Embed Size (px)
Citation preview
ResearchcommissionedbyCancerResearchUKandconductedbytheUniversityofBirmingham’sHealthServicesManagementCentreandICFInternational
ADVANCINGCARE,ADVANCINGYEARS:IMPROVINGCANCERTREATMENTANDCAREFORANAGEINGPOPULATIONJUNE2018

AdvancingCare,AdvancingYears 2
Researchcommissionedby
AdvancingCare,AdvancingYears 3
ACKNOWLEDGEMENTSCancerResearchUKcommissionedtheUniversityofBirminghamHealthServicesManagementCentreandICFInternationaltocarryouttheresearchunderpinningthisreport.
Theauthorsofthestudyareasfollows:
KerryAllen HSMC,UniversityofBirmingham
HilaryBrown HSMC,UniversityofBirmingham
KellySingh ICFInternational
HollyKrelle ICFInternational
AliceBennett ICFInternational
RoseGray CancerResearchUK
HelenBeck CancerResearchUK
Wearegratefulforthevaluableinputofoursteeringgroup.ThiswascomprisedofHelenBeck,MaggieKemner,NickOrmiston-Smith,ArniePurushotham,EmlynSamuel,SimonShears,RoxySquire,SarahTestoriandLynneWright.ItisparticularlyworthhighlightingthecontributionofLynneWright,whoensuredthattheviewsofpeopleaffectedbycancerwererepresentedthroughoutthisresearch.
Wewouldalsoliketothanktheolderpeoplewithexperienceofcancerserviceswhoco-designedthepatientsurvey,shapedtheanalysisandsharedverypersonalandvaluableinsightswithus.
Wearealsogratefultoallhealthprofessionalswhoparticipatedinoursurveys,whoallowedtheirMDTmeetingstobeobservedandwhotookthetimetodiscusstheirviewswithusthroughouttheproject.
ThankyoualsotoSeanDuffy,ArniePurushotham,RichardSimcock,JackieBridgesandallotherswhoprovidedcommentsonearlierdraftsofthereport.
Thisreportshouldbereferenced:‘CancerResearchUK(2018)Advancingcare,advancingyears:improvingcancertreatmentandcareforanageingpopulation’.
ABOUTCANCERRESEARCHUKCancerResearchUKistheworld’slargestindependentcancercharitydedicatedtosavinglivesthroughresearch.Itsupportsresearchintoallaspectsofcancerandthisisachievedthroughtheworkofover4,000scientists,doctorsandnurses.In2016/17,wespent£432milliononresearchinstitutes,hospitalsanduniversitiesacrosstheUK.WereceivenofundingfromtheGovernmentforourresearchandaredependentonfundraisingwiththepublic.CancerResearchUKwantstoaccelerateprogresssothatthreeinfourpeoplesurvivetheircancerfor10yearsormoreby2034.Cancer Research UK is a registered charity in England and Wales (1089464), Scotland(SC041666)andtheIsleofMan(1103)
AdvancingCare,AdvancingYears 4
CONTENTS
LISTOFACRONYMS
5
LISTOFFIGURESANDTABLES
6
EXECUTIVESUMMARY 7
1.BACKGROUND
19
2.OLDERPATIENTSHAVEMORECOMPLEXCARENEEDS–ANDTHESYSTEMISNOTSETUPTODEALWITHTHEM
30
3.TREATMENTDECISION-MAKINGDOESNOTALWAYSTAKEALLRELEVANTFACTORSINTOACCOUNT
37
4.THERIGHTINFORMATIONDOESNOTALWAYSGETTOTHERIGHTPEOPLETOSUPPORTCLINICALDECISION-MAKING
43
5.THECANCERWORKFORCECOULDBETTERSUPPORTTHENEEDSOFOLDERPATIENTS
52
6.WENEEDTOIMPROVEHOWINNOVATIONINTREATMENTANDCAREREACHESOLDERPEOPLEWITHCANCER
56
APPENDIX1.METHODOLOGY 59
APPENDIX2.PATIENTMESSAGESTOTHENHS 61
REFERENCES 63
AdvancingCare,AdvancingYears 5
LISTOFACRONYMS
ADL ActivitiesofDailyLiving
CanCORS CancerCareOutcomesandResearchSurveillanceConsortium
CRUK CancerResearchUK
CPET/CPEX CardiopulmonaryExerciseTesting
COPD ChronicObstructivePulmonaryDisease
CNS ClinicalNurseSpecialist
CGA ComprehensiveGeriatricAssessment
ECG Electrocardiogram
eFI Electronicfrailtyindex
EORTC TheEuropeanOrganisationforResearchandTreatmentofCancer
EUSOMA TheEuropeanSocietyofBreastCancerSpecialists
GP GeneralPractitioner
HDU HighDependencyUnit
HNA HolisticNeedsAssessment
ITU IntensiveTreatmentUnit
SIOG InternationalSocietyofGeriatricOncology
MDT Multidisciplinaryteam
NCIN NationalCancerInformationNetwork
NCCN TheUSNationalComprehensiveCancerNetwork
NICE NationalInstituteforHealthandCareExcellence
RWE Real-worldevidence
SMC ScottishMedicineConsortium
SDM Shareddecision-making
SCOPES SystematicCareforOlderPeopleinElectiveSurgery
AdvancingCare,AdvancingYears 6
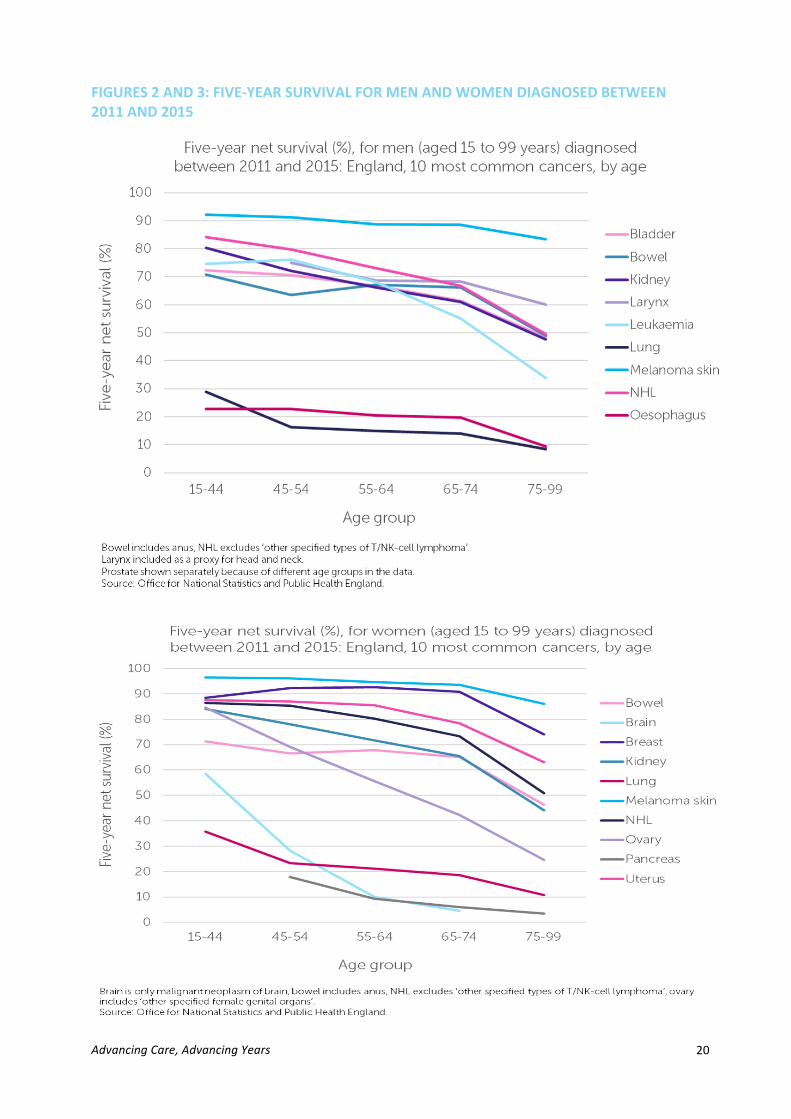
LISTOFFIGURESANDTABLESFigure1:projecteddemographicsforcancerincidenceandmortalityin2035Figure2:five-yearnetsurvival(%)formen(aged15to99years),diagnosedbetween2011and2015:England,10mostcommoncancers,byageFigure3:five-yearnetsurvival(%)forwomen(aged15to99years),diagnosedbetween2011and2015:England,10mostcommoncancers,byageFigure4:primarycarestaff’smethodologyforassessingfrailtyFigure5(primarycaresurvey)wouldyouliketoseeagreaterroleforprimarycareinpre-treatmentoptimisation?

AdvancingCare,AdvancingYears 7
EXECUTIVESUMMARYAround360,000peopleintheUKwerediagnosedwithcancerin2015.36%ofthesepeoplewere75andover.By2035,thisproportionwillrisetoalmosthalf(46%)1,becauseoftheUK’sageingpopulation.
Asthepatientpopulationchanges,servicesmustadapttomakesuretheyaremeetingeveryperson’sneedsandthatnogroupisleftbehind.Nowandinthefuture,itiscrucialthatolderpeoplewithcanceraregiventhesupporttheyneedtoaccessthemostappropriatetreatmentforthem,andtohavethebestpossibleexperienceofcare.
Inthisinstance,ageisaproxymeasureforcomplexity:increasingageiscorrelatedwithhavingmultiplehealthconditions,cognitiveissuesorcomplexsocialcareneeds–allofwhichcanrequirecancertreatmentandcareplanstobemodified.However,itisimportanttonotethatthisisnottrueforeverypersonover75andtherearemanypeopleunder75whoalsohavecomplexneeds.However,itisalsohighlylikelythatthisgroupofpatientswithmorecomplexneeds–andthereforemanypatientsover75–aretheoneswhowillbemostaffectedbywiderpressuresfacingtheNHS.Thesepressuresincludesevereshortagesinkeyprofessionalgroups,aswellasalackoftimeforlongconsultationsintheclinicandforcancermultidisciplinaryteams(MDTs)todiscusspatients’cases.Soalthoughtherecommendationsinthisbriefingaretargetedtowardsensuringcancerservicesmeettheneedsofolderpeoplewithcancer,ifimplementedmanyofthemwouldbenefitallpatientsintheNHS–ofallages.However,evidenceshowsthatrightnowthereareage-relatedinequalitiesincanceroutcomes.CancersurvivalisgenerallylowerforolderpatientsandthediscrepancybetweentheUK’sperformanceandthebest-performingcountriesisworseforolderpatientsthanitisforyoungerpatients2,3,4.Althoughoverallcancersurvivalhasdoubledinthelast40years,thediscrepancybetweencancer-specificsurvivalforolderandyoungerpatientshaspersisted.Ifwearetoachieveourambitionsofachievingworld-classoutcomesforeveryoneaffectedbycancer,itisvitalthatweimprovethetreatmentandcareofolderpatients.Olderpatientsarealsolesslikelytoreceivemanydifferenttypesoftreatment5.Someofthevariationinaccesstotreatmentcanbeaccountedforbypatientschoosingnottopursueactivetreatment.Thiscouldbebecausetheyaresimplytoounwellorbecause,forexample,theyareprioritisingmaintainingagoodqualityoflifeandspendingtimewithfamilyoverlengtheningtheirlife.However,theremayalsobesomewhoaresimplynotbeingofferedcurativetreatmentthatcouldbenefitthem,becauseassumptionshavebeenmadeabouttheirfitnessbasedontheirage.Incontrast,wealsoheardanecdotallythatsomefeelpressuredbytheirclinicianstoundergointensivecurativetreatment.Wemustgetthisbalanceright.Treatmentdecisionsshouldconsistentlybeshapedaroundeachperson’sindividualsituation.Achievingthisis,ofcourse,importantforeverypersondiagnosedwithcancer.However,itismostdifficulttoachievethisforthosewhohavemorecomplexmedicalorsocialneeds,orwhoneedmoretimeandsupporttocometoadecisionabouttheirtreatmentplan.Thisisthecurrentchallenge.

AdvancingCare,AdvancingYears 8
Onereasonforthis–ashighlightedbythe2015CancerStrategyforEngland6–isthatmethodsofassessingolderpatientsarenotfitforpurpose,resultinginolderpeople’sneedsnotbeingidentifiedorsufficientlywell-understood7.Therearealsoissueswiththeknowledgeandawarenessofthecancerworkforceaboutthespecificchallengesoftreatingolderpatients,andthereisalackofevidencetosupportnewcancertreatmentsinolderpopulations8.ThisreportpresentsresearchcommissionedbyCancerResearchUK(CRUK)andconductedbytheUniversityofBirmingham’sHealthServicesManagementCentreandICFInternational,whichsoughttounderstandthespecificneedsofolderpatients,andtoexploretheprocessofclinicaldecision-makingforolderpeoplewithcanceracrosstheUK.Thisresearchinvolvedaliteraturereview,clinicalobservationsateightcasestudysites,interviewswith15nationaldecision-makersand80healthprofessionals,andthreeUK-widesurveys(ofprimarycareprofessionals,secondarycareprofessionalsandolderpeopleaffectedbycancer).Thedirectionoftheresearchwasalsoinformedbyengagementwithagroupofolderpeopleaffectedbycancer,andbyextensiveengagementandinterviewswithnationalpolicymakers.FullmethodologyisavailableinAppendix1.
OLDERPEOPLEANDCANCERIn2035,itisprojectedthataround234,000casesofallcancerscombined1willbediagnosedinpeopleaged75andoverintheUK.Peopleaged75andoverareprojectedtoaccountfor46%ofallcancerdiagnosesand62%ofallcancerdeaths9.
Netsurvivalisgenerallylowerforpatientsover75,withsurvivalgenerallydecreasingwithincreasingage–evenafteradjustingformortalityfromcausesotherthancancer.Despiteoverallsurvivaldoublingoverthepast40years,thediscrepancybetweensurvivalforolderandyoungerpatientshasnotimproved10.
ThereisalsoevidencethatthegapbetweentheUK’scancersurvivalandthatofthebest-performingcountriesisworseforolderpatients.Forexample,mostofthesurvivaldifferenceforbreastcancerbetweentheUKandIrelandandtheEuropeanaveragecanbeaccountedforbythelowsurvivalofwomenage75andover11.Incolorectal(bowel)cancer,five-yearsurvivalwas15%lowerinUKpatientsaged75andolderthantheequivalentpatientsinCanadadiagnosedbetween2005-2007,whileitwas9.5%lowerforpatientsaged15-4412.
Thereareseveralreasonswhythisisthecase.Forexample,olderpeoplearemorelikelytohavepooreroverallhealth,andaremorelikelytobediagnosedinanemergency,whichisassociatedwithbeingdiagnosedatalaterstage,andwithpoorersurvival13.Between2006and2015,41%ofallcancersinthoseaged80-84werediagnosedinanemergencyinEngland,comparedwith14%ofcancersinthoseaged50-59.Althoughthereisaclearneedtoimproveearlydiagnosisofcancerinolderpatients,thatisoutsideofthescopeofthisbriefing.
However,therearealsodiscrepanciesinaccesstotreatmentforolderpeoplewithcancer.AreportbytheNationalCancerInformationNetwork(NCIN)andCRUKfoundthatacross20
1Around130,000inmalesandaround104,000infemales
AdvancingCare,AdvancingYears 9
cancersites,olderpatientswerelesslikelytohavemajorsurgicalresections14.Ithasalsobeenreportedthattheuseofchemotherapydeclineswithage,inseveraltypesofcancer15.Otherstudieshavefoundsimilar;forexample,olderwomenwithbreastcancerarelesslikelytoundergosurgery16;theuseofradiotherapyalsograduallydecreaseswithage17.Olderpeoplewithlungcancerhavealsobeenshowntobefarlesslikelytoundergosurgery18.
Insomecases,therearelegitimatereasonsfortheselowertreatmentrates.Forexample,olderpatientsaremorelikelytohaveotherhealthconditions,whichcouldmeantheyareunabletotolerateeitherthetreatmentitself,ortheside-effectsofthetreatment19,20,21.Somestudieshaveadjustedforcomorbiditiesandhavestillfoundvariationinaccess22,23–suggestingtherecouldbesomeinappropriatedecision-makingbasedonchronologicalage.However,somepatientsmayalsochoosenottopursuecurativetreatments,forvariousreasons.Recentresearchhasfoundthatwhenconsideringchemotherapy,overhalfofolderpatientssurveyedprioritisedoutcomesotherthansurvival,forexamplemaintainingtheirqualityoflife,independenceorcognitiveabilities24.
FINDINGSANDRECOMMENDATIONSOLDERPATIENTSOFTENHAVEMORECOMPLEXCARENEEDS–ANDTHESYSTEMISNOTSETUPTODEALWITHTHEM
Olderpeoplewithcanceraremorelikelytohavecomplexmedicalandsocialneeds,whichcanmeantheyrequireadditionalsupporttoaccesstreatment.Forexample,olderpatientsaremorelikelytohaveotherage-relatedillnesses,butalsomorelikelytorequiresocialcaresupport.Furthermore,upto40%ofolderpatientspresentwithcognitiveissuesthatcanimpairtheircapacitytomakecomplexdecisionsabouttreatment,adheretotreatmentplansandrecognisesymptomsoftoxicitythatmightrequiremedicalattention25.Throughourengagementwithhealthprofessionalsaspartofourresearch,weidentifiedfourmainclinicalfactorswhichtendtoimpactthetreatmentoptionsforolderpatients:
1. Thepatient’sfitnesstowithstandtherigoursoftreatment2. Thelikelihoodthatthepatientwilldiefromacauseotherthantheircancer3. Whetherthepatienthascomorbidities4. Ifthereisclinicalevidencetosupportaparticularcourseoftreatmentinanolder
patient
Manyolderpeoplewithcanceralsohaveadditionalsocialsupportneeds.Forexample,theymightcareforalovedoneorthemselvesrequirecarersupport.Thiscanalsoimpacttreatmentchoices.Theolderpeopleaffectedbycancerinvolvedinourresearchtoldusthatuncertaintyabouthowtheywouldaccessnon-medicalsupportcanbeamajorbarriertoaccessingtreatment.Similarly,46%ofcancermultidisciplinaryteam(MDT)memberssurveyedforthisresearchidentifiedalackofsocialorpracticalsupportasabarriertoolderpeopleaccessingthemosteffectivetreatmentfortheircancer.
AdvancingCare,AdvancingYears 10
Unfortunately,thesupportpatientsneedisoftennotavailable.Althoughourintervieweesvaluedcommunity-basedsupportsuchasoncologynursesorconvalescencehomes,availabilityofthissupportisvariable.Althoughpatientscansometimesarrangetheirownalternativecare,costcanoftenbeamajorbarrier.Thisspeakstoamuchbroaderissuewithsocialcare,whichiscruciallyimportantbutoutsidethescopeofthisresearch.However,therearedefinedactionsthatcouldhelpmakesureallthesupportneedsofpeoplewithcanceraremetthroughouttreatmentandrecovery.Forexample,anearlierassessmentofaperson’ssupportneedswouldhelpensurethereisenoughtimetoplansupportrequiredfortheweeksfollowingamajoroperation.Cancerservicescouldalsodomoretoembedconsiderationofthespecificneedsofolderpeoplewithcancerinhowservicesareplannedanddelivered.Wherethereareservicereconfigurations,theremustbearecognitionthatolderpatientsaremorelikelytorequireadditionalsupporttotraveltotreatment.Forexample,ourintervieweesbasedatsiteswherepatientsaremorelikelytohavetotravelfortreatment–suchastertiarycentresservingamostlyruralarea–expressedconcernsthatolderpatientscouldbeexcludedfromtreatment,orfromtakingpartinclinicaltrials.
Soyes,itismoredifficultforolderpeopletogettransportandit’spossiblethatalotofthemdon'twanttobeabothertotheirfamilies…gettingonbuses,trains,whatever,isnotidealandthekindofambulance,minibusservicetrailsthemroundthecountryso
theydon'tlikethat…it’sanotherburdenthattheyhave.(Medicaloncologist)
InEngland,whereradiotherapyservicesaresoontobere-organisedintonewRadiotherapyNetworks,thereisatimelyopportunitytoembedtheneedsofolderpeoplewithcancerinthisprocess,throughmeaningfulpatientinvolvementasservicesareplanned.1.Cancerservicemanagersshouldensurethatpatients’supportneedsareassessedatanearlystageinthepathway,sothattheyareabletoaccessthesupporttheyneedduringandaftercompletingtreatment.HealthserviceregulatorsshouldconsiderwaystoensurethatthisisdoneeffectivelyandconsistentlyacrosstheUK.2.UKhealthservicesshouldensurethatthespecificneedsofolderpatientsareconsideredinallnewserviceplansandworkforceplans.Forexample,emergingRadiotherapyNetworksinEnglandshouldconsidertheimpactofchangingtravelrequirementsonolderpatientsandshouldworkwithcharitiesandproviderstoensureallpatientsaregiventhesupporttheyneedtoreceivetreatment.TREATMENTDECISION-MAKINGDOESNOTALWAYSTAKEALLRELEVANTFACTORSINTOACCOUNTWecanonlybesurethattreatmentdecisionsarerightforpatientsifweareconfidentthatthedecisionstakeintoaccountallrelevantinformationaboutthatperson.Thisistrueforeverypatient,butisparticularlyimportantforpatientswithadditionalmedicalandsocial
AdvancingCare,AdvancingYears 11
needs–whichwillincludemanyolderpeople.Unfortunately,thesecomplexneedsareoftennotroutinelyconsideredaspartofthetreatmentdecision-makingprocessincancer.Thisispartlybecauseserviceslacktherighttoolstoassessfrailtyinthecancersetting,andComprehensiveGeriatricAssessmentsarestillrarelyusedinoncology.Thisisimportant:itiswidelyrecognisedthatchronologicalagealoneisnotastrongindicatorofhowwellapersonwilltoleratecancertreatment26.Frailtyassessmentscanbeusedtopredicthowwellapatientwillbeabletotoleratetreatment,ortohelpassesswhatadditionalsupportcouldhelpthem.Intheabsenceofarobustmethod,assessmentofapatient’sfitnessfortreatmentcaninsteadbeassumedbasedontheirage,orsimplyasubjectiveassessmentofhowtheyseemduringaconsultation.OurresearchalsofoundthatComprehensiveGeriatricAssessments–orCGAs–arerarelyusedinoncology.ACGAsupportscliniciansbyprovidinganevidence-basedassessmentoffrailty,reducingthesubjectivityoftheassessment,andhelpsmakesurecareiscentredaroundthepatientandtheirindividualneeds.While70%ofprimarycarestaffsurveyedtoldusthattheirassessmentofapatient’sfrailtyimpactstheirdecision-making,wefoundverylimitedevidenceofCGAusageandlowawarenessofthetoolsavailable.Similarly,althoughthemostsignificantfactorinclinicaldecision-makingidentifiedbymultidisciplinaryteam(MDT)meetingmemberswasfrailty,CGAswereusedinfewofthesitesweobservedascasestudies.Wealsoheardthatmanyclinicianswereunconvincedofthevaluethesetoolswouldadd,orthoughttheywouldnotbeworththeextraresourcesrequiredtoimplement.Cliniciansoftentendedtofavourmoreinformal,intuitiveassessmentratherthanarobustandformaltool.
Imeancertainlythedatawouldsuggestit(primarycarefrailtyassessment)maybepartoftheproblem.Ifyoulookatthesortofthecanceroutcomesandsortofstagesat
presentation,clearlythereisabiasandweareservingourelderlypatientslesswellthanwearetheiryoungercompatriots.
(Nationalinterviewee)Thesefindingsaredisappointing,howeverunsurprising:althoughthereiswidespreadconsensusaboutthevalueofCGAsingeneral,andevidenceoftheirbeneficialimpactinoncology,thereisnoclearevidenceregardingthebesttooltouse27andtheyhavenotbeenfullyintegratedintooncologypractice28.AlthoughthereareseveralpiecesofguidanceaboutconductingCGAsincancer,theiruseisstillhighlyvariable–oftenbecauseofalackofstaff,aswellasotherinstitutionaland/orfundingconstraints29.However,thereisclearvalueintheiruse:casestudysitesthathadembeddedgeriatrician-ledmultidisciplinaryCGAclinicsintothedecision-makingprocessdidreportbetterimprovedadherencetochemotherapyandincreasedratesofsurgery30.3.UKhealthservicesshouldpilottheroutineusageofgeriatricassessmentsforolderpeoplewithcancerandshouldseektogatherfurtherevidenceoftherelativebenefitsofdifferenttools.
AdvancingCare,AdvancingYears 12
THERIGHTINFORMATIONDOESNOTALWAYSGETTOTHERIGHTPEOPLETOSUPPORTCLINICALDECISION-MAKINGTherearealsosystemicissuesincancerservicesthatlimittheamountofinformationthatisavailabletosupportclinicaldecision-making.Again,theseissuesapplytoallpatients–butarefeltmoreacutelyinmorecomplexcases,andthereforeofteninolderpatients.Forexample,patientdataisoftennotsharedbetweenthefullrangeofhealthprofessionalscaringforapatient,orevenwiththepatientthemselves.
INFORMATIONDOESNOTFLOWFROMPRIMARYCARETOSECONDARYCARE37%ofpatientsdiagnosedinEnglandin2015werediagnosedthroughanurgentGPreferral,knownasthe“two-weekwait”31,arouteattachedwithtargetsinEnglandandWalesrequiringpatientstobeseenwithintwoweeksofGPreferral.Thesereferralsareprocessedusingforms,whicharespecifictoeachsuspectedtypeofcanceranddifferbetweentrustsandregions.Theseformsarebriefandthusthereisnospaceforprimarycarestafftocommunicatepeople’spersonalcircumstances,comorbidities,theirfrailtyorothermedicalhistory.Thismeansthatthecliniciansmakingdecisionsaboutpatients’treatmentoftendonothaveadvancedaccesstoinformationthatcouldlaterprovecritical–andsotheperson’sageismorelikelytobeusedasasurrogatemeasurefortheiroverallhealth.
Itdoesn’tsaywhatmedicationthey’reon,whataretheircomorbidities,whataretherealissues,whatarethesocialfactors,doesn’ttellanythingabouttheperson,itjust
tellsyoupotentiallywhatcouldberelatedtothedisease.(NationalInterviewee)
Arelativelysimplechangetotheseformscouldresultinasignificantimprovementintheamountofinformationavailabletoinformtreatmentdecisions–forallpatients.Asformsdifferfromregiontoregiontherearesomenotableexamplesofgoodpractice,wherethosemakingreferralshavespaceforadditionalinformation–butthishasnotbeendoneconsistently.Forexample,apilotinLeedsdevelopedadigitalsolutionthatautomaticallypopulatestheformwithallrequiredinformation32.TheremayalsobecaseswhereareferringGPhasincludedinformationinaletter,butthishasbeenlostinthesystem.4.CancerAlliancesanddevolvedcancernetworksshouldexploredigitalsolutionsforensuringthatsuspectedcancerGPreferralscanconsistentlyincorporateadditionalinformationthatcouldproverelevanttoafuturecancertreatmentplan.
THERIGHTINFORMATIONISOFTENNOTINCLUDEDINMDTDECISION-MAKINGEverypatientdiagnosedwithcancerintheUKhastheircasediscussedataMDTmeeting.AnMDTismadeupofavarietyofhealthprofessionalsinvolvedintreatingandcaringforpatients.TheMDTmeets,mostoftenweekly,todiscussindividualpatients’casesandmaketreatmentrecommendations.
AdvancingCare,AdvancingYears 13
IfMDTsaretomakeatreatmentrecommendationthatistrulyappropriateforthepatient,theymusthaveincludeallrelevantinformation.ButrecentresearchbyCRUKfoundthatonly14%ofMDTdiscussionsincludedinformationthatdidnotspecificallyrelatetothepatient’stumour33.WhilemanyMDTmembersseethisasaresponsibilityofClinicalNurseSpecialists(CNS),nursesdidnotcontributeinformationinover75%ofthemeetingsobservedinourresearch.ThisreflectsthelackoftimeavailableforfulldiscussionofcomplexpatientsinMDTmeetings,ratherthanalackofwillingnesstocontribute:theaveragediscussionobservedinourpastresearchlastedjust3.2minutes,inmeetingslastinguptofivehours,andeachdiscussionincludedanaverageofjustthreepeople–althoughanaverageof14peoplewereinattendance.Thispressurehasmajorimplicationsforthequalityoftreatmentdecision-making.Notincludingimportantinformationaboutapatient–suchastheirpreference,theirpsychosocialsituationortheircomorbidities–ispoorforpatientsandalsopoorforMDTefficiency:pastresearchhasfoundthatbetween10and15%ofrecommendationsmadebyanMDTwerenotimplementedbecausetheywerelaterfoundtobeinappropriateforthepatient34,35.ItislikelythatthisisadirectconsequenceoftheMDTnottakingallrelevantinformationaboutthepatientintoaccount.Whenthatadditionalinformationbecomesapparent,patientsareeitherdiscussedagainbytheMDT–addingadelaytotheirtreatment–oradecisionismadesolelybytheirindividualclinician,whomightlacktheexpertisetoknowhowtoincorporatethisinformationintothetreatmentplan.ThereisaclearneedtoreformandstreamlineMDTs,sothatmoretimeisavailabletodiscussthemostcomplexpatientsinenoughdepth–andtherefore,manyolderpatients.ItisalsoimportantthatMDTsconsistentlyhaveaccesstoallrelevantinformationaboutthepatientstheydiscuss,sothattheycanmaketreatmentrecommendationsthataretailoredtothepatient’sindividualcircumstances.While54%ofMDTmembersalreadyuseatypeofproformatofeedinformationintotheMDT,thisdoesnothappenconsistentlyandthereisnonationalguidanceontheircontent.81%ofMDTmemberssurveyedinourpastresearch2feltthatusingaproformawouldhaveabeneficialimpactonmeetingefficiency,byminimisingthechanceofthepatientreturningtotheMDTforre-discussionafterthefirstrecommendationwasrejected.5.UKhealthservicesshouldleadthedevelopmentofnationalproformatemplates,toberefinedbyMDTs.MDTsshouldrequireincomingcasesandreferralstohaveacompletedproformawithallinformationreadybeforediscussionatameeting.
COMMUNICATIONFROMSECONDARYCARETOPRIMARYCARESHOULDBEIMPROVEDFromoursurveysofclinicians,wealsoidentifiedanissuewiththeflowofinformationfromsecondarycarebacktoprimarycare.Thisisimportant:althoughcancercareismanagedprimarilybycancerclinicians,patients’otherhealthconditionsmightstillbemanagedin
21,258respondents.Fullresultsavailableatcruk.org/mdts-research
AdvancingCare,AdvancingYears 14
primarycare.Patientsmayalsoseekadvicefromprimarycareabouttheirtreatmentoptionsoranyside-effectstheyareexperiencing.AlthoughcliniciansshouldinformGPsofacancerdiagnosiswithin48hours,thisdoesnothappenuniformly.Primarycarestaffalsotoldustheywouldvalueadditionalinformationaboutapatient’sprognosis,theirtreatmentoptionsandtheirwidercareplan.
…itisnotuncommonforsomebodytobeinfloodsoftearsinthecaronthewayhomefromthehospital,phoningtheGP,askingforanurgentappointmenttotalkthings
throughbuttheGPdidn’tevenknowtheyhadacancerdiagnosisandwouldn’thavebeentoldfordays,sometimesweeks.(NationalintervieweeandGeneralPractitioner)
6.Healthcareprovidersmustensurethatprimarycarestaffareupdatedontheoutcomeofpatientdiscussionsinatimelymanner.Thisshouldincludewidespreaduseofdigitalsolutions.
PRESSURESONONCOLOGYSERVICESLIMITTHEQUALITYOFDECISION-MAKINGANDCOMMUNICATIONBETWEENOLDERPEOPLEWITHCANCERANDTHEIRCLINICIANSTheconceptofshareddecision-making(SDM)originatedinthedisabilityrightsmovementandisnowingrainedintotheethosofhealthservices,throughtheconceptof‘nodecisionaboutmewithoutme’.TheHealthFoundationandNICEdefineSDMas‘aprocessinwhichcliniciansandpatientsworktogethertoselecttests,treatments,management,orsupportpackages,basedonclinicalevidenceandpatients’informedpreferences’36.
Thereisstrongevidencethatshareddecision-makingisbeneficialforpeoplewithcancer37,forexamplebecauseitcanimprovepeople’sexperienceofcare38.However,achievingSDMcanbemoredifficultinpatientswithmultiplehealthconditions39,40,41,cognitiveimpairment,socialsupportneedsandcaringresponsibilities42.Thisisthereforemorelikelytobethecaseforolderpeoplewithcancer.Theolderpeoplewithcancerwhorespondedtooursurveyoftenreportednegativeexperienceswithdecision-makingandsomealsoreportedfeelingliketheirquestionswerenotwelcomed.Wealsoheardthatconversationsfocusedtoomuchonbenefitsoftreatment,glossingoverpotentialside-effectsorlong-termconsequences.
Mostly,itwasassumedthatIwoulddowhatevertheysuggested-whilstIwasnotunhappywithwhatwasbeingoffered,asIknewthattherewerenotalotofoptions,IdonotfeelinhindsightthatIwasgivenmuchchoiceorindeedsupportinmakingsuch
achoice.(Apatient)
Thesedifficultiesareexacerbatedbytimepressureinatreatmentconsultation–andthiswasreflectedinourengagementwithbotholderpatientsandclinicians.Whilealackoftimeeffectsallpatients,thereisagreaterimpactonpatientswithcomplexneeds,comorbiditiesorcognitiveissues–andtherefore,again,manyolderpeoplewithcancer.
TodayIhadapatientwhohascancerbuthasothercomorbidities…soIhadtodiscuss
AdvancingCare,AdvancingYears 15
that…andmakeitcleartothemthatthesearetheriskfactors,thesearethethingsthatgowrong…that20/30minutes…justgetsdraggedonto45minutes.Wecan’tjuststoptheconsultationbecauseit’sbeenrunningoutoftime.(Anaesthetist)
7.CancerMDTleadsandservicemanagersshouldconsiderreviewingthelengthofconsultationslots,factoringinadditionaltimeformorecomplexpatients,andprovidingadditionalsupportbefore,duringandafterconsultationsforthosewhoarelivingwithfrailtyorhavemultiplecomorbidities.
Cancertreatmentdecision-makingintheUKisalsostronglyimpactedbynationaltreatmenttargets.SeveralmembersofcancerMDTsinterviewedforthisstudyraisedtheissueofnationaltreatmenttargetscreatingunhelpfulpressure,fortworeasons:firstly,throughputtingpatientsunderpressuretomakeaquickdecision,butsecondlybylimitingopportunitiesfortestingpatients’likelihoodtobeabletotoleratetreatment,andthentotailortheirplanaccordingly.
They’reguidelinesnottramlinesandIthinkpeoplegetsocaughtupinthat,thatyouforgetthepatientmaynotwanttoworkinthetimescalethattheguidelinessay.(Nationalinterviewee)
Thishasbeenechoedinresearch,whichhasfoundthatservicetargetsthatfocusresourcesolelyoncancercandisadvantagepatientswithcomplexwiderneeds,asindividualcliniciansmaystruggletodelivereffectivetreatmentplanswithoutbreachingtargets43.8.Inongoingreviewsofcancerwaitingtimestargets,UKhealthservicesshouldconsiderwaystoensureoptimaltreatmentaccess,apositiveexperienceandbetteroutcomesforolderpeoplewithcancer.
THECANCERWORKFORCECOULDBETTERSUPPORTTHENEEDSOFOLDERPATIENTSCancerservicesintheUKareexperiencingsevereworkforcegapsacrossmanykeyprofessions,whichishavingarealimpactontheabilitytodiagnoseandtreatcancerquickly,aswellastogivepatientsthebestpossibleexperienceofcare44.Therearealsobroaderissuesrelatingtothepreparednessoftheworkforcetotreatthegrowingnumberofolderpatients,includingdeficitsineducation,knowledgeandattitudesandinthedevelopmentorspecificrolesandservicesthatmeetolderpeople’sneeds45.Forexample,a2013surveyofUKmedicaloncologytraineesfoundthatonly27.1%wereconfidentinassessingrisktomaketreatmentrecommendationsforolderpatients,comparedto81.4%beingconfidentabouttreatingyoungerpatients46.Forpeoplewithcomplexneeds,itiscriticalthathealthprofessionalswithspecialistexpertiseareavailabletosupportthemthroughouttreatmentdecision-makingandtreatmentitself.Thereisalsosomeevidenceofbenefitinprovidingadditionalspecialistsupport,targetedtogroupsofolderpeoplewithcomplexneeds,whoareatriskofundertreatment47.
Specialistcancernursesareaparticularlycriticalworkforcegroupforallpatients,actingasa‘keyworker’throughoutdiagnosis,treatmentdeliveryandpalliativecare.Patientsandhealthprofessionalspraisedthevalueofnursesconsistentlythroughoutthisresearch.
AdvancingCare,AdvancingYears 16
WhenIwasfirstdiagnosed7yearsagotherewasnoCNSinhaematologyatourlocal
hospitalanduntilIwasreferredelsewhere,Ididn'trealisetheseamazingnursesexisted.Fortunately,wehaveawonderfulCNSnowwhoisavailablebyphoneore-
mailwheneverneeded.(Cancerpatient,patientsurvey)The2015CancerStrategyforEnglandrecommendedthatallpatientsaregivenanamedClinicalNurseSpecialist(CNS)orkeyworkertocontact.Scotlandhavealsomadeastrategycommitmenttoputthenecessarylevelsoftraininginplacetoensurethatby2021,peoplewithcancerwhoneedithaveaccesstoaspecialistnurseduringandaftertheirtreatmentandcare.However,therearesignificantshortagesintheCNSworkforceacrosstheUK.WhilsttheproportionofpatientsinEnglandhavingaccesstoaCNShasrisenfrom84%in2010to90%in201648,thereisstillvariationacrossgeographiesandacrossdifferentcancersites.84%ofpatientsinScotlandreportedaccesstoaCNSin2015/1649;inWalesin2016,81%reportedaccessandinNorthernIrelandin2015,thisfigurewasjust72%.
Staffingissueswerealsorecognisedbynationalintervieweesforthisproject,particularlyforrarercancers.ThiswasechoedbyarecentcensusbyMacmillanCancerSupport,whichfoundthatupto15%ofcancernursingrolesinEnglandareunfilled,andthatthereiswidegeographicvariation50.Whilesupportingolderpatientsistheresponsibilityofallstaff–acrossprimary,secondaryandtertiarycare–thenursingworkforceisespeciallycrucialforthoseinhospitalcare,andsothismustbeaddressedasamatterofurgency.
Frequentlythere’sjustoneofthesenursesinateamandthereforeoncethey’reonholidayorthey’resickthere’snobackup,there’snothingelse,there’snobodyelsewho
canstepin.(NationalInterviewee)
Furthermore,theroleofaCNSishighlyvariable;theirjobtitlesandexpectationsareofteninconsistent.Becauseofwiderpressures,CNSsfrequentlyfillservicegapsintheirlocalcentres,ratherthandoingtheworkthatbestfitstheirexpertiseandtraining.AsurveyconductedaspartofCRUK’s2017researchintothenon-surgicaloncologytreatmentsworkforcefoundthat50%ofCNSsdidnotfeeltheyhadenoughpatient-facingtimeandwereconsistentlyworkinganaverageof5additionalhourseachweek–onaverage,15%oftheirworkinghours51.Geriatriciansarealsoimportantforthemedicalandsocialcareofolderpatients,howeverarenotalwaysinvolvedincancer-specificcare.Intervieweesinbothprimaryandsecondarycarenotedthevalueofrequestinggeriatricconsultantreviews–althoughfewMDTmembershaddonethisinpractice.Theroleofgeriatriciansincancercareshouldbeakeyconsiderationthroughoutallcancerworkforceplanning,andespeciallyinHealthEducationEngland’sphaseIIcancerworkforceplan.9.HealthEducationEngland,anditsequivalentsinthedevolvednations,shouldusetheCancerResearchUK‘bestpracticetreatmentmodel’toprojectrequiredworkforcenumbersbasedonpatientdemand,notonaffordability52.Organisationsshouldalsoincludeconsiderationofthespecificneedsofolderpeoplewithcancerinallfutureworkforceplans.
WENEEDTOIMPROVEHOWINNOVATIONREACHESOLDERPEOPLE
AdvancingCare,AdvancingYears 17
GETTINGTHERIGHTEVIDENCEResearchisthekeytoimprovingoutcomesforallpeopleaffectedbycancer.However,olderpatientsaretypicallyunder-representedinclinicaltrials53,whichcanhavestrictinclusioncriteriabasedonchronologicalage,comorbiditiesorcognitiveability.Thesefactorscombinedmeanthatthereisoftenrelativelylimitedevidenceonthespecificeffectsoftreatmentonthesepatients.Thismeansthatdecisionsabouttreatmentforpatientswithcomorbidities–andthereforeoftenolderpatients–cannotalwaysbebasedonstrongevidence.Atleast,notincomparisontodecisionsfortheiryoungerorotherwisefitcounterparts.
Themostimportantthingiswedon’thaveanyevidenceforsuchpatients…thenumberofpatientswhoare[in]clinicaltrialsabove75yearsofageisfarandfewbetweenandno
meaningfulconclusionscanbemadeonthat.(Medicaloncologist)
Morecouldstillbedonetogatherevidence,includingboostingnumbersofolderpatientsintrials–butalsodoingresearchthatenablespatientswithcomorbiditiesorfrailtytoreceiveoptimaltreatment,throughunderstandingtheinteractionsatplay.Thereisappetiteforchange:70%ofEuropeanhealthprofessionalsrespondingtothePREDICTstudyin2014didnotdidnotbelievethepresentarrangementsforclinicaltrialsrelatingtoolderpeopletobesatisfactory,and60%believedthateitherEuropeanornationalregulationofclinicaltrialsshouldbeamendedtoensuregreaterrepresentationofolderorlessfitpatients54.MostclinicaltrialsfundedbyCancerResearchUKdonothaveanupperagelimit,whenagelimitsareapplied,researchersareaskedtojustifytheboundaryselected.Exclusioncriteriarelatingtocomorbiditiesorpatientfitnessareusedinsometrialswheretheyriskconfoundingresultsoraddingasafetyrisk,however,andcomorbiditiesdoincreasewithage.CRUKalsofundsometrialsthataskspecificquestionsabouttreatmentforolderpatients,orpatientswhoarelessfit.Thequestionremainsabouthowbesttoensurethatthereissufficientevidenceofatreatment’sefficacyinpatientswhoarefrail,havecomorbiditiesorareelderly.Oneanswerisforresearcherstoidentifythepriorityquestionsforeachcancertype,andtoinvestigatetheseinclinicaltrials.
APPROVINGNEWTREATMENTS35%ofrespondentstooursurveyofMDTmembersfeltthatalackofclinicalevidenceabouttheefficacyoftreatmentinanolderpopulationwasabarriertotreatment.Thisisparticularlyproblematicincancerswherethereisapoorerunderstandingofthediseaseanditsprogression.Thiscanmakeitdifficultforclinicianstoassesstherisksoftreatmentandtoweighthatupagainstthepotentialbenefittothepatient.However,thisislikelypartofabroaderissueaboutevidenceincomorbidpopulations,ratherthanbeingrelatedsolelytochronologicalage.Thereisalsoscopeformakingchangestotheprocessofapprovingnewtreatmentssothatit
AdvancingCare,AdvancingYears 18
bettersupportsolderpeoplewithcancer,whomayvalueoutcomesotherthanjustimprovingsurvival–suchasmaintainingagoodqualityoflife,theirindependenceandcognition55.Forexample,nationaldrugapprovalsshouldconsiderincorporatingabroaderrangeofevidence,includingimpactonqualityoflife–whichwasrecommendedintheLifeSciencesIndustrialStrategy56,althoughtherecommendationswerenotspecificallytargetedtowardsolderpatients.Thereisalsobroaderscopeforincorporatingreal-worldevidence(RWE)ofadrug’seffectivenessinallpatients.Underthecurrentsystem,nationalapprovalbodies(suchasNICEinEnglandortheScottishMedicineConsortium)mustmaketheirdecisionatasinglepointintime–oftenbasedonarelativelynarrowscopeofevidence.Thepriceofthedrugisthenfixed,irrespectiveofhoweffectiveitprovestobeinroutineuse.WewouldliketoseebroaderuseofmanagedaccessschemeslikeEngland’sCancerDrugsFund,whichallowearlieraccesstoanewdrugwhilefurtherevidenceofitseffectivenessonallpatientsisgatheredintheNHS.ThisRWEisthencombinedwithclinicaltrialsdataandincorporatedintoafinaldecisionaboutapprovalandpricing.Inthelongerterm,weencourageUKhealthservicestoexploretheuseofflexiblepricingmechanismssuchasoutcomes-basedpricing,inwhichthepriceofadrugcanbereviewedatagreedstagesandaligneddirectlytopatientbenefit,beingincreasedordecreasedbasedonemergingnewdata.Thiswouldensurepricingandaccessdecisionsaregroundedintherealexperiencesofpatients.Totakethisforward,CancerResearchUKareexploringthefeasibilityofoutcomes-basedpricingthroughacommissionedresearchproject,inpartnershipwiththeGreaterManchesterHealthandSocialCarePartnership.
HIGH-QUALITYDATAAkeyenablertothisisrobust,routinelycollecteddataaboutcancertreatmentandoutcomes.Thisisnotanage-specificissueasitwouldsignificantlyimproveourabilitytounderstandtheeffectsoftreatmentonallpatients.AllUKorganisationsresponsibleforcollectinghealthdatashouldensuresignificantresourceisprovidedforimprovingthequalityandcompletenessoftreatmentsdatasets.Havingrobustdataabouttreatmentsandoutcomeswouldenablemorein-depthanalysesoftheextentofvariationinaccesstotreatmentandoutcomesforolderpatients,whichcouldsupplementclinicaltrialdataandsupporteffortstobenchmarkservices.10.Researchfundersshouldexplorehowtoensuremoreproportionaterecruitmentofolderpeoplewithcancerintoclinicaltrials,andhowtoensurethatresearchaddressesanyevidencegapsintheeffectivenessoftreatmentinolderpatients,orthosewithcomorbiditiesmorebroadly.
11.Nationaldrugappraisalbodiesshouldexplorewhatalternativemetricscouldbeconsideredduringappraisalsthatwouldbemorerelevanttoallpatients,includingolderpatients–suchasqualityoflifeandactivitiesofdailyliving.
AdvancingCare,AdvancingYears 19
1 .BACKGROUND1.1 OLDERPEOPLEWITHCANCERINTHEUKAround360,000peopleintheUKwerediagnosedwithcancerin2015.By2035thisnumbercouldreach500,000–mostlybecauseoftheageingpopulation,butalsopartlyduetolifestylechanges.
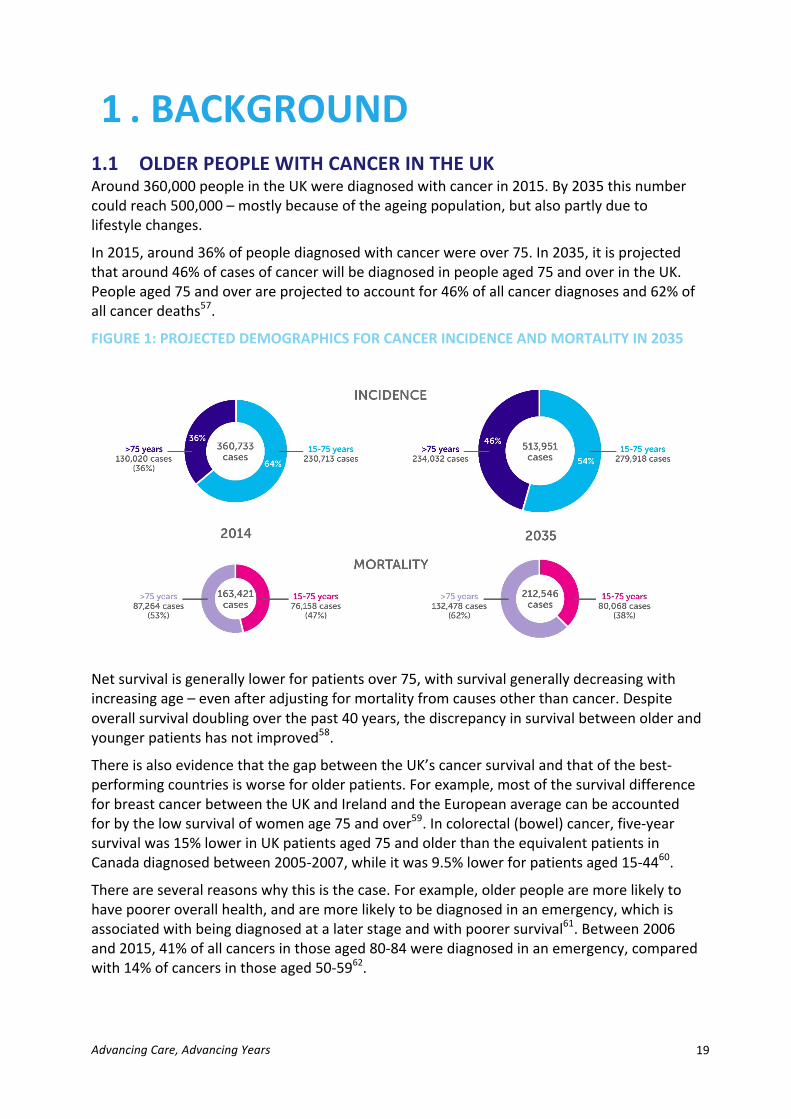
In2015,around36%ofpeoplediagnosedwithcancerwereover75.In2035,itisprojectedthataround46%ofcasesofcancerwillbediagnosedinpeopleaged75andoverintheUK.Peopleaged75andoverareprojectedtoaccountfor46%ofallcancerdiagnosesand62%ofallcancerdeaths57.
FIGURE1:PROJECTEDDEMOGRAPHICSFORCANCERINCIDENCEANDMORTALITYIN2035
Netsurvivalisgenerallylowerforpatientsover75,withsurvivalgenerallydecreasingwithincreasingage–evenafteradjustingformortalityfromcausesotherthancancer.Despiteoverallsurvivaldoublingoverthepast40years,thediscrepancyinsurvivalbetweenolderandyoungerpatientshasnotimproved58.
ThereisalsoevidencethatthegapbetweentheUK’scancersurvivalandthatofthebest-performingcountriesisworseforolderpatients.Forexample,mostofthesurvivaldifferenceforbreastcancerbetweentheUKandIrelandandtheEuropeanaveragecanbeaccountedforbythelowsurvivalofwomenage75andover59.Incolorectal(bowel)cancer,five-yearsurvivalwas15%lowerinUKpatientsaged75andolderthantheequivalentpatientsinCanadadiagnosedbetween2005-2007,whileitwas9.5%lowerforpatientsaged15-4460.
Thereareseveralreasonswhythisisthecase.Forexample,olderpeoplearemorelikelytohavepooreroverallhealth,andaremorelikelytobediagnosedinanemergency,whichisassociatedwithbeingdiagnosedatalaterstageandwithpoorersurvival61.Between2006and2015,41%ofallcancersinthoseaged80-84werediagnosedinanemergency,comparedwith14%ofcancersinthoseaged50-5962.
AdvancingCare,AdvancingYears 20
FIGURES2AND3:FIVE-YEARSURVIVALFORMENANDWOMENDIAGNOSEDBETWEEN2011AND2015
AdvancingCare,AdvancingYears 21
However,therearealsodiscrepanciesinaccesstotreatmentforolderpeoplewithcancer63.Forexample,arecentreportbytheNationalCancerInformationNetwork(NCIN)andCancerResearchUK(CRUK)foundthatacross20cancersites,olderpatientswerelesslikelytohavemajorsurgicalresections64.Otherstudieshavefoundsimilar;forexample,olderwomenwithbreastcancer65arelesslikelytoundergosurgery;theuseofradiotherapyalsograduallydecreaseswithage66.Olderpeoplewithlungcancerhavealsobeenshowntobefarlesslikelytoundergosurgery67.Thereisalsoevidencethatusageofchemotherapywithcurativeintentforlung68.69,70,breastandcolorectalcancer71,andasadjuvanttherapyforbreastcancer7273,declineswithage.
However,wemustbearinmindthatinsomecasestherearelegitimatereasonsforlowertreatmentratesinolderpopulations.Olderpatientsaremorelikelytohavemultiplehealthconditions,forexample,whichmayimpacttreatmenttoleranceandthereforethetreatmentoptionsthemselves74,75,76.
Somepatientsmayalsochoosenottopursuecurativetreatments,forvariousreasons.Recentresearchhasalsofoundthatwhenconsideringchemotherapy,overhalfofolderpatientssurveyedprioritisedoutcomesotherthansurvival,forexamplemaintainingtheirqualityoflife,independenceorcognition77.
Whilethiscanexplainsomefindings,somestudieshaveadjustedforthesefactorsandhavestillfoundvariation.Forexample,onestudyexaminingbreastcancersurgeryfoundthat‘inappropriateundertreatment’wasoccurringforwomenover8578,afteradjustingforhealthmeasuresandpatientpreferencesintreatmentdecisions.Similarly,asmallstudylookingattheuseofchemotherapyandbiologicaltreatmentinearly-stagebreastcancerfoundthatagewasamajorfactorinclinicaljudgement,irrespectiveofotherfactorssuchasageortumoursize79.
Giventhesedisparitiesinaccess,thisstudysoughttoidentifythebarriersthatolderpatientsfaceinaccessingtreatment,toexamineclinicaldecision-makingandrecommendsolutionsthatwouldensureolderpeoplewithcancercanaccesstherighttreatmentsforthem.
1.1 THISRESEARCHCancerResearchUKcommissionedanindependentresearchteamfromtheUniversityofBirmingham’sHealthServiceManagementCentreandICFInternationalforthisresearch.
Theaimoftheprojectwastounderstandclinicaldecision-makingforolderpeoplewithcanceracrosstheUKandtoidentifybarrierstooptimaldecision-making.
Thisreportpresentsevidencefromthefollowing:
- Areviewoftheliteraturerelevanttoclinicaldecision-makingforolderpeoplewithcancer
- Qualitativeinterviewswithnationaldecision-makers(n=15)- QualitativeinterviewswithhealthprofessionalsacrosseightUKsites(n=80)- Threesurveys:ofcancermultidisciplinaryteammembers,primarycareteam
membersandolderpeopleaffectedbycancer- Observationsofthreemultidisciplinaryteammeetingsandthreemultidisciplinary
clinics
ThereportpresentsthesefindingsalongsideadditionalCancerResearchUKpolicyresearchintoimprovingtheeffectivenessofcancermultidisciplinaryteams(MDTs)(“MeetingPatients’
AdvancingCare,AdvancingYears 22
Needs)andthenon-surgicaloncologyworkforce(“FullTeamAhead”).
FurtherdetailonthemethodologyisavailableinAppendix1.
1.2TREATMENTDECISION-MAKINGFOROLDERPEOPLEWITHCANCERThisresearchfocusedonunderstandingtheprocessofmakinganinitialtreatmentplanforolderpeoplewithcancer.
1.3THEROLEOFTHEMULTIDISCIPLINARYTEAMBeforebeginningtreatment,thevastmajorityofpatientsarediscussedatamultidisciplinaryteam(MDT)meeting.Inthismeeting,awiderangeofhealthprofessionalsmeettomakerecommendationsregardingpatients’treatmentandcare.MDTworkingisacentraltenetofcancerservicesandthe2015CancerStrategyforEnglanddescribedMDTsasthe‘goldstandard’forcancerpatientmanagement.However,recognisingthesignificantchallengesfacedbyMDTstoday,thestrategyalsomadeseveralrecommendationsforchange.ThemostrecentWelshcancerstrategyalsostatedthatMDTsremainthecornerstoneofpatientmanagementinsecondarycare,andsetouttheintentiontoenhancetheirroleasvehiclesforgovernanceandimprovement80.ArecentCancerResearchUKreportrecommendednewwaysofworkingformultidisciplinaryteammeetings,toallowmoretimefordiscussionofthemostcomplexpatients–includingolderpatients81.
UnderstandinghowthedifferentprofessionalgroupsperceiveMDTworkinganditsimpactondecision-makingisanareaacknowledgedasbeing‘underresearched’82,83.However,evidencesuggeststherearebenefitsofinvolvinggeriatriciansinMDTmeetings,tosupportdiscussionsofhowtreatmentsmightinteractwithcomorbiditiesandsubsequentsupportneeds84.
1.4GERIATRICASSESSMENTSGeriatricAssessments(CGAs)existtosupportcliniciansinmakingevidence-basedtreatmentdecisionsforolderpeople,byprovidingasystematicframeworkthatremovessomeofthesubjectivityinvolvedinassessinganolderpatient.Althoughtheseassessmentsvary,theymostofteninvolveassessingfunctionalstatusandcognition85.Anassessmentalsooftenincludesfatigue,comorbidity,cognition,mentalhealthstatus,socialsupport,nutritionandgeriatricsyndromes86.
Suchtoolsarealsoanimportantwayofensuringcareiscentredaroundthepatientandtheirindividualneeds.Patient-centredcareisacentralpillaroftheNHSConstitution,intheformoftheprinciple“nodecisionaboutmewithoutme”.
TheInternationalSocietyofGeriatricOncology(SIOG),theEuropeanSocietyofBreastCancerSpecialists(EUSOMA),theEuropeanOrganisationforResearchandTreatmentofCancer(EORTC)andtheUSNationalComprehensiveCancerNetwork(NCCN)nowrecommendtheuseofsomeformofgeriatricassessmenttohelpdeterminethebestcancertreatmentsforolderpatients,particularlyforwhomchemotherapyisconsidered.ACGAisnowthemostcommonlycitedandvalidatedexampleofageriatricassessment.
AdvancingCare,AdvancingYears 23
TheBritishGeriatricsSocietyhaveissuedagoodpracticedefinitionforCGAs:
Despitetheirwiderendorsement,CGAsarestillnotroutinelyusedinoncologyandthereisnostandardisedmethodforconductingCGAs87.Althoughthereisgeneralconsensusaboutwhichdomainsshouldbeassessed88,thereislittleconsensusonwhatconstitutesa‘comprehensive’assessmentorthemosteffectivemeasurementtools.
1.4.1ASSESSINGFRAILTYTheBritishGeriatricsSocietydefinesfrailtyasalong-termcondition;aclinicalstateofvulnerabilitycausedbydeclineofpsychologicalandphysicalreserves89.
Recognisingandassessingfrailtyisanessentialcomponentofeffectivecareforolderpeople.Recentyearshaveseenanincreaseininitiativesthataimtoimprovethequalityofcarebyaddressingthespecificneedsofpeoplewithfrailty.Forexample,theBritishGeriatricsocietyhaveworkedwithAgeUK,theRoyalCollegeofGeneralPractitionersandNHSEnglandtoprovidebestpracticeguidelinestomanagefrailtyinthecommunity(FitforFrailty)andspecialisedqualitychecklistsforpeoplewithfrailtyinacutesettings(Frailsafe).
MartinVernon,NationalDirectorforOlderPeopleandIntegratedCareatNHSEngland,hasarguedthatfrailtyshouldbetreatedasanyotherlong-termhealthcondition90.Thisisinlightoftheincreasingnumbersofpeoplewithfrailtyandthesystemiccostsofignoringtheimpactofthisonhospitalandcommunity-basedcare.Vernonseesbetteridentification,targetedassessmentandindividualcareplansasthefirststepstowardsavertingafrailtycrisisinhealthandsocialcare.Frailtydemandsawholesystemapproach,withVernon’srecommendationfocusingonuseoftheelectronicfrailtyindex(eFI)asstandardforroutinedataingeneralpractice.
TheIndependentCancerTaskforcealsohighlightedinteractionsbetweenfrailtyandcancer,aswellastheimportantroleoffrailtyassessmentsandCGAsininformingtreatment
Comprehensivegeriatricassessment(CGA)isamultidimensionalandusuallyinterdisciplinarydiagnosticprocessdesignedtodetermineafrailolderperson’smedicalconditions,mentalhealth,functionalcapacityandsocialcircumstances.Thepurposeistoplanandcarryoutaholisticplanfortreatment,rehabilitation,supportandlongtermfollowup.CGAispartofanintegratedapproachtoassessmentbasedonthefollowingprinciples:
• Theolderpersoniscentraltotheprocess.• Theircapacitytoparticipatevoluntarilymustbeassessed,andiflacking,then
thereneedsbeasystemtoaddresstheirneedsinanethicalfashion.• Linksbetweensocialandhealthcareshouldbegoodenoughforolderpeople
whoneedcomprehensiveassessmenttoreceiveitinatimelyandefficientmanner,andproportionatetotheirdegreeofneed.
• Assessmentsshouldbestandardisedandcarriedouttoareliablestandard.• Circumstanceswhichwarrantacomprehensiveassessmentinclude,among
others:o Acuteillnessassociatedwithsignificantchangeinfunctionalabilityo Transfersofcareforrehabilitation/re-enablementorcontinuingcareo Afrailpatientpriortosurgeryorexperiencingtwoormore“geriatric
syndromes”offalls,delirium,incontinenceorimmobility.

AdvancingCare,AdvancingYears 24
recommendationsandidentifyingadditionalsupportneeds.
1.4.2COMPREHENSIVEGERIATRICASSESSMENTSINONCOLOGYAtpresentthereisnoclearevidenceregardingthebesttooltouseforCGAsinoncology,orhowoncologyoutcomesareimprovedthroughusingCGAs91.
Overall,thereisrelativelylittlestrongevidenceabouttheimpactofCGAsoncancertreatmentdecisions.Forexample,threesystematicreviewslookingattheusageofCGAsinoncologyhaveconcludedthatthequalityofstudiesonimpactaregenerallypoortomoderate92andtherehasnotbeenanyrandomisedcontroltrialexaminingtheeffectivenessofCGAsinchangingtreatmentplans,orimprovingoveralloutcomesforolderpeoplewithcancer.However,therearesomepromisingfindingsabouttheimpactofCGAs:
- SeveralstudieshavefoundthatCGAsofteninfluencetreatmentdecisions,howevertheproportionofdecisionsimpactedisdisputed93.Onestudyconductedin2013foundthatCGAsidentifiedpreviouslyunknownissuesin51%ofthestudypopulation,whichresultedinchangestotreatmentdecisionsfor25%ofpatientsanddeterminedinterventionplansfor26%ofpatients94.However,nofollowupwasdonetounderstandtheextenttowhichthesedecisionsimpactedeventualoutcomes.
- ThereisevidencetosuggestthatCGAs–andspecificaspectsofCGAs,suchasfrailtyorperformancestatus–havepredictivevalueforchemotherapytoxicity95.
- KalsietalconcludedthatolderpatientsundergoingaCGAweremorelikelytocompletechemotherapyandfewerhadchangesmadetotheirtreatmentplans,asinterventionscouldbemadethataddressedapatient’swiderneeds,forexamplemanagingexistingconditionsorprovidingadditionalmedicalorsocialsupport46.Theauthorsrecommendedthat‘standardoncologycareshouldshifttowardsmodifyingcoexistingconditionstooptimisechemotherapyoutcomesforolderpeople’.
- Hamakeretal’ssystematicreviewin2012foundalinkbetweenCGAresultsandthelikelihoodofperioperativecomplications85.
AdvancingCare,AdvancingYears 25
TheMacmillanSCOPESproject(SystematicCareforOlderPeopleinElectiveSurgery)isaparticularlyinterestingcasestudy96.
AlthoughseveralorganisationshaveproducedguidelinesonconductingCGAsincancer3,theuseoftheseishighlyvariableacrosscountriesandcentres.Thisisoftenbecauseofalackofstaff,aswellasotherinstitutionaland/orfundingconstraints97.
Furthermore,oftenthetoolsthatarefamiliartogeriatriciansarenotusedbyoncologists,arenotfitforthespecificassessmentofolderpeoplewithcanceroraretoolongandcumbersometobeusedineverydayclinicalpractice98.Becauseofthislackofstandardisation,O’Donovanetal.arguethat‘…geriatricassessmenthasyettobeoptimallyintegratedintothefieldofoncologyinmostcountries’99.
ThisreportwilldiscusstheusageofCGAsintheassessmentofolderpeoplewithcanceracrosstheUK,gatheringviewsontheirutilityfromhealthprofessionals.
3NCCN,SIOG,EUSOMAandEORTC
SystematicCareforOlderPeopleinElectiveSurgery(SCOPES)
ThisprojectwasdevelopedatNottinghamUniversityHospitalsNHSTrustin2010forlowerlimbjointreplacementsurgery,butwaslaterextendedtouppergastrointestinalcancersurgery.
Anoutpatientclinicisheldonceaweek,involvingarangeofhealthprofessionals–includinggeriatricians,specialistnurses,dieticiansandsocialworkers.ACGAisundertakeninonevisit,withtheresultsfedbacktotheupperGIcancerMDT.
Patientscanthenreceiveadditionalsupportorclinicalinterventionstooptimisetheirfitnessbeforesurgery.TheSCOPESteamcanalsohelpcoordinatesocialcare,eitherforthepatientthemselvesoralovedonewhoisusuallycaredforbythepatient.Thisapproachhasresultedinanumberofpositiveresultsincludingreducinglengthofstay.
…atthemomentwe’relookingatareductionofapproximately28daysdownto16[inhousecalculations]nowalotofthatwillbeITU[IntensiveTreatmentUnit]care
becausethepurposeofwhatwedoistooptimisepatientstogetthroughwhateverthey’rehavingsoifwe’veoptimisedthemitmeanslesstimeintermsofcareorHDU
[HighDependencyUnit]whichmeanslesstimeinhospitalbecauseofbuildinguptheirfitnesswecangetthemhomebecausewe’vegottheirpackagesorganisedforthemtheydon’thavetowaitonawardblockingabed.(SCOPESProjectManager)
Recentevaluation–aprospectivecohortstudy–aimedtoexaminetheeffectoftheCGAoncancerMDTdecision-makingandclinicaloutcomes.ThisfoundthatsignificantlymorepatientsintheCGAgroup(33%)receivedpotentiallycurativesurgerythaninthecontrolgroup(18.2%).Six-monthmortalitywassignificantlylowerinthecontrolgroup(30.9%vs48.5%).OtheroutcomesweremoreconsistentbetweenCGAandcontrolgroups,forexamplepalliativetreatmentdecisions,post-operativelengthofstayandtotaluseofacutecare.Thishighlightshowdietary,occupationaltherapyandphysiotherapyreviewscandirectlycontributetotreatmentoptimisation.
AdvancingCare,AdvancingYears 26
1.5 SHAREDDECISION-MAKINGTheconceptofshareddecision-making(SDM)originatedinthedisabilityrightsmovement,expressedthroughthephrase‘nothingaboutme,withoutme’.Ithassinceplayedanincreasingroleinshapinghealthandcarepolicy,bothintheUKandinternationally,with‘person-centredcare’morerecentlyattheforefrontofNHSEngland’sFiveYearForwardView.TheNationalInstituteforHealthandCareExcellence(NICE)haveconvenedaSharedDecision-MakingCollaborative,havepublishedanactionplan100andhaveupdatedtheirprocessesfordevelopingguidancesothatshareddecision-makingisakeyconsideration.
Despitethiswidespreadsupportfortheprincipleofshareddecision-making,thereisstillnouniversallyagreeddefinition.ForthepurposesofthisreportwewillusethedefinitionadoptedbytheHealthFoundationandNICE:
‘aprocessinwhichcliniciansandpatientsworktogethertoselecttests,treatments,management,orsupportpackages,basedonclinicalevidenceandpatients’informedpreferences.Itinvolvestheprovisionofevidence-basedinformationaboutoptions,outcomesanduncertainties,togetherwithdecisionsupportcounsellingandsystemsforrecordingandimplementingpatients’treatmentpreferences.’101
Peoplewhoparticipateindecisionsabouttheircarearemorelikelytobesatisfiedwiththeircare102.ThereisalsostrongevidencethatSDMcanimprovepatients’self-efficacy,whichcaninturnhaveasignificantimpactonbehaviours103.Thereislimitedevidencethattheseimprovementsinself-efficacycan,inturn,impactqualityoflifeandclinicaloutcomes.Thisisbecauseindividualshavecarewhichfitsbetterwiththeirlifestyles104;moreinvolvementindecision-makingmayalsoincreasethechancethatindividualsadheretotheirmedication105.
However,individualcharacteristicswillaffecthowwillingorablethatpersonistoengageinSDM.Forexample,aperson’sattitudes,opinionsandlifeexperience,self-efficacy,activationandhealthliteracy,socioeconomicanddemographicstatusareallrelevantfactors.Whenpeoplehavelowhealthliteracy,self-efficacyoractivation,theymaylacktheconfidence,understandingorrecognitiontotakeanactiveroleindecisionsabouttheircare106.
1.5.1 SHAREDDECISION-MAKINGINCANCERSDM,particularlytheuseofdecisionaids,hasbeenrelativelyprominentincancercarecomparedtootherconditions.Thisispartlybecauseofthesheernumberofdecisionscancerpatientsarefacedwiththroughouttheirdiagnosisandtreatment,fromparticipatinginscreeningthroughtotreatmentoptions.
Thereisstrongevidencethatshareddecision-makingisbeneficialtocancerpatients.Forexample,the2015CanCORSstudyfoundthatwhenpatientsreportengaginginshareddecisionstheymoreoftenreportedexcellentqualitycareandgoodcommunicationfromtheirphysicians.Importantly,thisassociationheldregardlessofwhethertheindividualstatedaninitialpreferencetomakeshareddecisions107.
Theremayalsobevariationbycancersite;forexamplethereisevidencethatpatientswithprostateandbreastcanceraremostlikelytowanttobeinvolvedindecisionscomparedtothosewithcolorectal,gynaecologicalorlungcancers.However,theevidenceonthisislimitedandcross-cutbyothervariablesthatmightaffectengagement–suchasgender,ageanddiseaseseverity108.
AdvancingCare,AdvancingYears 27
1.5.2 SHAREDDECISION-MAKINGFOROLDERPATIENTSOlderpeoplewithcancerfaceaparticularsetofchallengeswhichmaymakeSDMmoredifficult.Atthesametime,thesechallengesmaketheprincipleofSDMevermoreimportant.Forexampletheymaybemorelikelytodefertoauthority,tobelievethatcliniciansshouldnotbequestioned,orthinktheylackthestatustodecideforthemselves109.
Whencancerformsjustoneaspectofanolderperson’smultipleconditions,decisionsbecomemorecomplexandarenotjustbasedonclinicalevidence110,111,112.Forolderpeoplewhoareexperiencingcognitiveimpairment,thedifferentoptionscanbeparticularlychallengingtounderstandandnavigate.
Inthetime-limitedcontextoftreatmentdecision-making,healthprofessionalscanperceivethisstruggletoengageinaconversationasalackofcompetence113,114,115.Thesocialandpracticalcontextofmanyolderpeople’slivescanalsoaddcomplexitytotreatmentdecisions.Inparticular,isolationorcaringcommitmentstoothersmaylimitolderpeople’sengagementintheirowntreatmentorpresentpracticalchallenges116.
Treatmentdecisionsarealsomorelikelytobemorecomplexforolderpatients.Olderpeople,moresothanyoungerpeople,mayneedtonotonlyconsiderthepotentialbenefitsofatreatmentoption,butalsoconsidertheirownlifeexpectancy,andtheeffectofanyoftheirotherconditions.Theymustbalancedecisionsaboutthequalityoflifetheywanttolead,againstthelengthoftimetheywanttolivefor.Thisisnotonlyahighlycomplexmedicalproblem,withanalmostimpossibletopredict‘right’answer,butachallengingemotionaldecision117.
Thiscomplexityiscompoundedbythefactthattheevidenceavailabletobothhealthprofessionsandpatientsonthepotentialimpactandsideeffectsofanytreatmentissignificantlylessthanforyoungerpeople,partlyaresultoftherebeingfewerolderpeople,andpeoplewithcomorbidities,inclinicaltrials118,119.
1.5.3 THEROLEOFFAMILYMEMBERSINSHAREDDECISION-MAKINGFamilymembersandcarersoftenplayakeyroleinprovidingcareforpeoplewithcancer,particularlyforolderpatients.Whenitworkswell,thereissomeevidencethatsharingdecisionsleadstogreaterpatientsatisfaction,bettertreatmentadherence,andallowsfamilymemberstoactaspatientadvocates,demandingthebestcarefortheirfamilymember120,121.
However,issuescanarisewheretherearediscordantviews.Thiscanbecommon,particularlywhenpatientsareolder,caregiversarelesseducatedorthepatient-caregiverrelationshipisparent-childratherthanspouse-patient122.Qualitativeresearchsuggeststhatthiscanbeparticularlydifficultwhendecisionsmustbemadeaboutswitchingfromcurativetopalliativetreatment:familymemberscanbelesswillingtostopactivetreatment,evenwhenitiscausingsevereside-effects.Patientsthemselvesareoftenreadiertoacceptandrecognisethattheyareseriouslyillthanfamilymembersare123.
1.5.4 THEROLEOFHEALTHPROFESSIONALSINSHAREDDECISION-MAKING
Thebehavioursandattitudesofhealthprofessionalshaveasignificantimpactonpatients’abilitytoengageinSDM.HealthprofessionaltrainingisthereforekeytoimplementingSDM:itcanovercomebarrierstoengagingwithhealthprofessionals,forexampleanyfalselyheld
AdvancingCare,AdvancingYears 28
beliefsthattheyalreadyworkinaperson-centredwayorbeliefsonthevalueand‘cost’ofensuringSDM.
Healthprofessionalsoftenunderestimatehowmuchpatientswanttobeinvolvedindecisionsabouttheircareandmakeassumptionsabouttheirskillsorabilitytodoso.Forexample,onestudyfoundthathealthprofessionalsthoughtpatientswerefarmorelikelytonottakepartinbowelcancerscreeningthantheyactuallywere124.
Similarly,healthprofessionalsmayassumethatcertaingroupsofolderpatientsarelessabletoengageindecisions125.Thisisproblematic,asthereisoftensignificantvariationwithingroups126.Secondly,aspreviouslynoted,individualsmayappearunwillingtoengageinSDMbutthismaybebecausetheycan’t,ratherthantheywon’t127–andthereforehealthprofessionalsshouldtryandsupportpatientstoparticipateinSDM,wherepossible.
1.5.5 THEROLEOFTHEHEALTHSERVICEINSHAREDDECISION-MAKING
ArangeoforganisationalandsystemicfactorsaffecttheavailabilityandimpactofSDM.Theseincludeseniorsupportandcommitment,alignmentwithwideragendas,ITsystemsandsupportcapacityandsupportivecommissioningandpaymentsystems.Ifthesefactorsareinplace,thesystemhasminimalbarrierstoSDMandincludesincentivesthatencouragepatientsandclinicianstotakepart.
Underlyingthis,theremustbesufficienttimeandintegrationtoallowmeaningfulSDM.AlackofintegrationbetweenhealthservicescanbeafurtherbarriertoSDM,andparticularlyincancerwhereindividualsareincreasinglylivinglong-term,withandbeyondcancer.Forthesepeople,careshiftsbetweenprimary,secondary,communityandsocialcare–andinformationalltoooftendoesnotflowbetweenthoseservices.Iftherearebreaksincare,patientscanfeelignored,demeanedandinsulted128.
AlackoftimeisalsoacommonbarriertoensuringSDM;cliniciansoftenperceiveSDMasmoretime-consumingthan‘usual’care,andthereissomeevidencethatthisistrue.ThismakeshealthprofessionalslesswillingtouseSDM,particularlywhenthetimeavailableforconsultationsisshort.Patientsalsoreportthatshortconsultationtimeslimittheirabilitytobeinformed,toreflectontheinformationreceivedandtoaskquestions.Thisisfeltparticularlyacutelyinthecontextofcurrentpressuresoncancerservices:patientsaresensitivetoclinicians’highworkloadsandareconsciousnotto‘takeuptheirtime’129.Thesepressuresparticularlyaffectolderpatients,whoaremorelikelytorequiremoretimetoprocessinformationandthinkthroughoptions.
1.6 THEPOLICYLANDSCAPEAllUKnationsrecognisethatcancerispredominantlyadiseaseofolderageandthattheageingpopulationpreventsfuturechallengestothehealthservice.However,giventhathealthisadevolvedissue,eachnationtakesadifferentapproachtotacklingthespecificchallengesofolderpeoplewithcancer.
1.6.1ENGLAND
The2015CancerStrategyforEngland,‘AchievingWorld-ClassCancerOutcomes:astrategyforcancer’,givesthemostexplicitattentiontoolderpeoplewithcancer130.Thestrategy
AdvancingCare,AdvancingYears 29
highlightsthatcurrentassessmentmethodsarenotfitforpurpose,whichcanresultinolderpeople’sneedsnotbeingidentifiedorsufficientlywell-understood.Italsohighlightstheroleofspecialistgeriatriciansinorthopaedicsasapositiveexample,transformingtheapproachtohipfractures,andidentifiesthattheremaybesimilaropportunitiesincancer.Thestrategymakestworecommendationstargetedtowardsolderpeoplewithcancer:
Recommendation41:NHSEngland,theTrustDevelopmentAuthorityandMonitorshouldpilotacomprehensivecarepathwayforolderpatients(aged75andoverinthefirstinstance).Thispathwayshouldincorporateaninitialelectronichealthneedsassessment,followedbyafrailtyassessment,andthenamorecomprehensivegeriatricneedsassessmentifappropriate.ThepilotshouldevaluateamodelinwhichtheoutputsoftheseassessmentsareconsideredbytheMDTinthepresenceofageriatrician,whowouldadviseonAHPneeds,co-morbiditiesetc.,andtheirimplicationsfortreatmentandemotionalandphysicalsupport.
Recommendation42:NHSEnglandshouldaskNIHRandresearchcharitiestodevelopresearchprotocolswhichenableabetterunderstandingofhowoutcomesforolderpeoplecouldbeimproved.
TheNationalCancerInformationNetwork(NCIN)hasalsoinvestigatedthespecificcharacteristicsofolderpeoplewithcancer;thekeymessagesfromtheir2015reporthaveunderpinnedthisreport131.Thereportsurmisesthatassessmentsarethekeytoensuringthatolderpeopleareofferedthebesttreatmentandthattheyarenotexcludedonthebasisofagealone.Theimportanceofevidence-based,systematicmechanismsofformulatingtreatmentrecommendationsiscentralwhenactingtoavoidtreatmentdecisionsbeingmadesolelyonage,withimplicitassumptionsoffrailty.Effectiveprevention,earlierdiagnosis,enhancedsupport(especiallyinthecommunity)andincreasedinvolvementinresearchareseenasothermajorprioritiesforimprovingolderpeople’soutcomes.
Morebroadly,NHSEngland’sFiveYearForwardView,publishedin2014,alsofocusesonolderpeople132.Thishastranslatedintosettingaresearchpriorityforunderstandingoutcomesforolderpeoplewithcancer,andpilotingacomprehensivecarepathwayforolderpatients.
1.6.2SCOTLAND
ThemostrecentcancerstrategyinScotlandis‘Beatingcancer:ambitionandaction’,publishedin2016133.Thestrategyhighlightstheincreasingnumberofolderpeopleandthe(related)growthinlong-termconditions,drawingattentiontonecessaryimprovementsinpreventionanddiagnosistomitigateincreaseddemandsonservices.Engagementwithpeopleofallagesisdescribedaskeytospreadingawarenessofcancersymptomsandultimatelyimprovingdetectionofcancerintheolderpopulation134,howeverthereisnospecificsectiononthetreatmentandcareofolderpatients.
1.6.2WALES
TheCancerDeliveryPlanforWales,publishedin2016,focusesoninequalitieswithintheolderpopulation135.TacklinghealthinequalitiesareseenasapriorityforWelshhealthpolicy,strategyandgovernance.Solutionsfocusontheimportanceoflocalisedapproachesandinvolvementofpartnersinpublichealthandthethirdsector,howeverthereisnospecificfocusonolderpeoplewithcancer.
AdvancingCare,AdvancingYears 30
1.6.2NORTHERNIRELAND
NorthernIrelanddoesnotcurrentlyhaveacancerstrategyandsoitisdifficulttoascertaintheextenttowhichthereisastrategicfocusontheneedsofolderpeoplewithcancer.However,wedoknowthatthereisaparticularinterestinruralisolationandtherelatedtransportissues.TheNorthernIrelandAssemblycancerservicesresearchandinformationbriefingsdirectlychallengetheconsequencesofservicecentralisationonthesegrounds136.
2 OLDERPATIENTSHAVEMORECOMPLEXCARENEEDS–ANDTHESYSTEMISNOTSETUPTODEALWITHTHEM
Olderpeoplewithcanceraremorelikelytohavecomplexmedicalandsocialneeds,andthereforemayrequireadditionalsupporttoaccesstreatment.Forexample,olderpatientsaremorelikelytohaveotherage-relatedillnesses,butalsomorelikelytorequiresocialcaresupport.Thesefactorsmakeitevermoreimportanttoensurethatdecision-makingisshapedaroundeachindividualpatient’scircumstances–andmorecouldbedonetoensurethatthisisalwaysthecase.
2.1 CLINICALFACTORSOlderpeoplehaveanincreasedprevalenceofage-relatedcomorbiditiessuchasdiabetes,hypotension,atheroscleroticdisease,chronicrespiratorydisease,arthritisandcognitiveissues137.Cognitiveissuescanposeaparticularchallenge;upto40%ofolderpatientspresentwithcognitiveissuesthatimpairtheircapacitytomakecomplexdecisionsabouttreatment,adheretotreatmentplansandrecognisesymptomsoftoxicitythatmightrequiremedicalattention138.
Thesefactorscombinedleadtodifficultdecisionsforcliniciansformingtreatmentplansforolderpatients.Aswellastreatmentefficacy,cliniciansmustalsoconsidertheimpactofatreatmentregimeonthepatient’squalityoflifeandtheirlikelihoodtoadheretoatreatmentregimen,interactionswithmultiplecomorbiditiesandthelikelihoodofthepatient’sconditiondeterioratingduringtreatmentbecauseofapre-existingcondition.
AdvancingCare,AdvancingYears 31
Ourthematicanalysisofallsurveyandcasestudymaterial,asidefromresponsesfromprimarycare,hasidentifiedfourmainclinicalfactorswhichwoulddeterminewhattreatmentanolderpatientmayreceive:
1. Thepatient’sfitnesstowithstandtherigoursoftreatment;2. Thelikelihoodthatthepatientwilldiefromacauseotherthantheircancer;3. Whetherthepatienthasco-morbidities;4. Ifthereisclinicalevidencetosupportaparticularcourseoftreatmentinanolder
patient
2.1.1 PATIENTFITNESSWherecliniciansareconcernedaboutaperson’sfitnesstowithstandtreatment,theywilloftenworkwiththepatienttooptimisetheirtreatmentoptions–oftenreferredtoas“pre-habilitation”.Forexample,theymightfocusonimprovingtheperson’sfitnessbeforesurgery,ortheycouldstartwithalowerdoseofchemotherapytocheckhowthepersonrespondstotoxicity.However,intervieweesrecognisedthatthiscouldrequireolderpatientstoundergomoreinvestigationstochecktheirfitness.Thiscanbechallengingtodowhilestillmeetingnationaltargets,astheseinterventionstakemoretime.Thishasbeenechoedinresearch,whichhasfoundthatservicetargetsthatfocusresourcesolelyoncancercandisadvantagepatientswithcomplexwiderneeds,asindividualcliniciansmaystruggletodelivereffectivetreatmentplanswithoutbreachingtargets139.
Thisisparticularlyrelevantforolderpeoplewithlungcancer,whooftenhaveparticularlycomplexneeds:manyareelderlyandcanhaverelatedcomorbiditiessuchascardiovasculardisease,vasculardisease,ChronicObstructivePulmonaryDisease(COPD)andlungdisease.Inthiscase,eveniftheindividualhasacurablecancer,theirtreatmentoptionscanbelimitedsincethepatientissimplytoounwelltocopewithextensivediagnostictestsandtreatment.
Wehavealotofpatientsthatcan’tgetthroughtests,becauseyouknowthey’vehadbleedingissuesfromtheircancerorthey’vegotpoorlungfunctiontest[results],theycan’tdoaneedlebiopsy.Ortheybledatbronchoscopy…Ortheyhaveastairtestand
theyonlymanagetwoflights.…Orthey’vegotlungfibrosissoIcan’tgivethemradiationofacurativetype.(Clinicaloncologist)
Thephysicalmobilityofapatientcanalsolimitoptions,includingintermsofdiagnostictests.
Soifapatientisunabletoelevatetheirarmthatmeanstheywouldn’tbeabletohaveradiotherapy…ifIcan’televatetheirarmthechancesareIwon’tformallyassessthe
axilla[armpit].(Radiologist)
However,cliniciansalsoreportedworkingaroundtheselimitationstoprovidethebestpossiblecareinthecircumstances.
…wecan’tworkthemupaswellaswewouldsomebodyyoungerbecausethey’renotphysicallyfitenoughtohavemammogramssay,butIwilloftenandmycolleagueswill
oftendoabiopsywiththemsaysittingintheirwheelchairsothatwecangetthehormonereceptivestatusandtreatmentwithchemotherapeuticagentssuchas
Tamoxifen,withouttheneedformoreinvasivetests.(Radiologist)
Anumberofintervieweesfromcasestudysiteswithaparticularlyelderlydemographic
AdvancingCare,AdvancingYears 32
mentionedtheirexperiencesofhaving‘pushedtheboundaries’ofwhatmightbeconsidered‘usualpractice’whenitcomestoolderpatients.
Andwehavehadsomesituations,elderlypatients,wherethey’renotfitenoughforageneral[anaesthetic].Wewouldn’tdoanauxiliaryclearanceforexampleunderalocal,but
wehavedonemastectomiesandwidelocalexcisionsunderlocalanaesthetic.(CancerNurseSpecialist)
Anaesthetistscanmakeasignificantcontributiontowardsoptimisingapatient’soptionsfortreatmentandthoseinterviewedforthestudyreporteddrawingonarangeofresourcesandexpertisetofacilitatethis.Thismightinvolveareferralbacktothepatient’sGPtooptimisesomeone’sinhaleruse,administeringironpre-operatively,oraskingcardiologiststoadjustsomeone’smedicationtoimprovecardiacoutput.
2.1.2 COMORBIDITIESANDPOLYPHARMACYOlderpeoplewithcanceraremorelikelytohaveotherpre-existinghealthconditions.Aswellasimplicatingapotentialtreatmentplan,thisalsomeansthattheyaremorelikelytodiefromsomethingotherthantheircancercomparedtoyoungerpatients140.Thiscancomplicatetreatmentdecision-making,sinceside-effectsofcancertreatmentcouldhaveasignificantnegativeeffect–ashighlightedbyanintervieweeforthisresearch.
Inelderlypatientswithsmallrenalmassesweare…morelikelytoadoptaconservativeapproachwherewewillmonitorthegrowthofthattumourbeforemakingadecisiontotreat,becauseifitturnsouttobeessentiallysessiletumourmassthatisnot
growing,thenthatpatientisprobablynevergoingtorunintobotherwiththattumourfortheremainderoftheirnaturallifeexpectancy.(Medicaloncologist)
Itcanalsobedifficulttocontrolforpossibleinteractionsbetweenmultiplemedications,whichisknownaspolypharmacy.Patientsandclinicianscanbefacedwithatrade-offbetweenmaintainingadrugregimethatcontrolstheirotherconditionsandpossiblydisruptingthattoreceivecancertreatments.Thiscanbethecaseforbothmentalhealthconditionsandphysicalhealthconditions.
2.1.3 CLINICALEVIDENCEAswillbediscussedfurtherinsection6,thereisoftenrelativelylimitedevidencetosupporttheuseofnewtreatmentsinanolderpopulation,sinceolderpatientsareunder-representedinclinicaltrials.
Thisisanimportantissue:aswellasbeingmorelikelytohavecomorbiditiesandtobeonothermedication,olderpatientscanalsohavebiologicaldifferencesthatcanimpacttreatmentefficacy.Aperson’schronologicalagecanhaveasignificanteffectontheirresponsetomedication.Forexample,age-relatedchangesinliver,kidneyandgutfunctionsignificantlyimpacthowdrugsareabsorbed,distributedaroundthebody,metabolisedandexcreted141.
2.2 SOCIALFACTORSSocialfactorscanhaveasignificanteffectonhowpeopleviewtheirownhealthand
AdvancingCare,AdvancingYears 33
treatmentoptions,particularlyifpatientsmusttravelasignificantdistancetoreceivetheirtreatment.
Thisresearchhashighlightedarangeofpotentialbarrierstoolderpeopleaccessingtreatmentortomakingadecisionthatisrightforthem.Somebarriersrelatetopracticalissues,whereasothersconcernattitudesorbeliefs.Itwasalsonotedthattheextenttowhichthesebarrierscouldberemovedvariessignificantly.
2.2.1 COGNITIVEIMPAIRMENTHealthcareprofessionalsfindthattreatmentdiscussionsareparticularlychallengingwhenpatientshavecognitiveimpairments.Cliniciansareoftenreliantonthepatient’sownassessmentoftheirabilities,whichmaybeinaccurate.Patientsmayalsooverestimatetheiractivitylevels,perhapsfromasenseofdenialofphysicaldecline,orfromadesiretoconvincetheclinicianthattheyarefitforsurgery.Intheseinstances,theinvolvementoffamilymembersorcarersisoftencritical.Dementiaaffects810,000adultsover65intheUKandjust40,000peopleundertheageof65142.Dementiahasahugeimpactondecision-makingingeneral,butparticularlyonsecuringpatientconsentfortreatment,sincememoryproblemscanimpactapatient’sabilitytoretaininformationandmakeaninformeddecision.Ifanindividualhassignificantmentalimpairmentsandisunabletounderstandtheoptionsoutlinedtothem,pursuingactiveor‘conventional’treatmentoptionscanbedifficult.Thisispartlybecausepatientsmaybeunabletorecognisenegativeside-effectsorcomplicationsoftreatment.However,throughourinterviewsweheardsomedoubtabouthowitcanbedifficulttoidentifypatientswithdementiaiftheydonotyethaveaformaldiagnosisandtheprogressionoftheirdiseaseismild.Furthermore,itisunclearhowpatientswithmoreseveredementiaareidentifiedandflaggedtotheMDTmanagingtheircare–aswillbediscussedlaterinthisreport.Othercognitiveissuescanalsohaveanimpactontreatments.Forexample,olderpatientswhohavesufferedastrokeorotherbraininjurymayhavedifficultyretaininginformationandmakingcomplexdecisions.Thisgivesfurtherweighttothecaseformorewidelyusedrobusttoolsthatcanfactortheseissuesintodecision-makinginaconsistentandrobustway.
2.2.2 SOCIALSUPPORTNEEDSFormanyolderpeoplewithcancer,theirwidersocialsituationhasasignificantimpactontreatmentdecisions.Forexample,patientsmayhavecaringresponsibilitiesormaythemselvesneedadditionalsocialsupport.Alackoffamilyorcarersupportcanbeaconcernforcliniciansmakingrecommendations,sinceitcanincreasethepatient’sriskofpost-treatmentcomplicationsandmakeithardertopursueactive,ongoingtreatment.Thisisparticularlythecaseforchemotherapy.
Iusechemotherapytotreatcancersandoneoftheimportantcriteriaistotheabilitytobesupportedandtheabilitytoseekhelpifthereisanyadverseeventsortoxicities…the
patientneedstobe…cluedintoseekhelpand…weknowpeoplecopewelliftheyaresupportedfromthefamilyandgiventhedensityofsomeofthechemotherapy.Idotakea
verycautiousviewifthepatientdoesnothaveanyadequatesocialfamilysupport.(Medical

AdvancingCare,AdvancingYears 34
oncologist)
46%ofMDTmemberssurveyedforthisresearchidentifiedthelackofsocialorpracticalsupportasabarriertoolderpeopleaccessingthemosteffectivetreatmentfortheircancer.Thiswasechoedbypatientsinvolvedinthestudy,whofeltstronglythatalackofcertaintyabouthowtheywillaccessnon-medicalsupportwasasignificantbarriertoaccessingtreatment.Thisfearwasoftenheightenedbypublicreportsoffinancialpressuresonthewiderhealthandcaresystem.
It’sonethingtochoosetodeclinetreatment,becausetheeffortofchemotherapyandhowillit’sgoingtomakeyoufeelisn’tworth(it)…It’sverydifferenttomakingadecisionbasedon‘Ican’tgetthecareformyhusbandorIcan’tgetthecareformywifeorIdon’thavetransporttogettothechemotherapy…OrI’llfeeltoorubbishafterwardsandthere’snobodyaroundtodomycookingandcleaning’….(Nationalinterviewee)
Reassuranceofdomiciliarycare,adaptationsanddevices,self-careadvice(physiotherapyanddiet),carerbenefitsandrespitewerealsodescribedasfactorsthatmighthaveanimpactintreatmentdecision-making,wheretheseneedsareidentifiedandaddressedearlyon.
Therealityofolderpatientsturningdowntreatmentbecauseitwouldmeantheywereunabletofulfiltheircaringresponsibilitieswasarecurringthemefromhealthprofessionalsandpatientsinvolvedinthisstudy.
Manyolderpeoplecareforsomeonewhoisdependentonthemandsuchresponsibilitiesaremorelikelytocausedifficultiesforolderpatientsthanyoungerones.Theseissuesareparticularlyprevalentamongstpatientswhosetreatmentislong-termanddebilitating.Thiscanhaveasignificanteffectonhowpeopleviewtheirownhealthandtreatmentoptions.
…hiswifehasseveredementia,hewashermaincarer,…AndIsaidtohim‘youknowwecandothissurgery,wecancutthetumourout,butIdon’tthinkyou’llgetoutof
hospitalforthreetosixmonths,youneedtobeawareofthat’,andhesaid‘wellIcan’tdothat,becauseIneedtocareformywife,andshe’sdeteriorating.’(Anaesthetist)
….Andthat’squiteacommonbarriertotreatmentactually,becausethepatientwillsay,youknow,Idon’twanttocompromisemyownhealthbecauseifmyownhealthis compromised,Imaynotbeabletocontinuelookingaftermyspouse.(Medical
oncologist)
Thoughitispossibleforalternativecaretobearrangedsothatpeoplecanreceivetreatmentandrecover,formanypeoplethiswillbealogisticalandemotionalstruggleatatimewhentheyarelikelytobefeelingunwellandvulnerable.Theseconcernsandfearscanbeexacerbatedifthepersonbeingcaredforhasdementiaorothercognitivedecline,asthiscanoftenincreaseanxietiesabouthowtheywillcopewithachangeincircumstances.
Furthermore,therecanoftenbeasignificantcostassociatedwitharrangingalternativecare,aswellaslogisticaldifficulties143.Althoughsomemaybeeligibleforfinancialassistance,manyarenot.Theseconsiderationsmightmeanthatpatientsdelayordiscounttreatmentaltogetherbutitmightalsoleadtounrealisticexpectationsofhowpeoplemightcopewithrecoveryandcaringforadependentspouseorpartner.
Ithinksometimespeopledon’tknowhowbigtheoperationis…andIdon’talwaysthinkthey’refullyawareofwhattheimplicationsmaybe…theymightthinkifI’moutof

AdvancingCare,AdvancingYears 35
hospitalafteraweekI’mgoingbacktolookingaftermywife….(Anaesthetist)
Inthesecases,theroleofcommunity-basedoncologynursesisvital,asareflexiblemodelsofdeliveringtreatmentsuchascommunity-orhome-basedchemotherapy.However,therangeofservicesavailablerangesconsiderablyacrossthecountry.
…insomeparts…we’vegotverygoodsupportbycommunityoncologynursessotheyseepatientswhoarehavingchemotherapyandcangivesomechemotherapyathome
aswellandmonitortheirsideeffectsbutinsomeotherareas…thatserviceisn’tavailable…thepalliativecareservicesareavailableacross[theregion]butagainthepalliativecareoccupationaltherapyservicesinsomeareasaren’tavailableforsome
patients.(CancerNurseSpecialist)
Forsurgery,thesupportavailabletoarecoveringpatientisimportant,howeverdidnotseemtolimitwhetherapatientwasofferedaparticularcourseoftreatment.
Idon’tknowifI’deverdenyanybodyanoperationiftheyhaven’tgotfamilysupportifeverythingelsewaskindofinthebalance…Ithinkit’sagoodthingifthey’vegotitbut
Idon’tthinkI’dholditagainstthemorweighitagainstthemiftheyhaven’t…(Anaesthetist)
Insomecases,hospital-basedcarecanbeextendedtoensurethatthepatientisrecoveredtoapointthattheywillbeabletocopeathome.Inothercases,patientscanbereferredtorehabilitationorconvalescencehomes.Unfortunately,thereareoftensignificantbedshortagesatthesefacilitiesandsothisisnotaviableoption.
Widerissueswiththesocialcaresystemalsohaveasignificantknock-oneffectoncancercare.Nationalintervieweesandtwosocialworkerslinkedtooncologyteamshighlightedthatthesocialcareassessmentprocessislimitedbyitbeingtooreactive,meaningthatpatientsmustwaituntilaftertreatmentforanyassessmenttobemade.
Wecanfullyanticipatethataftermajorsurgeryoraperiodofchemotherapysomeoneisgoingtobeinastatetoneedthecare.Sowhycanwenotplantoputitinandcancelit
whenwenolongerneedit?AndIthinkIknowwhattheanswertothatisandthat’saboutthefactthatwedon’thaveenoughresourcestocopewithwhatwe’vealreadygot.
(Nationalinterviewee)
2.2.3 TRAVELREQUIREMENTSSomepatientswillberequiredtotravelsomedistancetoaccesstreatmentthatismorespecialised.Forexample,intervieweesataNorthernIrishsitespokeoftheirpatientsbeingsenttoLeedsforstereotacticradiotherapyuntilalocalservicewasestablished.Butevenformoreroutinetreatment,frequencyandinconvenienceoftravelcanbeabarriertoaccess.
…dependingwhattreatmenttheyhavethatcanbequiteanintensescanningregime certaintypesoftreatmentinthefirstyearrequiresforyoutohavefourMRIscans
whicharenotthemostpleasantthingsintheworldsotherecanbealotoftravelinvolved.(Urologist)
Thisisaparticularissueforradiotherapy,whichrequiresregularattendance,oftenoverseveralweeks.Thoughthiscanbechallengingforpatientsofallages,olderandmoresociallydisadvantagedpeoplearemorelikelytobereliantonpublictransportorliftsfromfriendsandfamilywhentheyaccesspublicservices144.

AdvancingCare,AdvancingYears 36
Theseissueshaveclearimplicationsfortreatmentoptions.Forexample,cliniciansandpatientswithbreastcancermayoptforamastectomyiftheyareconcernedabouttheabilitytomanagethedailytravelrequirementsforradiotherapyfollowinglocalexcisionsurgery.
Allourpatientswhohavewidelocalsurgeryareofferedradiotherapyandifthey'rereallytooilltocomeupanddowntothehospital,…patientswhoreallycan’tcopewith
radiotherapyafterbreastcancersurgery,wefullyrecommendthemastectomy,becausethenthereisnorisktotherestofthebreast.(Radiologist)
Transportissuesaremostproblematicfortertiarycentreswhichserveamainlyruralarea.Theseissuesarethencompoundedwhentreatment(andmonitoring)requiresfrequenthospitalvisits,withminimalscopeforremoteorcommunity-basedsupport.
Obviouslyweworkwithlocalhospitalsandcommunitycaretomanagetoxicitiesand complicationsofthediseaseandthelike,butwehavenoalternativebuttoseethem
here.(Medicaloncologist)
Intervieweesbasedatsiteswherepatientsaremorelikelytotravelexpressedconcernsthatthiscouldexcludefrailerorolderindividualsfromtreatment.Thiswasalsoraisedasakeybarriertotakingpartinclinicaltrials.
Soyes,itismoredifficultforolderpeopletogettransportandit’spossiblethatalotofthemdon'twanttobeabothertotheirfamilies…gettingonbuses,trains,whatever,isnotidealandthekindofambulance,minibusservicetrailsthemroundthecountryso
theydon'tlikethat…it’sanotherburdenthattheyhave.(Medicaloncologist)
InEngland,whereradiotherapyservicesaresoontobere-organisedintonewRadiotherapyNetworks,thereisatimelyopportunitytoembedtheneedsofolderpeoplewithcancerinthisprocess,throughmeaningfulpatientinvolvementasservicesareplanned.Recommendation:UKhealthservicesshouldensurethatthespecificneedsofolderpatientsareconsideredinallnewserviceplansandworkforceplans.Forexample,emergingRadiotherapyNetworksinEnglandshouldconsidertheimpactofchangingtravelrequirementsonolderpatientsandshouldworkwithcharitiesandproviderstoensureallpatientsaregiventhesupporttheyneedtoreceivetreatment.
2.2.4 FINANCIALISSUESThecostofbeingillcanbesignificant.Forolderpeople,thiscostoftenrelatestotheneedtofundcarefordependentswhilethecaregiverisreceivingtreatment,aspreviouslydiscussed.Beyondthis,therecanalsobeafinancialcostofpayingforsupportforthepatientthemselves,includinghomecare,residentialnursingcareormoregeneralsocialcaresupport.Intervieweeshighlightedthatthisisoftenpoorlyunderstoodbypatientsandtheirfamilies.
WhatIfindverystrange…iswhenpeoplecomeintohospitalandwedischargethemwithacarepackagetheydonotknowhowmuchit’sgoingtocost.…I’venever
understoodwhynobodyeverchallengesthat…nobodyaskshowmuchit’sgoingtobeandthere’snowayofusbeingabletotellthemeither…(Oncologicalsocialworker)
Recommendation:Cancerservicemanagersshouldensurethatpatients’supportneedsareassessedatanearlystageinthepathway,sothattheyareabletoaccessthesupporttheyneedduringandaftercompletingtreatment.Healthserviceregulatorsshouldconsider

AdvancingCare,AdvancingYears 37
waystoensurethatthisisdoneeffectivelyandconsistentlyacrosstheUK.

AdvancingCare,AdvancingYears 38
3TREATMENTDECISION-MAKINGDOESNOTALWAYSTAKEALLRELEVANTFACTORSINTOACCOUNTWecanonlybesurethattreatmentdecisionsarerightforpatientsifweareconfidentthatdecisionshavebeenmadewithconsiderationofallrelevantinformationaboutthatperson’sindividualcircumstances.Thisistrueforeverypatient,butismostimportantforpatientswithadditionalmedicalandsocialneeds–andsooftenveryimportantforolderpatients.
Unfortunately,thesecomplexneedsareoftennotfullyconsideredaspartofthetreatmentdecision-makingprocessincancer.Thisisparticularlytrueforfrailtyassessments–whichcanhaveasignificantimpactonhowlikelyapersonistotoleratetreatment.Intheabsenceofarobustmethod,assessmentofapatient’sfitnessfortreatmentcanbeassumedbasedontheirchronologicalage,orhowtheyseemduringaconsultation.Onereasonforthis,asoutlinedinthemostrecentCancerStrategyforEngland,isthatstandardisedassessmenttools–suchasaCGA–arerarelyused.Thisisimportant:itiswidelyrecognisedthatchronologicalagealoneisnotastrongindicatorofhowwellapersonwilltoleratecancertreatment145.
3.1 THEUSEOFCOMPREHENSIVEGERIATRICASSESSMENTSINPRIMARYCARE
Inoursurveyofprimarycarestaff,70%ofrespondentstoldusthattheirassessmentofanolderperson’sfrailtyinfluencedtheirdecisionstoreferpatientsfordiagnostictestsortreatment.However,theuseofstandardised,evidence-basedassessmenttoolstomeasurefrailtyobjectivelywaslimited.Instead,GPsandotherprimarycarestafftendedtorelyonclinicalassessments,patienthistoryandphysicalexaminationstoassessfrailty(Figure4).
FIGURE4:PRIMARYCARESTAFF’SMETHODOLOGYFORASSESSINGFRAILTY
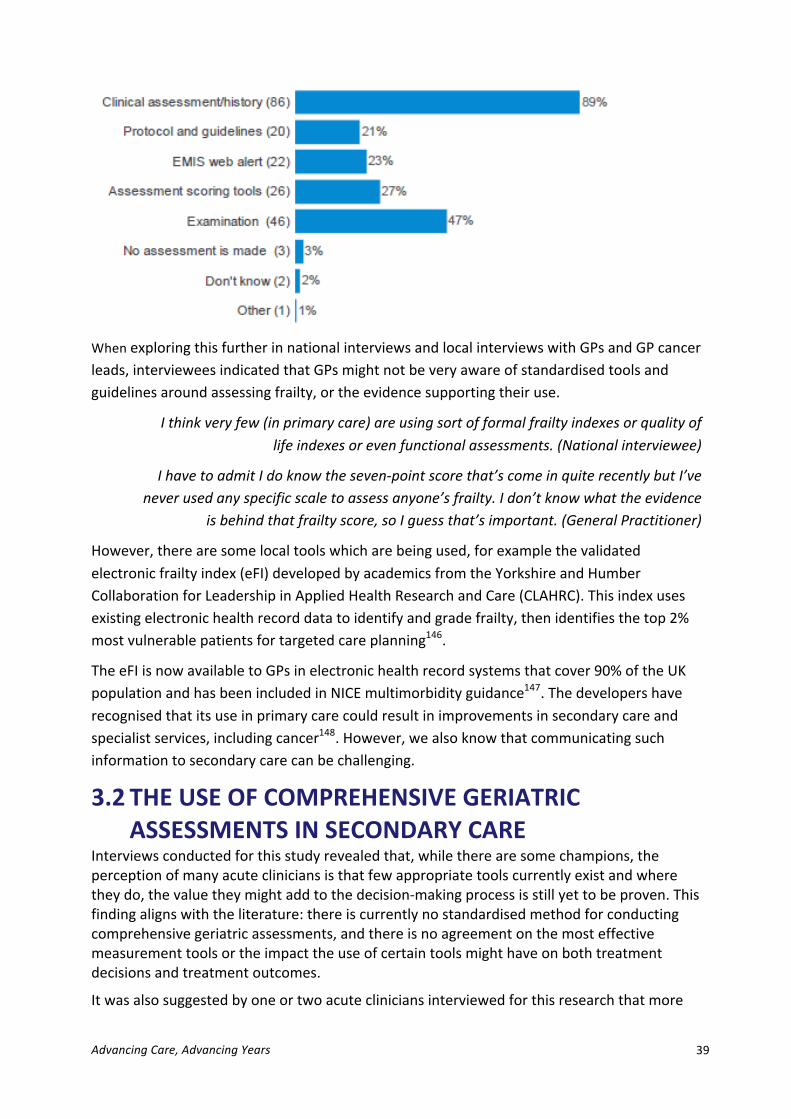
AdvancingCare,AdvancingYears 39
WhenexploringthisfurtherinnationalinterviewsandlocalinterviewswithGPsandGPcancerleads,intervieweesindicatedthatGPsmightnotbeveryawareofstandardisedtoolsandguidelinesaroundassessingfrailty,ortheevidencesupportingtheiruse.
Ithinkveryfew(inprimarycare)areusingsortofformalfrailtyindexesorqualityoflifeindexesorevenfunctionalassessments.(Nationalinterviewee)
IhavetoadmitIdoknowtheseven-pointscorethat’scomeinquiterecentlybutI’veneverusedanyspecificscaletoassessanyone’sfrailty.Idon’tknowwhattheevidence
isbehindthatfrailtyscore,soIguessthat’simportant.(GeneralPractitioner)
However,therearesomelocaltoolswhicharebeingused,forexamplethevalidatedelectronicfrailtyindex(eFI)developedbyacademicsfromtheYorkshireandHumberCollaborationforLeadershipinAppliedHealthResearchandCare(CLAHRC).Thisindexusesexistingelectronichealthrecorddatatoidentifyandgradefrailty,thenidentifiesthetop2%mostvulnerablepatientsfortargetedcareplanning146.
TheeFIisnowavailabletoGPsinelectronichealthrecordsystemsthatcover90%oftheUKpopulationandhasbeenincludedinNICEmultimorbidityguidance147.Thedevelopershaverecognisedthatitsuseinprimarycarecouldresultinimprovementsinsecondarycareandspecialistservices,includingcancer148.However,wealsoknowthatcommunicatingsuchinformationtosecondarycarecanbechallenging.
3.2 THEUSEOFCOMPREHENSIVEGERIATRICASSESSMENTSINSECONDARYCARE
Interviewsconductedforthisstudyrevealedthat,whiletherearesomechampions,theperceptionofmanyacutecliniciansisthatfewappropriatetoolscurrentlyexistandwheretheydo,thevaluetheymightaddtothedecision-makingprocessisstillyettobeproven.Thisfindingalignswiththeliterature:thereiscurrentlynostandardisedmethodforconductingcomprehensivegeriatricassessments,andthereisnoagreementonthemosteffectivemeasurementtoolsortheimpacttheuseofcertaintoolsmighthaveonbothtreatmentdecisionsandtreatmentoutcomes.
Itwasalsosuggestedbyoneortwoacutecliniciansinterviewedforthisresearchthatmore
AdvancingCare,AdvancingYears 40
formalassessmenttoolsshouldnotgetinthewayofthemoreinformalassessmentssuchas‘justseeinghowapatientwalksintotheconsultation’.
WhileCGA,frailtyassessmentetc.mightsoundmoretechnological,Ithinkinrealitytheywouldaddextraworkloadandwouldnotimproveontheendofbedassessmentthat
someoneisfitforintensivetreatmentorbetteronlessintensivetreatment.(Surgeon)
Usingageneralnotionoffrailtytoassessfitnessfortreatmentwascommonpracticeinsecondarycare,howeverparticipantsfoundtheobjectivemeasurementofthisconceptchallenging–preferringamoreintuitiveapproach.
Somesecondarycareintervieweesmentionedtheuseofahandgriptesttodeterminestrengthandthesittingandstandingtestbutappearedinpracticetoacceptafarmoreintuitivesenseofunderlyingstatusamongolderpatients–whilerecognisingtherearelimitationswiththisapproach.However,wedidfindsometoolsbeingused.
3.3 WHATASSESSMENTTOOLSAREBEINGUSED?
3.3.1 CARDIACANDRESPIRATORYFUNCTIONTESTSAcutesecondarycareteammemberssuggestedthatcardiacandrespiratoryfunctiontestswerethemostsignificantindicationsoffitnessforsurgery.ECGsareoftenusedtoassesscardiacfunction,toidentifyirregularitiessuchasatrialfibrillation–whichwouldbearedflagindicatingthatthepatientwouldbeunabletotolerateageneralanaesthetic.
Cardiopulmonaryexercisetesting(CPETorCPEX149testing)isconsideredthegoldstandardfortestingcardiorespiratoryfunction,howeveritrequiresspecialistequipment,facilitiesandstaffresource–whichmaynotalwaysbeavailable.Thistestingalsorequirescyclingactivity,whichmanypatientsmaybeunabletocomplete.Instead,studyparticipantsspokeofamoreinformalassessment,inwhichtheyascertainpatients’abilitytoundertakevariousactivitiesofdailyliving(ADL).
SoIaskabouttheiractivitiesofdailylivingwhattheycandoforthemselvesandthenintermsofexercisemyfirstquestionisiftheycanclimbtwoflightsofstairswekindofgeta roughguideofmetabolicequivalents…soiftheycanclimbtwoflightsofstairsthatmeanstheycanusuallyraiseitfourfoldwhichintheliteratureisconsideredadequatefor
majorsurgerywhentheyhaveabdominalsurgery.(Anaesthetist)
3.3.2 PERFORMANCESTATUSPerformancestatusisaWorldHealthOrganisationdefinitiondescribinghowmobileapersonis,fromascaleof0to5–with0beingsomeonewhoisfullyactiveandabletocarryonallpre-diseaseperformancewithoutrestriction.However,someclinicianintervieweesrecognisedthatthisisnotoftendetailedenoughtoinformtreatmentdecisionssinceitdoesnottakeimportantbiologicalfactorsintoaccount.
…theageofthepatientisanimportantfactor…I’vetreatedelderlypeoplewithsystemictreatmentandtheyareperformancestatusone,butthesepeoplehaveolderkidneys,oldliversandthedrugsthatthey’regettingareprocessedandmetabolised
oftenthroughoneoreitherbothofthoseorgans.Andyou’regettingpeoplewitholderbodyorgansandyou’regivingthemtoxicdrugswhichalreadyhaveariskofdeath.

AdvancingCare,AdvancingYears 41
(Clinicaloncologist)
Decisionscanbeparticularlydifficultwhenindividualsarefunctionallyfitandperceivethemselvestobeveryfit,buthaveotherhealthconditionsthatwouldjeopardisethesuccessandsafetyofsystemictreatment.Oneparticularlystrikingexamplewasgivenofapatientwhowasphysicallyveryfitandactivebuthadstagethreekidneydiseaseandaweakheartfromapreviousheartattack.
Forme,thatwasaverydifficultconversationtohavebecausehelookedsowellandhelookedfit…butI'veseenwhatonecycleofchemotherapycandowithsomeonewhosekidneyfunctionisalreadyextremelyborderline,I'veseenitputpeopleintocomplete
renalfailure.I'veseenittriggeranotherheartattack…(CancerNurseSpecialist)
Thisquotedemonstratesthevalueofamorecompletefrailtyassessmentthatincludesmedicalhistoryaswellasfunctionaltesting–andthatthisisparticularlypertinentfordecisionsrelatingtochemotherapy.
3.3.3 RISKSCOREASSESSMENTClinicianintervieweessawinformationonriskscoresashelpful,particularlyintermsofprovidinginformationtopatientssothattheycanbeinvolvedindecision-making.Riskscoresprovideanaveragescoreforapersonofaspecificage,withoutcomorbiditiesorunderlyingconditions,whichcanbecomparedagainstariskscoreforthesamepatientwithspecificcomorbiditiesorunderlyingconditions.Thesearewidelyused,forexamplePOSSUM(PhysiologicalandOperativeSeverityScorefortheenUmerationofMortalityandMorbidity150).
However,thesetoolsalsohavelimitations.OneintervieweenotedthattheseriskscoresarebasedonmeasuringtheaverageperformanceofUScentresundertakingtheseproceduresbutmaynothavethesameapplicabilityinaUKcontext.
…again(it’s)doneinbignumbersbutit’sstilldoneinAmericathere’salotofvariationfromcentretocentre.Asabigcentreweareprobablybetterthansomeofthe
Americancentres…youexpectthatitwillaverageoutbutifyouareoneofthewellperformingTrustsyournumberscouldbebetterthanthat,orifyou’renotsowell
performingyournumberscouldbeworsethanthat…(Anaesthetist)
3.3.4 HOLISTICNEEDSASSESSMENTAHolisticNeedsAssessment(HNA)isawide-rangingassessmentthatconsidersphysicalandpracticalconcerns,aswellasthepatient’semotionalandinformationneeds.Thisisoftenlinkedtothedevelopmentofacareplanthattakesthesefactorsintoaccount.
Atonesiteinvolvedinthisresearch,patientswithbreastcancerhaveanhour-long1:1pre-operativediscussionwithabreastcarenursethatincludesanHNA.
Wefindoutaboutthem,whentheyworked,whattheirlifewaswhentheywereinemployment,whatlifeexperiencesthey’vehad.Whetherthey’vehadanyexperience
ofcancer,whattheirfamilysituation,whattheirhomesituationis.Financesaswell…andwealsodoourhospitalanxietyanddepressionscoreaswell.(CancerNurse
Specialist)
WhileHNAshavesignificantmerit,theyarerelativelyresource-intensiveandintervieweesreportedthatalackoftimeandcapacitylimitstheiruse.
AdvancingCare,AdvancingYears 42
3.3.5 SUMMARYOnlyonecasestudysitesystematicallyusedanyformofCGAandingeneralwefoundverylowusageofvalidatedassessmenttools.Thisisparticularlyconcerningwhenconsideringthat‘frailty’washighlightedasthemostinfluentialfactorsinclinicaldecision-makinginthesurveyofMDTmembers(at79%).Manycliniciansinterviewedperceivedtheretobeveryfewappropriatetoolsandwereunconvincedofthevaluesuchtoolswouldaddtothedecision-makingprocess.
Overall,despiteseveralconcernsraisedastothevariabilityinhowcliniciansinacutesettingsmightassessaperson’sfrailty,wefoundthatvalidatedtoolswerenotwidelyusedinassessingolderpatientsandtherewasnoevidenceofthesystematicuseofanyformofcomprehensivegeriatricassessmentintheacutesector–asisechoedinacademicliteratureandin2012researchbyMacmillanCancerSupport151.
Weheardconcernsamongstsomenationalintervieweesthattheuseofsubjectiveassessmentsoffrailtycouldresultininequalitiesinaccesstotreatmentforolderpeoplewithcancer.
Imeancertainlythedatawouldsuggestit(primarycarefrailtyassessment)maybepartoftheproblem.Ifyoulookatthesortofthecanceroutcomesandsortofstagesat
presentation,clearlythereisabiasandweareservingourelderlypatientslesswellthanwearetheiryoungercompatriots.Therewillbebothpatientfactorsand
professionalfactors.Andit’salmostwhatIwouldcallamedicalsocietalissueandit’ssortofalongthelinesifwewanttoaddressitwewillhavetoaddressbothsidesof
thatequation.(Nationalinterviewee)
Ourinterviewsalsohighlightedthatpeoplelivingincarehomescouldbeparticularlyatriskofbeingoverlookedforpotentialtreatment.Inthisinstanceitispossiblethat,intheabsenceofanysystematicmethodofassessment,frailtyissimplyassumedandoverestimated,leadingtoalackofreferral.
Iwonderwhetherthey(primarycare)investigatepatientsinnursinghomesasmuchastheywouldiftheyweren’tinanursinghome–theremaybeadegreeassumptiongoingon‘Idon’tthinkMrsBloggsiswellenough’andIwonderwhetherthereisabetterwayofworkingwithGPstoassessperformancestatus.(Medicaloncologist)
Itisclearfromthisresearchthattheclinicalcommunityhasconcernsaboutsomeolderpeoplenotbeingassessedobjectively.However,thereisalsoarelativelackofevidenceaboutthemostappropriateformaltoolsandprotocols.Severalattemptshavebeenmadetorecommendbesttools,howevernostandardisedmethodhasbeenagreed.
TheUKMacmillanCancerSupportandDepartmentofHealthOlderPersonsPilotdemonstratedthatgeriatricianliaisonwasthemosteffectivewayofdeliveringCGA.However,KalsietalhavesuggestedthatCGAscouldbeundertakenbynursesorotherclinicians,iffacilitatedremotelybyageriatrician.Thisislikelytobemoremanageableforthehealthserviceatpresent,giventhecurrentworkforceshortages.
Recommendation:UKhealthservicesshouldpilottheroutineusageofgeriatricassessmentsforolderpeoplewithcancerandshouldseektogatherfurtherevidenceoftherelativebenefitsofdifferenttools.
AdvancingCare,AdvancingYears 43
4 THERIGHTINFORMATIONDOESNOTALWAYSGETTOTHERIGHTPEOPLETOSUPPORTCLINICALDECISION-MAKING
Theinformationaboutapatientthatisavailabletotheclinicianinvolvedinmakingtreatmentdecisionsishighlyvariable.Itdependsonthereferralroute,thepathwaythepatientisfollowingandthestageofthepathwaytheyarecurrentlyat.So,forexample,theinformationavailablefordecisionstobemadewillbequitedifferentifapatientisseenas:anemergencyinA&E;asaresultofatwo-weekurgentreferralfromtheirGP;followingreferralfromalocalhospitaltoatertiarycentre;oriftheyareonafollow-uppathway,havingpreviouslyreceivedtreatment.
Thereareseveralkeypointsoffocuswherethetransferofinformationisparticularlyimportant:betweenprimaryandsecondarycare,andtoandfromthemultidisciplinaryteam(MDT).
4.1 INCLUDINGTHERIGHTINFORMATIONFROMPRIMARYCARE
Primarycarecliniciansoftenhavethemostdetailedhistoryofapatient,includingtheirleveloffrailtyandanycomorbidities.However,thisinformationcanonlybefactoredintocancertreatmentdecision-makingifithasbeenpassedfromprimarycaretosecondarycare.Unfortunately,weheardfrombothprimaryandsecondarycareintervieweesthattheyoftenfinditdifficulttogetintouchwitheachotherdirectly.
Wetestedtheideaofincreasingtheinvolvementofprimarycareinpre-treatmentoptimisation.Whileprimarycarerespondentstooursurveywantedtosupportolderpeoplewithcancer,andsawvalueinusingGPs’knowledge,therewaswidespreadconcernovertheircapacitytodothis.45%ofrespondentssaidthattheydidnotknowiftheywouldliketoseeagreaterroleforprimarycareinpre-treatmentoptimisation,whichislikelyduetothetensionbetweenwhatisdesirableandwhatisrealisticinthecurrentresourcecontext.
ThechallengeatthismomentintimeisthatgeneralpracticeisseeingitsworstrecruitmentcrisisthatmostGPscanrememberandthereissimplynottheresourceavailabletotakeonmorework.Thereisnotthecapacityandlocally,Iseepracticesclose.It’snotalackofwillingness,it’sjustnotbeingabletoandIthinkwithregardstoimprovingservices,itwouldneedtobedoneinsuchawaythatitissotimelight,itjustneedstobedoneinsuchaclever,easy,encouragingway,ratherthanjustsimplyburdeningGPswithmorework.(GeneralPractitioner)
FIGURE5(PRIMARYCARESURVEY)WOULDYOULIKETOSEEAGREATERROLEFORPRIMARYCAREINPRE-TREATMENTOPTIMISATION?

AdvancingCare,AdvancingYears 44
4.1.1 THETWO-WEEKWAITREFERRALFORMAmajorissueraisedthroughtheprimarycaresurvey,nationalandlocalinterviewswasthenatureofthetwo-weekwaitreferralform,whichisusedwhenpatientsaregivenanurgentreferralforsuspectedcancer.37%ofpatientsin2015werediagnosedthroughthisrouteinEngland152.Theseformsarebriefandthusthereisnospaceforprimarycarestafftocommunicatepeople’spersonalcircumstances,comorbidities,theirfrailtyorothermedicalhistory.Thismeansthatthecliniciansmakingdecisionsaboutpatients’treatmentoftendonothaveadvancedaccesstoinformationthatcouldlaterprovecritical–andsotheperson’sageismorelikelytobeusedasasurrogatemeasurefortheiroverallhealth.
Oneofthebiggestproblemswehaveisthatwhenwerefersomebodyfromgeneralpracticewithasuspectedcancerdiagnosis,weusethistwo-weekreferralpathwaywhichinvolvesaverybasiconepageformwhichessentiallysays“What’sthethingyou’rereferringthemforandwhy?”Nothingelse.Itdoesn’tsaywhatmedication
they’reon,whataretheirco-morbidities,whataretherealissues,whatarethesocialfactors,doesn’ttellanythingabouttheperson,itjusttellsyoupotentiallywhatcould
berelatedtothedisease.(NationalInterviewee)
Itisunderstandablethatthisformisbrief:itisbynatureurgent,andthevastmajorityofpatientsgivenanurgentreferraldonotgoontoreceiveacancerdiagnosis.Butforthosewhoarethendiagnosedwithcancer,theclinicianresponsiblefortheirfuturetreatmenthasverylimitedinformationabouttheirpatienttofactorintotheirdecision-making.Thiswasdescribedasawasteofa‘phenomenalresource’byonenationalintervieweewhoisaGP.
Intheabsenceofacomprehensiveoverhaulofinformationsystemstofacilitatedata-sharingbetweenprimaryandsecondarycare,relativelysimplechangestoreferralformscouldresultinasignificantimprovementintheamountofinformationavailabletoinformtreatmentdecisions.Asformsdifferfromregiontoregiontherearesomenotableexamplesofgoodpractice,wherethosemakingreferralshavespaceforadditionalinformation.
TheGPbelowdescribeshowimportantfactorsfortreatmentdecisionscanbeoverlooked,suchasdementia.Thesetypesofsituationscanleadtoreversedtreatmentdecisions–whichintroduceavoidabledelaysthatcanbedistressingtopatientsandcaregivers,andultimatelyleadtowastedtimeandresource.
Whatmightbereallyimportantisworkingouthowtoworkefficiently,thinkingaboutinformationflows.Soiftherewouldbe,forexample,onthetwoweekwaitreferralform,thosefiveareasofcognition…itwouldjustbeasimpletickboxexerciseto
identifyareasthattheoncologistwouldneedtotakeintoaccount,becausesometimesifapatienthasbeenmuddledabitbutnobodyhastakentheinitiativetoinvestigate,thispatientcouldhaveundiagnoseddementiaand[is]beingreferredbythetwo-week
wait.(GeneralPractitioner)
AdvancingCare,AdvancingYears 45
4.2 THEROLEOFTHEMDTEverypatientdiagnosedwithcancerintheUKhastheircasediscussedataMDTmeeting.AnMDTismadeupofavarietyofhealthprofessionalsinvolvedintreatingandcaringforpatients.TheMDTmeets,mostoftenweekly,todiscussindividualpatients’casesandmaketreatmentrecommendations.
Thismeetingwilloftenoccurbeforethepatienthasmetasecondarycareclinician,meaninganyinformationoffrailtymustbegeneratedbytheprimarycareteamreferringthepatient.However,weknowthatmeanstotransferthisinformationarelimited.MDTmembersrespondingtooursurveyalsoexpressedthattheywouldlikemoreinformationfromprimarycare;specifically,othermedicationsandcomorbidities.
Again,knowledgeoffrailtyassessmentswithinsecondarycareprofessionalswasweak.
Becausethereisn’talwaysasolediagnostictestthatyoucansaythispersonisfrail-it’softenaconstellationofthingsandyouknowwe’reverygoodatpickinguppeoples’
comorbiditiesbuthowdoyoudefinesomeoneasdefinitelyfrailIdon’tthinkthat’staughtparticularlywellinmyopinion.(Anaesthetist)
ThepurposeoftheMDTdiscussionistomakeatreatmentrecommendation;thefinaldecisionmustthenbemadebytheclinicianandthepatient.TheMDTisanopportunityforavarietyofhealthprofessionalstocometogetherandsharetheirexpertise,toformulatethemostappropriaterecommendationfortheirpatients.
IfMDTsaretomakeatreatmentrecommendationthatistrulyappropriateforthepatient,theymustincludeallrelevantinformation.ButrecentresearchbyCRUKfoundthatonly14%ofMDTdiscussionsincludedinformationthatdidnotspecificallyrelatetothepatient’stumour153.Whilstthisisconcerningforallpatients,thisislikelytodisproportionatelyaffectolderpatientsastheyaremorelikelytobecomorbidandtohavecomplexsocialneedsthatwillimpacttreatmentdecisions.
Furthermore,pastresearchhasfoundthatbetween10and15%oftreatmentrecommendationswerenotimplementedbecausetheyweretooextremeforthepatient154.ItislikelythatthisisbecausetheMDTdidnottakeallrelevantfactorsintoaccount–forexamplecomorbidities,frailtyorthepatient’spreferences.
WhilstClinicalNurseSpecialistsareconsideredtobemostqualifiedtoprovidesuchinformation,nursesdidnotcontributeinformationinover75%ofmeetingsobservedduringthatresearch–perhapsasaresultofashortageofCNSs,aswellasthemarginalisationofnursesandotheralliedhealthprofessionals155.ThisreflectsthelackoftimeavailableforfulldiscussionofcomplexpatientsinMDTmeetings:theaveragediscussionobservedinourpastresearchlastedjust3.2minutes,inmeetingslastinguptofivehours,andincludedanaverageofjustthreepeople–althoughanaverageof14peoplewereinattendance.
Thispressurehasmajorimplicationsforthequalityoftreatmentdecision-making.Notincludingimportantinformationaboutapatient–suchastheirpreference,theirpsychosocialsituationortheircomorbidities–ispoorforpatientsandalsopoorforMDTefficiency.
ThereisaclearneedtoreformandstreamlineMDTs,sothatmoretimeisavailabletodiscussthemostcomplexpatientsinenoughdepth–andtherefore,manyolderpatients.ItisalsoimportantthatMDTsconsistentlyhaveaccesstoallrelevantinformationaboutthepatientstheydiscuss,sothattheycanmaketreatmentrecommendationsthataretailoredtothe
AdvancingCare,AdvancingYears 46
patient’sindividualcircumstances.
ThisreportalsorecommendedtheuseofaproformatoensurethatallrelevantinformationisincludedintheMDT’sdiscussion.Thiswouldbecompletedbythereferringclinicianandwouldincludeallrelevantdiagnosticinformation,aswellasinformationonpatientpreferencesanddemographics–includingfrailty.54%ofMDTmembersalreadyusesomeformofproforma,butthisisinconsistentandthereisnonationalguidanceontheircontent.81%ofMDTmembersfeltthatusingaproformawouldhaveabeneficialimpactonmeetingefficiency,sincethepatientwouldnotneedtobediscussedasecondtime.Weseethisashavingaparticularlystrongimpactonolderpatients.
Recommendation:UKhealthservicesshouldleadthedevelopmentofnationalproformatemplates,toberefinedbyMDTs.MDTsshouldrequireincomingcasesandreferralstohaveacompletedproformawithallinformationreadybeforediscussionatameeting.
4.3 THEFLOWOFINFORMATIONFROMSECONDARYTOPRIMARYCARE
Oursurveysandinterviewsofprimarycarestaffhighlightedaparallelfrustration,inthegapsintheinformationflowingfromsecondarycarebacktoprimarycare.Staffwereparticularlyinterestedinknowingapatient’sdiagnosis,treatmentrecommendations(andrationale),prognosis,furtherassessmentandtheinformationgiventothepatient.Respondentstooursurveysofhealthprofessionalsalsohighlightedtheroleofprimarycareinsupportingpatientstomanagetheircomorbiditiesandthusenablingthemtobefitenoughtoaccessagreaterrangeoftreatmentoptions.
IseemyroleasaGPishavinghonestconversationswithpatientstohelpthemunpickthisstuff.Nowalotofcancercareteamsareverygoodatprovidingpeoplewithinformationandgenerallywhathappensispeoplewillhaveahugeamountof
information,feelunabletomakeadecisionandgoawaythencometotheirGPwithquestionstotalkthemthrough.(NationalInterviewee)
StaffalsoreportedthatpatientswouldoftenattendaGPappointmenttodiscusstheirdiagnosis,treatmentanditsimpactontheirlives.Thisoftenhappenssoonafterpatientshaveattendedahospitalappointment,meaningthatthisinformationisneededveryquicklyaftertheevent.
Idon’thavetheinformationthat’sbeengiventothepatient,allI’vegotisthepatient’srecollectionorprint-out,Idon’thavewhatthedoctorinthehospitalwasactually
thinking,becauseittakessolongforcommunicationstogetthrough.Sogreateruseofelectroniccommunicationwhereby…what’ssaidtothepatientcanbesaidtotheGPalmostsimultaneously,becauseitisnotuncommonforsomebodytobeinfloodsoftearsinthecaronthewayhomefromthehospital,phoningtheGP,askingforanurgentappointmenttotalkthingsthroughbuttheGPdidn’tevenknowtheyhadacancerdiagnosisandwouldn’thavebeentoldfordays,sometimesweeks.(National
IntervieweeandGeneralPractitioner)
ThisisarecognisedissueandthestandardoperatingprocedureforinformingaGPoftheirpatient’sdiagnosisisofteneitherthesamedayorwithin48hoursofadiagnosis,howevertheextenttowhichthisactuallyhappensisvariable.
Wealsoheardfromprimarycarestaffthatthediagnosisalonewasoffairlylimiteduse.In
AdvancingCare,AdvancingYears 47
addition,theywouldvalueinformationabouttheprognosis,treatmentoptionsandwiderplaninordertosupportthemintheircareofthepatient.
Althoughstaffvaluedformsandelectronicsystems,theoptimalmechanismwouldbehavingasinglepersonwhotooktheleadoncoordinatingapatient’scareplanandcommunicatingtheircasebacktotheGP.Forthisreason,CNSswerehighlyvaluedfortheircontribution;thisisespeciallytrueformorecomplexpatients,asolderpeoplewithcanceroftenare.CNSsrelayinformationbetweenprimaryandsecondarycare,ultimatelyhelpingappropriatedecisionsbemade.However,primarycarestaffalsoflaggedthatthereissignificantlocalvariationaroundCNSavailability.
Recommendation:Healthcareprovidersmustensurethatprimarycarestaffareupdatedontheoutcomeofpatientdiscussionsinatimelymanner.Thisshouldincludewidespreaduseofdigitalsolutions.
4.4 PRESSURESONONCOLOGYSERVICESLIMITTHEQUALITYOFDECISION-MAKINGANDCOMMUNICATIONBETWEENOLDERPEOPLEWITHCANCERANDTHEIRCLINICIANS
Thereisstrongevidencethatshareddecision-making(SDM)isbeneficialtopeoplewithcancer4.However,achievingmeaningfulshareddecision-makingcanbemoredifficultforolderpatients,whoaremorelikelytohavemultipleconditionsandwhomaybebalancingdecisionsabouttreatmentwithmanyotherfactors.Thequalityofcommunicationtopatientswasthestrongestthemeidentifiedbythepatientsinvolvedinthisresearchaspartofinformeddecision-making;thisthemewasalsousedasthebasisforthepatientsurvey.
Theolderpeoplewithcancerandcaregiversinvolvedinthedesignanddeliveryofthisstudysawacontinuumofdecision-making.Atoneendwas‘decision-makingasconsent’,wherehealthprofessionalsmerelygainconsentfrompatientsforthetreatmenttheyprefer.Atthemostpositiveendofthespectrumwas‘decision-makingasreachingconsensus’,whichwasalengthierprocesswithmorescopeforpatientstolearnaboutanddiscussthedifferenttreatmentsoptions,beforemakinganinformedchoice.
Inoursurveyofolderpeopleaffectedbycancer,themostcommonstyleofdecision-makingreported(by40%ofrespondents)was“thedoctororotherhealthprofessionalled(thedoctororotherhealthprofessionalsmadeallthedecisionsbuttookmyviewsintoaccount)”.Thiswasfrequentlyreportedasanegativeexperience.
Thecurrentcontextoftime-stretchedcancerservicesarefurthercompromisingtheabilitytofacilitatetrueshareddecision-making,asevidencedbyrespondentstoourpatientsurvey.
TherisksweregivenverybrieflyandIwashandedthisinwrittenformontheconsentform.ThesideeffectsofradiotherapywerenotexplainedfullyandIfoundoutmore
informationformyselfandthenaskedquestions.(apatient)
Mostly,itwasassumedthatIwoulddowhatevertheysuggested-whilstIwasnot4 CanCORS study, 2015
AdvancingCare,AdvancingYears 48
unhappywithwhatwasbeingoffered,asIknewthattherewerenotalotofoptions,IdonotfeelinhindsightthatIwasgivenmuchchoiceorindeedsupportinmakingsuch
achoice.(apatient)
Anotherrespondentreportedfeelingthatquestionswere‘toleratedratherthanencouraged”.Inothercases,patientswereexpectedtomakeadecision,butdidnotfeeltheyhadthenecessaryknowledgetodoso.
Supportwasthereintheformof'hand-holding'whileitwasuptometomakethedecision.Statisticsshowedroughlythesameoutcomeforsurgeryorradiotherapy.ItwouldhavebeenjustassupportivetogivemeacointotosswhenwhatIreallyneededwassomeindicationastowhichwouldbebetterformyparticularcircumstances.PerhapsIwaslookingforguidancethatsimplyisn'tthere.(apatient)
Somecliniciansinvolvedintheresearchalsoreportedpatientsnotwantingtomakethedecisionthemselves.
Andsotheconversationgoessomethinglikethisyouknow;‘nowyouwanttreatment,Ihaveachoiceoftreatments,wouldyoulikemetotellyouaboutbothofthemandyoumakeyourdecisionorwouldyoulikemetomakearecommendation?’Andninety-eightpercentofpatientssay‘youmaketherecommendation’.(MedicalOncologist)
Thesequoteshighlighttheimportanceofgivingpatientsallrelevantinformationneededtomakeadecision,butalsoofflexingtheapproachaccordingtothepatient’swishes.
4.5 COMMUNICATIONCHALLENGES
4.5.1 CONFLICTINGINFORMATIONManynegativeresponseaboutcommunicationreceivedthroughourpatientsurveyfocusedonnotbeingabletounderstandinformation,andbeinggivenconflictingmessages.Thisreinforcestheimportanceofcoordinatingcareacrossthemultidisciplinaryteamandpresentingaunifiedmessagetothepatient.
Iwasconcernedthatthesurgeonandtheoncologistdidnotseemtohavequitethesameagendas-whilsttheysuperficiallyworkasateam,forexampletheoncologistwasverydismissiveofthesurgicaloption,whichIfoundconfusing.(apatient)
However,anaesthetistsinterviewedforthisstudyalsoacknowledgedthatonoccasion,theremaywellbedifferencesinopinionbetweenthecliniciansinvolvedastothebalanceofrisks.
Soitpaysyoutoknowexactlywhatpatientsknowwhentheyarrive,whatthey’vebeentoldandwherethey’reupto…there’sakindofagoldenrulethatifyou’regoing
toquotefiguresyoumustwritethemdown.Soifasurgicalcolleaguehasquotedfigurestheyshouldbeinhisclinicletter,whichIwillalwayshaveread…soImightsay
‘well,actuallyI’mgoingtoadjustMrX’sfiguresbecauseIdon’tthinkIfeelquiteasoptimisticashedoes’.Sothat’showI’dhandlethat.(Anaesthetist)
AdvancingCare,AdvancingYears 49
4.5.2 BENEFITVERSUSRISKPartoftreatmentdecision-makinginvolvesbalancingthebenefitoftreatmentwiththeriskofalowerqualityoflife,stemmingfromlong-lastingside-effectsoftreatment.Tomakethesedecisions,theymustbegiventhefullspectrumofinformation–butweheardfrompatientsinvolvedintheresearchthatthiswassometimesnotthecase,withemphasisdisproportionatelyplacedonbenefits.
Benefits[ofsurgery;removalofthetumour]wereclear.However,anileostomywasinvolvedandlittlewassaidaboutthisleavingmeunpreparedfortheresult.(apatient)
But[I]wouldhavelikedmoreinformationontheeffectsofchemoonyourbrainasIwasdefinitelyaffectedbythetreatment.Andalthoughmymentalacuityhasimproved
itisnotthesameasitwas.(apatient)
Thispicturewasnotreflectedbythecliniciansinterviewedaspartoftheresearch,whoreportedthatpresentinginformationonthebenefitsandrisksofdifferenttreatmentoptionsisanimportantelementofensuringpatientshaverealisticexpectationsandcanmakeappropriatedecisions.Thesuccessofdoingthisislikelytovaryconsiderablybetweenclinicians.
4.6 HAVINGSUFFICIENTTIMETOMAKEDECISIONSAnothercommonthemefromthisresearchwastheneedtohavesufficienttimetomakeaninformeddecision,andcurrentdifficultiesinachievingthis.Again,thisisfeltacrosscancerservicesbutmaydisproportionatelyimpactolderpatientsbecauseofthecomplexnatureofdecision-making.Aswellasimpactingtheprocessofdecision-making,thisislikelytoaffectpatients’broaderexperienceofcare.
Again,IwasnotabletotakeeverythinginatthetimeandittookquiteawhiletothencalmlygothroughthecarrierbagofleafletsIwashandedontheday.(apatient)
Thisperspectivewasreflectedbynationallevel,primaryandacutecareinterviewees,whoallhighlightedtheimportanceofgivingpatientstimetothinkthroughtheimplicationsoftreatmentandtheextentofsupporttheyarelikelytohaveavailable.
Thisisfeltparticularlyacutelyduringaconsultation,whenpatientscanbesensitivetoclinicians’highworkloadsandareconsciousnotto‘takeuptheirtime’5.Again,thisoftenimpactsolderpeoplemorethanyoungerpeople,astheymayrequiremoretimetoconsideroptions.
TodayIhadapatientwhohascancerbuthasothercomorbidities…soIhadtodiscussthat…andmakeitcleartothemthatthesearetheriskfactors,thesearethethingsthatgowrong…that20/30minutes…justgetsdraggedonto45minutes.Wecan’tjuststoptheconsultationbecauseit’sbeenrunningoutoftime.(Anaesthetist)
Atonesiteobservedinthisresearch,amoreflexiblebreastclinicsystemhasbeenimplemented.Thisprovidesmorerealisticclinicslots,redressingthewidespreadtrendforclinicswhichalwaysrunovertime–leadingtopoorexperiencesforhealthprofessionalsandpatients.
…sometimeswewereheretilleighto’clockatnight…Anditwasunfaironthe5 Joseph-Williams et al, 2014
AdvancingCare,AdvancingYears 50
patients.Itwasdrainingonthestaff…andbythetimeyou’regettingtotheendoftheclinic,youknow,yourenergylevelsarereallysortofhittinglowandyousortofhavetoquestionwhathaveIgottocontinuetoofferthisevening…Butit’scompletelydifferentnow.Sotheslotsarewellspreadout,clinicsarerunningtotime,patientsaren’tkeptwaitingandwe’refinishingatareasonabletimeaswell.(CancerNurseSpecialist)
Recommendation:CancerMDTleadsandservicemanagersshouldconsiderreviewingthelengthofconsultationslots,factoringinadditionaltimeformorecomplexpatients,andprovidingadditionalsupportbefore,duringandafterconsultationsforthosewhoarelivingwithfrailtyorhavemultiplecomorbidities.
4.7 NATIONALPRESSURESONDECISION-MAKINGTIMELINES
Cancertreatmentdecision-makingintheUKisalsostronglyshapedbynationaltreatmenttargets.SeveralmembersofcancerMDTsinterviewedforthisstudyraisedtheissueofnationaltreatmenttargetscreatingunhelpfulpressure,fortworeasons:firstly,throughputtingpatientsunderpressuretomakeaquickdecision,butsecondlybylimitingopportunitiesfortestingpatients’likelihoodtobeabletotoleratetreatment,andthenfortailoringtheirplanaccordingly.
Theotherissueisthatwiththegovernmenttargetsformakingadecision,oftenpeoplearehavingtomakeadecisionquitequicklyandIthinkyouknowsometimeswejust
needtogivepeoplemoretimetohelpsupportthemmaketherightdecisionforthem.(CancerNurseSpecialist)
They’reguidelinesnottramlinesandIthinkpeoplegetsocaughtupinthat,thatyouforgetthepatientmaynotwanttoworkinthetimescalethattheguidelinessay.
(Nationalinterviewee)
Andsomepeopleneedtoseefamily;theyneedtogetdaughtersandfamilyoverfromAustraliaorAmerica.Theywanttoseethembeforetheygothroughanoperationthattheymaynotsurvive...SoIthinkthepushtodeliveran18weekpathwaysometimes
detractsfromwhatthatpatient’sneedsare.(Anaesthetist)
Furthermore,nationaltargetscanalsomeanthattherearelimitedopportunitiestospendtimetestingandretestingpeopleforhowlikelytheyaretotoleratetreatment,andoptimisingthemifnecessary.Thishasbeenechoedinresearch,whichhasfoundthatservicetargetsthatfocusresourcesolelyoncancercandisadvantagepatientswithcomplexwiderneeds,asindividualcliniciansmaystruggletodelivereffectivetreatmentplanswithoutbreachingtargets156.
…there’sgoodevidencetoshowthatifyoutryandoptimisepeople…youcanimprovetheirCPEXtesting.Sowehaven’tgottimetodothatforcancersurgerybecause
obviouslythey’rewithinawindowthatwehavetoseethem.(Anaesthetist)
Recommendation:inongoingreviewsofcancerwaitingtimestargets,NHSEnglandanddevolvedhealthservicesshouldconsiderwaystoensureoptimaltreatmentaccess,a

AdvancingCare,AdvancingYears 51
positiveexperienceandbetteroutcomesforolderpeoplewithcancer.
4.7.1 IMPROVINGTHEPROCESSOFDECISION-MAKINGOlderpeopleinvolvedinthisstudyidentifiedseveralmeansofimprovingtheprocessoftreatmentdecision-making,suchascharity-runcancersupportservicesandpeeradvocacy.
‘Iwasutterlyconfused[afterdiagnosis]andcouldn’tunderstandwhytheworldwasstillturningreally.Itwasabreakthroughmeetingmyadvocates.Ihavebeenanadvocatemyselfforthelasttwoyears.Theadvocatesofferacaringapproachandtheyhavebeentherethemselves,weareallonthesamelevel.Mythirdadvocatewasagreatmatchformepersonalitywise.Theywentwithmetohospitalappointmentsandprovidedtransportandhelpmetofacethereality.’(Olderpersonwithcancerandco-researcher)
Somepeoplealsospokeaboutthevalueofimprovingcommunicationthroughasummarycard,heldbyeachpatient.ThiswasincludedasarecommendationoftheOxfordshire‘Cancer,OlderPeoplePeerAdvocatespatientexperienceGroup’reporttoHealthwatch6.Thecardwouldincludeasummaryofdiagnosis,treatmentrecommendations,currentmedicationsandthedetailsoftheprofessionalteamassignedtotheolderpatient,aswellashowtocontactthem.
6 Young/COPA Peer Advocates Patient Experience Group, 2016
AdvancingCare,AdvancingYears 52
5.THECANCERWORKFORCECOULDBETTERSUPPORTTHENEEDSOFOLDERPATIENTS
CancerservicesintheUKareexperiencingsevereworkforcegapsacrossmanykeyprofessions,whichishavingarealimpactontheabilitytodiagnoseandtreatcancerquickly,aswellastogivepatientsthebestpossibleexperienceofcare157.
Therearealsobroaderissuesrelatingtothepreparednessoftheworkforcetotreatthegrowingnumberofolderpatients,includingdeficitsineducation,knowledgeandattitudesandinthedevelopmentorspecificrolesandservicesthatmeetolderpeople’sneeds158.Forexample,a2013surveyofUKmedicaloncologytraineesfoundthatonly27.1%wereconfidentinassessingrisktomaketreatmentrecommendationsforolderpatients,comparedto81.4%beingconfidentabouttreatingyoungerpatients159.
Forpeoplewithcomplexneeds,itiscriticalthathealthprofessionalswithspecialistexpertiseareavailabletosupportthemthroughouttreatmentdecision-makingandtreatmentitself.Thereisalsosomeevidenceofbenefitinprovidingadditionalspecialistsupport,targetedtogroupsofolderpeoplewithcomplexneeds,whoareatriskofundertreatment160.
5.1EXPERTISEINTHEMDTAspreviouslydiscussed,just14%ofMDTdiscussionsobservedduringpastCRUKresearchincludedinformationthatdidnotdirectlyrelatetothepatient’stumour161,forexamplecomorbidities,socialneedsortreatmentpreferences.ThisisadirectresultofthegrowingmismatchbetweenanMDT’scapacityandthedemandtheyface,whichleadstoseveretimepressureontheirdiscussions.Thisislikelytohaveaparticularlysignificantimpactonolderpatients,whoaremorelikelytohavecomplexsocialandmedicalneeds.
OneoftheissuesforallMDTsismanagingtocomprehensivelygetthroughthecasesinameaningfulwayinwhichwe[healthcareprofessionals]maketherightselectionof
treatmentstrategieswhenyou’vemaybegot…fortypatientsplusatanMDT.(Clinicaloncologist)
Aswellasaproforma,ensuringanMDTdiscussioniscentredaroundtheneedsofanolderpatientcouldbeensuredbyincludingrelevantspecialistsinthemeeting.However,MDTmembersrespondingtooursurveyexpressedconcernthattheirMDTdidnotroutinelyincludespecialistswhocouldaddvaluetoadiscussionaboutanolderpatient,suchassocialworkers,occupationaltherapists,physiotherapists,dieticians,andpharmacists.
InoneMDTmeetingobservedforthisresearch(SCOPES),onememberofstaff–aleadnurse–attendedthemeeting,representingasmallermultidisciplinaryteamofalliedhealthprofessionalswhohadcompletedacomprehensivegeriatricassessment.TheycouldthenfeedtheresultsoftheassessmentbacktotheMDTandsuggesttheimplicationsfortreatment,andlikewisecouldfeedtheMDT’srecommendationbacktotheirteamofalliedhealthprofessionals.
AdvancingCare,AdvancingYears 53
Inanothersite,ajointsurgical-oncologyclinichadbeenestablishedsothatpatientscouldseeboththesurgeonandanoncologistforafullycomprehensivediscussiontocomparesurgicaloptionswithradiotherapyandchemotherapy.Thiswasintroducedtopreventpatientsbeingrecommendedforsurgery,foundtobeunfitandthenhavingtowaitagaintostartradiotherapy.Inthiscase,thecliniciansfounditvaluabletobounceideasoffeachotherwhenfinalisingtheirplans.
…wealwaystakeanotheropinion…wedon’thesitatetoringorevenbecausewehavetwoofusdoingtheclinicalwayspopinnextdoorandsaythisiswhatIthinkand
withthisinformationIamgivingdoyouthinkitisthatordoyouthinkdifferently?(Anaesthetist)
5.2SPECIALISTCANCERNURSESClinicalNurseSpecialists(CNS)playanimportantroleincancercare,supportinggoodpatientexperience162andactingasa‘keyworker’throughoutdiagnosis,treatmentdeliveryandpalliativecare163.Assuch,appreciationofCNSswasraisedconsistentlythroughoutthisresearch.
Theolderpeoplewithcancersurveyedgenerallyreportedthattheyhadbeenwellsupportedbyhealthprofessionals,withspecialistnursesparticularlyappreciated.Nurseswerealsorecognisedfortheirroleinprovidingpracticaladviceaboutmanagingtheirtreatment.
TheconsultantmadeclearnotesthatIcouldtakeaway.Thespecialistnursesfollowedupwithclearandnecessaryadvice.(apatient)
However,thiswasnotuniform–reflectingthesignificantchallengesfacedwithCNSstaffing.Thisisaconcern–the2015CancerStrategyforEnglandrecommendedthatallpeoplewithcancershouldbegivenanamedCNSorkeyworkercontact164;thisisalsoincludedinNICEguidelines.
WhenIwasfirstdiagnosed7yearsagotherewasnoCNSinhaematologyatourlocalhospitalanduntilIwasreferredelsewhere,Ididn'trealisetheseamazingnurses
existed.Fortunately,wehaveawonderfulCNSnowwhoisavailablebyphoneore-mailwheneverneeded.(apatient)
WhilsttheproportionofpatientsinEnglandhavingaccesstoaCNShasrisenfrom84%in2010to90%in2016165,thereisstillroomforimprovementandstillvariationacrossgeographiesandacrossdifferentcancersites.84%ofpatientsinScotlandreportedaccesstoaCNSin2015/16166;inWalesin2016,81%reportedaccessandinNorthernIrelandin2015,thisfigurewasjust72%.Staffingissueswerealsorecognisedbynationalinterviewees,withthisseenasaparticularchallengeforrarercancers.
Imeanthecancernursesarefantasticwheretheyexistandpatientsaredirectedtothem,that’sgreat.Theproblemisthattheytendtobethereforthebigger,more
commoncancers,sothecolorectalteamsareoftenfantastic,thebreastcancerteamsarefantastic.Butwhereit’smoreunusualcancersorwherethecancerseemstobe
moreofasuperficialthing,ImeanIcomeacrossthislessforskincancerthingsorlessforsomeoftheothergynaecologicalcancers.Frequentlythere’sjustoneofthese
nursesinateamandthereforeoncethey’reonholidayorthey’resickthere’snobackup,there’snothingelse,there’snobodyelsewhocanstepin.(NationalInterviewee)
AdvancingCare,AdvancingYears 54
ThishasanimpactontheabilityofaCNStosupportpatientsadequately.Forexample,pastresearchhasshownthatoverhalfofprostateCNSsfelttheydidn’thavethetimetoattendtotheholisticneedsandpsychosocialassessmentrequirementsoftheirroles167.
Furthermore,theroleofaCNSishighlyvariableandthejobtitleandexpectationscanbeinconsistent168.CNSsoftenfillservicegapsintheirlocalcentres,ratherthandoingtheworkthatbestfitstheirexpertise.AsurveyfromCRUKresearchintothenon-surgicaloncologyworkforcefoundthat50%ofCNSsdidnotfeeltheyhadenoughpatient-facingtimeandwereconsistentlyworkinganaverageof5additionalhourseachweek–onaverage,15%oftheirworkinghours.
Recommendation:HealthEducationEngland,anditsequivalentsinthedevolvednations,shouldusetheCancerResearchUK‘bestpracticetreatmentmodel’toprojectrequiredworkforcenumbersbasedonpatientdemand,notonaffordability.Organisationsshouldalsoconsiderthespecificneedsofolderpeoplewithcancerinallworkforceplans.
Recommendation:GovernmentshouldprovideinvestmenttosupportHealthEducationEngland’sphase2cancerworkforceplan,whichwillsayhowmanystaffwillneedtobetrainedandemployedtodelivereffectivecancercarebeyond2021.
5.3GERIATRICIANSIntervieweesacrossprimaryandsecondarycarealsoraisedthepotentialbenefitofinvolvingelderlycarespecialists.GPscommentedthatiftherewereconcernsaroundfrailtyandanolderperson’scapacitytowithstandinvestigativetests,theywouldseekfurtheradvicefromlocalelderlycarespecialistsorgeriatricconsultants.Thesemeasurestoavoidsimple‘non-referral’maybeimportantstepsinthepathwaytoimproveaccesstotreatmentforolderpeople.
IftheyareveryfrailIwouldaskfora[geriatric]consultantreviewratherthansendforinvasivediagnostictests(GeneralPractitioner)
WhilstMDTmembersreportedthatitwasnotthenormforgeriatricianstoattendMDTmeetings,someintervieweesnotedthattheywereabletoreferpatientstoageriatrician.However,fewhaddonethisinpracticeandthevalueofthiswascontested.
…wouldn’tactuallythink[a]CareoftheElderlyphysicianwouldknowverymuchaboutlunghealthorhowthatfeedsintoourabilitytogiveradicaltreatments…Icouldseethevalueoftheyknewthepatientandtheyhadsomethoughtsabouttheirwishesor
theirhomecircumstancesorthingsthatyoucoulddotoimprovetheperformancestatus.(Clinicaloncologist)
However,otherssawincreasingvalueininvolvinggeriatriciansintreatmentdecision-making;inasimilarwaytohowpalliativecarehasbeenrecognisedandexpandedoverrecentyears.
Manyyearsagotherewasalittlebitofpalliativemedicineandafewpalliativecarephysiciansandnopalliativecarenurses–whereisthereahospitalnowwithoutone,ortwo,orthreeorfour?It’sallgrownupandmyfeelingwouldbethatintimewe’llseeasimilarthingforolderpeople–there’llbeleadersforthatineachdepartment.’
(NationalInterviewee)
CurrentevidencesuggeststhatCGAsshouldbeledbyelderlycarespecialists,aspartofa

AdvancingCare,AdvancingYears 55
multidisciplinaryteam.Forexample,theMacmillan/DepartmentofHealthOlderPersonsPilotdemonstratedthatgeriatricianliaisonwasthemosteffectivewayofdeliveringCGA169.Otherresearchhasalsohighlightedthevalueofincludingelderlycarespecialistsincancerdecision-making,althoughitdoesnothappenroutinely.
Elderlycarespecialistsareexperiencedinco-managingmultiplehealthconditionsandpolypharmacy,aswellasengagingandmobilizingarangeofcommunity-basedhealthandsocialservicestoprovidepracticalsupport,buttheyarerarelyinvolvedindecision-
makingrelatedtocancertreatment.(Maher2016170)
Thereareanumberofinitiativeswhichseektoembedinputfromelderlycarespecialistsintocancertreatmentdecision-making.Forexample,NottinghamUniversityHospitalhaveageriatrician-ledCGAprocessthatfeedsdirectlyintoMDTmeetings(seeSCOPESexampleinsection2).
AdvancingCare,AdvancingYears 56
6 WENEEDTOIMPROVEHOWINNOVATIONINTREATMENTANDCAREREACHESOLDERPEOPLEWITHCANCER
Researchisthekeytoimprovingoutcomesforallpeopleaffectedbycancer.However,olderpatientsaretypicallyunder-representedinclinicaltrials171,whichcanhavestrictinclusioncriteriabasedonchronologicalage,comorbiditiesorcognitiveability.Thesefactorscombinedmeanthatthereisoftenrelativelylimitedevidenceonthespecificeffectsoftreatmentonolderpatients.Thismeansthatdecisionsabouttreatmentforpatientswithcomorbidities–andthereforeoftenolderpatients–cannotalwaysbebasedonstrongevidence.Atleast,notincomparisontodecisionsfortheiryoungerorotherwisefittercounterparts.
6.1 OLDERPATIENTSAREUNDER-REPRESENTEDINCLINICALTRIALS
Olderpeopleareingeneralunder-representedinclinicaltrials172,includingincancer173.Thisisparticularlyacutelyfeltfor“olderoldpatients”,whoaretypicallythemostfrailandcomorbid.Thiswasalsorecognisedbyourclinicianinterviewees:
Themostimportantthingiswedon’thaveanyevidenceforsuchpatients…thenumberofpatientswhoare[in]clinicaltrialsabove75yearsofageisfarandfew
betweenandnomeaningfulconclusionscanbemadeonthat.(Medicaloncologist)
Thediscrepancybetweenatrialpopulationanda“real”clinicalpopulationhasmajorimplicationsforhowapplicableevidencefromclinicaltrialsisintheclinic.Olderpatientscanrespondverydifferentlytotreatment,duetoarangeoffactors174.Forexample,age-relatedphysiologicalchangescanimpacthowadrugworksinthebody.Olderpatientsmayalsoexperiencedifferentorworseside-effects,whichmaynothavebeenpredictedfromtheyoungertrialpopulation.TheeffectofthiswassummarisedbyanexpertcommitteeoftheEuropeanMedicinesAgency:“thedrugsweareusinginolderpeoplehavenotbeenproperlyevaluated”175.
Morecouldstillbedonetogatherevidence,includingboostingnumbersofolderpatientsintrials–butalsodoingresearchthatenablespatientswithcomorbiditiesorfrailtytoreceiveoptimaltreatment,thataccountsfortheimpactofcomorbiditiesandfrailty.
Thereareseveralreasonsforthisunder-representation;thesearemostlyacombinationofstringenteligibilitycriteriaandconcernsfromcliniciansaboutsubjectingolder–orfrailer–patientstorigoroustreatment.Therearealsoothercomplicatingfactors,forexamplechallengesingaininginformedconsentfrompatientswithcognitiveissues,ordifficulty

AdvancingCare,AdvancingYears 57
assessingoutcomesinpatientswhoalreadyhaveseveralcomorbidities176.Furtherpracticalfactorsalsoexist,forexampletheinaccessibilityoftrialconsentforms177.
Thereisappetiteforchange:70%ofEuropeanhealthprofessionalsrespondingtothePREDICTstudyin2014didnotdidnotbelievethepresentarrangementsforclinicaltrialsrelatingtoolderpeopletobesatisfactory,and60%believedthateitherEuropeanornationalregulationofclinicaltrialsshouldbeamendedtoensuregreaterrepresentationofolderorlessfitpatients178.Therehavealsobeeneffortstoaddressthis,forexampletheEMA’s2011GeriatricMedicinesStrategy179ortheEU-fundedPREDICTinitiative(IncreasingtheParticipationoftheElderlyinClinicalTrials),whichproposeswaysofboostingrecruitmentofolderpatientstoclinicaltrials.
Inclusionofageriatricpatientgroupmayalsoaddtothevariabilityofanyendpoint,potentiallyresultingindecreasedeffectsifthestudyisnotadequatelypowered.Thismayresultinaneedforlargerstudiesofincreasedcomplexityandlikelylongerdrugdevelopmenttimelines,unlessalternativeapproachesarealsoconsidered(includingpost-authorisationdatacollection,asdiscussedinthenextsection).
MostclinicaltrialsfundedbyCancerResearchUKdonothaveanupperagelimit,whenagelimitsareapplied,researchersareaskedtojustifytheboundaryselected.Exclusioncriteriarelatingtocomorbiditiesorpatientfitnessareusedinsometrialswheretheyriskconfoundingresultsoraddingasafetyrisk,however,andcomorbiditiesdoincreasewithage.CRUKalsofundsometrialsthataskspecificquestionsabouttreatmentforolderpatients,orpatientswhoarelessfit.
Recommendation:Researchfundersshouldexplorehowtoensuremoreproportionaterecruitmentofolderpeoplewithcancerintoclinicaltrials,andhowtoensurethatresearchaddressesanyevidencegapsintheeffectivenessoftreatmentinolderpatients,orthosewithcomorbiditiesmorebroadly.
6.2 APPROVINGNEWTREATMENTSAswellasreviewingclinicaltrials,thereisscopeformakingchangestotheprocessofapprovingnewtreatmentssothatitbettersupportsolderpeoplewithcancerbygatheringmoreevidencethatappliestothosepatients.Thisshouldincludeembeddingthepatientperspectiveinapprovals,butalsoconsiderationofhowtheprocesscouldincorporateevidenceofatreatment’seffectivenessinamorevariedpatientpopulation–oratleastincludingmoreflexiblecriteriaindrugassessments.
35%ofrespondentstooursurveyofMDTmembersfeltthatalackofclinicalevidenceabouttheefficacyoftreatmentinanolderpopulationwasabarriertotreatment.Thisisparticularlyproblematicincancerswherethereisapoorerunderstandingofthediseaseanditsprogression,andthiscanmakeitdifficultforclinicianstoassesstherisksoftreatmentandtoweighthatupagainstthepotentialbenefittothepatient.However,thisislikelypartofabroaderissueaboutevidenceincomorbidpopulations,ratherthanbeingrelatedsolelytochronologicalage.
Thereisalsoscopeformakingchangestotheprocessofapprovingnewtreatmentssothatitbettersupportsolderpeoplewithcancer,whomayvalueoutcomesotherthanjustimprovingsurvival–suchasmaintainingagoodqualityoflife,theirindependenceandcognition180.For
AdvancingCare,AdvancingYears 58
example,nationaldrugapprovalsshouldconsiderincorporatingabroaderrangeofevidence,includingimpactonqualityoflife–whichwasrecommendedintheLifeSciencesIndustrialStrategy181,althoughtherecommendationswerenotspecificallytargetedtowardsolderpatients.
Inthelongerterm,weencourageUKhealthservicestoexploretheuseofflexiblepricingmechanismssuchasoutcomes-basedpricing,inwhichthepriceofadrugcanbereviewedatagreedstagesandaligneddirectlytopatientbenefit,beingincreasedordecreasedbasedonemergingnewdata.Thiswouldensurepricingandaccessdecisionsaregroundedintherealexperiencesofpatients.Totakethisforward,CancerResearchUKareexploringthefeasibilityofoutcomes-basedpricingthroughacommissionedresearchproject,inpartnershipwiththeGreaterManchesterHealthandSocialCarePartnership.
6.2.1 HIGH-QUALITYDATAAkeyenablertothisisrobust,routinelycollecteddataaboutcancertreatmentandoutcomes.Thisisnotanage-specificissueasitwouldsignificantlyimproveourabilitytounderstandtheeffectsoftreatmentonallpatients.AllUKorganisationsresponsibleforcollectinghealthdatashouldensuresignificantresourceisprovidedforimprovingthequalityandcompletenessoftreatmentsdatasets.Havingrobustdataabouttreatmentsandoutcomeswouldenablemorein-depthanalysesoftheextentofvariationinaccesstotreatmentandoutcomesforolderpatients,whichcouldsupplementclinicaltrialdataandsupporteffortstobenchmarkservices.
Recommendation:Nationaldrugappraisalbodiesshouldexplorewhatalternativemetricscouldbeconsideredduringappraisalsthatwouldbemorerelevanttoallpatients,includingolderpatients–suchasqualityoflifeandactivitiesofdailyliving.
AdvancingCare,AdvancingYears 59
APPENDIX1:METHODOLOGYRAPIDEVIDENCEASSESSMENTTheresearchbeganwitharapidevidenceassessment(REA),focussedontheidentificationofevidencetodirectandrefinetheresearchdesign.InitialsearcheswereundertakenbyHSMC’sspecialistlibraryanddocumentswereidentifiedviathefollowingdatabases:SocialScienceCitationIndex;Ageinfo;ASSIA;HMIC;Medline;Embase;Cinahl;SocialCareOnline.Whereparticularlyrelevantliteraturewasidentifiedinthisreview,additionalsearcheswereconductedofthereferencelistsofthosedocuments.
SURVEYSThreesurveyswerecarriedout,gainingatotalof197responses.Eachsurveygatheredquantitativeevidenceusingfixedresponsequestionsbutalsocontainedanumberofopenendedquestionsforfreetextresponses.Quotationsfromthesefreetextsurveyresponseshavebeenusedthroughoutthereport.Toachieveawidereachforbothofthesesurveys,a‘snowballing’approachwasalsoemployed,withrecipientsencouragedtosharethesurveylinkwiththeircolleaguesandcontacts.
Fulltextofsurveysisavailableonrequest.Thesurveyswereasfollows:
Primarycaresurvey:thisfocusedonhowprimarycarerespondstoolderpeoplewithsuspectedcancer,particularlywhatinformationispassedonforconsiderationatthepointofreferralandhowtheroleofprimarycareincancercaremaydevelopinfuture.Wereceived98responsestothesurvey.ThesurveywasdesignedwithinputformMacmillanCancerSupportandpilotedwith12MacmillanGPswhosharedfeedbackonboththedesignandcontentofthesurvey.ThesurveywasdistributedthroughMacmillanGPs,Doctors.net,CancerResearchUKprimarycarefacilitatorsandengagementteamandtheRoyalcollegeofGPs.
MDTsurvey:thisfocusedonwhatinformationandassessmentsarebeingusedtomaketreatmentrecommendations,andwhatsubsequentdecision-makingsupportisofferedtoolderpeople.ThesurveywasdistributedthroughnetworksofvariousRoyalColleges.Wereceived57responsestothesurvey.
Patientsurvey:apatientsurveywasdesignedtounderstandtheexperiencesandperspectivesofolderpeoplewhohavebeentreatedforcancerandhowtheycontributetotheirtreatmentdecisions.Thesurveydesignwasledbyourco-researchers.DistributionwasthroughCancerResearchUK’spatientinvolvementnewsletterandwebpages,CancerChatandMacmillaninvolvementnetwork.
INTERVIEWSANDOBSERVATIONSTheexperiencesandviewsofnationallevelintervieweeswerecapturedininterviews,withrepresentationacrossallUKcountriesfromrepresentativesofRoyalCollegesandprofessionalorganisations,researchersandpolicymakers.Sevenlocalcasestudiesexploredtheviewsofhealthprofessionalsinvolvedinthetreatmentdecisionmakingprocess.Atalocallevel,interviewswerecarriedoutwithMDTmembers,staffwhowereinvolvedin
AdvancingCare,AdvancingYears 60
assessingandsupportingbutnotinvolvedinMTDs(AHPsandanaesthetists)andprimarycarestaff.Twodevolvednationswillberepresentedinthissample.
Itshouldbenotedthatthisstudysampledcasestudysitestocapturepracticerepresentativeofcancerservicesforallolderpeople,ratherthantoidentifybestpractice.Assuch,includinginnovationwasjustoneaspectofsiteselection,alongside:distinctiveolderpopulationdemographics;BMEpopulations;ruralpoverty;arangeofcancertypes;primary,secondaryandtertiaryservices;andinclusionofdifferentstaffgroups(radiologists,anaesthetistsetc.).
Semi-structuredinterviewswereundertakenatcasestudysiteswith40healthprofessionals.Separatetopicguidesweredesignedforstaffprimarycareandacutesettings.Topicguideswereinformedbytheevidencereviewfindingsandaimedtopickuponthesurveythemesandexplorethemingreaterdepth.Allinterviewswerecarriedouteitherface-to-faceorbytelephone,aftergainingparticipants’consent.
Threeobservationswereundertaken;twoMDTmeetingsandahalfdaymultidisciplinaryclinic.Non-participativeobservationcanbeavaluableunobtrusivemethodofdatacollectionandcanhelptoprovidecontextandaricherunderstandingofinteractionandthenatureofservices.Theresearchteamdesignedasetofobservationalcuesthataddressedtheirresearchquestionsandtopicdirectly.
Allinterviewswererecordedandtranscribedtoallowforthematiccodingandanalysis.Observationalnoteswereincorporatedintotheanalysis.Thisinvolvestheinitialidentificationofanalyticalthemesderivedfromtheresearchquestionsandtheliterature,towhichadditionalthemesareaddedasnewinsightsemergefromthedata.Thevalueofthisapproachisthatitisparticularlywellsuitedtotheproblem-orientednatureofappliedandpolicyrelevantresearch,whilstalsoallowingforananalyticalprocesswhichremainsgroundedinanddrivenbyparticipants’accounts.
PATIENTINVOLVEMENTRecognisingthesignificanceofpatientsandcarersinthedecision-makingprocess,wealsorecruitedagroupofsevenolderpeopleaffectedbycancerasco-researchers.Acrossthreehalf-dayworkshops,thisgroupdesignedapatientsurveyandprovidedguidanceontheinterpretationoffindings,addinganessentialperspectivetoouroverallanalysis.
AdvancingCare,AdvancingYears 61
APPENDIX2:PATIENTMESSAGESTOTHENHS
Thefollowingmessageswerecontributedbytheolderpeopleconsultedforthisresearch.
‘WhatdoyouwanttosaytotheNHSaboutinvolvingolderpeopleintreatmentdecisionsaboutcancer?’
Alotofolderpeopledon'tunderstandthetreatmentssoexplainingthemallhelps.Andgivingoptionsandsomepamphletsabouttypesoftreatmentcanmakethemfeelbetter.
Ageisjustanumber!Whatshouldhappenforeverypatientwithcancerisafullexplanationofthediagnosisandthetreatmentoptions,includingnotreatmentifthatisappropriate,andhelpinmakingthatdecision.
Beclearabouttheafter-effectsandwhatsupportcouldbeavailableiflivingonown.Offerinformationthathelpscopewiththetraumaofbeingtoldandhowtomanagepost-op.
Bethoughtful,patientandkind.
Clearexplanationsofrisks/sideeffectsandbenefitsoftheparticulartreatment.Possibleoptionsofothertreatments.Patientandfamilytofeelsupportedduringandimportantlyafterdecisionmaking.
Clearsupportivecommunication.
Don'tpatroniseanddon'tmakeassumptions!
Employenoughstafftomakeconsultationslesshurried.Itwouldbehelpfultoseethesamedoctoreachtime,thoughIknowthisisnexttoimpossible.Atleastithelpsiftheyhaveactuallyreadyournotesbeforeyougetinthere.
Encouragethemtobringsomeonealongtoappointmentsandtreatment.Askfortheiropinions,listentothem,respondtotheirquestions.Don'tbepaternalistic.Makesuretheyhaveallthehelptheyneedathomeandhelpwithtransporttohospital.Introducethemtolocalsupportgroups.
Giveaccesstoasmuchinformationaspossibleabouteffects
Givethemaclearchoicei.e.WecandoAforyou,orBforyou,orC,foryou.Oracombinationofthem.SadlyatthemomenttheconsultantTELLSthepatientwhatisgoingtohappen,offeringthepatientnochoice.
Givethemenoughinformationintermsordinarynon-medicalpeoplecanunderstand.IhadthingsgiventomeinLaymen’sterms,butIdoknowofsomepeoplewherethemedicaljargonwasusedandunderstandablytheygotveryconfused.
Iam68andIcouldnothavewantedabetterDreverythingwasexplainedsoIunderstood
Ifeelalladultsshouldbeinvolvedintreatmentdecisionwhateverageapatientis
Ifindthisquestionratheroffensive,aswellasgrammaticallyflawed.Thequestionseemstoconfuseandconflatebeingagedover55withhavingmentalcapacityissues."Olderpeople",likeanyotheragegroup,requireaccurate,unbiased,objectiveinformation-including
AdvancingCare,AdvancingYears 62
potentialsideeffectsandaveragesurvivaltimeswithandwithouteachtreatment-inordertomakeinformeddecisionsabouttheirtreatment.Peoplewithmentalcapacityissues,regardlessoftheirage,mayneedsuchinformationtobepresentedinamoreeasilyunderstoodformat-inlinewiththerequirementsoftheMentalCapacityAct2005.
Ihavebeentreatedwithrespectduringmytreatment,butaftercaresupportcouldbeimproved.
IhavenothingbutpraisefortheNHSandthewayourhospitalinvolvesolderpatientsintheirtreatment.
Ireallythinkit'simportanttostressthesideeffectsofsurgery,radiotherapyandchemo.UnfortunatelypeoplewatchtheTVwherethesideeffectsarebrushedunderthetable.Theonlyissueseemstobelosingyourhair!Fore.g.theabilityofa40yearoldtorecoverfromamastectomyisgoingtobebetterthanan85yearold.Alsothingslikeneuropathyarenotcoveredatall.12yearssincemyfirsttrancheofchemoandIstillhavequitepainfulneuropathyinmyfingers.MysisterfinishedchemoandradiotherapyinFebruaryandhaslostallfeelinginherfootandiseffectivelyverydisablednow.Shehasbeentoldherfootmayneverrecover.Noonetoldherthis.Also,thereareNOrehabilitationservices,noMacmillaninmanypartsofthecountry.Soafitveryelderlypersonwillrecoverfromsurgery,butifyou'vespentthelast30yearssittinginachairandwatchingtellythenyouwon'trecoveratall.
Involvethemallalongtheway.
Itiscrucialtodoso.Itmaybethefirsttimethepersonhasnotbeenincontrolandadegreeofpatientinfluenceisessential.
AdvancingCare,AdvancingYears 63
REFERENCES1SmittenaarCR,PetersenKA,StewartK,MoittN.(2016)CancerIncidenceandMortalityProjectionsintheUKUntil2035.BritJCancer115,1147-1155.Availableat:https://go.nature.com/2KJNfGk(AccessedMay2018)2Coleman,M.P.etal,ICBPModule1WorkingGroup(2011)CancersurvivalinAustralia,Canada,Denmark,Norway,Sweden,andtheUK,1995–2007(theInternationalCancerBenchmarkingPartnership):ananalysisofpopulation-basedcancerregistrydata.TheLancet,vol377,no9760,pp127–38.Availableat:http://bit.ly/2jouEWS(AccessedFebruary2018)3Berrino,F.etal(2007)‘SurvivalforeightmajorcancersandallcancerscombinedforEuropeanadultsdiagnosed1995–99:resultsoftheEurocare-4study’.TheLancetOncology,vol8,pp773–83.Availableat:http://bit.ly/2EJXfQR(AccessedFebruary2018)4WoodsLM,RachetB,O’ConnellD,LawrenceG,TraceyE,WillmoreA,ColemanMP(2009).‘LargedifferencesinpatternsofbreastcancersurvivalbetweenAustraliaandEngland:acomparativestudyusingcancerregistrydata’.InternationalJournalofCancer,vol124,no10,pp2391–9.Availableat:http://bit.ly/2oeTIQ4(AccessedFebruary2018)5Foot,C.etal(2011),Howtoimprovecancersurvival:explainingEngland’srelativelypoorrates,TheKing’sFund,June2011.Availableat:http://bit.ly/2CB8epz(AccessedFebruary2018)6IndependentCancerTaskforce(2015)Achievingworld-classcanceroutcomes:astrategyforEngland2015-2020.London:IndependentCancerTaskforce.Availableat:http://bit.ly/1Idwf5W(AccessedJune2018)7Ibid.8Bridges,J.andSimcock,R.(2017)Guesteditorial:Meetingtheworkforcechallengesforolderpeoplelivingwithcancer.InternationalJournalofNursingStudies65(2017)A1-A2.Availableat:https://bit.ly/2y61hQf(AccessedJune2018)9SmittenaarCR,PetersenKA,StewartK,MoittN.(2016)CancerIncidenceandMortalityProjectionsintheUKUntil2035.BritJCancer115,1147-1155.Availableat:https://go.nature.com/2KJNfGk(AccessedMay2018)10Quaresma,M.,Coleman,M.P.andRatchet,B.(2015)40-yeartrendsinanindexofsurvivalforallcancerscombinedandsurvivaladjustedforageandsexforeachcancerinEnglandandWales,1971-2011:apopulation-basedstudy.Lancet.2015,28,285(9974).Availableat:https://bit.ly/2sSZXLC(AccessedJune2018)11DeAngelis,R.etal(2014)CancersurvivalinEurope1999-2007bycountryandage:resultsofEUROCARE--5-apopulation-basedstudy.LancetOncol.,2014.15(1):23-34.Availableat:https://bit.ly/2LK6qja(AccessedJune2018)12NationalCancerIntelligenceNetwork(2015)Olderpeopleandcancer.NCIN,June2015.Availableat:https://bit.ly/12NFOXb(AccessedJune2018)13NCIN(2015)RoutestoDiagnosis:exploringemergencypresentations,2012-2013workbook.NationalCancerIntelligenceNetwork,February2018.Availableat:http://bit.ly/1OelnIH(AccessedJune2018)14PublicHealthEnglandandCancerResearchUK(2015),Majorresectionsbycancersite,inEngland;2006to2010shortreport.NationalCancerIntelligenceNetwork,June2015.Availableat:http://bit.ly/15Sy6gH(AccessedFebruary2018)15NHSEnglandNationalCancerQualityInitiativeandABPIPharmaceuticalOncologyInitiative(2013)Areolderpeoplereceivingcancerdrugs?Ananalysisofpatternsincancerdrugdeliveryaccordingtotheageofpatient.NHSEnglandandabpi,December2013.Availableat:https://bit.ly/2BE3d2R(AccessedMay2018)16Ahmat,N.(2012)Accessallages:assessingtheimpactofageonaccesstosurgicaltreatment.RoyalCollegeof
Surgeons,October2012.Availableat:http://bit.ly/2sM6s5c(AccessedFebruary2018)17PublicHealthEnglandandAssociationofBreastSurgery(ABS)(2015)Anauditofscreendetectedbreast
cancersfortheyearofscreeningApril2013toMarch2014.AssociationofBreastSurgery,June2015.Availableat:http://bit.ly/2ofWGUx(AccessedFebruary2018)
18Raine,R.,etal.,Socialvariationsinaccesstohospitalcareforpatientswithcolorectal,breast,andlungcancerbetween1999and2006:retrospectiveanalysisofhospitalepisodestatistics.BMJ,2010.340:p.b5479.Availableat:http://bit.ly/2EIcZUp(AccessedFebruary2018)19Ahmat,N.(2012)Accessallages:assessingtheimpactofageonaccesstosurgicaltreatment.RoyalCollegeofSurgeons,October2012.Availableat:http://bit.ly/2sM6s5c(AccessedFebruary2018)20MacmillanCancerSupport,AgeUKandtheDepartmentofHealth(2012)CancerServicesComingofAge:LearningfromtheImprovingCancerTreatmentAssessmentandSupportforOlderPeopleProject.MacmillanCancerSupport,December2012.Availableat:http://bit.ly/2HyaHVB(AccessedFebruary2018)

AdvancingCare,AdvancingYears 64
21TheNationalCancerEqualityInitiative(NCEI)andPharmaceuticalOncologyInitiative(2012)Theimpactof
patientageonclinicaldecision-makinginoncology.DepartmentofHealth,2012.Availableat:http://bit.ly/2Fjfvxr(AccessedFebruary2018)
22Lavelle,K.,etal.,IslackofsurgeryforolderbreastcancerpatientsintheUKexplainedbypatientchoiceorpoorhealth?Aprospectivecohortstudy.BritishJournalofCancer,2014.110(3):p.573-583.Availableat:https://www.nature.com/articles/bjc2013734(AccessedFebruary2018)
23Ring,A.,Theinfluencesofageandco-morbiditiesontreatmentdecisionsforpatientswithHER2-positiveearlybreastcancer.CritRevOncolHematol,2010.76(2):p.127-32.Availableat:http://bit.ly/2Gzg5GJ(AccessedFebruary2018)24PerezDeCelis,E.S.etal,June2018.Patient-definedgoalsandpreferencesamongolderadultswithcancerstartingchemotherapy(CT).In:ASCO,June2018,ChicagoUSA.Availableat:https://bit.ly/2JMPFqa(AccessedJune2018)25Lycke,M.,Ketelaars,L.,Boterberg,T.,Pottel,L.,Pottel,H.,Vergauwe,P.,Goethals,L.,VanEygen,K.,Werbrouck,P.,Debruyne,D.,Derijcke,S.,Borms,M.,Ghekiere,V.,Wildiers,H.andDebruyne,P.(2014)'ValidationoftheFreundClockDrawingTestasaScreeningTooltoDetectCognitiveDysfunctionsinElderlyCancerPatientsUndergoingComprehensiveGeriatricAssessment',Psycho-oncology,23,pp.114-114.https://www.ncbi.nlm.nih.gov/pubmed/24729471[accessedFebruary2017]26Bridges,J.Hughes,J.Farrington,N.etal(2015)Cancertreatmentdecision-makingprocessesforolderpatientswithcomplexneeds:aqualitativestudy.BMJOpen2015;5.Availableat:https://bit.ly/2LK3oLG(AccessedJune2018)27Puts,M.T.,Hardt,J.,Monette,J.,Girre,V.,Springall,E.,Alibhai,S.M.(2012)Useofgeriatricassessmentforolderadultsintheoncologysetting:asystematicreview.JNatlCancerI,104(15),pp.1133–1163.Availableat:http://bit.ly/2CAYwDN(AccessedFebruary2018)andPuts,M.T.E.,Santos,B.,Hardt,J.,Monette,J.,Girre,V.,Atenafu,E.G.,Springall,E.andAlibhai,S.M.H.,(2014)Anupdateonasystematicreviewoftheuseofgeriatricassessmentforolderadultsinoncology.AnnOncol,25(2),pp.307-315.Availableat:http://bit.ly/2EKtLy2(AccessedFebruary2018)28O'Donovan,A.,Mohile,S.G.andLeech,M.(2015)'Expertconsensuspanelguidelinesongeriatricassessmentinoncology',EuropeanJournalofCancerCare,24(4),pp.574-589.Availableat:http://bit.ly/2ogx5Lb(AccessedFebruary2018)29Lycke,M.,Pottel,Letal.(2015)Integrationofgeriatriconcologyindailymultidisciplinarycancercare:Thetimeisnow.EuropeanJournalofCancerCare,24(2)pp.143-146.Availableat:http://bit.ly/2sPunRE(AccessedFebruary2018)30Morris,R.,Cowley,A.,Sims,A.,Pattinson,J.andMasud,T.(2016)DoesComprehensiveGeriatricAssessmentAffectDecisionmaking&OutcomesforOlderAdultstreatedforUpperGastro-intestinalcancer.PosterpresentationtotheSIOGannualconference2016,Milan.EuropeanGeriatricMedicine7S1(2016)S29-S259.Availableat:http://bit.ly/2oneMmC(AccessedFebruary2018)31NCIN(2015)RoutestoDiagnosis,2006-2015workbook.NationalCancerintelligenceNetwork,February2018.Availableat:http://bit.ly/1OelnIH(AccessedMarch2018)32Eastham,R.,Duffy,S.,Foster,C.andBeaumont,A.(2017)DART:anewlookatthe2-weeksuspectedcancerreferralprocess.BritishJournalofGeneralPractice67(665),pp.550.Availableat:https://bit.ly/2rud1pc(AccessedMay2018)33Gray,R.,Gordon,B.andMeredith,M.(2017)Meetingpatient’sneeds:Improvingtheeffectivenessofmultidisciplinaryteammeetingsincancerservices.CancerResearchUK,January2017.Availableat:http://bit.ly/2j3npQf(AccessedFebruary2018)34Blazeby,J.M.etal(2006)Analysisofclinicaldecision-makinginmultidisciplinarycancerteams.AnnOncol17,pp.457-60.http://bit.ly/2gcZ2yz(AccessedMarch2018)35Wood,J.J.etal(2008)Anevaluationoftreatmentdecisionsatacolorectalcancermultidisciplinaryteam.ColorectalDis.10,pp.769-72.http://bit.ly/2fjHHEK(AccessedMarch2018)36Coulter,A.andCollins,A.(2011)Makingshareddecision-makingareality:Nodecisionaboutme,withoutme.TheKingsFund,2011.Availableat:http://bit.ly/2ELPM3m(AccessedFebruary2018)37Kehl,K.L.,Landrum,M.B.,Arora,N.K.,Ganz,P.A.,vanRyn,M.,Mack,J.W.,Keating,N.L.(2015)Associationofactualandpreferreddecisionroleswithpatient-reportedqualityofcare:shareddecisionmakingincancercare.JAMAOncol.1(1),50-8.Availableat:http://bit.ly/2Fku3wz(AccessedFebruary2018)38DaSilva,D.(2012)Helpingpeoplesharedecision-making:areviewofevidenceconsideringwhethershareddecisionmakingisworthwhile.TheHealthFoundation,June2012.Availableat:http://bit.ly/2Ca6oQX(AccessedFebruary2018)39Bridges,J.,Hughes,J.,Farrington,N.&Richardson,A.(2015)Cancertreatmentdecision-makingprocessesfor
AdvancingCare,AdvancingYears 65
olderpatientswithcomplexneeds:aqualitativestudy.BMJOpen5(12).Availableat:http://bit.ly/2HyMU85(AccessedFebruary2018)40Handforth,C.,Clegg,A.,YoungC,etal.(2015)Theprevalenceandoutcomesoffrailtyinoldercancerpatients:asystematicreview.Ann.Oncol.26(6),pp.1091-101.Availableat:http://bit.ly/2CdaTdv(AccessedFebruary2018)41ChenR.C.,RoyceTJ,ExtermannM,etal.(2012)Impactofageandcomorbidityontreatmentandoutcomesinelderlycancerpatients.Semin.Radiat.Oncol.22(4)pp.265–271.Availableat:http://bit.ly/2CBgoya(AccessedFebruary2018)42Broome,S.,Dellot,B.,Lindley,E.,Norris,E.,Rowson,J.Soopramanien,D.andTruch,E.(2012)Improvingdecisionmakinginthecareofolderpeople:Exploringthedecisionecology.JosephRowntreeFoundation,2012.Availableat:http://bit.ly/2HAarFJ(AccessedFebruary2018)43Bridges,J.Hughes,J.Farrington,N.etal(2015)Cancertreatmentdecision-makingprocessesforolderpatientswithcomplexneeds:aqualitativestudy.BMJOpen2015;5.Availableat:https://bit.ly/2LK3oLG(AccessedJune2018)4444Burns,K.,Meredith,M.,Williams,M.,Huxley,C.andPallesen,C.(2017)Fullteamahead:understandingtheUKnon-surgicalcancertreatmentsworkforce.CancerResearchUK,December2017.Availableat:http://bit.ly/2DEVMra(AccessedMarch2018)45Bridges,J.,Lucas,G.,Wiseman,T.etal(2016)PreparednessofUKworkforcetodelivercancercaretoolderpeople:summaryreportfromascopingreview.UniversityofSouthampton,2016.Availableat:46Kalsi,T.,Payne,S.,Brodie,H.etal(2013)AretheUKoncologytraineesadequatelyinformedabouttheneedsofolderpeoplewithcancer?Br.J.Cancer108(10),1936-1941.47Bridges,J.,Lucas,G.,Wiseman,T.etal(2017)Workforcecharacteristicsandinterventionsassociatedwithhigh-qualitycareandsupporttoolderpeoplewithcancer:asystematicreview.BMJOpen2017,7.Availableat:https://bit.ly/2JE6OPC(AccessedJune2018)48QualityHealth(2017)NationalCancerPatientExperienceSurvey.QualityHealth,July2017.Availableat:http://bit.ly/2jZ8Hf1(AccessedFebruary2018)49NHSScotland(2016)ScottishCancerPatientExperienceSurvey2015/16.ScottishGovernment,June2016.Availableat:http://bit.ly/2CaEfJq(AccessedFebruary2018)50MacmillanCancerSupport(2018)CancerWorkforceinEngland:acensusofcancer,palliativeandchemotherapyspecialtynursesandsupportworkersinEnglandin2017.MacmillanCancerSupport,April2018.Availableat:https://bit.ly/2Kqza0j(AccessedMay2018)51Burns,K.,Meredith,M.,Williams,M.,Huxley,C.andPallesen,C.(2017)Fullteamahead:understandingtheUKnon-surgicalcancertreatmentsworkforce.CancerResearchUK,December2017.Availableat:http://bit.ly/2DEVMra(AccessedMarch2018)52Burns,K.,Meredith,M.,Williams,M.,Huxley,C.andPallesen,C.(2017)Fullteamahead:understandingtheUKnon-surgicalcancertreatmentsworkforce.CancerResearchUK,December2017.Availableat:http://bit.ly/2DEVMra(AccessedMarch2018)53Watts,G.(2012)Whytheexclusionofolderpeoplefromclinicalresearchmuststop.BMJ344.Availableat:http://bit.ly/2BJzFkr(AccessedFebruary2018)54Crome,P.,Cherubini,A.andOristrell,J.(2014)ThePREDICT(increasingtheparticipationoftheelderlyinclinicaltrials)study:thecharterandbeyond.ExpertRev.Clin.Pharmacol.7(4)pp.457-468.Availableat:http://bit.ly/2EJJwW5(AccessedFebruary2018)55PerezDeCelis,E.S.etal,June2018.Patient-definedgoalsandpreferencesamongolderadultswithcancerstartingchemotherapy(CT).In:ASCO,June2018,ChicagoUSA.Availableat:https://bit.ly/2JMPFqa(AccessedJune2018)56Bell,J.(2017)Lifesciences:industrialstrategy.OfficeforLifeSciences,August2017.Availableat:http://bit.ly/2wRQJms(AccessedMarch2018)57SmittenaarCR,PetersenKA,StewartK,MoittN.(2016)CancerIncidenceandMortalityProjectionsintheUKUntil2035.BritJCancer115,1147-1155.Availableat:https://go.nature.com/2KJNfGk(AccessedMay2018)58Quaresma,M.,Coleman,M.P.andRatchet,B.(2015)40-yeartrendsinanindexofsurvivalforallcancerscombinedandsurvivaladjustedforageandsexforeachcancerinEnglandandWales,1971-2011:apopulation-basedstudy.Lancet.2015,28,285(9974).Availableat:https://bit.ly/2sSZXLC(AccessedJune2018)59DeAngelis,R.etal(2014)CancersurvivalinEurope1999-2007bycountryandage:resultsofEUROCARE--5-apopulation-basedstudy.LancetOncol.,2014.15(1):23-34.Availableat:https://bit.ly/2LK6qja(AccessedJune2018)60NationalCancerIntelligenceNetwork(2015)Olderpeopleandcancer.NCIN,June2015.Availableat:https://bit.ly/12NFOXb(AccessedJune2018)
AdvancingCare,AdvancingYears 66
61NCIN(2015)RoutestoDiagnosis:exploringemergencypresentations,2012-2013workbook.NationalCancerIntelligenceNetwork,February2018.Availableat:http://bit.ly/1OelnIH(AccessedJune2018)62NCIN(2015)RoutestoDiagnosis,2006-2015workbook.NationalCancerintelligenceNetwork,February2018.Availableat:http://bit.ly/1OelnIH(AccessedFebruary2018)63Foot,C.etal(2011),Howtoimprovecancersurvival:explainingEngland’srelativelypoorrates,TheKing’sFund,June2011.Availableat:http://bit.ly/2CB8epz(AccessedFebruary2018)64PublicHealthEnglandandCancerResearchUK(2015),Majorresectionsbycancersite,inEngland;2006to2010shortreport.NationalCancerIntelligenceNetwork,June2015.Availableat:http://bit.ly/15Sy6gH(AccessedFebruary2018)65Ahmat,N.(2012)Accessallages:assessingtheimpactofageonaccesstosurgicaltreatment.RoyalCollegeof
Surgeons,October2012.Availableat:http://bit.ly/2sM6s5c(AccessedFebruary2018)66PublicHealthEnglandandAssociationofBreastSurgery(ABS)(2015)Anauditofscreendetectedbreast
cancersfortheyearofscreeningApril2013toMarch2014.AssociationofBreastSurgery,June2015.Availableat:http://bit.ly/2ofWGUx(AccessedFebruary2018)
67Raine,R.,etal.,Socialvariationsinaccesstohospitalcareforpatientswithcolorectal,breast,andlungcancerbetween1999and2006:retrospectiveanalysisofhospitalepisodestatistics.BMJ,2010.340:p.b5479.Availableat:http://bit.ly/2EIcZUp(AccessedFebruary2018)68Patel,N.,etal.,Variationintheuseofchemotherapyinlungcancer.BrJCancer,2007.96(6):p.886-90.Availableat:http://go.nature.com/2FkFRPG(AccessedFebruary2018)69Rich,A.L.,etal.,Howdopatientandhospitalfeaturesinfluenceoutcomesinsmall-celllungcancerinEngland?BrJCancer,2011.105(6):p.746-52.Availableat:http://go.nature.com/2ohbX7m(AccessedFebruary2018)70NHSEnglandandABPI(2013)Areolderpeoplereceivingcancerdrugs?Ananalysisofpatternsincancerdrug
deliveryaccordingtotheageofpatient.NHSEngland,December2013.Availableat:http://bit.ly/2HBWaYT(AccessedFebruary2018)
71Ibid.72Ring,A.,etal.,InfluenceofComorbiditiesandAgeonRiskofDeathWithoutRecurrence:ARetrospective
AnalysisoftheArimidex,TamoxifenAloneorinCombinationTrial.JournalofClinicalOncology,2011.29(32):p.4266-4272.Availableat:http://bit.ly/2CbdnJo(AccessedFebruary2018)
73PublicHealthEnglandandAssociationofBreastSurgery(ABS)(2015)AnauditofscreendetectedbreastcancersfortheyearofscreeningApril2013toMarch2014.AssociationofBreastSurgery,June2015.Availableat:http://bit.ly/2ofWGUx(AccessedFebruary2018)
74Ahmat,N.(2012)Accessallages:assessingtheimpactofageonaccesstosurgicaltreatment.RoyalCollegeofSurgeons,October2012.Availableat:http://bit.ly/2sM6s5c(AccessedFebruary2018)75MacmillanCancerSupport,AgeUKandtheDepartmentofHealth(2012)CancerServicesComingofAge:LearningfromtheImprovingCancerTreatmentAssessmentandSupportforOlderPeopleProject.MacmillanCancerSupport,December2012.Availableat:http://bit.ly/2HyaHVB(AccessedFebruary2018)76TheNationalCancerEqualityInitiative(NCEI)andPharmaceuticalOncologyInitiative(2012)Theimpactof
patientageonclinicaldecision-makinginoncology.DepartmentofHealth,2012.Availableat:http://bit.ly/2Fjfvxr(AccessedFebruary2018)
77PerezDeCelis,E.S.etal,June2018.Patient-definedgoalsandpreferencesamongolderadultswithcancerstartingchemotherapy(CT).In:ASCO,June2018,ChicagoUSA.Availableat:https://bit.ly/2JMPFqa(AccessedJune2018)78Lavelle,K.,etal.,IslackofsurgeryforolderbreastcancerpatientsintheUKexplainedbypatientchoiceor
poorhealth?Aprospectivecohortstudy.BritishJournalofCancer,2014.110(3):p.573-583.Availableat:https://www.nature.com/articles/bjc2013734(AccessedFebruary2018)
79Ring,A.,Theinfluencesofageandco-morbiditiesontreatmentdecisionsforpatientswithHER2-positiveearlybreastcancer.CritRevOncolHematol,2010.76(2):p.127-32.Availableat:http://bit.ly/2Gzg5GJ(AccessedFebruary2018)80WalesCancerNetworkandWelshGovernment(2016).CancerDeliveryPlanforWales2016-20:thehigheststandardofcareforeveryonewithcancer.http://bit.ly/2gC1ke1(AccessedFebruary2018)8182Taylor,C.,Munro,A.J.,Glynne-Jones,R.,Griffith,C.,Trevatt,P.,Richards,M.&Ramirez,A.J.(2010)Multidisciplinaryteamworkingincancer:whatistheevidence?BMJ,340,c951.Availableat:http://bit.ly/2FiHP2K(AccessedFebruary2018)83Taylor,C.,Shewbridge,A.,Harris,J.&Green,J.S.(2013)Benefitsofmultidisciplinaryteamworkinthemanagementofbreastcancer.BreastCancer:TargetsandTherapy5,pp.79-85.Availableat:http://bit.ly/2GusTxO(AccessedFebruary2018)
AdvancingCare,AdvancingYears 67
84IndependentCancerTaskforce(2015)Achievingworld-classcanceroutcomes:astrategyforEngland2015-2020.London:IndependentCancerTaskforce.Availableat:http://bit.ly/1Idwf5W(AccessedFebruary2018)85HamakerME,VosAG,SmorenburgCH,deRooijSE,vanMunsterBC(2012)Thevalueofgeriatricassessmentsinpredictingtreatmenttoleranceandall-causemortalityinolderpatientswithcancer.Oncologist17(11),pp.1439–1449.Availableat:http://bit.ly/2GxfF3m(AccessedFebruary2018)86WildiersH,HeerenP,PutsM,TopinkovaE,Janssen-HeijnenML,ExtermannM,FalandryC,ArtzA,BrainE,CollocaG,FlamaingJ,KarnakisT,KenisC,AudisioRA,MohileS,RepettoL,VanLeeuwenB,MilisenK,HurriaA(2014)InternationalSocietyofGeriatricOncologyConsensusonGeriatricAssessmentinOlderPatientsWithCancer.J.Clin.Oncol.32(24),pp.2596-2603.Availableat:http://bit.ly/2EHafqa(AccessedFebruary2018)87Kirkhus,L.,etal(2017)Geriatricassessmentissuperiortooncologists’clinicaljudgementinidentifyingfrailty.BrJCancer117(4)pp.470-477.Availableat:http://bit.ly/2CAlA5D(AccessedFebruary2018)88Wildiers,H.,Heeren,P.,Puts,M.,Topinkova,E.,Janssen-Heijnen,M.L.,Extermann,M.,Falandry,C.,Artz,A.,Brain,E.,Colloca,G.,Flamaing,J.,Karnakis,T.,Kenis,C.,Audisio,R.A.,Mohile,S.,Repetto,L.,VanLeeuwen,B.,Milisen,K.,Hurria,A.(2014)‘InternationalSocietyofGeriatricOncologyConsensusonGeriatricAssessmentinOlderPatientsWithCancer’.JClinOncol32(24),pp.2596-2603.Availableat:http://bit.ly/2EHafqa(AccessedFebruary2018)89BritishGeriatricsAssociation(2014)FitforFrailtyConsensusBestPracticeGuidanceforthecareofolderpeoplelivingwithfrailtyincommunityandoutpatientsettings,Part1.BritishGeriatricsSociety,RoyalCollegeofGeneralPractitionersandAgeUK,2014.Availableat:http://bit.ly/1OvPuXo(AccessedFebruary2018)90Vernon,M(2016)Blog:whyisdiagnosingfrailtyimportant?NHSEngland,September2016[online]http://bit.ly/2Cb8oYV(AccessedFebruary2018)91Puts,M.T.,Hardt,J.,Monette,J.,Girre,V.,Springall,E.,Alibhai,S.M.(2012)Useofgeriatricassessmentforolderadultsintheoncologysetting:asystematicreview.JNatlCancerI,104(15),pp.1133–1163.Availableat:http://bit.ly/2CAYwDN(AccessedFebruary2018)andPuts,M.T.E.,Santos,B.,Hardt,J.,Monette,J.,Girre,V.,Atenafu,E.G.,Springall,E.andAlibhai,S.M.H.,(2014)Anupdateonasystematicreviewoftheuseofgeriatricassessmentforolderadultsinoncology.AnnOncol,25(2),pp.307-315.Availableat:http://bit.ly/2EKtLy2(AccessedFebruary2018)92Puts,M.T.,Hardt,J.,Monette,J.,Girre,V.,Springall,E.,Alibhai,S.M.(2012)Useofgeriatricassessmentforolderadultsintheoncologysetting:asystematicreview.JNatlCancerI,104(15),pp.1133–1163.Availableat:http://bit.ly/2CAYwDN(AccessedFebruary2018);Puts,M.T.E.,Santos,B.,Hardt,J.,Monette,J.,Girre,V.,Atenafu,E.G.,Springall,E.andAlibhai,S.M.H.,(2014)Anupdateonasystematicreviewoftheuseofgeriatricassessmentforolderadultsinoncology.AnnOncol,25(2),pp.307-315.Availableat:http://bit.ly/2EKtLy2(AccessedFebruary2018);HamakerME,VosAG,SmorenburgCH,deRooijSE,vanMunsterBC(2012)Thevalueofgeriatricassessmentsinpredictingtreatmenttoleranceandall-causemortalityinolderpatientswithcancer.Oncologist17(11),pp.1439–1449.Availableat:http://bit.ly/2GxfF3m(AccessedFebruary2018)93Puts,M.T.,Hardt,J.,Monette,J.,Girre,V.,Springall,E.,Alibhai,S.M.(2012)Useofgeriatricassessmentforolderadultsintheoncologysetting:asystematicreview.JNatlCancerI,104(15),pp.1133–1163.Availableat:http://bit.ly/2CAYwDN(AccessedFebruary2018);Chaibi,P.,Magne,N.,Breton,S.,Chebib,A.,Watson,S.,Duron,J.J.,Hannoun,L.,Lefranc,J.P.,Piette,F.,Menegaux,F.,Spano,J.P.(2011)Influenceofgeriatricconsultationwithcomprehensivegeriatricassessmentonfinaltherapeuticdecisioninelderlycancerpatients.Crit.Rev.Oncol.Hematol.79(3),pp.302–307.Availableat:http://bit.ly/2GAJxw7(AccessedFebruary2018)Caillet,P.,Canoui-Poitrine,F.,Vouriot,J.,Berle,M.,Reinald,N.,Krypciak,S.,Bastuji-Garin,S.,Culine,S.,Paillaud,E.(2011)Comprehensivegeriatricassessmentinthedecision-makingprocessinelderlypatientswithcancer:ELCAPAstudy.J.Clin.Oncol.29(27),pp.3636–3642.Availableat:http://bit.ly/2CBBeNV(AccessedFebruary2018)94Kenis,C.,Bron,D.,Libert,Y.,etal.(2013)Relevanceofasystematicgeriatricscreeningandassessmentinolderpatientswithcancer:resultsofaprospectivemulticentricstudy.J.Oncol.Manag.24(5),pp.1306–1312.Availableat:http://bit.ly/2FkPzkL(AccessedFebruary2018)95Puts,M.T.,Hardt,J.,Monette,J.,Girre,V.,Springall,E.,Alibhai,S.M.(2012)Useofgeriatricassessmentforolderadultsintheoncologysetting:asystematicreview.JNatlCancerI,104(15),pp.1133–1163.Availableat:http://bit.ly/2CAYwDN(AccessedFebruary2018);Puts,M.T.E.,Santos,B.,Hardt,J.,Monette,J.,Girre,V.,Atenafu,E.G.,Springall,E.andAlibhai,S.M.H.,(2014)Anupdateonasystematicreviewoftheuseofgeriatricassessmentforolderadultsinoncology.AnnOncol,25(2),pp.307-315.Availableat:http://bit.ly/2EKtLy2(AccessedFebruary2018)96Morris,R.,Cowley,A.,Sims,A.,Pattinson,J.andMasud,T.(2016)DoesComprehensiveGeriatricAssessment
AdvancingCare,AdvancingYears 68
AffectDecisionmaking&OutcomesforOlderAdultstreatedforUpperGastro-intestinalcancer.PosterpresentationtotheSIOGannualconference2016,Milan.EuropeanGeriatricMedicine7S1(2016)S29-S259.Availableat:http://bit.ly/2oneMmC(AccessedFebruary2018)97Lycke,M.,Pottel,Letal.(2015)Integrationofgeriatriconcologyindailymultidisciplinarycancercare:Thetimeisnow.EuropeanJournalofCancerCare,24(2)pp.143-146.Availableat:http://bit.ly/2sPunRE(AccessedFebruary2018)98Gosney,M.(2007)Contributionofthegeriatriciantothemanagementofcancerinolderpatients.EuropeanJournalofCancer43(15),pp.2153-2160.Availableat:http://bit.ly/2BLcBBU(AccessedFebruary2018)99O'Donovan,A.,Mohile,S.G.andLeech,M.(2015)'Expertconsensuspanelguidelinesongeriatricassessmentinoncology',EuropeanJournalofCancerCare,24(4),pp.574-589.Availableat:http://bit.ly/2ogx5Lb(AccessedFebruary2018)100NICE[online]NICEguideline,shareddecision-making.http://bit.ly/2cYuQ72(AccessedFebruary2018)101Coulter,A.andCollins,A.(2011)Makingshareddecision-makingareality:Nodecisionaboutme,withoutme.TheKingsFund,2011.Availableat:http://bit.ly/2ELPM3m(AccessedFebruary2018)102DaSilva,D.(2012)Helpingpeoplesharedecision-making:areviewofevidenceconsideringwhethershareddecisionmakingisworthwhile.TheHealthFoundation,June2012.Availableat:http://bit.ly/2Ca6oQX(AccessedFebruary2018)103Ahmad,N.,Ellins,J.,Krelle,H.andLawrie,M.(2014)Person-centredcare:fromideastoaction.TheHealthFoundation,October2014.Availableat:http://bit.ly/2FhYeo4(AccessedFebruary2018)104DaSilva,D.(2012)andAhmad,N.etal(2014)105DaSilva,D.(2012);Banning,M.(2008)Areviewofclinicaldecision-making:modelsandcurrentresearch.JournalofClinicalNursing17,pp.187-195.Availableat:http://bit.ly/2C9j9Lm(AccessedFebruary2018)106DaSilva,2012andAhmadetal,2014107Kehl,K.L.,Landrum,M.B.,Arora,N.K.,Ganz,P.A.,vanRyn,M.,Mack,J.W.,Keating,N.L.(2015)Associationofactualandpreferreddecisionroleswithpatient-reportedqualityofcare:shareddecisionmakingincancercare.JAMAOncol.1(1),50-8.Availableat:http://bit.ly/2Fku3wz(AccessedFebruary2018)108Tariman,J.,Berry,D.,Cochrane,B.etal(2009)Preferredandactualparticipationrolesduringhealthcaredecisionmakinginpersonswithcancer:asystematicreview.AnnalsofOncology,21(6),pp.1145-1151.Availableat:http://bit.ly/2GDynqd(AccessedFebruary2018)109Joseph-Williams,N.,Elwyn,G.,Edwards,A.(2014)Knowledgeisnotpowerforpatients:Asystematicreviewandthematicsynthesisofpatient-reportedbarriersandfacilitatorstoshareddecision.PatientEducationandCounseling94,pp.291–309.Availableat:http://bit.ly/2EHEitY(AccessedFebruary2018)110Bridges,J.,Hughes,J.,Farrington,N.&Richardson,A.(2015)Cancertreatmentdecision-makingprocessesforolderpatientswithcomplexneeds:aqualitativestudy.BMJOpen5(12).Availableat:http://bit.ly/2HyMU85(AccessedFebruary2018)111Handforth,C.,Clegg,A.,YoungC,etal.(2015)Theprevalenceandoutcomesoffrailtyinoldercancerpatients:asystematicreview.Ann.Oncol.26(6),pp.1091-101.Availableat:http://bit.ly/2CdaTdv(AccessedFebruary2018)112ChenR.C.,RoyceTJ,ExtermannM,etal.(2012)Impactofageandcomorbidityontreatmentandoutcomesinelderlycancerpatients.Semin.Radiat.Oncol.22(4)pp.265–271.Availableat:http://bit.ly/2CBgoya(AccessedFebruary2018)113Sparks,L.andNussbaum,J.F.(2008)Healthliteracyandcancercommunicationwitholderadults'.Patienteducationandcounseling,71(3),pp.345-350.Availableat:http://bit.ly/2ogB2zvhttp://bit.ly/2HzIbmp114Leydon,G.M.,Boulton,M.,Moynihan,C.etal.(2000)Cancerpatients'informationneedsandinformation-seekingbehaviour:indepthinterviewstudy.BritishMedicalJournal320,7239,pp.909-913.Availableat:http://bit.ly/2HzIbmp(AccessedFebruary2018)115Giacalone,A.,Talamini,R.,Fratino,L.,Simonelli,C.,Bearz,A.,Spina,M.andTirelli,U.(2009)Cancerintheelderly:Thecaregivers'perceptionofseniorpatients'informationalneeds.ArchivesofGerontologyandGeriatrics,49(2),pp.e121-e125.Availableat:http://bit.ly/2EJLQjV(AccessedFebruary2018)116Broome,S.,Dellot,B.,Lindley,E.,Norris,E.,Rowson,J.Soopramanien,D.andTruch,E.(2012)Improvingdecisionmakinginthecareofolderpeople:Exploringthedecisionecology.JosephRowntreeFoundation,2012.Availableat:http://bit.ly/2HAarFJ(AccessedFebruary2018)117Sivell,S.,Edwards,A.,Elwyn,G.andManstead,A.S.R.(2011)Understandingsurgerychoicesforbreastcancer:howmighttheTheoryofPlannedBehaviourandtheCommonSenseModelcontributetodecisionsupportinterventions?HealthExpectations,14,pp.6-19.Availableat:http://bit.ly/2HyTnjn(AccessedFebruary2018)118Johnson,M.(2012)'Chemotherapytreatmentdecisionmakingbyprofessionalsandolderpatientswith
AdvancingCare,AdvancingYears 69
cancer:anarrativereviewoftheliterature',EuropeanJournalofCancerCare,21(1),pp.3-9.Availableat:http://bit.ly/2omT820(AccessedFebruary2018)119Strohschein,F.J.,Bergman,H.,Carnevale,F.A.andLoiselle,C.G.(2011)PatientDecisionMakingAmongOlderIndividualsWithCancer.Qualitativehealthresearch21(7),pp.900-926.Availableat:http://bit.ly/2sQC9uz(AccessedFebruary2018)120Hobbs,G.,Landrum,M.,Arora,N.Ganz,P.A.,vanRyn,M.,Weeks,J.C.,Mack,J.W.andKeating,N.L.(2015)Theroleoffamiliesindecisionsregardingcancertreatments.Cancer,121(7).Availableat:http://bit.ly/2sNsWTM(AccessedFebruary2018)121Zhang,A.Y.,&Siminoff,L.A.(2003)Theroleofthefamilyintreatmentdecisionmakingbypatientswithcancer.OncologyNursingForum,30,1022–1028.Availableat:http://bit.ly/2oomk8H(AccessedFebruary2018)122Shin,D.,Cho,J.,Roter,D.etal(2013)“Preferencesforandexperiencesoffamilyinvolvementincancertreatmentdecision-making:patient-caregiverdyadsstudy”,Psychooncology,22(11)Availableat:http://bit.ly/2GxbhS2(AccessedFebruary2018)123Zhang,A.Y.,&Siminoff,L.A.(2003)Theroleofthefamilyintreatmentdecisionmakingbypatientswithcancer.OncologyNursingForum,30,1022–1028.Availableat:http://bit.ly/2oomk8H(AccessedFebruary2018)124MarshallD.,Johnson,F.,KulinN.,etal(2009)Howdophysicianassessmentsofpatientpreferencesforcolorectalcancerscreeningtestsdifferfromactualpreferences?AcomparisoninCanadaandtheUnitedStatesusingastated-choicesurvey.HealthEconomics18(12)pp.1420-1439.Availableat:http://bit.ly/2EXMKII(AccessedFebruary2018)125Braun,A.K.,Kubiak,T,KuntscheJetal.SGS:astructuredtreatmentandteachingprogrammeforolderpatientswithdiabetesmellitus-aprospectiverandomisedcontrolledmulti-centretrial.AgeAgeing38(4),pp.390-396.Availableat:http://bit.ly/2BG7XF7(AccessedFebruary2018)126Evans,N.,Pasman,H.R.W.,Payne,S.A.,Seymour,J.,Pleschberger,S.,Deschepper,R.,Onwuteaka-Philipsen,B.D.andEuroImpact(2012)Olderpatients'attitudestowardsandexperiencesofpatient-physicianend-of-lifecommunication:asecondaryanalysisofinterviewsfromBritish,DutchandBelgianpatients.BMCPalliativeCare11,pp.24.Availableat:http://bit.ly/2EXK8uh(AccessedFebruary2018)127Joseph-Williams,N.,Elwyn,G.andEdwards,A.(2014)Knowledgeisnotpowerforpatients:Asystematicreviewandthematicsynthesisofpatient-reportedbarriersandfacilitatorstoshareddecisionmaking.PatientEduc.Couns.94(3),pp.291-309.Availableat:http://bit.ly/2EVDdBV(AccessedFebruary2018)128DaSilva,D.(2012)Helpingpeoplesharedecisionmaking:areviewofevidenceconsideringwhethershareddecisionmakingisworthwhile.TheHealthFoundation,June2012.Availableat:http://bit.ly/2Ca6oQX(AccessedFebruary2018)Joseph-Williams,N.,Elwyn,G.andEdwards,A.(2014)Knowledgeisnotpowerforpatients:Asystematicreviewandthematicsynthesisofpatient-reportedbarriersandfacilitatorstoshareddecisionmaking.PatientEduc.Couns.94(3),pp.291-309.Availableat:http://bit.ly/2EVDdBV(AccessedFebruary2018)130IndependentCancerTaskforce(2015)Achievingworld-classcanceroutcomes:astrategyforEngland2015-2020.London:IndependentCancerTaskforce.Availableat:http://bit.ly/1Idwf5W(AccessedFebruary2018)131NCIN(2015)Olderpeopleandcancer(version3.0).Availableat:http://bit.ly/12NFOXb(AccessedFebruary2018)132NHSEngland(2014)‘Fiveyearforwardview’.NHSEngland,October2014.Availableat:http://bit.ly/1IvuwY5(AccessedFebruary2018)133TheScottishGovernment(2016)‘Beatingcancer:ambitionandaction’.TheScottishGovernment.Availableat:http://bit.ly/1TKZqDT(AccessedFebruary2018)134Ibid.135WalesCancerNetwork(2016)CancerDeliveryPlanforWales2016-2020,Thehigheststandardofcareforeveryonewithcancer.WelshGovernment,November2016.Availableat:http://bit.ly/2gC1ke1(AccessedFebruary2018)136Black,L.(2013)ResearchandInformationServiceBriefingNote1Paper142/13Cancerservices:NorthernIrelandandtheRepublicofIreland.NorthernIrelandAssembly,October2013.Availableat:http://bit.ly/28YXSTg(AccessedFebruary2018)137Zbar,A.P.,Gravitz,A.andAudisio,R.A.(2012)PrinciplesofSurgicalOncologyintheElderly.Clinicsingeriatricmedicine28(1)pp.51-71.Availableat:http://bit.ly/2ofDUMY(AccessedFebruary2018)138Lycke,M.,Ketelaars,L.,Boterberg,T.,Pottel,L.,Pottel,H.,Vergauwe,P.,Goethals,L.,VanEygen,K.,Werbrouck,P.,Debruyne,D.,Derijcke,S.,Borms,M.,Ghekiere,V.,Wildiers,H.andDebruyne,P.(2014)ValidationoftheFreundClockDrawingTestasaScreeningTooltoDetectCognitiveDysfunctionsinElderlyCancerPatientsUndergoingComprehensiveGeriatricAssessment.Psycho-oncology23,pp.114-114.Availableat:http://bit.ly/2olcsMW(AccessedFebruary2018)
AdvancingCare,AdvancingYears 70
139Bridges,J.Hughes,J.Farrington,N.etal(2015)Cancertreatmentdecision-makingprocessesforolderpatientswithcomplexneeds:aqualitativestudy.BMJOpen2015;5.Availableat:https://bit.ly/2LK3oLG(AccessedJune2018)140JørgensenTL,HallasJ,FriisS,andHerrstedt,J.(2012)Comorbidityinelderlycancerpatientsinrelationtooverallandcancer-specificmortality.BrJCancer106(7),pp.1353-1360.Availableat:http://bit.ly/2EIEtVR(AccessedFebruary2018)141Shenoy,P.andHarugeri,A.(2015)Elderlypatients’participationinclinicaltrials.Perspect.Clin.Res.6(4),pp.184-189.Availableat:http://bit.ly/2CacgJL(AccessedFebruary2018)142Alzheimer’sResearchUK(2017)10thingsyouneedtoknowaboutprevalence.Availableat:http://bit.ly/2Cb7coq(AccessedFebruary2018)143LaingandBuisson(2015)CareofolderpeopleUKmarketreport,twenty-seventhedition.Availableat:http://bit.ly/2EY0QtF(AccessedFebruary2018)144HouseofCommonsEnvironmentalAuditCommittee(2013)Transportandaccessibilitytopublicservices,ThirdReportofSession2013–14,VolumeIIWrittenevidence.HouseofCommons,June2013.Availableat:http://bit.ly/2BKu8K6(AccessedFebruary2018)145Bridges,J.Hughes,J.Farrington,N.etal(2015)Cancertreatmentdecision-makingprocessesforolderpatientswithcomplexneeds:aqualitativestudy.BMJOpen2015;5.Availableat:https://bit.ly/2LK3oLG(AccessedJune2018)146NIHRCLAHRCYorkshireandHumber[online]DevelopmentofanelectronicFrailtyIndex(eFI)http://bit.ly/2c9fc8J(AccessedFebruary2018)147NICE[online]NICEguideline[NG56)Multimorbidity:clinicalassessmentandmanagement,September2016.https://www.nice.org.uk/guidance/ng56(AccessedFebruary2018)148Handforth,C.,Clegg,A.,YoungC,etal.(2015)Theprevalenceandoutcomesoffrailtyinoldercancerpatients:asystematicreview.Ann.Oncol.26(6)pp.1091–1101.Availableat:http://bit.ly/2CdaTdv(AccessedFebruary2018)149Agnew,N.(2010)Preoperativecardiopulmonaryexercisetesting.ContinuingEducationinAnaesthesiaCriticalCare&Pain10(2),pp.33-37.Availableat:http://bit.ly/2GwXx9T(AccessedFebruary2018)150Smith,J(2016)[online]Riskpredictioninsurgery.http://bit.ly/2onYJVA(AccessedFebruary2018)151MacmillanCancerSupport(2012)CancerServicescomingofage.MacmillanCancerSupport,December2012.Availableat:http://bit.ly/2HyaHVB(AccessedFebruary2018)152NCIN(2015)RoutestoDiagnosis,2006-2015workbook.NationalCancerintelligenceNetwork,February2018.Availableat:http://bit.ly/1OelnIH(AccessedMarch2018)153Gray,R.,Gordon,B.andMeredith,M.(2017)Meetingpatient’sneeds:Improvingtheeffectivenessofmultidisciplinaryteammeetingsincancerservices.CancerResearchUK,January2017.Availableat:http://bit.ly/2j3npQf(AccessedFebruary2018)154Ibid.155Lamb,B.W.etal.(2011)TeamworkandTeamDecision-makingatMultidisciplinaryCancerConferences:Barriers,FacilitatorsandOpportunitiesforImprovement.WorldJ.Surg.35(9),pp.1970–1976.Availableat:http://bit.ly/2gekjr4(AccessedFebruary2018)156Bridges,J.Hughes,J.Farrington,N.etal(2015)Cancertreatmentdecision-makingprocessesforolderpatientswithcomplexneeds:aqualitativestudy.BMJOpen2015;5.Availableat:https://bit.ly/2LK3oLG(AccessedJune2018)157157Burns,K.,Meredith,M.,Williams,M.,Huxley,C.andPallesen,C.(2017)Fullteamahead:understandingtheUKnon-surgicalcancertreatmentsworkforce.CancerResearchUK,December2017.Availableat:http://bit.ly/2DEVMra(AccessedMarch2018)158Bridges,J.,Lucas,G.,Wiseman,T.etal(2016)PreparednessofUKworkforcetodelivercancercaretoolderpeople:summaryreportfromascopingreview.UniversityofSouthampton,2016.Availableat:159Kalsi,T.,Payne,S.,Brodie,H.etal(2013)AretheUKoncologytraineesadequatelyinformedabouttheneedsofolderpeoplewithcancer?Br.J.Cancer108(10),1936-1941.160Bridges,J.,Lucas,G.,Wiseman,T.etal(2017)Workforcecharacteristicsandinterventionsassociatedwithhigh-qualitycareandsupporttoolderpeoplewithcancer:asystematicreview.BMJOpen2017,7.Availableat:https://bit.ly/2JE6OPC(AccessedJune2018)161Ibid.162CancerResearchUK[online]Cancerincidenceforcommoncancers.http://bit.ly/1QsChBj(AccessedFebruary2018)163EastMidlandsCancerNetwork.Recommendedstagesforallocationofkeyworker&holisticassessment.AccessedMarch2017.
AdvancingCare,AdvancingYears 71
164ibid.165QualityHealth(2017)NationalCancerPatientExperienceSurvey.QualityHealth,July2017.Availableat:http://bit.ly/2jZ8Hf1(AccessedFebruary2018)166NHSScotland(2016).ScottishCancerPatientExperienceSurvey2015/16.ScottishGovernment,June2016.Availableat:http://bit.ly/2CaEfJq(AccessedFebruary2018)167ProstateCancerUK(2014)ThespecialistnursingworkforcecaringformenwithprostatecancerintheUK.Availableat:http://bit.ly/2sJ24UP(AccessedFebruary2018)168Henry,R.(2015)Theroleofthecancerspecialistnurse.NursinginPractice,November2015.Availableat:http://bit.ly/2HBp0J5(AccessedFebruary2018)169Kalsi,T.,Babic-Illman,G.,Ross,P.J.,Maisey,N.R.,Hughes,S.,Fields,P.,Martin,F.C.,Wang,Y.andHarari,D.(2015)Theimpactofcomprehensivegeriatricassessmentinterventionsontolerancetochemotherapyinolderpeople.BritishJournalofCancer112,pp.1435–1444.Availableat:http://go.nature.com/2EHJEW5(AccessedFebruary2018)170Maher,J.‘Strategiestoimproveoutcomesforoldercancerpatients:learningfromimprovingcancertreatmentassessmentandsupportforolderpeopleproject’inRing,A.,Harari,D.,Kalsi,T.,Mansi,J.andSelby,P.(2016)‘Problemsolvinginoldercancerpatients’.Oxford:ClinicalPublishing(AssociationofCancerPhysiciansandtheBritishGeriatricsSociety).Availableat:http://bit.ly/2oq37DB(AccessedFebruary2018)171Watts,G.(2012)Whytheexclusionofolderpeoplefromclinicalresearchmuststop.BMJ344.Availableat:http://bit.ly/2BJzFkr(AccessedFebruary2018)172Watts,G.(2012)Whytheexclusionofolderpeoplefromclinicalresearchmuststop.BMJ344.Availableat:http://bit.ly/2BJzFkr(AccessedFebruary2018)173LewisJH,KilgoreML,GoldmanDP,TrimbleEL,KaplanR,MontelloMJ,etal.(2003)Participationofpatients65yearsofageorolderincancerclinicaltrials.J.Clin.Oncol.21(7),pp.1383–1389.Availableat:http://bit.ly/2HDRyl6(AccessedFebruary2018)174Shenoy,P.andHarugeri,A.(2015)Elderlypatients’participationinclinicaltrials.Perspect.Clin.Res.6(4),pp.184-189.Availableat:http://bit.ly/2CacgJL(AccessedFebruary2018)175Watts,G.(2012)Whytheexclusionofolderpeoplefromclinicalresearchmuststop.BMJ2012;344:e3445.Availableat:http://bit.ly/2BIm7W8(AccessedFebruary2018)176Shenoy,P.andHarugeri,A.(2015)Elderlypatients’participationinclinicaltrials.Perspect.Clin.Res.6(4),pp.184-189.Availableat:http://bit.ly/2CacgJL(AccessedFebruary2018)177Watts,G.(2012)Whytheexclusionofolderpeoplefromclinicalresearchmuststop.BMJ2012;344:e3445.Availableat:http://bit.ly/2BIm7W8(AccessedFebruary2018)178Crome,P.,Cherubini,A.andOristrell,J.(2014)ThePREDICT(increasingtheparticipationoftheelderlyinclinicaltrials)study:thecharterandbeyond.ExpertRev.Clin.Pharmacol.7(4)pp.457-468.Availableat:http://bit.ly/2EJJwW5(AccessedFebruary2018)179EuropeanMedicinesAgency(2011)EMAgeriatricmedicinesstrategy.EMA,February2012.Availableat:http://bit.ly/2EYGoJi(AccessedFebruary2018)180PerezDeCelis,E.S.etal,June2018.Patient-definedgoalsandpreferencesamongolderadultswithcancerstartingchemotherapy(CT).In:ASCO,June2018,ChicagoUSA.Availableat:https://bit.ly/2JMPFqa(AccessedJune2018)181Bell,J.(2017)Lifesciences:industrialstrategy.OfficeforLifeSciences,August2017.Availableat:http://bit.ly/2wRQJms(AccessedMarch2018)





























