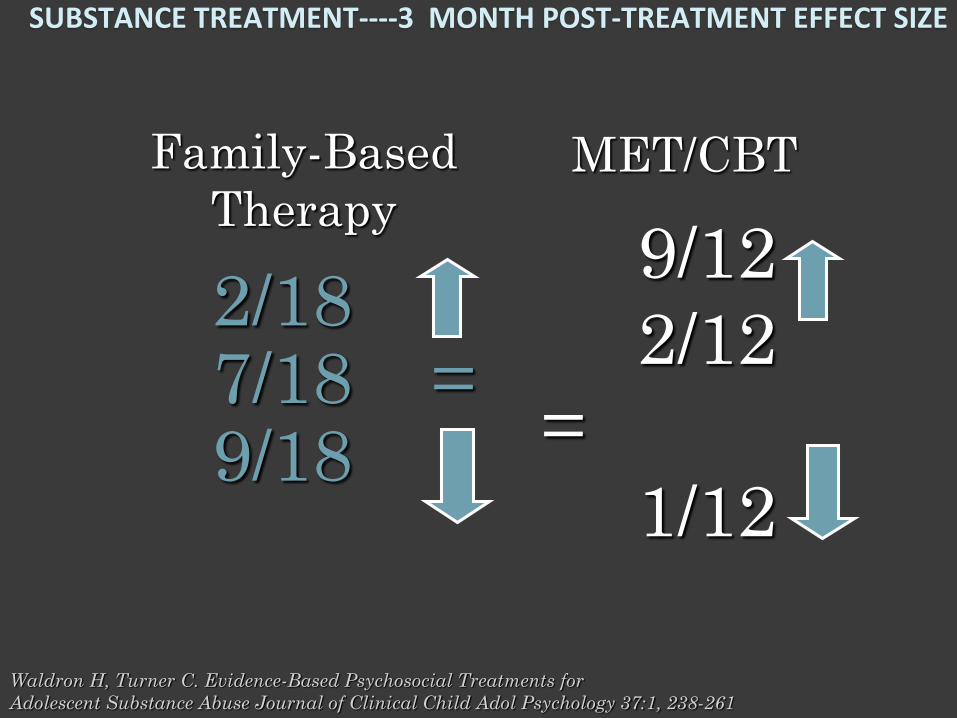
SUBSTANCE TREATMENT----3 MONTH POST-TREATMENT EFFECT SIZE
MET/CBTFamily-Based
Therapy
Waldron H, Turner C. Evidence-Based Psychosocial Treatments for
Adolescent Substance Abuse Journal of Clinical Child Adol Psychology 37:1, 238-261
9/12
2/12
=
1/12
2/187/18 =9/18
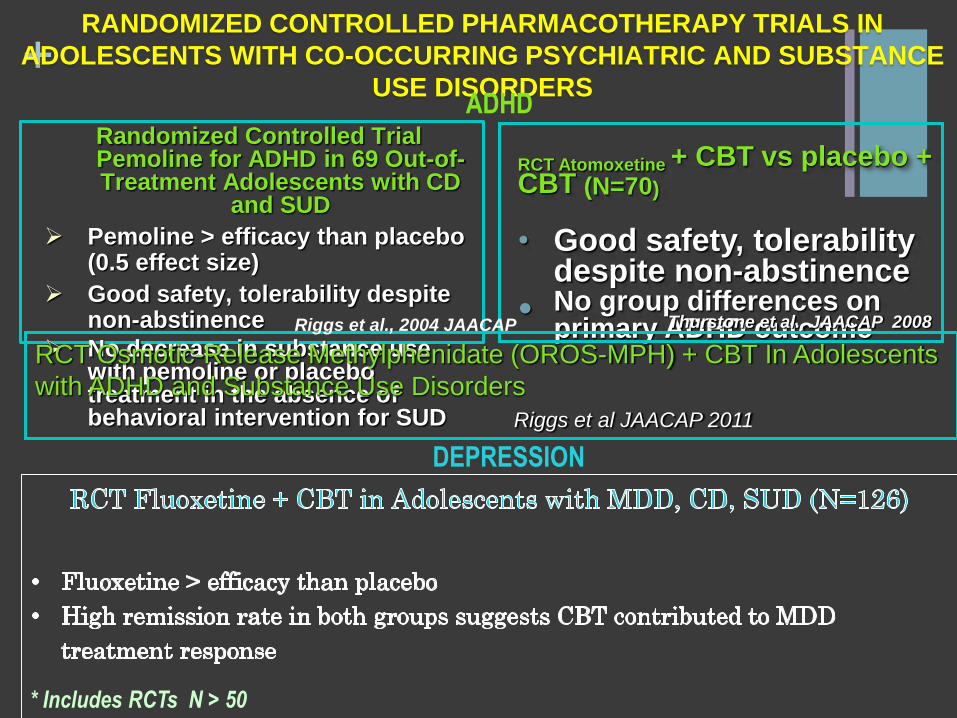
+RANDOMIZED CONTROLLED PHARMACOTHERAPY TRIALS IN
ADOLESCENTS WITH CO-OCCURRING PSYCHIATRIC AND SUBSTANCE
USE DISORDERS
Randomized Controlled Trial Pemoline for ADHD in 69 Out-of-Treatment Adolescents with CD
and SUD
Pemoline > efficacy than placebo (0.5 effect size)
Good safety, tolerability despite non-abstinence
No decrease in substance use with pemoline or placebo treatment in the absence of behavioral intervention for SUD
RCT Atomoxetine + CBT vs placebo + CBT (N=70)
• Good safety, tolerability despite non-abstinence
• No group differences on primary ADHD outcome
RCT Osmotic-Release Methylphenidate (OROS-MPH) + CBT In Adolescents
with ADHD and Substance Use Disorders
Riggs et al JAACAP 2011
Riggs et al., 2004 JAACAP Thurstone et al., JAACAP 2008
DEPRESSION
ADHD
* Includes RCTs N > 50

Placebo N= 63
Withdrawals::
4 Went to Jail/Detention
3 Went to Residential Treatment at a
Facility Unable to Continue Study
3 Lost to Follow-up
+ 1 Moved Out of Area
11 Participants Withdrawn
Withdrawals:
1 Went to Jail/Detention
3 Lost to Follow-up
3 Moved Out of Area
+ 2 Withdrew Consent
9 Participants Withdrawn
13 Not Meeting Inclusion Criteria
+ 4 Admitted to Residential Treatment
17 Excluded
16 week completers N=52 16 week completers N = 54
328 TelephonePre-Screen Calls
126 Randomized
143 Assessed for Eligibility
Fluoxetine N = 63
Randomized Controlled Trial
Fluoxetine vs Placebo + 16 weeks CBT
80% tx completion; medication follow up compliance weekly medication visits;
>80 % compliance with CBT
Cannabis Youth Treatment Study:
Main findings from two randomized trials
“Of the adolescents assigned to one of the four
12- to 14-week treatment interventions,
52% had lengths of stay that reached 90 days”
Dennis et al J Subst Ab Tx 2004
That’s
weird!

Change in Depression (CDRS-R)
Fluoxetine v Placebo
Change in Depression Severity
Depression Remission (CDRS<29)
Fluoxetine v Placebo
70%
52%
P<.05P<.01P<.05
*High remission in both fluoxetine and placebo
groups support antidepressant action of CBT
Manualized behavioral therapies such as CBT have been shown to decrease substance or alcohol use
and/or depressive symptoms (Carroll, 2004; Maude-Griffin et al., 1998; Brown et al., 1997).
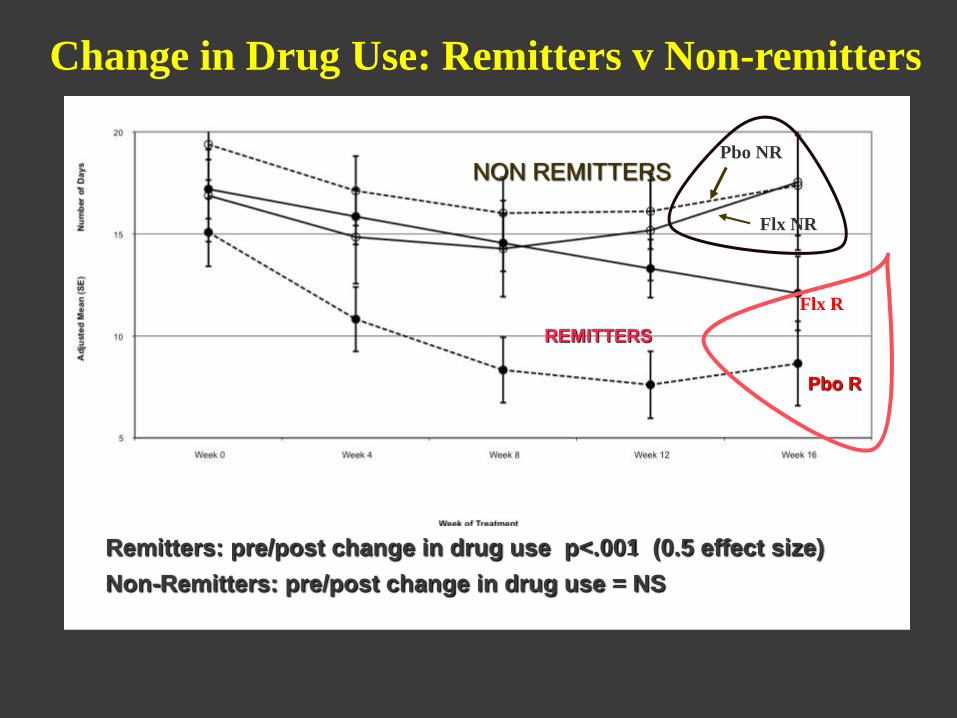
Pbo R
Flx NR
Pbo NR
Flx R
Change in Drug Use: Remitters v Non-remitters
REMITTERS
NON REMITTERS
Remitters: pre/post change in drug use p<.001 (0.5 effect size)
Non-Remitters: pre/post change in drug use = NS

+Depression and Drug Use
Acute Treatment and 1 Year Outcomes
Remitters v Non-remitters
Treatment ends
Depression
Remitters v Non-remitters
Treatment ends
Drug Use

+ CONDUCT DISORDER
ACUTE TREATMENT AND 1 YEAR OUTCOMES
Treatment ends
Treatment endsTreatment ends
Treatment ends
Remitters v Non-remitters

19
Figure 15.2 Study Flow Diagram
Telephone Prescreened N=1334
Informed Consent Baseline Screening
N=446
Non-completes N=43 (28.3%) 11 withdrew consent 1 moved form area 3 practical problems 5 incarceration 1 pressure/advice from outsiders 1 feels treatment not working 17 failed to return to clinic and lost 4 other
Placebo + CBT N=152
143 Excluded (32%) 139 Not eligible (97.2%) 4 Other (2.8%)
Non-completes N=33 (21.9%) 11 withdrew consent 3 moved form area 2 practical problems 4 incarceration 1 pressure/advice from outsiders 9 failed to return to clinic and lost 3 other
16 week completers N=109 (71.7%) 16 week completes N=118 (78.1%)
Completed 1 month follow-up N=105 (69.1%)
Completed 1-month follow-up N=109 (72.2%)
OROS-MPH + CBT N=151
Randomized N=303
OROS/MPH + MET/CBT v Placebo + MET/CBT
72% CBT compliance 69% CBT compliance
Not so weird…..
replication of fluoxetine RCT
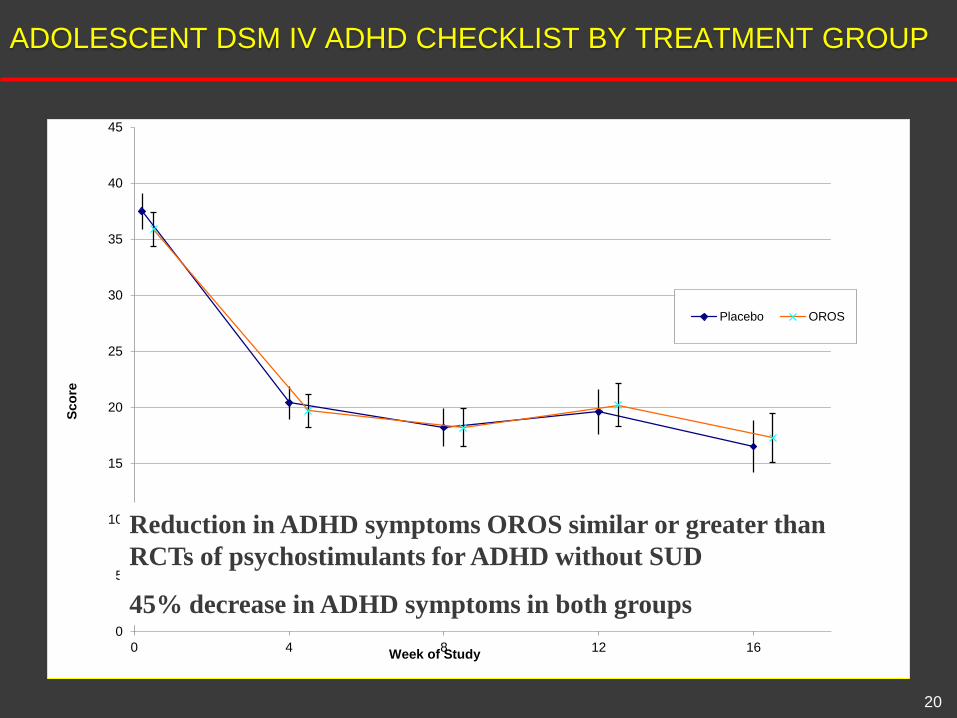
ADOLESCENT DSM IV ADHD CHECKLIST BY TREATMENT GROUP
20
0
5
10
15
20
25
30
35
40
45
0 4 8 12 16
Sco
re
Week of Study
Placebo OROS
Reduction in ADHD symptoms OROS similar or greater than
RCTs of psychostimulants for ADHD without SUD
45% decrease in ADHD symptoms in both groups

+CHANGE IN PAST 28 DAY SUBSTANCE USE
The trajectories of past 28 day drug use based on adolescent self-reports did
not differ between treatment groups (Chi-square = 3.04, 3 df, p = 0.3855 ; Proc
Glimmix).
0
2
4
6
8
10
12
14
16
18
0 4 8 12 16
Days o
f U
se
Week of Study
Placebo
OROS
- 6.1 days 44% OROS-3.8 – UDS
- 4.9 days 33% PBO
2.8 - UDS
3.8 – UDS
P<.05
• More subjects
treated with
OROS-MPH had
> 75% reduction
in drug use
ADHD tx responders regardless of
medication group assignment had:
• 2x neg UDS (6 v 3)
• > days abstinent (median=94, R vs 77 days,
NR)
Clinically and statistically significant decrease in drug use both groups but difference
between groups not statistically significant; > negative UDS OROS > Placebo
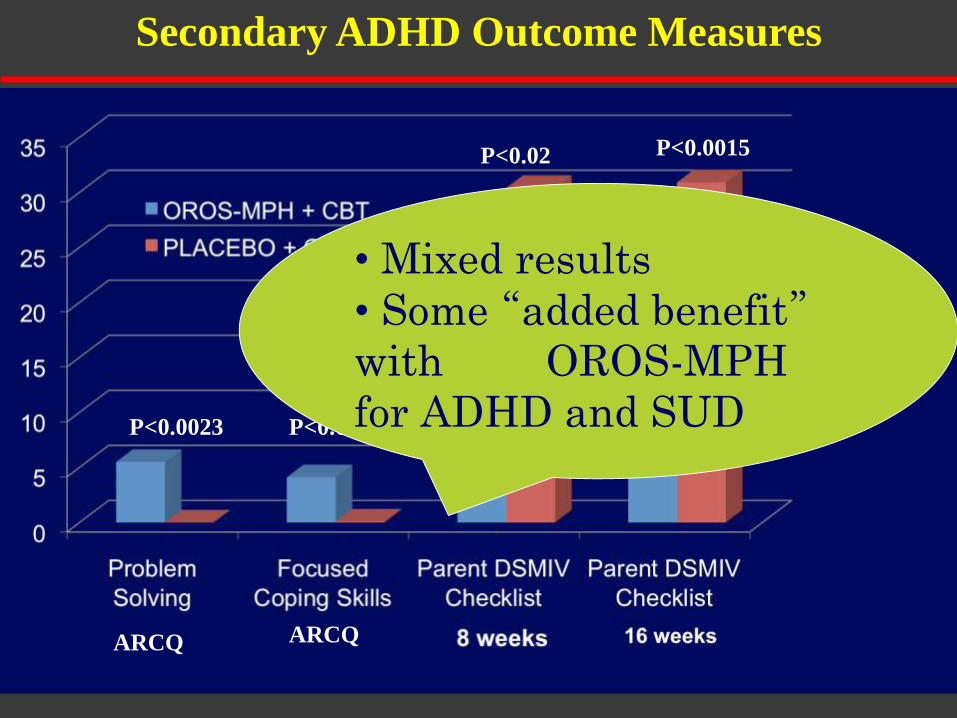
ARCQ
P<0.023P<0.0023
P<0.02 P<0.0015
Secondary ADHD Outcome Measures
ARCQ ARCQ
• Mixed results
• Some “added benefit”with OROS-MPH
for ADHD and SUD

23
1. Comprehensive diagnostic and clinical evaluation
2. Concurrent Treatment for substance and psychiatric
disorders
3. Baseline and repeated measures:
• Psychiatric symptom severity
• ADHD (DSM symptom checklist
• Depression (CDRS-R, PHQ-9 )
• Anxiety Disorders ( MASC, SCARED)
• For substance use
• Urine drug screens (baseline, weekly)
• TLFB (calendar method)—
1. Baseline days/28 days
2. All days during treatment
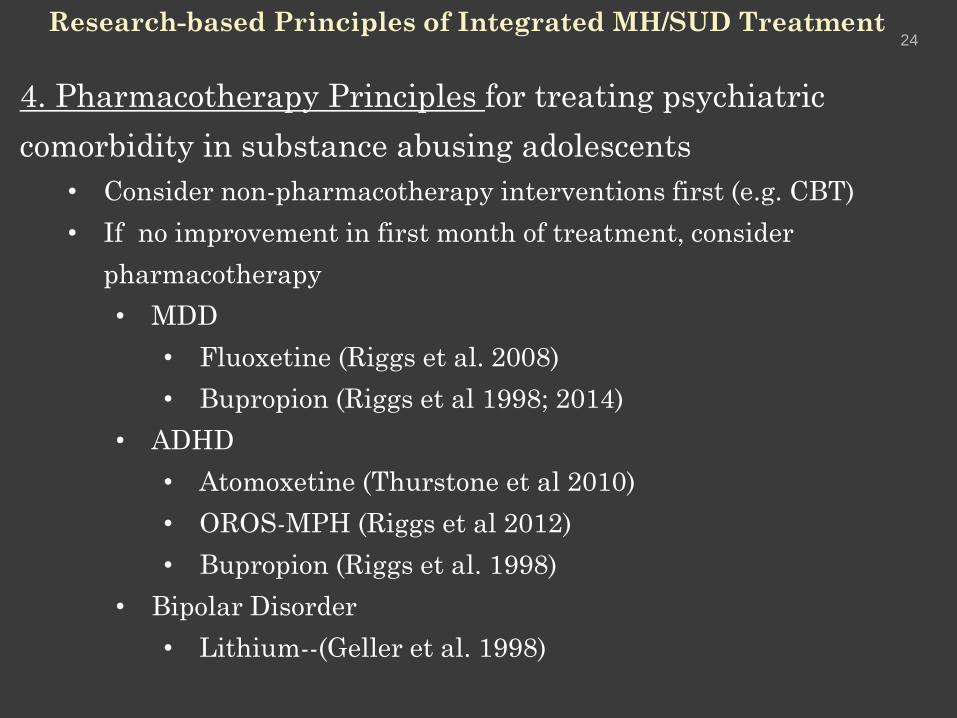
24Research-based Principles of Integrated MH/SUD Treatment
4. Pharmacotherapy Principles for treating psychiatric
comorbidity in substance abusing adolescents
• Consider non-pharmacotherapy interventions first (e.g. CBT)
• If no improvement in first month of treatment, consider
pharmacotherapy
• MDD
• Fluoxetine (Riggs et al. 2008)
• Bupropion (Riggs et al 1998; 2014)
• ADHD
• Atomoxetine (Thurstone et al 2010)
• OROS-MPH (Riggs et al 2012)
• Bupropion (Riggs et al. 1998)
• Bipolar Disorder
• Lithium--(Geller et al. 1998)

25Research-based Principles of Integrated MH/SUD Treatment
3. Continuing Care
• Regular check-ups
• Early intervention for lapses/relapses
• Establish linkage (“warm handoff”) with primary care,
mental health, substance treatment, and recovery
support services as clinically indicated

Evolution of an
Integrated
Treatment
Model
ENCOMPASS
Integrated
Treatment
for
Adolescents
and Young
Adults

Research Practice
Incentives/CM
paid $25 per visit; free tx*
Could not apply additional incentives/contingencies to enhance abstinence rates
Psychiatric treatment
Constrained by single pharmacotherapy/placebo
Could not individually tailor treatment as clinically indicated
Relapse prevention/ continuing care
Constrained by research protocol
16 week CBT + Contingency
Management/ Incentives “fishbowl”
Compliance
Abstinence
Psychiatric treatment
Broader range of options
Psychotherapy
Pharmacotherapy
Relapse prevention
Early involvement in + community-based
activity to build internalized motivation
Augment paucity of continuing care
treatment services

ONLY ABOUT 10% OF ADOLESCENTS WHO COULD
BENEFIT, RECEIVE SUBSTANCE TREATMENT
2002 2003 2004 2005 2006 2007 2008 2009 2010
Recovery Research Institute, SAMHSA 2011
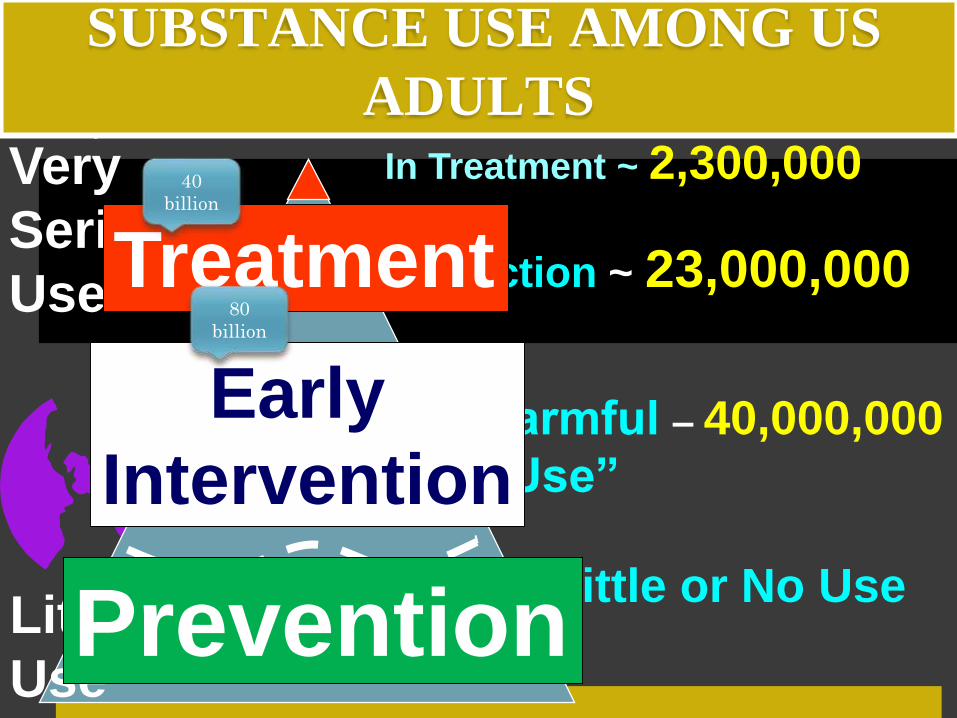
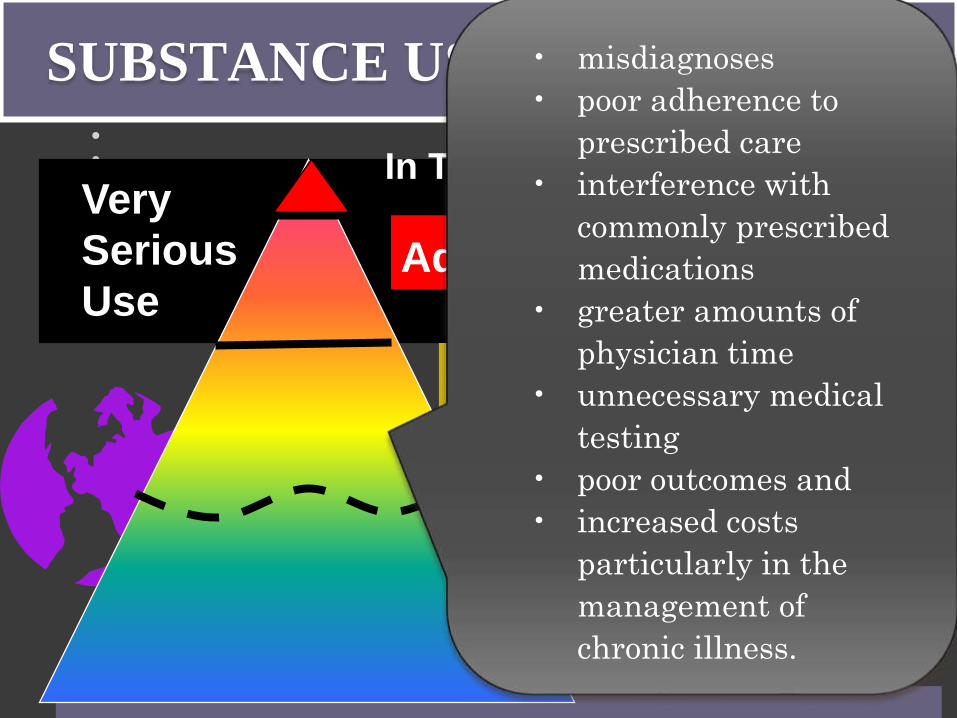
SUBSTANCE USE AMONG US
ADULTS
Addiction ~ 23,000,000
“Harmful – 40,000,000
Use”
Little or No UseLittle/No
Use
Very
Serious
Use
In Treatment ~ 2,300,000
Prevention
Early
Intervention
Treatment
40
billion
80
billion

16 week, N=240 School-Based
8 session, N=13
AGE
GENDER
16.9 15.46
MALES 16.6 (66%) 15.38 (62%)
FEMALES 17.5 15.6
PSYCHIATRIC DX (any) 232 (97%) 5 (38% )
Mean # psychiatric dx 2.3 0.54
SUD DX (any)
# substance diagnoses
Days/past 28 day substance use
240(100%)
2.7 incl tob
2.4 w/o tob
11/28
13 (100%)
1.3 incl tob
1.2 w/o tob
12/28
BASELINE DEMOGRAPHIC
CLINICAL CHARACTERISTICS
Compared to 16 week
community-based
Encompass, HS students
referred to school-based
Encompass:
• About 1 year younger
• 4x less
psychopathology/psychiat
ric comorbidity
• ½ as many SUD
diagnoses
• …but all met dx
criteria for cannabis
use disorder (CUD)
and were using as
many days at
baseline

TREATMENT
COMPLETION
CBT COMPLIANCE* Encompass
16 week
N=180
School -based
8 session
N=13
Tx Completion
CBT Compliance
61%
90%
69%
94%
% achieving at least 1 month 46% 56%
Abstinence by end of
treatment (UDS)
Cannabis Youth Treatment Study: Main findings from 2 Randomized
Trials
“Of the adolescents assigned to one of the four 12- to 14-week treatment
interventions, 52% had at least 90 day lengths of stay”; < 20 % achieved abstinence
by the end of treatment Dennis et al J Subst Ab Tx 2004
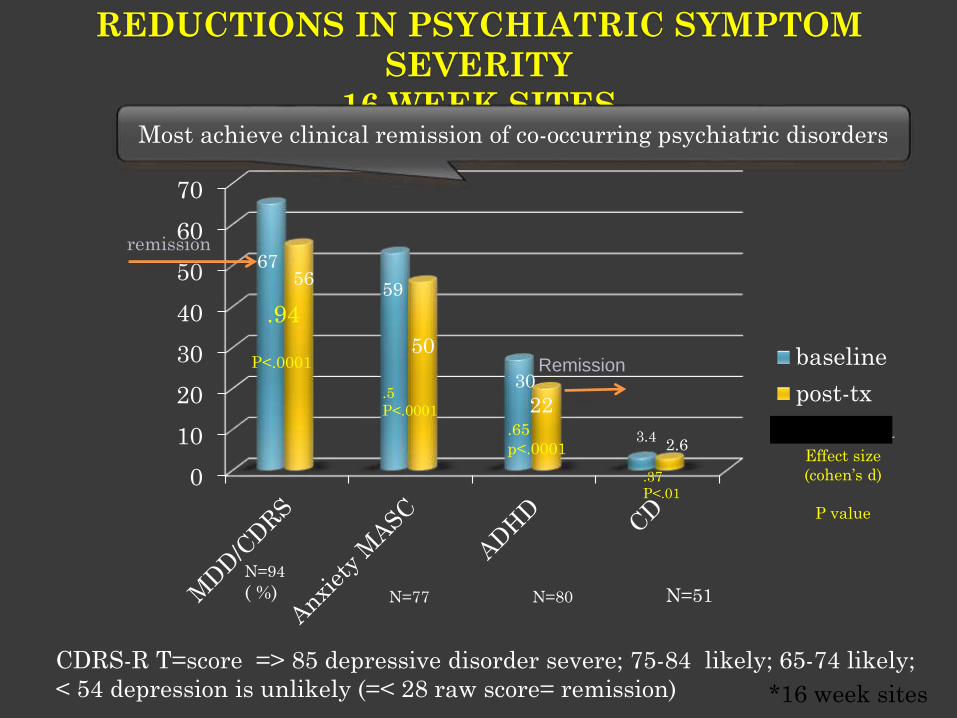
REDUCTIONS IN PSYCHIATRIC SYMPTOM
SEVERITY
16 WEEK SITES
*16 week sites
0
10
20
30
40
50
60
70
baseline
post-tx
Column1
Remission
remission67
5659
50
30
3.42.6
N=94
( %) N=77 N=80 N=51
Most achieve clinical remission of co-occurring psychiatric disorders
Effect size
(cohen’s d)
P value
.94
.65
p<.0001
P<.0001
.5
P<.0001
.37
P<.01
CDRS-R T=score => 85 depressive disorder severe; 75-84 likely; 65-74 likely;
< 54 depression is unlikely (=< 28 raw score= remission)
22

1
1. Because it will improve 2. Save money
3. It’s the law.
“Substance use disorders” will soon be part of
mainstream healthcare
1. Improve medical care
BECAUSE IT WILL
SUBSTANCE USE PREVALENCE
Addiction ~ 23,000,000
Harmful – 40,000,000Use
Little or No Use
Very
Serious
Use
In Treatment ~ 2,300,000
• misdiagnoses
• poor adherence to
prescribed care
• interference with
commonly prescribed
medications
• greater amounts of
physician time
• unnecessary medical
testing
• poor outcomes and
• increased costs
particularly in the
management of
chronic illness.
EXAMPLE #1
ALCOHOL USE AND BREAST CANCER
Before Diagnosis – heavy drinkers
1.5 times chance of contracting
2.3 times chance w/BRAC2 gene
After Diagnosis – ANY Drinking
Increases risk of relapse
Interferes radio & chemo therapy

SUBSTANCE USE COST IN
HEALTHCARE
Addiction ~ 23,000,000
“Harmful – 40,000,000
Use”
Little or No UseLittle/No
Use
Very
Serious
Use
In Treatment ~ 2,300,000
$80
B/Yr
$40
B/ Yr

• Physician Visits – 100%
• Clinic Visits – 100%
• Home Health Visits – 100%
• LABS-Glucose Tests, Monitors, Supplies – 100%
• HgA1C, eye, foot exams 4x/yr – 100%
• MEDS-Insulin and 4 other Meds –100%
• Smoking Cessation – 100%
• Personal Care Visits – 100%
• Language Interpreter – Negotiated
2010 MEDICAID BENEFIT
DIABETES BENEFIT SUD
• Detoxification – 100%
Ambulatory – 80%
• Opioid Substitution Therapy – 50%
• Urine Drug Screen – 100%
7 per year
NEW SUD BENEFIT
• Physician Visits – 100%
– Screening, Brief Intervention, Assessment
– Evaluation, medication – Tele monitoring
• Clinic Visits – 100%
• Home Health Visits – 100%
– Family Counseling
• LABS- Alcohol and Drug Testing – 100%
• Monitoring Tests (urine, saliva, other)
• MEDS --Maintenance and Anti-Craving Meds – 100%
• Smoking Cessation – 100%
•
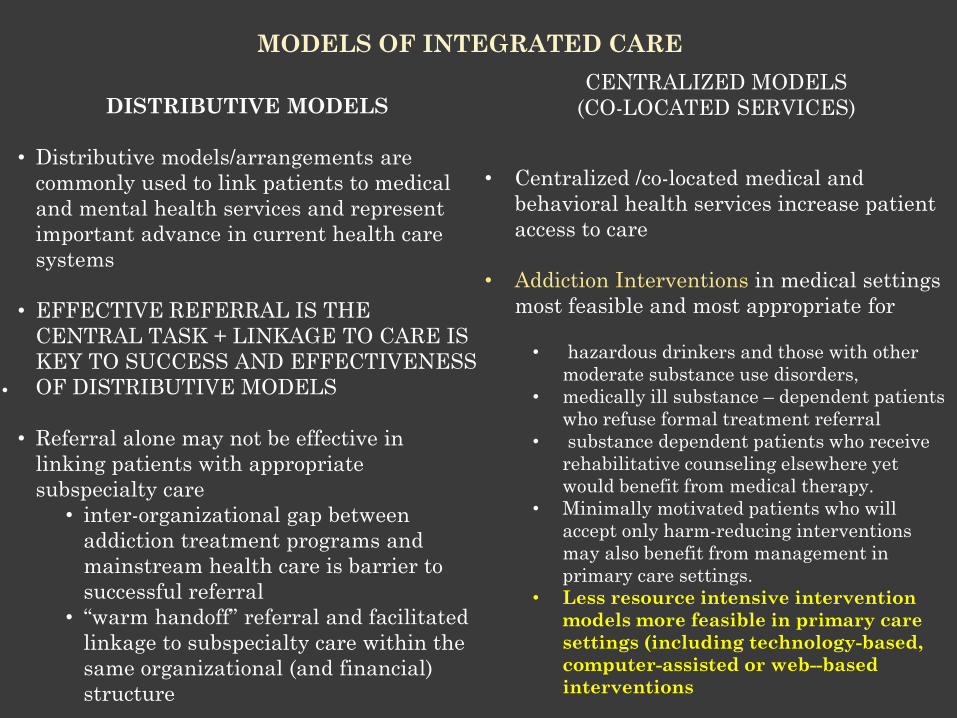
MODELS OF INTEGRATED CARE
CENTRALIZED MODELS
(CO-LOCATED SERVICES)
• Centralized /co-located medical and
behavioral health services increase patient
access to care
• Addiction Interventions in medical settings
most feasible and most appropriate for
• hazardous drinkers and those with other
moderate substance use disorders,
• medically ill substance – dependent patients
who refuse formal treatment referral
• substance dependent patients who receive
rehabilitative counseling elsewhere yet
would benefit from medical therapy.
• Minimally motivated patients who will
accept only harm-reducing interventions
may also benefit from management in
primary care settings.
• Less resource intensive intervention
models more feasible in primary care
settings (including technology-based,
computer-assisted or web--based
interventions
DISTRIBUTIVE MODELS
• Distributive models/arrangements are
commonly used to link patients to medical
and mental health services and represent
important advance in current health care
systems
• EFFECTIVE REFERRAL IS THE
CENTRAL TASK + LINKAGE TO CARE IS
KEY TO SUCCESS AND EFFECTIVENESS
OF DISTRIBUTIVE MODELS
• Referral alone may not be effective in
linking patients with appropriate
subspecialty care
• inter-organizational gap between
addiction treatment programs and
mainstream health care is barrier to
successful referral
• “warm handoff” referral and facilitated
linkage to subspecialty care within the
same organizational (and financial)
structure
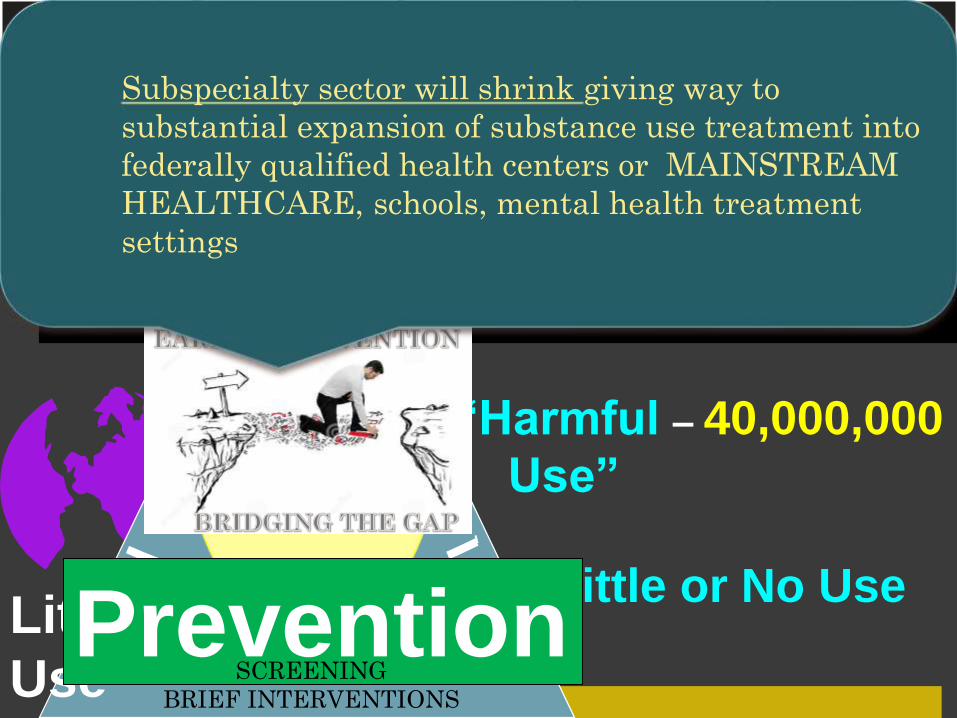
SUBSTANCE USE AMONG US
ADULTS
Addiction ~ 23,000,000
“Harmful – 40,000,000
Use”
Little or No UseLittle/No
Use
Very
Serious
Use
In Treatment ~ 2,300,000
Prevention
Treatment
SCREENING
BRIEF INTERVENTIONS
Subspecialty sector will shrink giving way to
substantial expansion of substance use treatment into
federally qualified health centers or MAINSTREAM
HEALTHCARE, schools, mental health treatment
settings

Comments ?
Questions ?
Discussion?





























