Embed Size (px)
Citation preview

Blood Reviews xxx (2016) xxx–xxx
YBLRE-00462; No of Pages 18
Contents lists available at ScienceDirect
Blood Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /b l re
REVIEW
After 10 years of JAK2V617F: Disease biology and current managementstrategies in polycythaemia vera
Jacob Grinfeld, Anna L Godfrey ⁎Department of Haematology, Cambridge University Hospitals NHS Foundation Trust, Hills Rd, Cambridge CB2 0QQ, UK
⁎ Corresponding author.E-mail addresses: [email protected] (J. Grinfeld), anna
(A.L. Godfrey).
http://dx.doi.org/10.1016/j.blre.2016.11.0010268-960X/© 2016 Published by Elsevier Ltd.
Please cite this article as: Grinfeld J, Godpolycythaemia vera, Blood Rev (2016), http:
a b s t r a c t
a r t i c l e i n f oAvailable online xxxx
The JAK2V617Fmutation accounts for the vastmajority of patients with polycythaemia vera (PV) and around halfof those with other Philadelphia-negative myeloproliferative neoplasms. Since its discovery in 2005, numerousinsights have been gained into the pathways bywhich JAK2V617F causesmyeloproliferation, including activationof JAK-STAT signalling but also through other canonical and non-canonical pathways. A variety of mechanismsexplain how this one mutation can be associated with distinct clinical disorders, demonstrating how constitu-tional and acquired factorsmay interact in the presence of a singlemutation to determine disease phenotype. Im-portant biological questions remainunanswered in PV, in particular how JAK2V617F affects stem cell function andwhat mechanisms drive myelofibrotic and leukaemic transformation. Whilst current management is largelycentred on prevention of cardiovascular events, future therapiesmust aim to target the JAK2-mutant clone, to re-verse the underlying marrow pathology and to address the risk of transformation events.© 2016 Published by Elsevier Ltd.
Keywords:Polycythaemia veraErythrocytosisMyeloproliferativeJAK2
1. Introduction
Polycythaemia vera (PV), one of the Philadelphia-negative myelo-proliferative neoplasms (MPNs), is a clonal haematopoietic stem celldisorder characterised by an increased red cell mass, associated withproliferation of erythroid, granulocytic and megakaryocytic elementsof the bonemarrow [1]. In 2005 the identification of the JAK2V617Fmu-tation elucidated a molecular basis for the disorder in over 95% of pa-tients [2–5], followed two years later by the identification of JAK2exon 12 mutations in most remaining patients [6,7]. The vast majorityof patients with PV therefore carry mutations in a single gene, and awealth of studies has since illuminated themanymolecular and cellularconsequences of these mutations.
Whilst JAK2 exon 12mutations are specific to PV, the JAK2V617Fmu-tation is also found in other myeloid disorders: 50 to 60% of those withessential thrombocythaemia (ET) or primary myelofibrosis (PMF) [2–5], about half of patients with the MDS/MPN entity “refractory anaemiawith ring sideroblasts and marked thrombocytosis” (RARS-T) [8], andlower frequencies in AML, other myeloproliferative andmyelodysplastic disorders [9,10]. ET and PMF in particular share impor-tant clinical features with PV, including the presence of neutrophiliaand/or thrombocytosis in some patients, hypercellularity of the bonemarrow, frequent splenomegaly, and risks of thrombosis and
frey AL, After 10years of JA//dx.doi.org/10.1016/j.blre.20
haemorrhage [1]. In aminority of patients, PV, ET and PMF can all trans-form into acute myeloid leukaemia (AML) [11–13], those with ET maydevelop transformation to PV [14], and both ET and PV may transforminto secondary myelofibrosis [11,13,14]. The identification ofJAK2V617F offered some basis for the clinical similarities betweenthese MPNs, but the molecular mechanisms behind the phenotypic dif-ferences between the JAK2V617F-positive disorders has remained thesubject of intensive investigation.
The identification of JAK2mutations in PV led to the introduction of arapid and non-invasive diagnostic test, with mutation testing nowwidely available and incorporated into national and international clini-cal guidelines [1,15–17]. Moreover the development of JAK2 inhibitorshas led to a much-needed novel therapeutic avenue for patients withmyelofibrosis [18,19], and most recently these drugs have also beenshown to benefit certain patients with PV [20]. However, clinical man-agement of PV remains predominantly centred on the reduction of vas-cular complications and symptoms. In spite of significant advances thathave beenmade in understanding the disease biology of PV, agents thatcan target the underlying neoplastic clone have remained elusive andthe risk of disease transformation, with its almost inevitably poor out-come, remains an important and unmet clinical need.
This reviewwill first examine current understanding of themolecu-lar basis of PV, both in terms of the pathological effects of JAK2 muta-tions and the factors that may contribute to phenotypic differencesbetween PV and other JAK2-mutated MPNs. Diagnostic criteria andtheir controversies will be considered. Key prognostic factors in PVwill then be examined, followed by a discussion of currentmanagementstrategies and unresolved clinical challenges.
K2V617F: Disease biology and current management strategies in16.11.001

2 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
2. The molecular and cellular effects of JAK2 mutations
JAK2 is one of a family of cytoplasmic tyrosine kinases that mediatessignal transduction from cell surface cytokine receptors, including theerythropoietin and thrombopoietin receptors [21]. Binding of ligand toreceptor leads to JAK autophosphorylation, receptortransphosphorylation and creation of binding sites for signalling mole-cules such as STAT proteins. STATs are phosphorylated, translocate tothe nucleus and affect target gene transcription. For example, bindingof erythropoietin to its receptor (EpoR) causes phosphorylation ofJAK2 and STAT5 [22], together with activation of other effectors includ-ing MAP kinase and phosphoinositide 3-kinase (PI3K)/Akt pathways[23].
2.1. Biochemical effects of JAK2 mutations
In early studies, the V617Fmutationwas found to have activating ef-fects on JAK2 signalling activity, cytokine sensitivity and cytokine-de-pendent survival in cell lines [2–5]. This activation of JAK2 is thoughtto reflect the location of the mutation within the JH2 “pseudokinase”domain of the protein, which normally has auto-inhibitory effects onthe catalytically active JH1 kinase domain [24–27]. Mechanismsmay in-clude the interference of the mutation with direct phosphorylation ofJH1 by JH2 [28], and cooperation of V617F with other residues in JH2to enhance JH1 kinase activity [29,30]. Interestingly, recent work onthe JAK1 JH2 crystal structure has also suggested that JAK2V617F activa-tion requires a specific conformational change in the SH2-JH2 linker do-main [31], which is the area targeted by exon 12 mutations. Exon 12mutations appear have similar activating effects to V617F in cell lines,including cytokine independence and constitutive activation of JAK2and its downstream mediators in the absence of erythropoietin [6].
Several signalling changes appear to mediate the cellular effects ofJAK2V617F. Increased phosphorylation of STAT5 has been demonstratedin numerous experimental systems, including cultured erythroid cellsand bone marrow trephine biopsies from patients with MPNs, and inJAK2V617F knock-in mouse models [2,4,5,32–41]. The particular impor-tance of STAT5 activation in PV is illustrated by the observation that ex-pression of constitutively active STAT5 in erythroid progenitors candrive formation of the same erythropoietin-independent endogenouserythroid colonies that are typical of PV [42]. Moreover it has beenshown more recently that Stat5 deletion in either a Jak2V617F knock-inmouse [43] or retroviral bonemarrow transplantationmodel [44] ab-rogates the marked erythrocytosis that is seen in the presence of Stat5.
Other signalling processes that appear to be activated by JAK2V617Finclude the PI3K/Akt and MAPK/ERK pathways, which have been stud-ied in many experimental systems [2,5,33,34,36,38,45]. There is evi-dence that the mutation has direct effects on apoptosis, both throughthe extrinsic pathway that acts through cell surface death receptorssuch as Fas [46], and through the intrinsic pathway, with increasedlevels of the anti-apoptotic protein Bcl-xL and impairment of its normalrole in the DNA damage response [47–49]. Other mediators implicatedin apoptotic dysregulation include ID1, Pim1/2 kinases, the BH3-onlyproteins Bad and Bim and the Bcl2-like protein Mcl-1, downstream ofSTAT3, STAT5 and ERK1/2 pathways [50–53]. Several studies have sug-gested that JAK2V617F may not only impair the normal cellular re-sponses to DNA damage but may also directly contribute to increasedDNA damage and to levels of intracellular reactive oxygen species [39,54–56].
Whilst activation of pathways such as STAT5 are considered canon-ical effects of JAK2V617F, several other “non-canonical” effects havebeen reported including modification of chromatin. JAK2 can enter thenucleus and phosphorylate histone H3 at Tyr41 (Y41), which preventsbinding of the heterochromatin protein HP1α [57]. This allows JAK2 tohave direct effects on the regulation of gene expression, a processwhich can occur in combination with, or independently of, STAT pro-teins [58]. JAK2V617F may also modulate chromatin by
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
phosphorylating the arginine methyltransferase PRMT5 and impairingits histone methylation activity, which may in turn promote growthand erythroid differentiation of haematopoietic cells [59].
There is evidence that JAK2V617Fmay not only act through intrinsiccellular pathways, but may have important effects through the micro-environment. For example, the mutation has been reported to increaselevels of the cytokine TNFα, which is increased in the serumofMPN pa-tients and may paradoxically stimulate growth of JAK2-mutant cells[60]. An important role for the microenvironment was also suggestedby two reports that macrophage depletion abrogates erythrocytosis inmouse models of JAK2V617F-driven polycythaemia [61,62].
2.2. Cellular effects of JAK2 mutations
Early studies of the cellular effects of JAK2V617F on haematopoiesisanalysed cell populations at different stages of differentiation from pri-mary patient samples, with or without a period of ex vivo culture. Thesestudies were mostly in keeping with an expansion advantage forJAK2V617F-mutant cells at later stages of myeloerythroid differentia-tion, particularly at low erythropoietin levels and in the presence of ho-mozygosity for the V617F mutation [63–67]. The effects of JAK2mutations on haematopoietic cells have been elucidated further usingmouse models. Importantly, early work demonstrated that expressionof JAK2V617F in retroviral bone marrow transplantation models couldcause a myeloproliferative phenotype [2,5], confirming the causal roleof the mutation in human MPNs. These models had high, dysregulatedlevels of JAK2V617F expression, whilst knock-in models allow observa-tion of the phenotypes obtained when the gene is expressed at physio-logical levels, under the normal regulatory elements of the mouse Jak2gene. These knock-in models have supported the conclusions from pa-tient studies, showing that JAK2V617F is associatedwith increased num-bers of lineage-restricted progenitors, including those of themegakaryocyte/erythroid and granulocyte/macrophage lineages [38–41,68].
The effects of JAK2V617F on haematopoietic stem cells (HSCs) havebeenmore controversial. Early studies used xenotransplantation exper-iments, inwhich CD34+ cells fromMPNpatientswere transplanted intoNOD/SCIDmice.Whilst these cells could engraft in themice, the propor-tion of JAK2V617F-positive cells was frequently reduced in thereconstituted marrow compared to the original cells, arguing againstan advantage for JAK2V617F-positive over wild-type HSCs [69,70]. Intwo knock-in models of murine Jak2V617F, an increase in the stemcell-enriched Lin−Sca-1+Kit+ (LSK) cell compartment was reported[38,68], whilst in another LSK numbers were unchanged [40]. With re-spect to HSC function, competitive transplantation experiments in oneof these models suggested a selective advantage for JAK2V617F-mutantcells in primary transplantation, associatedwith an increase in HSC pro-liferation and decrease in apoptosis, but this advantage was not main-tained in secondary transplants [68]. Similarly, competitivetransplantation experiments in a second model suggested normalearly function but a late advantage in primary recipients [40,71], whilstsubsequent data have suggested a lack of advantage in secondary recip-ients [72]. In the one knock-in model with a human JAK2V617F con-struct there was a quantitative and qualitative HSC defect, withreduced LSK cell numbers and evidence of increased DNA damage, re-duced cell cycling, and impaired function in competitive transplantationexperiments, which was most marked in cells homozygous forJAK2V617F [39,73]. Further studies of this latter model suggested thatthe mutation may promote differentiation of HSCs at the expense ofself-renewal [74].
Interestingly the concept of a JAK2V617F-induced HSC defect is con-sistent with other evidence from the human MPNs. For example, alleleburdens for JAK2V617F are low in many patients [64] and may remainstable over years [75], and it was reported that JAK2V617F-positivecells did not expand in the recipient of an allogeneic stem cell transplantfrom a JAK2V617F-positive donor [76]. Conversely it was reported that a
K2V617F: Disease biology and current management strategies in16.11.001

3J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
JAK2V617I mutation, found in a family with hereditary thrombocytosisin the absence of additional MPN-associated molecular abnormalities,was associated with increased numbers of phenotypic HSCs and an ad-vantage in xenotransplantation assays [77]. However this mutation alsoshowed qualitative signalling differences to V617F andmay be associat-edwith a different HSC phenotype, andmoreover the constitutional na-ture of the V617I variant would obviate the requirement for acompetitive advantage in human disease. The concept that oncogenesmay not impart a stem cell advantage is also consistent with datafrom other malignancies. For example, the BCR-ABL fusion gene hasbeen associated with reduced HSC self-renewal in vitro [78], in NOD/SCID transplantation experiments [79] and in secondary transplantsfroma transgenicmousemodel [80], and oncogene-induced senescenceis a recognised barrier to malignant progression in certain haematolog-ical and non-haematological neoplasms [81,82].
In summary, numerous studies have contributed to a body of knowl-edge regarding the biochemical and cellular consequences of JAK2 mu-tations. However, it has remained less clear how the various signallingperturbations contribute to the specific clinical features of MPNs, andwhich are the other factors that distinguish between the differentJAK2-mutant MPN phenotypes. For example, STAT5 activation appearsto play an important role in erythrocytosis, the defining feature of PV,since knockdown of Stat5 in JAK2V617F-driven models oferythrocytosis abrogates this aspect of the phenotype [43,44]. By con-trast Stat5 deletion did not prevent development of myelofibrosis in aJak2V617F retroviral bone marrow transplantation model [44]. More-over studies of haematopoietic cells from MPN patients found that pat-terns of pSTAT3, pSTAT5, pERK1/2 and pAkt correlated better withMPNsubtype rather than with the presence or burden of the JAK2V617Fmu-tation [83], highlighting a potential role for additional molecular mech-anisms in these signalling changes.
3. Factors determining phenotype in PV vs other JAK2-mutatedMPNs
In 2005, analysis of ET patients in the PT1 trial demonstrated that incomparison to JAK2V617F-negative patients, JAK2V617F-positive pa-tients showed higher haemoglobin levels, neutrophil counts, morebone marrow erythropoiesis and granulopoiesis, lower platelet counts,mean corpuscular volume (MCV), serum erythropoietin and ferritin,and more frequent PV transformation [84]. Subsequent studies con-firmed these associations [14,85–88], suggesting that JAK2V617F-posi-tive ET has some characteristics of a mild form of PV, as well as asimilar incidence of thrombosis [89]. These clinical similarities betweenPV and JAK2V617F-positive ET aremirrored by certain biological similar-ities (e.g. a low frequency of driver mutations additional to JAK2V617F[90]) and are in keeping with a model in which the two disordersform a phenotypic continuum [84]. However there are also importantdifferences between PV and JAK2V617F-positive ET, which haveprompted speculation and investigation of the factors that push anindividual's phenotype towards one or other disorder. These factors in-clude the presence and size of clones homozygous for the JAK2V617Fmutation; the presence of additional mutations and their subclonal hi-erarchy in relation to JAK2V617F; germline genetic factors; differencesin gene expression; and other constitutional factors including age andgender. We discuss these factors in more detail below.
3.1. The role of JAK2V617F homozygosity in PV phenotype
A “homozygous” JAK2V617F sequence (N50%mutant) in granulocyteDNA was originally identified in 25–30% of those with PV, 9–20% withPMF, and 0–3% with ET [2–5]. Clinical studies next investigated howJAK2V617F allele burden, a measure of “gene dosage” for the mutationthat ismost oftenmeasured in granulocyte DNA, correlatedwith certainclinical features. Initial studies divided PV patients into “heterozygous”(b50% mutant allele) and “homozygous” (N50% mutant allele) groups,
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
whilst subsequent studies analysed mutant allele burden as a continu-ous variable. Together these studies indicated that within PV, higherJAK2V617F allele burdens were associated with higher haemoglobinlevels, higher white cell counts and lower platelet counts, togetherwith other features suggesting a “more extreme” PV phenotype(lowerMCV, lower serum ferritin and erythropoietin, more splenomeg-aly, more pruritus and more need for cytoreductive therapy) [13,63,64,91–95]. These data suggested that a higher JAK2V617F allele burdenmight promote a more “PV-like”, rather than “ET-like”, phenotype.Within ET, higher JAK2V617F allele burdens were associated withsome of the same features as in PV (higher white cell counts and moresplenomegaly), but in contrast to PV there was an association withhigher platelet counts [63,64,88]. This may reflect a limitation of mea-suring allele burden in bulk granulocyte DNA: the assays did not dem-onstrate the contribution of JAK2V617F-heterozygous andhomozygous cells to the overall mutant allele burden.
Whilst these early patient studies showed a correlation betweenJAK2V617F allele burden and PV phenotype, mouse models have sincebeen used to establish the causal nature of this relationship. One trans-genicmousemodelwas consistentwith the concept that a phenotype ofET or PV could result from lower and higher levels of JAK2V617F expres-sion levels, respectively, suggesting a role for gene dosage in determin-ing MPN phenotype [96]. However the same switch from ET to PV wasnot seen with increasing gene dosage in other transgenic models [97,98], and all transgenicmodels are complicated by variable transgene ac-tivation between cells.
More recently the development of knock-in mouse models hasallowed study of JAK2V617F when expressed at physiological levelsunder its normal regulatory elements [38–41,68]. Four knock-inmodelswith a heterozygous murine mutant Jak2 allele developed a phenotypeconsistentwith PVwith erythrocytosis, leucocytosis, splenomegaly, var-iable thrombocytosis and increased megakaryocyte-erythroid progeni-tors [38,40,41,68]. One of these studies reported generation of ahomozygous-mutant mouse, which showed more pronouncedleucocytosis, thrombocytosis and splenomegaly but reduced or un-changed haemoglobin levels compared to heterozygousmice [38]; sim-ilar phenotypes were observed in a hemizygous mouse with deletion ofthe wild-type Jak2 allele [99]. By contrast in a fifth model with a humanJAK2V617F allele, mice heterozygous for themutation showed amoder-ate thrombocytosis with minimal erythrocytosis, normal spleen sizeand plasma erythropoietin levels, whilst homozygosity was associatedwith marked erythrocytosis and reduced platelet counts, significantsplenomegaly and suppressed plasma erythropoietin levels. These fea-tures closely parallel those of human ET and PV, respectively, and pro-vided direct genetic evidence that homozygosity for human JAK2V617Fcan be associatedwith a switch from ET-like disease to a PV-like pheno-type [73]. The reasons behind the phenotypic variation between the dif-ferent knock-in models remain unclear however, and may reflectdifferences in technical aspects of the targeting strategies or inherentdifferences in the mutant human and mouse proteins.
Further analysis of the precise role of JAK2V617F homozygosity inhuman PV has utilised genotyping of individual erythroid coloniesgrown fromMPN patient samples. This approach circumvents the limi-tations of allele burden studies in bulk granulocyte DNA, by investigat-ing the presence and frequency of homozygosity at the level of singleprecursors. An early study of BFU-E colonies grown in high erythropoi-etin conditions found that while virtually all PV and ET patients pro-duced both wild-type and mutant colonies, JAK2V617F-homozygouscolonies were detectable in almost all of the PV patients, but in noneof the cohort with ET [100]. Subsequent studies largely supportedthese observations [63,64], but raised the possibility that JAK2V617F-ho-mozygous erythroid colonies could be found in a small number of pa-tients with ET [63,64,101], whilst PV patients lacking JAK2V617F-homozygous colonies were also described [63,64]. A large study of PVand ET patients then analysed the genotypes of erythroid coloniesgrown in low erythropoietin conditions, aiming to select for even the
K2V617F: Disease biology and current management strategies in16.11.001

4 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
smallest homozygous-mutant clones. This study confirmed thatJAK2V617F-homozygous precursors could be identified from approxi-mately 80% of PV patients [102]. A higher proportion of JAK2V617F-ho-mozygous erythroid precursors, relative to heterozygous precursors,was associated with more pronounced PV-like clinical features, againsupporting a causal role for homozygosity in this phenotype [103].However small homozygous-mutant clones could also be identified re-producibly in approximately half of ET patients [102]. Moreover manypatientswith PV andETwere shown to have acquired JAK2V617Fhomo-zygosity on multiple occasions in independent subclones, but PV wasdistinguished by the expansion of one dominant homozygous-mutantsubclone.
Together these data have demonstrated that in the 80% of PV pa-tients with significant JAK2V617F-homozygous clones, these may havea causal role in the PV phenotype. However mitotic recombination oc-curs at the JAK2 locus remarkably frequently; this observation remainsunexplained, although JAK2V617F itself has also been associated withincreased homologous recombination and DNA replication stress [54,56]. Moreover acquisition of homozygosity is not sufficient to drive aphenotype of PV, but the important step appears to bewhether a homo-zygous-mutant clone expands sufficiently to impact on the disease phe-notype. Further work has aimed to investigate what factors may drivethe expansion of individual subclones, together with the additional fac-tors that may influence phenotype in the presence of a particular bal-ance of JAK2V617F-homozygous and -heterozygous subclones.
3.2. Other mutations and PV phenotype
Since the identification of JAK2V617F, a range of other mutationshave been identified in MPNs. Mutations in CALR, MPL and LNK arefound predominantly in JAK2-unmutated MPNs and seem likely to behave parallel effects on cellular signalling that drive the specific MPNphenotype. By contrast many of the other mutations (Table 1) arefound in other myeloid malignancies as well as MPNs and seem likelyto contribute to disease through less specific effects on HSC survival orself-renewal [104]. Amongst the MPNs these mutations tend to becommonest in myelofibrosis and/or blast-phase disease with low fre-quencies in PV, but nonetheless they are candidates for driving expan-sion of JAK2-mutant subclones in PV and ET. For example, TET2 andDNMT3A mutations have been identified patients with PV who lackJAK2V617F-homozygous precursors [105,106]. These patients tend tohave particularly large heterozygous-mutant subclones, perhaps ac-counting for the development of sufficient erythrocytosis to meet a di-agnosis of PV rather than ET [63,102]. It is likely that these additionalmutations may contribute to the phenomenon of “clonal dominance”,a description used for patients with a similar JAK2V617F allele burdenin CD34+ progenitor cells compared to neutrophils [64]. This featureis particularly seen in myelofibrosis but is also commoner in patientswith PV compared to those with ET, the latter tending to show lower
Table 1Genes other than JAK2, MPL and CALR that show recurrentmutations in humanMPNs, andtheir frequencies in PV and other disorders.
Gene PV (%) ET (%) MF (%) Blast phase (%)
LNK [240–242] 25* 0–7 0–6 10TET2 [105,243,244] 10–16 b5 7–17 17–32DNMT3A [245–247] 3–7 b5 2–15 14–17ASXL1 [247–250] 2–7 b5 13–32 18–33SRSF2 [251–254] b5 b5 6–17 19–33EZH2 [249,255,256] b5 b5 7–13 b5CBL [147,247,257–259] b5 b5 0–8 6–9IDH1/2 [260,261] b5 b5 b5 9–22SF3B1 [247,252,262] b5 b5 b5 b5
Note that the list is not exhaustive and exome sequencing studies have shown additionalgenes to be mutated in small proportions of patients [90]. *JAK2-negative idiopathicerythrocytosis.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
JAK2V617F allele burdens in CD34+ progenitor cells compared to moremature granulocytes [107].
A recent finding is that it is not only the combination of mutationsthat is important in determining subclonal balance and phenotype,but also the order of their acquisition. In a series of patients carryingboth JAK2 and TET2 mutations, acquisition of mutant JAK2 prior toTET2 was more likely to be associated with a phenotype of PV than ET,and as expected this correlated with a higher proportion ofJAK2V617F-homozygous colonies [108]. The double-mutant clone waslarger in these patients at the level of haematopoietic stem and progen-itor cells (HSPCs), in contrast to the “TET2-first” group in which TET2-single-mutant HSPCs predominated, and “JAK2-first” patients also hada higher risk of thrombosis. Certain other mutations may not only pro-mote the expansion of JAK2-mutant clones but may also contribute di-rectly to PV phenotype. An example is that of truncating NF-E2mutations that were identified in a small number of patients withJAK2V617F-positive PV, as well as some with myelofibrosis [109].These mutations are associated with a proliferative advantage inhaematopoietic colony assays and cell lines. Moreover a murine bonemarrow transplantation model showed erythrocytosis, thrombocytosisand neutrophilia in the presence of an NF-E2mutation, but the combi-nation with JAK2V617F led to an even more pronounced erythrocytosisthan JAK2V617F alone, suggesting a cooperative effect on phenotype.
The factors contributing to clonal balance are frequently unclearhowever. There is evidence to suggest that in some patients, additionalmutations may not account for differential subclonal expansion. In twoPV patients with multiple JAK2V617F-homozygous subclones, an addi-tional “driver” mutation was identified by exome sequencing in thedominant homozygous-mutant subclone [110]. However these muta-tionswere not specific to the dominant subclone andwere each presentin at least one minor homozygous-mutant subclone. These findingsraise the possibility that in some patients, stochastic mechanisms mayaccount for the relative sizes of JAK2-mutant clones and therefore fordifferences in phenotype.
3.3. Germline factors in the phenotype of JAK2-mutated MPNs
Germline JAK2mutations affecting V617 (V617I) [77] and other res-idues outside the pseudokinase domain [111,112] have recently beenreported to cause hereditary thrombocytosis, and all have been sug-gested to have weaker consequences for JAK2 function than V617F[77,111,112]. Equivalent mutations have not been identified in patientswith acquired ET or PV, however.
Germline factors are important in genetic predisposition to acquiredMPNs: a specific constitutional JAK2 haplotype, designated 46/1, isstrongly associated with the development of JAK2V617F-positiveMPNs [113,114], aswell as with JAK2 exon 12-mutated andMPL-mutat-ed disease [115–117]. These findings suggested that either the specifichaplotype is associatedwith an increased risk of developing a pathogen-ic JAK2 mutation, or that the acquisition of a mutation is more likely tolead to clinical disease in the presence of the 46/1 haplotype [118]. Asmall study of PV patients suggested that homozygosity for the 46/1haplotype was associated with a greater likelihood of increasing alleleburden over time [119], raising the possibility that this genotype maypromote the development or expansion of JAK2V617F-homozygousclones. A study in the Chinese population also suggested that the 46/1haplotype is associated with a higher haemoglobin and white cellcount at diagnosis in ET and PMF, and with higher platelet counts inPMF [120], although other studies have not found associations withclinical features [118].
More recently, extensive genome-wide association studies haveidentified a number of other novel single-nucleotide polymorphisms(SNPs) associated with MPNs. A germline variant in the TERT genewas associated with MPNs but not with disease phenotype or with thepresence of the JAK2V617Fmutation [121,122], and recently additionalvariants related to the TET2 and SH2B3 gene loci have been described
K2V617F: Disease biology and current management strategies in16.11.001

5J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
[123]. A particularly interesting observation was that a SNP located be-tween theHBS1L andMYB genes showed an association with CALR- andMPL-mutant MPNs, but within JAK2-mutated patients showed a signifi-cantly different allele frequency between ET and PV [122]. The risk allelewas found to specifically increase the risk of ET but not PV and was as-sociatedwith significantly lowerMYB expression in haematopoietic col-onies; moreover MYB-knockdown mice show a transplantable ET-likedisease [124]. These findings, together with other studies [125–127],suggest a potentially important role of germline factors in determiningdisease phenotype within JAK2-mutant MPNs.
3.4. Differential gene expression in JAK2-mutant PV and ET
A number of studies have investigated differences in gene expres-sion between the different MPNs. One novel approach was to use clon-ally-derived erythroid cells from patients with PV and ET, in each casecomparing JAK2V617F-heterozygousmutant cells to awild-type samplefrom the same patient and thus controlling for inter-individual variationin gene expression [128]. In ET but not in PV, JAK2-mutant cells showedupregulation of interferon target genes compared to wild-type cells, as-sociated with increased activation of pSTAT1, which was absent in PVpatients. Functional experiments suggested that differential activationof STAT1 could contribute to altered megakaryocytic and erythroid dif-ferentiation. These findings are also consistent with data from aJAK2V617F transgenic mouse model, in which loss of Stat1 resulted inmore marked erythrocytosis and reduction of thrombocytosis com-pared to normal Stat1 levels [129]. Interestingly this study found thatserum interferon-gamma levels were increased in the mice withthrombocytosis and also in patients with ET, with lower levels inthose with PV. These findings raise the possibility that varying levelsof interferon-gamma might account for differences in signalling seenbetween PV and ET patients. However the molecular explanation forthese data in patients remains elusive and it is unclear if this phenome-non may relate to acquired or constitutional differences in interferonbiology.
Within PV, a microarray-based study of CD34+ peripheral bloodcells suggested that gene expression could be used to differentiate be-tween two groups of PV patientswhoalso showed differences in diseaseduration, haemoglobin level, thromboembolic events, splenomegaly,exposure to chemotherapy, leukaemic transformation and survival[130]. These findings were independent of JAK2V617F allele burdenand raise the possibility that differences in gene expression between pa-tients with PV may contribute to phenotypic heterogeneity, althoughthe genetic or epigenetic mechanisms are uncertain. Deregulation ofmicroRNA expression has also been implicated in the biology of PV[131] and a small study suggested that perturbations in microRNA ex-pression may also differ between PV and ET patients [132].
In summary, a number of factors are likely to play a role in determin-ing a precise phenotype PV or ET in the presence of a JAK2 mutation.There are likely to be many other germline genetic influences. For ex-ample, we have studied two patients with beta-thalassaemia trait inwhom colony assays have revealed large JAK2V617F-homozygousclones, typical of PV (unpublished data). However in both cases a phe-notype of ET is evident clinically, a phenomenon that seems likely to re-flect a constraining effect of the beta-globin abnormalities on thedevelopment of erythrocytosis. Age may influence the phenotype ob-tained and gender may be particularly important, possibly throughmodulating the phenotypic effects of large JAK2V617F-homozygousclones [103,133]. It has also been reported that gender may be associat-ed with additional phenotypic features in PV including age of presenta-tion, presence of splenomegaly and thrombotic events [133,134].Genome-wide association studies in normal individuals have identifieda number of genetic loci associated with full blood count parameters[135–138], confirming for example that variants in genes related toiron metabolism may influence haemoglobin levels [139,140]. Giventhat haemoglobin and platelet levels are polygenic traits in the normal
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
population, they are likely to be similarly influenced by genetic determi-nants in patients withMPNs. The timing of presentation tomedical careand institution of therapy may also be important, since many PV pa-tients show a thrombocytosis during the evolution of their disease andcould gain a diagnostic label of ET if they receive cytoreduction beforethe full PV phenotype is allowed to develop [141]. Together all ofthese data support a model in which JAK2-mutant PV and ET form a bi-ological continuum, with the precise phenotype determined by a rangeof discrete and continuous variables (Fig. 1).
3.5. JAK2 exon 12 mutations in PV
Over 20 differentmutations in exon 12 of JAK2 have been reported inPV but have not been described in ET. Exon 12mutations tend to be as-sociated with a particular clinical phenotype: compared to PV patientswith JAK2V617F, patients are younger, with higher haemoglobin con-centrations, lowerwhite cell and platelet counts, and isolated bonemar-row erythroid hyperplasia without granulocytic or megakaryocyticmorphological abnormalities [6,142]. In a series of 106 patients withexon 12 mutations, 64% presented with isolated erythrocytosis, with15% having additional leucocytosis, 12% additional thrombocytosis and9% both, with a similar incidence of thrombosis, myelofibrosis, acuteleukaemia and death to those with JAK2V617F [142]. By contrast toJAK2V617F-positive PV, patients tend to carry predominantly heterozy-gous-mutant clones, with small homozygous-mutant clones detectablein 40–50% of patients (similar to ET) [102].
The mechanism for the marked, and relatively isolated,erythrocytosis seen in patients with JAK2 exon 12 mutations is not en-tirely clear. Some in vitro studies [6], but not others [143], have sug-gested that these mutations might be associated with more markedactivation of JAK2 than V617F. Expression profiling has demonstratedthat STAT1 activation is preserved in the presence of exon 12mutationsand that attenuated STAT1 signalling is therefore not the explanation forerythrocytosis in these patients [144].
3.6. Factors contributing to disease transformation from PV: myelofibrosisand acute myeloid leukaemia
Whilst JAK2V617F is also found in 50 to 60% of thosewith PMF, it ap-pears likely that additional factors contribute to thismore complex, het-erogeneous phenotype. Transformations of ET and PV to secondarymyelofibrosis are well recognised and patients diagnosed with “prima-ry” myelofibrosis may show evidence of a prior undiagnosed chronic-phaseMPN [145], supporting the concept ofmyelofibrosis as an acceler-ated phase of disease. It is clear that additional genetic lesions are im-portant. Exome sequencing studies have demonstrated a higheraverage number of somatic mutations in patients with myelofibrosiscompared to those with PV or ET [90], and consistent with this, mostof the other recurrent mutations identified in chronic-phase MPNs arealso commonest in PMF (Table 1). Moreover the spectrum of genetic le-sions in PMF shows increasing overlap both with secondary AML andwith poor prognostic subgroups of other myeloid malignancies. Manyof the genes affected are predicted to alter DNA and/or histone modifi-cations through a variety of mechanisms, or to affect the RNA splicingmachinery.
The role of JAK2V617F in progression of chronic-phase PV to AML isparticularly complex. In individuals in whom JAK2V617F is detectablein the leukaemic blasts, the mutation may have contributed to diseaseevolution by causing increased DNA damage [54] and an impaired apo-ptotic response to DNA damage [49]. Other patients with JAK2V617F-positive chronic MPNs may however develop JAK2V617F-negativeAML [146,147]. A variety of molecular lesions have been implicated tohave a specific role in leukaemic transformation, including mutationsin TP53, RUNX1, c-CBL, IKZF1, NRAS and KRAS [104,147,148].
K2V617F: Disease biology and current management strategies in16.11.001

ET PV
High JAK2V617F allele burden
JAK2V617F homozygosity
Gender STAT1 signaling
HBS1L/MYB Other germline
genes
Phenotypic mutations
e.g. NF-E2
Timing of
presentation
Mutation order &
subclonal selection
Fig. 1. Factors that may determine a phenotype of PV or ET in the presence of a JAK2V617Fmutation. Numerous factors may modulate the relative sizes of JAK2V617F-heterozygous andJAK2V617F-homozygous subclones, as well as the phenotypic effects of these clones.
6 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
4. Diagnostic criteria for PV
Clinical assessment of a patient with suspected PV should aim toidentify possible alternative causes of erythrocytosis. Examples includesecondary erythrocytosis associated with respiratory disease, renal dis-ease or obstructive sleep apnoea, relative erythrocytosis that reflects acontracted plasma volume, or congenital causes of erythrocytosis. In-vestigations are described in guidelines such as those published by theBritish Committee for Standards in Haematology (BCSH) [15,149], butan essential laboratory investigation is screening for JAK2V617F (and,if necessary, exon 12mutations), for which guidelines are also available[150].
Where an MPN is suspected, criteria have been published by theWorld Health Organisation (WHO) or BCSH to define those patientswho should be diagnosed with PV (Table 2) [1,15,151]. An essentialcomponent in both cases is the presence of an erythrocytosis, but theparameters and thresholds used to define this key criterion remain con-troversial [152]. TheWHO criteria have been recently updated and nowsuggest the use of absolute haemoglobin level, haematocrit, or red cellmass [151], whilst the BCSH criteria depend on either haematocrit orred cell mass [15]. Although scintigraphic measurement of red cellmass may be considered the gold standard investigation, it is not
Table 2Diagnostic criteria for polycythaemia vera.
World Health Organisation, 2016 revision[151]
Diagnosis of PV requires: All 3 major criteria,or major (1) + (2), and + minor criterion
British Committee for Standards inHaematology, 2007 [15]
Diagnosis of PV requires A1 + A2Additional criteria used forJAK2-negative PV
Major (1): Hb N 165 g/l (M) or 160 g/l (F) orHct N 0.49 (M) or N0.48 (F) orRCM N 25% above mean normal predicted
A1: Hct N 0.52 (M) or N0.48 (F) orRaised RCM (N 25% abovepredicted)
Major (2): BM biopsy showinghypercellularity for age with trilineagegrowth (panmyelosis), includingpleomorphic, mature megakaryocytes
A2: Mutation in JAK2
Major (3): Presence of JAK2V617F or JAK2exon 12 mutation
Minor: Subnormal serum erythropoietin level
M = male, F = female, and RCM= red cell mass.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
universally available and is not absolutely required in either set ofcriteria. However, haemoglobin or haematocrit levels do not provide aperfect surrogate for red cell mass and their use in diagnostic thresholdsfor PV have been questioned [153,154]. This issue relates to unpredict-able changes in plasma volume in PV, especially in the presence ofsplenomegaly [155–157], and it has been suggested that more system-atic measurement of red cell masswould be helpful [158]. Iron deficien-cy may further confound the clinical presentation. The term “maskedPV” has been used for those patients whose bone marrow morphologyis in keepingwith a diagnosis of PV but who do not meet haemoglobin-or haematocrit-based thresholds for erythrocytosis [159]. These pa-tients may represent an important group since they were reported tohave higher rates of myelofibrotic transformation, acute leukaemiaand thrombosis with inferior survival, compared to those with overtPV [159–161], although this was not confirmed in all studies [162]. In-terestingly it was found that the use of BCSH criteria resulted in a small-er proportion of patients falling into this category compared to the 2008WHO criteria (which depended on absolute haemoglobin level or a doc-umented rise in haemoglobin, but not haematocrit) [160]. These datasupport the use of haematocrit rather than haemoglobin as an indicatorof erythrocytosis.
In clinical practice, the issue of defining erythrocytosis is most rele-vant in distinguishing PV from ET in the presence of a JAK2 mutation.Both WHO and BCSH criteria for ET require the exclusion of PV andtherefore, to at least some extent, depend on the same thresholdsused to define erythrocytosis. A study of patients with PV (overt ormasked) and ET suggested that the most optimal cut-offs to distinguishbetween JAK2-mutated ET and PV are a haemoglobin level of 165 g/l inmales and 160 g/l in females, or haematocrit of 49% in males and 48% infemales [163], which is reflected in the 2016 WHO criteria (Table 2)[151]. However these criteria have not been validated prospectively[164].
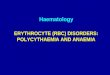
The BCSH and WHO criteria also differ in the importance given tobone marrow morphology. Although the classical histological featuresof PV are identifiable inmost patients (Fig. 2), the use of histology to de-termine diagnosis within the MPNs, as recommended by the WHO, re-mains controversial. Indeed BCSH criteria allow a diagnosis of PV to bemade in the presence of erythrocytosis and a JAK2 mutation without abonemarrowbiopsy. In one study of 272 bonemarrowbiopsies, blindedhistological evaluation by seven haematopathologists resulted in a diag-nostic consensus in only 53% of patients, and even where a histological
K2V617F: Disease biology and current management strategies in16.11.001

Fig. 2. Bonemarrow histology in PV. Low power (left) and high power (right) images of a bonemarrow trephine (H&E stain), showing typical histological features of PV includingmarkedhypercellularity, trilineage hyperplasia (“panmyelosis”) and megakaryocyte pleomorphism and clustering.
7J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
consensus was obtained, the concordance rate with the clinician's diag-nosis was only 71% [165]. There are therefore ongoing uncertaintiesabout the reliability of histology in discriminating between PV andJAK2-mutated ET in routine clinical practice. WHO criteria also retainserum erythropoietin level as a minor criterion for the diagnosis of PV,although this has been shown to add little to the accuracy of PV diagno-sis in the era of JAK2 mutation testing [166].
Although PV and JAK2-mutated ET are discriminated predominantlyon the basis of pragmatic thresholds for red cell mass, haemoglobin orhaematocrit levels, it is clear that these thresholds are somewhat arbi-trary and some patients with JAK2V617F-positive ET will be more “sim-ilar” to PV than others. Moreover this dichotomous classification doesnot fully capture the phenotypic heterogeneity within and overlap be-tween the two groups of patients. As discussed above, JAK2V617F-posi-tive PV and ET can be considered as two ends of a biological continuum[84] inwhich specific phenotypic features (blood count parameters, andperhaps others such as spleen size and thrombotic risk) may be influ-enced by the balance between clones of different JAK2 genotype togeth-er with genetic and environmental modifiers (Fig. 1). This concept of adisease spectrum rather than a dichotomy raises questions as to wheth-er it is appropriate to divide treatment studies and guidelines accordingto current diagnostic criteria, in which JAK2V617F-positive and-negative ET are considered together, and quite separate to PV [16,149]. Interestingly one report suggested that higher rates of thrombosisin masked PV might reflect a lower intensity of treatment as comparedto overt PV [161]. This raises the possibility that amore unified diagnos-tic (andmanagement) approach to those with JAK2-mutated MPNs (PVor ET)might improve outcomes, but this has not yet been tested in clin-ical trials.
5. Prognosis in PV
5.1. Factors predictive of overall survival and vascular events
Patients with PV have a reduced life expectancy in comparison to anage-matched healthy population and compared to patients with ET. Astudy of 396 consecutive PV patients demonstrated a 15-year survivalof 65%, compared to 73% in ET [167], while a multi-centre study of1545 PV patients showed a median survival of 14.1–18.9 years [168].Age and thrombotic history have been identified as independent poorprognostic factors for overall survival in several studies [168,169] andleucocytosis, abnormal karyotype and a leucoerythroblastic bloodsmear have also been shown to confer an adverse prognosis [168].
Venous and arterial thromboses are the leading causes of mortalityin patients with PV and are the presenting feature in 20% [170]. After di-agnosis, the rate of thrombotic events has been estimated as 3.4–5.5 per100 patients per year, with age at diagnosis and history of prior throm-botic episodes being most strongly predictive of further events [169,170]. The European Collaboration on Low-Dose Aspirin in Polycythemia
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
Vera (ECLAP) study also found that a smokinghistory carried a small butsignificant risk for thrombosis (hazard ratio 1.9), but there is little con-vincing evidence that other factors traditionally associated with cardio-vascular risk, such as hypertension, hyperlipidaemia or diabetesmellitus, play a significant role in the context of PV [171].
A correlation between haematocrit and risk of thrombosis was firstdescribed in a retrospective report in 1978 [172], leading to the recom-mendation that the haematocrit should be maintained below 0.45. Aswell as being associated with increased blood viscosity, a raisedhaematocrit may also contribute to increased platelet activation dueto displacement towards the vessel wall, and may be associated withred cell aggregates [173]. Polycythemia Study Group (PVSG)-01 and05, a large randomised controlled study initiated in 1967, allowed fur-ther indirect assessment of the impact of haematocrit on thromboticrisk, since a fall in thrombotic events in the venesection-only arm wasobserved once the target haematocrit was reduced from 0.52 to 0.45[174,175]. However the use of the haematocrit as a therapeutic targetwas only validated formally in the recent CytoPV study [176]. This pro-spective study randomised 365 patients with PV to intensive (targethaematocrit b0.45) or less intensive (target haematocrit 0.45–0.50)treatment, with the choice of therapy (venesection, cytoreduction orboth) at the investigator's discretion. With a median follow-up of31 months, 9.8% of patients in the low-intensity arm met the primaryendpoint of death from cardiovascular ormajor thrombotic events com-pared to 2.7% in the intensive treatment arm. Although this lends moredefinitive support to a haematocrit target of b0.45, it remains unclearwhether an even lower threshold might offer a further reduction inthrombotic events. A number of centres advocate different targets formales and females – i.e. b0.45 and b0.42, respectively - based on differ-ences in steady-state physiological levels [155,177]. This is reasonablebut currently there is no prospective or retrospective evidence to sup-port the use of different targets.
Interpretation of the CytoPV study is confounded by the fact that pa-tients in the lower-intensity arm tended to have higher white cellcounts than those in the intensive arm,most likely reflecting differencesin the use of cytoreductive drugs. This is important because leucocytosismay itself be a risk factor for thrombosis. In ET, a leucocyte countN15 × 109/l was identified as an independent predictor both of overallsurvival and thrombosis in a study of 322 patients [178], and the pro-spective PT1 study also found a linear relationship between leucocytecount on follow-up and the estimated hazard ratio for thrombosis[179]. Proposed mechanisms for this association include the activationof platelets by granule-derived proteases, and direct interactions viaCD11b-CD42b or -CD63b [173,180]. Data are more limited in the con-text of PV however. Analysis of the prospective ECLAP cohort did dem-onstrate an increased thrombotic risk in patients with a leucocytosis(HR 1.71), mainly reflecting an increased risk of myocardial infarction[171], although no association was seen in a retrospective analysisthat included 153 PV patients [181].
K2V617F: Disease biology and current management strategies in16.11.001

8 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
There have been mixed reports regarding the significance ofJAK2V617F homozygosity in determining thrombotic risk both in PVand ET. Tefferi et al. [95] compared rates of thrombosis between 13JAK2V617F-“homozygous” and 45 JAK2V617F-“heterozygous” patientsand found no difference, with a later larger study reaching a similar con-clusion [13]. However these were both retrospective studies that distin-guished between homozygous and heterozygous patients using semi-quantitative techniques. Subsequently JAK2V617F allele burden wasassessed using quantitative real-time PCR in diagnostic samples from acohort of 173 PV patients, with a median follow-up of 24 months [91].The 18% of patients with mutant allele burdens of N75% had greaterrates of cardiovascular events at the time of, and following, diagnosis,as well as greater numbers of thrombotic events post-diagnosis. Alleleburden remained the only independent variable predictive of cardiovas-cular events in amultivariate analysis that included age, prior thrombo-sis and leucocytosis.
In summary, age and thrombotic history remain established risk fac-tors for thrombosis in PV, whilst leucocytosis and JAK2V617F allele bur-den may have significance and warrant further investigation inprospective studies. Interestingly there has been no evidence, either inET or PV, that the degree of thrombocytosis correlates with thromboticrisk. In fact, in ET a U-shaped relationship has been demonstrated be-tween platelet count and the risk of haemorrhage [179], which is likelyto be explained by the development of an acquired vonWillebrand syn-drome at high platelet counts (generally N1000 × 109/l) [182]. In PV,analysis of the ECLAP cohort demonstrated a prior bleeding history asthe only independent predictor for haemorrhage [169], while datafrom the German Study Alliance Leukaemia MPN registry, which in-cludes 142 patients with PV, identified prior thrombosis, splenomegalyand heparin use as risk factors for bleeding in univariate analyses [183].
5.2. Factors predictive of transformation to myelofibrosis or acuteleukaemia
Factors that have been associatedwith increased risk ofmyelofibrot-ic transformation in PV include the presence of increased bone marrowfibrosis at diagnosis [184] and a diagnostic white cell count N15 × 109/l[185]. JAK2V617F allele burdenwas associatedwith risk of disease trans-formation in a prospective study of 338 patients with PV [93]; 2% of pa-tients transformed to secondary myelofibrosis, all of whom had alleleburdens N50%, and this association remained significant onmultivariateanalysis. Although the latter study did not identify an association be-tween allele burden and progression to AML, the frequency of this end-point was low (3%). The incidence of leukaemic transformation varieswidely between studies, and has been reported as high as up to N30%in trials with follow-up of N20 years [186]. Studies with higher ratesof transformation to AML have implicated leucocytosis, age and abnor-mal karyotype as additional risk factors [168,187]. There is also a strongassociation with the use of certain cytoreductive agents (see Section6.4).
Although a number of somatic mutations have been associated withprogression to myelofibrosis or acute leukaemia (see Section 3.6), it isless clear whether themutational profile at diagnosis can predict trans-formation events or other outcomemeasures. A number of studies haveaddressed this question in primary myelofibrosis, but only one study todate has comprehensively investigated other MPN subtypes. Lundberget al. [188] screened for mutations in 104 genes in a 197 patient cohortthat included 94 patients with PV. Of these, only mutations of TP53 andTET2were associated with increased rates of leukaemic transformation.
6. Management of PV
The aims of treatment in PV are to reduce disease-related symptomsand the risk of venous and arterial thrombosis, while minimising treat-ment-related toxicity, haemorrhagic risk and, in particular, the risk ofprogression to post-PV myelofibrosis and acute leukaemia. As such
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
management largely adopts a risk-adapted approach, targetingcytoreductive treatment towards those at higher thrombotic orhaemorrhagic risk. Although, with the exception of smoking, there isno association between established cardiovascular risk factors andthrombotic risk in the context of PV, it is generally accepted that theseshould be targeted regardless of other specific management steps.
6.1. Use of anti-platelet agents
Since platelet activation seems to be a central mechanism in MPN-associated thrombosis [173,189] and there is evidence of increasedplatelet thromboxane biosynthesis in PV [190], there has been interestin the use of anti-platelet agents, in particular aspirin, forthromboprophylaxis in MPNs. High-dose aspirin (900 mg) ordipyridamole (225 mg) was used in the venesection arm of the PVSG-05 trial (which was a comparator for pipobroman), but this wasdiscontinued early due to excessive gastrointestinal bleeds and deathsfrom haemorrhage [175]. This initially led to the avoidance of aspirinin patients with MPNs, but subsequently the use of low-dose aspirinwas assessed in the ECLAP trial [191]. This multicentre, double-blindtrial randomised 518 high- or low-risk PV patients without a specific in-dication for aspirin to receive daily aspirin 100 mg or placebo, with amean follow-up period of three years. The composite primary end-point of non-fatal myocardial infarction, non-fatal stroke, pulmonaryembolism, major venous thrombosis, or death from cardiovascularcauses wasmet in 7.9% of the placebo-treated group and 3.2% of the as-pirin treated group (p = 0.03), with overall incidences of thromboticevents of 15.5% and 6.7% respectively (p=0.003). No significant differ-enceswere seen in the incidence ofmajor, orminor bleeding. It is worthnoting that this studywas terminated early due to poor recruitment andonly one third of the target number of patients were actually recruited;as such it may have been under-powered to detect significant differ-ences in bleeding complications [192]. Nonetheless this studyestablished a role for low-dose aspirin in primary prevention of throm-botic events in PV and did not demonstrate a significant increase inhaemorrhagic events, leading to the widespread use of aspirin acrossall risk groups in PV, as well as in ET [16]. This approach is further sup-ported by a recent retrospective study in low-risk ET that showed a re-duction in venous events in JAK2-mutated patients who receivedantiplatelets, compared to observation alone (although an increase inbleeding, without a reduction in thrombosis, was seen in CALR-mutatedET patients and it is now unclear that universal aspirin use remains ap-propriate in this latter group) [193]. A Cochranemeta-analysis [194] in-cluded both the ECLAP study and an earlier study by Gruppo ItalianoStudio Policitemia that assessed the safety of low-dose aspirin(40 mg), and included thrombotic/embolic events as secondary end-points [195]. The reduction in thrombosis-related mortality did notreach significance in this analysis, but there was no significant increasein haemorrhagic complications. This review also concluded that aspirinis safe to use in PV. However, these and other authors have highlightedthe need for further research into which subgroups might benefit mostor might be at greater risk of bleeding complications, as well as into al-ternatives, for example thienopyridine anti-platelet agents such asclopidogrel, which might be used in patients intolerant of or resistantto aspirin [192].
6.2. Venesection
As discussed above, a number of studies have indicated that throm-botic risk is significantly reduced when the haematocrit is maintainedbelow 0.45 and that venesection of 250–500 ml per session can be suf-ficient to achieve this target. This is achieved both by immediate reduc-tion in haematocrit by the removal of red cells with compensatoryexpansion of the plasma volume, but also by the longer term inductionof an iron-deficient state that constrains erythropoiesis. Furthermore,venesection alone compared favourably compared to radiophosphorus
K2V617F: Disease biology and current management strategies in16.11.001

9J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
(32P) and chlorambucil in the PVSG trials, which randomised 431 pa-tients to these three treatments with median survivals of 13.9, 11.8and 8.9 years respectively. However, higher rates of early thromboticevents were observed in the venesection-only arm, particularly in pa-tients over 70 [196]. This has led to the recommendation that venesec-tion (rather than cytoreduction) may be adequate to controlhaematocrit in low-risk patients but raised the question of whethercytoreductive agents have a particularly important role in the high-risk group. Conversely the fact that a haematocrit target of 0.52 was ini-tially used in this trial, and subsequently reduced to 0.45, doesmakes itsinterpretation problematic. Venesection is generally well tolerated andavoids potential toxicities associated with cytoreductive drugs but ne-cessitates regular outpatient visits (in some cases it may need to be per-formed daily until the haematocrit is range). Other potential problemsinclude difficult venous access, anxiety regarding the use of needles,and symptoms resulting from iron deficiency (such as fatigue, cognitiveimpairment or restless legs) or cardiovascular instability/vasovagalevents (where isovolaemic venesection may be more appropriate).
6.3. Historical perspective: cytoreduction using radiophosphorus oralkylating agents
32P has been used for cytoreduction since the 1940s and has the ad-vantage that only intermittent treatments are required, but has longbeen associated with increased risk of leukaemic transformation. Anumber of early trials therefore addressed whether other myelosup-pressive, predominantly alkylating, agents could provide an alternative.However, even greater rates of leukaemic transformation were seenwith the use of chlorambucil in the PVSG trials (6% with 32P and 11%with chlorambucil, compared to 1% in the venesection arm) [196]. TheEuropean Organisation for Research on Treatment of Cancer (EORTC)group randomised 293 patients to 32P or busulfan [197]. No differenceswere seen in rates of leukaemic transformation (1–2% with median fol-low-up of 8 years), but the busulfan-treated group had longer durationsof remission and lower rates of thrombosis and non-haematologicalmalignancies.
Pipobroman, a piperazine derivative structurally similar to manyalkylating agents, has also been assessed as a first line agent in a numberof trials and demonstrated rates of haematological remission of N92%,but rates of leukaemic transformation by 10 years of 5–14% [187,198,199]. In the French Polycythaemia Study Group (FPSG) study 292 pa-tients aged under 65 years were randomised to hydroxycarbamide orpipobroman [186,200]. Although there was no observed difference inthrombotic or haemorrhagic events, rates of transformation to AML ormyelodysplasia were significantly higher in patients treated withpipobroman (52% compared to 24% by 20 years). This was associatedwith a median overall survival of 15.4 years in the pipobroman armcompared to 20.3 years in the hydroxycarbamide arm [186].
The rates of leukaemic transformation in alkylator- or 32P–treated oruntreated patients are inconsistent between trials, which may reflectdifferences in patient selection or treatment intensity. These associa-tions were assessed more systematically in the larger ECLAP trial,where the leukaemia transformation rate was 1.8 per 100 patients peryear in 32P/alkylator-treated patients compared to 0.29 per 100 patientsper year in patients treated with venesection alone, or interferon-alpha[201]. Similarly Tefferi et al. reported an overall incidence of AML of 2.3%by 10 years, with significantly higher rates seen in patients treatedwithsingle agent 32P, pipobroman, chlorambucil or combined pipobromanand busulfan therapy [168].
6.4. Hydroxycarbamide use in PV and leukaemogenic potential
Given the associations between leukaemic transformation andalkylating agents, the use of hydroxycarbamide, a ribonucleoside reduc-tase inhibitor that interferes with DNA replication and may also act as anitric oxide donor, has been explored as an alternative. An early phase 2
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
study demonstrated its tolerability and efficacy in a cohort of 118 PV pa-tients [202]. There has been a relative paucity of phase 3 data examiningthe use of hydroxycarbamide in PV, although the FPSG trial describedabove showed comparable efficacy in preventing vascular events ascompared to pipobroman [200]. However subsequent data fromrandomised trials in ET have been informative in establishinghydroxycarbamide as a safe and effective first-line agent for the preven-tion of vascular events in high-risk MPNs. Cortelazzo et al. randomised114 high-risk ET patients to hydroxycarbamide or nomyelosuppressivetreatmentwith amedian follow-up of 27months, and reported vascularevents in 24% of the untreated arm but only 3.6% of thehydroxycarbamide-treated arm [203]. In the high risk arm of the PT1trial, 806 ET patients were randomised to aspirin plus anagrelide, an in-hibitor of cyclic AMPphosphodiesterase that blocksmegakaryocytic dif-ferentiation and proliferation, or hydroxycarbamide plus aspirin [11].Patients in the anagrelide arm were more likely to reach the compositeprimary end-point of arterial or venous thrombosis, serious haemor-rhage or death from thrombotic or haemorrhagic causes, and showedhigher rates ofmyelofibrotic transformation, arterial thrombosis and se-rious haemorrhage.
The risk of leukaemia associated with hydroxycarbamide therapyhas been more controversial. From trials such as the FPSG b65 study itis clear that the risk of AML is lower with hydroxycarbamide thanwith alkylating agents, but even in this study a surprisingly high AML/MDS transformation rate of 24.2% was seen in the hydroxycarbamidearm at 20 years (16.6% in patients who had only receivedhydroxycarbamide and no other therapy) [186]. Nonetheless AML ispart of the natural history of PV and a major issue has been the lack oftrials in PV comparing hydroxycarbamide to venesection alone, or toother “non-leukaemogenic agents”. Analysis of the ECLAP cohortshowed no difference in the rate of transformation in venesected/inter-feron-treated patients compared to those treated withhydroxycarbamide [201]. This was also the case in a Swedish case-con-trol study that included 162 patients with transformation [204] and an-other cohort of 1545 PV patients [168]. Further evidence against asignificant leukaemogenic effect of hydroxycarbamide comes from ananalysis of hprt locus mutations and “illegitimate” VDJ recombinationevents in untreated patients, hydroxycarbamide-treated MPN patientsand hydroxycarbamide-treated patients with sickle cell anaemia [205].No differencewas seen inmutation rates betweenMPN patients treatedwith prolonged hydroxycarbamide exposure compared to those withshort exposure or untreated controls. However, it is worth noting thatassessment of VDJ recombination is only of relevance in T cells, andwhether the conclusions of this analysis can be extended to myeloidor haematopoietic stem/progenitor cells is unclear.
Although the available data do not conclusively support a directleukaemogenic effect of hydroxycarbamide monotherapy, combinationtherapywith other agentsmay increase the risk of AML. In the FPSG trialof patients older than 65 years, patients were randomised to 32P or 32Pwith hydroxycarbamide maintenance [206]. A higher actuarial risk ofleukaemic transformation was observed in the latter arm, despite thepotential to reduce the radiation dose with hydroxycarbamide mainte-nance. In the long-term follow-up of the Italian ET study describedabove, higher rates of leukaemic transformation and of other secondarymalignancies were also seen when hydroxycarbamide was used se-quentially following busulfan, but were much rarer in those treatedwith hydroxycarbamide alone [207].
In summary, hydroxycarbamide is an effective treatment to achievehaematological responses and reduce vascular events in MPNs. There isevidence that the leukaemic risk associated with hydroxycarbamide ismuch lower than that seen with many other myelosuppressive agents,specifically alkylating agents and 32P, but this risk may be increased ifhydroxycarbamide is used in combination or sequentially with theseagents. The European Leukaemia Network (ELN) have generated re-sponse criteria for the treatment of PV [208] (Table 3), which dependlargely on features of PV biology rather than the development of
K2V617F: Disease biology and current management strategies in16.11.001

Table 3European Leukaemia Network criteria for response in polycythaemia vera.(Adapted from Barosi et al., 2013 [208]).
Criteria for complete response (A, B, C AND D are ALL required):A: Resolution of disease-related signs for at least 12 weeks, includinghepatosplenomegaly and improvement in MPN-SAF TSS of at least 10 points
B: Haematocrit maintained below 0.45 (without phlebotomy), platelet countbelow 400 × 109/l and white cell count below 10 × 109/l for at least 12 weeks.
C: No evidence of disease progression or thrombotic or haemorrhagic events.D: Histological remission, defined as normocellularity, absence of trilineagehyperplasia, and reticulin fibrosis b2
Criteria for partial response: A, B, AND C (as defined above) without:D: Histological remission, defined as resolution of trilineage hyperplasia
Criteria for no response:Failure to meet complete or partial response criteria.
10 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
complications. Approximately 11% of patients fail to achieve an ade-quate response with hydroxycarbamide, and a further 14% will discon-tinue due to intolerance, such as development of mucocutaneousulceration, skin cancers, pneumonitis or gastrointestinal side effects[209]. Resistance to hydroxycarbamide, as defined according to ELNcriteria [210] (Table 4), has been shown to identify a subset of patientswith increased risk of death and transformation to acute leukaemia ormyelofibrosis in one retrospective study [209]. In particular, the lackof resolution in leucocytosis was associatedwithworse overall survival,and lack of platelet control with risk of thrombosis and bleeding. Per-haps surprisingly, control of haematocrit did not correlate with throm-botic risk. Hydroxycarbamide-resistant patients therefore represent adifficult group of patients to manage and this has driven the search forother effective non-leukaemogenic agents.
6.5. Interferon-alpha and anagrelide in PV
Recombinant interferon alpha is an attractive agent for first-linetreatment in PV. It has no known leukaemogenic potential, can achievegood haematocrit and platelet count control, and has been shown to se-lectively inhibit the growth of the malignant clone leading to a reduc-tion of JAK2V617F burden or reversion of cytogenetic abnormalities,and restoration of polyclonal haematopoiesis [211,212]. Furthermore,it can antagonise platelet-derived growth factor and impair fibroblastdifferentiation, providing possible theoreticalmechanisms for an inhibi-tion of myelofibrotic transformation, supported by some evidence inearly myelofibrosis [213]. To date however, trials evaluating interferonhave predominantly been small, single-arm studies and there havebeen no randomised controlled trials allowing comparison with other
Table 4Criteria for the diagnosis of clinical resistance or intolerance to hydroxycarbamide.(Adapted from Barosi et al., 2010 [210]).
A: Need for phlebotomy to maintain haematocrit b0.45 after 3 months of at least2 g/day of hydroxycarbamide
B: Platelet count N400 × 109/l AND white blood cell count N10 × 109/l after3 months of at least 2 g/day of hydroxycarbamide
C: Failure to reduce massive splenomegaly (i.e. N10 cm below costal margin) byN50%, or to reduce splenomegaly-associated symptoms after 3 months of at least2 g/day of hydroxycarbamide
D: Absolute neutrophil count b1.0 × 109/l OR platelet count b100 × 109/l orhaemoglobin b100 g/l at the lowest dose of Hydroxycarbamide required toachieve a complete or partial clinico-haematological response (defined in Table3).
E: Presence of leg ulcers or other unacceptable hydroxycarbamide-relatednon-haematological toxicities, such as mucocutaneous manifestations,
gastrointestinal symptoms, pneumonitis or fever at any dose of hydroxycarbamideAny one of A, B, C, D or E is sufficient for the diagnosis of hydroxycarbamideresistance or intolerance.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
agents such as hydroxycarbamide. A literature review of trials per-formed in PV has provided evidence for the efficacy and tolerability ofinterferon for a total of 349 patients across 16 studies [214], althougha formal meta-analysis was not possible due to differences in the drug(interferon alpha 2a/2b, pegylated/unpegylated) and response criteriaused. This analysis demonstrated that on average 60% of patients wereable to discontinue venesection, although this was as high as 97% insome studies, and patients generally suffered low rates of thrombosis.Treatment was limited by discontinuation rates of 30–40%, with themain side effects including fatigue, headache, pyrexia, myalgia and neu-ropsychiatric symptoms. This tolerability profile, togetherwith the needfor subcutaneous administration, are themain factors limiting use of in-terferon in practice.
Pegylated interferons are those that are bound by urethane or amidebonds to a polyethylene glycol molecule. This property prolongs theirhalf-lives so that weekly rather than 24–48 hourly dosing is possible,and the reduced peak dose may potentially reduce toxicity. Three stud-ies have assessed response rates and tolerability using pegylated inter-ferons in PV. Kuriakose et al. assessed 76 patients with PV, 28 ofwhom were treated with recombinant interferon-alpha-2b, 18 withpegylated interferon-alpha-2a (Pegasys), 8 with hydroxycarbamideand 19 with other agents (imatinib, dasatinib, 32P and busulfan)[215]. Haematological responses were seen in 89.3%, 88.9% and 59.3%in the interferon-alpha-2b, pegylated interferon and non-interferongroups respectively. Discontinuation rates were 16.1% in the non-pegylated interferon arm, compared to 5.6% with pegylated treatment.Low rates of molecular response were observed across all arms (15.2%of interferon-treated patients having a partial molecular response)andwere independent of haematological response. By contrast, Pegasystreatment in two other studies of 40 and 37 PV patients was associatedwith molecular responses in 54% and 90% of patients respectively andcomplete molecular responses (i.e. undetectable JAK2V617F) in 14%and 24%, with haematological responses in 80% and 100% [212,216].Five patients in the former study had a sustained complete molecularand haematological response after discontinuing Pegasys, and nothrombotic events were observed in the study. Discontinuation rateswere 10% and 24.3% respectively, suggesting pegylated inteferons maybe a viable alternative to other interferon preparations or tohydroxycarbamide as a first-line treatment.
Phase 3 clinical trials comparing interferonswith hydroxycarbamideare ongoing andmay further inform the choice of first-line agents in fu-ture. These include the PROUD-PV study (NCT01949805), in which pa-tients were randomised to either hydroxycarbamide or pegylatedinterferon alpha-2b (PEG-intron), as well as DALIAH (NCT01387763)and NCT01259856, which compare hydroxycarbamide to Pegasys and/or PEG-intron. Further molecular characterisation may also help targetthe use of interferons: there is evidence that sensitivity to interferonmay correlate with the presence of JAK2V617F-homozygous clones[217] and, conversely, that clones carrying non-JAK2 mutations (e.g.TET2) may be more resistant to interferon [218,219].
Anagrelide selectively targets platelet production and therefore itsrole in PV is limited. However, it has demonstrated responses whenused in combination with hydroxycarbamide in a cohort ofhydroxycarbamide-resistant patients, suggesting combination therapymay be a possibility as a second-line option [220]. Anagrelide has theadvantage of being non-leukaemogenic but its use is further limitedby the increased potential for myelofibrotic transformation [11] andits side effect profile which includes tachycardias, fluid retention andheadaches.
6.6. JAK2 inhibitors in PV
Ruxolitinib is a JAK1/JAK2 inhibitor currently approved for clinicaluse in myelofibrosis and in patients with PV resistant or intolerant ofhydroxycarbamide. A Phase 2 trial first assessed its use in a cohort of34 PV patients who were resistant or intolerant to hydroxycarbamide,
K2V617F: Disease biology and current management strategies in16.11.001

11J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
with a median follow-up of 152 weeks [221]. Haematological response(by ELN criteria) was achieved in 97% of patients with 61% achieving adurable response (no requirement for venesection) for 144 weeks.70% of patients with splenomegaly showed responses in spleen sizewithin 24 weeks.
This was followed by the Phase 3 RESPONSE trial comparingruxolitinib to best available therapy in 222 PV patients with bothhydroxycarbamide resistance/intolerance and splenomegaly [20]. Theprimary composite end-point of haematocrit control and reduction inspleen size of at least 35% was met in 20.9% of the ruxolitinib arm and0.9% of the standard therapy arm, with 23.6% and 8.9% of patients, re-spectively, achieving a complete response by ELN criteria. Ruxolitinibwas particularly effective in improving constitutional symptoms, aswas seen in previous trials in myelofibrosis [18,19]. Although the trialwas not sufficiently powered to detect a difference, there was a lowrate of thrombosis in the ruxolitinib arm (1 patient, compared to 6 inthe standard therapy arm). Overall ruxolitinib had a good safety profile:anaemia was seen in 43.6% of patients and thrombocytopenia in 24.5%but grade III/IV toxicity was only seen in 1.8% and 5.4% respectively,compared to 0% and 3.6% in the standard treatment arm. Themost com-monly reported side effects were headache, fatigue, diarrhoea, musclespasms and dizziness and the rate of discontinuation due to toxicitywas low (3.6%). These studies therefore indicate a role for ruxolitinibin achieving haematological control in hydroxycarbamide-resistant/in-tolerant patients with PV and also suggest that ruxolitinib may offer ad-ditional advantages in terms of reduction of splenomegaly andsymptom control. However, the generalisability of the results is limitedby the highly selected patient group; in particular the presence of signif-icant splenomegaly. The RESPONSE-2 and MAJIC studies are comparingruxolitinib to best available therapy in hydroxycarbamide-resistant or-intolerant patients without a requirement for splenomegaly and theirresults should therefore be more generalisable to routine practice.
6.7. Histone deacetylase inhibitors and other agents in PV
Histone deacetylase (HDAC) inhibitors have been shown to haveanti-tumour activity in AML and multiple myeloma, and also haveanti-angiogenic properties. A phase 2 study assessed the use ofvorinostat in a 63 patient cohort that included 44 patients with PV. Al-though patients achieved complete resolution of pruritus (present ini-tially in 19% of patients), improvement in splenomegaly withresolution in 23% of patients and a decrease in JAK2V617F burden in65% of patients, 44% discontinued treatment during the 24-week trialperiod due to adverse events that included severe fatigue, diarrhoea,vomiting and weight loss [222]. Givinostat, which has been shown invitro to selectively inhibit JAK-STAT signalling and proliferation ofJAK2-mutant primary cells and cell lines [223], was tolerated better ina pilot study of 12 PV, 1 ET and 16 myelofibrosis patients [224]. Al-though patients also experienced diarrhoea (62%), nausea (10%), fatigue(7%) and abdominal pain (17%), thesewere Grade I-II in almost all casesand only one patient discontinued treatment because of drug-relatedadverse events. Seven of the thirteen PV or ET patients showed a clinicalresponse by ELN criteria. This study was followed by a trial of 50 or100 mg givinostat in combination with hydroxycarbamide in a cohortof 44 patients who were non-responsive to maximal doses ofhydroxycarbamide [225]. The combination was generally well tolerat-ed, with only 18% discontinuing treatment within 24 weeks. Responseswere seen in 55% of patients on 50 mg and 50% on 100 mg givinostat,with resolution of pruritus in 64% and 67%, respectively. These studiestherefore suggest a potential role for HDAC inhibitors in disease controland symptomatic management of hydroxycarbamide-resistantpatients.
There are a number of other agents currently under investigation forhydroxycarbamide-resistant patients. These include inhibitors of signal-ling down-streamof JAK2 (such as as TGR-1202, a PI3K-delta inhibitor).CEP-701 (lestaurtinib, a FLT3 inhibitor), RG7388 (a selective inhibitor of
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
p53-MDM2 binding), AUY922 (an inhibitor of heat-shock protein 90)and Imelestat (a telomerase inhibitor that has shown some efficacy inET and myelofibrosis [226,227]).
6.8. Symptom burden and control in PV
Beyond themorbidity and mortality related to PV-related complica-tions such as thromboses, haemorrhage and disease transformation, PVitself carries a significant symptomatic burden. This can be formallyquantified using the MPN symptom assessment form (MPN-SAF),where severity of a number of symptoms are scored from 1 to 10, andfrom which a total symptom score (TSS, out of 100) can be calculatedas a globalmeasure ofmorbidity [228]. This scorewas found to correlatewell with othermeasures of quality of life, with PV patients in a large in-ternational study having a mean TSS of 21.3, compared to 18.7 for thosewith ET and 25.7 for thosewithmyelofibrosis [229]. Fatigue showed thegreatest severity in patients with PV (mean 4.4/10, present in 88%),followed by itch (62%), concentration problems (65%), early satiety(64%) and inactivity (61%), and the incidence and severity of all ofthese symptoms was higher for patients with PV than those with ET.
The RESPONSE trial reported significant improvements in constitu-tional symptomswith ruxolitinib compared to standard therapy, partic-ularly those related to cytokines such as pruritus, sweats, fatigue andmuscle aches [20]. The effects on symptoms and quality of life were de-scribed further in a post-hoc analysis that used a number of tools includ-ing the MPN-SAF and EORTC QLQ-C30 quality of life questionnaire[230]. Ruxolitinib treatment was associated with a fall in TSS and withimprovements in other globalmeasures of quality of life, social, physicaland emotional functioning, while patients in the standard treatmentarm showed a deterioration on average in all thesemeasures. More spe-cifically the EORTC QLQ-C30 demonstrated improvements in fatigue,pain, anorexia, dyspnoea, diarrhoea and constipation in the ruxolitinibarm but not the standard treatment arm, while insomnia improved inboth treatment arms. The symptomatic benefit of ruxolitinib was fur-ther assessed in the RELIEF study, a double blind, double-dummy switchstudy which randomised symptomatic patients who were otherwisewell controlled on hydroxycarbamide, with no venesection require-ment or splenomegaly, to either ruxolitinib and hydroxycarbamide-pla-cebo, or hydroxycarbamide at the same dose/schedule and ruxolitinib-placebo [231]. Both ruxolitinib- and hydroxycarbamide-treatedpatientsshowedmean improvements in cytokine-related total symptom scores,although a significant difference between these arms was not observed.
Pruritus is particularly an issue in PV and is seen in 62% of patientscompared to 46% of those with ET and 50% with MF [229]. It can be as-sociated with discomfort, problems sleeping, social embarrassment,mood changes, intolerance of bathing, depression and even suicidal ide-ation [232]. Antihistamines are widely prescribed but the literature isinconsistent on whether they are beneficial. Phototherapy has beenused in small numbers of patients to good effect, and there is alsosome evidence for the use of selective serotonin reuptake inhibitoranti-depressant agents (reviewed in Saini et al. [232].). A review in2000 of 11 reports of use of interferon alpha found that 81% of the 80PV patients evaluated showed improvement in pruritus on interferontreatment, as well as improvements in splenomegaly in 77% [233].Most recently there is not only evidence that ruxolitinib can significant-ly improve the pruritus associated with PV [20,230], but also that HDACinhibitors may prove to be useful in this setting [225].
6.9. Management of special situations in PV: pregnancy and splanchnicthrombosis
Recommendations on the management of PV in pregnancy are lim-ited by its low incidence (median age at presentation is 60 and there is amale predominance) and the fact that most reports include only smallnumbers of patients and are retrospective. The experience in ET showsthat myeloproliferative conditions carry a significant risk to the mother
K2V617F: Disease biology and current management strategies in16.11.001

12 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
and fetus. A literature review of 291 pregnancies in 190womenwith ETrevealed a first trimester miscarriage rate of 39% and a live birth rate ofonly 61% [234], while the rates of maternal thrombosis and haemor-rhage were 3% and 2%, respectively. In PV a review of 36 pregnanciesin 18 patients reported a neonatal survival rate of only 50% [235].Three mothers suffered thrombotic complications, one a large post-partum haemorrhage, four developed pre-eclampsia and there wasone maternal death.
On the basis of this limited experience, the following recommenda-tions have been suggested [234,235]. Patients should continue on aspi-rin 50–100 mg and thromboembolic deterrent (TED) stockings shouldbeworn throughout pregnancy and for six weeks post-partum. 4week-ly full blood counts should be performed until 24weeks gestation and 2weekly thereafter to ensure adequate haematocrit control, and iron sup-plementation should be avoided. Patients over 35 years old, with previ-ous pregnancy complications or microcirculatory events, additionalthrombophilic factors (such as a positive lupus anticoagulant) or plate-let count over 1000× 109/l should be considered high risk and thereforeshould be considered for additional low molecular weight heparin(LMWH) or cytoreduction. Cytoreduction, in particular, would be indi-cated if there is inadequate control of the haematocrit or a rising plateletcount, while the use of LMWH is supported by experience of patientswith multiple other thrombotic risk factors in pregnancy, outside ofthe context of PV [236]. Those with a previous thromboembolic orhaemorrhagic event are considered at highest risk, in which case bothlow molecular weight heparin and cytoreduction would be indicated.No studies have addressed the optimal haematocrit in pregnancy.Given the expansion in plasma volume in this state, resulting in a signif-icantly lower haematocrit for a given red cell mass, a target of b0.36 hasbeen recommended by some [155].
Where indicated, prophylactic doses of subcutaneous LMWH areused (for example, 5000 units dalteparin or 40 mg enoxaparin daily)and monitoring of anti-Xa levels are recommended every 2–3 months.Ultrasound scanning is recommended at weeks 12, 20, 26, 30 and 36and uterine artery Doppler at 20 and 24weeks, and evidence of placen-tal insufficiency would be an indication to escalate LMWH treatment orto consider cytoreduction. There is evidence, predominantly from ani-mal studies, of teratogenicity with hydroxycarbamide use, andanagrelide can potentially cross the placenta. Therefore interferonalpha is the agent of choice for cytoreduction. If aspirin is discontinuedfor spinal or epidural analgesia, this period should be covered with pro-phylactic LMWH, with the last dose at least 12 h before. Aspirin andLMWH should be continued for at least 6 weeks post-partum for allrisk groups, as the post-partum period carries a high thrombotic riskfor the mother.
The proportion of patients with splanchnic vein thrombosis (SVT)found to have an underlying myeloproliferative neoplasm can be ashigh as 70% in some series, and this complication is seen in up to 5% ofpatients with PV [237]. The diagnosis of PV may be masked by plasmavolume expansion or bleeding/iron deficiency in those with portal hy-pertension, and therefore needs to be considered even in those with anormal haematocrit at diagnosis. Molecular studies are essential andred cell mass studies may be helpful in the situation. Currently thereare no specific recommendations for the management of SVT, beyondthose for the management of venous thrombosis in general. Immediateanticoagulation with therapeutic LMWH is required and usually follow-ed with a vitamin K antagonist. The duration of treatment required isunclear, but in patients with spontaneous SVT an argument can bemade for indefinite anticoagulation, given that SVT is potentially life-threatening and PV remains an ongoing risk factor. The utility of noveloral anticoagulant agents in this context is unclear and there is a riskof interactions with JAK inhibitors. The occurrence of thrombosis is anindicator of high-risk PV and warrants cytoreduction but data are lack-ing regarding blood count targets; a more stringent haematocrit targetof b0.42 has been adopted in some centres and may be more appropri-ate given both the high thrombotic risk in these patients, and the fact
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
that splanchnic vein thromboses may be associated with expansion ofplasma volume [238].
6.10. Summary of recommendations for the management of PV
Together the available evidence indicates that the use of low-doseaspirin and achievement of a haematocrit target of b0.45 (and poten-tially even lower in some contexts) are effective strategies for reducingthrombotic risk in patients with PV. These measures are therefore rec-ommended for all patients, regardless of the presence of additionalrisk factors. Venesection is a safe and generally well-tolerated therapyfor haematocrit control.
Cytoreduction is indicated for high-risk patients – those over the ageof 60 and/or those with a history of previous thrombosis – or for pa-tients intolerant of or inadequately controlled on venesection, thosewith intractable symptoms such as pruritus, evidence of progressivemyeloproliferation such as worsening splenomegaly or leucocytosis (it-self a risk factor for thrombosis) or with progressive thrombocytosis(and therefore at increased risk of haemorrhage) [239]. Patients withSVT require cytoreduction as well as anticoagulation and it is uncertainwhether more stringent treatment targets would result in better out-comes in this group. There is insufficient evidence to determine wheth-er cytoreductive agents are beneficial in patients at intermediate risk –i.e. those under 60 with additional risk factors such as diabetes mellitus– but the management of these patients should include modification ofrisk factors and a lower threshold for considering cytoreductive agents.
First-line cytoreduction should be either with recombinant interfer-on alpha or hydroxycarbamide. Interferon alphahas the advantages thatit is not associated with leukaemic transformation, has been shown toreduce the JAK2 mutant allele burden and potentially reduce diseaseprogression in myelofibrosis, and can be effective in reducing pruritus.However its significant side effects limit its use in older patients and itis contraindicated in those with a history of autoimmune or psychiatricconditions. Pegylated interferons may be better tolerated and requireless frequent dosing. Hydroxycarbamide does not share these advan-tages and there still is a lack of certainty about potentialleukaemogenicity, but it is generally better tolerated. Therefore it is gen-erally the drug of choice in older patients (over 50 years) and should beusedwith caution in patients with previous exposure to leukaemogenicagents. Patients failing either first-line agent can be changed to the re-maining agent if tolerated. Further options at this point would includeJAK inhibitor therapy if available, busulfan or pipobroman (whichcarry an increased risk of disease transformation and should be reservedfor patients over 75 years), anagrelide (for thrombocytosis) or a trial ofother experimental agents.
7. Conclusions
Since the identification of the JAK2V617Fmutation in themajority ofpatients with PV, significant progress has been made in elucidating themechanisms by which this genetic abnormality causes disease. Theidentification of canonical and non-canonical downstream pathwayshas demonstrated the diverse molecular and cellular effects of this sin-gle mutation on haematopoietic precursors and how they contribute toMPN phenotype, particularly that of erythrocytosis. It remains less clearhowever how JAK2V617F affects haematopoietic stem cell function andwhether other advantageous genetic lesions are generally involved inthe persistence of chronic-phase disease.
The question of how the single JAK2V617Fmutation can be associat-ed with multiple different clinical phenotypes has also been widely in-vestigated. Myelofibrosis is characterised by a wider spectrum andheavier burden of other mutations, and appears to represent a more ac-celerated phase of disease. By contrast JAK2V617F-positive ET and PVhave characteristics of a biological continuum and there is evidencethat a number of continuous and discrete variables may determine theexact clinical phenotype and diagnosis. This clinical spectrum of
K2V617F: Disease biology and current management strategies in16.11.001

13J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
JAK2V617F-positive ET/PV and its differences from JAK2-negative ET arenot yet fully reflected in international diagnostic criteria, managementguidelines or clinical trials.
Together the biological data indicate that disease phenotype andpersistence in JAK2-mutated PV reflect a broad diversity of molecularperturbations. Moreover themechanisms that determine themost clin-ically damaging events – those of disease transformation – are evenmore complex and are likely to depend on additional, heterogeneousgenetic lesions. This complexity accounts for the relative lack of prog-ress in development of therapies that affect the underlying disease biol-ogy and in particular the size of the JAK2-mutant clone and risk ofdisease transformation. It is clear that inhibition of JAK2 in PV and relat-ed disorders does not result in the same clonal response that is seenwith inhibitors of BCR-ABL in chronic myeloid leukaemia. Althoughthere are promising suggestions that newer agents such as pegylated in-terferonsmay specifically target the disease clone, the challenge is nowto elucidate which characteristics of a patient and their disease accountfor and predict response to these treatments. Moreover no agent has yetbeen shown to prevent or delay disease progression. In the meantime,management of PV remains centred on prevention of cardiovascularcomplications and studies continue to clarify the roles of specificcytoreductive agents and their respective treatment targets. Nonethe-less important areas such as the use of additional thrombotic riskmarkers, the impact of novel agents (e.g. JAK2 inhibitors) on thrombo-sis, and management of JAK2V617F-associated splanchnic vein throm-bosis, require further study in prospective trials.
7.1. Practice points
• Optimisation of cardiovascular risk factors and aspirin 75–100 mgdaily (unless contraindicated) should be employed for all patients.
• A target haematocrit of b0.45 should be used for all risk groups. Somecentres advocate lower targets in females and in certain high-risk sit-uations. Venesection alone may be sufficient to achieve this and ispreferable in low-risk patients. Given the evidence for a biologicalcontinuum between JAK2-mutated ET and PV and the possibility ofmasked PV, there is an argument for maintaining haematocrit b0.45in all JAK2-mutated patients.
• Consider interferon-alpha for low-risk patients if intolerant of vene-section or symptomatic, particularly with pruritus.
• Cytoreduction with interferon-alpha or hydroxycarbamide is indicat-ed in high-risk patients (age N 60 and/or previous thrombosis) andshould be considered in cases with progressive myeloproliferation(rising white cell count, splenomegaly), uncontrolled thrombocytosisor contraindications to venesection.
• In patients with an inadequate response, alternative first-line agentscan be attempted and patients should be considered for clinical trials.In older patients (e.g. N75 years) busulfan or pipobromanmay be con-sidered.
• Individualised molecular characterisation (such as JAK2V617F alleleburden and presence of additional somatic mutations e.g. TET2 andTP53) may in future offer improved risk stratification and inform thechoice of therapeutic agent.
7.2. Research agenda
• Effects of JAK2V617F on haematopoietic stem cells andmechanisms bywhich disease clones persist in chronic-phase PV
• Prospective evaluation of leucocytosis and JAK2V617F allele burden aspossible additional markers of thrombotic risk in PV
• Role of additional genetic lesions in disease transformation and inidentifying patients as candidates for novel therapies
• Effects of interferon-alpha, JAK2 inhibitors and other novel therapieson thrombotic risk, JAK2 mutant burden and risk of disease
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
transformation• Relationship between PV and JAK2V617F-positive ET, as compared toJAK2-negative ET, in clinical practice, especially the role of haematocritin thrombotic risk in JAK2V617F-positive ET
• Treatment targets in very high risk patients, especially those withsplanchnic vein thrombosis and for other subgroups, e.g. males vs. fe-males, pregnancy.
• The use of novel agents or first-line JAK inhibitors in high-riskpatients.
Conflict of interest statement
JG has no conflicts of interest to declare. ALG has received speakerhonoraria from Novartis and Shire.
References
[1] Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. WHO classifica-tion of Tumours of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.
[2] James C, Ugo V, Le Couedic JP, Staerk J, Delhommeau F, Lacout C, et al. A uniqueclonal JAK2 mutation leading to constitutive signalling causes polycythaemiavera. Nature 2005;434(7037):1144–8.
[3] Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N, Swanton S, et al. Acquiredmutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lan-cet 2005;365(9464):1054–61.
[4] Kralovics R, Passamonti F, Buser AS, Teo SS, Tiedt R, Passweg JR, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med 2005;352(17):1779–90.
[5] Levine RL, Wadleigh M, Cools J, Ebert BL, Wernig G, Huntly BJ, et al. Activating mu-tation in the tyrosine kinase JAK2 in polycythemia vera, essentialthrombocythemia, and myeloid metaplasia with myelofibrosis. Cancer Cell 2005;7(4):387–97.
[6] Scott LM, Tong W, Levine RL, Scott MA, Beer PA, Stratton MR, et al. JAK2 exon 12mutations in polycythemia vera and idiopathic erythrocytosis. N Engl J Med2007;356(5):459–68.
[7] Scott LM, Beer PA, Bench AJ, Erber WN, Green AR. Prevalance of JAK2 V617F andexon 12 mutations in polycythaemia vera. Br J Haematol 2007;139(3):511–2.
[8] Wardrop D, Steensma DP. Is refractory anaemia with ring sideroblasts andthrombocytosis (RARS-T) a necessary or useful diagnostic category? Br J Haematol2009;144(6):809–17.
[9] Levine RL, Loriaux M, Huntly BJ, Loh ML, Beran M, Stoffregen E, et al. TheJAK2V617F activating mutation occurs in chronic myelomonocytic leukemia andacute myeloid leukemia, but not in acute lymphoblastic leukemia or chronic lym-phocytic leukemia. Blood 2005;106(10):3377–9.
[10] Jones AV, Kreil S, Zoi K, Waghorn K, Curtis C, Zhang L, et al. Widespread occurrenceof the JAK2 V617F mutation in chronic myeloproliferative disorders. Blood 2005;106(6):2162–8.
[11] Harrison CN, Campbell PJ, Buck G, Wheatley K, East CL, Bareford D, et al. Hydroxy-urea compared with anagrelide in high-risk essential thrombocythemia. N Engl JMed 2005;353(1):33–45.
[12] Gangat N, Caramazza D, Vaidya R, George G, Begna K, Schwager S, et al. DIPSS plus:a refined dynamic international prognostic scoring system for primary myelofibro-sis that incorporates prognostic information from karyotype, platelet count, andtransfusion status. J Clin Oncol 2011;29(4):392–7.
[13] Vannucchi AM, Antonioli E, Guglielmelli P, Rambaldi A, Barosi G, Marchioli R, et al.Clinical profile of homozygous JAK2 617 V N F mutation in patients with polycythe-mia vera or essential thrombocythemia. Blood 2007;110(3):840–6.
[14] Dahabreh IJ, Zoi K, Giannouli S, Zoi C, Loukopoulos D, Voulgarelis M. Is JAK2 V617Fmutationmore than a diagnostic index? Ameta-analysis of clinical outcomes in es-sential thrombocythemia. Leuk Res 2009;33(1):67–73.
[15] McMullin MF, Reilly JT, Campbell P, Bareford D, Green AR, Harrison CN, et al.Amendment to the guideline for diagnosis and investigation of polycythaemia/erythrocytosis. Br J Haematol 2007;138(6):821–2.
[16] Harrison CN, Bareford D, Butt N, Campbell P, Conneally E, Drummond M, et al.Guideline for investigation and management of adults and children presentingwith a thrombocytosis. Br J Haematol 2010;149(3):352–75.
[17] Reilly JT, McMullin MF, Beer PA, Butt N, Conneally E, Duncombe A, et al. Guidelinefor the diagnosis and management of myelofibrosis. Br J Haematol 2012;158(4):453–71.
[18] Harrison C, Kiladjian JJ, Al-Ali HK, Gisslinger H, Waltzman R, Stalbovskaya V, et al.JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. NEngl J Med 2012;366(9):787–98.
[19] Verstovsek S, Mesa RA, Gotlib J, Levy RS, Gupta V, DiPersio JF, et al. A double-blind,placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med 2012;366(9):799–807.
[20] Vannucchi AM, Kiladjian JJ, Griesshammer M, Masszi T, Durrant S, Passamonti F,et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera.N Engl J Med 2015;372(5):426–35.
[21] Ward AC, Touw I, Yoshimura A. The Jak-Stat pathway in normal and perturbed he-matopoiesis. Blood 2000;95(1):19–29.
K2V617F: Disease biology and current management strategies in16.11.001

14 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
[22] Penta K, Sawyer ST. Erythropoietin induces the tyrosine phosphorylation, nucleartranslocation, and DNA binding of STAT1 and STAT5 in erythroid cells. J BiolChem 1995;270(52):31282–7.
[23] Rane SG, Reddy EP. Janus kinases: components of multiple signaling pathways. On-cogene 2000;19(49):5662–79.
[24] Saharinen P, Silvennoinen O. The pseudokinase domain is required for suppressionof basal activity of Jak2 and Jak3 tyrosine kinases and for cytokine-inducible activa-tion of signal transduction. J Biol Chem 2002;277(49):47954–63.
[25] Saharinen P, Vihinen M, Silvennoinen O. Autoinhibition of Jak2 tyrosine kinase isdependent on specific regions in its pseudokinase domain. Mol Biol Cell 2003;14(4):1448–59.
[26] Lindauer K, Loerting T, Liedl KR, Kroemer RT. Prediction of the structure of humanJanus kinase 2 (JAK2) comprising the two carboxy-terminal domains reveals amechanism for autoregulation. Protein Eng 2001;14(1):27–37.
[27] Sanz A, Ungureanu D, Pekkala T, Ruijtenbeek R, Touw IP, Hilhorst R, et al. Analysisof Jak2 catalytic function by peptide microarrays: the role of the JH2 domain andV617F mutation. PLoS One 2011;6(4), e18522.
[28] Ungureanu D, Wu J, Pekkala T, Niranjan Y, Young C, Jensen ON, et al. Thepseudokinase domain of JAK2 is a dual-specificity protein kinase that negativelyregulates cytokine signaling. Nat Struct Mol Biol 2011;18(9):971–6.
[29] Dusa A, Mouton C, Pecquet C, HermanM, Constantinescu SN. JAK2 V617F constitu-tive activation requires JH2 residue F595: a pseudokinase domain target for specificinhibitors. PLoS One 2010;5(6), e11157.
[30] Bandaranayake RM, Ungureanu D, Shan Y, Shaw DE, Silvennoinen O, Hubbard SR.Crystal structures of the JAK2 pseudokinase domain and the pathogenic mutantV617F. Nat Struct Mol Biol 2012;19(8):754–9.
[31] Toms AV, Deshpande A, McNally R, Jeong Y, Rogers JM, Kim CU, et al. Structure of apseudokinase-domain switch that controls oncogenic activation of Jak kinases. NatStruct Mol Biol 2013;20(10):1221–3.
[32] Wernig G, Mercher T, Okabe R, Levine RL, Lee BH, Gilliland DG. Expression ofJak2V617F causes a polycythemia vera-like disease with associated myelofibrosisin a murine bone marrow transplant model. Blood 2006;107(11):4274–81.
[33] Zaleskas VM, Krause DS, Lazarides K, Patel N, Hu Y, Li S, et al. Molecular pathogen-esis and therapy of polycythemia induced inmice by JAK2 V617F. PLoS One 2006;1,e18.
[34] Laubach JP, Fu P, Jiang X, Salter KH, Potti A, Arcasoy MO. Polycythemia vera ery-throid precursors exhibit increased proliferation and apoptosis resistance associat-ed with abnormal RAS and PI3K pathway activation. Exp Hematol 2009;37(12):1411–22.
[35] Teofili L, Martini M, Cenci T, Petrucci G, Torti L, Storti S, et al. Different STAT-3 andSTAT-5 phosphorylation discriminates among Ph-negative chronic myeloprolifera-tive diseases and is independent of the V617F JAK-2 mutation. Blood 2007;110(1):354–9.
[36] Grimwade LF, Happerfield L, Tristram C, McIntosh G, Rees M, Bench AJ, et al.Phospho-STAT5 and phospho-Akt expression in chronic myeloproliferative neo-plasms. Br J Haematol 2009;147(4):495–506.
[37] Aboudola S, Murugesan G, Szpurka H, Ramsingh G, Zhao X, Prescott N, et al. Bonemarrow phospho-STAT5 expression in non-CML chronic myeloproliferative disor-ders correlates with JAK2 V617F mutation and provides evidence of in vivo JAK2activation. Am J Surg Pathol 2007;31(2):233–9.
[38] Akada H, Yan D, Zou H, Fiering S, Hutchison RE, MohiMG. Conditional expression ofheterozygous or homozygous Jak2V617F from its endogenous promoter induces apolycythemia vera-like disease. Blood 2010;115(17):3589–97.
[39] Li J, Spensberger D, Ahn JS, Anand S, Beer PA, Ghevaert C, et al. JAK2 V617F impairshematopoietic stem cell function in a conditional knock-in mouse model of JAK2V617F-positive essential thrombocythemia. Blood 2010;116(9):1528–38.
[40] Mullally A, Lane SW, Ball B, Megerdichian C, Okabe R, Al-Shahrour F, et al. Physio-logical Jak2V617F expression causes a lethal myeloproliferative neoplasm with dif-ferential effects on hematopoietic stem and progenitor cells. Cancer Cell 2010;17(6):584–96.
[41] Marty C, Lacout C, Martin A, Hasan S, Jacquot S, Birling MC, et al. Myeloproliferativeneoplasm induced by constitutive expression of JAK2V617F in knock-in mice.Blood 2010;116(5):783–7.
[42] Garcon L, Rivat C, James C, Lacout C, Camara-Clayette V, Ugo V, et al. Constitutiveactivation of STAT5 and Bcl-xL overexpression can induce endogenous erythroidcolony formation in human primary cells. Blood 2006;108(5):1551–4.
[43] Yan D, Hutchison RE, Mohi G. Critical requirement for Stat5 in a mouse model ofpolycythemia vera. Blood 2012;119(15):3539–49.
[44] Walz C, Ahmed W, Lazarides K, Betancur M, Patel N, Hennighausen L, et al. Essen-tial role for Stat5a/b in myeloproliferative neoplasms induced by BCR-ABL1 andJAK2(V617F) in mice. Blood 2012;119(15):3550–60.
[45] Hobbs CM, Manning H, Bennett C, Vasquez L, Severin S, Brain L, et al. JAK2V617Fleads to intrinsic changes in platelet formation and reactivity in a knock-inmouse model of essential thrombocythemia. Blood 2013;122(23):3787–97.
[46] Zeuner A, Pedini F, Signore M, Ruscio G, Messina C, Tafuri A, et al. Increased deathreceptor resistance and FLIPshort expression in polycythemia vera erythroid pre-cursor cells. Blood 2006;107(9):3495–502.
[47] Silva M, Richard C, Benito A, Sanz C, Olalla I, Fernandez-Luna JL. Expression of Bcl-xin erythroid precursors from patients with polycythemia vera. N Engl J Med 1998;338(9):564–71.
[48] Ciurea SO, Merchant D, Mahmud N, Ishii T, Zhao Y, Hu W, et al. Pivotal contribu-tions of megakaryocytes to the biology of idiopathic myelofibrosis. Blood 2007;110(3):986–93.
[49] Zhao R, Follows GA, Beer PA, Scott LM, Huntly BJ, Green AR, et al. Inhibition of theBcl-xL deamidation pathway in myeloproliferative disorders. N Engl J Med 2008;359(26):2778–89.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
[50] Gozgit JM, Bebernitz G, Patil P, Ye M, Parmentier J, Wu J, et al. Effects of the JAK2inhibitor, AZ960, on Pim/BAD/BCL-xL survival signaling in the human JAK2 V617Fcell line SET-2. J Biol Chem 2008;283(47):32334–43.
[51] Will B, Siddiqi T, Jorda MA, Shimamura T, Luptakova K, Staber PB, et al. Apoptosisinduced by JAK2 inhibition is mediated by Bim and enhanced by the BH3 mimeticABT-737 in JAK2 mutant human erythroid cells. Blood 2010;115(14):2901–9.
[52] Rubert J, Qian Z, Andraos R, Guthy DA, Radimerski T. Bim andMcl-1 exert key rolesin regulating JAK2V617F cell survival. BMC Cancer 2011;11:24.
[53] Wood AD, Chen E, Donaldson IJ, Hattangadi S, Burke KA, DawsonMA, et al. ID1 pro-motes expansion and survival of primary erythroid cells and is a target ofJAK2V617F-STAT5 signaling. Blood 2009;114(9):1820–30.
[54] Plo I, NakatakeM,Malivert L, de Villartay JP, Giraudier S, Villeval JL, et al. JAK2 stim-ulates homologous recombination and genetic instability: potential implication inthe heterogeneity of myeloproliferative disorders. Blood 2008;112(4):1402–12.
[55] Marty C, Lacout C, Droin N, Le Couedic JP, Ribrag V, Solary E, et al. A role for reactiveoxygen species in JAK2 myeloproliferative neoplasm progression. Leukemia 2013;27(11):2187–95.
[56] Chen E, Ahn JS, Massie CE, Clynes D, Godfrey AL, Li J, et al. JAK2V617F promotesreplication fork stalling with disease-restricted impairment of the intra-S check-point response. Proc Natl Acad Sci U S A 2014;111(42):15190–5.
[57] Dawson MA, Bannister AJ, Gottgens B, Foster SD, Bartke T, Green AR, et al. JAK2phosphorylates histone H3Y41 and excludes HP1alpha from chromatin. Nature2009;461(7265):819–22.
[58] DawsonMA, Foster SD, Bannister AJ, Robson SC, Hannah R,Wang X, et al. Three dis-tinct patterns of histone H3Y41 phosphorylation mark active genes. Cell Rep 2012;2(3):470–7.
[59] Liu F, Zhao X, Perna F, Wang L, Koppikar P, Abdel-Wahab O, et al. JAK2V617F-me-diated phosphorylation of PRMT5 downregulates its methyltransferase activity andpromotes myeloproliferation. Cancer Cell 2011;19(2):283–94.
[60] Fleischman AG, Aichberger KJ, Luty SB, Bumm TG, Petersen CL, Doratotaj S, et al.TNFalpha facilitates clonal expansion of JAK2V617F positive cells in myeloprolifer-ative neoplasms. Blood 2011;118(24):6392–8.
[61] Chow A, Huggins M, Ahmed J, Hashimoto D, Lucas D, Kunisaki Y, et al. CD169(+)macrophages provide a niche promoting erythropoiesis under homeostasis andstress. Nat Med 2013;19(4):429–36.
[62] Ramos P, Casu C, Gardenghi S, Breda L, Crielaard BJ, Guy E, et al. Macrophages sup-port pathological erythropoiesis in polycythemia vera and beta-thalassemia. NatMed 2013;19(4):437–45.
[63] Dupont S, Masse A, James C, Teyssandier I, Lecluse Y, Larbret F, et al. The JAK2V617F mutation triggers erythropoietin hypersensitivity and terminal erythroidamplification in primary cells from patients with polycythemia vera. Blood 2007;110(3):1013–21.
[64] Moliterno AR, Williams DM, Rogers O, Isaacs MA, Spivak JL. Phenotypic variabilitywithin the JAK2 V617F-positive MPD: roles of progenitor cell and neutrophil alleleburdens. Exp Hematol 2008;36(11):1480–6.
[65] Anand S, Stedham F, Beer P, Gudgin E, Ortmann CA, Bench A, et al. Effects of theJAK2 mutation on the hematopoietic stem and progenitor compartment inhuman myeloproliferative neoplasms. Blood 2011;118(1):177–81.
[66] Ishii T, Bruno E, Hoffman R, Xu M. Involvement of various hematopoietic-cell line-ages by the JAK2V617F mutation in polycythemia vera. Blood 2006;108(9):3128–34.
[67] Gaikwad A, Nussenzveig R, Liu E, Gottshalk S, Chang K, Prchal JT. In vitro expansionof erythroid progenitors from polycythemia vera patients leads to decrease in JAK2V617F allele. Exp Hematol 2007;35(4):587–95.
[68] Hasan S, Lacout C, Marty C, Cuingnet M, Solary E, Vainchenker W, et al. JAK2V617Fexpression in mice amplifies early hematopoietic cells and gives them a competi-tive advantage that is hampered by IFNalpha. Blood 2013;122(8):1464–77.
[69] Ishii T, Zhao Y, Sozer S, Shi J, Zhang W, Hoffman R, et al. Behavior of CD34+ cellsisolated from patients with polycythemia vera in NOD/SCID mice. Exp Hematol2007;35(11):1633–40.
[70] James C,Mazurier F, Dupont S, Chaligne R, Lamrissi-Garcia I, TulliezM, et al. The he-matopoietic stem cell compartment of JAK2V617F-positive myeloproliferative dis-orders is a reflection of disease heterogeneity. Blood 2008;112(6):2429–38.
[71] Mullally A, Poveromo L, Schneider RK, Al-Shahrour F, Lane SW, Ebert BL. Distinctroles for long-term hematopoietic stem cells and erythroid precursor cells in a mu-rinemodel of Jak2V617F-mediated polycythemia vera. Blood 2012;120(1):166–72.
[72] Mullally A, Bruedigam C, Poveromo L, Heidel FH, Purdon A, Vu T, et al. Deple-tion of Jak2V617F myeloproliferative neoplasm-propagating stem cells by in-terferon-alpha in a murine model of polycythemia vera. Blood 2013;121(18):3692–702.
[73] Li J, Kent DG, Godfrey AL, Manning H, Nangalia J, Aziz A, et al. JAK2V617F-homozy-gosity drives a phenotypic switch between myeloproliferative neoplasms in a mu-rine model, but is insufficient to sustain clonal expansion. Blood 2014.
[74] Kent DG, Li J, Tanna H, Fink J, Kirschner K, Pask DC, et al. Self-renewal of singlemouse hematopoietic stem cells is reduced by JAK2V617F without compromisingprogenitor cell expansion. PLoS Biol 2013;11(6), e1001576.
[75] Theocharides A, Passweg JR, Medinger M, Looser R, Li S, Hao-Shen H, et al. The al-lele burden of JAK2 mutations remains stable over several years in patients withmyeloproliferative disorders. Haematologica 2008;93(12):1890–3.
[76] Van Pelt K, Nollet F, Selleslag D, Knoops L, Constantinescu SN, Criel A, et al. TheJAK2V617F mutation can occur in a hematopoietic stem cell that exhibits no prolif-erative advantage: a case of human allogeneic transplantation. Blood 2008;112(3):921–2.
[77] Mead AJ, Chowdhury O, Pecquet C, Dusa A, Woll P, Atkinson D, et al. Impact of iso-lated germline JAK2V617I mutation on human hematopoiesis. Blood 2013;121(20):4156–65.
K2V617F: Disease biology and current management strategies in16.11.001

15J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
[78] Petzer AL, Eaves CJ, Barnett MJ, Eaves AC. Selective expansion of primitive normalhematopoietic cells in cytokine-supplemented cultures of purified cells from pa-tients with chronic myeloid leukemia. Blood 1997;90(1):64–9.
[79] Dazzi F, Hasserjian R, Gordon MY, Boecklin F, Cotter F, Corbo M, et al. Normal andchronic phase CML hematopoietic cells repopulate NOD/SCID bone marrow withdifferent kinetics and cell lineage representation. Hematol J 2000;1(5):307–15.
[80] Schemionek M, Elling C, Steidl U, Baumer N, Hamilton A, Spieker T, et al. BCR-ABLenhances differentiation of long-term repopulating hematopoietic stem cells. Blood2010;115(16):3185–95.
[81] Michaloglou C, Vredeveld LC, Soengas MS, Denoyelle C, Kuilman T, van der HorstCM, et al. BRAFE600-associated senescence-like cell cycle arrest of human naevi.Nature 2005;436(7051):720–4.
[82] Wajapeyee N, Wang SZ, Serra RW, Solomon PD, Nagarajan A, Zhu X, et al. Senes-cence induction in human fibroblasts and hematopoietic progenitors by leukemo-genic fusion proteins. Blood 2010;115(24):5057–60.
[83] Anand S, Stedham F, Gudgin E, Campbell P, Beer P, Green AR, et al. Increased basalintracellular signaling patterns do not correlate with JAK2 genotype in humanmy-eloproliferative neoplasms. Blood 2011;118(6):1610–21.
[84] Campbell PJ, Scott LM, Buck G, Wheatley K, East CL, Marsden JT, et al. Definition ofsubtypes of essential thrombocythaemia and relation to polycythaemia vera basedon JAK2 V617F mutation status: a prospective study. Lancet 2005;366(9501):1945–53.
[85] Antonioli E, Guglielmelli P, Pancrazzi A, Bogani C, Verrucci M, Ponziani V, et al. Clin-ical implications of the JAK2 V617F mutation in essential thrombocythemia. Leuke-mia 2005;19(10):1847–9.
[86] Wolanskyj AP, Lasho TL, Schwager SM, McClure RF, Wadleigh M, Lee SJ, et al. JAK2mutation in essential thrombocythaemia: clinical associations and long-term prog-nostic relevance. Br J Haematol 2005;131(2):208–13.
[87] Cheung B, Radia D, Pantelidis P, Yadegarfar G, Harrison C. The presence of the JAK2V617F mutation is associated with a higher haemoglobin and increased risk ofthrombosis in essential thrombocythaemia. Br J Haematol 2006;132(2):244–5.
[88] Kittur J, Knudson RA, Lasho TL, Finke CM, Gangat N, Wolanskyj AP, et al. Clinicalcorrelates of JAK2V617F allele burden in essential thrombocythemia. Cancer2007;109(11):2279–84.
[89] Rumi E, Pietra D, Ferretti V, Klampfl T, Harutyunyan AS, Milosevic JD, et al. JAK2 orCALR mutation status defines subtypes of essential thrombocythemia with sub-stantially different clinical course and outcomes. Blood 2013;123(10):1544–51.
[90] Nangalia J, Massie CE, Baxter EJ, Nice FL, Gundem G,Wedge DC, et al. Somatic CALRmutations in myeloproliferative neoplasms with nonmutated JAK2. N Engl J Med2013;369(25):2391–405.
[91] Vannucchi AM, Antonioli E, Guglielmelli P, Longo G, Pancrazzi A, Ponziani V, et al.Prospective identification of high-risk polycythemia vera patients based onJAK2V617F allele burden. Leukemia 2007;21(9):1952–9.
[92] Tefferi A, Strand JJ, Lasho TL, Knudson RA, Finke CM, Gangat N, et al. Bone marrowJAK2V617F allele burden and clinical correlates in polycythemia vera. Leukemia2007;21(9):2074–5.
[93] Passamonti F, Rumi E, Pietra D, Elena C, Boveri E, Arcaini L, et al. A prospectivestudy of 338 patients with polycythemia vera: the impact of JAK2 (V617F) alleleburden and leukocytosis on fibrotic or leukemic disease transformation and vascu-lar complications. Leukemia 2010;24(9):1574–9.
[94] Silver RT, Vandris K, Wang YL, Adriano F, Jones AV, Christos PJ, et al. JAK2(V617F)allele burden in polycythemia vera correlates with grade of myelofibrosis, but isnot substantially affected by therapy. Leuk Res 2011;35(2):177–82.
[95] Tefferi A, Lasho TL, Schwager SM, Strand JS, Elliott M,Mesa R, et al. The clinical phe-notype of wild-type, heterozygous, and homozygous JAK2V617F in polycythemiavera. Cancer 2006;106(3):631–5.
[96] Tiedt R, Hao-Shen H, Sobas MA, Looser R, Dirnhofer S, Schwaller J, et al. Ratio ofmutant JAK2-V617F to wild-type Jak2 determines the MPD phenotypes in trans-genic mice. Blood 2008;111(8):3931–40.
[97] Shide K, Shimoda HK, Kumano T, Karube K, Kameda T, Takenaka K, et al. Develop-ment of ET, primary myelofibrosis and PV in mice expressing JAK2 V617F. Leuke-mia 2008;22(1):87–95.
[98] Xing S, Wanting TH, Zhao W, Ma J, Wang S, Xu X, et al. Transgenic expression ofJAK2V617F causes myeloproliferative disorders in mice. Blood 2008;111(10):5109–17.
[99] Akada H, Akada S, Hutchison RE, Mohi G. Loss of wild-type Jak2 allele enhancesmyeloid cell expansion and accelerates myelofibrosis in Jak2V617F knock-inmice. Leukemia 2014;28(8):1627–35.
[100] Scott LM, Scott MA, Campbell PJ, Green AR. Progenitors homozygous for the V617Fmutation occur in most patients with polycythemia vera, but not essentialthrombocythemia. Blood 2006;108(7):2435–7.
[101] Pardanani A, Lasho TL, Finke C, Mesa RA, Hogan WJ, Ketterling RP, et al. ExtendingJak2V617F andMplW515mutation analysis to single hematopoietic colonies and Band T lymphocytes. Stem Cells 2007;25(9):2358–62.
[102] Godfrey AL, Chen E, Pagano F, Ortmann CA, Silber Y, Bellosillo B, et al. JAK2V617Fhomozygosity arises commonly and recurrently in PV and ET, but PV is character-ized by expansion of a dominant homozygous subclone. Blood 2012;120(13):2704–7.
[103] Godfrey AL, Chen E, Pagano F, Silber Y, Campbell PJ, Green AR. Clonal analyses re-veal associations of JAK2V617F homozygosity with hematologic features, age andgender in polycythemia vera and essential thrombocythemia. Haematologica2013;98(5):718–21.
[104] Vainchenker W, Delhommeau F, Constantinescu SN, Bernard OA. New mutationsand pathogenesis of myeloproliferative neoplasms. Blood 2011;118(7):1723–35.
[105] Delhommeau F, Dupont S, Della Valle V, James C, Trannoy S, Masse A, et al. Muta-tion in TET2 in myeloid cancers. N Engl J Med 2009;360(22):2289–301.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
[106] Nangalia J, Nice FL, Wedge DC, Godfrey AL, Grinfeld J, Thakker C, et al. DNMT3Amutations occur early or late in patients with myeloproliferative neoplasms andmutation order influences phenotype. Haematologica 2015;100(11):e438–42.
[107] Stein BL, Williams DM, Rogers O, Isaacs MA, Spivak JL, Moliterno AR. Disease bur-den at the progenitor level is a feature of primary myelofibrosis: a multivariableanalysis of 164 JAK2 V617F-positive myeloproliferative neoplasm patients. ExpHematol 2011;39(1):95–101.
[108] Ortmann CA, Kent DG, Nangalia J, Silber Y, Wedge DC, Grinfeld J, et al. Effect of mu-tation order on myeloproliferative neoplasms. N Engl J Med 2015;372(7):601–12.
[109] Jutzi JS, Bogeska R, Nikoloski G, Schmid CA, Seeger TS, Stegelmann F, et al. MPN pa-tients harbor recurrent truncating mutations in transcription factor NF-E2. J ExpMed 2013;210(5):1003–19.
[110] Godfrey AL, Nangalia J, Baxter EJ, Massie CE, Kent DG, Papaemmanuil E, et al. Non-genetic stochastic expansion of JAK2V617F-homozygous subclones in polycythe-mia vera? Blood 2014;124(22):3332–4.
[111] Etheridge SL, Cosgrove ME, Sangkhae V, Corbo L, Roh M, Seeliger MA, et al. A novelactivating, germline JAK2 mutation, JAK2R564Q, causes familial essentialthrombocytosis. Blood 2013;123(7):1059–68.
[112] Marty C, Saint Martin C, Pecquet C, Grosjean S, Saliba J, Mouton C, et al. GermlineJAK2 mutations in the kinase domain are responsible for hereditarythrombocytosis and are resistant to JAK2 and HSP90 inhibitors. Blood 2014;123(9):1372–83.
[113] Jones AV, Chase A, Silver RT, Oscier D, Zoi K, Wang YL, et al. JAK2 haplotype is amajor risk factor for the development of myeloproliferative neoplasms. NatGenet 2009;41(4):446–9.
[114] Olcaydu D, Harutyunyan A, Jager R, Berg T, Gisslinger B, Pabinger I, et al. A commonJAK2 haplotype confers susceptibility to myeloproliferative neoplasms. Nat Genet2009;41(4):450–4.
[115] Olcaydu D, Skoda RC, Looser R, Li S, Cazzola M, Pietra D, et al. The ‘GGCC’ haplotypeof JAK2 confers susceptibility to JAK2 exon 12 mutation-positive polycythemiavera. Leukemia 2009;23(10):1924–6.
[116] Jones AV, Campbell PJ, Beer PA, Schnittger S, Vannucchi AM, Zoi K, et al. The JAK246/1 haplotype predisposes to MPL-mutated myeloproliferative neoplasms. Blood2010;115(22):4517–23.
[117] Kilpivaara O, Mukherjee S, Schram AM, Wadleigh M, Mullally A, Ebert BL, et al. Agermline JAK2 SNP is associated with predisposition to the development ofJAK2(V617F)-positivemyeloproliferative neoplasms. Nat Genet 2009;41(4):455–9.
[118] Jones AV, Cross NC. Inherited predisposition to myeloproliferative neoplasms. TherAdv Hematol 2013;4(4):237–53.
[119] Alvarez-Larran A, Angona A, Martinez-Aviles L, Bellosillo B, Besses C. Influence ofJAK2 46/1 haplotype in the natural evolution of JAK2V617F allele burden in pa-tients with myeloproliferative neoplasms. Leuk Res 2012;36(3):324–6.
[120] Wang J, Xu Z, Liu L, Gale RP, Cross NC, Jones AV, et al. JAK2V617F allele burden,JAK2 46/1 haplotype and clinical features of Chinese with myeloproliferative neo-plasms. Leukemia 2013;27(8):1763–7.
[121] Oddsson A, Kristinsson SY, Helgason H, Gudbjartsson DF, Masson G, Sigurdsson A,et al. The germline sequence variant rs2736100_C in TERT associates with myelo-proliferative neoplasms. Leukemia 2014;28(6):1371–4.
[122] Tapper W, Jones AV, Kralovics R, Harutyunyan AS, Zoi K, Leung W, et al. Geneticvariation atMECOM, TERT, JAK2 and HBS1L-MYB predisposes tomyeloproliferativeneoplasms. Nat Commun 2015;6:6691.
[123] Hinds DA, Barnholt KE, Mesa RA, Kiefer AK, Do CB, Eriksson N, et al. Germline var-iants predispose to both JAK2 V617F clonal hematopoiesis and myeloproliferativeneoplasms. Blood 2016;128(8):1121–8.
[124] Garcia P, ClarkeM, Vegiopoulos A, Berlanga O, Camelo A, LorvellecM, et al. Reducedc-Myb activity compromises HSCs and leads to a myeloproliferation with a novelstem cell basis. EMBO J 2009;28(10):1492–504.
[125] Varricchio L, Masselli E, Alfani E, Battistini A, Migliaccio G, Vannucchi AM, et al. Thedominant negative beta isoform of the glucocorticoid receptor is uniquelyexpressed in erythroid cells expanded from polycythemia vera patients. Blood2011;118(2):425–36.
[126] Poletto V, Rosti V, Villani L, Catarsi P, Carolei A, Campanelli R, et al. A3669G poly-morphism of glucocorticoid receptor is a susceptibility allele for primary myelofi-brosis and contributes to phenotypic diversity and blast transformation. Blood2012;120(15):3112–7.
[127] Hernandez-Boluda JC, Pereira A, Cervantes F, Alvarez-Larran A, Collado M, Such E,et al. A polymorphism in the XPD gene predisposes to leukemic transformationand new nonmyeloid malignancies in essential thrombocythemia and polycythe-mia vera. Blood 2012;119(22):5221–8.
[128] Chen E, Beer PA, Godfrey AL, Ortmann CA, Li J, Costa-Pereira AP, et al. Distinct clin-ical phenotypes associated with JAK2V617F reflect differential STAT1 signaling.Cancer Cell 2010;18(5):524–35.
[129] Duek A, Lundberg P, Shimizu T, Grisouard J, Karow A, Kubovcakova L, et al. Loss ofStat1 decreases megakaryopoiesis and favors erythropoiesis in a JAK2-V617F-driv-en mouse model of MPNs. Blood 2014;123(25):3943–50.
[130] Spivak JL, Considine M, Williams DM, Talbot Jr CC, Rogers O, Moliterno AR, et al.Two clinical phenotypes in polycythemia vera. N Engl J Med 2014;371(9):808–17.
[131] Guglielmelli P, Tozzi L, Bogani C, Iacobucci I, Ponziani V, Martinelli G, et al. Overex-pression of microRNA-16-2 contributes to the abnormal erythropoiesis in polycy-themia vera. Blood 2011;117(25):6923–7.
[132] Zhan H, Cardozo C, Yu W, Wang A, Moliterno AR, Dang CV, et al. MicroRNA dereg-ulation in polycythemia vera and essential thrombocythemia patients. Blood CellsMol Dis 2013;50(3):190–5.
[133] Stein BL, Williams DM, Wang NY, Rogers O, Isaacs MA, Pemmaraju N, et al. Sex dif-ferences in the JAK2 V617F allele burden in chronic myeloproliferative disorders.Haematologica 2010;95(7):1090–7.
K2V617F: Disease biology and current management strategies in16.11.001

16 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
[134] Spivak JL. The polycythemia vera stem cell. Leuk Suppl 2014;3(Suppl. 1):S23–4.[135] Soranzo N, Spector TD, Mangino M, Kuhnel B, Rendon A, Teumer A, et al. A ge-
nome-wide meta-analysis identifies 22 loci associated with eight hematologicalparameters in the HaemGen consortium. Nat Genet 2009;41(11):1182–90.
[136] Ganesh SK, Zakai NA, van Rooij FJ, Soranzo N, Smith AV, Nalls MA, et al. Multipleloci influence erythrocyte phenotypes in the CHARGE consortium. Nat Genet2009;41(11):1191–8.
[137] Nalls MA, Couper DJ, Tanaka T, van Rooij FJ, Chen MH, Smith AV, et al. Multiple lociare associated with white blood cell phenotypes. PLoS Genet 2011;7(6), e1002113.
[138] Li J, Glessner JT, Zhang H, Hou C, Wei Z, Bradfield JP, et al. GWAS of blood cell traitsidentifies novel associated loci and epistatic interactions in Caucasian and African-American children. Hum Mol Genet 2013;22(7):1457–64.
[139] Chambers JC, Zhang W, Li Y, Sehmi J, Wass MN, Zabaneh D, et al. Genome-wide as-sociation study identifies variants in TMPRSS6 associated with hemoglobin levels.Nat Genet 2009;41(11):1170–2.
[140] Benyamin B, Ferreira MA, Willemsen G, Gordon S, Middelberg RP, McEvoy BP, et al.Common variants in TMPRSS6 are associated with iron status and erythrocyte vol-ume. Nat Genet 2009;41(11):1173–5.
[141] Thiele J, Kvasnicka HM, Diehl V. Initial (latent) polycythemia vera withthrombocytosis mimicking essential thrombocythemia. Acta Haematol 2005;113(4):213–9.
[142] Passamonti F, Elena C, Schnittger S, Skoda RC, Green AR, Girodon F, et al. Molecularand clinical features of the myeloproliferative neoplasm associated with JAK2 exon12 mutations. Blood 2011;117(10):2813–6.
[143] Gnanasambandan K, Magis AT, Sayeski PP. A shift in the salt bridge interaction ofresidues D620 and E621 mediates the constitutive activation of Jak2-H538Q/K539L. Mol Cell Biochem 2012;367(1–2):125–40.
[144] Godfrey AL, Chen E, Massie CE, Silber Y, Pagano F, Bellosillo B, et al. STAT1 activa-tion in association with JAK2 exon 12 mutations. Haematologica 2016;101(1):e15–9.
[145] Beer PA, ErberWN, Campbell PJ, Green AR. How I treat essential thrombocythemia.Blood 2011;117(5):1472–82.
[146] Campbell PJ, Baxter EJ, Beer PA, Scott LM, Bench AJ, Huntly BJ, et al. Mutation ofJAK2 in the myeloproliferative disorders: timing, clonality studies, cytogenetic as-sociations, and role in leukemic transformation. Blood 2006;108(10):3548–55.
[147] Beer PA, Delhommeau F, LeCouedic JP, Dawson MA, Chen E, Bareford D, et al. Tworoutes to leukemic transformation after a JAK2 mutation-positive myeloprolifera-tive neoplasm. Blood 2010;115(14):2891–900.
[148] Beer PA, Ortmann CA, Stegelmann F, Guglielmelli P, Reilly JT, Larsen TS, et al. Mo-lecular mechanisms associated with leukemic transformation of MPL-mutant my-eloproliferative neoplasms. Haematologica 2010;95(12):2153–6.
[149] McMullin MF, Bareford D, Campbell P, Green AR, Harrison C, Hunt B, et al. Guide-lines for the diagnosis, investigation and management of polycythaemia/erythrocytosis. Br J Haematol 2005;130(2):174–95.
[150] Bench AJ, White HE, Foroni L, Godfrey AL, Gerrard G, Akiki S, et al. Molecular diag-nosis of the myeloproliferative neoplasms: UK guidelines for the detection of JAK2V617F and other relevant mutations. Br J Haematol 2013;160(1):25–34.
[151] Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016revision to the World Health Organization classification of myeloid neoplasms andacute leukemia. Blood 2016;127(20):2391–405.
[152] McMullin MF, Wilkins BS, Harrison CN. Management of polycythaemia vera: a crit-ical review of current data. Br J Haematol 2015;172(3):337–49.
[153] Johansson PL, Safai-Kutti S, Kutti J. An elevated venous haemoglobin concentrationcannot be used as a surrogate marker for absolute erythrocytosis: a study of pa-tients with polycythaemia vera and apparent polycythaemia. Br J Haematol 2005;129(5):701–5.
[154] Cassinat B, Laguillier C, Gardin C, de Beco V, Burcheri S, Fenaux P, et al. Classificationof myeloproliferative disorders in the JAK2 era: is there a role for red cell mass?Leukemia 2008;22(2):452–3.
[155] Spivak JL. Polycythemia vera: myths, mechanisms, and management. Blood 2002;100(13):4272–90.
[156] Spivak JL, Silver RT. The revised World Health Organization diagnostic criteria forpolycythemia vera, essential thrombocytosis, and primary myelofibrosis: an alter-native proposal. Blood 2008;112(2):231–9.
[157] Lamy T, Devillers A, Bernard M, Moisan A, Grulois I, Drenou B, et al. Inapparentpolycythemia vera: an unrecognized diagnosis. Am J Med 1997;102(1):14–20.
[158] Spivak JL. Polycythemia vera, the hematocrit, and blood-volume physiology. N EnglJ Med 2013;368(1):76–8.
[159] Barbui T, Thiele J, Gisslinger H, Finazzi G, Carobbio A, Rumi E, et al. Masked polycy-themia vera (mPV): results of an international study. Am J Hematol 2014;89(1):52–4.
[160] Barbui T, Thiele J, Carobbio A, Gisslinger H, Finazzi G, Rumi E, et al. Masked polycy-themia vera diagnosed according to WHO and BCSH classification. Am J Hematol2014;89(2):199–202.
[161] Lussana F, Carobbio A, Randi ML, Elena C, Rumi E, Finazzi G, et al. A lower intensityof treatment may underlie the increased risk of thrombosis in young patients withmasked polycythaemia vera. Br J Haematol 2014;167(4):541–6.
[162] Alvarez-Larran A, Angona A, Ancochea A, Garcia-Pallarols F, Fernandez C, LongaronR, et al. Masked polycythaemia vera: presenting features, response to treatmentand clinical outcomes. Eur J Haematol 2016;96(1):83–9.
[163] Barbui T, Thiele J, Carobbio A, Guglielmelli P, Rambaldi A, Vannucchi AM, et al. Dis-criminating between essential thrombocythemia andmasked polycythemia vera inJAK2 mutated patients. Am J Hematol 2014;89(6):588–90.
[164] Spivak JL, Silver RT. The revised World Health Organization diagnostic criteria forpolycythemia vera, essential thrombocytosis, and primary myelofibrosis: an alter-native proposal. Blood 2008;112(2):231–9.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
[165] Madelung AB, Bondo H, Stamp I, Loevgreen P, Nielsen SL, Falensteen A, et al. WorldHealth Organization-defined classification of myeloproliferative neoplasms: mor-phological reproducibility and clinical correlations–the Danish experience. Am JHematol 2013;88(12):1012–6.
[166] Ancochea A, Alvarez-Larran A, Morales-Indiano C, Garcia-Pallarols F, Martinez-Aviles L, Angona A, et al. The role of serum erythropoietin level and JAK2 V617F al-lele burden in the diagnosis of polycythaemia vera. Br J Haematol 2014;167(3):411–7.
[167] Passamonti F, Rumi E, Pungolino E, Malabarba L, Bertazzoni P, Valentini M, et al.Life expectancy and prognostic factors for survival in patients with polycythemiavera and essential thrombocythemia. Am J Med 2004;117(10):755–61.
[168] Tefferi A, Rumi E, Finazzi G, Gisslinger H, Vannucchi AM, Rodeghiero F, et al. Surviv-al and prognosis among 1545 patients with contemporary polycythemia vera: aninternational study. Leukemia 2013;27(9):1874–81.
[169] Marchioli R, Finazzi G, Landolfi R, Kutti J, Gisslinger H, Patrono C, et al. Vascular andneoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol2005;23(10):2224–32.
[170] Polycythemia vera: the natural history of 1213 patients followed for 20 yearsGruppo Italiano Studio PolicitemiaAnn Intern Med 1995;123(9):656–64.
[171] Landolfi R, Di Gennaro L, Barbui T, De Stefano V, Finazzi G, Marfisi R, et al. Leukocy-tosis as a major thrombotic risk factor in patients with polycythemia vera. Blood2007;109(6):2446–52.
[172] Pearson TC, Wetherley-Mein G. Vascular occlusive episodes and venoushaematocrit in primary proliferative polycythaemia. Lancet 1978;2(8102):1219–22.
[173] Barbui T, Finazzi G, Falanga A. Myeloproliferative neoplasms and thrombosis. Blood2013;122(13):2176–84.
[174] Berk PD, Goldberg JD, Donovan PB, Fruchtman SM, Berlin NI, Wasserman LR. Ther-apeutic recommendations in polycythemia vera based on Polycythemia Vera StudyGroup protocols. Semin Hematol 1986;23(2):132–43.
[175] Tartaglia AP, Goldberg JD, Berk PD, Wasserman LR. Adverse effects ofantiaggregating platelet therapy in the treatment of polycythemia vera. SeminHematol 1986;23(3):172–6.
[176] Marchioli R, Finazzi G, Specchia G, Cacciola R, Cavazzina R, Cilloni D, et al. Cardio-vascular events and intensity of treatment in polycythemia vera. N Engl J Med2013;368(1):22–33.
[177] Tefferi A. Polycythemia vera: a comprehensive review and clinical recommenda-tions. Mayo Clin Proc 2003;78(2):174–94.
[178] Wolanskyj AP, Schwager SM, McClure RF, Larson DR, Tefferi A. Essentialthrombocythemia beyond the first decade: life expectancy, long-term complica-tion rates, and prognostic factors. Mayo Clin Proc 2006;81(2):159–66.
[179] Campbell PJ, MacLean C, Beer PA, Buck G, Wheatley K, Kiladjian JJ, et al. Correlationof blood counts with vascular complications in essential thrombocythemia: analy-sis of the prospective PT1 cohort. Blood 2012;120(7):1409–11.
[180] Falanga A, Marchetti M, Vignoli A, Balducci D, Barbui T. Leukocyte-platelet interac-tion in patients with essential thrombocythemia and polycythemia vera. ExpHematol 2005;33(5):523–30.
[181] Gangat N, Wolanskyj AP, Schwager SM, Hanson CA, Tefferi A. Leukocytosis at diag-nosis and the risk of subsequent thrombosis in patients with low-risk essentialthrombocythemia and polycythemia vera. Cancer 2009;115(24):5740–5.
[182] Michiels JJ. Acquired von Willebrand disease due to increasing platelet count canreadily explain the paradox of thrombosis and bleeding in thrombocythemia.Clin Appl Thromb Hemost 1999;5(3):147–51.
[183] Kaifie A, Kirschner M, Wolf D, Maintz C, Hanel M, Gattermann N, et al. Bleeding,thrombosis, and anticoagulation in myeloproliferative neoplasms (MPN): analysisfrom the German SAL-MPN-registry. J Hematol Oncol 2016;9(1):18.
[184] Barbui T, Thiele J, Passamonti F, Rumi E, Boveri E, Randi ML, et al. Initial bone mar-row reticulin fibrosis in polycythemia vera exerts an impact on clinical outcome.Blood 2012;119(10):2239–41.
[185] Passamonti F, Rumi E, Caramella M, Elena C, Arcaini L, Boveri E, et al. A dynamicprognostic model to predict survival in post-polycythemia vera myelofibrosis.Blood 2008;111(7):3383–7.
[186] Kiladjian JJ, Chevret S, Dosquet C, Chomienne C, Rain JD. Treatment of polycythemiavera with hydroxyurea and pipobroman: final results of a randomized trial initiat-ed in 1980. J Clin Oncol 2011;29(29):3907–13.
[187] Kiladjian JJ, Gardin C, Renoux M, Bruno F, Bernard JF. Long-term outcomes of poly-cythemia vera patients treatedwith pipobroman as initial therapy. Hematol J 2003;4(3):198–207.
[188] Lundberg P, Karow A, Nienhold R, Looser R, Hao-Shen H, Nissen I, et al. Clonal evo-lution and clinical correlates of somaticmutations inmyeloproliferative neoplasms.Blood 2014;123(14):2220–8.
[189] Falanga A, Marchetti M. Thrombotic disease in the myeloproliferative neoplasms.Hematology Am Soc Hematol Educ Program 2012;2012:571–81.
[190] Landolfi R, Ciabattoni G, Patrignani P, Castellana MA, Pogliani E, Bizzi B, et al. In-creased thromboxane biosynthesis in patients with polycythemia vera: evidencefor aspirin-suppressible platelet activation in vivo. Blood 1992;80(8):1965–71.
[191] Landolfi R, Marchioli R, Kutti J, Gisslinger H, Tognoni G, Patrono C, et al. Efficacy andsafety of low-dose aspirin in polycythemia vera. N Engl J Med 2004;350(2):114–24.
[192] Patrono C, Rocca B, De Stefano V. Platelet activation and inhibition in polycythemiavera and essential thrombocythemia. Blood 2013;121(10):1701–11.
[193] Alvarez-Larrán A, Pereira A, Guglielmelli P, Hernández-Boluda JC, Arellano-RodrigoE, Ferrer-Marín F, et al. Antiplatelet therapy versus observation in low-risk essentialthrombocythemia with a CALR mutation. Haematologica 2016;101(8):926–31.
[194] Squizzato A, Romualdi E, Passamonti F, Middeldorp S. Antiplatelet drugs for polycy-thaemia vera and essential thrombocythaemia. Cochrane Database Syst Rev 2013;4, CD006503.
K2V617F: Disease biology and current management strategies in16.11.001

17J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
[195] Low-dose aspirin in polycythaemia vera: a pilot study Gruppo Italiano StudioPolicitemia (GISP)Br J Haematol 1997;97(2):453–6.
[196] Berk PD, Goldberg JD, Silverstein MN, Weinfeld A, Donovan PB, Ellis JT, et al. In-creased incidence of acute leukemia in polycythemia vera associated withchlorambucil therapy. N Engl J Med 1981;304(8):441–7.
[197] Treatment of polycythaemia vera by radiophosphorus or busulphan: a randomizedtrial “leukemia and Hematosarcoma” cooperative group, European Organizationfor Research on Treatment of Cancer (EORTC)Br J Cancer 1981;44(1):75–80.
[198] Brusamolino E, Salvaneschi L, Canevari A, Bernasconi C. Efficacy trial of pipobromanin polycythemia vera and incidence of acute leukemia. J Clin Oncol 1984;2(6):558–61.
[199] Passamonti F, Brusamolino E, Lazzarino M, Barate C, Klersy C, Orlandi E, et al. Effi-cacy of pipobroman in the treatment of polycythemia vera: long-term results in163 patients. Haematologica 2000;85(10):1011–8.
[200] Najean Y, Rain JD. Treatment of polycythemia vera: the use of hydroxyurea andpipobroman in 292 patients under the age of 65 years. Blood 1997;90(9):3370–7.
[201] Finazzi G, Caruso V, Marchioli R, Capnist G, Chisesi T, Finelli C, et al. Acute leukemiain polycythemia vera: an analysis of 1638 patients enrolled in a prospective obser-vational study. Blood 2005;105(7):2664–70.
[202] Donovan PB, Kaplan ME, Goldberg JD, Tatarsky I, Najean Y, Silberstein EB, et al.Treatment of polycythemia vera with hydroxyurea. Am J Hematol 1984;17(4):329–34.
[203] Cortelazzo S, Finazzi G, Ruggeri M, Vestri O, Galli M, Rodeghiero F, et al. Hydroxy-urea for patients with essential thrombocythemia and a high risk of thrombosis.N Engl J Med 1995;332(17):1132–6.
[204] Bjorkholm M, Derolf AR, Hultcrantz M, Kristinsson SY, Ekstrand C, Goldin LR, et al.Treatment-related risk factors for transformation to acute myeloid leukemia andmyelodysplastic syndromes in myeloproliferative neoplasms. J Clin Oncol 2011;29(17):2410–5.
[205] Hanft VN, Fruchtman SR, Pickens CV, Rosse WF, Howard TA, Ware RE. AcquiredDNA mutations associated with in vivo hydroxyurea exposure. Blood 2000;95(11):3589–93.
[206] Najean Y, Rain JD. Treatment of polycythemia vera: use of 32P alone or in combina-tion withmaintenance therapy using hydroxyurea in 461 patients N65 years of age.The French Polycythemia Study Group Blood. 1997;89(7):2319–27.
[207] Finazzi G, Ruggeri M, Rodeghiero F, Barbui T. Second malignancies in patients withessential thrombocythaemia treated with busulphan and hydroxyurea: long-termfollow-up of a randomized clinical trial. Br J Haematol 2000;110(3):577–83.
[208] Barosi G, Mesa R, Finazzi G, Harrison C, Kiladjian JJ, Lengfelder E, et al. Revised re-sponse criteria for polycythemia vera and essential thrombocythemia: an ELNand IWG-MRT consensus project. Blood 2013;121(23):4778–81.
[209] Alvarez-Larran A, Pereira A, Cervantes F, Arellano-Rodrigo E, Hernandez-Boluda JC,Ferrer-Marin F, et al. Assessment and prognostic value of the EuropeanLeukemiaNet criteria for clinicohematologic response, resistance, and intoleranceto hydroxyurea in polycythemia vera. Blood 2012;119(6):1363–9.
[210] Barosi G, Birgegard G, Finazzi G, Griesshammer M, Harrison C, Hasselbalch H, et al.A unified definition of clinical resistance and intolerance to hydroxycarbamide inpolycythaemia vera and primary myelofibrosis: results of a European LeukemiaNet(ELN) consensus process. Br J Haematol 2010;148(6):961–3.
[211] Massaro P, Foa P, Pomati M, LaTargia ML, Iurlo A, Clerici C, et al. Polycythemia veratreated with recombinant interferon-alpha 2a: evidence of a selective effect on themalignant clone. Am J Hematol 1997;56(2):126–8.
[212] Kiladjian JJ, Cassinat B, Chevret S, Turlure P, Cambier N, Roussel M, et al. Pegylatedinterferon-alfa-2a induces complete hematologic and molecular responses withlow toxicity in polycythemia vera. Blood 2008;112(8):3065–72.
[213] Silver RT, Vandris K, Goldman JJ. Recombinant interferon-alpha may retard pro-gression of early primary myelofibrosis: a preliminary report. Blood 2011;117(24):6669–72.
[214] Kiladjian JJ, Chomienne C, Fenaux P. Interferon-alpha therapy in bcr-abl-negativemyeloproliferative neoplasms. Leukemia 2008;22(11):1990–8.
[215] Kuriakose E, Vandris K, Wang YL, Chow W, Jones AV, Christos P, et al. Decrease inJAK2 V617F allele burden is not a prerequisite to clinical response in patientswith polycythemia vera. Haematologica 2012;97(4):538–42.
[216] Quintas-Cardama A, Kantarjian H, Manshouri T, Luthra R, Estrov Z, Pierce S, et al.Pegylated interferon alfa-2a yields high rates of hematologic and molecular re-sponse in patients with advanced essential thrombocythemia and polycythemiavera. J Clin Oncol 2009;27(32):5418–24.
[217] Hasan S, Cassinat B, Droin N, Le Couedic JP, Favale F, Monte-Mor B, et al. Use of the46/1 haplotype to model JAK2(V617F) clonal architecture in PV patients: clonalevolution and impact of IFNalpha treatment. Leukemia 2014;28(2):460–3.
[218] Kiladjian JJ, Masse A, Cassinat B,Mokrani H, Teyssandier I, le Couedic JP, et al. Clonalanalysis of erythroid progenitors suggests that pegylated interferon alpha-2a treat-ment targets JAK2V617F clones without affecting TET2 mutant cells. Leukemia2010;24(8):1519–23.
[219] Quintas-Cardama A, Abdel-Wahab O, Manshouri T, Kilpivaara O, Cortes J, RoupieAL, et al. Molecular analysis of patients with polycythemia vera or essentialthrombocythemia receiving pegylated interferon alpha-2a. Blood 2013;122(6):893–901.
[220] Ahn IE, Natelson E, Rice L. Successful long-term treatment of Philadelphia chromo-some-negative myeloproliferative neoplasms with combination of hydroxyureaand anagrelide. Clin Lymphoma Myeloma Leuk 2013;13(Suppl. 2):S300–4.
[221] Verstovsek S, Passamonti F, Rambaldi A, Barosi G, Rosen PJ, Rumi E, et al. A phase 2study of ruxolitinib, an oral JAK1 and JAK2 inhibitor, in patients with advancedpolycythemia vera who are refractory or intolerant to hydroxyurea. Cancer 2014;120(4):513–20.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
[222] Andersen CL, McMullin MF, Ejerblad E, Zweegman S, Harrison C, Fernandes S, et al.A phase II study of vorinostat (MK-0683) in patients with polycythaemia vera andessential thrombocythaemia. Br J Haematol 2013;162(4):498–508.
[223] Guerini V, Barbui V, Spinelli O, Salvi A, Dellacasa C, Carobbio A, et al. The histonedeacetylase inhibitor ITF2357 selectively targets cells bearing mutatedJAK2(V617F). Leukemia 2008;22(4):740–7.
[224] Rambaldi A, Dellacasa CM, Finazzi G, Carobbio A, Ferrari ML, Guglielmelli P, et al. Apilot study of the histone-deacetylase inhibitor givinostat in patients withJAK2V617F positive chronic myeloproliferative neoplasms. Br J Haematol 2010;150(4):446–55.
[225] Finazzi G, Vannucchi AM, Martinelli V, Ruggeri M, Nobile F, Specchia G, et al. Aphase II study of givinostat in combination with hydroxycarbamide in patientswith polycythaemia vera unresponsive to hydroxycarbamide monotherapy. Br JHaematol 2013;161(5):688–94.
[226] Baerlocher GM, Oppliger Leibundgut E, Ottmann OG, Spitzer G, Odenike O,McDevitt MA, et al. Telomerase inhibitor Imetelstat in patients with essentialthrombocythemia. N Engl J Med 2015;373(10):920–8.
[227] Tefferi A, Lasho TL, Begna KH, Patnaik MM, Zblewski DL, Finke CM, et al. A pilotstudy of the telomerase inhibitor Imetelstat for myelofibrosis. N Engl J Med2015;373(10):908–19.
[228] Mesa RA, Schwager S, Radia D, Cheville A, Hussein K, Niblack J, et al. The myelofi-brosis symptom assessment form (MFSAF): an evidence-based brief inventory tomeasure quality of life and symptomatic response to treatment in myelofibrosis.Leuk Res 2009;33(9):1199–203.
[229] Emanuel RM, Dueck AC, Geyer HL, Kiladjian JJ, Slot S, Zweegman S, et al. Myelopro-liferative neoplasm (MPN) symptom assessment form total symptom score: pro-spective international assessment of an abbreviated symptom burden scoringsystem among patients with MPNs. J Clin Oncol 2012;30(33):4098–103.
[230] Mesa R, Verstovsek S, Kiladjian JJ, Griesshammer M, Masszi T, Durrant S, et al.Changes in quality of life and disease-related symptoms in patients with polycy-themia vera receiving ruxolitinib or standard therapy. Eur J Haematol 2016;97(2):192–200.
[231] Mesa R, Vannucchi AM, Yacoub A, Zachee P, Garg M, Lyons R, et al. The efficacy andsafety of continued hydroxyurea therapy versus switching to ruxolitinib in patientswith polycythemia vera: a randomized, double-blind, double-dummy, symptomstudy (RELIEF). Blood. 124(21):3168–8.
[232] Saini KS, PatnaikMM, Tefferi A. Polycythemia vera-associated pruritus and its man-agement. Eur J Clin Invest 2010;40(9):828–34.
[233] Lengfelder E, Berger U, Hehlmann R. Interferon alpha in the treatment of polycy-themia vera. Ann Hematol 2000;79(3):103–9.
[234] Griesshammer M, Struve S, Barbui T. Management of Philadelphia negative chronicmyeloproliferative disorders in pregnancy. Blood Rev 2008;22(5):235–45.
[235] Robinson S, Bewley S, Hunt BJ, Radia DH, Harrison CN. The management and out-come of 18 pregnancies in women with polycythemia vera. Haematologica 2005;90(11):1477–83.
[236] Royal college of obstetricians and gynaecologists. Reducing the risk of venousthromboembolism during pregnancy and the puerperium. Green-top Guideline;2015[No 37a].
[237] SekharM,McVinnie K, Burroughs AK. Splanchnic vein thrombosis inmyeloprolifer-ative neoplasms. Br J Haematol 2013;162(6):730–47.
[238] Vannucchi AM. How I treat polycythemia vera. Blood 2014;124(22):3212–20.[239] Barbui T, Barosi G, Birgegard G, Cervantes F, Finazzi G, Griesshammer M, et al. Phil-
adelphia-negative classical myeloproliferative neoplasms: critical concepts andmanagement recommendations from European LeukemiaNet. J Clin Oncol 2011;29(6):761–70.
[240] Oh ST, Simonds EF, Jones C, Hale MB, Goltsev Y, Gibbs Jr KD, et al. Novel mutationsin the inhibitory adaptor protein LNK drive JAK-STAT signaling in patients withmyeloproliferative neoplasms. Blood 2010;116(6):988–92.
[241] Lasho TL, Pardanani A, Tefferi A. LNK mutations in JAK2 mutation-negativeerythrocytosis. N Engl J Med 2010;363(12):1189–90.
[242] Pardanani A, Lasho T, Finke C, Oh ST, Gotlib J, Tefferi A. LNK mutation studies inblast-phase myeloproliferative neoplasms, and in chronic-phase disease withTET2, IDH, JAK2 or MPL mutations. Leukemia 2010;24(10):1713–8.
[243] Tefferi A, Pardanani A, Lim KH, Abdel-Wahab O, Lasho TL, Patel J, et al. TET2 muta-tions and their clinical correlates in polycythemia vera, essential thrombocythemiaand myelofibrosis. Leukemia 2009;23(5):905–11.
[244] Abdel-Wahab O, Mullally A, Hedvat C, Garcia-Manero G, Patel J, Wadleigh M, et al.Genetic characterization of TET1, TET2, and TET3 alterations in myeloid malignan-cies. Blood 2009;114(1):144–7.
[245] Abdel-Wahab O, Pardanani A, Rampal R, Lasho TL, Levine RL, Tefferi A. DNMT3Amutational analysis in primary myelofibrosis, chronic myelomonocytic leukemiaand advanced phases of myeloproliferative neoplasms. Leukemia 2011;25(7):1219–20.
[246] Stegelmann F, Bullinger L, Schlenk RF, Paschka P, Griesshammer M, Blersch C, et al.DNMT3A mutations in myeloproliferative neoplasms. Leukemia 2011;25(7):1217–9.
[247] Brecqueville M, Rey J, Bertucci F, Coppin E, Finetti P, Carbuccia N, et al. Mutationanalysis of ASXL1, CBL, DNMT3A, IDH1, IDH2, JAK2, MPL, NF1, SF3B1, SUZ12, andTET2 in myeloproliferative neoplasms. Genes Chromosomes Cancer 2012;51(8):743–55.
[248] Stein BL, Williams DM, O'Keefe C, Rogers O, Ingersoll RG, Spivak JL, et al. Disruptionof the ASXL1 gene is frequent in primary, post-essential thrombocytosis and post-polycythemia vera myelofibrosis, but not essential thrombocytosis or polycythe-mia vera: analysis of molecular genetics and clinical phenotypes. Haematologica2011;96(10):1462–9.
K2V617F: Disease biology and current management strategies in16.11.001

18 J. Grinfeld, A.L. Godfrey / Blood Reviews xxx (2016) xxx–xxx
[249] Abdel-Wahab O, Pardanani A, Patel J,WadleighM, Lasho T, Heguy A, et al. Concom-itant analysis of EZH2 and ASXL1 mutations in myelofibrosis, chronicmyelomonocytic leukemia and blast-phase myeloproliferative neoplasms. Leuke-mia 2011;25(7):1200–2.
[250] Carbuccia N, Murati A, Trouplin V, Brecqueville M, Adelaide J, Rey J, et al. Mutationsof ASXL1 gene in myeloproliferative neoplasms. Leukemia 2009;23(11):2183–6.
[251] Lasho TL, Jimma T, Finke CM, Patnaik M, Hanson CA, Ketterling RP, et al. SRSF2 mu-tations in primary myelofibrosis: significant clustering with IDH mutations and in-dependent association with inferior overall and leukemia-free survival. Blood2012;120(20):4168–71.
[252] Zhang SJ, Rampal R,Manshouri T, Patel J, Mensah N, Kayserian A, et al. Genetic anal-ysis of patients with leukemic transformation of myeloproliferative neoplasmsshows recurrent SRSF2 mutations that are associated with adverse outcome.Blood 2012;119(19):4480–5.
[253] Voso MT, Fabiani E, Fianchi L, Falconi G, Criscuolo M, Santangelo R, et al. Mutationsof epigenetic regulators and of the spliceosome machinery in therapy-related my-eloid neoplasms and in acute leukemias evolved from chronic myeloproliferativediseases. Leukemia 2013;27(4):982–5.
[254] Brecqueville M, Rey J, Devillier R, Guille A, Gillet R, Adelaide J, et al. Array compar-ative genomic hybridization and sequencing of 23 genes in 80 patients with mye-lofibrosis at chronic or acute phase. Haematologica 2014;99(1):37–45.
[255] Ernst T, Chase AJ, Score J, Hidalgo-Curtis CE, Bryant C, Jones AV, et al. Inactivatingmutations of the histone methyltransferase gene EZH2 in myeloid disorders. NatGenet 2010;42(8):722–6.
Please cite this article as: Grinfeld J, Godfrey AL, After 10years of JApolycythaemia vera, Blood Rev (2016), http://dx.doi.org/10.1016/j.blre.20
[256] Guglielmelli P, Biamonte F, Score J, Hidalgo-Curtis C, Cervantes F, Maffioli M, et al.EZH2 mutational status predicts poor survival in myelofibrosis. Blood 2011;118(19):5227–34.
[257] Schnittger S, Bacher U, Eder C, Dicker F, Alpermann T, Grossmann V, et al. Molecularanalyses of 15,542 patients with suspected BCR-ABL1-negative myeloproliferativedisorders allow to develop a stepwise diagnostic workflow. Haematologica 2012;97(10):1582–5.
[258] Schnittger S, Bacher U, Alpermann T, Reiter A, Ulke M, Dicker F, et al. Use of CBLexon 8 and 9 mutations in diagnosis of myeloproliferative neoplasms andmyelodysplastic/myeloproliferative disorders: an analysis of 636 cases.Haematologica 2012;97(12):1890–4.
[259] Makishima H, Cazzolli H, Szpurka H, Dunbar A, Tiu R, Huh J, et al. Mutations of e3ubiquitin ligase cbl family members constitute a novel common pathogenic lesionin myeloid malignancies. J Clin Oncol 2009;27(36):6109–16.
[260] Tefferi A, Lasho TL, Abdel-Wahab O, Guglielmelli P, Patel J, Caramazza D, et al. IDH1and IDH2 mutation studies in 1473 patients with chronic-, fibrotic- or blast-phaseessential thrombocythemia, polycythemia vera or myelofibrosis. Leukemia 2010;24(7):1302–9.
[261] Pardanani A, Lasho TL, Finke CM, Mai M, McClure RF, Tefferi A. IDH1 and IDH2mu-tation analysis in chronic- and blast-phase myeloproliferative neoplasms. Leuke-mia 2010;24(6):1146–51.
[262] Papaemmanuil E, Cazzola M, Boultwood J, Malcovati L, Vyas P, Bowen D, et al. So-matic SF3B1mutation inmyelodysplasia with ring sideroblasts. N Engl J Med 2011;365(15):1384–95.
K2V617F: Disease biology and current management strategies in16.11.001