Embed Size (px)
Citation preview

Advances in the Treatment ofChronic Hepatitis C
Gregory T Everson, MDProfessor of MedicineDirector of Hepatology
University of Colorado Denver

Disclosures
Advisory Boards: Roche/Genentech, Merck, Vertex, BMS, GlobeImmune, Abbott, Eisai, Novartis, Pfizer, Gilead, Biotest, Tibotec/Janssen
Consulting: Roche-Genentech, Novartis, BMS, Eisai,Kadmon, Vertex, Abbott, Biotest, Tibotec/Janssen
DSMB: CentocorStock/Ownership: Source, HepQuant LLCManagement: HepQuant LLCResearch Grants: Roche/Genentech, Schering-Plough/Merck,
Vertex, GlobeImmune, Gilead, Novartis, BMS, Pfizer, Source, Eisai, GSK, Pharmassett,Ortho Biotech, Tibotec/Janssen, Amgen, Medtronic, Abbott

Primer on HCV

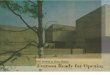
Worldwide Prevalence of HCV
WHO, Wkly Epidemiol Rec, 2000

Genotype and Viral Load in US
50%
24%
22%4%
Geno 1 HVL> 800,000 IU/ml
Geno 2 & 3
Geno 1 LVL
Approximately 2/3 cases of GT1 infection in the USare due to the GT1a subtype.

Natural History of HCV Infection
Mild Moderate Severe
15%-45% 55%-85%
Acute HCV InfectionAcute HCV Infection
RecoveryRecovery Chronic HCV InfectionChronic HCV Infection
Chronic Hepatitis CChronic Hepatitis C
CirrhosisCirrhosis
Hepatocellular CarcinomaHepatocellular CarcinomaEnd-Stage Liver DiseaseEnd-Stage Liver Disease
Liver TransplantationLiver Transplantation DeathDeath
There are an estimated 3 to 5 million cases of chronic hepatitis C in the US.

Hepatitis C Testing for Anyone Born During1945-1965: New CDC Recommendations
If you were born during 1945-1965 (baby boomer), talk to
your doctor about getting tested for Hepatitis C. The only
way to know if you have Hepatitis C is to get tested.
Early detection can save lives.
Reasons for this recommendation:1. Baby boomers – represent 75% of cases in US). 2. This one-time testing may prevent more than 120,000 deaths.3. Most cases are undiagnosed - testing would find 800,000 new cases.4. There have been recent advances in treatment.
Source: CDC. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945–1965. MMWR 2012;61(No. RR–4).

Recommendations for the Identification of Chronic Hepatitis C Virus Infection Among Persons Born
during 1945–1965*
• Adults born during 1945–1965 should receive one-time testing for HCV without prior ascertainment of HCV risk.
• All persons with identified HCV infection should receive a brief alcohol screening and intervention as clinically indicated, followed by referral to appropriate care and treatment services for HCV infection and related conditions.
Source: CDC. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945–1965. MMWR 2012;61(No. RR–4).

Case

A baby boomer is screened for HCV and HCV-Ab is positive. You order a polymerase-chain-reaction-based test for HCV RNA quantification. What is the likelihood
that the HCV RNA will be positive?
1. 0%
2. ~ 25%
3. ~ 50%
4. ~ 75%
5. 100%

A baby boomer is screened for HCV and HCV-Ab is positive. You order a polymerase-chain-reaction-based test for HCV RNA quantification. What is the likelihood
that the HCV RNA will be positive?
1. 0%
2. ~ 25%
3. ~ 50%
4. ~ 75%
5. 100%

The HCV RNA is positive. Standard laboratory tests are normal except for ALT 85 IU/mL. Further evaluation reveals HCV genotype 1a, advanced fibrosis (F3), and
IL28B genotype CT. Given these factors, what would you advise for treatment?
1. None
2. Silymarin (milk thistle)
3. Peginterferon alone
4. Peginterferon + Ribavirin
5. Peginterferon + Ribavirin + DAA

The HCV RNA is positive. Standard laboratory tests are normal except for ALT 85 IU/mL. Further evaluation reveals HCV genotype 1a, advanced fibrosis (F3), and
IL28B genotype CT. Given these factors, what would you advise for treatment?
1. None
2. Silymarin (milk thistle)
3. Peginterferon alone
4. Peginterferon + Ribavirin
5. Peginterferon + Ribavirin + DAA

Treatment

The Goal of Treatment is SVRSustained Virologic Response
Undetectable HCV RNA - 3 months (SVR12) or6 months (SVR24) after Treatment
The Primary Objective ofTherapy for Chronic Hepatitis C

SVR Equates with CURE
Swain MG, et al. Gastroenterology 2010;139:1593-1601.

Established Benefits of SVR
1. Probably “Cured” of HCV infection – chance for late relapse <1%.
2. Halts progression of liver disease.
3. Reduces risk for HCC – although patients with bridging fibrosis or cirrhosis may develop HCC after SVR and still need to be screened.
4. HCV-related extrahepatic manifestations disappear or are ameliorated
5. Health-related (HCV) Quality of Life Improves

Past and Current Treatment for HCV GT2 & 3
1629
69 6680
0
20
40
60
80
100
IFN 24 IFN 48 IFN/RBV 24 IFN/RBV 48 PEG/RBV 24
% of Patients Achieving SVR
1991 Year of FDA Approval 2002

Triple TherapyThe Current Standard-of-Care for
HCV Genotype 1
First Generation Protease Inhibitors
TelaprevirBoceprevir
with Peginterferon/Ribavirin

Past and Current Treatment for HCV GT1
27
1628
40
75
0
20
40
60
80
100
IFN 24 IFN 48 IFN/RBV 24 IFN/RBV 48 PEG/RBV 48 TT-TPV
% of Patients Achieving SVR
1991 Year of FDA Approval 2002 2011

Predictors of SVR with TT inTreatment Naïve Patients
Interferon Sensitivity IL28B Polymorphism HCV RNA decline during Lead-In with
PEG/RBV
On-treatment (TT) Response (eRVR)
Stage of Fibrosis

IL28b Polymorphism


Telaprevir (TPV): Treatment-NaïveSVR by IL28B Polymorphism
64
90
25
71
23
73
0
20
40
60
80
100
PR TPV-based
% SVR
CC CT TT CC CT TT
∆ = 18%
∆ = 50%

Boceprevir (BOC): Treatment-NaïveSVR by IL28B Polymorphism
78 82 80
28
6571
27
55 59
0
20
40
60
80
100
PR BOC-RGT BOC-48
% SVR
CC CT TT CC CT TTCC CT TT
∆ = 9 to 27%
∆ = 50%

IL28b Polymorphism inTreatment-Naïve
1. Highly predictive when treatment is peginterferon plus ribavirin (PR)
2. Less predictive when treatment has higher chance of success in CT and TT polymorphisms – less predictive when treatment is triple therapy.

Lead-In
Boceprevir Trial of Treatment-Naïve(SPRINT-2)

Boceprevir (BOC): Treatment-NaïveSVR by Log10 HCV RNA Decline during Lead-In with PR
4
2838
51
81 79
0
20
40
60
80
100
PR BOC-RGT BOC-48
< 1 Log10 Decline ≥ 1 Log10 Decline
% SVR
SPRINT-2 Study. N Engl J Med 2011;364:1195-1206.

Lead-In inTreatment-Naïve
1. Predicts likelihood of SVR with Boceprevir-based triple therapy
2. SVR is still greater than 30% in the patients treated with triple therapy who have < 1 Log10 decline in HCV RNA during Lead-in - < 1 Log10 decline is NOT a Stop Guideline

Extended Rapid Virologic Response(eRVR)

Extended Rapid Virologic ResponseeRVR Identifies the “Super” Responders who can Stop Early
Two components of eRVR HCV RNA <10 IU/mL at Week 4 of Triple Therapy (RAPID) HCV RNA <10 IU/mL subsequently (EXTENDED)
Telaprevir (T12/PR24) HCV RNA <10 IU/mL Weeks 4 through 12 Stop treatment at Week 24 (58% & 65% of patients1) ILLUMINATE, randomized trial of eRVR, 24 vs 48 wks PR
Boceprevir (LI PR4, B24/PR24) HCV RNA <10 IU/mL Weeks 8 through 24 eRVR – Stop treatment at Week 28 (44% of patients2)
1 ADVANCE. N Engl J Med 2011;364:2405-2416. ILLUMINATE. N Engl J Med 2011;365:1014-1024.2 SPRINT-2. N Engl J Med 2011;364:1195-1206.

eRVR and Treatment DurationILLUMINATE study of Telaprevir – 65% Achieved eRVR
92 88
0
20
40
60
80
100
24 Weeks 48 Weeks
% SVR
ILLUMINATE Study. N Engl J Med 2011;365:1014-1024.

Stage of Fibrosis

Impact of Stage of FibrosisTelaprevir and Boceprevir: Treatment-Naive
0
20
40
60
80
100
ADVANCE T12 ADVANCE T8 ILLUMINATEeRVR24
ILLUMINATEeRVR48
SPRINT-2 RGT SPRINT-2 48
F0-F2 F3-F4
SVR (%)
Jacobson IM, et al. ADVANCE trial. N Eng J Med 2011;364:2405-2416.Sherman KE, et al. ILLUMINATE trial. N Engl J Med 2011;365:1014-1024.
Poordad F, et al. SPRINT-2 trial. N Engl J Med 2011; 364:1195-1206.
* Biggest Impact of reducing duration of TPV in ADVANCE, or PR in ILLUMINATE, was in F4 patients.
*
*

Case

The Patient Elects Treatment with Telaprevir-based Triple Therapy. HCV RNA is undetectable from Weeks 1 through 8.
Base Wk 1 Wk 4 Wk 8 Post-Rx Wk4
Post-Rx Wk12
Post-Rx Wk16
Post-Rx Yr2
0
500000
1000000
1500000
2000000
2500000
3000000
Diverticulitis
GT1a, F3, IL28b CTNo viral variants at baseline
HCV RNA negative
HCV RNA (IU/mL)

The patient is admitted to the hospital with fever, LLQ abdominal pain, and leucocytosis. CT confirms sigmoid
diverticulitis and blood cultures were positive for E. coli. Best management includes antibiotic therapy and:
1. Continuation of TPV, PEG, and RBV
2. Continuation of PEG and RBV only
3. Continuation of PEG only
4. Discontinuation of TPV, PEG, and RBV

The patient is admitted to the hospital with fever, LLQ abdominal pain, and leucocytosis. CT confirms sigmoid
diverticulitis and blood cultures were positive for E. coli. Best management includes antibiotic therapy and:
1. Continuation of TPV, PEG, and RBV
2. Continuation of PEG and RBV only
3. Continuation of PEG only
4. Discontinuation of TPV, PEG, and RBV

Pitfalls of Current DAA Rx
• Single DAA – low barrier to resistance• Only indicated for HCV GT1• Complex treatment algorithms• High pill burden• Rx duration of 24 to 48 weeks• Requires PEG/RBV – SEs, AEs, SAEs• Unique SEs, AEs, SAEs• Drug-Drug Interactions

Viral Resistance

Case

TPV, PEG, and RBV are discontinued and HCV RNA is monitored.
Base Wk 1 Wk 4 Wk 8 Post-Rx Wk4
Post-Rx Wk12
Post-Rx Wk16
Post-Rx Yr2
0
500000
1000000
1500000
2000000
2500000
3000000
V36M -T54A -R155K -A156V -
Stopped allMeds due toDiverticulitis
HCV RNAPositive30 IU/mL
HCV RNA negative

After confirming relapse by repeat testing of HCV RNA, a blood sample is analyzed for variants of HCV resistant to TPV.
Base Wk 1 Wk 4 Wk 8 Post-Rx Wk4
Post-Rx Wk12
Post-Rx Wk16
Post-Rx Yr2
0
500000
1000000
1500000
2000000
2500000
3000000
V36M - -T54A - -R155K - +A156V - -
Stopped allMeds due toDiverticulitis
R155KDetected
HCV RNAPositive
HCV RNA negative

Complex Treatment Algorithms

Telaprevir: Treatment-Naïve Patients
TripleTherapy
withTPV+P+R
For12 weeks
Additional12 weeks of
P+R*
Additional36 weeks of
P+R
eRVRHCV RNA negative
At Weeks 4 & 12
NO eRVRSlow Responder**
HCV RNA is quantified at weeks 4, 8, 12 while the
patient is taking TPV – to evaluate for viral response
and resistance.
TPV is stopped if there is evidence of rebound in HCV
RNA.Treatment is discontinued if HCV
RNA is >1000 IU/mL at week 4 or 12 or detectable at week 24
* FDA recommends extending P+R for 36 weeks in patients with cirrhosis.** Slow responder is RNA positive at week 4 but RNA negative prior to or at week 24.

Boceprevir: Treatment-Naïve Patients
Lead-InWith
4 weeksP+R
TripleTherapy
withBOC+P+R
For additional24 weeks*
Noadditional
Treatment*
(28 weeks total)
Additional8 weeks of
BOC+P+R and 12 weeks P+RTreatment*
(48 weeks total)
eRVR’8 - 24 wk RNA neg
NO eRVR’Slow Responder
HCV RNA at Weeks 4, 8, 12, 24 while the patient is taking BOC – to evaluate for viral response and resistance.
All treatment is discontinued if either HCV RNA >100 IU/mL at wk 12
or HCV RNA detectable at wk 24
The drop in HCV RNA predicts likelihood of
responding to subsequent triple therapy with BOC.
Patients with <1log10 decrease (Poor response)
have SVR ~30%.
* Cirrhotic patients and Poor Responders are treated for 44 weeks BOC+P+R, regardless of eRVR’.** Slow responders are RNA positive at week 8 but RNA negative prior to or at week 24.

Unique Side Effects

Telaprevir and Rash
Can be nasty (DRESS, S-J syndrome)!
Occurs in over 50% of patients, mild in most cases (hydroxyzine, topicals)
Telaprevir discontinued in 5 - 10% due to rash. Systemic steroids may be required. All treatment stopped in 1-2% due to rash.

Ribavirin Rash

Telaprevir – Mild to Moderate Rash

Telaprevir – Moderate to Severe Rash

December 19, 2012. The U.S. Food and Drug Administration (FDA) received reports of serious skin reactions, some fatal, in patients taking the hepatitis C drug Incivek (telaprevir) in combination with the drugs peginterferon alfa and ribavirin (Incivek combination treatment). Significantly, some patients died when they continued to receive Incivek combination treatment after
developing a worsening, or progressive rash and systemic symptoms (symptoms affecting the entire body). As a result, FDA is adding a boxed
warning to the Incivek drug label stating that Incivek combination treatment must be immediately stopped in patients experiencing a rash with systemic symptoms or a progressive severe rash. Consideration should also be given to stopping any other medications that may be associated with serious skin reactions. Typical systemic symptoms and signs may include fever, nausea,
diarrhea, mouth sores or ulcers, facial swelling (edema), red or inflamed eyes, or swelling or inflammation of the liver (hepatitis). All patients with
serious skin reactions should also receive urgent medical care.
Black Box Warning – Severe Rash

Telaprevir and Anal Pain
Ring of Fire! Aggravating.
Occurs in about 20% of patients, mild in most, occasionlly severe. Topical lidocaine, steroid supporitories. May respond to amitryptyline?
Typically have not stopped treatment due to this.

Anemia
Telaprevir and Boceprevir

Med
ian
Hem
og
lob
in (
g/d
L)
0
Weeks
4 8 12 16 20 24
11
12
13
14
15
8
9
10
Anemia during triple therapy withTelaprevir or Boceprevir
CHC PegIFN+RBV
CHC PegIFN+RBV+ TPV
CHC PegIFN+RBV+BOC
McHutchison JG et al, N Engl J Med. 2010
Poordad F, et al. Hepatology 2010;52(Suppl.):402ABacon, B, et al. Hepatology 2010; 52(Suppl):430A
This Slide courtesy of X Forns, MDModified by GTE

Management of Anemia
Step 1: RBV Dose Reduction
Step 2: EPA therapy
Step 3: Transfusion
Step 4: Discontinuation of TPV or BOC

Drug-Drug Interactions(CNIs)

Drug XOral
Drug XIV
KidneyP-gp → Urine
CYP3A4 → Metabolism
LiverP-gp → Bile
CYP3A4 → Metabolism
IntestineP-gp → Int Lumen
CYP3A4 → Metabolism
Drug X SystemicExposureIncreases
IS MedsStatins
BenzodiazepinesAntipsychotics?
E-mycinsAnticonvulsants
HIV PIs, NNIsα-Adren BlkrsCa++-Ch Blkrs
Impact of BOC or TPV on Drug X
X
X
X
X
X
X
Kiser J, et al. Review and Management of Drug Interactions with Boceprevir and Telaprevir. Hepatology 2012;55:1620-8

Garg V, et al. Effect of Telaprevir on the PK of CSA and TAC. Hepatology 2011;54:20-27.
Tacrolimus

0
1
2
3
4
5
6
7
8
9
Ratio AUCs for Drug (w/wo TPV)
From tables in Prescribing Information for INCIVEK, May 2011Kiser J, et al. Review and Management of DDIs with Boceprevir and Telaprevir. Hepatology 2012.
Drug X AUC Ratio w/wo TPV

Management
• Dose Adjust DRUG X
• Adjust Duration between doses of DRUG X
• Monitor Closely– Drug Levels– Laboratory Parameters– Clinical Assessment of the Patient

Resources for DDIs
• Outstanding – University of Liverpool (David Back, Editorial Board, EASL reps); sponsored by Janssen, MSD, Roche, Vertex:– http://www.hep-druginteractions.org
• FDA:– http://www.fda.gov/Drugs/DrugSafety/
• Other Online Resources –– http://www.drugs.com/drug-interactions/html– http://www.merckmedicus.com/pp/us/hep– Epocrates– Micromedex, Lexicomp and Others

Goals of Future Treatments Improve rates of SVR to 100% Activity against all HCV genotypes and subtypes Simplify treatment algorithms Extend treatment to the “difficult to treat”, “difficult to cure”
Eliminate side effects Eliminate peginterferon Eliminate ribavirin Avoid rash, anemia, anal pain, and dysgeusia Reduce drug-drug interactions
Reduce complexity and pill burden by avoiding - Injections (shots) 24, up to 48, total Ribavirin up to 6/d Telaprevir 6/d x 3 months Boceprevir 12/d from 24 to 44 wks
Reduce treatment duration
Reduce costs

What’s on the Horizon?

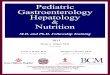
HCV Proteins and their Functions
Charles M. Rice, PhD. Top Antivir Med 2011;19:117-120.

Timelines
2011 2013 2015 2017
PR
PR + 1st Gen DAA
PR + 2nd Gen DAA
IFN-FreeRegimens
QUAD or QUINT Rescue

Simiprevir
Inhibitor of NS3/4a Protease

Daclatasvir
Inhibitor of NS5a Protein

Sofusbivir
Inhibitor (Nuc) of NS5b Polymerase

Regimens of DAA + PEG/RBV(Virologic Responses in Rx-Naïve Patients with HCV GT1)
BOC MCB TPV DAC DNV SMV FDP SOF ABT0
20
40
60
80
100
50
6065
78 79 8287
92100
% of Pts with HCV RNA (<10 IU/mL) weeks 4 - 12
Increased potency also reduces risk for emergence of resistant viral variants – e.g., MK-5172 isactive in vitro against common variants with resistance to TPV or BOC.

Case

Two years after triple therapy another blood sample is analyzed for resistant variants of HCV.
Base Wk 1 Wk 4 Wk 8 Post-Rx Wk4
Post-Rx Wk12
Post-Rx Wk16
Post-Rx Yr2
0
500000
1000000
1500000
2000000
2500000
3000000
V36M - - -T54A - - -R155K - + -A156V - - -
Stopped allMeds due toDiverticulitis
R155KDetected
WT
HCV RNAPositive
HCV RNA negative

Within a few weeks of discontinuing Triple Therapy, the patient had relapsed and tested positive for R155K, an
HCV variant with resistance to TPV. On retesting, 2 years after triple therapy, only wild-type and no variant of HCV could be detected. Assuming all options listed below are
available, which re-treatment would be most successful in achieving SVR?
1. Peginterferon/Ribavirin (PR)
2. Telaprevir + PR
3. Boceprevir + PR
4. Simeprevir + PR
5. Sofusbevir + PR

Within a few weeks of discontinuing Triple Therapy, the patient had relapsed and tested positive for R155K, an
HCV variant with resistance to TPV. On retesting, 2 years after triple therapy, only wild-type and no variant of HCV could be detected. Assuming all options listed below are
available, which re-treatment would be most successful in achieving SVR?
1. Peginterferon/Ribavirin (PR)
2. Telaprevir + PR
3. Boceprevir + PR
4. Simeprevir + PR
5. Sofusbevir + PR

IFN-Free Combinations

Dual DAA (Daclatasvir+Asunaprevir)
GT 1 Null Responders to PEG/RBV

DUAL DAA in GT1 Null Responders Daclatasvir + Asunaprevir (n=11)
RVR cEVR EOT SVR120
20
40
60
80
100
63.6
45.5 45.536.4
% HCV RNA <10 IU/mL
Lok A, et al. RVR/cEVR presented at AASLD 2010. SVR12 presented EASL 2011. N Engl J Med 2012;366:216-224 .Daclatasvir 60 mg qd, Asunaprevir 600 mg bid, 24 weeks treatment.
All breakthroughsOccurred in
Patients with G1a

QUAD (or QUINT) Therapy
When all else fails!

QUAD in the Treatment of G1 Null RespondersBMS-790052/BMS-650032 + PR (n=10), 24 Weeks of Rx
RVR cEVR EOT SVR120
20
40
60
80
100
60
100 10090
% HCV RNA <10 IU/mL
Lok A, et al. N Engl J Med 2012;366:216-224.790052 60 mg qd, 650032 600 mg bid; SVR at week24 post-Rx

Optimistic Results in Phase 2 TrialsGT
2/3
SOF
R 12
W
GT2/
3 SO
F DA
C...
GT1b
DAC
ASV
24W
GT1a
DAC
ASV
P...
GT1
CC 5
885
945.
..
GT1
CC 5
885
945.
..
GT1
SOF
DAC
12W
GT1
DAC
ASV
71...
GT1
AA D
tT S
OF
...
GT1
ABT4
50r 2
67...
GT1
Nul
l ABT
450.
..
GT1
Fib
DNV
MER
...
GT1b
Nul
l DAC
A...
GT1
Nul
l DAC
AS.
..
GT1b
FAL
127
R...
GT1a
FAL
127
R...
GT1
SOF
PR 1
2W
GT4
SOF
PR 1
2W
GT6
SOF
PR 1
2W
GT1
SOF
5885
R...
0
20
40
60
80
100
% SVR

Thompson A, et al. Six Weeks of an NS5A Inhibitor (GS-5885) and a Protease Inhibitor (GS-9451) Plus Peginterferon+Ribavirin Achieves High SVR4 Rates in Genotype 1 IL28B CC Treatment-Naïve Hepatitis C Virus Patients: Interim Results of a Prospective, Randomized Trial. AASLD
2012.
Lok AS, et al. Preliminary Study of two antiviral agents for Hepatitis C Genotype 1. N Engl J Med 2012;366:216-224.
Chayama K, et al. Dual therapy with the nonstructural protein 5A inhibitor, daclatasvir, and the nonstructural protein 3 protease inhibitor, asunaprevir, in hepatitis C virus genotype 1b-infected null responders. Hepatology 2012;55:742-748.
Sulkowski M, et al. High Rate of Sustained Virologic Response With the All-Oral Combination of Daclatasvir (NS5A Inhibitor) Plus Sofosbuvir (Nucleotide NS5B Inhibitor), With or Without Ribavirin, in Treatment-Naive Patients Chronically Infected With HCV GT 1, 2, or 3. AASLD 2012.
Everson GT, et al. An Interferon-Free, Ribavirin-Free 12-Week Regimen of Daclatasvir (DCV), Asunaprevir (ASV), and BMS-791325 Yielded SVR4 of 94% in Treatment-Naïve Patients with Genotype (GT) 1 Chronic Hepatitis C Virus (HCV) Infection. AASLD 2012.
Osinusi A, et al. High Efficacy of GS-7977 in Combination with Low or Full dose Ribavirin for 24 weeks in Difficult to Treat HCV Infected Genotype 1 Patients. AASLD 2012.
Kowdley KV, et al. A 12-week Interferon-free Treatment Regimen With ABT-450/r, ABT 267, ABT-333, and Ribavirin Achieves SVR12 Rates (Observed Data) of 99% in Treatment-naïve Patients and 93% in Prior Null Responders With HCV Genotype 1 Infection. AASLD 2012.
Jacobson IM, et al. Safety and efficacy of ritonavir-boosted danoprevir (DNVr), peginterferon alfa-2a (40KD), and ribavirin with or without mericitabine in HCV genotype 1-infected treatment-experienced patients with advanced hepatic fibrosis: the MATTERHORN study. AASLD
2012.
Lok AS, et al. Sustained Virologic Response in Chronic HCV Genotype (GT) 1-Infected Null Responders With Combination of Daclatasvir (DCV; NS5A Inhibitor) and Asunaprevir (ASV; NS3 Inhibitor) With or Without Peginterferon Alfa-2a/Ribavirin (PEG/RBV) . AASLD 2012.
Zeuzem S, et al. Sustained Virologic Response in Chronic HCV Genotype (GT) 1-Infected Null Responders With Combination of Daclatasvir (DCV; NS5A Inhibitor) and Asunaprevir (ASV; NS3 Inhibitor) With or Without Peginterferon Alfa-2a/Ribavirin (PEG/RBV) . AASLD 2012
Hassenein T, et al. Once Daily Sofosbuvir (GS-7977) plus PEG/RBV In Treatment-Naïve Patients With HCV Genotype 1, 4, and 6 Infection: The ATOMIC Study. AASLD 2012.
Gane E, et al. 100 Percent Sustained Virologic Response Rate (SVR4) for an Interferon-Free Regimen of Sofosbuvir (GS-7977), GS-5885 and Ribavirin in Treatment-Naïve Genotype 1 Hepatitis C Infected Patients. AASLD 2012.

The Promise of Future Treatments
1. Pan-genotypic coverage
2. IFN-Free Regimens (Gilead, Abbott, BMS, Roche/Genentech, BI)
3. Greater Potency – higher rates of SVR
4. Shortened Duration of Treatment
5. Improved Tolerability and Safety
6. Less bone marrow suppression or hemolysis

Perspective

Future Treatment for HCV GT1
2 716
2840
70 85 92 98100
020406080
100
% of Patients with SVR
1991 Yr of FDA Approval 2011 2013 2015

Future Treatment for HCV GT2 & 3
1629
69 6680 90 100 100
020406080
100
% of Patients with SVR
1991 Yr of FDA Approval 2002 2013 2015

The Real Impact Could Be -
1. Reduction in costs of care for HCV
2. Reduction in liver-related death
3. Reduction in Hepatocellular carcinoma
4. Reduction in need for liver transplantation
5. Reduction in autoimmune disorders
6. Reduction in adult-onset diabetes mellitus
7. Reduction in B-cell lymphoma