Embed Size (px)
Citation preview

1732 JADA, Vol. 129, December 1998
A B S T R A C T It is ironic that use of one of dentistry’s most important develop-ments of the last 15 years, predictable implant dentistry, is actuallybeing discouraged by many dentists.1,2 Patients who want implantsoften have to search for dentists to provide this care.
Predictable osseointegrated implants have been used in theUnited States since 1982, when the Nobelpharma implant(Brånemark system, Nobel Biocare, Gothenburg, Sweden) was in-troduced into North America. Unfortunately, many of the tech-niques associated with that implant made it difficult and costly totreat partially edentulous patients. The excessive chair time, com-ponent costs and laboratory expense have limited the use of im-plants to only a few dentists and relatively affluent patients.Although it has been reported that as many as 40, 50 or even 60percent of general dentists are restoring implants, most of themhave used implants in very few cases.3 It has been estimated thatonly 4,000 of the 110,000 general dentists in the United States re-store four or more implant cases a year.4
In an attempt to promote affordable implant dentistry, andthereby encourage more restorative dentists to treat more of theiraverage patients with implants, I reviewed the literature on thetechniques being used, which perhaps were based more on histori-cal use than dental common sense. With the use of a screwless im-plant system and elimination or modification of some of the oldtechniques, implant prosthetics can be just as affordable as conven-tional crown-and-bridge dentistry.
OPERATIVE SETTING
The first thing to examine is the reported need for sterility at the level found in hospital operating rooms, or ORs. Professor Per-Ingmar Brånemark, who introduced osseointegration techniques intoNorth America, had a background as an orthopedist, and as such wasused to operating under very sterile conditions in hospital ORs.5 Itmade sense to his team of surgeons and engineers to design an im-plant fixture consistent with their orthopedic experience, and to de-sign a procedure for placing it that required an OR environment.
However, this requirement created problems when dentists in
AFFORDABLE IMPLANT PROSTHETICSUSING A SCREWLESS IMPLANT SYSTEMNORMAN J. SHEPHERD, D.M.D.
Many dentists have been reluc-
tant to place dental implants be-
cause they have found that most
implants are costly and time-con-
suming to place and have long-
term maintenance problems.
Most of these problems are
caused by using screws to con-
nect the abutment to the im-
plant, the crown to the abutment
or both. The use of a screwless
implant system and conventional
prosthetics, the author con-
tends, can make implant den-
tistry affordable, versatile and
easy to incorporate into all gen-
eral dental practices.
JA D
A
CO
NT
I
NU
I N G E D UC
AT
IO
N
✷✷
ARTICLE 3
Copyright ©1998-2001 American Dental Association. All rights reserved.

which allowed easy access tothe individual fixtures for ex-amination during the experi-mentation years. It also allowedeasy access to the stacked com-ponents for maintenance pur-poses. Unfortunately, screw-re-tained prosthetics created amultiplicity of problems, suchas screw loosening and break-age.7-13 Screws are time-consum-ing to place, costly and unpre-dictable. Connecting a crown toan implant has to be one of themost basic acts of implant den-tistry; yet, after 15 years, westill see journal articles abouthow to keep screws tight. Thisfact alone raises questionsabout the entire process. Ifscrews are used, the dentistneeds not only a variety ofscrewdrivers, but also expensivetorque drivers.
An increasing number of clin-icians have begun to realizethat use of cement-retainedprosthetics is a better tech-nique. One large commerciallaboratory in the United Statessent letters to all of its dentistcustomers explaining that itwould no longer fabricate im-plants that used screw-retainedprosthetics (James R. Glidewell,written communication, Oct. 5,1993). There are many advan-tages to cement-retainedcrowns, such as the ability tomaintain normal anatomy, im-proved esthetics and compensa-tion for casting inaccuracies. Onthe other hand, there are manyfactors that cause implantscrews to loosen: dpoor occlusion; dparafunctional habits; dcantilevers;dpoor component tolerances;dinaccurate castings;dinadequate tightening;dtoo much tightening;dsingle tooth torque.
JADA, Vol. 129, December 1998 1733
CLINICAL PRACTICE
the United States attempted toduplicate their suggestions.Most health insurance pro-grams would not cover hospital-ization for dental implants, andconverting a typical dental op-eratory into an OR is extremelytime-consuming and expensive.
In 1993, a group from NewYork University published an ar-
ticle demonstrating that im-plants could be placed successful-ly in a dental office or a clinic.6
This eliminates the need for themore costly hospital OR setting.
PROBLEMS WITH SCREW-RETAINED PROSTHETICS
The Brånemark group usedscrew-retained prosthetics,
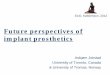
Figure 1. Cross-section of the Bicon implant (Bicon Implant System)demonstrating locking taper. Compare with conventional implantcomponents.
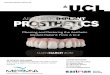
Figure 2. Bicon abutment ready for final impression. Note the soft-tissuematuration and the preformed gingival sulcus.
Copyright ©1998-2001 American Dental Association. All rights reserved.

1734 JADA, Vol. 129, December 1998
CLINICAL PRACTICE
The literature indicates thatthe main advantage of screw-re-tained prosthetics is retrievabili-ty, but bridgework retained bytemporary cement is much moreeasily retrievable than a pros-thesis retained by multiplescrews. Since neither caries norsensitive dentin is a problem ifcement washes out, there is noreal reason not to use temporarycement. Use of cementable pros-thetics for treating natural teethis the standard in dental schools,and dentists are familiar andcomfortable with this approach.Screw-retained prosthetics re-quire totally different techniquesand instrumentation that mustbe learned if a dentist wishes topractice implant dentistry.
PROBLEMS WITHEXTERNAL HEXIMPLANTS
Another concern is the externalhex-top implant, a configurationthat has been copied by morethan a dozen implant compa-nies and has become the indus-try standard for prosthetic at-tachments. Unfortunately, thisdesign has two inherent prob-lems: metal dilation and embed-ment relaxation.
Metal dilation. The hex topwas designed as a rotationaltorque transfer mechanism toturn the implant into the bone,and it successfully performs thattask.14 Unfortunately, the classi-cal external hex is a poor way toconnect other components. It isnot a true antirotational device,and this leads to micromotion,bacterial leakage and bone cra-tering.15,16 The 0.7-millimeterheight of the hex gives very littleprotection against lateral forces,and the thinness of the hex wallsmakes them subject to metal di-lation, which in turn createslooseness at the top threads.
This looseness is a predictor ofbroken screws.
The distance across the flatsof the external hex is 2.68 mil-limeters, and the diameter ofthe internal thread that passesthrough the top is 2.02 mm. Thedistance across the flats shouldbe greater than 3.03 mm to pre-vent the hex wall from dilating.Unfortunately, this dilation,which is caused by the wedgingaction of the screw as it is tight-ened, remains throughout thelife of the implant.17
Embedment relaxation. Asecond problem is embedmentrelaxation. When two machinedcomponents are screwed togeth-er with a torque wrench, it willtighten to that particulartorque. After a few minutes, theclinician will find that he or shecan turn the wrench againslightly to reach that sametorque. What is happening isthat the slight machining irreg-ularities of the surfaces actuallyflatten and allow the two com-ponents to be more closely ap-proximated. This flattening or
Figure 3. Crown cemented on Bicon abutment with either temporary orpermanent cement.
creep continues under occlusalforces; therefore, the preload thatoriginally had been used whentightening was first accomplishedloses its effect and contributes tobroken screw problems.18
COST-EFFECTIVETECHNIQUES FORIMPLANT DENTISTRY
Eliminating these expensive prob-lems is one part of creating cost-effective implant dentistry. Theother part is to use less expensivetechniques for fabricating pros-thetics. The first prerequisite,then, is to use a true nonrotation-al system. Most of these havesome sort of a bevel at the abut-ment-implant interface to providegood metal-to-metal contact.Friction between the two surfacesprevents the rotation. Some sys-tems use screws to hold the com-ponents together. One system, theBicon Implant (Bicon ImplantSystem), uses a locking taper thatrequires no screw at the abut-ment-implant interface (Figure 1).This is a true nonrotational con-nection that has been used in or-
Copyright ©1998-2001 American Dental Association. All rights reserved.

JADA, Vol. 129, December 1998 1735
CLINICAL PRACTICE
thopedic hip replacements formany years. It also is used tohold the chuck to the shaft ofthe dental lathe. This lockingtaper allows no micromotionand also provides a bacterialseal.16
When a true nonrotationalabutment such as this is used,the final abutment can beplaced during second-stagesurgery, and it then is treatedlike a natural tooth. There is noneed for healing caps, impres-sion posts or transfer copings.This eliminates a great deal ofinventory and extra office visits.If the abutment needs modifica-tion, it can be done either out ofthe mouth before placement orin the mouth after placement. Anumber 1557 carbide bur (S.S.White Burs Inc.) cuts the titani-um very effectively with mini-mum heat.19 A temporary crowncan be placed at the second-stage visit if needed (areas thatare not esthetically importantrequire no temporary crown).The final impression is takenafter soft-tissue maturation hasoccurred, and the crown is thencemented in place (Figures 2and 3). Temporary cement is
used for large bridges; perma-nent cement generally is usedfor single-tooth implants. Thelaboratory bills will be the sameas those for natural tooth pros-
thetics, and the chair time is ac-tually less than that for the fab-rication of a crown for a naturaltooth. The ability to use conven-tional prosthetic techniques torestore the implant abutment iscritical for truly cost-effectiveimplant dentistry. The restora-tive dentist does not need topurchase an implant prosthetickit. All of the necessary restora-tive procedures are familiar tothe dentist, the office staff andthe dental laboratory.
Ironically, the only otherscrewless implant systems thatcan be used in this manner are
those that were used in the1960s and 1970s. These systemsused one-piece implants, suchas blades, screws and subperio-steal implants, in which theabutment was part of the im-plant and therefore treated similarly to a natural tooth.Unfortunately, osseointegrationwas not as predictable as it waswith the two-stage implant sys-tems or the more recent one-stage unloaded systems.
Modern implant manufactur-ers are aware of the problemand have tried to find an an-swer. The ITI implant(Strauman) and the Astratechimplant systems (Astratech) usea beveled abutment-implant in-terface to address the antirota-tional problem. The Calcitek(Sulzer Calcitek) spline has amechanical interlock, andScrew-Vent (Paragon) has aninternal hex with a slight taperlock. All of these implant sys-tems, however, still require ascrew to mechanically clampthe parts together.
In the case of an edentulouspatient, the nonrotational natureof these abutments eliminatesthe need for a cast bar, and this
TABLE
BICON IMPLANT SYSTEM
Implant Type Implant Type
OTHER IMPLANT SYSTEMS
CostCost
COMPARISON OF LABORATORY COSTS.
$190
$80 ($40 if done chairside)
$160 ($80 if donechairside)
$80-$130 (lab feessame as those fornatural teeth)
$450-$1,000
$900-$1,400
$500-$700
$300-$400
Bicon Bar*
O-rings: implants
O-rings: implants
Single Crown
Porcelain fused to metal
Cast Overdenture Bar
Two implants
Four implants
Single Crown on Hex Top
Cera One-type abutment(Nobel Biocare Inc.)
UCLA
* Bicon Implant System.
The ability to useconventional pros-thetic techniques torestore the implantabutment is criticalfor truly cost-effec-tive implant dentistry.
Copyright ©1998-2001 American Dental Association. All rights reserved.

1736 JADA, Vol. 129, December 1998
CLINICAL PRACTICE
in turn allows individual balls orO-ring abutments to be used. If apatient can afford the surgerynecessary to place two implants,then the prosthetic cost of an O-ring–retained overdenture isminimal. These are simpler tech-niques with significantly lowerlaboratory cost (Table). Much ofthe fabrication can be done atchairside if the patient alreadyhas a well-made denture.20 Thelocking taper shaft of the BiconImplant allows for the use of 15-degree O-ring abutments, whichis a considerable help in treatingmaxillary cases. If a patient al-ready has denture support of twoballs or O-rings, the dentist canlater add additional implantsand convert the overdenture tofixed bridgework, even if the pa-tient has to wear a laboratory-cured provisional bridge for ayear or two before he or she canafford the final metal-porcelainbridge. In other words, definitivetreatment does not have to bedone at one time. A patient canstart with a relatively inexpen-sive treatment and then, as he orshe can afford it, graduate to amore ideal fixed prosthesis.
A true overdenture should besoft-tissue–borne and retainedonly by the mechanical deviceattached to the implant. Forthis reason, it is not necessaryto link the implants. Such link-age certainly is not needed toprevent rotation of the individu-al abutments. The flexibility ofthese abutments allows a regu-lar menu of treatment optionsthat permit implant dentistry tobecome affordable to the majori-ty of dental patients, instead ofjust the wealthy.
The single-tooth implantrestoration—which in manysystems is extremely difficult, if not impossible, to place inposterior areas because of the
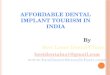
rotational torque—becomes avery simple post-and-core pros-thetic restoration with screw-less implants. Single-molar implants can be restored andseveral single crowns can evenbe placed side by side (Figure4). This obviates the problem of inaccurate casting for multi-ple crowns. It more closely duplicates normal anatomy and allows the patient the luxu-
Figure 4. A. Four individual premolar and molar crowns—three on Biconabutments and the anterior crown on a natural tooth. B. Radiographicappearance.
A
B
ry of normal hygiene tech-niques. Unlike a natural-toothcrown, the margin of an implantcrown needs to be placed sub-gingivally only in estheticallyimportant areas. The castingcan be at or above the gingivallevel in the mesial, distal orpalatal/lingual areas (Figure 5).
The single-tooth implantrestoration allows the cost of asingle implant and crown to be
Copyright ©1998-2001 American Dental Association. All rights reserved.

ever, to perform implant pros-thetics in a cost-effective man-ner, which in turn greatly in-creases the availability of thetreatment modality to the gen-eral dental population. By com-bining a screwless implant system with simple and famil-iar prosthetic techniques, allrestorative dentists can providecare for their patients who maybenefit from implant dentistry.The four main prerequisites forcost-effective implant dentistryare as follows: dplace the implants in theproper position;duse nonrotational abutments;dprovide for the patient’s fi-nancial and functional needs;duse conventional dental prosthetics. ■
Dr. Shepherd is in private practice withNorthern Essex Oral Surgery Associates Inc.,390 Water St., Haverhill, Mass. 01830.Address reprint requests to Dr. Shepherd.
Dr. Shepherd holds an equity interest inBicon Implant System.
1. Christensen G. Bicon Dental Implants.Clin Res Assoc Newsletter 1996;20(12):2.
2. Park N. Implants now simpler. NobelBiocare Update 1997;8(3):2.
JADA, Vol. 129, December 1998 1737
CLINICAL PRACTICE
competitive with that of a three-unit bridge. If a dental practicehas a prosthetic unit charge of$600, a three-unit bridge wouldcost $1,800. The single implantcan be placed for $900 to $1,100,and the crown would cost $600,the same as that for a crown ona natural tooth; therefore, theimplant and crown would cost$1,500 to $1,700. This allowsimplant dentistry to be afford-able to most dental patients.
Because of the flexibility ofangled abutments, full-archfixed bridges also can be createdwith abutments prepared for ce-mented prostheses. These an-gled abutments can be rotated afull 360 degrees, and it is there-fore relatively easy to mixstraight and angled abutmentsto achieve parallelism.
A very important require-ment of cost-effective implantdentistry is that the implant isplaced in the proper position. Todo this, an accurate, user-friendly stent or stents shouldbe used. I recommend that apalatal or lingual stent be usedto position the implant, and avacu-press clear stent be usedto ascertain the position of theabutment. In most stents thatare discussed in the literature,either there is an occlusal posi-tional hole or the buccal cuspshave been retained. This type ofstent looks very good on a labo-ratory bench, but once in themouth it often obstructs thesurgeon’s vision and preventshim or her from seeing the tipof the guide bur and the bone atthe same time. When a surgeonis uncomfortable with theamount of visibility, he or sheoften will not use the stent thathas been made. The stents Irecommend are made fromwaxed-up articulated studymodels, because they mechani-
cally direct the surgeon’s bur,and the implant will be in theprecise location that therestorative dentist requires.Such a stent is shown in
Figure 6, along with the out-come of the treatment.
SUMMARY
For the most part, implant den-tistry today is more expensiveand time-consuming than con-ventional crown-and-bridgeprosthetics. It is possible, how-
Figure 5. Schematic showing that the crown casting is subgingival onlyin the esthetic facial area. It may be at or above the gingival margin inthe mesial, distal or palatal/lingual areas.
The stents I recom-mended are madefrom waxed-up artic-ulated study models,because they me-chanically direct thesurgeon’s bur, andthe implant will be inthe precise locationthat the restorativedentist requires.
Copyright ©1998-2001 American Dental Association. All rights reserved.

1738 JADA, Vol. 129, December 1998
CLINICAL PRACTICE
3. Watson MT. Implant dentistry: a ten-year retrospective. Dental Products Report1996;30(12):26-31.
4. Dental implants: emerging technologytrends and oral and maxillofacial and perio-dontal surgery. Irvine, Calif.: Medical Data
International Inc.; 1993:1-27.5. Johansson F. Brånemark System: surgi-
cal operatory set-up procedures. Westmont,Ill.: Nobelpharma USA Inc.; 1994.
6. Scharf DR, Tarnow DP. Success rates ofosseointegration for implants placed under
sterile versus clean conditions. J Periodontol1993;64:954-6.
7. Zarb GA, Schmitt A. The longitudinalclinical effectiveness of osseointegrated dentalimplants: The Toronto Study. Part III: prob-lems and complications encountered. JProsthet Dent 1990;64:185-94.
8. Jemt T. Failures and complications in391 consecutively inserted fixed prosthesessupported by Brånemark implants in edentu-lous jaws: a study of treatment from the timeof prosthesis placement to the first annualcheckup. Int J Oral Maxillofac Implants1991;6:270-6.
9. Tolman DE, Laney WR. Tissue-integrat-ed prosthesis complications. Int J OralMaxillofac Implants 1992;7:477-84.
10. Naert I, Quirynen M, Theuniers G, vanSteenberghe D. Prosthetic aspects of osseoin-tegrated fixtures supporting over-dentures: a4-year report. J Prosthet Dent 1991;65:671-80.
11. Jemt T, Linden B, Lekholm U. Failuresand complications in 127 consecutively placedfixed partial prostheses supported byBrånemark implants: from prosthetic treat-ment to first annual checkup. Int J OralMaxillofac Implants 1992;7:40-4.
12. Naert I, Quirynen M, van SteenbergheD. A six-year prosthodontic study of 509 con-secutively inserted implants for the treatmentof partial edentulism. J Prosthet Dent1992;67:236-45.
13. Kallus T, Bessing C. Loose gold screwsfrequently occur in full-arch fixed prosthesessupported by osseointegrated implants after 5years. Int J Oral Maxillofac Implants1994;9:169-78.
14. Beaty K. The role of screws in implantsystems. Int J Oral Maxillofac Implants 1994;9(special supplement):52-4.
15. Balfour A, O’Brien GR. Comparativestudy of anti-rotational single tooth abut-ments. J Prosthet Dent 1995;73(1):36-43.
16. Muftu A, Mulcahy HL, Chapman R.Comparison of Streptococcus sanguis penetra-tion through various implant connectionmechanisms (abstract 585). J Dent Res1997;76(special issue):87.
17. Blake A. What every engineer shouldknow about threaded fasteners. New York:Marcel Dekker; 1986:32-5.
18. Dixon DL, Breeding LC, Sadler JP,McKay ML. Comparison of screw loosening,rotation, and deflection among three implantdesigns. J Prosthet Dent 1995;74:270-8.
19. Gros M, Laufer BZ, Oriniamar Z. An in-vestigation on heat transfer to the implant-bone interface due to abutment preparationwith high-speed cutting instruments. Int JOral Maxillofac Implants 1995;10:207-12.
20. Shepherd N. A general dentist’s guide toproper dental implant placement from an oralsurgeon’s perspective. Compend Contin EducDent 1996;17(2):118-30.
Figure 6. A. Panoramic radiograph of the mouth in the finished case. B.Clinical view of the mouth in the finished case.
A
B
Copyright ©1998-2001 American Dental Association. All rights reserved.