Embed Size (px)
Citation preview

1
(Preliminary and Incomplete)
Adverse Selection and Subsidies: Evidence from
Non-group Health Insurance Markets
Rajeev Cherukupalli*
Columbia University
October 15 2008
Abstract
Adverse selection is a problem in health insurance markets when premiums do not fully reflect individuals' risks. Premium subsidies in such markets can potentially reduce adverse selection by encouraging low-risk individuals to participate and seek greater insurance coverage. I test this premise using Current Population Survey and income tax data in the context of two concurrent and unrelated policy changes that have affected state non-group markets. Adverse selection was induced in the subset of state non-group markets which adopted community rating, a set of premium restrictions that increased the price of coverage for younger, healthier individuals. Over the same period, a series of federal tax law changes reduced the effective after-tax premiums for the self-employed, providing a subsidy to a subset of participants in non-group markets over and above that induced by the tax system in the crosssection. In line with the theory, I find that healthier individuals in the segment of the market affected by rating restrictions were more likely to purchase insurance if they received a larger effective subsidy.
* I thank Sherry Glied, Dan O’Flaherty and Wojeciech Kopczuk for their guidance and support, and Amitabh Chandra and participants at student colloquia at Columbia University for helpful comments. This paper is as yet incomplete, and all errors are mine.

2
I. Introduction and Literature
Adverse selection is a problem in markets with asymmetric information. Insurance markets typify
this situation, and insurers tend to offer menus of contracts with different combinations of premiums and
coverage to separate buyers on the basis of their risk. If buyers in an insurance market are offered a
uniform premium, the set of individuals who find it worth buying coverage will tend to have above-
average risks. The problem is compounded in health insurance markets, when insurers are restricted in
their ability to use different dimensions of risk in arriving at the premium they charge a customer.
This delinking of health risk from the price that people pay to be insured against those risks is a
feature of both group insurance offered by employers and of insurance purchased in some non-group
markets. In an employer sponsored plan, a sicker and a healthier employee might pay the same price
despite their very different expected health expenses. Analogously, in some non-group markets, insurers
are barred from using risk-related characteristics like age and gender in the price of the plans they offer.
When voluntary health insurance purchase is combined with such pricing restrictions, the concern is that
the composition of buyers in the market can shift to sicker individuals. Adverse selection can cause
insurers to raise premiums higher, further reducing avenues for coverage for the larger population.
Adverse selection imposes a negative externality in that the inability to use private information in
pricing insurance contracts spills over into under-insurance. A natural question to ask is whether a subsidy
can help reduce or eliminate adverse selection. This paper examines the question of whether tax subsidies
mitigate adverse selection by exploiting two concurrent and unrelated policy changes that have interacted
to affect state-level non-group insurance markets in the United States since the early 1990s. While one
policy induced selection in a set of states that adopted it, the other policy changed the magnitude of
subsidies available to a sub-segment of the market over time.
The state policy variation that potentially induced selection is community rating, implemented by
states that sought to ensure that high-cost individuals were not priced out of insurance. Community rating
restrictions have the effect of reducing insurers’ ability to separate consumers based on health risks.
While the intent of community rating is to make access to care more equitable, its viability depends on
lower risks staying in the insurance pool. Different sources, both descriptive and in the empirical
literature suggest that community rating was associated with increased premiums, and with reduced
enrollment and exit by insurers (Wachenheim and Leida, 2007; LoSasso and Lurie, 2007).
3
The tax-system induced variation in subsidies that potentially mitigated adverse selection
occurred in the form of a sequence of federally legislated increases in the fraction of health insurance
premiums that the self-employed, a substantial group of potential participants in the non-group market,
can deduct before computing taxable income. A federally mandated tax subsidy targeted at the self-
employed has the effect of reducing the relative premiums that a sub-group of healthy individuals needs
to pay for coverage. These two policy changes allow for comparing the ex-ante health status of the
subpopulation of potential participants in the non-group market in community rated states who received a
larger subsidy for a reason unrelated to their health with the health status of control populations within
and across states over time to identify the effect of subsidies on selection.
This paper contributes to the literatures on selection in non-group insurance markets, the role of
tax policy in healthcare, and the broader policy question of increasing insurance coverage. Researchers
have debated the extent of selection due to community rating restrictions since the time of their
introduction in the early 1990s. Community rating disallows the use of particular risk factors (usually age,
gender or health status or a combination of these) in setting premiums. More typically, rating restrictions
force insurers to limit the range of premiums to a band. Buchmueller and Dinardo (2002) concluded that
the effect of rating restrictions on the percentage insured in the small group through 1996 was minimal in
New York, though it possibly changed the structure of the market towards relatively greater HMO
penetration. A move to a more cost-conscious organizational form is one way in which insurers might
have responded to separate high-risk individuals when regulation prevented it in the non-group market.
More recent work (Lo Sasso and Lurie, 2007) that controls for states’ propensity to be community
rated finds evidence that rating restrictions lowered the propensity of healthier people to participate in the
non-group market, improved the likelihood of higher-risks participating, and increased the likelihood of
younger and healthier individuals being uninsured. The present study builds on this literature, but, rather
than relying primarily on observed outcomes of ex-post insurance purchases, it attempts to analyze
selection by employing health insurance industry data to assess how legal changes affected the
characteristics of participants. Further, previous studies considering the effect of rating restrictions on
participation in the non-group market typically do not recognize the role of taxes in inducing an additional
level of price variation across consumers with identical health risks. An exception to this is Auerbach and
Ohri (2006), a study that models the participation decision in nongroup markets as a function of the after-
tax premiums that individuals potentially face. That study, however, focuses on premium variation as a
way to identify demand elasticities and does not consider the issue of adverse selection.
4
The relation between tax policy and health insurance coverage has been the subject of continued
research in economics and public policy. Income taxation interacts with individuals’ insurance purchase
decisions at different levels—employers’ contributions to insurance are not subject to tax, individuals can
often purchase coverage out of pre-tax dollars, and medical expenses above a threshold can be deducted
to reduce overall tax liability. Given the pervasiveness of this interaction, studies are typically concerned
with two aspects of the influence of the tax system on health: the effectiveness of the tax subsidies in
improving coverage (Gruber and Poterba, 1994, Finkelstein, 2002), and the moral hazard induced by the
reduction in the effective price of medical care (Gruber and Washington, 2004). The present study
considers a less researched dimension of the tax system in the spirit of Cutler and Zeckhauser (1998),
namely the extent to which subsidies might act as a risk adjusment to restrict the degree of adverse
selection in situations where premiums are imperfectly related to purchasers’ health risks.
Cutler and Zeckhauser (1998) represents a smaller body of literature that examines the the effect
of subsidies on mitigating selection, typically in employer sponsored groups. Their study examined the
effect of the suspension of an equal contribution rule in a university’s health plan offerings. The step,
analogous to the withdrawal of an untargeted subsidy, encouraged low-risk individuals to withdraw from
more comprehensive and expensive plans. This sort of unraveling of plans is at the heart of the tradeoff
between pooling individuals of different risks to achieve a viable level of cross-subsidizing and curbing
incentives to use excessive and expensive care . Selden and Gray (2002) study the effect of a subsidy on
the Federal Employees Health Benefits Program, where the presence of both a national plan with fixed
premiums and a set of several local plans with varying premiums made it optimal for healthier employees
to select into the lowest cost plan they faced to avoid subsidizing high-cost employees. The FEHBP has a
nominally set maximum allowable premium subsidy, resulting in variation in the implied real local-level
subsidy. Selden and Gray find that older individuals selected into plans with higher premiums, but this
apparent adverse selection was slightly dampened by the larger effective subsidy that younger participants
received.
Ketsche (2004) uses cross-sectional data from the National Medical Expenditure Survey, 1987, to
ask whether receiving a larger subsidy on account of having a higher marginal tax rate increases the
participation of workers who are less healthy, or who have families with members in poorer health. The
present study is closest in its approach to Ketsche’s paper, with the advantage of having better
identification than was available in the cross-sectional setting that Ketsche uses. On the side of selection,
the variation in the present study that induces healthier people to be less likely to be insured is cross-state
differences in regulation of the non-group and small-group markets. Ketsche’s study does not have a

5
similar exogenous source driving the incentive for healthier people to drop coverage, and is confined to
using state income tax deciles rather than the precise imputed state tax to identify variation in subsidies.
On the side of variation in price that might mitigate adverse selection, the present study investigates state
insurance markets over more than a decade. Over this period the subsidy changes for a sub-population of
buyers were increases in allowable tax deductions of a magnitude ranging from 25 to 100 per cent of the
premium paid. These operate over and above the differences in effective after-tax subsidy brought about
by individuals being placed at different income levels and having different marginal taxes.
A more general interpretation of this paper is in the context of externalities in insurance markets.
Adverse selection is a negative externality that causes a deviation from the first best outcome of optimal
insurance for all health risks, since low risk individuals willing to purchase insurance are induced to
obtain suboptimal coverage or to drop coverage. A subsidy to such individuals, whether through the tax
system as in this instance, or though other conceivable forms, can improve welfare in contexts that make
insurance markets imperfect. Einav, Finkelstein and Cullen (2008), for example, suggest that adverse
selection is associated with an efficiency cost of 3 per cent relative to what obtains with efficient pricing.
How efficiently a tax subsidy serves to correct selection depends on the costs the subsidy imposes relative
to the benefits of reduced selection. The present study attempts to measure some of these potential
benefits in a context where the source of the externality and the subsidy affecting this externality are
identified relatively cleanly.
The paper proceeds as follows. Section II briefly examines the theoretical reasons for how a
subsidy can mitigate selection in a standard Rothschild-Stiglitz (1979) framework. Section III outlines the
empirical strategy and the two contexts, community rating and tax-policy induced variation in premiums
that this study exploits in identifying the effect of subsidies on adverse selection. Section IV describes the
data used in the analysis and presents evidence pointing to the differential effect of subsidies on selection
in community rated and non- community rated states. Section V develops the empirical models used and
discusses the results on selection and whether the tax system reduced selection, and Section VI concludes.
II. Theoretical Framework
Figure 1 depicts the standard Rothschild-Stiglitz (R-S) equilibrium in a health insurance market
in the absence of any subsidy. The horizontal axis represent individuals’ wealth in the event of their
facing no health loss, while the vertical axis represents wealth in the event that individuals face a health
loss. The 45-degree line OO´ represents equal wealth combinations in each state, and therefore first-best

6
outcomes of equal wealth in both states. Individuals placed at an initial endowment, W, can do better if
they are offered insurance contracts that allow them to trade wealth in states with no loss(a premium) for
insurance against the erosion of wealth in states when they do face a health loss
In comparison to a healthy person (a low risk, L), a less healthy individual (a high risk, H)
typically needs to pay a greater premium to obtain the same protection against wealth losses when faced
with a health event. This accounts for the flatter slope of the high-risk individual’s insurance curves. Fair-
odds contracts for any individual are those that make zero expected profits—for the high risk individual,
the fair-odds line is FHW. Contracts north-east of this line involve the insurer making a negative expected
profit off the high-risk individual. The standard separating equilibrium in the R-S framework involves the
high-risk individual selecting FH (full insurance), while the low-risk individual selects into SL, an
incentive-compatible contract that the high-risk individual is indifferent to. WW´ represents market odds,
and will tend to be skewed more toward the origin O, the higher the proportion of unhealthy individuals
in the market. In the standard R-S framework, pooling is unviable. Contracts northeast of ŪL will be
selected by both low and high risks, and result in negative profits if the market odds are as depicted.
A simple take on community rating is to model the insurer as being forced to offer a contract
invariant to risk-types, that is, being forced to pool risks. Given the market odds, the non-zero profit
contracts offered will be on or south-west of WW´. All of these contracts leave low-risk individuals worse
off. In particular, point P1 represents pooling with the high-risk individual deriving the same utility as
with the separating equilibrium, and the low-risk individual being worse off. P2 is preferred by the high-
risk individual, while P3 makes both risk-types worse off.
Economists’ and policy makers’ concern with the introduction of community rating in the 1990s
(Buchmueller and Dinardo, 2002) was of the possibility of an adverse selection spiral resulting when the
profile of the non-group market is progressively skewed towards higher risk individuals and premiums
rise to keep pace with the higher average risks. In terms of Figure 1, a shift in composition of the
insurance market towards higher risks would be depicted by a pivoting of the market odds line in the
direction of WFH, and a progressive reduction of welfare for low-risk participants.
Figure 2 depicts an easier way to think of the consequences of a subsidy on take-up at the level of
the market. Healthier individuals have both a lower willingness to pay (as depicted by the negatively
sloped demand curve) and add less to insurers’ costs than sicker individuals (resulting in a negatively
sloped marginal cost curve). Efficient insurance purchase is at Qeff. Adverse selection results from

7
insurers having to charge a uniform price, at the point where average costs equal willingness to pay in the
figure. In a competitive equilibrium, the mass of individuals covered—or, more generally, the quantify of
coverage offered in the market—is Q1, resulting in an efficiency loss equal to the area ABC. A subsidy,
represented by an outward shift of the demand curve, can potential offset some of this efficiency loss,
while increasing coverage to Q3. An untargeted subsidy carries its own efficiency loss (the area ADE),
but to the extent that a subsidy scheme can be designed to mimic the marginal cost curve, the lower these
losses will tend to be.
III. Empirical Strategy
Subsidies can influence selection along two margins—who chooses to purchase insurance, and
how much coverage they demand. This paper focuses on the former decision. An ideal experiment to test
if subsidies reduce the extent of selection would involve offering two insurance contracts with identical
coverage but different subsidies to two populations with an identical distribution of health risks. A
measure of the effect of the subsidy is the extent to which take-up in the subsidized population exceeds
that in the unsubsidized population. A second measure is the generosity of coverage individuals select,
but that cannot be captured in the data.
In the absence of the ideal experiment, I investigate adverse selection in the context of two policy
induced variations affecting the non-group (and small-group) insurance market in the United States. In
line with related empirical work, I first compare the observable risk profile of individuals in the market
for nongroup insurance in community rated states with those in unregulated states to verify whether
restricting the range of premiums induces higher risk individuals to participate, and/or reduces the
purchase of insurance by lower risk individuals. Thereafter, I test if receiving a larger subsidy has the
effect of inducing lower risk individuals in community rated states to purchase insurance. The empirical
strategy is thus to develop variants of the following estimation equation
— (1)
CR in the above is an indicator of whether a state is community rated (or of years since the enforcement
of rating regulations). Affected is an indicator for potential purchasers of nongroup insurance affected by
the rating restrictions, and healthy is one of different proxies for individuals’ health risks. The coefficients
εγγγ
γγγβ
effects year effects state6subsidy*healthy * affected* CR5healthy * affected* CR 4subsidy*affected*CR
3healthy * affected* CR affected* CR CR X ed)Prob(insur
++++++
+++= 21

8
of particular interest are 3γ and 5γ . If the model is correctly identified, a negative 3γ indicates that the
community rating tends to draw less healthy participants, while a positive 5γ indicates if and to what
extent a subsidy restores the balance towards healthier participants.
Community rating restrictions
The non-group market in the US accounts for about 7 per cent of all insurance purchases and is
largely unregulated. Given the predominance of employer-sponsored insurance, the non-group market is
typically a residual market with a large variation in the number of insurers and types of contracts on offer.
Beginning in the early 1990s, a some states began to implement regulations to make insurance in the non-
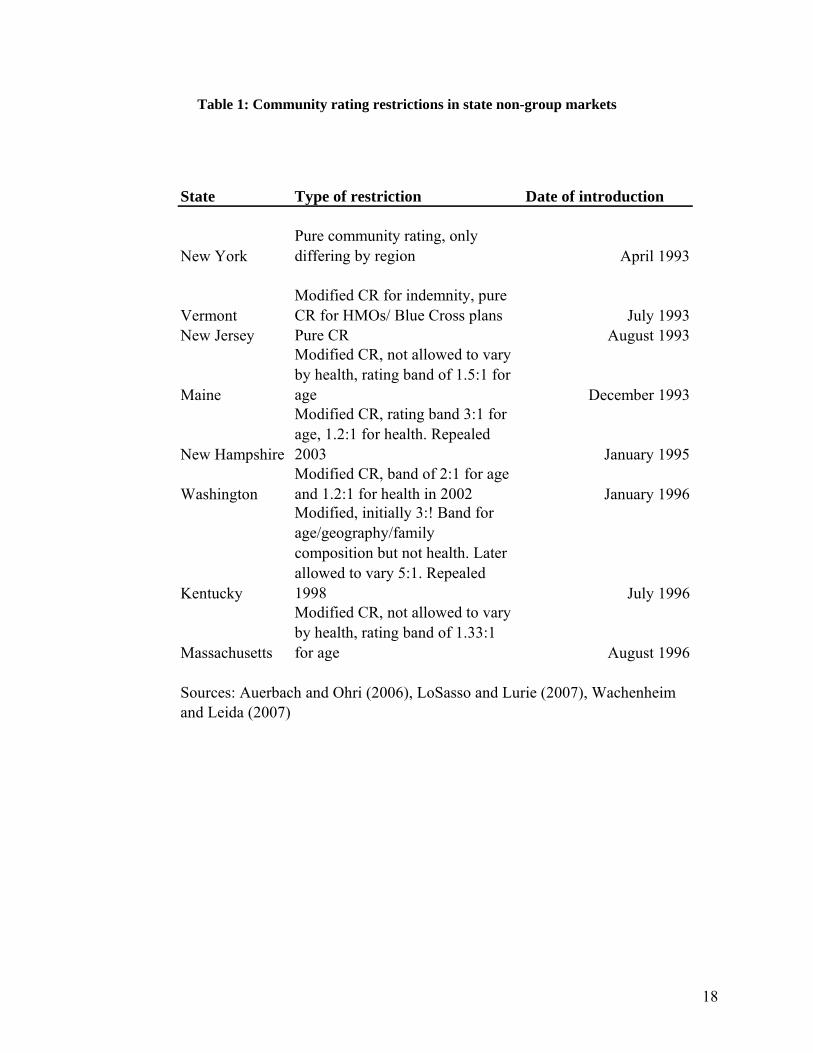
group market more affordable to high-riks individuals. Table 1 outlines these restrictions. New York is
the one state with pure community rating: while premium variation is allowed in benefit plan design,
family type and geographic regions, premiums are not allowed to vary by age or health for any given plan.
Other states typically prescribe a band within which premiums can vary—a 3:1 age band, for instance,
would allow a 60 year old male to be charged a premium that is at most three times what a 20 year old
male is charged, even though, by some estimates, the expected health expenses.
Whether community rating changes participation and risk composition in non-group markets is an
empirical question. There are a few factors that can attenuate any effect. The first is the presence of
institutional factors that pre-empt rating restrictions. While New York’s was an instance of pure
community rating, the official rule largely followed the existing voluntary rating practice of the largest
insurance carrier in the combined non-group and small group market. Second, there are several ways in
which insurers might respond to circumvent rating restrictions. States with weaker restrictions, for
instance, have both a larger menu of plans offered and higher rates of rejection of applicants by their
dominant insurance carriers (Turnbull and Kane, 2005). Observed changes in participation in community
rated states are thus necessarily reduced-form effects of purchase decisions of individuals conditional on
the menu of plans offered.
A larger set of states adopted restrictions in the small-group market in the same period of the
study, and the shift to community rating restrictions was associated with decline in coverage for low-risk
individuals and a passing on of the costs of increased premiums to workers (Simon, 2005). I also consider
these states in the empirical model of the decision of those affected by rating restrictions to be privately
insured.
9
Tax price variation
The income tax system induces variation in the after-tax price that individuals pay for insurance.
Two individuals with the same health risks and offered the same insurance contract face different after-
tax prices depending on their incomes, deductions and state of residence.The marginal tax price of
insurance is a measure of the after-tax cost of an additional dollar of premium purchased. To the extent
that insurance purchases are made out of after-tax incomes, the price of additional coverage decreases in
the marginal tax rate.
Given a schedule of premiums and individuals’ insurance purchase decisions, identifiying the
effect of price subsidies is confounded by the fact that unobservables might drive both the decision to be
covered and the tendency to select contracts with higher premiums. The advantage to using tax prices in
considering the effect of subsidies on selection is that federal tax policy induces exogenous variation in
the price of insurance. There are, however, caveats to using tax prices as a method of identifying the
effect of prices (Feenberg, 1987; Andreoni, 2006). What matters for the economic analysis of decisions
on the margin is the additional dollar of insurance, or the last dollar tax price. The last dollar tax price,
however, is a function of premiums paid—a taxpayer with a large premium potentially faces a higher
effective tax price. A solution is to use the first dollar price, a price computed as if individuals had no
insurance and were contemplating paying a premium of one dollar.
A more serious concern is that while the tax price is largely exogenous to individuals’ health risks,
it tends to be highly correlated with income, marital status and the number of dependents an individual
has, all of which are important determinants of coverage. At the very least, the measure of income used
needs to be different from that used to calculate the tax price. Variation in state taxes provides another
level of exogeneity, but if states with higher tax regimes are also states that are more likely to have
community rating restrictions, then the necessity of using state fixed effects to control for heterogeneity
cancels out the identification deriving from state tax variation. Figure 4 provides an indication of how tax
price and income are related—they tend to be negatively correlated, but the relationship is far from linear.
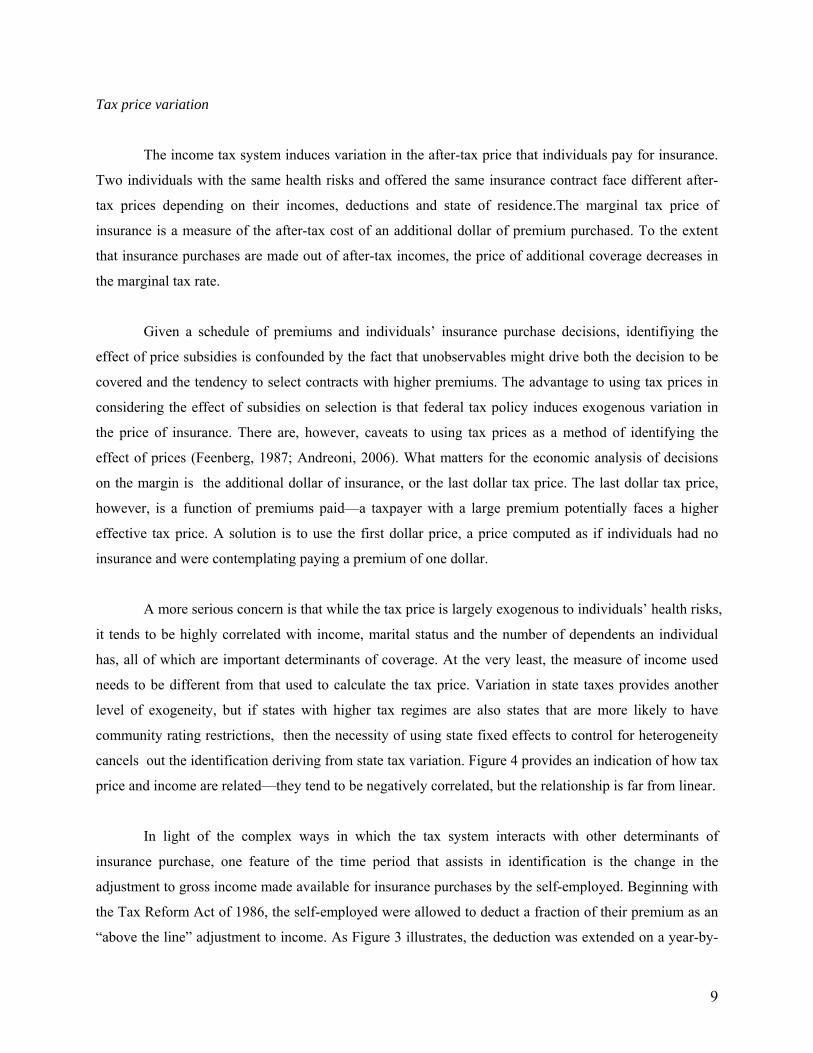
In light of the complex ways in which the tax system interacts with other determinants of
insurance purchase, one feature of the time period that assists in identification is the change in the
adjustment to gross income made available for insurance purchases by the self-employed. Beginning with
the Tax Reform Act of 1986, the self-employed were allowed to deduct a fraction of their premium as an
“above the line” adjustment to income. As Figure 3 illustrates, the deduction was extended on a year-by-

10
year basis over the decade, and was increased periodically from 25 per cent through 1995 to 100 per cent
by 2003. Self-employed taxpayers constitute between 8 and 21 percent percent of taxpayers in state non-
group markets and 14 percent nationwide. This is relevant to identifying the effect of subsidies on
selection through sources other than cross-sectional variation, since the self-employed are a subgroup of
the potential market for nongroup insurance that received a subsidy that others did not receive. Panel A in
Figure 5 displays how this variation plays out along the income distribution in community rated states—
over time, the effective tax price declined for the self-employed at all levels of the income distribution.
Panel B suggests that there are variations in insurance purchase beyond that observed across the income
distribution, though insurance purchase for the self-employed tends to be noisier.
IV. Data
I use March Current Population Survey data for 1990-2005 for the purpose of the estimation
exercise. The advantages of the CPS are the ability to identify good proxies for income, to retain large
sample sizes for estimating effects on subgroups such as the selfemployed in a subset of states, and, in
contrast to the SIPP, the ability to identify firm size easily, firm size being an important determinant of
the likelihood of insurance offer and purchase. These advantages come with well-recognized
disadvantages, including the cross-sectional nature of the data, and the absence of detailed measures of
health insurance plan attributes and individuals’ health status. Further, when estimating empirical models
that use self-reported health status as a control, I am restricted to periods after 1995 when the health status
questions were introduced in the CPS.
The unit of observation is the individual tax payer in the age group 19 to 64. I drop individuals
covered by Medicare, Medicaid or other forms of publicly funded and military coverage since the
insurance purchase calculus is considerably different for these groups. I compute tax prices using NBER’s
TAXSIM software to obtain marginal tax rates for individuals in the sample. For employees of firms, the
tax price is computed as
(1-tfed-tstate-tFICA/2) if wage/salary employee (1- θ(tfed+ tstate)) if self-employed
where tfed, tstateA and tFICA represent the federal, state and social security marginal tax rates and θ is the
fraction of the insurance premium that can be deducted as an adjustment to income by the self-employed
(0.25 through 1995 and a 100 per cent from 2003).

11
Table 2 displays summary statistics for the start and end period considered. Aside of family
income, there appears little variation in means of the variables, though there is a 20 per cent decline in
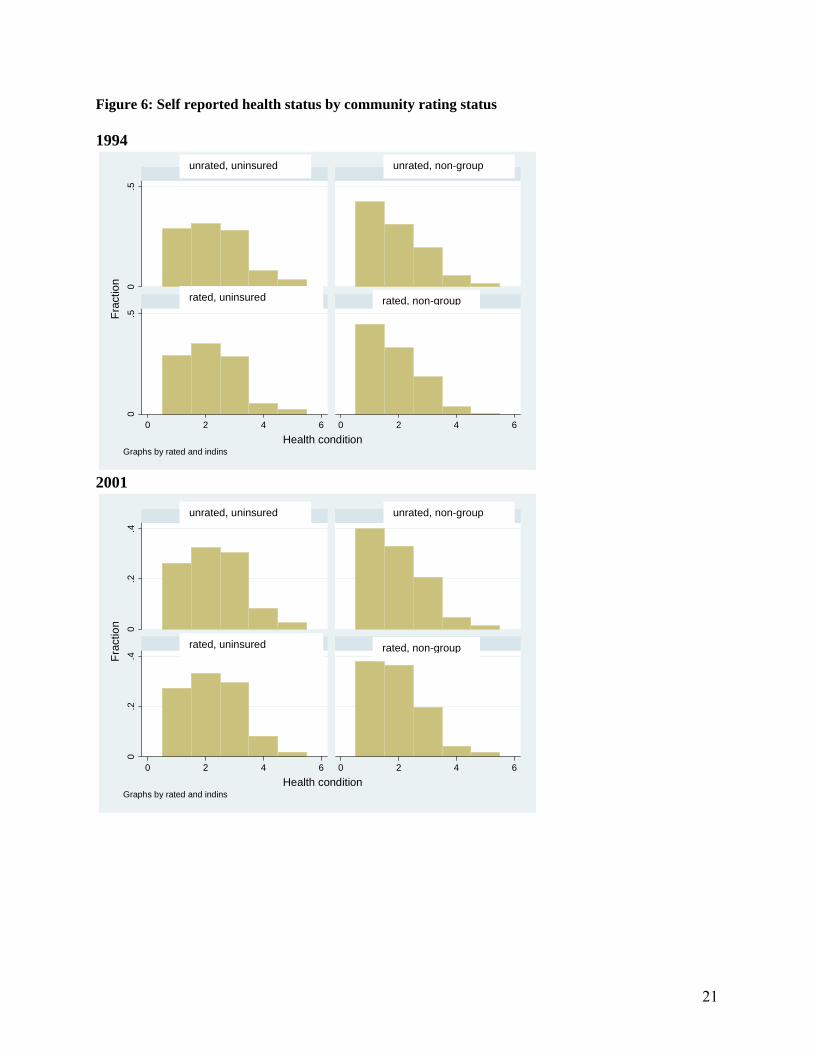
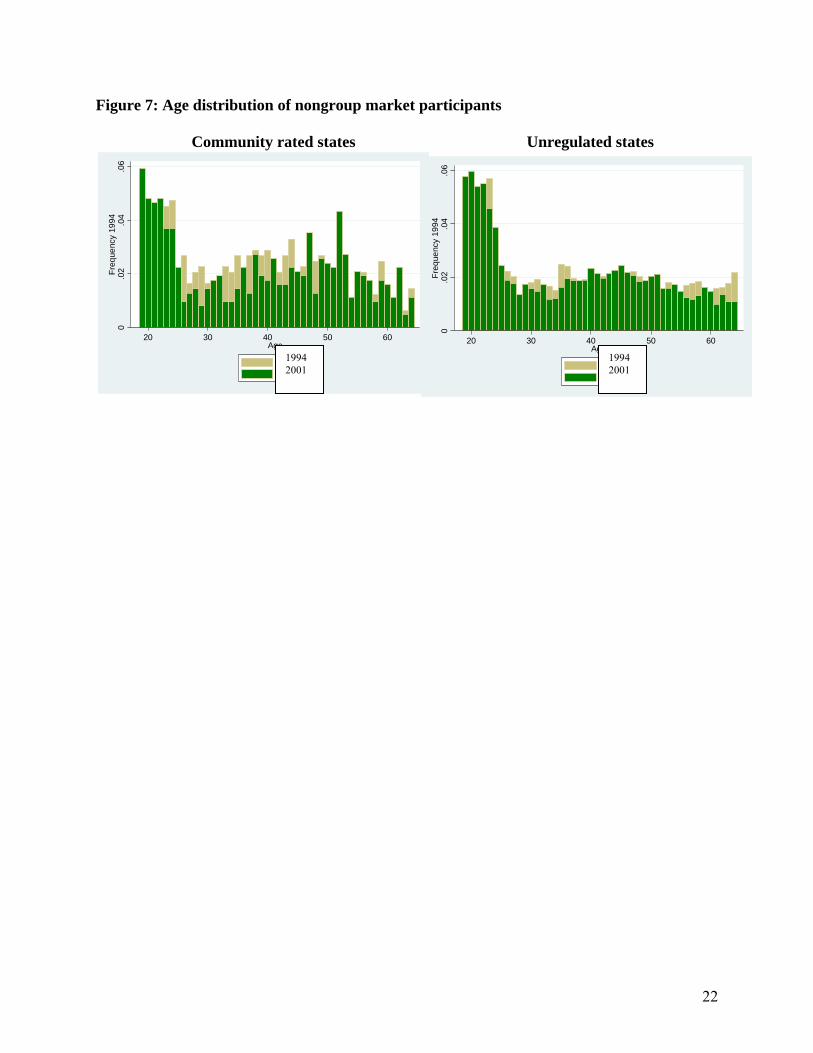
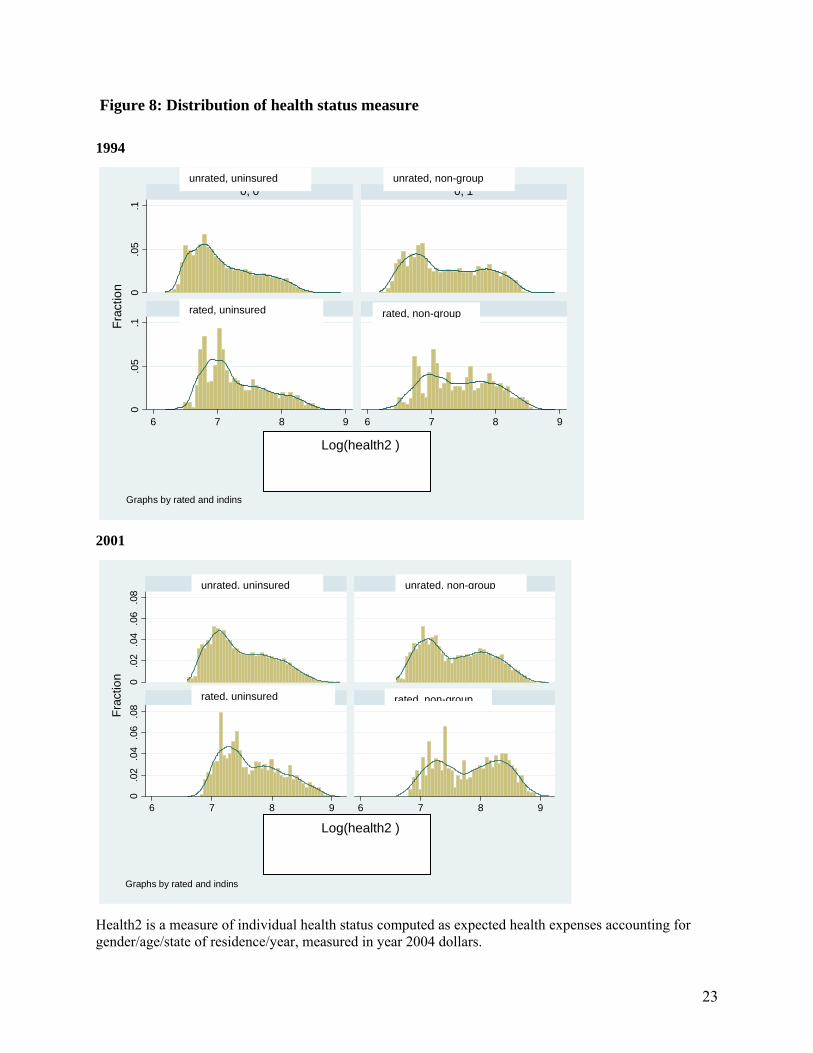
participation in the nongroup market in community rated states. Figures 6 through 8 offer a better picture
of some of the transitions in the rated and unregulated states over the period. Figure 6 indicates a small
increase in the fraction of non-group insured people in community rated states reporting poor health status.
Figure 7 indicates that there might have been a transition in age profile in the nongroup market in
community rated states, with the distribution becoming more bimodal than previously. In comparison, the
unregulated states have a stable distribution of age profiles.
Age and self-reported health status are important dimensions of health risk, but are obviously
imperfect proxies. To get at a better approximation of the distribution of health risks in states, I construct
two measures of individuals expected health status, Healthrisk and Healthrisk2, building on Auerbach
and Ohri (2006). The measure is a lower bound estimate of health expenses that any individual can expect
to have and is constructed as follows: Using a nation-wide insurer’s schedule of premiums for plans
offered in Florida (an unregulated state), I compute age- and gender-specific annual premiums for every
individual in any part of the country. Adding the deductible gives an estimate of expected health expenses
for individuals as if they were all residing in Florida in 2004. To convert this measure into the state- and
year-specific expenses they can expect, I use the league tables of state- and year-specific per capita
personal health care expenditures from the Center of Medicare and Medicaid Services (CMS) to construct
an index of expenses over time and states of residence relative to Florida in 2004. Figure 8 thus captures
the transition of health risks as the result of changes in age and gender composition in rated and unrated
states, and suggests that rated states might have seen a concentration at both the upper and the lower ends
of the distribution. Healthrisk2 is a measure that further adjusts Healthrisk1 upwards for individuals with
self-reported health on the basis of MEPS data on how the expected health expenses of individuals with
different self-reported health status relates to those in excellent health. While necessarily arbitrary, these
measures are intended to capture the fact that age, gender and self-reported health interact in predictable
ways and are used by insurers in forming an idea of the risk composition of the markets they sell in.
V. Models and results
V. 1 Evidence from Subpopulations on Selection
As a first pass at understanding if community rating affects coverage, I estimate models of the following
form:

12
— (2)
— (3)
where rated is one of two variables: being community rated, or years since being community rated. The
latter is intended to check if there is any evidence of a compounding of selection over time, in line with
the “death spiral” that was of concern when community rating was introduced.
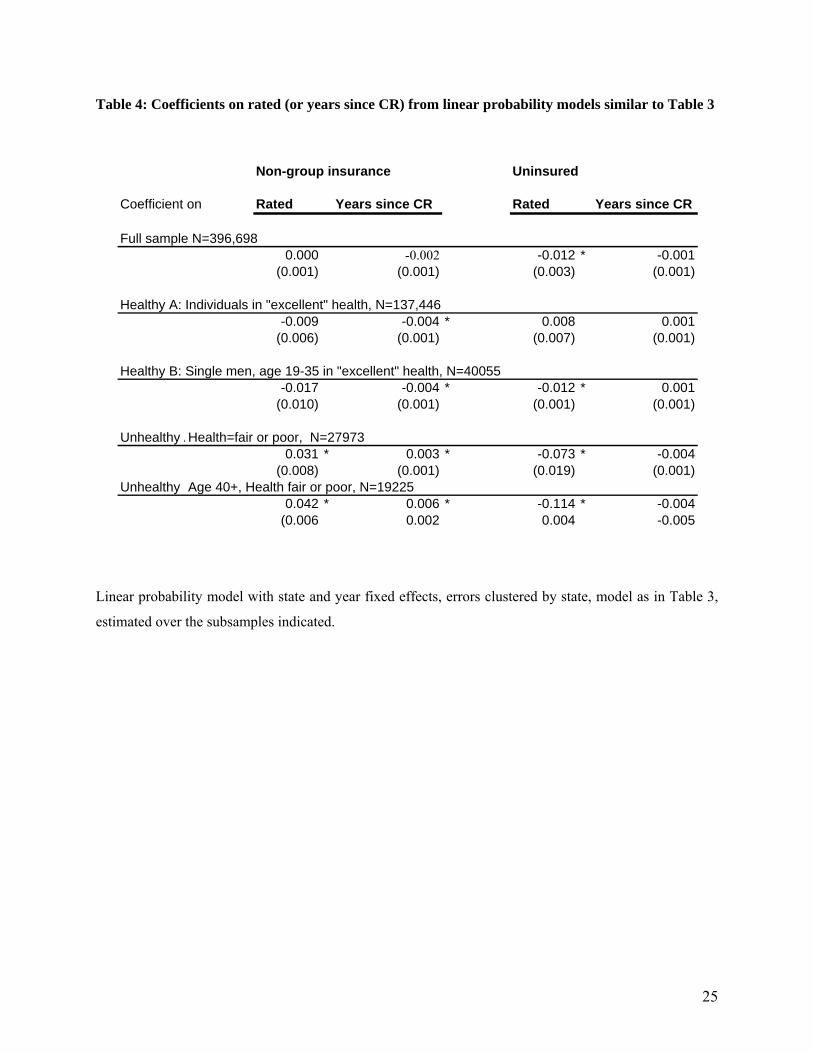
Table 3 presents results for a simple linear model of nongroup purchase as in equation (2) above, ,
while Table 4 collects the coefficients from running models (2) and (3) with the same covariatesas in
Table 3 on subsets of the population. All regressions cluster errors at the state level to address the possible
autocorrelation of errors (Bertrand et al., 2004) Overall, while there is little change at the entire sample
level, there does appear to be selection when the sample is restricted to the lowest and the highest risks.
Being in a community rated state is associated with younger men dropping non-group coverage, while
less healthy individuals stay on in the nongroup market. Remaining uninsured seems less likely to be the
case in rated states across all risks, though additional years since the introduction of community rating do
not tend to reduce uninsurance.
The above method of modeling is in line with recent work identifying the effect of community
rating as being different for the healthy and for those in poor health status (LoSasso and Lurie, 2007), and
the results are similar to that study. An advantage of the approach is that it indicates how a sample-level
result might mask compositional changes in precisely the issue of relevance to the present study, the
manner in which groups with different risks respond to rating restrictions. However, an estimation of the
decision to be in the nongroup market over the entire sample, or even on subgroups of health risks obtains
an average effect that confounds the different reasons why individuals might purchase insurance.
V.2 Purchase decisions and selection
To get a tighter prediction on whether community rating matters and whether it differentially
affects individuals along the distribution of health risks, I identify the subgroup most likely to be affected
by rating restrictions and estimate the following model:
— (4)
( )( ) εγβ
εγβ effects year effects state rated X uninsuredProb effects year effects state rated X nongroupProb
++++=++++=
11
εγγ
γγγβ
effects year effects state5healthy * affected* CR4healthy * affected
3healthy * CR affected* CR CR X ed)Prob(insur
+++++
+++= 21

13
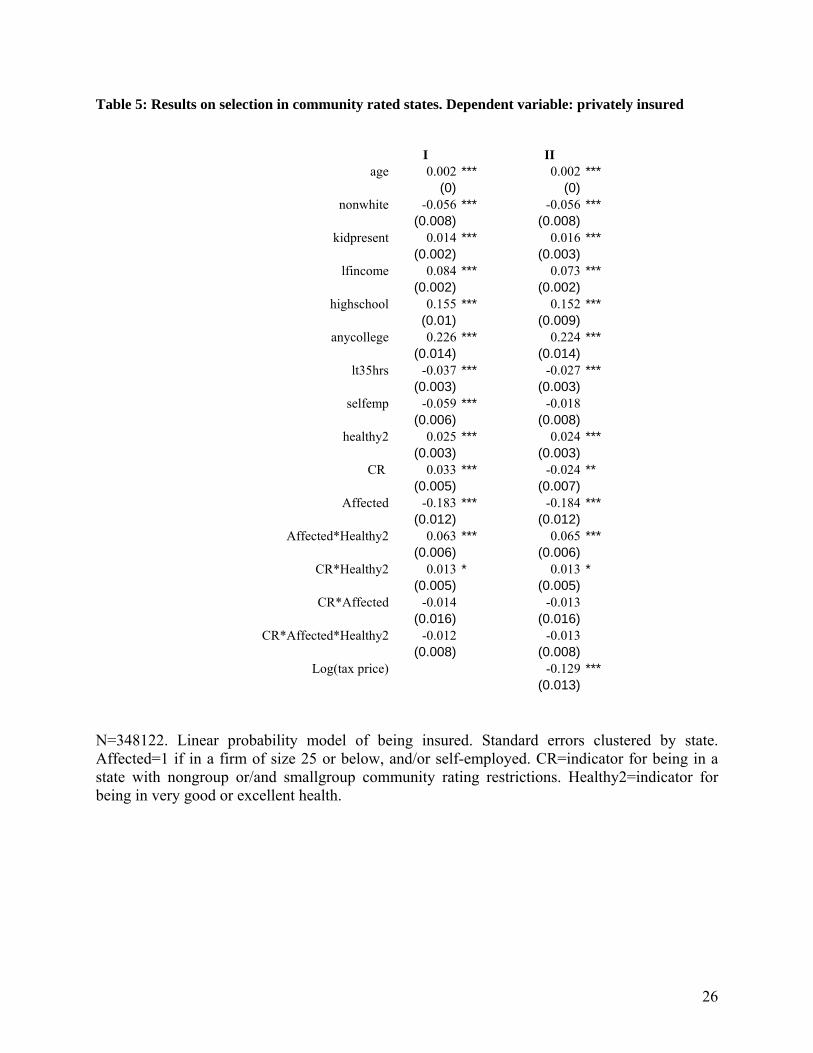
In the above, affected is an indicator for whether a person is in a firm of size less than 25, and/or
self-employed. CR is an indicator for having nongroup or small-group community rating restrictions and
healthy is an indicator for being in excellent or very good health. I later experiment with the more
continuous definition of health risk described in Section IV above . Table 5 indicates that those affected
in community rated states are slightly less likely to purchase insurance, the sign on the differential effect
for the healthiest for these individuals is as expected (the healthiest in the affected group less likely to
participate in rated states) but is not individually significant. Log(tax price) in Column II of Table 5
carries the expected sign—larger subsidies are associated with lower participation.
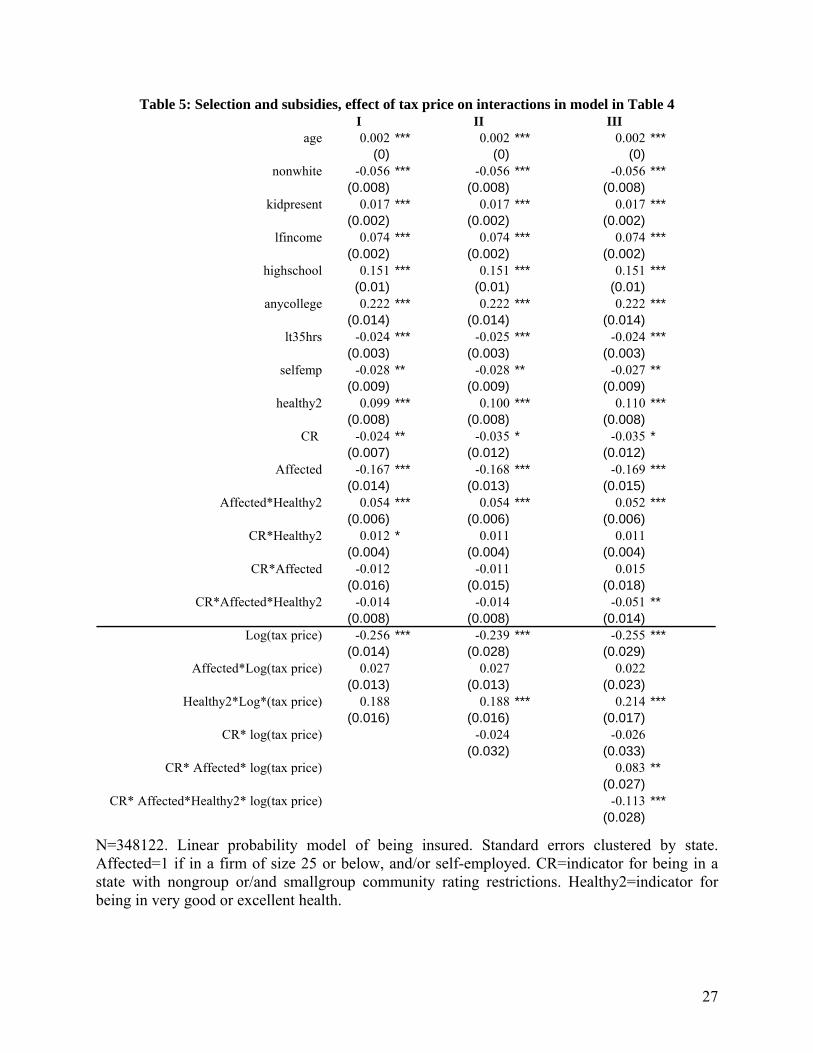
V.2 Effect of Subsidies
Modifying equation (4) above to incorporate the variation in tax prices yields estimation
equations of the form outlined in section III
— (5)
While Model (5) appears complex, it differs from (4) only in the addition of the variable
log(taxprice) and the interaction of log(taxprice) with the variables that identify a differential participation
by healthier individuals subjected to adverse selection. The main coefficient of interest is now 11γ , the
differential effect of being subsidized for healthier individuals in the affected subgroup in community
rated states. A higher tax price for healthier individuals is lowers their probability of purchasing insurance.
This is consistent with a subsidy being differentially beneficial in retaining healthier individuals in the
presence of adverse seleciton.
VI.3 Results with a continuous measure of health status
I now restrict the sample further to assess if the above model holds when the population
considered closer to those affected by nongroup market regulations (rather than both nongroup and small
εγ
γγγγγ
γγγγγβ
effects year effects state11ce)log(taxpri*healthy* affected* CR
10ce)log(taxpri*healthy* affected ce)log(taxpri*healthy * CR ce)log(taxpri* affected* CR 7price) log(tax*CR6 price) log(tax
5healthy * affected* CR4y health* affected 3healthy * CR affected* CR CR X ed)Prob(insur
++++
+++++
+++++=
98
21

14
group ratings). To select an appropriate sample for the exercise, I drop taxpayers in firms of employee
size between 25 to 500, where the likelihood of being offered employer sponsored insurance is higher. I
also drop individuals who receive coverage as dependents to focus on those without options to purchasing
insurance in their own name.The model I consider is simpler than (4) and (5) above but the health proxy I
now use is the continuous measure of expected health expenses outlined in Section IV. The model I
estimate is
— (6)
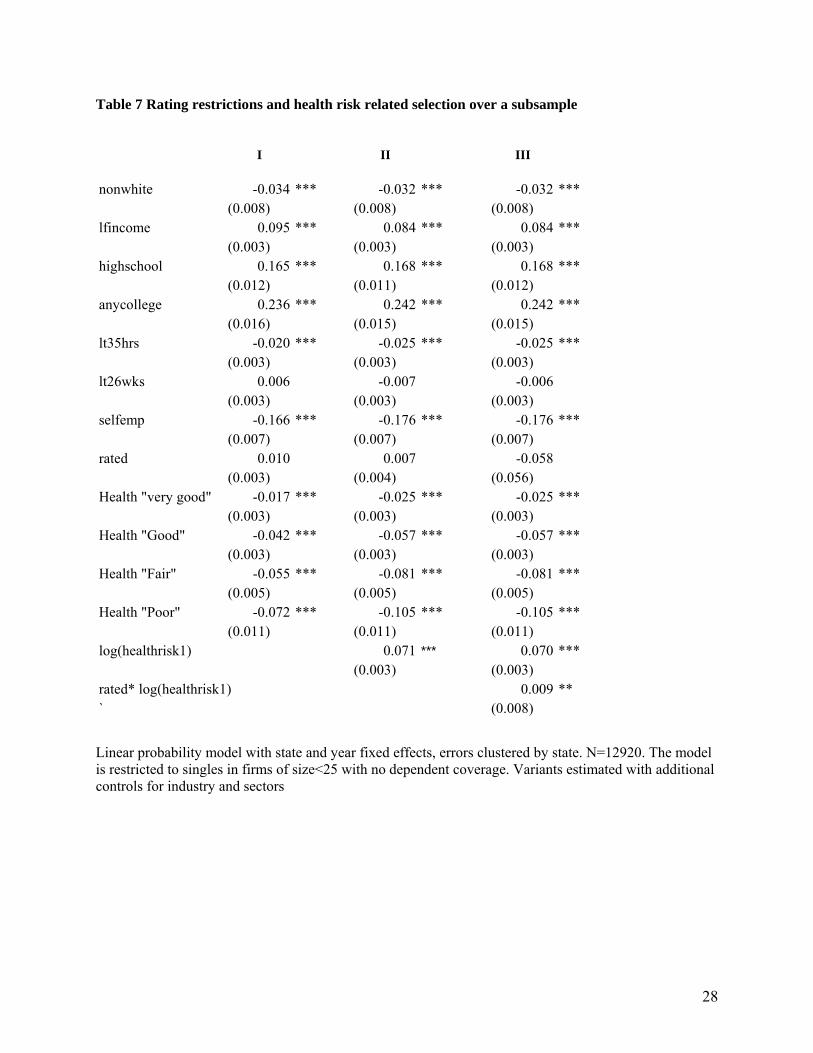
Table 7 presents results on selection using the measure Healthrisk1. Column III suggests that
residing in a community rated state increases the probability of an individual with higher expected health
expenses to purchase insurance. This might appear at odds with the result that poorer self-reported health
status is associated with lower purchase of insurance, but is consistent with the variables that drive
variation in Healthrisk1 (age and gender).
To assess if price variation has a differential role in affecting risk composition in community
rated states, I modify (4) above to estimate a model
The coefficient of interest is now 6γ . If subsidies have a role in preventing lower risks from
exiting the market for insurance in a community rated state, we would expect 6γ to be negative.
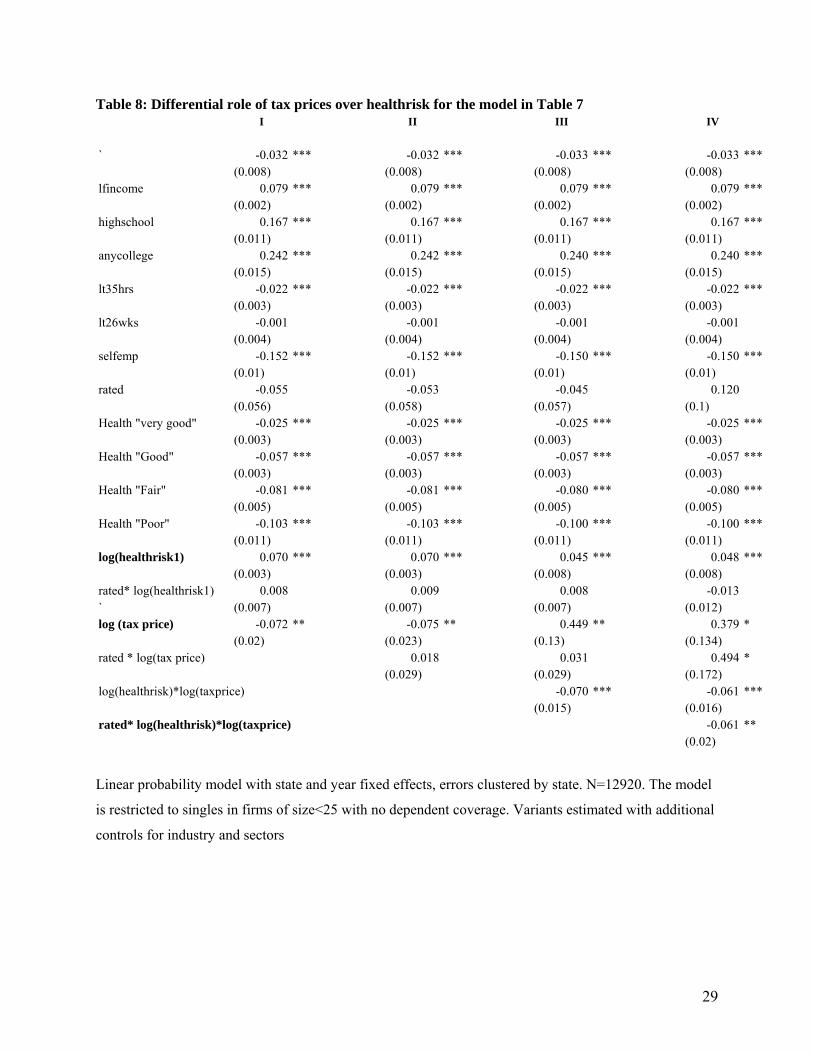
Table 8 presents results from Table 7 when the role of subsidies is accounted for. Columns I and II
suggest that tax prices matter—facing a one percent decline in tax price is associated with an increase
of .07 in the probability of purchasing insurance. The interaction of log(healthrisk1) and log(taxprice) in
Column III indicates that facing higher taxes—or lower subsidies—reduces the participation of those with
larger expected health expenses. Finally, column IV suggests that higher tax prices lower the
participation of more expensive individuals in community rated states. Put another way, receiving a larger
subsidy is differentially beneficial to individuals with lower health expenses in community rated states.
εγγγβ
effects year effects state 3 healthrisk* CR * CR CR X ed)Prob(insur
++++++= 21
εγγγ
γγγβ
effects year effects state6 healthrisk* CR*ce)log(taxpri 5CRtaxprice 4taxprice
3 healthrisk* CR CR CR X ed)Prob(insur
++++++
+++=*)log()log(
21

15
VI. Conclusion
The models estimated in the present study give credence to the concern that community rating restrictions
operate to change the profile of participants in the market for insurance, while subsidies—at least in the
context of subsidies implicitly induced by the tax system. From a policy standpoint, a subsidy offered
explicity, or one targeted better than the tax subsidy is likely to have an impact of a different magnitude.
The paper throws some light on considerations for how states might go about improving coverage. While
the take-up decision tends to be relatively insensitive to tax subsidies, premium subsidies likely impact
the risk profile of the pool of participants. The question this leads to, and one that cannot be answered
with the present data, is which particular ways individuals respond on the dimension of generosity of plan
choice, and whether subsidies can be more targeted to preserve the incentive for healther individuals to
participate, while also improving risk adjustment in insurance pools
16
REFERENCES Andreoni, J., 2006. “Philanthropy” in S-C. Kolm and J. Mercier Ythier, eds., Handbook of Giving, Reciprocity and Altruism, Amsterdam: North Holland, 2006, page 1201-1269 Auerbach, D and Ohri, S, 2006. “Price and the Demand for Non-Group Health Insurance,” Inquiry, 43(2), 122-134. Bertrand,M., Esther Duflo, D and Mullainathan,S., 2004. "How Much Should We Trust Differences-in-Differences Estimates?"; Quarterly Journal of Economics, 2004, 119(1), pp. 249-75. Buchmueller, T.C., and DiNardo, J., 2002. “Did Community Rating Induce an Adverse Selection Death Spiral? Evidence from New York, Pennsylvania and Connecticut,” American Economic Review, 92(1): 280-94. Cutler, D.M., and R.J. Zeckhauser, 1998. "Adverse selection in health insurance", in: A. Garber, ed., Frontiers in Health Policy Research, Vol. 1 (MIT Press, Cambridge, MA) 1-31. Heistaro, S, Jousilahti, P, Lahelma, E, Vartiainen, E, Puska, P, 2001. “Self rated health and mortality: a long term prospective study in eastern Finland.”J Epidemiol Community Health 55: 227-232 Herring, B., and M. Pauly, 2001. “Premium Variation in the Individual Insurance Market,” International Journal of Health Care Finance and Economics 1.1, 43-58. Lo Sasso, A.T., and Lurie I.Z., “Community Rating and the Market for Private Non-Group Health Insurance,” April 2007
Pauly, M. V., and L. M. Nichols, 2002. "The Non-Group Insurance Market: Short on Facts, Long on Opinions and Policy Disputes"
Pauly, M.V., A. Percy, and B. Herring, 1999. "Individual Versus Job-Based Health Insurance: Weighing the Pros and Cons." Health Affairs 18 (96): 28-44
Rothschild, M. and J.E. Stiglitz, 1976. “Equilibrium in Competitive Insurance Markets: An Essay on the Economics of Imperfect Information.” Quarterly Journal of Economics; 90(4):629-649. Royalty, A. B., 2000.Tax Preferences for Fringe Benefits and Workers' Eligibility for Employer Health Insurance, Journal of Public Economics, 75(2): 209-227. Selden, T., 1999. Premium Subsidies for Health Insurance: Excessive Coverage vs. Adverse Selection, Journal of Health Economics, 18: 709-725. Simon, K. 2005. "Adverse Selection in Health Insurance Markets: Evidence from State Small-Group Health Insurance Reforms".Journal of Public Economics, 89, pp.1865-1877. Turnbull, N.C. and Nancy M. Kane, N.M., 2005. Insuring the Healthy or Insuring the Sick? The Dilemma of Regulating the Individual Health Insurance Market Findings from a Study of Seven States. The Commonwealth Fund. Wachenheim L and Leida H, 2007 "The Impact of Guaranteed Issue and Community Rating Reforms on Individual Insurance Markets," report prepared by Milliman, Inc. on behalf of America’s Health Insurance Plans, August 2007

17
Wealth, health loss
W
Wealth, no health loss
FL
FH
P1
SL
O
O´
W´
ŪL
ŪH
P3
P2
Tables and Figures
Figure 1: Rothschild-Stiglitz separation and community-rating induced pooling.
Figure 2: Coverage without and with a subsidy
Q1 Q3 Qeff Quantity (take-up ) With a subsidy With adverse selection
A D E B F C
Average cost Marginal Cost Demand curve with subsidy
Price
Demand curve
18
Table 1: Community rating restrictions in state non-group markets
State Type of restriction Date of introduction
New YorkPure community rating, only differing by region April 1993
VermontModified CR for indemnity, pure CR for HMOs/ Blue Cross plans July 1993
New Jersey Pure CR August 1993
Maine
Modified CR, not allowed to vary by health, rating band of 1.5:1 for age December 1993
New Hampshire
Modified CR, rating band 3:1 for age, 1.2:1 for health. Repealed 2003 January 1995
WashingtonModified CR, band of 2:1 for age and 1.2:1 for health in 2002 January 1996
Kentucky
Modified, initially 3:! Band for age/geography/family composition but not health. Later allowed to vary 5:1. Repealed 1998 July 1996
Massachusetts
Modified CR, not allowed to vary by health, rating band of 1.33:1 for age August 1996
Sources: Auerbach and Ohri (2006), LoSasso and Lurie (2007), Wachenheimand Leida (2007)

19
Figure 3: Schedule of self-employed health Figure 4: Variation in tax price
deduction allowable as adjustment to income
Figure 5: Variation in tax price and variation in fraction insured over time in CR states
Panel A
Panel B
Tax subsidy (% premium)
0
20
40
60
80
100
120
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
Variation in mean taxprice within CR states, 1994 vs 2001
mean tp nonselfmp 94
mean tp selfemp 94
mean tp nonselfmp 01
mean tp selfemp 01
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10
Income decile
Mea
n ta
x pr
ice
Mean tax price by income decile, 1994
0.600
0.700
0.800
0.900
1.000
1 2 3 4 5 6 7 8 9 10
Income decile
Mea
n ta
x pr
ice
uninsured
insured
Variation in fraction insured within CR states, 1994 vs 2001
0.200
0.300
0.400
0.500
0.600
0.700
0.800
0.900
1.000
1 2 3 4 5 6 7 8 9 10
Income decile
Mea
n ta
x pr
ice
mean insurednonselfmp 94mean insured selfemp94
mean insurednonselfmp 01
mean insured selfemp01

20
Table 2: Summary statistics
1994 2001Unreg CR Unreg CR
Age 37.60 37.61 38.33 38.61(0.066) (0.161) (0.062) (0.13)
Female 0.34 0.39 0.43 0.44(0.003) (0.006) (0.002) (0.005)
Married 0.44 0.41 0.42 0.40(0.003) (0.006) (0.002) (0.005)
Nonwhite 0.17 0.19 0.19 0.18(0.002) (0.005) (0.002) (0.004)
Family income 35103.03 38120.68 49367.19 54032.51(172.318) (471.679) (271.413) (643.825)
Insured 0.77 0.76 0.77 0.78(0.002) (0.006) (0.002) (0.004)
Self employed 0.10 0.07 0.08 0.07(0.003) (0.006) (0.002) (0.005)
Nongroup insured 0.24 0.24 0.24 0.20
(0.004) (0.01) (0.004) (0.008)Healthy 0.89 0.93 0.90 0.90
(0.003) (0.006) (0.003) (0.006)Health2 1429.43 1726.54 2060.24 2488.04
(7.951) (22.55) (10.575) (28.683)Taxprice 0.79 0.78 0.79 0.79
(0.002) (0.004) (0.001) (0.003)
CR stands for Community Rated (the 8 states of NY, VT, NJ, ME, NH, WA, KY, MA). Sample means and standard errors are computed using CPS person weights. Healthy stands for individuals with self-reported health good/verygood or excellent. Health2 is a measure of individual health status computed as expected health expenses accounting for gender/age/state of residence/year, measured in year 2004 dollars.
21
Figure 6: Self reported health status by community rating status 1994
0.5
0.5
0 2 4 6 0 2 4 6
0, 0 0, 1
1, 0 1, 1
Frac
tion
Health conditionGraphs by rated and indins
2001
0.2
.40
.2.4
0 2 4 6 0 2 4 6
0, 0 0, 1
1, 0 1, 1
Frac
tion
Health conditionGraphs by rated and indins
unrated, uninsured unrated, non-group
rated, non-grouprated, uninsured
unrated, uninsured unrated, non-group
rated, non-grouprated, uninsured
22
0.0
2.0
4.0
6Fr
eque
ncy
1994
20 30 40 50 60Age
FractionFraction
Figure 7: Age distribution of nongroup market participants
Community rated states Unregulated states 0
.02
.04
.06
Freq
uenc
y 19
94
20 30 40 50 60Age
FractionFraction
1994 2001
1994 2001
23
Figure 8: Distribution of health status measure
1994 0
.05
.10
.05
.1
6 7 8 9 6 7 8 9
0, 0 0, 1
1, 0 1, 1
Fractionkdensity lprem1
Frac
tion
lprem1
Graphs by rated and indins
2001
0.0
2.0
4.0
6.0
80
.02
.04
.06
.08
6 7 8 9 6 7 8 9
0, 0 0, 1
1, 0 1, 1
Fractionkdensity lprem1
Frac
tion
lprem1
Graphs by rated and indins
Health2 is a measure of individual health status computed as expected health expenses accounting for gender/age/state of residence/year, measured in year 2004 dollars.
Log(health2 )
Log(health2 )
unrated, uninsured unrated, non-group
rated, non-grouprated, uninsured
unrated, uninsured unrated, non-group
rated non-grouprated, uninsured

24
Table 3: Linear probability model of private non-group market participation on covariates N=396,698. Linear probability model with state and year fixed effects, errors clustered by state.Emplsz stands for categories of firm size
I IIAge 25-29 -0.045 *** -0.045 ***
(0.004) (0.004)30-34 -0.049 *** -0.049 ***
(0.005) (0.005)35-39 -0.041 *** -0.041 ***
(0.005) (0.005)40-44 -0.036 *** -0.036 ***
(0.005) (0.005)45-49 -0.034 *** -0.034 ***
(0.005) (0.005)50-54 -0.029 *** -0.029 ***
(0.005) (0.005)55-59 -0.019 *** -0.019 ***
(0.005) (0.005)60-64 -0.010 * -0.010
(0.006) (0.006)female 0.003 ** 0.003 **
(0.001) (0.001)nonwhite -0.016 *** -0.016 ***
(0.002) (0.002)married -0.029 *** -0.029 ***
(0.002) (0.002)kidpresent 0.002 * 0.002 *
(0.001) (0.001)lfincome -0.007 *** -0.007 ***
(0.002) (0.002)highschool 0.026 *** 0.026 ***
(0.002) (0.002)anycollege 0.053 *** 0.053 ***
(0.004) (0.004)less than35hrs 0.049 *** 0.049 ***
(0.003) (0.003)less than 26 wk 0.019 *** 0.019 ***
(0.003) (0.003)agmincon -0.048 ** -0.048 **
(0.013) (0.013)manuf -0.046 ** -0.046 **
(0.013) (0.013)services -0.037 ** -0.037 **
(0.013) (0.013)_Iemplsz_1 0.087 *** 0.087 ***
(0.015) (0.015)_Iemplsz_2 0.042 ** 0.042 **
(0.015) (0.015)_Iemplsz_3 0.023 0.023
(0.014) (0.014)_Iemplsz_4 0.012 0.012
(0.015) (0.015)_Iemplsz_5 0.008 0.008
(0.015) (0.015)_Iemplsz_6 0.006 0.006
(0.015) (0.015)selfemp 0.135 *** 0.135 ***
(0.007) (0.007)rated 0.000
(0.003)Years since CR -0.002 **
25
Table 4: Coefficients on rated (or years since CR) from linear probability models similar to Table 3
Non-group insurance Uninsured
Coefficient on Rated Years since CR Rated Years since CR
Full sample N=396,6980.000 -0.002 -0.012 * -0.001
(0.001) (0.001) (0.003) (0.001)
Healthy A: Individuals in "excellent" health, N=137,446-0.009 -0.004 * 0.008 0.001
(0.006) (0.001) (0.007) (0.001)
Healthy B: Single men, age 19-35 in "excellent" health, N=40055-0.017 -0.004 * -0.012 * 0.001
(0.010) (0.001) (0.001) (0.001)
Unhealthy AHealth=fair or poor, N=279730.031 * 0.003 * -0.073 * -0.004
(0.008) (0.001) (0.019) (0.001)Unhealthy Age 40+, Health fair or poor, N=19225
0.042 * 0.006 * -0.114 * -0.004(0.006 0.002 0.004 -0.005
Linear probability model with state and year fixed effects, errors clustered by state, model as in Table 3,
estimated over the subsamples indicated.
26
Table 5: Results on selection in community rated states. Dependent variable: privately insured
I IIage 0.002 *** 0.002 ***
(0) (0)nonwhite -0.056 *** -0.056 ***
(0.008) (0.008)kidpresent 0.014 *** 0.016 ***
(0.002) (0.003)lfincome 0.084 *** 0.073 ***
(0.002) (0.002)highschool 0.155 *** 0.152 ***
(0.01) (0.009)anycollege 0.226 *** 0.224 ***
(0.014) (0.014)lt35hrs -0.037 *** -0.027 ***
(0.003) (0.003)selfemp -0.059 *** -0.018
(0.006) (0.008)healthy2 0.025 *** 0.024 ***
(0.003) (0.003)CR 0.033 *** -0.024 **
(0.005) (0.007)Affected -0.183 *** -0.184 ***
(0.012) (0.012)Affected*Healthy2 0.063 *** 0.065 ***
(0.006) (0.006)CR*Healthy2 0.013 * 0.013 *
(0.005) (0.005)CR*Affected -0.014 -0.013
(0.016) (0.016)CR*Affected*Healthy2 -0.012 -0.013
(0.008) (0.008)Log(tax price) -0.129 ***
(0.013)
N=348122. Linear probability model of being insured. Standard errors clustered by state. Affected=1 if in a firm of size 25 or below, and/or self-employed. CR=indicator for being in a state with nongroup or/and smallgroup community rating restrictions. Healthy2=indicator for being in very good or excellent health.
27
Table 5: Selection and subsidies, effect of tax price on interactions in model in Table 4 I II III
age 0.002 *** 0.002 *** 0.002 ***(0) (0) (0)
nonwhite -0.056 *** -0.056 *** -0.056 ***(0.008) (0.008) (0.008)
kidpresent 0.017 *** 0.017 *** 0.017 ***(0.002) (0.002) (0.002)
lfincome 0.074 *** 0.074 *** 0.074 ***(0.002) (0.002) (0.002)
highschool 0.151 *** 0.151 *** 0.151 ***(0.01) (0.01) (0.01)
anycollege 0.222 *** 0.222 *** 0.222 ***(0.014) (0.014) (0.014)
lt35hrs -0.024 *** -0.025 *** -0.024 ***(0.003) (0.003) (0.003)
selfemp -0.028 ** -0.028 ** -0.027 **(0.009) (0.009) (0.009)
healthy2 0.099 *** 0.100 *** 0.110 ***(0.008) (0.008) (0.008)
CR -0.024 ** -0.035 * -0.035 *(0.007) (0.012) (0.012)
Affected -0.167 *** -0.168 *** -0.169 ***(0.014) (0.013) (0.015)
Affected*Healthy2 0.054 *** 0.054 *** 0.052 ***(0.006) (0.006) (0.006)
CR*Healthy2 0.012 * 0.011 0.011(0.004) (0.004) (0.004)
CR*Affected -0.012 -0.011 0.015(0.016) (0.015) (0.018)
CR*Affected*Healthy2 -0.014 -0.014 -0.051 **(0.008) (0.008) (0.014)
Log(tax price) -0.256 *** -0.239 *** -0.255 ***(0.014) (0.028) (0.029)
Affected*Log(tax price) 0.027 0.027 0.022(0.013) (0.013) (0.023)
Healthy2*Log*(tax price) 0.188 0.188 *** 0.214 ***(0.016) (0.016) (0.017)
CR* log(tax price) -0.024 -0.026(0.032) (0.033)
CR* Affected* log(tax price) 0.083 **(0.027)
CR* Affected*Healthy2* log(tax price) -0.113 ***(0.028)
N=348122. Linear probability model of being insured. Standard errors clustered by state. Affected=1 if in a firm of size 25 or below, and/or self-employed. CR=indicator for being in a state with nongroup or/and smallgroup community rating restrictions. Healthy2=indicator for being in very good or excellent health.
28
Table 7 Rating restrictions and health risk related selection over a subsample
I II III
nonwhite -0.034 *** -0.032 *** -0.032 ***(0.008) (0.008) (0.008)
lfincome 0.095 *** 0.084 *** 0.084 ***(0.003) (0.003) (0.003)
highschool 0.165 *** 0.168 *** 0.168 ***(0.012) (0.011) (0.012)
anycollege 0.236 *** 0.242 *** 0.242 ***(0.016) (0.015) (0.015)
lt35hrs -0.020 *** -0.025 *** -0.025 ***(0.003) (0.003) (0.003)
lt26wks 0.006 -0.007 -0.006(0.003) (0.003) (0.003)
selfemp -0.166 *** -0.176 *** -0.176 ***(0.007) (0.007) (0.007)
rated 0.010 0.007 -0.058(0.003) (0.004) (0.056)
Health "very good" -0.017 *** -0.025 *** -0.025 ***(0.003) (0.003) (0.003)
Health "Good" -0.042 *** -0.057 *** -0.057 ***(0.003) (0.003) (0.003)
Health "Fair" -0.055 *** -0.081 *** -0.081 ***(0.005) (0.005) (0.005)
Health "Poor" -0.072 *** -0.105 *** -0.105 ***(0.011) (0.011) (0.011)
log(healthrisk1) 0.071 *** 0.070 ***(0.003) (0.003)
rated* log(healthrisk1) 0.009 **` (0.008)
Linear probability model with state and year fixed effects, errors clustered by state. N=12920. The model is restricted to singles in firms of size<25 with no dependent coverage. Variants estimated with additional controls for industry and sectors
29
Table 8: Differential role of tax prices over healthrisk for the model in Table 7 I II III IV
` -0.032 *** -0.032 *** -0.033 *** -0.033 ***(0.008) (0.008) (0.008) (0.008)
lfincome 0.079 *** 0.079 *** 0.079 *** 0.079 ***(0.002) (0.002) (0.002) (0.002)
highschool 0.167 *** 0.167 *** 0.167 *** 0.167 ***(0.011) (0.011) (0.011) (0.011)
anycollege 0.242 *** 0.242 *** 0.240 *** 0.240 ***(0.015) (0.015) (0.015) (0.015)
lt35hrs -0.022 *** -0.022 *** -0.022 *** -0.022 ***(0.003) (0.003) (0.003) (0.003)
lt26wks -0.001 -0.001 -0.001 -0.001(0.004) (0.004) (0.004) (0.004)
selfemp -0.152 *** -0.152 *** -0.150 *** -0.150 ***(0.01) (0.01) (0.01) (0.01)
rated -0.055 -0.053 -0.045 0.120(0.056) (0.058) (0.057) (0.1)
Health "very good" -0.025 *** -0.025 *** -0.025 *** -0.025 ***(0.003) (0.003) (0.003) (0.003)
Health "Good" -0.057 *** -0.057 *** -0.057 *** -0.057 ***(0.003) (0.003) (0.003) (0.003)
Health "Fair" -0.081 *** -0.081 *** -0.080 *** -0.080 ***(0.005) (0.005) (0.005) (0.005)
Health "Poor" -0.103 *** -0.103 *** -0.100 *** -0.100 ***(0.011) (0.011) (0.011) (0.011)
log(healthrisk1) 0.070 *** 0.070 *** 0.045 *** 0.048 ***(0.003) (0.003) (0.008) (0.008)
rated* log(healthrisk1) 0.008 0.009 0.008 -0.013` (0.007) (0.007) (0.007) (0.012)log (tax price) -0.072 ** -0.075 ** 0.449 ** 0.379 *
(0.02) (0.023) (0.13) (0.134)rated * log(tax price) 0.018 0.031 0.494 *
(0.029) (0.029) (0.172)log(healthrisk)*log(taxprice) -0.070 *** -0.061 ***
(0.015) (0.016)rated* log(healthrisk)*log(taxprice) -0.061 **
(0.02)
Linear probability model with state and year fixed effects, errors clustered by state. N=12920. The model
is restricted to singles in firms of size<25 with no dependent coverage. Variants estimated with additional
controls for industry and sectors