Embed Size (px)
Citation preview

International Journal of
Molecular Sciences
Review
Advances in Skin Regeneration UsingTissue Engineering
Komal Vig *, Atul Chaudhari, Shweta Tripathi, Saurabh Dixit, Rajnish Sahu, Shreekumar Pillai,Vida A. Dennis and Shree R. Singh
Center for Nanobiotechnology Research, Alabama State University, 1627 Harris Way, Montgomery,AL 36104, USA; [email protected] (A.C.); [email protected] (S.T.); [email protected] (S.D.);[email protected] (R.S.); [email protected] (S.P.); [email protected] (V.A.D.); [email protected] (S.R.S.)* Correspondence: [email protected]; Tel.: +1-334-229-5132
Academic Editor: John G. HardyReceived: 9 February 2017; Accepted: 4 April 2017; Published: 7 April 2017
Abstract: Tissue engineered skin substitutes for wound healing have evolved tremendously over thelast couple of years. New advances have been made toward developing skin substitutes made up ofartificial and natural materials. Engineered skin substitutes are developed from acellular materialsor can be synthesized from autologous, allograft, xenogenic, or synthetic sources. Each of theseengineered skin substitutes has their advantages and disadvantages. However, to this date, a completefunctional skin substitute is not available, and research is continuing to develop a competent fullthickness skin substitute product that can vascularize rapidly. There is also a need to redesign thecurrently available substitutes to make them user friendly, commercially affordable, and viable withlonger shelf life. The present review focuses on providing an overview of advances in the field oftissue engineered skin substitute development, the availability of various types, and their application.
Keywords: tissue engineering; skin regeneration; skin substitutes
1. Introduction
Skin is the barrier between the internal and external environment and is the largest organ ofthe human body. Due to the presence of stem cells, the wounded epidermis is able to stimulateself-regeneration. However, in case of deep injuries and burns, the process of healing is not adequate,thus leading to a chronic wound. Any loss of full-thickness skin more than 4 cm diameter needsgrafting for its treatment [1]. Additionally, many chronic wounds fail to heal, which can lead toamputations and mortality. These can also escalate health care costs. Surgical procedures availablefor skin healing often have limited availability of healthy donor tissue. The use of foreign tissue doesprovide a substitute; however, it also poses a risk of infection and immune rejection.
Tissue engineered skin substitutes are upcoming alternatives to traditional wound healingstrategies and tissue regeneration. Among the tissue engineered organs, skin was the first engineeredorgan that went from laboratory research to patient care [2]. Over recent decades, variousbioengineered and synthetic substitutes have been developed, which are generally positioned withinthe injury and provide the barrier function along with protection against microorganisms, reduction ofpain in wounds, and promotion of wound healing by tissue regeneration [3–5].
The field of tissue engineering is an evolving field, and newer procedures are being developedand adopted to generate skin substitutes for clinical applications, even though the high cost fordeveloping these substitutes is a major concern. The current review highlights the progress in the fieldof tissue-engineering and investigates various commercially available skin substitutes along with theiradvantages and shortcomings.
Int. J. Mol. Sci. 2017, 18, 789; doi:10.3390/ijms18040789 www.mdpi.com/journal/ijms

Int. J. Mol. Sci. 2017, 18, 789 2 of 19
2. Anatomy of Skin
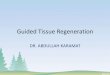
The skin is the largest organ of the body. It compromises 15% of the total adult body weightand provides protection against external physical, chemical, and biologic agents. It also plays role inthermoregulation. Skin consists of three layers: epidermis, dermis, and hypodermis (subcutaneouslayer) (Figure 1). The outermost portion of the epidermis, the Stratum corneum, is comparatively morewaterproof than other layers and thus inhibits entry of pathogens and other foreign substancesinto the body. It is multi-layered, with cells extending from the basement membrane to thedermis. The basement membrane contains progenitor cells, which differentiate into keratinocytes.Keratinocytes differentiate and mature as they move towards the surface of skin. The keratinizedlayer of dead cells at the skin provides barrier properties to skin [6]. Skin color pigment, melaninproduced by melanocytes, are present in basal layer of the epidermis. Melanin also helps to filter outultraviolet radiation from sunlight. The epidermis also has Langerhans cells, which are part of theskin’s immune system.
Int. J. Mol. Sci. 2017, 18, 789 2 of 18
field of tissue-engineering and investigates various commercially available skin substitutes along with their advantages and shortcomings.
2. Anatomy of Skin
The skin is the largest organ of the body. It compromises 15% of the total adult body weight and provides protection against external physical, chemical, and biologic agents. It also plays role in thermoregulation. Skin consists of three layers: epidermis, dermis, and hypodermis (subcutaneous layer) (Figure 1). The outermost portion of the epidermis, the Stratum corneum, is comparatively more waterproof than other layers and thus inhibits entry of pathogens and other foreign substances into the body. It is multi-layered, with cells extending from the basement membrane to the dermis. The basement membrane contains progenitor cells, which differentiate into keratinocytes. Keratinocytes differentiate and mature as they move towards the surface of skin. The keratinized layer of dead cells at the skin provides barrier properties to skin [6]. Skin color pigment, melanin produced by melanocytes, are present in basal layer of the epidermis. Melanin also helps to filter out ultraviolet radiation from sunlight. The epidermis also has Langerhans cells, which are part of the skin’s immune system.
Figure 1. Normal skin structure.
The dermis is the thickest of the three layers of skin and is present just below the epidermis. It is a connective tissue made of extra cellular matrix (ECM), fibroblasts, vascular endothelial cells, along with hair follicles, sweat glands, sebaceous glands, blood vessels and nerve endings [6]. Fibroblasts are the main population of the dermis, which secretes collagen and elastin and thus provides mechanical strength and elasticity to the skin.
Below the dermis is the adipose tissue hypodermis layer. It provides insulation and cushioning between the skin and skeletal structures, such as bone and muscle. It also serves as an energy storage area [6].
3. Wounds
Each year in the United State alone, there are 70,000 burn injuries [7] and 600,000–1,500,000 venous leg ulcers injuries [8]. The treatment of wounds costs nearly $20 billion annually in the US [9].
Wound treatment mainly includes quick closure of wound to reinstate the barrier function of skin and prevent infection, along with pain suppression and functional recovery. Wound healing in skin is initiated by fibroblasts, which deposit a temporary tissue matrix. This is followed by inflammation and re-epithelization by keratinocytes. Further wound revascularization along with ECM deposition, angiogenesis, and remodeling takes place for wound healing and restoration [6,10].
Figure 1. Normal skin structure.
The dermis is the thickest of the three layers of skin and is present just below the epidermis. It is aconnective tissue made of extra cellular matrix (ECM), fibroblasts, vascular endothelial cells, alongwith hair follicles, sweat glands, sebaceous glands, blood vessels and nerve endings [6]. Fibroblasts arethe main population of the dermis, which secretes collagen and elastin and thus provides mechanicalstrength and elasticity to the skin.
Below the dermis is the adipose tissue hypodermis layer. It provides insulation and cushioningbetween the skin and skeletal structures, such as bone and muscle. It also serves as an energy storagearea [6].
3. Wounds
Each year in the United State alone, there are 70,000 burn injuries [7] and 600,000–1,500,000 venousleg ulcers injuries [8]. The treatment of wounds costs nearly $20 billion annually in the US [9].
Wound treatment mainly includes quick closure of wound to reinstate the barrier function of skinand prevent infection, along with pain suppression and functional recovery. Wound healing in skin isinitiated by fibroblasts, which deposit a temporary tissue matrix. This is followed by inflammationand re-epithelization by keratinocytes. Further wound revascularization along with ECM deposition,angiogenesis, and remodeling takes place for wound healing and restoration [6,10].

Int. J. Mol. Sci. 2017, 18, 789 3 of 19
Every trauma often results in acute skin wounds. After the repair process, these wounds oftenlead to a benign scar if not treated in time [11]. However, depending upon the extent of the wound areaand/or depth, sometime, a chronic or non-healing wound can also result. Wounds that do not proceedthrough orderly and timely restitution of structural and functional integrity often results in chronicwounds. Generally, vascular insufficiency, local-pressure effects, and conditions like diabetes mellitus,along with compromised nutritional or immunological status, are the major causes of non-healing skinwounds. Healing capability of a wound is affected by aging, which leads to decreased strength andelasticity of skin, decreased blood flow to the extremities, and psychological stress [12,13].
4. Process of Skin Wound Healing
After a skin injury, the damaged tissue is restored through coordinated signaling that constitutesthe cutaneous healing response. This cutaneous response proceeds in three phases: the inflammatoryphase, proliferation phase, and maturation phase. The inflammatory phase of wound healing typicallylasts for the initial four days [14] and begins with coagulation of blood resulting in a blood clotthat provides a temporary shield against pathogens as well as fluid loss. It is followed by increasedblood flow in the areas adjacent to the wound trailed by swelling and redness due to increasedvascular permeability by local inflammatory agents (activated complement, histamine, etc.) leadingto plasma extravasation and generation of a fibrin matrix [6]. Neutrophils, monocytes, and otherimmunocompetent cells invade this matrix to remove dead tissue and control infection.
After the inflammatory phase, between 5–20 days, proliferation of vascular endothelial cells andfibroblasts is promoted due to secretion of growth factors by inflammatory cells. Fibrin matrix isgradually replaced by collagen secreted by fibroblasts. Fibroblasts can differentiate into myofibroblastsexpressing actin resulting in contraction and reduction of the wound area. Adjacent healthy tissue,as well as endothelial progenitors, initiate angiogenesis, which leads to invasion of vascular endothelialcells and capillaries, resulting in the formation of “granulation tissue” [6]. It is followed by migrationof keratinocytes from the edges of the wound to the surface of the granulation tissue, below the bloodclot [14].
During the last phase of maturation, re-epithelialization of the wound takes place along withdermis regaining its tensile strength. However, the scar continues to remodel over several months toyears [6].
5. Conventional Treatments for Wound Healing
Different strategies have been employed for wound treatments, which are discussed below:
5.1. Skin Grafting with Autograft
Due to lack of keratinocytes to reform the epithelium, deeper dermal wounds heal slowly andinadequately. Skin grafting with an “autograft” is recommended for such wounds [15]. Skin autografttechnique was used in India in premodern times [16]. A thin layer of skin that includes the fullepidermis and a portion of the dermis, known as split-thickness graft, is shaved from the donor site,such as inner thighs and buttocks, using a dermatome, and is then placed on the wound site [17].The healing of wound depends on thickness of the underlying dermis in the graft. Thick dermis leadsto faster healing and better cosmetic and aesthetic aspect of the healed wound. Donor sites can bereharvested a few times after healing, as the sites thin down due to lack of regeneration of the dermisafter each harvest. Since an autograft is derived from the patient’s own tissue, there is no risk ofrejection [15].
5.2. Skin Allografts
A method to overcome the limitation of donor tissue for skin grafting with an autograft is to useallografts. Human skin allograft clinical use was first described in the manuscript of Branca of Sicily in1503. Skin allografts have been used since World War II.

Int. J. Mol. Sci. 2017, 18, 789 4 of 19
Cadavers are a good source of allografts. As cadavers are stored frozen in skin banks, they can beused as needed [18]. Allografts from cadavers are used extensively in burn wound management inmany burn centers all over the world. Skin allografts can also be obtained from living donors.
A viable skin allograft can revascularize like autologous split skin grafts. Though allografts notonly provide a barrier along with promoting angiogenesis, providing growth factors, and essentialcytokines for wound healing [19], they also serve as a temporary cover due to immunogenic rejectionby the host’s immune system [15,20] and viral transmission (e.g., hepatitis B and C or HIV). Applicationof human skin allograft guards underlying tissue while allowing granulation tissue formation andwound contraction. Subsequent skin autograft and secondary skin contraction and epithelializationprovide satisfactory wound closure [21].
5.3. Xenografts
A surgical graft from one species to another dissimilar species is known as xenograft. Skinsubstitutes harvested from the animals that are used on human wounds constitute xenograft andcan be used as temporary grafts for human wounds. Xenograft fuses exogenous collagen into thewound, thus assisting dermal regeneration. These xenografts get absorbed as the wound heals, thusmaking them perfect for surgical wounds [22]. Skin xenograft was reported in the Papyrus of Ebersin the 15th century BC [19]. The earliest reported xenograft was with frog skin in 1500 BC. These areusually employed as temporary coverage [23]. Most commonly used xenografts are from porcine skin,which is often used in burn care [19].
5.4. Amnion
Since 1910, amnion has been used as a dressing for burns [19]. Amnion is primarily used for partialthickness burns, such as facial burns, and is one of the most effective biological skin substitutes [24].Amnion is also used in sandwich grafting technique. Amnion is usually collected from the placentaeof selected and screened donors and preserved for further use. It reduces loss of protein, electrolytes,and fluids, minimizes pain, decreases the risk infection, and accelerates wound healing. In a recentclinical trial, amnion dressing was used for the donor site on 32 patients, which resulted in fastepithelialization and wound healing [25], thus, improving pain, through use of less analgesics, lowrate of immobilization, and resulted in the earlier discharge of patients. Amniotic membrane is rich incollagen and several growth factors that support the healing process to both advance wound closureand diminish scar formation. Its distinctive properties include the lack of immunologic markers,antibacterial properties, and the ability to reduce pain on application. Recently, techniques havebeen developed to dehydrate the amnion while preserving many of these wound-healing attributes,to produce a temperature-stable allograft [26].
6. Newer Approaches for Tissue Engineering
Different strategies, such as injecting growth factors and extracellular matrix, are being adoptedtowards tissue re-growth and wound healing. Some of the recent strategies are listed below.
6.1. Cell Cocultures
Cell-based approach to develop skin substitutes usually involves differentiated, embryonic,or induced pluripotent stem cells. Cells such as human dermal fibroblasts [27], foreskin derivedkeratinocytes [28], keratinocyte stem cells [29], hair follicle stem cells [30], angiogenic endothelialprogenitor cells [31], bone marrow-derived mesenchymal stem cells [32], and adipose tissuederived mesenchymal stem cells [33] are mainly used for wound healing and tissue regeneration.Work is progressing toward co-culturing cells for tissue generation that involves keratinocytes andfibroblasts [34,35]. Keratinocyte sheets of stratified epithelia can be reconstructed from human epithelialcells [36,37]. Moreover, cultured dermal substitutes containing fibroblasts can be added to keratinocytessheets. Fibroblast cells can stimulate keratinocyte growth and differentiation by either secreting soluble

Int. J. Mol. Sci. 2017, 18, 789 5 of 19
growth factors or via cell–cell contacts and cell matricial element contacts. In turn, keratinocytes canpositively affect fibroblast proliferation [38]. Dermal fibroblasts are also important in skin remodelingand acute wound contraction [39]. Melanocytes and Langerhans’ cells can also be cultured along withkeratinocytes and fibroblasts. Melanocytes can recreate the natural pigmentation process whereasLangerhans’ cells monitor skin immunological reactions. Recently, complex three-dimensional (3D)models are being developed using these co-cultured cells with the goal of making engineered tissuessimilar to their natural counterparts. An exclusive full-thickness 3D skin equivalent was developed tomodel early melanoma invasion by incorporating an inert scaffold with suitable pore sizes to supportthe 3D development and cell–cell interaction of primary human dermal fibroblasts [40].
6.2. Cultured Epithelial Autografts
Epithelial autografts are used in burn care [41,42] and were first reported in clinical use in1981. These autografts can be constructed using keratinocytes. Keratinocytes were first culturedsuccessfully in the laboratory about 30 years ago [43,44]. Keratinocyte cells can be generated froma small biopsy of healthy skin, expanded into sheets for few weeks, which is then co-cultured onmouse fibroblasts [45,46]. Epithelial autografts are, however, limited due to difficulty of handling,unpredictable uptake, and high cost, and thus need a delivery system or a support dressing.
6.3. Tissue Engineered Skin Substitutes
Due to deficiency of donor skin graft supplies, tissue-engineered skin substitutes present anefficient alternative in substituting donor skin grafts. Skin substitutes are emerging therapeutic toolswith a wide range of applications. Skin substitutes act as a temporary protective cover of the woundbed, thus protecting damaged regions from fluid loss and contamination along with accelerating thewound-healing processes by promoting release of cytokines and growth factors at the wound site [47].
An absorbent dressing made of cotton wool sandwiched between layers of gauze was describedby Joseph Gamgee in 1880 and used as “skin substitutes” for treating wounds [48]. Likewise, in1895, Mangoldt described a technique of “epithelial cell seeding” for treating chronic wounds [45].His technique involved harvesting epithelial cells from superficial epithelium of skin and seedingthem onto the wounds [49]. Similarly, in 1897, Lunggren kept skin fragments alive by inoculatingthem in ascitic fluid at room temperature [45,50]. Likewise, keratinocytes were grown successfully onlethally irradiated murine fibroblasts [43,45]. Cultured autologous epithelium was used to cover burndefects for the first time by O’Conner [42,48]. Likewise, a dermal substitute was developed based oncollagen gel with fibroblasts to which an epidermal layer was added, thus making a “skin equivalent”,“composite culture”, or “organotypical culture” [45,50].
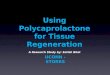
Tissue engineered skin substitute preparation involves cells and/or extracellular matrix(ECM) [18] (Figure 2). An ideal synthesized skin substitute should be sterile, act like a barrier, havelow inflammatory response, provide no local or systemic toxicity, and allow water vapor transmissionsimilar to normal skin. These skin substitutes should also adhere to wound surface rapidly, haverequired physical and mechanical properties, and go through controlled degradation [51]. They shouldalso be easy to handle, agile to conform to irregular wound surfaces, relatively inexpensive, andfacilitate angiogenesis. They should also have a long shelf-life with low storage requirements andstress resistance in engineered skin substitutes [52]. When biomaterials are used for substitutes, theyshould be biodegradable, repairable, non-toxic, non-immunogenic, and non-inflammatory with lowrisk of disease transmission. Easy availability, long-shelf life, and user-friendliness makes an idealengineered substitute. A suitable biomaterial is crucial in the development of functional engineeredtissues. Different approaches have been adopted to develop engineered tissues, such as syntheticmembranes for mono- or multi-layered cultures and 3D matrices for full-thickness models. Propertiesof the “ideal” skin substitute for in vivo use have recently been reviewed by MacNeil [51].

Int. J. Mol. Sci. 2017, 18, 789 6 of 19
Int. J. Mol. Sci. 2017, 18, 789 6 of 18
[7,46,53,54]. The presence of a large number of cells, especially stem cells, in tissue engineered skin enables regeneration of native-like skin in burn patients.
Figure 2. Tissue engineered skin substitute preparation. Bold lines indicate cell type for tissue engineered substitute and dotted lines indicate cell source.
Tissue engineered skin is mainly of three types: (a) cultured epidermal cells with no dermal components; (b) with only dermal components; or (c) a bilayer containing both dermal and epidermal components [55]. Although, each of these has their own advantages and applications, none of them can fully simulate native skin.
7. Types of Skin Substitutes
Currently, available skin-substitutes can be classified in different ways [4,49,51,55–57]. Based on duration of cover, they are classified as permanent, semi-permanent or temporary. Based on anatomical structure, they are classified as epidermal, dermal, or dermo-epidermal (composite). They can also be classified based on skin substitute composition as cellular or acellular. Similarly, based on the type of the biomaterial used, they can be biological (autologous, allogeneic, xenogeneic) or synthetic (biodegradable, non-biodegradable).
Synthetic skin substitutes are made up of acellular materials. They are designed primarily to function as barriers to fluid loss and microbial contamination. Commonly used synthetic acellular skin substitutes are Biobrane®, Integra®, Alloderm™, and TransCyte™. The natural skin substitutes, commonly called tissue engineered skin, are mainly cultured allogenic or autologous cell suspensions or sheets, which are used on their own or along with a dermal matrix. Examples of frequently used natural skin substitutes with allogeneic cells include Dermagraft™, Apligraf™, and OrCel™, while those with autologous cells include Epicel™ (Table 1). These substitutes are further described below.
7.1. Acellular Skin Substitutes
The use of acellular skin substitute started in late 1970s and is used mainly as a temporary skin substitute for superficial or mid-dermal partial thickness wounds and burns. They can also be used for donor sites and congenital diseases, such as epidermolysis bullosa [58,59] and in hydradenitis suppurativa [60]. They usually consist of a nylon mesh or collagen, acting as a “dermis” and a silicon membrane as an “epidermis”. There are three kinds of commercial available acellular skin substitutes: Biobrane®, Integra®, and Alloderm (Figure 3a). Details about their composition are in Table 1.
Figure 2. Tissue engineered skin substitute preparation. Bold lines indicate cell type for tissueengineered substitute and dotted lines indicate cell source.
Tissue engineered skin provides both epidermal and dermal components required to achievefunctional wound closure and have therefore been used to effectively close full-thickness burn woundsand treating burns that are greater than 50% of the total burn surface area (TBSA) [7,46,53,54].The presence of a large number of cells, especially stem cells, in tissue engineered skin enablesregeneration of native-like skin in burn patients.
Tissue engineered skin is mainly of three types: (a) cultured epidermal cells with no dermalcomponents; (b) with only dermal components; or (c) a bilayer containing both dermal and epidermalcomponents [55]. Although, each of these has their own advantages and applications, none of themcan fully simulate native skin.
7. Types of Skin Substitutes
Currently, available skin-substitutes can be classified in different ways [4,49,51,55–57]. Based onduration of cover, they are classified as permanent, semi-permanent or temporary. Based on anatomicalstructure, they are classified as epidermal, dermal, or dermo-epidermal (composite). They can alsobe classified based on skin substitute composition as cellular or acellular. Similarly, based on thetype of the biomaterial used, they can be biological (autologous, allogeneic, xenogeneic) or synthetic(biodegradable, non-biodegradable).
Synthetic skin substitutes are made up of acellular materials. They are designed primarily tofunction as barriers to fluid loss and microbial contamination. Commonly used synthetic acellularskin substitutes are Biobrane®, Integra®, Alloderm™, and TransCyte™. The natural skin substitutes,commonly called tissue engineered skin, are mainly cultured allogenic or autologous cell suspensionsor sheets, which are used on their own or along with a dermal matrix. Examples of frequently usednatural skin substitutes with allogeneic cells include Dermagraft™, Apligraf™, and OrCel™, whilethose with autologous cells include Epicel™ (Table 1). These substitutes are further described below.
7.1. Acellular Skin Substitutes
The use of acellular skin substitute started in late 1970s and is used mainly as a temporary skinsubstitute for superficial or mid-dermal partial thickness wounds and burns. They can also be usedfor donor sites and congenital diseases, such as epidermolysis bullosa [58,59] and in hydradenitissuppurativa [60]. They usually consist of a nylon mesh or collagen, acting as a “dermis” and a siliconmembrane as an “epidermis”. There are three kinds of commercial available acellular skin substitutes:Biobrane®, Integra®, and Alloderm (Figure 3a). Details about their composition are in Table 1.

Int. J. Mol. Sci. 2017, 18, 789 7 of 19Int. J. Mol. Sci. 2017, 18, 789 7 of 18
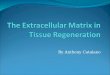
Figure 3. Tissue engineered skin substitutes. (a) Acellular: i. Karoderm ii. Biobrane iii. Integra (b) Epidermal Autologous: i. Cell Spray ii. Epicel iii. Laserskin (c) Dermal Autologous: i. Hyalograft 3D (d) Dermal Allogenic: i. TransCyte ii. Dermagraft (e) Dermal Xenogenic: i. Permacol (f) Epidermal/Dermal (Composite) Autologous i. Tissue tech Autograft system (g) Epidermal/Dermal (Composite) Allograft i. Apligraf.
Figure 3. Tissue engineered skin substitutes. (a) Acellular: i. Karoderm ii. Biobrane iii. Integra (b) Epidermal Autologous: i. Cell Spray ii. Epicel iii. Laserskin (c)Dermal Autologous: i. Hyalograft 3D (d) Dermal Allogenic: i. TransCyte ii. Dermagraft (e) Dermal Xenogenic: i. Permacol (f) Epidermal/Dermal (Composite)Autologous i. Tissue tech Autograft system (g) Epidermal/Dermal (Composite) Allograft i. Apligraf.

Int. J. Mol. Sci. 2017, 18, 789 8 of 19
7.2. Cellular Allogenic Skin Substitutes
Cellular allogenic skin substitutes are mainly produced using living neonatal foreskin fibroblastswith a mesh or a matrix. They have been used successfully in vestibuloplasty, after mucogingivaljunction and supra-periosteal dissection [46,49]. They have also been used for treatment of venousand diabetic ulcers along with wound management in epidermolysis bullosa, skin cancer, and inburns [46,49]. Examples include Transcyte®, Dermagraft®, Apligraf®, and Graftskin® (Figure 3d,f,g).
7.3. Cellular Autologous Skin Substitutes
Acellular or cellular allogenic skin substitutes only provide temporary coverage to raw skinsurfaces. These have to be either replaced by a split skin graft or re-grafted in the case of large wounds.In the case of smaller wounds, gradual epithelialization from the wound itself is required.
Cultured autologous keratinocytes provide more permanent skin coverage for various types ofwounds. These cells are cultured based on the Rheinwald and Green [43,44] technique. There aretwo types of cellular autologous skin substitutes available: Cultured Epidermal Autograft (CEA) andCultured Skin Substitutes (CSS).
CEA involves the culture of autologous keratinocytes, derived from skin biopsy of thepatient [45,46]. However, after few weeks, it is challenging to handle these keratinocytes, thus requiringa delivery system or a supporting dressing [48,49]. Commercially available CEAs have differentdelivery or carrier systems. Keratinocytes alone may not heal full thickness wounds or burns. Anotherconcern with CEA is the growth of blisters with friction, since their dermal epidermal junction is notcompletely developed. It can also lead to increased scarring, contracture and hyperkeratosis [46].Furthermore, due to the digestive properties of collagenase enzymes within the wound bed, theuptake of CEA is reduced to about 30%–80%. To overcome the issue of CEA uptake, an alternatemethod was developed [18,48], which included acclimatization of the wound bed with cadavericallogenic skin for four days before grafting followed by placing autologous cells after stripping theallo-epidermis [18,48].
CSS is an autologous graft with both epidermal and dermal components. It acts as a permanentcoverage with well-formed dermal-epidermal junction and is easy to handle. CSS is expensive and hasa longer preparation time. [18,46,49]. Different dermal biosynthetic scaffolds are being used to developseveral types of CSS. Hyaluronic acid derived substitute is often used to prepare CSS. These types ofCSS can stimulate fibroblasts growth and movement, controls osmoregulation and matrix hydration,scavenge free radicals and regulate inflammation [61,62].
7.4. Commercially Available Skin Substitutes
There are many commercial skin substitutes, permanent or temporary, that are available inthe market designed for use with specific clinical issues [19,22,51,55,63,64]. Commercially availableengineered skin substitutes’ models vary in techniques and cell sources (Figure 3). Table 1 lists some ofthe commercially available skin substitutes.
Table 1. Commercially available skin substitutes.
Substitute Type Product Company Components References
Acellular
Alloderm® LifeCell Inc., Branchburg,NJ, USA Human acellular lyophilized dermis [18,22,46,49,65]
SureDerm HANS BIOMEDCorporation, Daejeon, Korea Human acellular lyophilized dermis -
OASIS Wound Matrix Cook Biotech Inc., WestLafayette, IN, USA
Porcine acellular lyophilized smallintestine submucosa [66]
Biobrane® Mylan BertekPharmaceuticals, USA
Ultrathin silicone as epidermal analog film and3D nylon filament as dermal analog with type Icollagen peptides
[46,49,55]
Integra® DRT (dermalregeneration template)
Integra® LifeSciences Corp.,USA
Dermal analog—bovine collagen andchondroitin-6-sulfate GAG; epidermalanalog—silicone polymer polysiloxane
[18,46,49,55]

Int. J. Mol. Sci. 2017, 18, 789 9 of 19
Table 1. Cont.
Substitute Type Product Company Components References
Epidermal
Autologous
EpiDex Modex Therapeutiques,Lausanne, Switzerland
Cultured keratinocytes from outer root sheathof scalp hair follicles (confluent cell sheet) [67]
EPIBASE Laboratoires Genevrier,Antibes, France Cultured keratinocytes (confluent cell sheet) -
MySkin CellTran Ltd., UKCultured keratinocytes (subconfluent cell sheet)silicone support layer with a speciallyformulated surface coating
[68]
Bioseed-S BioTissue TechnologiesGmbH, Germany
Cultured keratinocytes (subconfluent cellsuspension) fibrin sealant [69]
CellSpray Clinical Cell Culture (C3),Australia
Non-/cultured keratinocytes(subconfluent cell suspension) [70–72]
Epicel® Genzyme Biosurgery, USA Sheets of autologous keratinocytes attached topetrolatum gauze support [73]
Laserskin® orVivoderm
Fidia AdvancedBiopolymers Srl, Italy
Autologous keratinocytes and fibroblasts,grown on microperforated hyaluronicacid membranes
[74]
Autoderm(Autologous InferiorDermal Sling)
XCELLentis NV, Belgium Cultured keratinocytes [75]
TransDerm XCELLentis NV, Belgium Cultured keratinocytes [75]
Lyphoderm XCELLentis NV, Belgium Lyophilized neonatal keratinocytes [76]
Cryoceal XCELLentis NV, Belgium Cryopreserved keratinocytes [77]
Dermal
Autologous
denovoDerm™ EUROSKINGRAFT,Switzerland Autologous dermal substitute [78]
PelnacStandard/Fortified Gunze Ltd., Japan Porcine tendon derived atelocollagen type I,
sponge layer with silicone film -
Hyalomatrix PA Fidia AdvancedBiopolymers, Italy
HYAFF (an ester of hyaluronic acid) layered onsilicone membrane -
Hyalograft 3D Fidia AdvancedBiopolymers, Italy
Cultured fibroblasts hyaluronic acidmembrane (HAM) [79,80]
Allogenic
Dermagraft® Advanced BioHealing, Inc.,USA
Bioabsorbable polygalactin mesh matrixseeded with human neonatal fibroblastsand cryopreserved
[78]
TransCyte® Advanced BioHealing, Inc.,USA
Collagen-coated nylon mesh seeded withallogenic neonatal human foreskin fibroblasts [81]
Terudermis Olympus TerumoBiomaterial Corp., Japan
Silicone, bovine lyophilized crosslinkedcollagen sponge made ofheat-denatured collagen
[82]
Cyzact (ICX-PRO) Intercytex, St John’sInnovation Center, UK
Cultured allogeneic human dermal fibroblastsembedded in a human fibrin gel matrix -
ICX-SKN skin graftreplacement
Intercytex, St John’sInnovation Center, UK
Cultured dermal fibroblasts natural humancollagen matrix -
Polycaprolactonecollagen nanofibrousmembrane
National University ofSingapore, Singapore
Cultured dermal fibroblastspolycaprolactone-blended collagen electrospunnanofibrous membrane
[83]
Tegaderm-nanofibreconstruct
National University ofSingapore, Singapore
Cultured dermal fibroblasts poly(e-caprolactone)/gelatin nanofibrous scaffoldelectrospun on polyurethane dressing
-
Collagen–glycosaminoglycan–chitosan dermal matrixseeded with fibroblasts
INSERM, FranceCultured dermal fibroblasts bovine collagenI/chondroitin-4/6-sulfate/chitosanlyophilized dermal matrix
[46,49,55]
Human hairkeratincollagen sponge
Southern Medical University,China
Cryomilled porcine acellular diisocyanitecross-linked dermis -
Hyaluronan-FNfdshydrogel matrix SUNY at Stony Brook, USA Hyaluronan coupled with fibronectin
functional domains [84]
Compositenano-titaniumoxide–chitosanartificial skin (NTCAS)
Cardinal Tien College ofHealthcare andManagement, Taiwan
Composite nano-titanium oxide–chitosan withgelatin and hyaluronic acid -

Int. J. Mol. Sci. 2017, 18, 789 10 of 19
Table 1. Cont.
Substitute Type Product Company Components References
Xenogeneic
Permacol SurgicalImplant
Tissue Science Laboratoriesplc, UK
Porcine acellular diisocyanitecrosslinked dermis [79,85]
Matriderm Dr Suwelack Skin andHealthCare AG, Germany
Bovine non-cross-linked lyophilized dermis,coated with a-elastin hydrolysate [79,85]
EZ DermTM Brennen Medical Inc., USA Porcine aldehyde cross-linked reconstituteddermal collagen [18]
Bovine collagencross-linked withmicrobialtransglutaminase
National University ofIreland, Ireland
Freeze-dried bovine collagen scaffoldcross-linked with microbial transglutaminase [86–88]
Collatamp SYNTACOLL AG,Switzerland Multilayer bovine collagen matrix -
Synthetic
Hybrid nanofibrousPLGA/chitosanmembrane
Tianjin University, China PLGA/chitosan hybrid electrospunnanofibrous membrane [83,89]
Biodegradablepolyurethanemicrofibers
University of Delaware,USA Biodegradable polyurethane microfibres [90]
Epidermal/Dermal (Composite)
Autologous
Permaderm™(Cincinnati ShrinersSkin Substitute)
Regeninic Inc.USAAutologous fibroblasts and keratinocytes inculture with bovine collagen andGAG substrates
[78]
Tiscover™ (A-Skin) Advanced Tissue MedicinalProduct, Netherlands Autologous full thickness cultured skin [78]
denovoSkin™ EUROSKINGRAFT, Univ. ofZurich, Switzerland
Autologous full thickness substitute consistingof dermal and epidermal layers [78]
PolyActive HC Implants BV,Netherlands
Cultured keratinocytes and fibroblastspolyethylene oxide terephthalate(PEO)/polybutylene terephthalate (PBT)
[91]
TissueTech AutograftSystem (Laserskin andHyalograft 3D)
Fidia AdvancedBiopolymers, Italy
Cultured keratinocytes and fibroblastsmicroperforated hyaluronic acidmembrane (HAM)
[74,79]
Allogenic
Apligraf® Organogenesis Inc., USA Bovine collagen matrix seeded with neonatalforeskin fibroblasts and keratinocytes [19,63,92,93]
OrCel®Ortec International Inc.,USA
Type I collagen matrix seeded with neonatalforeskin fibroblasts and keratinocytes [86–88]
Karoskin (Karocells) Karocell Tissue EngineeringAB, Sweden
Native human cadaver skin with dermal andepidermal cells [55]
CeladermTM Celadon Science LLC, USA Sheets of cells derived from neonatal(allogenic) foreskin [19,63,92,93]
StrataGraft™ Stratatech Corporation, USA Full thickness skin substitute with dermal andfully differentiated epidermal layers [79,94–96]
AcuDress DFB Pharmaceuticals, Inc.,USA Cultured keratinocytes fibrin substrate -
Allox DFB Pharmaceuticals, Inc.,USA
Sprayed suspension of allogeneic keratinocytesand fibroblasts in fibrin substrate -
Xenogeneic Oasis® Healthpoint Biotherapeutics,USA
Intact matrix from porcine small-intestinesubmucosa and intended for wound closurestimulation in acute, chronic andburns wounds
[79,85]
Skin substitutes like Biobrane®, Integra®, and Alloderm are made of acellular material, such asa nylon mesh or collagen (Figure 3a). Biobrane® and Integra® are synthetic bilayer skin substitutes.Biobrane® is made of a nylon mesh mimicking as a “dermis” and a silicone membrane as an“epidermis” implanted in porcine collagen [46,49,55]. Integra® consists of a silicone membrane asan epidermal layer and dermal layer made of bovine collagen and shark chondroitin-6-sulphateglycosaminoglycan [18,46,49]. Although, Biobrane is used for covering partial thickness burns in asingle stage procedure, it has the drawback of being intolerant to contaminated wound beds. Integra,on the other hand, has good long term aesthetic and functional outcome, but is a two stage processwith high cost and poor adhesion [97–100]. Integra may also include a high vulnerability to infection,graft loss and fluid entrapment, requiring fenestration of the tissue. Another substitute that fallsin this category is Advanced Wound Bioengineered Alternative Tissue (AWBAT) [22,101], which is

Int. J. Mol. Sci. 2017, 18, 789 11 of 19
made of porous silicone membrane bonded with a continuous 3D nylon structure that contains noncross–linked porcine type 1 collagen peptides.
Alloderm, Graftjacket, and GammaGraft are allografts derived from an acellular matrix obtainedfrom a cadaveric dermis [22]. As a decellularized tissue-engineered skin substitute, alloderm consistof a cell-free matrix incorporated into the wound bed [65]. It has a basement membrane but lacks anepidermal layer. The acellular matrix provides a good natural medium for fibroblast and endothelialcells to regenerate from the neoderm [18,46,49]. It is immunologically inert and offers natural dermalporosities for renewal and vascularization on the wound bed, but has the drawback of being a twostage very expensive technique with a risk of transmitting disease [51,91,102,103].
Other commercial skin substitutes such as ApligrafTM, CeladermTM, DermagraftTM, TrancyteTM,and OrCelTM (Figure 3), are constructed from sheets of cells derived from neonatal (allogenic)foreskin [19,63,92,93]. TransCyte™ has similar configuration to Biobrane® and consists of a nylonmesh seeded with fibroblasts cultured from neonatal human foreskin. The foreskin secretes ECMcomponents and growth factors for efficient tissue regeneration. It is often used as a temporary coverfor excised burns and considered more beneficial for wound healing compared to strictly syntheticskin substitutes [81,104]. Transcyte has the advantage of immediate availability and easy storage but isonly a temporary solution.
Dermagraft, on the other hand, is an allogeneic dermal substitute created by the combinationof living neonatal foreskin fibroblasts cells and biodegradable mesh from polyglycolic acidbiomaterials [105]. The fibroblasts are cryopreserved at −80 ◦C and when implanted to the wound,they regain their viability and proliferate and produce growth factors and ECM components [106].The polyglycolic acid mesh is absorbed within 3–4 weeks [46,49]. Dermagraft is easy to handle withcoverage to chronic wounds and diabetic ulcers with no rejection. However, it lacks strong ECMstructure leading to infections and cellulitis [51,98,103].
Skin substitutes of composite allograft category include ApligrafTM and OrcelTM. ApligrafTM
contain both living dermis and epidermis and is formulated by mixing living fibroblasts from neonatalforeskin with bovine collagen. This mixture is further exposed to heat to produce a loose matrix, whichdevelops a dermal fibrous network. Cells are proliferated on the dense fibrous matrix [61]. In thetreatment of venous leg ulcers and diabetic foot ulcers, Apligraf™ is often used [61]. Treating woundswith Apligraf for more than four weeks results in enhanced healing when compared with any otherskin substitute currently available in the market. The downside of Apligraf is that it is rather expensive,with a short shelf-life (range: 5–10 days), and although the risk is significantly low, there is a likelihoodof disease transmission owing to Apligraf being allogenic in nature [107,108]. Similar to ApligrafTM,OrCelTM is another skin substitute that is made up of fibroblasts seeded into a bovine collagen type Imatrix (dermal side) and keratinocytes cultured at the air–liquid interface (epidermal side) [86–88].It provides a favorable matrix for host cell migration and is used for grafting onto partial-thicknesswounds; nonetheless, there is an amplified risk of rejection and disease due to the presence of thebovine collagen [52,107].
Other skin substitutes like Permacol, Matriderm, and Oasis belong to the xenograft category [79,85].Permacol is made of porcine dermis, whereas Matriderm® is made of a matrix of bovine type I collagenwith elastin (Figure 3e). It is utilized for dermal regeneration. With the progression of healing process,fibroblasts lay down the ECM and the Matriderm® resorbs [109]. Permacol has a good aesthetic andfunctional outcome but is prone to infection, hematomas, and seromas [73,74], whereas, Matriderminvolves a single stage procedure with increased vascularization and elasticity of regenerating tissuebut lacks enough scientific evidence to verify its efficacy of a one-step procedure [103,110,111]. Anothersubstitute is Oasis, which is derived from porcine intestinal submucosa [79,85].
The commercially available CAE substitutes, such as Epicel™, are made of autologouskeratinocytes sheets attached to a petrolatum gauze support, which is detached approximately oneweek after grafting [73]. Epicel™ is used on patients with full-thickness burns covering more than30% total body surface area (TBSA). It is also used on patients with giant congenital nevus [73]. Epicel,

Int. J. Mol. Sci. 2017, 18, 789 12 of 19
however, has a longer generation time. It takes almost three weeks to culture the tissue for use. Sincethe tissue is an autograft, there is a very low risk of rejection [107,112].
Another variation of CAE substitutes is a suspension, such as Cell Spray (Figure 3b). Keratinocytesharvested in a suspension from a split-thickness donor biopsy is placed in the wound to createan epidermal cover. As the application is aerosolized, it allows complete coverage of contouredwounds [70–72,79]. The downside of this application is that there is a risk of infection or donorrejection [77–79].
Epidex is an additional CAE substitute, having small keratinocyte sheets cultured from patient’sfollicles [67]. It can be expanded in vitro for large burn areas. Though it is a permanent substitute, it isalso fragile and expensive [41,42]. Like Cell Spray CAE, subconfluent cells on a carrier make epithelialsubstitutes, such as Myskin (CellTran) [68].
Hyalograft 3D is another autologous dermal substitute. In this product, autologous culturedfibroblasts are seeded onto a 3D hyaluronic acid derived scaffold [79]. Hyalomatrix® is a bilayerhyaluronan base scaffold with autologous fibroblasts and an outer silicone membrane (Figure 3c).The silicone membrane acts as a temporary epidermal barrier and hyaluronan is delivered to thewound bed [84]. Laserskin is another autologous epidermal substitute [74]. Another similar substituteis TissueTech autograft system, which has been used in successful treatment of diabetic foot ulcers(Figure 3f) [80]. It combines two tissue-engineered biomaterials, a dermal replacement constructHyalograft 3D and an epidermal substitute Laser skin [80]. In this system, autologous keratinocytesand fibroblasts are grown on micro perforated hyaluronic acid membranes. Up to 70.3% of woundclosure with an area greater than 5 cm2 in 85% of cases was accomplished in many full-thicknessulcers using TissueTech autograft system [80]. The rate of recurrence was also low with this TissueTechAutograft System. Although this system may allow for absolute wound closure, it is not a “rue”bilayered skin substitute where both dermal and epidermal layers are present, as it entails grafting oftwo products and may be difficult to use in a clinical setting [80].
Other skin substitutes are based on fibroblasts seeded onto a synthetic polymer membrane [89],such as polylactic-glycolic acid (PLGA), polycaprolactone (PCL), a combination of PLGA/PCL,and mixtures made of hyaluronic acid (HA). Polypyrrole (PPy) can be used as a cultured dermalsubstitute [83]. PPy and HA, in particular, are reported to promote skin regeneration and cellgrowth. Polypyrrole (PPy) has good in vitro and in vivo biocompatibility and can be fabricatedwith a large surface area, with different porosities. However, PPy is very difficult to further processonce synthesized, as its molecular structure makes it non-thermoplastic, mechanically rigid, brittleand insoluble after synthesis [113–115].
An allogenic living epidermal substitute such as Stratagraft is a full thickness skin substituteconsisting of human dermal fibroblasts as a dermal component and neonatal keratinocytes as afully-stratified epidermis [79,94–96]. It serves as a bridge before autografting in burn patients andother severe skin wounds. Stratagraft is well-tolerated and is not acutely immunogenic in patientswith traumatic wounds [87].
Alternative skin substitute Permaderm™ contains both epidermal and dermal componentscomposed of autologous fibroblasts and keratinocytes cultured on a collagen substrate. It has theadvantage of being a one-step procedure with permanent replacement of dermal and epidermal layers.However, no clinical trials have been reported yet [46,116–120]. Another full thickness skin substitutethat is used in chronic therapy-resistant leg/foot ulcers is Tiscover™. Similarly, DenovoDerm™ andDenovoSkin™ are also full-thickness dermal skin substitutes that are currently undergoing trials.Denovoskin has a near normal skin architecture but has long culture times with no clinical series yetreported [7,51]. However, each of these products has its own limitations, and there is no perfect orideal skin substitute yet [78].

Int. J. Mol. Sci. 2017, 18, 789 13 of 19
8. Limitations of Commercially Available Skin Substitutes
There are several limitations to the commercially available skin substitutes, like reducedvascularization, poor mechanical integrity, failure to integrate, scarring, and immune rejection [51].Due to the inability to revascularize, cells in the substitute die and slough away from the host tissue.Few commercially available skin substitutes allow limited vascularization. Moreover, the developmentof engineered skin is a time consuming process involving 2–3 weeks of cell culture before it is readyfor grafting. Technical advances in cell and tissue culture protocols are required to overcome cellgrowth issues of skin substitutes. Currently, available skin substitutes mainly consist of fibroblasts andkeratinocytes and therefore lack the ability to make differentiated structures, like hair and sweat glands.Therefore, there is a need to include additional cells types, such as endothelial cells in engineeredskin. There is also a need to reduce the cost of current skin substitutes. The cost to cover 1% bodysurface area with Epicel™ is more than $13,000 [78,121]. In order to meet the massive demand for skinsubstitutes from hospitals for clinical applications, it is necessary to improve large-scale production.
9. Future Perspectives
Tissue engineered skin substitutes hold a promise for future tissue regeneration and woundhealing therapeutics. There is still a need for improvement in vascularization of these substitutesto increase their life span and provide better integration with host tissues. One way of increasingvascularization is by using bioreactors to provide mechanical stimulation necessary to develop matureblood vessels [122]. An important step in developing reliable substitutes will be to standardize theproduction process and reduce manufacturing costs. Moreover, the standardization of storage andpreservation is also important to extend their life spans. Further investigation is also required toassess the possibility of increased risk of future malignancies in such cells. One way to eradicate theseissues will be to mimic more properties of in vivo skin. Although there is an urgent need to improvetissue engineered skin substitutes due to practical and therapeutic limitations, the field has come along way in patient healing and does hold promise in the near future for skin and wound healing.Better and efficient products can be developed by a detailed understanding of the mechanism of thetherapeutic action of bioengineered skin. There are several skin substitutes currently available, but skinsubstitutes constructed from a combination of stem cells and biomaterials remain a promising solutionfor the future.
Acknowledgments: Support for this review is provided by grants from the National Science FoundationNSF-CREST (HRD-1241701), NSF-HBCU-UP (HRD-1135863) and the US Department of Education—The MinorityScience and Engineering Improvement Program (MSEIP) (P120A150008). The authors thank Golden Muse(www.golden-muse.com) for all illustrations in this review.
Author Contributions: Komal Vig, Atul Chaudhari, Shweta Tripathi, Saurabh Dixit and Rajnish Sahu contributedtowards manuscript writing and figures; Shreekumar Pillai, Vida A. Dennis and Shree R. Singh contributedtowards manuscript editing and critical revision.
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Herndon, D.N.; Barrow, R.E.; Rutan, R.L.; Rutan, T.C.; Desai, M.H.; Abston, S. A comparison of conservativeversus early excision. Therapies in severely burned patients. Ann. Surg. 1989, 209, 547–552. [CrossRef][PubMed]
2. Rheinwald, J.G. Human epidermal keratinocyte cell culture and xenograft systems: Applications in thedetection of potential chemical carcinogens and the study of epidermal transformation. Prog. Clin. Biol. Res.1989, 298, 113–125. [PubMed]
3. Alonso, L.; Fuchs, E. Stem cells of the skin epithelium. Proc. Natl. Acad. Sci. USA 2003, 100, 11830–11835.[CrossRef] [PubMed]
4. Clark, R.A.; Ghosh, K.; Tonnesen, M.G. Tissue engineering for cutaneous wounds. J. Investig. Dermatol. 2007,127, 1018–1029. [CrossRef] [PubMed]

Int. J. Mol. Sci. 2017, 18, 789 14 of 19
5. De Mel, A.; Seifalian, A.M.; Birchall, M.A. Orchestrating cell/material interactions for tissue engineering ofsurgical implants. Macromol. Biosci. 2012, 12, 1010–1021. [CrossRef] [PubMed]
6. Harvey, C. Wound healing. Orthop. Nurs. 2005, 24, 143–157. [CrossRef] [PubMed]7. Boyce, S.T.; Warden, G.D. Principles and practices for treatment of cutaneous wounds with cultured skin
substitutes. Am. J. Surg. 2002, 183, 445–456. [CrossRef]8. Phillips, T.J. Current approaches to venous ulcers and compression. Dermatol. Surg. 2001, 27, 611–621.
[PubMed]9. Braddock, M.; Campbell, C.J.; Zuder, D. Current therapies for wound healing: Electrical stimulation,
biological therapeutics, and the potential for gene therapy. Int. J. Dermatol. 1999, 38, 808–817. [CrossRef][PubMed]
10. Wu, Y.; Chen, L.; Scott, P.G.; Tredget, E.E. Mesenchymal stem cells enhance wound healing throughdifferentiation and angiogenesis. Stem Cells 2007, 25, 2648–2659. [CrossRef] [PubMed]
11. Atiyeh, B.S.; Ioannovich, J.; Al-Amm, C.A.; El-Musa, K.A. Management of acute and chronic open wounds:The importance of moist environment in optimal wound healing. Curr. Pharm. Biotechnol. 2002, 3, 179–195.[CrossRef] [PubMed]
12. Cole-King, A.; Harding, K.G. Psychological factors and delayed healing in chronic wounds. Psychosom. Med.2001, 63, 216–220. [CrossRef] [PubMed]
13. Walburn, J.; Vedhara, K.; Hankins, M.; Rixon, L.; Weinman, J. Psychological stress and wound healing inhumans: A systematic review and meta-analysis. J. Psychosom. Res. 2009, 67, 253–271. [CrossRef] [PubMed]
14. Rhett, J.M.; Ghatnekar, G.S.; Palatinus, J.A.; O’Quinn, M.; Yost, M.J.; Gourdie, R.G. Novel therapies forscar reduction and regenerative healing of skin wounds. Trends Biotechnol. 2008, 26, 173–180. [CrossRef][PubMed]
15. Janeway, C.A., Jr.; Walport, M.; Travers, P.; Shlomchik, M.J. Immunobiology: The Immune System in Health andDisease, 5th ed.; Garland Science: New York, NY, USA, 2001.
16. Davis, J.S. Address of the president: The story of plastic surgery. Ann. Surg. 1941, 113, 641–656. [CrossRef][PubMed]
17. Akan, M.; Yildirim, S.; Misirlioglu, A.; Ulusoy, G.; Akoz, T.; Avci, G. An alternative method to minimize painin the split-thickness skin graft donor site. Plast. Reconstr. Surg. 2003, 111, 2243–2249. [CrossRef] [PubMed]
18. Bello, Y.M.; Falabella, A.F.; Eaglstein, W.H. Tissue-engineered skin. Current status in wound healing. Am. J.Clin. Dermatol. 2001, 2, 305–313. [CrossRef] [PubMed]
19. Halim, A.S.; Khoo, T.L.; Mohd Yussof, S.J. Biologic and synthetic skin substitutes: An overview. Indian J.Plast. Surg. 2010, 43, 23–28. [CrossRef] [PubMed]
20. Cardinal, M.; Eisenbud, D.E.; Armstrong, D.G.; Zelen, C.; Driver, V.; Attinger, C.; Phillips, T.; Harding, K.Serial surgical debridement: A retrospective study on clinical outcomes in chronic lower extremity wounds.Wound Repair Regen. 2009, 17, 306–311. [CrossRef] [PubMed]
21. Rockwell, W.B.; Daane, S.; Zakhireh, M.; Carroll, K.L. Human skin allograft used to treat open wounds afterclub foot release. Ann. Plast. Surg. 2003, 51, 593–597. [CrossRef] [PubMed]
22. Nathoo, R.; Howe, N.; Cohen, G. Skin substitutes: An overview of the key players in wound management.J. Clin. Aesthet. Dermatol. 2014, 7, 44–48. [PubMed]
23. Shores, J.T.; Gabriel, A.; Gupta, S. Skin substitutes and alternatives: A review. Adv. Skin Wound Care 2007, 20,493–508. [CrossRef] [PubMed]
24. Bujang-Safawi, E.; Halim, A.S.; Khoo, T.L.; Dorai, A.A. Dried irradiated human amniotic membrane as abiological dressing for facial burns—A 7-year case series. Burns 2010, 36, 876–882. [CrossRef] [PubMed]
25. Eskandarlou, M.; Azimi, M.; Rabiee, S.; Seif Rabiee, M.A. The healing effect of amniotic membrane in burnpatients. World J. Plast. Surg. 2016, 5, 39–44. [PubMed]
26. Fetterolf, D.E.; Snyder, R.J. Scientific and clinical support for the use of dehydrated amniotic membrane inwound management. Wounds Compend. Clin. Res. Pract. 2012, 24, 299–307.
27. Thangapazham, R.L.; Darling, T.N.; Meyerle, J. Alteration of skin properties with autologous dermalfibroblasts. Int. J. Mol. Sci. 2014, 15, 8407–8427. [CrossRef] [PubMed]
28. Li, A.; Pouliot, N.; Redvers, R.; Kaur, P. Extensive tissue-regenerative capacity of neonatal human keratinocytestem cells and their progeny. J. Clin. Investig. 2004, 113, 390–400. [CrossRef] [PubMed]

Int. J. Mol. Sci. 2017, 18, 789 15 of 19
29. Fortunel, N.O.; Vaigot, P.; Cadio, E.; Martin, M.T. Functional investigations of keratinocyte stem cells andprogenitors at a single-cell level using multiparallel clonal microcultures. Methods Mol. Biol. 2010, 585, 13–23.[PubMed]
30. Dong, R.; Liu, X.; Liu, Y.; Deng, Z.; Nie, X.; Wang, X.; Jin, Y. Enrichment of epidermal stem cells by rapidadherence and analysis of the reciprocal interaction of epidermal stem cells with neighboring cells using anorganotypic system. Cell Biol. Int. 2007, 31, 733–740. [CrossRef] [PubMed]
31. King, A.; Balaji, S.; Keswani, S.G.; Crombleholme, T.M. The role of stem cells in wound angiogenesis.Adv. Wound Care 2014, 3, 614–625. [CrossRef] [PubMed]
32. Dabiri, G.; Heiner, D.; Falanga, V. The emerging use of bone marrow-derived mesenchymal stem cells in thetreatment of human chronic wounds. Expert Opin. Emerg. Drugs 2013, 18, 405–419. [CrossRef] [PubMed]
33. Jackson, W.M.; Nesti, L.J.; Tuan, R.S. Concise review: Clinical translation of wound healing therapies basedon mesenchymal stem cells. Stem Cells Transl. Med. 2012, 1, 44–50. [CrossRef] [PubMed]
34. Nayak, S.; Dey, S.; Kundu, S.C. Skin equivalent tissue-engineered construct: Co-culturedfibroblasts/keratinocytes on 3d matrices of sericin hope cocoons. PLoS ONE 2013, 8, e74779. [CrossRef][PubMed]
35. Zuliani, T.; Saiagh, S.; Knol, A.C.; Esbelin, J.; Dreno, B. Fetal fibroblasts and keratinocytes withimmunosuppressive properties for allogeneic cell-based wound therapy. PLoS ONE 2013, 8, e70408.[CrossRef] [PubMed]
36. Dragunova, J.; Kabat, P.; Koller, J. Skin explant cultures as a source of keratinocytes for cultivation.Cell Tissue Bank. 2013, 14, 317–324. [CrossRef] [PubMed]
37. Guerra, L.; Dellambra, E.; Panacchia, L.; Paionni, E. Tissue engineering for damaged surface and liningepithelia: Stem cells, current clinical applications, and available engineered tissues. Tissue Eng. Part B Rev.2009, 15, 91–112. [CrossRef] [PubMed]
38. Boehnke, K.; Mirancea, N.; Pavesio, A.; Fusenig, N.E.; Boukamp, P.; Stark, H.J. Effects of fibroblasts andmicroenvironment on epidermal regeneration and tissue function in long-term skin equivalents. Eur. J.Cell Biol. 2007, 86, 731–746. [CrossRef] [PubMed]
39. Sun, T.; Jackson, S.; Haycock, J.W.; MacNeil, S. Culture of skin cells in 3D rather than 2D improves theirability to survive exposure to cytotoxic agents. J. Biotechnol. 2006, 122, 372–381. [CrossRef] [PubMed]
40. Hill, D.S.; Robinson, N.D.; Caley, M.P.; Chen, M.; O’Toole, E.A.; Armstrong, J.L.; Przyborski, S.; Lovat, P.E.A novel fully humanized 3D skin equivalent to model early melanoma invasion. Mol. Cancer Ther. 2015, 14,2665–2673. [CrossRef] [PubMed]
41. Gallico, G.G.; O’Connor, N.E.; Compton, C.C.; Kehinde, O.; Green, H. Permanent coverage of large burnwounds with autologous cultured human epithelium. New Engl. J. Med. 1984, 311, 448–451. [CrossRef][PubMed]
42. O’Connor, N.E.; Mulliken, J.; Banks-Schlegel, S.; Green, H. Grafting of burns with cultured epitheliumprepared from autologous epidermal cells. Lancet 1981, 317, 75–78. [CrossRef]
43. Rheinwald, J.G.; Green, H. Serial cultivation of strains of human epidermal keratinocytes: The formation ofkeratinizing colonies from single cells. Cell 1975, 6, 331–343. [CrossRef]
44. Rheinwald, J.G.; Green, H. Epidermal growth factor and the multiplication of cultured human epidermalkeratinocytes. Nature 1977, 265, 421–424. [CrossRef] [PubMed]
45. Leigh, I.M.; Watt, F.M. The culture of human epidermal keratinocytes. In Keratinocyte Handbook; CambridgeUniversity Press: Cambridge, UK, 1994; pp. 43–51.
46. Supp, D.M.; Boyce, S.T. Engineered skin substitutes: Practices and potentials. Clin. Dermatol. 2005, 23,403–412. [CrossRef] [PubMed]
47. Kroner, E.; Kaiser, J.S.; Fischer, S.C.; Arzt, E. Bioinspired polymeric surface patterns for medical applications.J. Appl. Biomater. Funct. Mater. 2012, 10, 287–292. [CrossRef] [PubMed]
48. Ho, W.S. Skin substitutes: An overview. Ann. R. Coll. Surg. 2002, 6, 102–108. [CrossRef]49. Horch, R.E.; Kopp, J.; Kneser, U.; Beier, J.; Bach, A.D. Tissue engineering of cultured skin substitutes. J. Cell.
Mol. Med. 2005, 9, 592–608. [CrossRef] [PubMed]50. Leigh, I.M.; Watt, F.M. Keratinocyte Methods; Cambridge University Press: Cambridge, UK, 1994.51. MacNeil, S. Progress and opportunities for tissue-engineered skin. Nature 2007, 445, 874–880. [CrossRef]
[PubMed]

Int. J. Mol. Sci. 2017, 18, 789 16 of 19
52. Metcalfe, A.D.; Ferguson, M.W. Tissue engineering of replacement skin: The crossroads of biomaterials,wound healing, embryonic development, stem cells and regeneration. J. R. Soc. Interface 2007, 4, 413–437.[CrossRef] [PubMed]
53. Boyce, S.T.; Kagan, R.J.; Meyer, N.A.; Yakuboff, K.P.; Warden, G.D. The 1999 clinical research award. Culturedskin substitutes combined with integra artificial skin to replace native skin autograft and allograft for theclosure of excised full-thickness burns. J. Burn Care Rehabil. 1999, 20, 453–461. [CrossRef] [PubMed]
54. Passaretti, D.; Billmire, D.; Kagan, R.; Corcoran, J.; Boyce, S. Autologous cultured skin substitutes conservedonor autograft in elective treatment of congenital giant melanocytic nevus. Plast. Reconstr. Surg. 2004, 114,1523–1528. [CrossRef] [PubMed]
55. Shevchenko, R.V.; James, S.L.; James, S.E. A review of tissue-engineered skin bioconstructs available for skinreconstruction. J. R. Soc. Interface 2010, 7, 229–258. [CrossRef] [PubMed]
56. Atiyeh, B.S.; Costagliola, M. Cultured epithelial autograft (CEA) in burn treatment: Three decades later.Burns 2007, 33, 405–413. [CrossRef] [PubMed]
57. Patel, M.; Fisher, J.P. Biomaterial scaffolds in pediatric tissue engineering. Pediatr. Res. 2008, 63, 497–501.[CrossRef] [PubMed]
58. Shakespeare, P.; Shakespeare, V. Survey: Use of skin substitute materials in UK burn treatment centres. Burns2002, 28, 295–297. [CrossRef]
59. Shakespeare, P.G. The role of skin substitutes in the treatment of burn injuries. Clin. Dermatol. 2005, 23,413–418. [CrossRef] [PubMed]
60. Melkun, E.T.; Few, J.W. The use of biosynthetic skin substitute (Biobrane) for axillary reconstruction aftersurgical excision for hidradenitis suppurativa. Plast. Reconstr. Surg. 2005, 115, 1385–1388. [CrossRef][PubMed]
61. Curran, M.P.; Plosker, G.L. Bilayered bioengineered skin substitute (Apligraf): A review of its use in thetreatment of venous leg ulcers and diabetic foot ulcers. BioDrugs 2002, 16, 439–455. [CrossRef] [PubMed]
62. Price, R.D.; Myers, S.; Leigh, I.M.; Navsaria, H.A. The role of hyaluronic acid in wound healing: Assessmentof clinical evidence. Am. J. Clin. Dermatol. 2005, 6, 393–402. [CrossRef] [PubMed]
63. Hellman, K.B. Engineered tissues: The regulatory path from concept to market. Adv. Exp. Med. Biol. 2006,585, 363–376. [PubMed]
64. Alrubaiy, L.; Al-Rubaiy, K.K. Skin substitutes: A brief review of types and clinical applications. Oman Méd. J.2009, 24, 4–6. [CrossRef] [PubMed]
65. Gordley, K.; Cole, P.; Hicks, J.; Hollier, L. A comparative, long term assessment of soft tissue substitutes:Alloderm, enduragen, and dermamatrix. JPRAS 2009, 62, 849–850. [CrossRef] [PubMed]
66. Hodde, J.P.; Ernst, D.M.; Hiles, M.C. An investigation of the long-term bioactivity of endogenous growthfactor in oasis wound matrix. J. Wound Care 2005, 14, 23–25. [CrossRef] [PubMed]
67. Tausche, A.K.; Skaria, M.; Bohlen, L.; Liebold, K.; Hafner, J.; Friedlein, H.; Meurer, M.; Goedkoop, R.J.;Wollina, U.; Salomon, D.; et al. An autologous epidermal equivalent tissue-engineered from follicular outerroot sheath keratinocytes is as effective as split-thickness skin autograft in recalcitrant vascular leg ulcers.Wound Repair Regen. 2003, 11, 248–252. [CrossRef] [PubMed]
68. Haddow, D.B.; Steele, D.A.; Short, R.D.; Dawson, R.A.; Macneil, S. Plasma-polymerized surfaces for cultureof human keratinocytes and transfer of cells to an in vitro wound-bed model. J. Biomed. Mater. Res. Part A2003, 64, 80–87. [CrossRef] [PubMed]
69. Hüsing, B.; Bührlen, B.; Gaisser, S. Human tissue engineered products: Today’s markets and future prospects.Fraunhofer Inst. Syst. Innov. Res. 2003, 1, 54.
70. Goedkoop, R.; Juliet, R.; You, P.H.; Daroczy, J.; de Roos, K.P.; Lijnen, R.; Rolland, E.; Hunziker, T.Wound stimulation by growth-arrested human keratinocytes and fibroblasts: Hp802-247, a new-generationallogeneic tissue engineering product. Dermatology 2010, 220, 114–120. [CrossRef] [PubMed]
71. Kirsner, R.S.; Marston, W.A.; Snyder, R.J.; Lee, T.D.; Cargill, D.I.; Slade, H.B. Spray-applied cell therapy withhuman allogeneic fibroblasts and keratinocytes for the treatment of chronic venous leg ulcers: A phase 2,multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2012, 380, 977–985. [CrossRef]
72. Magnusson, M.; Papini, R.P.; Rea, S.M.; Reed, C.C.; Wood, F.M. Cultured autologous keratinocytes insuspension accelerate epithelial maturation in an in vivo wound model as measured by surface electricalcapacitance. Plast. Reconstr. Surg. 2007, 119, 495–499. [CrossRef] [PubMed]

Int. J. Mol. Sci. 2017, 18, 789 17 of 19
73. Carsin, H.; Ainaud, P.; Le Bever, H.; Rives, J.; Lakhel, A.; Stephanazzi, J.; Lambert, F.; Perrot, J. Culturedepithelial autografts in extensive burn coverage of severely traumatized patients: A five year single-centerexperience with 30 patients. Burns 2000, 26, 379–387. [CrossRef]
74. Caravaggi, C.; de Giglio, R.; Pritelli, C.; Sommaria, M.; Dalla Noce, S.; Faglia, E.; Mantero, M.; Clerici, G.;Fratino, P.; Dalla Paola, L.; et al. Hyaff 11-based autologous dermal and epidermal grafts in the treatmentof noninfected diabetic plantar and dorsal foot ulcers: A prospective, multicenter, controlled, randomizedclinical trial. Diabetes Care 2003, 26, 2853–2859. [CrossRef] [PubMed]
75. Dietz, J.; Lundgren, P.; Veeramani, A.; O’Rourke, C.; Bernard, S.; Djohan, R.; Larson, J.; Isakov, R.; Yetman, R.Autologous inferior dermal sling (Autoderm) with concomitant skin-envelope reduction mastectomy:An excellent surgical choice for women with macromastia and clinically significant ptosis. Ann. Surg. Oncol.2012, 19, 3282–3288. [CrossRef] [PubMed]
76. Harding, K.G.; Krieg, T.; Eming, S.A.; Flour, M.L.; Jawien, A.; Cencora, A.; Kaszuba, A.; Noszcyk, W.;Willems, P.; de Deene, A.; et al. Efficacy and safety of the freeze-dried cultured human keratinocyte lysate,lyphoderm 0.9%, in the treatment of hard-to-heal venous leg ulcers. Wound Repair Regen. 2005, 13, 138–147.[CrossRef] [PubMed]
77. Paquet, P.; Quatresooz, P.; Braham, C.; Pierard, G.E. Tapping into the influence of keratinocyte allograftsand biocenosis on healing of chronic leg ulcers: Split-ulcer controlled pilot study. Dermatol. Surg. 2005, 31,431–435. [CrossRef] [PubMed]
78. Varkey, M.; Ding, J.; Tredget, E.E. Advances in skin substitutes-potential of tissue engineered skin forfacilitating anti-fibrotic healing. J. Funct. Biomater. 2015, 6, 547–563. [CrossRef] [PubMed]
79. Limova, M. Active wound coverings: Bioengineered skin and dermal substitutes. Surg. Clin. N. Am. 2010,90, 1237–1255. [CrossRef] [PubMed]
80. Uccioli, L. A clinical investigation on the characteristics and outcomes of treating chronic lower extremitywounds using the tissuetech autograft system. Int. J. Low. Extremity Wounds 2003, 2, 140–151. [CrossRef][PubMed]
81. Noordenbos, J.; Dore, C.; Hansbrough, J.F. Safety and efficacy of transcyte for the treatment ofpartial-thickness burns. J. Burn Care Rehabil. 1999, 20, 275–281. [CrossRef] [PubMed]
82. Groeber, F.; Holeiter, M.; Hampel, M.; Hinderer, S.; Schenke-Layland, K. Skin tissue engineering—In vivoand in vitro applications. Adv. Drug Deliv. Rev. 2011, 63, 352–366. [CrossRef] [PubMed]
83. Ng, K.W.; Hutmacher, D.W. Reduced contraction of skin equivalent engineered using cell sheets cultured in3D matrices. Biomaterials 2006, 27, 4591–4598. [CrossRef] [PubMed]
84. Myers, S.R.; Partha, V.N.; Soranzo, C.; Price, R.D.; Navsaria, H.A. Hyalomatrix: A temporary epidermalbarrier, hyaluronan delivery, and neodermis induction system for keratinocyte stem cell therapy. Tissue Eng.2007, 13, 2733–2741. [CrossRef] [PubMed]
85. Cullen, B. The role of oxidized regenerated cellulose/collagen in chronic wound repair. Part 2.Ostomy Wound Manag. 2002, 48, 8–13.
86. Stark, H.J.; Boehnke, K.; Mirancea, N.; Willhauck, M.J.; Pavesio, A.; Fusenig, N.E.; Boukamp, P. Epidermalhomeostasis in long-term scaffold-enforced skin equivalents. J. Investig. Dermatol. Symp. Proc. 2006, 11,93–105. [CrossRef] [PubMed]
87. Ackermann, K.; Borgia, S.L.; Korting, H.C.; Mewes, K.R.; Schafer-Korting, M. The phenion full-thickness skinmodel for percutaneous absorption testing. Skin Pharmacol. Physiol. 2010, 23, 105–112. [CrossRef] [PubMed]
88. Still, J.; Glat, P.; Silverstein, P.; Griswold, J.; Mozingo, D. The use of a collagen sponge/living cell compositematerial to treat donor sites in burn patients. Burns 2003, 29, 837–841. [CrossRef]
89. Lindberg, K.; Badylak, S.F. Porcine small intestinal submucosa (SIS): A bioscaffold supporting in vitroprimary human epidermal cell differentiation and synthesis of basement membrane proteins. Burns 2001, 27,254–266. [CrossRef]
90. Rockwood, D.N.; Woodhouse, K.A.; Fromstein, J.D.; Chase, D.B.; Rabolt, J.F. Characterization ofbiodegradable polyurethane microfibers for tissue engineering. J. Biomater. Sci. Polym. 2007, 18, 743–758.[CrossRef] [PubMed]
91. Van Dorp, A.G.; Verhoeven, M.C.; Koerten, H.K.; van Blitterswijk, C.A.; Ponec, M. Bilayered biodegradablepoly (ethylene glycol)/poly (butylene terephthalate) copolymer (polyactive) as substrate for humanfibroblasts and keratinocytes. J. Biomed. Mater. Res. 1999, 47, 292–300. [CrossRef]

Int. J. Mol. Sci. 2017, 18, 789 18 of 19
92. Dodson, B.P.; Levine, A.D. Challenges in the translation and commercialization of cell therapies.BMC Biotechnol. 2015, 15, 70. [CrossRef] [PubMed]
93. Ferreira, M.C.; Paggiaro, A.O.; Isaac, C.; Teixeira Neto, N.; dos Santos, G.B. Skin substitutes: Current conceptsand a new classification system. Rev. Bras. Cir. Plást. 2011, 26, 696–702. [CrossRef]
94. Centanni, J.M.; Straseski, J.A.; Wicks, A.; Hank, J.A.; Rasmussen, C.A.; Lokuta, M.A.; Schurr, M.J.; Foster, K.N.;Faucher, L.D.; Caruso, D.M.; et al. Stratagraft skin substitute is well-tolerated and is not acutely immunogenicin patients with traumatic wounds: Results from a prospective, randomized, controlled dose escalation trial.Ann. Surg. 2011, 253, 672–683. [CrossRef] [PubMed]
95. Schurr, M.J.; Foster, K.N.; Centanni, J.M.; Comer, A.R.; Wicks, A.; Gibson, A.L.; Thomas-Virnig, C.L.;Schlosser, S.J.; Faucher, L.D.; Lokuta, M.A.; et al. Phase I/II clinical evaluation of stratagraft: A consistent,pathogen-free human skin substitute. J. Trauma 2009, 66, 866–873. [CrossRef] [PubMed]
96. Supp, D.M.; Karpinski, A.C.; Boyce, S.T. Expression of human β-defensins HBD-1, HBD-2, and HBD-3 incultured keratinocytes and skin substitutes. Burns 2004, 30, 643–648. [CrossRef] [PubMed]
97. Cheah, A.K.W.; Chong, S.J.; Tan, B.K. Early experience with biobrane™ in singapore in the management ofpartial thickness burns. Proc. Singap. Healthc. 2014, 23, 196–200. [CrossRef]
98. Chua, A.W.; Khoo, Y.C.; Tan, B.K.; Tan, K.C.; Foo, C.L.; Chong, S.J. Skin tissue engineering advances in severeburns: Review and therapeutic applications. Burns Trauma 2016, 4, 3. [CrossRef] [PubMed]
99. Greenwood, J.E.; Clausen, J.; Kavanagh, S. Experience with biobrane: Uses and caveats for success. Eplasty2009, 9, e25. [PubMed]
100. Tan, H.; Wasiak, J.; Paul, E.; Cleland, H. Effective use of biobrane as a temporary wound dressing prior todefinitive split-skin graft in the treatment of severe burn: A retrospective analysis. Burns 2015, 41, 969–976.[CrossRef] [PubMed]
101. Woodroof, E.A. The search for an ideal temporary skin substitute: Awbat. Eplasty 2009, 9, e10. [PubMed]102. Conconi, M.T.; de Coppi, P.; di Liddo, R.; Vigolo, S.; Zanon, G.F.; Parnigotto, P.P.; Nussdorfer, G.G. Tracheal
matrices, obtained by a detergent-enzymatic method, support in vitro the adhesion of chondrocytes andtracheal epithelial cells. Transplant Int. 2005, 18, 727–734. [CrossRef] [PubMed]
103. Shahrokhi, S.; Arno, A.; Jeschke, M.G. The use of dermal substitutes in burn surgery: Acute phase.Wound Repair Regen. 2014, 22, 14–22. [CrossRef] [PubMed]
104. Dickinson, L.E.; Gerecht, S. Engineered biopolymeric scaffolds for chronic wound healing. Front. Physiol.2016, 7, 341. [CrossRef] [PubMed]
105. Lev-Tov, H.; Li, C.S.; Dahle, S.; Isseroff, R.R. Cellular versus acellular matrix devices in treatment ofdiabetic foot ulcers: Study protocol for a comparative efficacy randomized controlled trial. Trials 2013, 14, 8.[CrossRef] [PubMed]
106. Raguse, J.D.; Gath, H.J. The buccal fad pad lined with a metabolic active dermal replacement (dermagraft)for treatment of defects of the buccal plane. Br. J. Plast. Surg. 2004, 57, 764–768. [CrossRef] [PubMed]
107. Armstrong, D.G.; Lepow, B.D.; Downey, M.; Yurgelon, J.; Klassen, L. Bioengineered tissues in wound healinga progress report. Expert Rev. Dermatol. 2011, 6, 255–262.
108. Kim, P.J.; Heilala, M.; Steinberg, J.S.; Weinraub, G.M. Bioengineered alternative tissues and hyperbaricoxygen in lower extremity wound healing. Clin. Podiatr. Med. Surg. 2007, 24, 529–546. [CrossRef] [PubMed]
109. Ryssel, H.; Gazyakan, E.; Germann, G.; Ohlbauer, M. The use of matriderm in early excision and simultaneousautologous skin grafting in burns—A pilot study. Burns 2008, 34, 93–97. [CrossRef] [PubMed]
110. Kolokythas, P.; Aust, M.C.; Vogt, P.M.; Paulsen, F. Dermal subsitute with the collagen-elastin matrixmatriderm in burn injuries: A comprehensive review. Handchir. Mikrochir. Plast. Chir. 2008, 40, 367–371.[CrossRef] [PubMed]
111. Van Zuijlen, P.P.; van Trier, A.J.; Vloemans, J.F.; Groenevelt, F.; Kreis, R.W.; Middelkoop, E. Graft survivaland effectiveness of dermal substitution in burns and reconstructive surgery in a one-stage grafting model.Plast. Reconstr. Surg. 2000, 106, 615–623. [CrossRef] [PubMed]
112. Greenberg, J.E.; Falabella, A.F.; Bello, Y.M.; Schachner, L.A. Tissue-engineered skin in the healing of woundstumps from limb amputations secondary to purpura fulminans. Pediatr. Dermatol. 2003, 20, 169–172.[CrossRef] [PubMed]
113. Akkouch, A.; Shi, G.; Zhang, Z.; Rouabhia, M. Bioactivating electrically conducting polypyrrole withfibronectin and bovine serum albumin. J. Biomed. Mater. Res. Part A 2010, 92, 221–231. [CrossRef] [PubMed]

Int. J. Mol. Sci. 2017, 18, 789 19 of 19
114. Cui, X.; Hetke, J.F.; Wiler, J.A.; Anderson, D.J.; Martin, D.C. Electrochemical deposition and characterizationof conducting polymer polypyrrole/PSS on multichannel neural probes. Sens. Actuators A Phys. 2001, 93,8–18. [CrossRef]
115. Li, Y.; Neoh, K.G.; Kang, E.T. Plasma protein adsorption and thrombus formation on surface functionalizedpolypyrrole with and without electrical stimulation. J. Colloid Interface Sci. 2004, 275, 488–495. [CrossRef][PubMed]
116. Austin, R.E.; Merchant, N.; Shahrokhi, S.; Jeschke, M.G. A comparison of biobrane and cadaveric allograft fortemporizing the acute burn wound: Cost and procedural time. Burns 2015, 41, 749–753. [CrossRef] [PubMed]
117. Cooper, M.L.; Andree, C.; Hansbrough, J.F.; Zapata-Sirvent, R.L.; Spielvogel, R.L. Direct comparison of acultured composite skin substitute containing human keratinocytes and fibroblasts to an epidermal sheetgraft containing human keratinocytes on athymic mice. J. Investig. Dermatol. 1993, 101, 811–819. [CrossRef][PubMed]
118. Farroha, A.; Frew, Q.; El-Muttardi, N.; Philp, B.; Dziewulski, P. The use of biobrane® to dress split-thicknessskin graft in paediatric burns. Ann. Burns Fire Disasters 2013, 26, 94–97. [PubMed]
119. Pandya, A.N.; Woodward, B.; Parkhouse, N. The use of cultured autologous keratinocytes with integra inthe resurfacing of acute burns. Plast. Reconstr. Sur. 1998, 102, 825–828. [CrossRef]
120. Pham, C.; Greenwood, J.; Cleland, H.; Woodruff, P.; Maddern, G. Bioengineered skin substitutes for themanagement of burns: A systematic review. Burns 2007, 33, 946–957. [CrossRef] [PubMed]
121. Rue, L.W., 3rd; Cioffi, W.G.; McManus, W.F.; Pruitt, B.A. Wound closure and outcome in extensively burnedpatients treated with cultured autologous keratinocytes. J. Trauma 1993, 34, 662–667. [CrossRef] [PubMed]
122. Lovett, M.; Lee, K.; Edwards, A.; Kaplan, D.L. Vascularization strategies for tissue engineering. Tissue Eng.Part B Rev. 2009, 15, 353–370. [CrossRef] [PubMed]
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open accessarticle distributed under the terms and conditions of the Creative Commons Attribution(CC BY) license (http://creativecommons.org/licenses/by/4.0/).