Embed Size (px)
Citation preview

1
PART 1 AGENDA ITEM 6
Title of Board paper
Chief Executive’s Report
Board meeting date 31 July 2014
Purpose
To draw the Board’s attention to key issues
Actions Recommended
Discussion / Noting / Decision
Publication
This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms None
Any communications actions after the meeting
None
Report of Karen James
Paper prepared by Tom Neve

2
Quarter 1 Monitor Submission
The Trust has to make its Quarter 1 In-Year Submissions to Monitor by the end of
July 2014 covering:
- A declaration of risks against healthcare targets and indicators for 2014/15
- An In-Year governance statement from the Board
Information about Board changes and Governor elections will be reported to reflect
the recent Executive Director appointments and the most recent public Governor
election.
The declaration of risks against healthcare targets and indicators for 2014/15 will
reflect that the trust was unable to complete the submission for incomplete RTT
pathways.
The submission will also reflect that the Trust remains in Special Measures.
The Trust is complaint with all other targets and standards in respect of quarter 1.
An In-Year Governance statement from the board is required and the board is
required to respond “confirmed” or “not confirmed” to the following statements:
The board anticipates that the trust will continue to maintain a Continuity of Service
risk rating of at least 3 over the next 12 months.
The board is asked to approve a “not confirmed” response.
For governance, that:
The board is satisfied that plans in place are sufficient to ensure on going
compliance with all existing targets (after the application of thresholds) as set out in
Appendix A of the Risk Assessment Framework; and a commitment to comply with
all known targets going forward.
In light of the trust’s not being in a position to submit data for incomplete RTT
pathways, the board is asked to approve a “not confirmed” response.
Otherwise:
The board confirms that there are no matters arising in the quarter requiring an
exception report to Monitor (per the Risk Assessment Framework page 21, diagram
6) which have not already been reported.
The board is asked to approve a “confirmed” response.

3
Plans to encourage the recovery of migrant NHS healthcare costs.
The department has announced plans to help the NHS to recover more of the costs
of migrant and visitor healthcare.
Some patients from outside Europe using the NHS will be charged 150% of the cost
of treatment under new incentives for the NHS to recover costs from visitors and
migrants using the NHS. Visitors and migrants can currently get free NHS care
immediately or soon after arrival in the UK. The government is now asking the NHS
to identify these patients more effectively so costs can be recovered from them.
This will make sure that by the middle of the next parliament, the NHS will recover
up to £500 million a year from treating foreign visitors and migrants.
In June it was revealed that the NHS will receive and extra 25% on top of the cost of
every procedure they perform for an European Economic Area (EAA) migrant visitor
with a European Health Insurance Card (EHIC). A non-EAA visitor will be charged
for their care plus an extra 50%.
Steps are being taken to help the NHS charge more effectively and consistently and
a clear timetable is being issued and a new National Intensive Support Team will be
on hand to assist.
Financial sanctions will be put in place for trusts who fail to identify and bill
chargeable patients.
Requirements for registration with the Care Quality Commission
The Department of Health has published a combined response to three separate
consultations recently undertaken:
• Introducing fundamental standards: consultation on proposals to change
CQC registration regulations
• Consultation on the fit and proper persons test
• Introducing the statutory Duty of Candour
Following these consultations, the DH has decided to introduce these measures in
the following sequence:
• The Duty of Candour will be introduced for NHS bodies only in October 2014
• The fit and proper persons requirement will be introduced for NHS bodies
only in October 2014
• The fundamental standards will be introduced for all providers in April 2015.
• The Duty of Candour and fit and proper persons requirements will be
extended to all CQC registered providers from April 2015

4
Further detail of what is included in these measures can be found in the Department
of Health’s publication Requirements for registration with the Care Quality
Commission published in July 2014.
Sign up to Safety
Sign up to Safety is a new national patient safety strategy campaign. Launched on
24 June 2014 with the mission to strengthen patient safety in the NHS and make it
the safest healthcare system in the world.
Organisations and individuals who sign up to the campaign commit to setting out
actions they will undertake in response to the following five pledges
1. Put safety first. Commit to reduce avoidable harm in the NHS by half and
make public the goals and plans developed locally.
2. Continually learn. Make their organisations more resilient to risks, by acting
on the feedback from patients and by constantly measuring and monitoring
how safe their services are.
3. Honesty. Be transparent with people about their progress to tackle patient
safety issues and support staff to be candid with patients and their families if
something goes wrong.
4. Collaborate. Take a leading role in supporting local collaborative learning, so
that improvements are made across all of the local services that patients use.
5. Support. Help people understand why things go wrong and how to put them
right. Give staff the time and support to improve and celebrate the progress.
A National Co-ordinating and Support Group has been established, chaired by Sir
David Dalton who is supported by Dr Suzette Woodward as Campaign Director.
This Trust will be signing up to the campaign and the organisation will commit to
strengthening patient safety by:
• Setting out the actions it will undertake in response to the five Sign up to
Safety pledges and agree to publish this on the website for staff, patients and
the public to see.
• Commit to turn the trust’s actions into a safety improvement plan which will
indicate how this organisation intends to save lives and reduce harm for
patients over the next 3 years.

5
NHS England Launches Integrated Personal Commissioning (IPC)
Simon Stevens the CEO of the NHS has set out plans for a new Integrated
Personal Commissioning (IPC) programme. Speaking recently at a Local
Government Association conference he stated that high-need individuals are to be
offered the ability to control their own blended NHS and community care, in
partnership with voluntary sector.
The NHS will offer local councils across England a radical new option in which
individuals could control their combined health and social care support.
Four groups of high-need individuals are likely to be included in the first wave from
next April 2015, although councils, voluntary organisations, and NHS clinical
commissioning groups may also propose others. These are:
• people with long term conditions, including frail elderly people at risk of care
home admission
• children with complex needs
• people with learning disabilities, and
• people with severe and enduring mental health problems.
At the same time, voluntary/Third Sector organisations will be commissioned locally
to support personal care planning, advocacy and service ‘brokerage’ for these
individuals enrolled in the IPC programme.
This new approach builds upon, but is in addition to, the joint work now under way
locally on the Better Care Fund.
Under the new IPC programme, a combined NHS and social care funding
endowment will be created based on each individual’s annual care needs. This will
blend funds contributed from local authorities and NHS commissioners (CCGs and
NHS England). Individuals enrolled in the programme will be able to decide how
much personal control to assume over how services are commissioned and
arranged on their behalf.
NHS care will in all cases remain free at the point of use, and available according to
individual need.
NHS England will now work with partners in local government, CCGs, patient
groups and the voluntary sector to develop an IPC Prospectus which will be
published at the end of July. This will formally invite local expressions of interest in
jointly developing and participating in the IPC programme from April 2015.

6
NHS England will provide technical support to develop projects, and fund
independent evaluation. Wider scale rollout of successful projects is envisaged from
2016/17.
The Friends and Family Test for Staff Introduction NHS England announced earlier this year that all NHS organisations providing acute, community, ambulance and mental health services are required to implement the Staff Friends and Family Test (FFT) between 1 April and 30 June 2014. The FFT for Staff asks how likely staff are to recommend the services they have received, or work in, to friends and family who need similar treatment or care to that which they have received or deliver. Implementation All staff must have at least one opportunity to complete per year. The Trust has taken the opportunity to include an additional 23 questions around our values and behaviours. The Results
Q1 2014
Description Target %
Q1 2014
1 How likely are you to recommend this organisation to friends and family if they needed care or treatment?
67 77
2 How likely are you to recommend this organisation to friends and family as a place to work?
61 71
5 I work in a clean, safe environment. 0 90
6 Staff at this Trust take responsibility for all the things that they do.
0 64
7 Staff at this Trust are confident to challenge others to improve standards.
0 62
8 Safety and quality are extremely important to all staff at this Trust.
0 73
9 Staff at this Trust are always caring and compassionate. 0 71
10 Staff at this Trust always offer and show comfort, support and understanding.
0 71
11 I always involve patients and their relatives in their care. 0 74
12 The Trust cares about staff and their welfare. 0 58
13 Staff at this Trust respect privacy and confidentiality at all 0 80

7
times.
14 The Trust promotes and encourages my learning. 0 63
15 I motivate myself. 0 97
16 I try to help other colleagues develop. 0 96
17 In my team we recognise and celebrate achievements. 0 75
18 In my team we learn from incidents, complaints and compliments received.
0 90
19 Staff at this Trust are always recognised, valued and respected.
0 44
20 All staff and patients are treated with dignity and kindness at the Trust.
0 63
21 Staff at this Trust are always polite and professional. 0 68
22 The Trust encourages staff to actively listen to patients, their relatives, carers and colleagues
0 83
23 Staff at this Trust are always open and honest. 0 60
24 The Trust encourages and welcomes feedback from staff and patients.
0 83
25 I know what the Trust’s priorities are. 0 85
26 I know how well the Trust is performing. 0 79
27 I know how my role contributes to the success of the Trust. 0 87
Staff awards 2014 As many of you will be aware, we held this year’s staff awards on the 11th July 2014. Unlike previous years, we hired, thanks to our sponsors, the summer marquee at the Village Hotel in Ashton-under-Lyne – just to make it that little bit special. Our staff certainly weren’t disappointed on the night. The venue looked fabulous with over 250 members of staff, partners and sponsors attending the evening, it was a roaring success. All the ladies wore dinner dresses and the gentlemen wore suits and tuxedos, everybody looked wonderful. The awards were closely followed by a summer disco in the marquee for all staff, where they had the opportunity to let their hair down after a very challenging year for the hospital. I want to pay a special tribute to all of our finalists and winners on the evening. They have all gone the extra mile over the last 12 months and fully deserved their recognition on the night. It is this kind of dedication and commitment to the hospital which gives our patients an excellent service. Well done to all.
CQC Report
We are obviously disappointed with the “Inadequate” rating given to the trust arising
out of the CQC inspection in May 2014. The report does however acknowledge a
number of examples of excellent care and the significant and positive change in the

8
culture of the organisation. The trust will remain in special measures until it is re-
inspected towards the end of the calendar year. An action plan is being developed
to address the remaining concerns of the CQC in order to ensure it is removed from
special measures.

Page 1
PART 1
AGENDA ITEM 7
Title of Board paper
Improvement Update
Board meeting date 31st July 2014
Purpose
The purpose of this paper is to update the Board on the future monitoring arrangements for the actions that were determined from the following reviews: Deanery Change Plan July 2013 Keogh Responsive Review Change Plan Recovery Plan based on The ECIST & GMUMT Reviews at TFT April 2013 Monitor Letter on 2nd July 2013 CQC July 2103 CQC May 2014
Actions Recommended
Discussion / Noting / Decision
Publication This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms
ICPA – Improvement Central Action Plan KPIs – Key Performance Indicators MAU – Medical Assessment Unit UHSM – University Hospital of South Manchester CIP – Cost Improvement Programme KPI- Key Performance Indicator SPC- Statistical Process Charts PMO- Project Management Office BAF-Board Assurance Framework QIA-Quality Impact Assessment CQUIN-Commissioning for Quality and Innovation
Any communications actions after the meeting
The content of this report will be communicated to external stakeholders.
Report of Karen James Interim Chief Executive
Paper prepared by Naomi Ledwith Programme Director Improvement

Page 2
Tameside Hospital NHS Foundation Trust
Keogh Update
1. Background
The Board has been receiving monthly reports on the Improvement Central Action Plan (ICPA) since October 2013. The ICAP was created to allow the Trust to articulate the Improvement Strategy, in response to the reviews listed below, and to align business to that strategy.
• Deanery Action Plan July 2013
• Keogh Responsive Review Change Plan
• Recovery Plan based on The ECIST & GMUMT Reviews at TFT April 2013
• Monitor Letter on 2nd July 2013
• CQC Inspection visit July 2103 In recognition of the importance of the programme the ICAP has been delivered and monitored through its own bespoke governance structure; both internally within the Trust and externally to the Clinical Commissioning Group (CCG). The ICAP is delivered and monitored through the Improvement Board, which is accountable to the Trust Board. The Improvement Board provides assurance to the Clinical Commissioning Group (CCG) through reports to the monthly Trust/CCG Interface meeting and attendance, by the Trust, to the CCG Quality Committee. The Improvement Board also provides assurance to Monitor via the submission of monthly progress reports on the ICAP. In addition updates are provided to the Health and Wellbeing Board.
2. Refresh of Improvement Central Action The May 2014 Care Quality Committee (CQC) Inspection recognised that the Trust is on a journey and significant improvement has been made in the 10 months since the Keogh review. The majority of the actions within the ICAP have been delivered; therefore it is appropriate to refresh the plan to reflect the recent CQC inspection ensuring that we continue to look forward on our improvement journey. The proposal is that the work streams within this plan continue to be monitored through the Improvement Board and reported to the Trust Board on a monthly basis, for the time that the Trust remains in Special Measures. The Programme Management Office will act as the delivery unit for the RICAP working with the transformational, clinical, governance, managerial and operational teams within the Trust to ensure delivery. The RICAP will be closely linked to the Board Assurance Framework and be reported on through a risk based approach. See Appendix 1 for the Governance Structure. The Board should expect to receive a report on progress against the RICAP at the August 2014 meeting.

Page 3
3. Historic Improvement Central Action Plan
In the time that the ICAP governance structure has been operational, the CCG’s and the Trust’s governance structures have both matured significantly. Therefore it has been recommended by the Improvement Board that those historic ICAP actions that have been delivered (ie Green or Blue), and that are not recommended for improvement in the CQC report will be monitored on an on-going basis through core governance process from August 2014. Internally within the Trust historic ICAP actions will be reported on a risk based approach through the Board Assurance Framework (BAF). The CCG will seek assurance from the Trust through the Performance and Quality Contract Groups. 5. Conclusion The key to ensuring permanent change and a culture of continuous improvement is to enable operational and clinical staff to take ownership for improvement and monitoring. Transferring the monitoring of delivered historic ICAP actions to core governance will encourage ownership and delivery within divisions, directorates and wards. Maintaining focus on the key actions recommend by CQC in July 2014 will continue to be managed through the PMO Delivery Unit. The Trust’s Service Transformation team is also currently being enhanced to create the additional capacity required to secure the pace of change that is required over the next ten to twelve months. A more detailed report which outlines the approach and plan to deliver the on-going service transformation and operational improvements will be submitted to the August Board meeting.

Page 4
Appendix 1 Refreshed ICAP Governance Structure

PART 1 AGENDA ITEM 8
Title of Board paper Integrated Quality Report : June 2014
Board meeting date 31st July 2014
Purpose The Board is asked to review current performance
Actions Recommended
Discussion / Noting / Decision
Publication This paper will be published under the THFT publication scheme
Unusual acronyms
ADT Admission, Discharge, Transfer C DIFF Clostridium difficile CIP Cost Improvement Plan CQC Care Quality Commission CT Computerised Tomography CWT Cancer Waiting Times DNA Did-not-Attend DPH Director of Public Health FFT Friends & Family Test GMCCN Greater Manchester & Cheshire Cancer Network HSMR Hospital Standardised Mortality Ratio HAS Hospital Arrival Screen MRSA Methicillin-resistant staphylococcus aureus MSA Mixed-sex Accommodation RAMI Risk-adjusted Mortality Index RCA Root Cause Analysis RIDDOR Reporting of Injuries, Diseases and Dangerous Occurrences Regulations RTT Referral-to-Treatment SHMI Summary Hospital-level Mortality Indicator STAR Staff Accident Rate
StEIS Strategic Executive Information System
TIA Transient Ischaemic Attack
VTE Venous Thromboembolism
YTD Year-to-Date
Any communication actions after meeting
None
Report of
Trish Cavanagh, Director of Operations Brendan Ryan, Medical Director John Goodenough, Director of Nursing Amanda Bromley, Director of HR Barbara Herring, Director of Finance
Paper prepared by Kay Holland, Deputy Chief Operating Officer

Page 2 QUALITY ACCOUNT: July 2014 Board (June 2014 performance)
Board of Directors’ Meeting: 31st July 2014
Quality Account 2014/15 Contents Introduction 3 Quality Dashboard June 2014/15 4 Exception Reports Director of Operations
Readmission 5
RTT- 18 Week incomplete pathways 6
Outpatient slot utilisation 7
Outpatient Did-Not-Attend (DNA) rate 7
Theatre Utilisation 8
Stroke 9
Director of Nursing
Nutrition Risk Assessment 10
Director of Human Resources
Staff Attendance 11
Appraisals (rolling 12 months) 11
Trust induction 11
Mandatory Training compliance 11

Page 3 QUALITY ACCOUNT: July 2014 Board (June 2014 performance)
Quality Account Report – June 2014 Performance
Introduction
The Quality Account report provides the Trust Board with an overview of the Trusts performance across a range of quality and operational indicators for the month of June 2014 and year to date performance, along with a RAG rating of performance to support the Board in evaluating how the Trust is performance against each indicator.
Exception Reports
Alongside the Quality and Performance Dashboard, the report includes exception reports which responds to the performance data and will allow the Executive team and Trust Board to be assured of and contribute to plans to rectify performance and quality issues.
June Performance
The issue previously reported to Board around consistency of compliance with standard operating procedures and their impact on tracking 18 week performance continues, specifically in relation to incomplete pathways. An RTT validation team have been appointed who are systematically working through the issues. We have been unable to report our compliance with the incomplete pathway indicator and have discussed the issues with both Monitor and the Health & Social Care Information Centre and an exception report is provided to inform the Board of the issues and actions.
NHS England requires all Trusts to reduce the number of patients waiting longer than 18 weeks during July and August even if it results in a dip in monthly performance; the one month forecast for July has been amended to reflect this requirement.
Recommendation
The Trust Board is asked to review the quality and performance standards noted in the Quality Account.

Page 4
THFT Quality Dashboard June 2014/15
* Governance indicators, which appear in Monitor's Compliance Framework
Target Actual 4-mth Actual Current 1-mth Target Actual 4-mth Actual Current 1-mth Target Actual 4-mth Actual Current 1-mth
14/15 YTD Trend Month Period F'cast 14/15 YTD Trend Month Period F'cast 14/15 YTD Trend Month Period F'cast
Mortality Stroke Waiting times
≤100 91.2 NA ≥90% 90.17% 90.10%
SHMI (rolling 12 months)# ≤100 NA ≥95% 97.26% 98.11%
Infection Prevention & Control ≥80% 77.50% 73.91% ≥92% - -
0 0 0 RTT waits (>52 weeks) 0 0 0
41 9 2 ≤1% 0.50% 0.36%
NHS Safety Thermometer A&E
N/A 96.99% 95.91% Target Actual 4-mth Actual Current 1-mth ≥95% 95.40% 94.55%
≥95% 99.43% 100.00% 14/15 YTD Trend Month Period F'cast Trolley waits in A&E (>12 hrs) 0 0 0
Patient Safety 0 4 0 HAS compliance ≥95% 76.06% 74.03%
≥95% 95.42% 96.97% Cancer
93% 98.50% 97.34%
NA 101 0 NA NA 93% 100.00% 100.00%
≥90% 91.26% 79.31% 96% 98.18% 96.00%
Staff accident rate# 94% 100.0% 100.00%
(STAR) 98% 100.0% 100.0%
0 0 0 85% 86.89% 88.57%
0 12 2 Target Actual 4-mth Actual Current 1-mth 85% 92.86% 89.47%
0 0 0 14/15 YTD Trend Month period F'cast
0 0 0 ≥96.6% 95.37% 95.20% Target Actual 4-mth Actual Current 1-mth
0 2 1 ≥95% N/A 83.60% 14/15 YTD Trend Month Period F'cast
Moves after 11pm (% of Admissions) NA 3.13% 2.70% NA - ≥95% N/A 96.60% ≥85% 68.57% 68.74%
Safer Staffing ≥95% N/A 86.60% ≤7.5% 11.05% 11.51%
TBA 93.08% 93.63% ≥85% 71.43% 73.09%
TBA 113.16% 114.95% Target Actual 4-mth Actual Current 1-mth ≤0.8% 0.77% 0.55%
14/15 YTD Trend Month Period F'cast
Target Actual 4-mth Actual Current 1-mth Green R - NA R -
14/15 YTD Trend Month Period F'cast 3 1 - NA 1 -
0 0 0 None 8 - NA 8 - Actual 4-mth Actual Current Yr-end
FFT Net Promoter Score 50 48 47 YTD Trend Month Period F'cast
FFT positive responses NA 87.21% 87.19% NA - Cum. Net surplus (£'m) -7161 -2,109 -17500
FFT response rate 15% 29.38% 35.36% strong improvement Cum. CIP (% of plan) 90.6% 96.8% 100%
Complaints received N/A 113 39 NA improvement Cum. Capital (% of plan) +/-15% of plan 67.5% 97.3% 100%
Complaints responded to within ≥90% 65.77% 84.85% no change Cum. CQUIN (% of plan) 70.0% 70.0% 70%
agreed timescale deterioration
Ombudsman cases upheld 0 1 0 strong deterioration
≤-£17500
The one-month forecast is an informed prediction of the
next month's performance, which may be based on part-
month data, operational intelligence and historical
trends.
≥100% of plan
≥70% of plan
1-month forecast 4-month trend
Patient Experience
Theatre utilisation
RegulatoryCancelled operations (last-minute)
MSA breaches
Urgent operations cancelled
Governance Risk Rating* for second time0
RN/RM hrs on shift (% of planned)
HCA hrs on shift (% of planned)
Financial Risk Rating*
CQC concerns*Finance
Target
0 0
14/15
Never Events reported (StEIS) Staff attendanceOperational Efficiency
Regulation 28 reports (inquests) Appraisals - rolling 12 mths
Trust induction Outpatient slot utilisation#
Mandatory training Outpatient DNA rate
Failure of safer-surgery process 62-day from referral*#
<10 0.13 0.00
Serious Incidents reported (StEIS)People
62-day from upgrade of urgency*#
'Duty of Candour' breaches
Nutrition risk assessment# due to staff accidents 31-day treatment*#
Emergency re-admissions within10.0% 14.98% 14.14%
31-day surgery*#
30 days (rolling 3 months)# 31-day drug treatment*#
Lost-time accidents 2-week referral*
on admission# Calendar days lost 2-week breast symptomatic*
RIDDOR incidents reported
VTE risk assessments Consecutive safe days
Medicines reconciled≥94% - Qtrly Qtrly
C-difficile - actual cases YTD* within 24 hours Diagnostic wait time, 6 weeks
Harm-free care (all harms)Staff Health & Safety
4-hour wait*
Harm-free care (new harms)
% time on Stroke Unit 18-week incomplete*
MRSA - actual cases YTD* High-risk TIA cases treated ≥60% 21.74% 21.05%
18-week admitted*
from arrival (<4 hours)# 18-week non-admitted*
Actual year-to-date (YTD) is June 2014 unless otherwise indicated. # identifies indicators reporting on previous months data
Overall Clinical Quality Specialty Clinical Quality Patient Access
HSMR # (rolling 12 months) Time to stroke bed≥80% 62.50% 57.14%
QUALITY ACCOUNT: July 2014 Board (June 2014 performance)
June 2014

Page 5
QUALITY ACCOUNT EXCEPTION REPORTS: Director of Operations (1/5)
Overall Clinical Quality Target Trend Position (last 4 months)
Cum Performance 2014/15 Forecast
Emergency Readmissions within 30 days (rolling 3 months) 10%
14.98%
ISSUE: The 30 day readmission rate has started to improve during this reporting period. An audit of 100 readmissions was carried out which established that chronic disease management of chronic obstructive pulmonary disease, cardiac related issues and urinary tract infections accounted for the vast majority of cases. It is recognised that all complex patients are reviewed by a multi-agency team prior to discharge and thus any actions taken must be on a cross-economy, pathway basis, rather than by the acute provider in isolation. ACTIONS COMPLETED:
1. Audit of 100 cases completed. New audit pro-forma drafted 2. Coding reviewed and work in progress to further refine
FUTURE ACTIONS:
1. Re-admission audit being planned into regular audit cycle 6 monthly 2. COPD – Further pathway development with other providers to redesign out of
hospital respiratory pathways (pre and post admission) as part of the Care Together programme.
3. Develop a business case to be submitted to the Care Together Programme Board in August.
4. Cardiac – A similar workstream is planned with the CCG. However, the audit also established some data quality issues within this area which are being rectified.
5. UTI – An ambulatory care pathway is being introduced, which will ensure that all patients are treated in accordance with established best practice. This will be in practice by August 14.
ASSESSING IMPROVEMENT: Improvement will be tracked by visualising an improving trend.
Emergency Readmission rate
Expected date to meet target
End Q4 Signed off by Mike Griffiths
Signed off by Trish Cavanagh

Page 6
QUALITY ACCOUNT EXCEPTION REPORTS: Director of Operations (2/5)
Patient Access (Waiting Times) Target Trend Position (last 4 months)
Cum Performance
2014/15 Forecast
Referral to Treatment time (RTT) – 18 week incomplete pathways 92%
ISSUE: The number of patients on incomplete pathways increased substantially following implementation of Lorenzo. This is mainly due to data quality issues and the Trust has been unable to submit Incomplete Pathway data to NHS England. The data quality issues relate to the creation of multiple pathways for patients due to system and procedural processes. ACTIONS COMPLETED:
1. The 18 week validation team continue to validate the backlog as a priority. Due to the lack of a confirmed date for a system fix from CSC the July 2014 deadline for completion of this will not be achieved.
2. Collaboration with other Lorenzo organisations is underway to share areas of concern and potential process changes.
3. Mandatory Lorenzo system training for targeted users is underway and will be completed by the end of July 2014.
PROPOSED ACTIONS: 1. The validation process has been amended to prioritise patients >18 weeks to enable
the trust to recommence external reporting of incomplete pathways. This is likely to take 3 months to complete.
2. Additional data entry clerks are being recruited on a temporary basis to support and speed up the validation process.
3. CSC providing on-site system support before the end of July 2014. 3. A robust action plan is in place to pick up, address and monitor all issues identified, to
ensure swift resolution and compliance. ASSESSING IMPROVEMENT: Consistent reporting of performance against all national targets. Compliance against the 18 week incomplete pathway target of 92%.
Incomplete Pathway Backlog
Expected date to meet target
TBC – Dependent on CSC System Fix
Signed off by Angela Brierley
Signed off by Trish Cavanagh

Page 7
QUALITY ACCOUNT EXCEPTION REPORTS: Director of Operations (3/5)
Operational Efficiency (Outpatients) Target Trend Position (last 4 months)
Cum Performance
2014/15 Forecast
Outpatient Slot Utilisation Outpatient DNA Rate
85%
7.5%
68.57%
11.05%
ISSUE: Templates continue to be reviewed as part of the Clinic Template Reconfiguration project in conjunction with the Outpatient Efficiency project. Progress has been delayed due to a review of benefits and a revised proposal is due for sign off on 24
th July 2014. Until the revised templates have been fully rolled out, the
clinic utilisation will remain low as we currently hold a large number of unusable slots in our templates. The DNA rate was impacted in June 14, due to an issue relating to non-delivery of appointment letters. This has now been resolved. Work has started on procurement of an alternative appointment reminder service.
PROPOSED ACTIONS: Support sign-off for Clinic Template restructure project and implement changes. Commence Procurement process for Appointment Reminder Service. Continue to pilot further DNA reduction initiatives with Paediatrics service.
ASSESSING IMPROVEMENT: Increased outpatient slot utilisation Reduction in the DNA Rate Increase in OP appointment availability Reduction in OP Waiting time
Expected date to meet target
December 2014 Signed off by S Ashworth
Signed off by Trish Cavanagh

Page 8
QUALITY ACCOUNT EXCEPTION REPORTS: Director of Operations (4/5)
Operational Efficiency (Theatre Utilisation) Target Trend Position (last 4 months)
Cumulative Performance
2014/15 Forecast
In theatre operating utilisation (Capped) Last Minute Cancelled Operations
92%
0.8%
71.43%
0.77%
ISSUES:
Late starts remain high, but a number of workshops have been run to address bed pressures on lists and late starts. Cancellations and DNA’s have impacted utilisation which is tracking close to target trajectory. SUMMARY OF PROGRESS TO DATE
Theatre utilisation continues to improve in line with the trajectory and the planned utilisation and management of lists has improved. Theatre Policy has been drafted and is under review. Successfully recruited Theatre Scheduler, to commence on 18
th August 2014
The project continues to focus effort on late starts and is reviewing the issues relating to bed availability, consenting and delays in getting patients to theatre on time. Proposal centralisation of booking processes under review and revision. PROPOSED ACTIONS:
Continued focus on late starts
Establish improvements in patient preparation and bed availability
Commence implementation of Theatres Policy
Complete draft of Centralised Booking Proposal ASSESSING IMPROVEMENT:
Improved theatre utilisation, productivity, reduction in cancellations and a reduction in waiting list initiatives being undertaken out of hours.
Theatre Utilisation Trajectory for Improvement
Expected date to meet target April 15 Signed off by S Ashworth
Signed off by Trish Cavanagh

Page 9
QUALITY ACCOUNT EXCEPTION REPORTS: Director of Operations (5/5)
Specialist Clinical Efficiency (Stroke) Target Trend Position (last 4 months)
Cum Performance
2014/15 Forecast
Stroke – time to stroke bed from arrival (4hr target) Stroke - % of time on Stroke unit TIA – high risk TIA’s treated within 24hrs
80%
80%
60%
62.50%
77.50%
21.74%
ISSUE: Time on Stroke Ward / Direct Admission
Early identification of Stroke patients in the ED remains a problem. Any training initiatives are having limited success due to the high number of ad hoc locums at middle grade level that deliver variation in consistency. This can mean that patients are admitted through the AMU pathway before a formal stroke diagnosis is made. TIA Key issues: The historical issues of GP referral processes, patient choice and internal booking practices have been thoroughly discussed in previous Boards. The TIA Ambulatory Pathway is now live, although issues with referral practice via GP’s continue. PROPOSED ACTIONS
TIA: The ambulatory TIA pathway has commenced. Engagement work with the CCG continues via monthly meetings with the designated commissioner to ensure the correct referral pathway is used. Weekly monitoring of TIA is established with individual cases being reviewed and action taken where issues have been identified. A newsletter explaining our Ambulatory Pathways has been circulated to GP Practices. Direct Admission / Time on a Stroke Ward: Identification of new strokes using ROSIER scoring as part of the ED React Process and continued feedback of issues to clinicians is being taken through the ED Governance channel. Robust breach analysis and cascade through specialist teams is now incorporated into a daily report which is sent to speciality teams to respond. The stroke co-ordinator rota has been reviewed to provide enhanced cover for ED inreach ASSESSING IMPROVEMENT:
Improvements in SSNAP data / Improving trajectory against direct admissions / Improving trajectory against TIA metrics. Auditing the number of patients accessing services through TIA AEC
% Time on Stroke Unit (4 month trend)
Time to Stroke Bed (4 month Trend)
Expected date to meet target August 2014 Signed off by M Griffiths
Signed off by Trish Cavanagh

Page 10
QUALITY ACCOUNT EXCEPTION REPORTS: Director of Nursing (1/1)
Overall Clinical Quality Target Trend Position (last 4 months)
Cum Performance 2014/15 Forecast
Nutrition Risk Assessment ≥90%
91.26%
ISSUE:
Introduction of new Nutrition Screening Document (Malnutrition Universal Screening Tool – MUST).
Slow uptake of E Learning for new MUST document.
Change of reporting tool (no longer using North West Care Indicator document) no clear tool to use in its replacement.
No clear guidance on required sample size (possibly too small).
ACTIONS COMPLETED:
Ward managers to record screening tool data on a weekly basis to identify areas of poor compliance.
Ward Managers to support staff in access and completion of MUST e-learning package to improve understanding.
FUTURE ACTIONS:
Weekly reviews of compliance with nutritional screening tool use.
Weekly review of staff completion of MUST e-learning. ASSESSING IMPROVEMENT:
Spot check ward reviews completed by Nutrition Nurse in Q3 to ensure on projected target for compliance.
Nutrition Risk Assessment
Expected date to meet target End Q4 Signed off by
Signed off by John Goodenough

Page 11
QUALITY ACCOUNT EXCEPTION REPORTS: Director of Human Resources (1/1)
People Target Trend Position (last 4 months)
Month Performance
2013/14 Forecast
Staff attendance Appraisals - rolling 12 mths Trust induction Mandatory training
96.6%
95%
95%
95%
95.20%
83.60%
96.60%
86.60%
ISSUE: The following are below the Trust target - sickness absence, mandatory training and PDR compliance. Compliance with induction is now above target, following changes in the way that induction is provided and new starters are processed. PROPOSED ACTIONS: The following actions are taking place to improve compliance:
Divisions have been asked to provide an improvement trajectory to meet 95% compliance with PDR and Mandatory Training
A review of the delivery of Mandatory Training has taken place to ensure there are enough sessions for staff to attend.
Sickness absence meetings are held monthly with Divisional managers and the Director of HR
Attendance Management Training for managers is now run on a regular basis, and is being targeted to areas with a low take up to-date, or where sickness absence is high.
ASSESSING IMPROVEMENT: Improvements will be measured through a reduction in sickness absence and an increase in compliance with induction, mandatory training and PDRs.
Sickness Absence
Monthly Sk Abs %
4.8% Trust Target
3.4%
Long Term Sick %
2.9% 12 Month Sk Abs % 4.7%
Short Term Sick %
1.9% Calendar Days Lost 3891
Estimated Monthly Cost
£246,602 Number of Episodes 384
PDR
PDR Completion % 84%
Mandatory Training Wkbook incld IG Completion %
86% Resus % 82%
Manual Handling % 91% Overall Compliance
86%
Expected date to meet target Signed off by E Devlin
Signed off by Amanda Bromley

1
PART 1 AGENDA ITEM 9
Title of paper
Finance & Activity Report – June 2014
Board meeting date 31st July 2014
Purpose
To update the Trust Board on the financial position
Actions Recommended
To note the contents of the report and discuss
Publication This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms None
Any communications actions after the meeting
None
Report of Director of Finance – Barbara Herring
Paper prepared by Deputy Director of Finance – Suzanne Holroyd

2
Summary Financial Position Key Financial Metrics: Month 03 – June 2014
The waterfall graphs below bridge the financial planned position to the actual position.
Financial Position– The Trust is reporting a cumulative normalised deficit of £7.16m at the end of June, against a planned deficit of £4.95m, £2.207m behind plan, and a Continuity of Service Risk Rating of 1 against an expected rating of 1, the worst possible rating. In month the Trust is £1.1m behind plan with an in month deficit of £2.6m.
PlannedSurplus/(Deficit)
ClinicalIncome
OtherIncome
PayCosts
Non PayCosts
Depreciation
PFIInterest
&contingent Rent
Dividends
Othertechnica
lcosts/in
come
ActualSurplus/(Deficit)
Value (4,954) (1,751) 153 (1,109) 413 87 2 0 (2) (7,161)
(4,954)
(1,751)
153
(1,109)
413 87 2 0
(2)
(7,161) (8,000)
(7,000)
(6,000)
(5,000)
(4,000)
(3,000)
(2,000)
(1,000)
0
1,000
Surp
lus
(De
fici
t)
£'0
00
Planned (Deficit) v Actual (Deficit)
Current Month Plan
£000
Current Month Actual £000
Current Month
Variance £000
YTD Plan
£000
YTD Actual
£000
YTD Variance
£000
FY Plan
£000
Income – Clinical activity 11,539 10,781 (758) 34,429 32,678 (1,751) 140,021
Income - Other 903 946 43 2,726 2,879 153 10,921
Expenditure (13,199) (13,612) (413) (39,800) (40,496) (696) (159,057)
EBITDA (757) (1,886) (1,129) (2,645) (4,939) (2,294) (8,115)
Financing (767) (739) 28 (2,309) (2,222) 87 (9,385)
Exceptional Items 0 0 0 0 0 0 0
Net (Deficit) Surplus (1,524) (2,625) (1,101) (4,954) (7,161) (2,207) (17,500)
Exceptional Items 0 0 0 0 0 0 0
Normalised (Deficit)Surplus
(1,524) (2,625) (1,101) (4,954) (7,161) (2,207) (17,500)
CoSRR 1.0 1.0 0 1
Capital expenditure 87 25 62 203 137 66 3,175
Cash 500 2,650 2,150 500
CIP 408 385 (24) 1,129 1,023 (106) 6,100

3
The main driver of the deficit is below planned activity/income performance and above planned pay expenditure as shown in the bridge chart above.
No funding has been released in month or cumulatively to support the financial position.
EBITDA is behind plan by £2,294k.
Income – Clinical income, is below plan in June and has under-performed by £758k, and £1.75m year to date. The chart below details the reasons. In June clinical income is behind plan due to under- performance on non-elective admissions of £696k, elective of £368k, outpatients £135k, offset by over-performance on other of £417k, and A&E of £24k.
Activity remains well below plan and activity levels at this time last year across the key points of delivery, with the exception of accident and emergency, and ambulatory care which are up against plan and last years’ activity. June – Activity (Spells / attendances)
Activity Plan Month
Actual Month
Variance Plan Cum
Actual Cum
Variance June 13 Actual Cum
Elective 1,863 1,832 (31) 5,462 5,094 (368) 5,336
Non Elective 2,187 1,923 (264) 6,690 5,979 (711) 6,730
Ambulatory Care
55 155 100 165 536 371 125
Outpatients 20,482 19,154 (1,328) 59,510 57,538 (1,972) 58,846
A & E 6,495 6,710 215 19,698 20,429 731 19,545
Expenditure Costs are overspending by £413k in the month, and £696k year to date. The chart below tracks the causes of the overspend. Further information can be found in Appendix C. The main cause of the deterioration both in month and year to date is pay costs.

4
Analysis of pay variance – Year to June
Variance £’000
Comment
Medical Pay 6 Vacancy & use of agency staff
Nursing Pay (648) Over-establishment & agency
Other Pay (467) Lorenzo, IT, and Information, UHSM recharge
Total (1,108)
The graph below analyse the actual WTE compared with budgeted WTE for the main staff groups. The main issue is the over-establishment on nursing. This is due to non-delivery of CIP and having escalation beds open, along with ward staffing being above approved levels in many of the wards.
PlannedExpendit
ure
PayCosts
Drugs
ClinicalSupplies
&Services
GeneralSupplies
&Services
Establishment
Expenses &
Costs
Premises &
FixedPlant
OtherCosts
ActualExpendit
ure
Value (39,800) (1,108) 113 (54) 194 (107) (43) 311 (40,496)
(39,800)
(1,108)
113
(54)
194
(107) (43)
311
(40,496) (45,000)
(40,000)
(35,000)
(30,000)
(25,000)
(20,000)
(15,000)
(10,000)
(5,000)
0
5,000
£'0
00
Planned Expenditure V Actual
332
1,096 1,013
317
1,267
936
-
200
400
600
800
1,000
1,200
1,400
Pay Medical Pay Nursing Pay Other
Current month Budget v Actual WTE Trust Total
Sum of Wte Budget SUM Sum of Wte Actual SUM
Values
Summary pay category
Sum of Wte Budget SUM Sum of Wte Actual SUM
Period Num Division

5
CIP - Underperformance against the CIP target is £24k in June, and £3.36m
in year. Of the in-year savings achieved to date of £2.77m, £1.63m has been achieved non-recurrently and £1.14m being recurrent. Recurrently the full year effect of identified savings is £1.212m.
Cash - Cash balances are above plan by £2,150k. This performance has been mainly driven by below plan I&E performance, offset by a net increase in liabilities compared with plan. Cash Flow performance information can be found in Appendices F1 to F3. The Trust has received the planned £622k PDC requested from the DoH for June. This is currently only temporary PDC which would need to be repaid on the 4th of August. However, the department has indicated that this should be made permanent prior to the required repayment date.
The detailed I&E report can be found at Appendix A.
Conclusion At the end of June the Trust is cumulatively behind plan by £2.2m, with a deficit of £7.2m. The Trust is behind plan by £1.1m in the month with a deficit of £2.63m against a planned deficit of £1.52m. The main factors driving this position are;
below planned levels of activity
continued high levels of pay expenditure at premium rates, and over-establishments
Non-delivery of CIP by 9% cumulatively The Trust is increasing the level of financial control such that all areas manage within the available funds. In order to support this process the Trust is undertaking a full review of activity and income recording. In addition recovery plans for activity, income and expenditure are being finalised by two Directorates to address the financial position. Recommendation The Committee is requested to discuss and note the contents of this report.

Key Measures
Cumulative
Plan
Cumulative
Actual Variance
£000 £000 £000
EBITDA (2,645) (4,939) (2,294)
Net Surplus/(Deficit) (4,954) (7,161) (2,206)
Net Surplus/(Deficit) before Exceptional Items (4,954) (7,161) (2,206)
CIP 1,129 1,023 (106)
Margins Annual Plan
Cumulative
Actual Variance
% % %
EBITDA Margin % -5.38% -13.89% -8.52%
EBITDA % Achieved of Plan 99.40% 186.73% 87.33%
I&E Surplus Margin % 1.10% -20.14% -21.24%
Annual Plan
Cumulative
Actual
COSRR 1 1
1. Key risk is the non-delivery of CIP, and its associated impact on achieving financial recovery.
2. Activity underperformance.
3. In year cost pressures.
FINANCE DASHBOARD AS AT 30 JUNE 14
Key Risks
-3000.00
-2500.00
-2000.00
-1500.00
-1000.00
-500.00
0.00
500.00
1000.00
1500.00
April May June July Aug Sept Oct Nov Dec Jan Feb March
Su
rplu
s/(D
efi
cit)
£0
00
Month
Normalised Monthly Surplus/(Deficit)
Plan Actual 14/15 Actual 13/14
-
200
400
600
800
1,000
1,200
1,400
£0
00
Month
Capital Programme
Plan Actual
-
1,000
2,000
3,000
4,000
5,000
6,000
7,000
£0
00
Month
Cash Balances
Plan Actual

Appendix A
Budget Actual Variance Budget Actual VarianceAnnual
budget
£000 £000 £000 £000 £000 £000 £000
IncomeClinical Income 11,539 10,781 (758) 34,429 32,678 (1,751) 140,021
Research & Development 11 34 23 32 137 105 129
Education & Training 309 329 20 928 954 26 3,714
Other Clinical & other non-clinical income 583 574 (9) 1,765 1,729 (36) 7,078
PFI Specific Income (transitional) 0 8 8 0 59 59 0
Total Income 12,442 11,726 (715) 37,155 35,557 (1,599) 150,942
ExpenditurePay Costs (8,981) (9,529) (548) (26,969) (28,078) (1,108) (107,785)
Non-pay cost (incl internal recharges) (3,980) (3,837) 144 (12,111) (11,639) 472 (48,384)
PFI Specific Expenditure - UP (237) (238) (0) (720) (721) (0) (2,888)
PFI Specific Expenditure - transitional 0 (9) (9) 0 (59) (59) 0
Total Costs (13,199) (13,612) (413) (39,800) (40,496) (696) (159,057)
EBITDA (757) (1,886) (1,129) (2,645) (4,939) (2,294) (8,115)
EBITDA as a % of Income -6.09% -16.08% -10.00% -7.12% -13.89% -6.77% -5.38%
Technical Items
Profit/(loss) on asset disposal 0 0 0 0 0 0 0
Exceptional income ( fixed asset impairment) 0 0 0 0 0 0
Exceptional costs ( fixed asset impairment) 0 0 0 0 0 0
Restructuring Costs 0 0 0 0 0 0
Plus Income from Donated Assets 0 0 0 0 0 0
Less Total Depreciation (423) (396) 28 (1,270) (1,183) 87 (5,219)
Plus Total Interest Receivable 2 3 1 5 7 2 20
Less Total Interest payable on loans and leases - PFI (200) (200) 0 (607) (607) (0) (2,437)
PFI Contingent Rent (64) (64) (0) (193) (194) (1) (775)
Less Other Finance Cost - Unwinding Discount (1) (2) (1) (4) (5) (1) (15)
Less PDC Dividend (80) (80) 0 (240) (239) 0 (960)
Net Surplus/(deficit) (1,524) (2,625) (1,101) (4,954) (7,161) (2,207) (17,500)
For Information
Net Surplus/(deficit) before exceptional items (1,524) (2,625) (1,101) (4,954) (7,161) (2,207) (17,500)
INCOME & EXPENDITURE REPORT JUNE 14
In Month Year to Date

Appendix B1
Budget Actual Variance Budget Actual VarianceAnnual
budget
£000 £000 £000 £000 £000 £000 £000
Clinical Income by type
Elective 2,006 1,638 (368) 5,874 5,029 (845) 23,360
Non-Elective 3,776 3,080 (696) 11,466 10,127 (1,339) 47,371
Outpatient 2,239 2,104 (135) 6,508 6,273 (234) 26,065
A&E 695 719 24 2,108 2,190 81 8,455
Other 2,822 3,239 417 8,474 9,059 585 34,770
Total 11,539 10,781 (758) 34,429 32,678 (1,751) 140,021
Clinical Income by Commissioner
Tameside CCG 9,903 9,020 (883) 29,573 28,188 (1,385) 119,985
Manchester CCG 435 379 (56) 1,302 1,121 (181) 5,265
Oldham CCG 607 567 (40) 1,799 1,553 (246) 7,250
Stockport CCG 91 80 (11) 272 245 (28) 1,103
Specialised Services 576 561 (15) 1,707 1,579 (128) 6,872
All other income contracts and CIP (74) 174 248 (223) (7) 216 (454)
Total 11,539 10,781 (758) 34,429 32,678 (1,751) 140,021
Other income:Research & Development 11 34 23 32 137 105 129
Education & Training 309 329 20 928 954 26 3,714
Other clinical & other non-clinical income 583 574 (9) 1,765 1,729 (36) 7,078
PFI Specific Income - Transitional 0 8 8 0 59 59 0
Total 903 946 43 2,726 2,879 153 10,921
Total Income 12,442 11,726 (715) 37,155 35,557 (1,599) 150,942
Activity (Spells/ attendances)
Elective 1,863 1,832 (31) 5,462 5,094 (368) 21,893
Non Elective 2,187 1,923 (264) 6,690 5,979 (711) 27,775
Ambulatory Care 55 155 100 165 536 371 660
Outpatients (inc OPPROC) 20,482 19,154 (1,328) 59,510 57,538 (1,972) 238,370
A&E Attendances 6,495 6,710 215 19,698 20,429 731 78,999
31,081 29,774 (1,307) 91,525 89,576 (1,949) 367,697
In Month Year to Date
INCOME REPORT JUNE 14

APPENDIX C
ANALYSIS OF EXPENDITURE
Annual
Budget Actuals Budget Actuals Variance Budget Actuals Variance Budget
wte wte £000's £000's £000's £000's £000's £000's £000's
Expenditure
Pay Costs:-
Medical 332 275 (2,592) (2,322) 270 (7,793) (7,009) 784 (30,999)
Medical Agency - 42 (160) (517) (357) (479) (1,257) (777) (1,947)
Nursing 1,083 1,216 (3,589) (3,664) (74) (10,777) (10,739) 38 (43,233)
Nursing Agency - 50 (0) (160) (159) (1) (687) (686) (3)
Other 1,002 936 (2,618) (2,591) 27 (7,854) (7,616) 238 (31,341)
Other Agency 11 - (22) (276) (254) (65) (771) (705) (262)
0
Total Pay Costs 2,429 2,520 (8,981) (9,529) (548) (26,969) (28,078) (1,108) (107,785)
Non-Pay Costs:-
Drugs (658) (631) 28 (1,994) (1,881) 113 (7,853)
Clinical Supplies & Services (1,002) (1,020) (18) (3,088) (3,143) (54) (12,243)
General Supplies & Services (530) (473) 57 (1,615) (1,421) 194 (6,458)
Establishment Expenses (119) (128) (8) (361) (445) (83) (1,359)
Other Establishment Costs (610) (607) 3 (1,831) (1,855) (24) (7,317)
Premises & Fixed Plant (547) (556) (10) (1,682) (1,725) (43) (7,009)
Other (514) (422) 92 (1,540) (1,170) 370 (6,145)
PFI - UP (237) (238) (0) (720) (721) (0) (2,888)
PFI - Transitional Costs 0 (9) (9) 0 (59) (59) 0
Total Non-Pay Costs 0 0 (4,218) (4,083) 135 (12,831) (12,418) 413 (51,272)
Total Expenditure 2,429 2,520 (13,199) (13,612) (413) (39,800) (40,496) (696) (159,057)
The above table excludes expenditure on technical items as detailed in Appendix A such as depreciation, dividends and exceptional items.
Year-to-Date
EXPENDITURE REPORT JUNE 14
In Month

TAMESIDE HOSPITAL NHS FOUNDATION TRUST Appendix D
Column A Column B Column C Column D
Period Ending
31 March
2014
£'000s
Period Ending
31 May
2014
£'000s
Period Ending
30 June
2014
£'000s
Movement in the
month May
- June 2014
£'000s
Non Current Assets
Property, plant and equipment 69,396 68,862 68,562 (300)
PFI: Property, plant and equipment 36,798 36,657 36,586 (71)
Trade and Other Receivables
> Accrued Income (CRU Income grt than 1 yr) 203 71 109 39
> Prepayments - PFI Related 2,309 2,421 2,476 55
Total Non Current Assets 108,707 108,010 107,733 (277)
Current Assets
Inventories - Stock - Finished Goods 1,300 1,461 1,358 (103)
Trade & Other Receivables:-
> NHS Trade Receivables 1,432 1,653 1,189 (464)
> Non NHS Trade Receivables 730 98 117 19
> Other Receivables 531 618 471 (147)
> Accrued Income 2,105 2,463 2,298 (165)
> Prepayments - Non PFI Related 740 1,171 1,399 229
0
Cash 2,586 2,292 2,650 358
Investments 2,000 1,500 0 (1,500)
Total Current Assets 11,424 11,255 9,482 (1,773)
Current Liabilities
Trade & Other Payables:-
> NHS Trade Creditors (1,501) (1,442) (1,134) 308
> Non NHS Trade Creditors (2,548) (3,092) (2,004) 1,089
> Other Creditors (3,105) (4,453) (4,481) (28)
> Capital Creditors (491) (133) (111) 22
Other Liabilities:-
> Accruals (10,808) (12,728) (14,419) (1,691)
> Deferred Income (1,880) (1,863) (1,520) 343
>PFI Leases (1,428) (1,428) (1,428) 0
>PDC Dividend Creditor (40) (200) (279) (80)
Provisions (190) (182) (174) 7
Total Current Liabilities (21,991) (25,519) (25,549) (30)
Net Current Assets/Liabilities (10,567) (14,264) (16,068) (1,803)
Non Current Liabilities
Other Financial Liabilities:-
> Deferred Income (312) (698) (698) 0
> PFI Leases (57,440) (57,202) (57,084) 117
Provisions (638) (632) (632) 0
Total Non Current Liabilities (58,390) (58,532) (58,415) 117
TOTAL ASSETS EMPLOYED 39,749 35,213 33,250 (1,963)
Financed By Taxpayers Equity
PDC 53,168 53,168 53,830 662
Revaluation Reserve 19,347 19,347 19,347 0
I&E Reserve (33,895) (33,895) (33,895) 0
I&E Reserve 2013/14 1,130 1,130 1,130 0
I&E reserve 2014/15 0 (4,536) (7,161) (2,625)
TOTAL TAXPAYERS EQUITY 39,749 35,213 33,250 (1,963)
STATEMENT OF POSITION 2014/15

Appendix E1
Actual April
2014 £'000
Actual
May 2014
£'000
Actual
June 2014
£'000
YTD Actual
£'000
YTD
Movement to
plan £'000
Q2
2014/15
£'000
Q3
2014/15
£'000
Q4
2014/15
£'000
Revised
Plan
2014/15
£'000
Operating Surplus/(deficit) after tax (2,427) (2,109) (2,625) (7,161) (2,206) (4,150) (4,591) (1,598) (17,500)
Depreciation and Amortimisation 394 394 396 1,184 (85) 1,266 1,336 1,433 5,219
Impairment losses/(reversals) 0 0 0 0 0 0 0 0 0
PDC Dividend 80 80 80 240 (0) 240 240 240 959
Gain/loss on disposal of property, plant and equipment 0 0 0 0 0 0 0 0 0
Other increases/(decreases) to reconcile to profit/(loss) from operation items 262 272 262 796 (7) 803 803 810 3,212
Non-Cash flows in operating surplus/(deficit) total 736 746 737 2,219 (92) 2,309 2,378 2,483 9,389
Operating Cash Flows before movement in working capital (1,691) (1,363) (1,888) (4,942) (2,299) (1,841) (2,213) 885 (8,111)
Increase/(Decrease) in working capital
(Increase)/Decrease in inventories (62) (99) 103 (58) (58) 58 0 0 (0)
(Increase)/Decrease in NHS Trade Receivables 11 (232) 464 243 (244) 244 (70) (417) (0)
(Increase)/Decrease in Non NHS Trade Receivables 573 59 (19) 613 (97) 44 (100) (15) 542
(Increase)/Decrease in other receivables 66 (153) 147 60 27 (27) 0 (33) 0
(Increase)/Decrease in accrued income (316) (42) 165 (193) 181 12 (171) 352 (0)
(Increase)/Decrease in prepayments (346) (85) (229) (660) 298 (764) 50 1,374 0
Increase/(Decrease) in Trade Creditors 677 (193) (1,397) (913) (1,147) (34) 0 1,555 608
Increase/(Decrease) in Other Creditors 1,292 56 28 1,376 228 (278) 0 50 1,148
Increase/(Decrease) in accruals 1,264 655 1,691 3,610 5,122 (2,145) (1,045) (3,115) (2,695)
Increase/(Decrease) in Deferred Income (exl Donated Assets) 615 (246) (343) 27 27 (27) 0 0 (0)
Increase/(Decrease) in provisions (16) 1 (7) (22) (22) 22 0 0 (0)
Increase/(Decrease) in other - Other Financial Liabilities 0 0 0 0 0 0 0 0 0
Increase/(Decrease) in working capital total 3,758 (279) 604 4,083 4,315 (2,895) (1,336) (249) (397)
Net cash inflow/(outflow) from operating activities 2,067 (1,642) (1,284) (859) 2,017 (4,736) (3,549) 636 (8,508)
Net cash inflow/(outflow) from Investing activies
Property, plant and equipment - maintenance expenditure (71) (41) (25) (137) 66 (441) (1,895) (702) (3,175)
Increase/(decrease) in Capital Creditor (304) (54) (22) (380) 66 226 697 (908) (365)
Net cash inflow/(outflow) from Investing activies - Total (375) (95) (47) (517) 132 (215) (1,198) (1,610) (3,540)
Net cash inflow/(outflow) before financing 1,692 (1,736) (1,331) (1,375) 2,149 (4,951) (4,747) (974) (12,048)
Net cash inflow/(outflow) from Financing activities
Public Dividend Capital Received 0 0 662 662 0 4,675 6,141 2,822 14,300Public Dividend Capital Repaid 0 0 0 0 0 0 0 0 0
PDC Dividends paid 0 0 0 0 0 (479) 0 (480) (959)
Interest element of finance lease rentals on balance sheet (264) (273) (264) (801) (1) (809) (809) (792) (3,212)
Capital element of finance lease rental payments - on balance sheet (172) (178) (172) (522) 1 (530) (530) (519) (2,101)
Interest received on cash and cash equivalent 2 2 3 7 2 5 5 5 22
(Increase)/decrease in non-current receivables 177 (44) (39) 94 (86) (60) (60) (60) (86)
Net cash inflow/(outflow) from Financing activities - Total (257) (493) 190 (560) (84) 2,802 4,747 976 7,964
Net increase/(decrease) in cash and cash equivalents 1,435 (2,229) (1,141) (1,936) 2,065 (2,150) (0) 2 (4,083)
Opening cash and cash equivalents 4,586 6,021 3,792 4,586 86 2,650 500 500 4,586
Closing cash and cash equivalents 6,021 3,792 2,650 2,650 2,150 500 500 500 500
Monitor Plan 14/15 4,370 3,178 500 500 0 500 500 500 500
Variance to Monitor Plan 14/15 1,651 614 2,150 2,150 2,150 0 0 0 (0)
Tameside Hospital NHS Foundation Trust
Cashflow Statement 2014/15

Plan
July
2014
£'000
Plan
August
2014
£'000
Plan
Sept
2014
£'000
Plan
October
2014
£'000
Plan
November
2014
£'000
Plan
December
2014
£'000
Plan
January
2015
£'000
Plan
February
2015
£'000
Plan
March
2015
£'000
Revised Plan
2014/15 £'000
Operating Surplus/(deficit) after tax (1,230) (1,421) (1,498) (1,346) (1,400) (1,846) (1,144) (1,664) 1,210 (17,500)
Depreciation and Amortimisation 422 422 422 445 445 445 478 478 478 5,219
Impairment losses/(reversals) 0 0 0 0 0 0 0 0 0 0
PDC Dividend 80 80 80 80 80 80 80 80 80 959
Gain/loss on disposal of property, plant and equipment 0 0 0 0 0 0 0 0 0 0
Other increases/(decreases) to reconcile to profit/(loss) from operation items 268 268 268 268 268 268 268 268 275 3,212
Non-Cash flows in operating surplus/(deficit) total 770 770 770 793 793 793 825 825 832 9,389
Operating Cash Flows before movement in working capital (461) (652) (729) (553) (607) (1,053) (318) (839) 2,042 (8,111)
Increase/(Decrease) in working capital
(Increase)/Decrease in inventories 58 0 0 0 0 0 0 0 0 (0)
(Increase)/Decrease in NHS Trade Receivables 544 (200) (100) (90) 220 (200) 100 (250) (267) (0)
(Increase)/Decrease in Non NHS Trade Receivables 97 (53) 0 0 0 (100) (15) 0 0 542
(Increase)/Decrease in other receivables (27) 0 0 0 0 0 0 0 (33) 0
(Increase)/Decrease in accrued income 12 0 0 (205) 0 34 100 126 126 (0)
(Increase)/Decrease in prepayments (481) (183) (100) 0 100 (50) 50 662 662 0
Increase/(Decrease) in Trade Creditors 247 (100) (181) 100 (100) 0 45 250 1,260 608
Increase/(Decrease) in Other Creditors (228) (50) 0 0 0 0 0 0 50 1,148
Increase/(Decrease) in accruals (2,036) (9) (100) (102) 96 (1,039) 1,050 (969) (3,196) (2,695)
Increase/(Decrease) in Deferred Income (exl Donated Assets) 531 (279) (279) 558 (279) (279) 558 (279) (279) (0)
Increase/(Decrease) in provisions 22 0 0 0 0 0 0 0 0 (0)
Increase/(Decrease) in other - Other Financial Liabilities 0 0 0 0 0 0 0 0 0 0
Increase/(Decrease) in working capital total (1,261) (874) (760) 261 37 (1,634) 1,888 (460) (1,677) (397)
Net cash inflow/(outflow) from operating activities (1,722) (1,526) (1,489) (292) (570) (2,687) 1,570 (1,299) 365 (8,508)
Net cash inflow/(outflow) from Investing activies
Property, plant and equipment - maintenance expenditure (57) (133) (251) (506) (1,258) (131) (236) (203) (263) (3,175)
Property, plant and equipment - non -maintenance expenditure 0 0 0 0 0 0 0 0 0 0
Increase/(decrease) in Capital Creditor 32 76 118 255 817 (375) (1,022) (33) 147 (365)
Proceeds from sale of assets 0 0 0 0 0 0 0 0 0 0
Net cash inflow/(outflow) from Investing activies - Total (25) (57) (133) (251) (441) (506) (1,258) (236) (116) (3,540)
Net cash inflow/(outflow) before financing (1,747) (1,583) (1,622) (543) (1,011) (3,193) 312 (1,535) 249 (12,048)
Net cash inflow/(outflow) from Financing activities
Public Dividend Capital Received 66 2,053 2,556 1,012 1,466 3,663 158 1,963 701 14,300Public Dividend Capital Repaid 0 0 0 0 0 0 0 0 0 0
PDC Dividends paid 0 0 (479) 0 0 0 0 0 (480) (959)
Interest element of finance lease rentals on balance sheet (273) (273) (264) (273) (264) (273) (273) (246) (273) (3,212)
Capital element of finance lease rental payments - on balance sheet (177) (177) (176) (177) (176) (177) (177) (165) (177) (2,101)
Interest received on cash and cash equivalent 0 0 5 0 5 0 0 5 0 22
(Increase)/decrease in non-current receivables (20) (20) (20) (20) (20) (20) (20) (20) (20) (86)
Net cash inflow/(outflow) from Financing activities - Total (404) 1,583 1,622 542 1,011 3,193 (312) 1,537 (249) 7,964
Net increase/(decrease) in cash and cash equivalents (2,150) (0) 0 (0) (0) 0 0 0 0 (4,083)
Opening cash and cash equivalents 2,650 500 500 500 500 500 500 500 500 4,586
Closing cash and cash equivalents 500 500 500 500 500 500 500 500 500 500
Monitor Plan 14/15 500 500 500 500 500 500 500 500 500 500
Variance to Monitor Plan 14/15 0 0 0 0 0 0 (0) (0) (0) (0)
Tameside Hospital NHS Foundation Trust
Rolling 12 Month Cashflow Statement July 2014 - June 2015

Variance
MonthActual
April 14
Actual
May 14
Actual
June 14
Total YTD
2014/15
YTD Variance
To Plan
2014/15
Plan
July 14
Plan
August 14
Plan
September 14
Plan
October 14
Plan
November 14
Plan
December 14
Plan
January 15
Plan
February 15
Plan
March 15Total 2014/15
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Bank Accounts
Current Account (RBS/Lloyds/Citi) 2,558 4,014 2,272 2,643 494 493 493 493 493 493 494 493
Patient Monies (2) (2) (2) (2) (2) (2) (2) (2) (2) (2) (2) (2)
Petty Cash 8 8 8 8 8 8 8 8 8 8 8 8
National Loans Fund 2,000 2,000 1,500 0 0 0 0 0 0 0 0 0
Total Cash Balance 4,565 6,021 3,779 4,565 65 2,650 500 500 500 500 500 500 500 500 4,565
Cash Income Receipts
NHS Contract Income 11,334 11,791 11,706 34,831 (154) 12,161 11,989 11,602 11,989 11,759 11,419 11,918 11,312 12,125 141,106
Overperformance/(Underperformance) 62 0 7 68 1,337 (2,174) 0 0 0 0 0 0 0 0 (2,106)
NCA Income 73 54 109 235 43 114 100 100 140 100 100 100 100 70 1,160
Other Income 744 712 1,411 2,868 424 1,039 664 663 1,090 685 685 985 686 685 10,050
Total Income 12,212 12,557 13,232 38,002 1,650 11,140 12,753 12,365 13,219 12,544 12,204 13,003 12,098 12,880 150,208
Cash Expenditure Payments
Payroll (4,375) (4,515) (4,517) (13,407) (75) (4,447) (4,444) (4,444) (4,444) (4,444) (4,444) (4,444) (4,444) (4,444) (53,406)
Tax, NI & Superannuation (1,784) (3,051) (3,083) (7,918) 31 (3,080) (3,080) (3,080) (3,080) (3,081) (3,081) (3,081) (3,081) (3,081) (35,640)
Agency/Other Pay (1,321) (1,024) (958) (3,303) 375 (1,147) (1,099) (1,099) (1,200) (1,200) (1,200) (1,200) (1,200) (1,200) (13,848)
NHSP (479) (551) (830) (1,860) (34) (600) (600) (600) (600) (600) (600) (600) (600) (600) (7,260)
Total Pay (7,959) (9,141) (9,388) (26,488) 297 (9,275) (9,223) (9,223) (9,324) (9,325) (9,325) (9,325) (9,325) (9,325) (110,155)
Non Pay Revenue (3,212) (5,309) (5,213) (13,734) 648 (4,435) (5,295) (4,855) (5,023) (4,119) (5,066) (4,025) (4,373) (3,322) (54,246)
PFI Payment, all monthly outgoing inc VAT (821) (679) (851) (2,351) (120) (834) (834) (834) (834) (807) (834) (834) (753) (834) (9,749)
PDC Dividend 0 0 0 0 0 0 0 (479) 0 0 0 0 0 (520) (999)
Total Non Pay (4,032) (5,988) (6,065) (16,085) 528 (5,269) (6,129) (6,168) (5,857) (4,926) (5,900) (4,859) (5,126) (4,676) (64,995)
Total Expenditure (11,991) (15,129) (15,452) (42,573) 825 (14,544) (15,352) (15,391) (15,181) (14,251) (15,225) (14,184) (14,451) (14,001) (175,150)
Income/Expenditure 221 (2,572) (2,220) (4,571) 2,476 (3,404) (2,598) (3,025) (1,962) (1,707) (3,020) (1,180) (2,353) (1,120) (24,942)
Other cash receipts/payments
Capital (375) (95) (47) (517) 132 (25) (57) (133) (251) (361) (1,245) (180) (211) (187) (3,167)
VAT Debtor 518 437 529 1,484 47 500 500 500 500 500 500 500 500 500 5,984
Recharges/Payroll Deductions 448 (13) (53) 382 (615) 114 102 102 102 102 102 102 102 106 1,316
Deferred Income 645 0 0 645 45 600 0 0 600 0 0 600 0 0 2,445
PDC Drawdown 0 0 662 662 0 66 2,053 2,556 1,012 1,466 3,663 158 1,963 701 14,300
Total Other 1,236 330 1,091 2,656 (391) 1,255 2,598 3,025 1,963 1,707 3,020 1,180 2,354 1,120 20,878
Cash Movement in the month 1,456 (2,242) (1,129) (1,915) 2,085 (2,149) 0 0 0 0 0 0 0 0 (4,065)
Opening cash Balance 4,565 6,021 3,779 4,565 65 2,650 500 500 500 500 500 500 500 500 4,565
Closing Monthly Cash Balance 6,021 3,779 2,650 2,650 2,150 500 500 500 500 500 500 500 500 500 500
Monitor Plan 14/15 4,370 3,178 500 500 0 500 500 500 500 500 500 500 500 500 500
Movement to Monitor Plan 14/15 1,651 601 2,150 2,150 2,150 0 0 0 0 0 0 0 0 0 0
Summary 12 Month Cash Plan Forecast 2014/15
Actual 13 Week Cashflow Forecast
Appendix E3

1
PART 1 AGENDA ITEM 10
Title of Board paper
Sealed Documents – Quarter 1 – 2014/15
Board meeting date 31st July 2014
Purpose
To notify the Board of the documents to which the Trust seal has been applied in Quarter 1
Actions Recommended
Discussion / Noting / Decision
Publication This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms None
Any communications actions after the meeting
None
Report of Barbara Herring, Director of Finance
Paper prepared by Barbara Herring, Director of Finance

2
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
Sealed Documents - Quarter 1 – 2014/15 The Trust’s Standing Orders require a quarterly report to the Trust Board identifying all documents to which the Common Seal has been applied during the preceding quarter. These documents were secured and sealed under the “Tameside Hospital NHS Foundation Trust”. The Trust’s seal was used on one occasion during Quarter 1.
• Contract for building works – Ladysmith Building.

Part 1
Agenda Item 11
Title of paper
Significant Risk Report
Meeting date 31st July 2014
Purpose
The significant risk register report provides the Trust Board with details on all identified significant risk exposure through the Risk Register and Board Assurance Framework throughout Tameside Hospital NHS Foundation Trust
Actions Recommended
Discussion / Noting / Decision
Publication This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms None
Any communication actions after meeting
Dissemination and communication
Report of
Karen James Chief Executive
Paper prepared by Peter Weller Director of Quality and Governance

Page 2 of 34
July 2014 - Significant Risk Register Report
1.0 Summary Narrative
1.1 The significant risk register report provides Trust Board with details on all identified significant risk exposure through the Risk Register and Board Assurance Framework throughout Tameside Hospital NHS Foundation Trust. These risks were subject to review by the Quality and Governance Unit following discussion with each responsible Director.
1.2 The Trust has identified a range of significant risks, which are currently
being mitigated, whose impact could have a direct bearing on compliance with Monitors Provider Licence, CQC registration or the achievement of corporate objectives in the following areas should the mitigation plans be ineffective. Currently, the significant risks relate to the following areas:
• Infection Prevention (C. difficile target)
• Finance (Cost control, CIP delivery and liquidity)
• Compliance (Monitors Provider Licence and CQC Registration ) • Lorenzo ( Lorenzo related implementation issues, IM&T infrastructure) • Discharge Processes
• Recruitment 1.3 The main controls and action plans for each significant risk in each area are
being reviewed and collated in the Trust Electronic Risk Register. The programme has incorporated the Corporate Risks and aligned them to the Board Assurance Framework. The new risk number and the previous risk number are included in the report to ensure continuity. Appendix 1 summarises the current significant risks. Appendix 2 provides the Board with the controls and mitigation for the significant risk analysis. Detailed and focussed work is taking place within the Divisions to ensure risk registers are updated and monitored. The responsible Committees are identified on the report.
1.4 New Significant Risks None
1.5 Increased Risk Scores There are no increased risk scores from the previous report. Controls are in
place and further actions are on-going to minimise risk.

Page 3 of 34
1.6 Downgraded Risks The risks are currently being fully reviewed in light of the CQC regulatory inspection report published in July 2014. All risk handlers and risk owners are systematically meeting with the Quality and Governance Unit senior staff to review their risks for assurance and controls. 1.7 Notable Changes / Update Appendix 2 of the significant risk report includes updated information on notable actions.

Page 4 of 34
Appendix 1
CORPORATE SUMMARY – SIGNIFICANT RISK THFT SHOWING RISKS 15 OR ABOVE
� Residual Risk Score (Current Risk) Risk Trend Unmitigating Risk Score �
� (Target Risk / Risk Appetite Threshold) � Reducing � Increasing � Static * New Risk
Risks scoring 25 on the Corporate Risk Register and Assurance Framework
Risk 723
Previously
C2 also
AF2.5
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to meet, deliver Trusts
financial plan
financial/contractual/demand
targets including CIP delivery
Finance and
Performance
Committee
� �
�
Risk 718
Previously
C24
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Continuing implementation of
Lorenzo (risks to patient safety
quality, information governance
and performance trajectories)
Quality and
Governance
Committee
� �
�
Risk
AF1.17
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to discharge patients
with adequate information
Quality and
Governance
Committee
� �
�
Risk
AF 4.2
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to ensure on-going
compliance with terms of FT
authorisation (monitor
requirements)
Trust Board � �
�

Page 5 of 34
Risks scoring 15 - 20 on the Corporate Risk Register and Assurance Framework
Risk AF4.4
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
ACCIDENT &
EMERGENCY 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to achieve A&E
quality indicators
Executive
Management
Team/
Finance and
Performance
Committee
� �
�
Risk 743
Previously
C57 also
AF1.17
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Effective discharge of Patients
ensuring adequate information and
knowledge of medication
Quality and
Governance
Committee
�
�
�
Risk
AF1.13
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to comply with the CQC
Essential Standards of Quality
and Safety relating to record
keeping
Quality and
Governance
Committee
� �
�
Risk
AF4.1
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to comply with the CQC
Essential Standards of Quality
and Safety
Quality and
Governance
Committee
� �
�
Risk 3132
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Incomplete referral to
treatment (RTT) pathway data
submission
Executive
Management
Team/Finance
and
Performance
� �
�
Risk 758
Previously
C16 also
AF1.3
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Trust SHMI indicating potential
areas of concern regarding
mortality and equality
Quality and
Governance
Committee
� �
�
Risk 734
Previously Risk EM4
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Nursing vacancies, leadership
and Nursing staffing
recruitment across Medicine
and the ability to provide safe
care
Executive
Team � �
�
Risk 737
Previously
C8 also
AF1.7
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Healthcare associated infection
prevention
(MRSA, C-DIFF, MSSA, E-Coli)
Quality and
Governance
Committee
� �
�
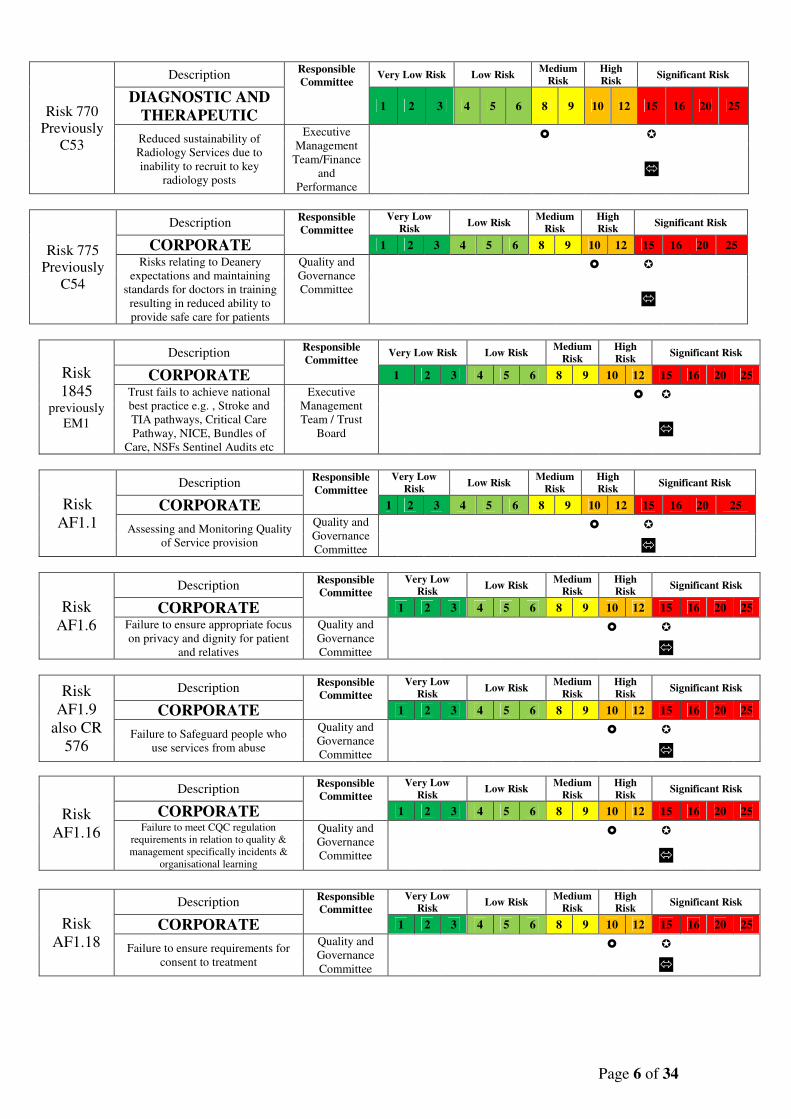
Page 6 of 34
Risk 770
Previously
C53
Description Responsible
Committee Very Low Risk Low Risk
Medium
Risk
High
Risk Significant Risk
DIAGNOSTIC AND
THERAPEUTIC 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Reduced sustainability of
Radiology Services due to
inability to recruit to key
radiology posts
Executive
Management
Team/Finance
and
Performance
� �
�
Risk 775
Previously
C54
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Risks relating to Deanery
expectations and maintaining
standards for doctors in training
resulting in reduced ability to
provide safe care for patients
Quality and
Governance
Committee
� �
�
Risk
1845 previously
EM1
Description Responsible
Committee Very Low Risk Low Risk
Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Trust fails to achieve national
best practice e.g. , Stroke and
TIA pathways, Critical Care
Pathway, NICE, Bundles of
Care, NSFs Sentinel Audits etc
Executive
Management
Team / Trust
Board
� �
�
Risk
AF1.1
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Assessing and Monitoring Quality
of Service provision
Quality and
Governance
Committee
� �
�
Risk
AF1.6
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to ensure appropriate focus
on privacy and dignity for patient
and relatives
Quality and
Governance
Committee
� �
�
Risk
AF1.9
also CR
576
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to Safeguard people who
use services from abuse
Quality and
Governance
Committee
� �
�
Risk
AF1.16
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to meet CQC regulation
requirements in relation to quality &
management specifically incidents &
organisational learning
Quality and
Governance
Committee
� �
�
Risk
AF1.18
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to ensure requirements for
consent to treatment
Quality and
Governance
Committee
� �
�

Page 7 of 34
Risk
AF1.22
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to ensure that staff have the
relevant mandatory skills and
training to ensure safe practice.
Quality and
Governance
Committee
� �
�
Risk
AF1.23
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to ensure adequate staffing
levels to ensure patient safety and
quality of services.
Executive
Management
Team / Trust
Board
� �
�
Risk
AF1.24
Description Responsible
Committee Very Low Risk Low Risk
Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Increased demands beyond
predicted levels which is outside
current capacity
Executive
Management
Team /
Finance and
Performance
Committee
� �
�
Risk
AF1.25
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to fulfil CQC requirements
with management of Complaints
Quality and
Governance
Committee
� �
�
Risk
AF4.6
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to minimise delayed
transfers of care
Improveme
nt Board
� �
�
Risk
AF4.8
Description Responsible
Committee
Very Low
Risk Low Risk Medium
Risk
High
Risk Significant Risk
CORPORATE 1 2 3 4 5 6 8 9 10 12 15 16 20 25
Failure to have in place a IM&T
infrastructure and Service
supporting organisational
objectives
Executive
Management
Team and
Board
� �
�
� Residual Risk Score (Current Risk) Risk Trend Unmitigating Risk Score �
� (Target Risk / Risk Appetite Threshold) � Reducing � Increasing � Static * New Risk

Page 8 of 34
July 2014
APPENDIX 2: SIGNIFICANT RISK ANALYSIS Regulatory | National Target | CORPORATE
Potential Risk Location Owner/Responsible
Committee/Group RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk Source
CORPORATE All Clinical
and
Corporate
directorates
Director of Finance
Directors of all
services
Finance and
Performance
Committee
25
RED
����
• Monthly monitoring
reports to Trust
Board
• Reporting to Trust
Board Sub-
Committees of
constituent actions
and plans to reduce
risk.
• Divisions to risk
assess impact,
manage and monitor
activity, performance
targets and progress
of CIPs and escalate
any potential or
actual performance
issues or clinical risks
arising out of the
financial plan to
Directors.
• Local and Board
monitoring of
performance and
patient experience
indicators.
• Monitor oversight
and reporting
framework
• Turnaround Director and
revised programme
• Greater Manchester
‘Healthier Together’
Strategy
• Certify that all material
non recurrent CIP's have
also been subject to a
rigorous QIA
• Fully develop schemes to
deliver the full 2014/15 CIP
target on a recurrent basis
• Commission a review of
2015/16 CIPs.
• Develop and submit to
regulators milestones and
financial modelling
None
Operational
Performance
Incidents
Complaints
and Claims
Risk
723
(C2)
Also
AF2.5
Failure to meet, deliver Trusts
financial plan financial/
contractual/demand targets
including CIP delivery Review
Date /
Frequency
September
2014
Quarterly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 9 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location Owner/Responsible
Committee RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk Source
CORPORATE All
Clinical
&
Corporate
Directorates
CIO & Chief
Operating Officer
Executive
Management
Team
25
RED
����
• Initial
implementation plan
complete which
involved clinicians
from each area and
Clinical Reference
Group.
• Medway overlap to
ensure continuity.
• EPR Group
monitoring of post
implementation
performance.
• Live action log
• On-going monitoring
of Lorenzo reported
incidents and
triangulation of
information.
• Monitoring progress
report to Trust Board
• Prioritisation of
urgent information
requests to delivery
of safe and effective
patient care.
• Post-implementation issue
specific plans progressed
and monitored by the EPR
Group, Quality and
Governance Committee and
sub committees.
• Routine reporting to Board
• Assessment of issues by
maintenance and
monitoring of Operational
Performance
• All key operational standards
continue to be monitored
• Business Continuity Plans
implemented if required to
ensure staff assisted and
able to continue delivering
their services.
None
Risk
Register
Incident,,
Operational
Performance
Risk
718
(C24)
Implementation of Lorenzo
information system (Risks to
Patient Safety Quality,
Information Governance and
Performance Trajectories) Review Date /
Frequency
August 2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 10 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk
Source
CORPORATE All Clinical
and
Corporate
Directorates
Director of
Nursing and
Medical
Director
Quality and
Governance
Committee
Risk
Management
Group
25
RED
����
• Discharge policy and
procedures in place
• Monitoring of
operational
performance activity
and review of discharge
and transfer services
undertaken.
• Pre - printed discharge
summaries given to
each patient,
addressing all the
discharge issues
• Divisional Governance
Monitoring
• Audit programme
• Key Metrics monitored
• Trust wide implementation
of the discharge and patient
flow action plan through the
Discharge task and finish
group.
• Discharge and Patient Flow
Work Stream None
Third
party
reviews
Patient
feedback
Incidents
complaints
and claims
Risk
AF1.17
Failure to discharge patients with
adequate information
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 11 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location Owner/Responsible
Committee RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE Corporate
Directorates
Director of Finance
Trust Board
25
RED
����
• Board reporting in
line with FT provider
licence
requirements
• Board Financial
reporting
procedures fit for
purpose
• FT metric
performance
framework.
• Regular contact with
Monitor and Board
reporting re actions
taken to maintain
authorisation
• Continuous
implementation of
required actions by all
staff at levels required
• Implementation of
action plan re CIP
identification and
implementation of Trust
Improvement
Programme and Agreed
Monitoring action
None
Monitors
Provider
licence
requirements
and
Regulatory
Monitoring
Risk
AF4.2
Failure to ensure on-going
compliance with terms of FT
authorisation (monitor
provider licence
requirements)
Review Date
/ Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate to assure Monitor requirements are being discussed and progressed with this.

Page 12 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location Owner/Responsible
Committee RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk Source
CORPORATE Trust wide
Chief Operating
Officer
Executive
Management Team
/ Finance and
Performance
Committee
20
RED
����
• Detailed recovery plan
in place
• Aim to see patients
within 2 hours of
attendance in the
Emergency
Department;
• Potential admissions to
be identified early by
the Emergency
Department;
• Wards to actively seek
to admit patients from
the Emergency
Department as soon as
bed available;
• The use of early senior
review will be assessed
and ‘best practice’
principles developed;
• Additional consultant
ward rounds during the
weekend over the
winter period;
• Bed management
meetings strategic
• Board rounds in ED;
• Non-elective health-
economy (NWAS,
Primary Care, Social
Care, TGH) action plan
generated;
• Implementation of
agreed Medical Model
• Non-Elective Action
Plan includes:
• Rapid Assessment and
Treatment (RAT)
model:
• ED in-reach by
consultants
• Board rounds in ED;
• Provision of
Ambulatory Care
Services
• Discharge and patient
flow work stream
• Review ward round
‘timetable’.
None Performance
management
Risk
AF4.4
Failure to achieve Emergency
Department quality indicators
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
Mitigation plans are designed to achieve compliance with performance target.

Page 13 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location Owner/Responsible
Committee RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE Trust wide
Director of Nursing
Chief Operating
Officer
Executive
Management Team
and Quality and
Governance
20
RED
����
• Workforce planning
and recruitment
plans.
• Nurse staffing levels
based on acuity –
Daily close
monitoring and
management of
staffing, escalation
process and provision
of cover by Senior
Nursing staff.
• Completion of
staffing
levels/incident
reports forms to
enable analysis of
impact.
• Recruitment in to the
vacant posts is
underway and to
continue under
monitoring.
• Monitoring of KPI’s
• Utilisation of a
partnership model and
secondment
opportunities from
other trusts.
• Recruitment from
abroad
None
Operational
Performance
Risk register
Incident and
Complaint
Risk
734
(EM4)
Nursing vacancies, leadership
and Nursing staffing
recruitment across Medicine
and the ability to provide safe
care
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
Mitigation plan is designed to effect recruitment to agreed staffing complement and reduce reliance on agency staffing,

Page 14 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All clinical
and
Corporate
directorates
Director of
Nursing/Director
of Infection
Prevention and
Control and
Chief Operating
Officer ( for
Delivery)
Quality and
Governance
Committee
20
RED
����
• Systematic monitoring of
performance by Infection
Prevention & Control
Team,
• IC assurance framework
• RCA process used in every
case of MRSA, C.Diff,
MSSA and E Coli.
• Recovery plan and
monitoring report
presented to Board
• District Wide Infection
Prevention and Control
Group Meetings.
• Hospital Infection Control
Committee meetings.
• Zero tolerance approach
to HCAI
• Infection Prevention and
control policies and
procedures
• Antimicrobial Policy
framework and
prescribing policy and
stewardship
• Systematic
monitoring
determines actions
to be taken.
• Trust working to
recovery plan agreed
with CCG and
regulators.
• ICA framework
actions
None
Operational
performance
Patient
Safety
Quality
Incidents
complaints
and claims
Risk
737
(C8)
Also
AF1.7
Healthcare associated infection
prevention (MRSA, C-DIFF,
MSSA, E-Coli) Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 15 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk
Source
CORPORATE All Clinical
and
Corporate
directorates
Medical
Director and
Director of
Nursing
Quality and
Governance
Committee
20
RED
����
• Discharge policy and
procedures in place
• Monitoring of
operational
performance activity
and review of
discharge and transfer
services undertaken.
• Board reporting
• Patient experience
sampling and
monitoring
• Audit programme
• Review during Senior clinician
and/Nursing walk round
• Implementation of processes
to support ward based
intervention and
reconciliation.
• Monitoring of the on-going
usage of Care Bundles
through Patient Safety
Programme
• Implementation of the
Urgent Care Recovery Plan.
• Discharge and patient flow
action plan monitored by
task and finish group
• Board Rounds
None
External
reports
Patient
feedback,
incidents
and
complaints
Risk
743
(C57)
Also
AF1.17
Effective discharge of Patients
ensuring adequate information and
knowledge of medication Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 16 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
and
corporate
directorates
Medical
Director
Quality and
Governance
Committee
20
RED
����
• Health records
standards and policies
in place.
• Professional Standards
for record keeping
• Clinical Coding
Standards
• Clinical Coding
awareness training for
Clinicians.
• Monitoring of coding
completeness and data
quality
• Electronic access to
“intelligence” on best
practice. Electronic
access to Policies and
Protocols.
Development of EPR
• Health Records
Committee
• Clinical audit and
Effectiveness
programme
• Assurance via Clinical
leads and Senior Nurse
walk round/visits
• Assurance from First
Friday visit programme
• Executive Walk round
programme
• NED Walk round
programme.
• Audit programme
None
Operational
Performance
Incidents
Complaints
and Claims
Risk
AF1.13
Failure to comply with the CQC
Essential Standards of Quality and
Safety relating to record keeping Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.
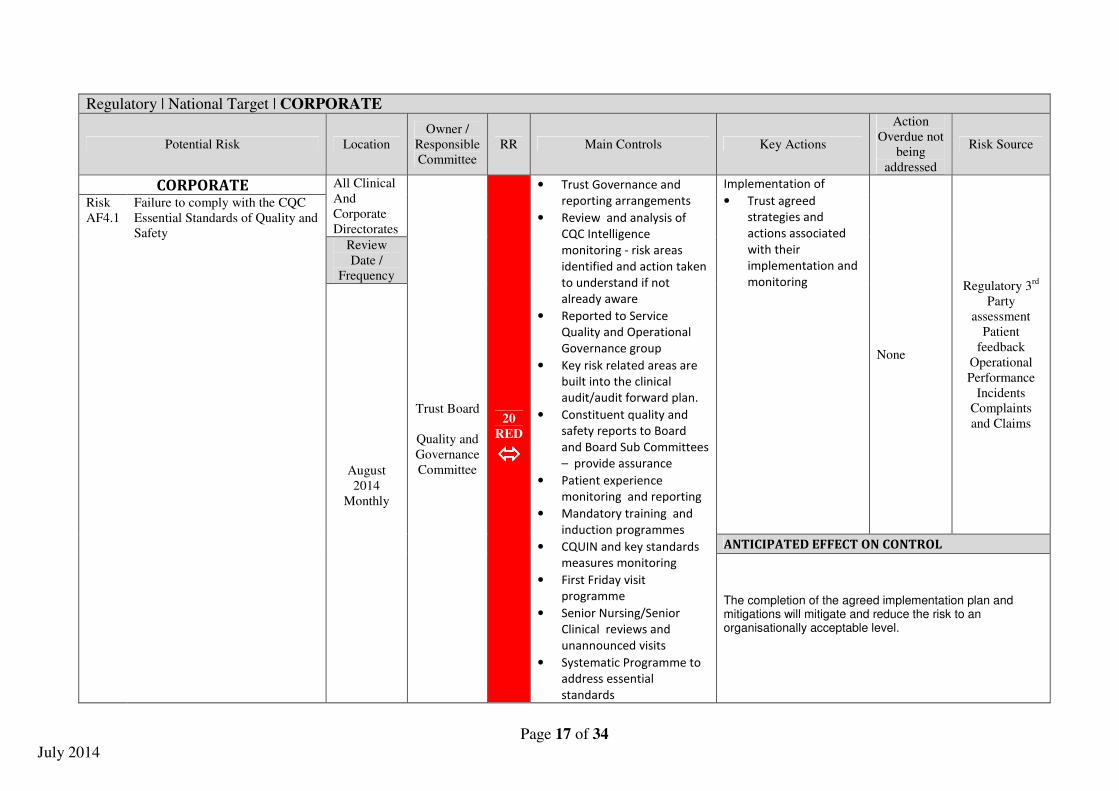
Page 17 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
And
Corporate
Directorates
Trust Board
Quality and
Governance
Committee
20
RED
����
• Trust Governance and
reporting arrangements
• Review and analysis of
CQC Intelligence
monitoring - risk areas
identified and action taken
to understand if not
already aware
• Reported to Service
Quality and Operational
Governance group
• Key risk related areas are
built into the clinical
audit/audit forward plan.
• Constituent quality and
safety reports to Board
and Board Sub Committees
– provide assurance
• Patient experience
monitoring and reporting
• Mandatory training and
induction programmes
• CQUIN and key standards
measures monitoring
• First Friday visit
programme
• Senior Nursing/Senior
Clinical reviews and
unannounced visits
• Systematic Programme to
address essential
standards
Implementation of
• Trust agreed
strategies and
actions associated
with their
implementation and
monitoring
None
Regulatory 3rd
Party
assessment
Patient
feedback
Operational
Performance
Incidents
Complaints
and Claims
Risk
AF4.1
Failure to comply with the CQC
Essential Standards of Quality and
Safety Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 18 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
Directorates
16
RED
����
The Trust has
implemented the interim
controls;
• established a
dedicated validation team
to validate each and every
patient on an incomplete
pathway in order to be
able to report our
incomplete pathway
performance accurately
The Trust:
• Has developed a
comprehensive recovery
plan within a clear project
management and
governance structure to
ensure this problem is
rectified appropriately
within agreed timescales
• Is working with our
Corporate Information
Team to develop a solution
to manage RTT reporting
outside of Lorenzo using
our own data warehouse
• Have informed Monitor
(our regulator) and our
local commissioners of our
current technical problems
None
External
Monitoring,
National
reports,
Operational
performance
Incidents
inquests
complaints
and claims
Risk
3132 Incomplete Referral To Treatment
pathway (RTT) data submission Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and
mitigations will mitigate and reduce the risk to an
organisationally acceptable level.
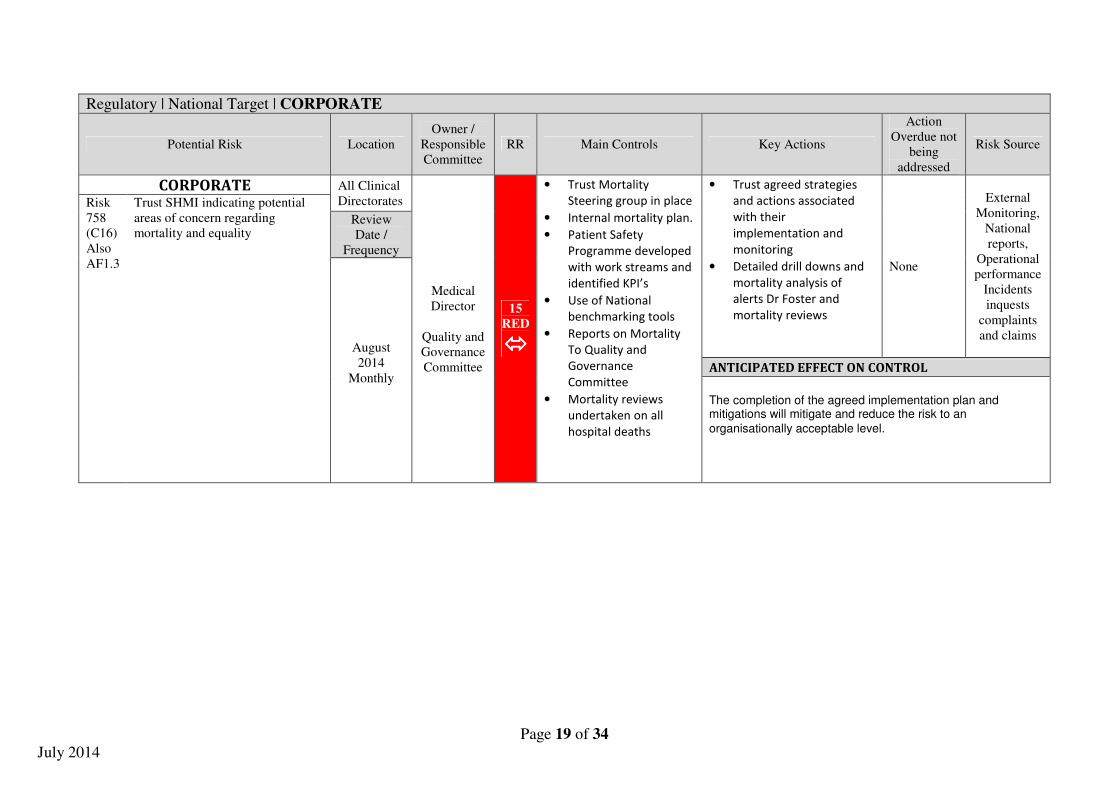
Page 19 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
Directorates
Medical
Director
Quality and
Governance
Committee
15
RED
����
• Trust Mortality
Steering group in place
• Internal mortality plan.
• Patient Safety
Programme developed
with work streams and
identified KPI’s
• Use of National
benchmarking tools
• Reports on Mortality
To Quality and
Governance
Committee
• Mortality reviews
undertaken on all
hospital deaths
• Trust agreed strategies
and actions associated
with their
implementation and
monitoring
• Detailed drill downs and
mortality analysis of
alerts Dr Foster and
mortality reviews
None
External
Monitoring,
National
reports,
Operational
performance
Incidents
inquests
complaints
and claims
Risk
758
(C16)
Also
AF1.3
Trust SHMI indicating potential
areas of concern regarding
mortality and equality Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an
organisationally acceptable level.

Page 20 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location Owner RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE Diagnostic
and
Therapeutic
Chief
Operating
Officer
Executive
Management
Team /
Finance and
Performance
Committee
15
RED
����
• Trust recruitment
strategy to vacancies
• Collaboration with a
Partnership to provide
a long term strategy for
provision of services.
• The Trust has
outsourced reporting
to address service
pressures across
radiology
• Use of waiting list
initiatives for substantive
consultants to help
address shortfall.
• Use of external locums to
support breast service.
• Further recruitment of a
Breast Radiologist being
considered further
• Agency options being
explored.
• Consideration of training
for Breast Surgeon to
perform breast
ultrasound.
None
Operational
Performance
Incidents
Complaints
and Claims
Risk
770
(C53)
Reduced sustainability of
Radiology services due to inability
to recruit to key Radiology posts Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will assist mitigate and reduce the risk to an organisationally acceptable level.

Page 21 of 34
July 2014
•
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk
Source
CORPORATE All Clinical
and
Corporate
Directorates
Medical
Director &
Director of
Human
Resources
Quality and
Governance
Committee
15
RED
����
• Medical Education
coordinated within an
agreed framework
• Monitoring of Deanery
action plan
• Clinical Leaders forum
• Improvement
Programme for doctors
in training.
• Regular scheduled
meetings with Junior
doctor
• Monitoring of incident
reporting and support
for Junior doctors with
reporting- monitored
through Quality and
Governance Committee
• Accessibility of reporting
system - monitored
through Quality and
Governance Dept.
• Analysis of the themes
of reporting included in
the Trust Quality and
Governance Summary
report.
• Deanery Action plan
• Trust agreed strategies and
actions associated with their
implementation and
monitoring
None
Deanery
and Junior
Doctor
feedback
External
review,
incidents,
complaints
Risk
775
(C54)
Failure to ensure the requirements
of the Deanery are being met) and
therefore those doctors in training
receive adequate supervision and
support) resulting in reduced
ability to provide safe care and the
Deanery withdrawing doctors in
training and therefore
unsustainability of services.
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level. .

Page 22 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
Directorates
Director of
Nursing
Quality and
Governance
Committee
15
RED
����
The use of the ROSIER
scoring has commenced as
part of Emergency
Department “React
Process” along with
feedback to clinicians.
Robust breach analysis
and cascade through
specialist teams is now
incorporated into a daily
reporting which is sent to
speciality teams to
respond. In addition the
stroke co-ordinator rota
has been reviewed to
ensure maximum
availability of response to
ED.
The Stroke Action plan is
being reviewed to ensure
it captures the issues
arising from SSNAP Audit
and will be assertively
progressed through the
Trust Stroke Group.
Plans to co-locate the
Acute Stroke Ward (W5)
and Stroke Rehabilitation
Ward (W45) are being
reviewed to ensure that
• Delivery of Consolidated
action plan actions
• Detailed drill downs and
analysis of performance
• Progress against these
actions will continue to
be systematically
monitored and reported
on through the
Divisional and Corporate
structures, by the
Executive teams and
Trust Board
None
External
Monitoring,
National
reports,
Operational
performance
Incidents
inquests
complaints
and claims
Risk 1845
Previously
EM1
Trust fails to achieve national
best practice e.g. Stroke and TIA
pathway, Critical Care Pathway,
NICE, Bundles of Care, NSFs,
Sentinel Audits etc
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 23 of 34
July 2014
the proposed bed
numbers remain correct
and we have the capacity
required.
TIA- the ambulatory
assessment room has now
been completed,
guaranteeing capacity to
assess patients. The
ambulatory TIA pathway
has commenced and is
being audited. Further
work is being undertaken
by the division to consider
how we July be able to
provide partial cover at
weekends the Emergency
Department.
The Critical Care Pathway
is being reviewed to
identify specific areas of
improvement and actions
required.

Page 24 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk Source
CORPORATE All Clinical
and
Corporate
Directorates
Director of
Nursing
and
Medical
Director
Quality and
Governance
Committee
15
RED
����
• Revised Quality and
Governance committee and
reporting structure in place
• Systematic process for review
being implemented
• Patient Safety Programme
developed with key work
streams and KPI’s
• Review and analysis of CQC
QRP risk areas identified and
action taken to understand if
not already aware
• Reported to Service Quality
and Operational Governance
group
• Key risk related areas are built
into the clinical audit forward
plan. These are reviewed an
monitored within key Quality
and Governance
• Constituent quality and safety
reports to Board and Board
Sub Committees – provide
assurance
• Patient experience monitoring
and reporting
• Mandatory training and
induction programmes
• CQUIN Key measures
monitoring
• First Friday visit programme
• Senior Nursing /Clinician
reviews/unannounced visits
Implementation of
• Constituent action
plans
• revised and
strengthened
Governance
Systems
• Organisational
Leadership and
Staffing structures
• Patient Safety
programme
• Patient Experience
programme
• Values and
Behaviour work
streams.
• Oversight by the
Board, EMT and
Quality and
Governance
Committee
Structure
None
Third party
review/
inspection
Operational
Performance,
Incidents,
Complaints,
Claims, Inquests
external reviews
Risk
AF1.1
Assessing and Monitoring
Quality of Service provision
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level. Review process based on regulator assessment

Page 25 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
and
Corporate
Directorates
Director of
Nursing/Medical
Director
Quality and
Governance
Committee
15
RED
����
• Revised Quality and
Governance committee
and reporting structure in
place
• Programme developed
with key work streams
and KPI’s
• Reported to Service
Quality and Operational
Governance group
• Key risk related areas are
built into the clinical audit
forward plan.
• Constituent quality and
safety reports to Board
and Board Sub
Committees – provide
assurance
• Patient experience
monitoring and reporting
• Mandatory training and
induction programmes
• CQUIN measures
monitoring
• First Friday visit
programme
• Senior Nursing reviews
and unannounced visits
• Values and Behaviours
work programme
• Board Reports Assurance
Reports
• Quality Account
Implementation of
• Constituent action
plan
• revised and
strengthened
Governance Systems
• Organisational
Leadership and
Staffing structures
• Patient Safety
programme
• Patient Experience
programme
• Values and
Behaviour work
streams.
• Oversight by the
Improvement board
and Quality and
Governance
Committee Structure
• Ward Accreditation
framework in use
and challenge in
system
None
Third party
review/
inspection
Operational
Performance,
Incidents,
Complaints,
Claims,
Inquests
external
reviews
Risk
AF1.6
Failure to ensure appropriate
focus on privacy and dignity
for patient and relatives Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level. Review process based on regulator assessment

Page 26 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk Source
CORPORATE All Clinical
and Corporate
Directorates
Director of
Nursing
Quality and
Governance
Committee
15
RED
����
• Policies, procedures and
guidelines for children and
adults and constituent policies
impacting upon safeguarding.
• Contractual requirements
against specific standards/
requirements
• Deprivation Of Liberty (DOLS)
arrangements,
• IMCA ( Advocacy arrangements)
• Revised Mental Health Act
infrastructure and partnership
agreement with Pennine Care
• Staff awareness training
• Collaboration with other care
agencies
• Mandatory Training in place.
• Trust fully engaged with child
protection /adult protection
structures.
• Audit Tools and programme.
• Trust is a member of TMBC
Safeguarding Boards
• Specific initiatives on Prevent,
Mental Health and Learning
Disability Work streams, Specific
Unborn and Children's
safeguarding work streams
• Internal Safeguarding Board
established monitoring key
metrics reporting through to
Quality & Governance
Committee
• Increased staff awareness
of safeguarding concerns
• Increase utilisation of
DOLS
• Review of systems and
implementation of Mental
Health act process
agreement in place with
Pennine Care
• Rollout of training plans
• System of receipt of
Mental Health Act papers
to be monitored with
Pennine Care now agreed
None
Operational
management
incidents
safeguarding
concerns
Risk
AF1.9
Also
CR
576
Failure to Safeguard
people who use services
from abuse Review Date /
Frequency
August 2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 27 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk
Source
CORPORATE All Clinical
and
Corporate
Directorates
Director of
Nursing and
Medical
Director
Quality and
Governance
Committee
15
RED
����
• Revised Governance committee
and reporting structures
• Policies and procedures
highlight the standards to be
achieved in respect of the
requirements e.g. handling and
investigating such events-
inquests, claims, incidents and
how associated learning is
disseminated
• External Assessment of claims
by NHSLA
• Coronial Involvement for
Inquests and reporting of deaths
• Systematic process for incident
reporting and handling
• Process for reporting deaths in
place
• Key risk related areas are built
into the clinical audit forward
plan. These are reviewed an
monitored within key Quality
and Governance
• Aggregated learning reports
• Patient experience monitoring
and reporting
• Mandatory training and
induction programmes
• CQUIN measures monitoring
• First Friday visit programme
• Senior Nursing /Clinician
reviews and unannounced visits
Implementation of
• Consolidated/constituent
action plan
• revised and
strengthened
Governance Systems
• Organisational
Leadership and Staffing
structures
• Patient Safety
programme
• Patient Experience
programme
• Values and Behaviour
work streams.
• Oversight by the
Improvement board and
Quality and Governance
Committee Structure
None
External
review
Internal
assurance
systems
Risk
AF1.16
Failure to meet CQC regulation
requirements in relation to
quality & management
incidents & organisational
learning
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 28 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location Owner RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk
Source
CORPORATE All Clinical
Directorates
Medical
Director
Quality and
Governance
Committee
15
RED
����
• Clear procedure and
training in place
• Policies and guidelines
outline expected
standards and process of
audit enables monitoring
of these
• Consultant Staff required
to appraise Juniors on
skills and knowledge
• Medical Director’s
annual appraisal of
senior medical staff
• Professional staff where
delegated consent in
place required to have
appropriate competency
checks and supervision
• Clinical Audit Programme
• Increased staff
awareness of
safeguarding concerns
• Increase utilisation of
DOLS
• Review of systems for
implementation of
Mental Health Act has
taken place
• Focussed consent
programme to be
redeveloped via Patient
safety officers. Task
and finish work stream
reporting through to
Quality and
Governance
None
External
third party
review ,
patient
feedback
and
incidents
complaints
and claims
Risk
AF1.18
Failure to ensure requirements for
consent to treatment Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level. Anticipated date for reduction of risk score to below 15 Quarter 4, 2014/15 Review process based on regulator assessment

Page 29 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk
Source
CORPORATE All Clinical
and
Corporate
Directorates
Director of
Human
Resources
and Director
of Nursing
and Chief
Operating
Officer
Quality and
Governance
Committee
15
RED
����
• Annual Mandatory
Training requirements
and review annually of
training needs analysis
• Induction process
• Education Governance
Group to coordinate
and systematically
apply educational
governance
• Delivery of the
consolidated action
plan
• Education Governance
Group Work streams and
Plan
• Training plan aligned to
OD strategy
• Divisional ownership and
actions to be
strengthened further
None
External
review and
internal
monitoring
Risk
AF1.22
Failure to ensure that staff have the
relevant mandatory skills and
training to ensure safe practice.
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 30 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
and
Corporate
Directorates
Director of
Human
Resources
Chief
Operating
Officer
Executive
Management
Team/ Trust
Board
15
RED
����
• Workforce planning
and recruitment
strategy.
• Nurse staffing levels
based on acuity – Daily
close monitoring and
management of
staffing, escalation
process and provision
of cover by Senior
Nursing staff.
• Completion of staffing
levels/incident reports
forms to enable
analysis of impact.
• Introduction of
Divisional Governance
support.
• Recruitment from
abroad has informed
our plans
• Implementation of the
Consolidated action
plan and oversight by
Improvement board
• Trust wide Consolidated
action plan and
implementation
monitored through
Improvement board
• Recruitment in to the
vacant posts is underway
and to continue under
monitoring.
• Weekly monitoring of
KPI’s
• Utilisation of a
partnership and
secondment
opportunities from other
trusts.
None
Third party
review and
internal
monitoring
Incidents
complaints
Claims and
Operational
performance
and impact
Risk
AF1.23
(AF1.21)
Failure to ensure adequate
staffing levels to ensure patient
safety and quality of services Review
Date /
Frequency
August
2014
monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 31 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
Directorates
and
Divisions
Chief
Operating
officer
Executive
Management
Team
Finance and
Performance
Committee
15
RED
����
• Capacity Plans in place
• Demand Management
implications are being
implemented.
• Regular meetings with
CCG and other partners
to improve availability
of, and access to,
intermediate care beds.
• Risk assessments are
completed for any areas
used for escalation.
• Patients are required to
be appropriately risk
assessed before being
admitted to escalation
areas.
• Partnership working with
other providers to
ensure a long term
strategy is in place
regarding sustainability
and service provision.
• Development of
integration strategy in
key partners
• Implementation of
workforce action s in
consolidated action
plan monitored by
Improvement board
None
Third party
review and
internal
monitoring
Incidents
complaints
Claims and
Operational
performance
Risk
AF1.24
Increased demands beyond
predicted levels which is outside
current capacity Review
Date /
Frequency
September
2014
Quarterly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 32 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue
not being
addressed
Risk Source
CORPORATE All Clinical
and
corporate
Directorates
Director of
Nursing
Quality and
Governance
Committee
15
RED
����
• Complaints procedure is
in place and widely
publicised and available
– positive and negative
feedback is encouraged
• Complaints sign off by
CEO
• Complaints and PALS
processes are
divisionally supportive
and operationally
managed centrally in
the Trust Quality and
Governance Unit
• Routine Board reporting
• Detailed reports to
Quality and Governance
Committee
• Divisions routinely
receive detailed
information re
complaints and issues
identified
• Service Quality and
operational Committee
receives assurance and
aggregated learning
reports
• Quality and Governance
Committee receives
assurance and
aggregated learning
reports
•
• Internal Complaints review
continuously taking place.
• Independent review of
complex complaints.
• Complaints management
training package is being
delivered to patient-facing
managers / senior
clinicians Additional
resources addressing
historical outstanding
issues
• Revised process and
actions to be implemented
None
Third party
review and
internal
monitoring
Incidents
complaints
Claims and
Operational
performance
Risk
AF1.25
Failure to fulfil CQC
requirements with management of
Complaints Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 33 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
and
corporate
directorates
Chief
Operating
officer
Improvement
Board
15
RED
����
• Capacity Plans in place
• Demand Management
implications are being
implemented.
• Regular meetings with
CCG and other
partners to improve
availability of, and
access to,
intermediate care
beds.
• Risk assessments are
completed for any
areas used for
escalation.
• Patients are to be
appropriately risk
assessed before being
admitted to escalation
areas.
• Partnership working
to ensure a long term
strategy is in place
regarding
sustainability and
service provision.
• Development of
integration strategy in
conjunction with Key
partners
• Implementation of
workforce action s in
consolidated action plan
monitored by
Improvement board
None Operational
performance
Risk
AF4.6
Failure to minimise delayed
transfers of care
Review
Date /
Frequency
August
2014
Monthly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and mitigations will mitigate and reduce the risk to an organisationally acceptable level.

Page 34 of 34
July 2014
Regulatory | National Target | CORPORATE
Potential Risk Location
Owner /
Responsible
Committee
RR Main Controls Key Actions
Action
Overdue not
being
addressed
Risk Source
CORPORATE All Clinical
and
corporate
directorates
Chief
Operating
officer
Executive
Management
Team and
Trust Board
15
RED
����
• IM&T team reporting
the Chief Operating
Officer reporting to an
identified Executive
Director – Director of
Finance with policy
and procedures and
operating framework
to National Standards
• Development of
technology
infrastructure through
capital programme
• Revised IM&T strategy
• Review of resources
• Consistency to address
any gaps in controls
• IM&T Committee and
supporting Committees
to be strengthened and
re-established post
Lorenzo go live to ensure
systematic reporting of
IM&T assurances through
to Board
• Infrastructure to be
proposed and progressed
in line with Governance /
Committee Review
None Operational
performance
Risk
AF4.8
Failure to have in place a IM&T
infrastructure and Service
supporting organisational
objectives Review
Date /
Frequency
September
2014
Quarterly
ANTICIPATED EFFECT ON CONTROL
The completion of the agreed implementation plan and
mitigations will mitigate and reduce the risk to an
organisationally acceptable level.

PART 1
AGENDA ITEM 12 Title of Board paper
Safe Staffing Report June 2014
Board meeting date 25th July 2014
Purpose
To provide the Board with an update on the safe staffing of wards.
Actions Recommended
Discussion / Noting / Decision
Publication
This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms
TGH Tameside General Hospital NHSP NHS Professionals ITU Intensive Therapy Unit CCU Critical Care Unit NICE National Institute of Clinical Excellence AUKUH Association of UK Hospitals
Any communications actions after the meeting
Report of John Goodenough - Director of Nursing
Paper prepared by
Anne Alison – E rostering Project Nurse

2
Safe Staffing Update Report
1. Purpose In-line with the ‘Hard Truths Commitments Regarding the Publishing of Staffing Data’, the Trust Board is required to review staffing data on a monthly basis. The aim of this report is to provide the monthly update on the continuing actions and developments to support safe staffing. 2. Current Position The second UNIFY upload of TGH Staffing Data for June occurred on 15th July and will be published via NHS Choices. This data is currently available via our public website in a specific designated section ‘Safe Staffing’. Tameside Hospital - Nurse Staffing (www.tamesidehospital.nhs.uk/nurse-staffing.htm) 3. June 2014 Staffing Each month the data collection compares the number of staff hours ‘Planned’ against the number of staff hours used ‘Actual’. This is collected by ward, by shift, and is reported by calendar month as a % fill rate by day and by night: Appendix 1 Provides a summary of the June position. It has been suggested that in the future a RAG rating will be applied to the results, but this has yet to be clarified by NHS England. The overall Trust position for June is:
Day Night
RN/RM Average Fill rate 91.7 % (74 – 100.5%) 96.4% (84.4 – 108.3%)
Care Staff Average Fill rate 112.1% (80.4 – 151.2%) 119.9% (96.7 – 166.7%)
0
20
40
60
80
100
120
140
May-14 Jun-14 Jul-14
% F
ill
Rate
Average Fill Rates
RN Fill DAY
RN Fill NIGHT
Care Staff FillDAY
Care Staff FillNIGHT

3
4. Exception Report The exception report looks at the information broken down by the two key staff groups Registered Nurse / Midwife and Care Staff Registered Nurse/Midwife 7 areas are reporting <85% fill rates for Registered Nurses (RN). These are : Area Fill (%) Comments
Surgical Unit 83.4% Day 2.42wte Sickness & Mat Leave
Ward 5 74% Day 2.1wte Vacancies AP bridges RN requirements but is reported in Care Staff %
Ward 43 79.7% Day 3.0wte vacancies 1.54wte sickness
Ward 44 80.4% Day 3.3wte vacancies 1.16wte sickness
Ward 46 80.4% Day 1.5wte vacancies 1.01wte sickness
WHU 81.4% Day 0.63wte Establishment currently under review
The main reasons for the shortfalls are current vacancies, sickness, maternity leave, supernumerary staff and special leave. Table1 (above) illustrates the main reasons for the low fill-rates (1.0wte equates to 150hrs over a 4-week period). All staffing shortfalls are requested to be filled utilising NHS Professionals with a current NHSP/Agency fill rate of 70.4% for Registered Nurse shifts. Care Staff – Nursing Assistants The majority of areas are reporting fill rates of greater than 100%. The reason for this is due to the number of additional staff requested for 1:1 patient care/specialling due to patient acuity and safety needs. Areas needing additional 1:1 care staff will always report >100% fill rates as these additional staff are not accounted for in the ‘Planned’ staffing numbers as they are not part of the funded and planned staffing establishments due to the adhoc and unpredictable demand. ‘Specialing’ currently accounts for 17% of all Temporary Staffing requests made by the Trust. 5. Actions to address shortfalls All vacancies are currently being advertised and/or are in the process of being actively recruited to, with a trajectory for full recruitment by September 2014.

4
16 International recruits are currently in-post undertaking an enhanced induction/competency programme. These staff should be included within the RN establishments from August/September 2014. Temporary staffing requirements are requested through NHS(P), with escalation to Agency as per the Trust policy. Current NHSP/Agency fill rate is 89.9% for unqualified shifts and 70.5% RN shifts. Incident reports submitted in relation to staffing shortfalls are monitored and addressed divisionally. The table below illustrates no significant increase in incidents reported relating to nursing staff shortfalls:
Staffing issues Mar Apr May Jun
Staffing - Lack Of Nursing Staff 23 17 21 25
Staffing - Lack Of Medical Staff 1 3 4 5
Staffing - Lack Of Other Staff 3 4 4 2
Staffing - Improper Delegation -Unsupervised Staff
2 1 0 0
Grand Total 29 25 29 32
Further work is required/on-going in certain areas to review staffing requirements against current establishments:
• Maternity, Women’s Health Unit, - review underway in relation to clinic staffing, rotation of staff and working across community, led by Head of Midwifery
• ITU,/ MHDU and CCU – proposal to manage patient flows differently and align Cardiology with CCU and merge ICU/MHDU will inform the staffing establishments going forward, and address any shortfalls. This was highlighted as an area of work that needed to be undertaken following the Acuity & Dependency review in February 2014 as referenced in the Board Paper of 29th May 2014.
There has also been a review of the AUKUH staffing tool in relation to Medical Assessment Units which has been used to inform our current MAU establishment in the recent acuity and dependency data collection. The full results of the most recent Acuity & Dependency review will be reported in the next Board Report. NICE published their guidance on ‘Safe Staffing for nursing adult inpatient wards in acute hospitals on 15th July 2014. Work is currently underway to benchmark the Trusts current position against the NICE recommendations.

5
6. Recommendations The Trust Board is requested to receive this update and note the processes that are in place for safe staffing to support the delivery of a high quality care to our patients
Mr John Goodenough Director of Nursing July 2014

6
Appendix 1 : Safe Staffing Data June 2014
June-14 Planned Staff Vs Actual
Comments WARD SPECIALTY SHIFT
Registered Staff
Care Staff
Elective Unit General Surgery
Day 96.3% 104.9% • Additional staff booked for escalation area and 1:1 care.
Night 108.3% 166.7%
Surgical Unit
General Surgery
Day 83.4% 131.4% • Long-term patient requiring 1:1
care.
• Additional staff booked for escalation area.
• 2.42wte RN Sickness & Mat Leave
Night 101.7% 130%
Trauma Unit Trauma &
Orthopaedics
Day 95.7% 111.1%
Night 96.7% 105.8%
ITU Critical Care
Medicine
Day 95.9% 90%
Night 98.7% Not
Applicable
Ward 5 General Medicine
Day 74% 93.9% • AP in-post bridges RN/Care
Staff requirements, inc in Care Staff %
• 2.1wte RN vacancies
• 5.64wte Care Staff vacancies/sickness
• 1.0wte International Recruit *
Night 100% 100%
Ward 30 General Medicine
Day 100.5% 111.3% 1.0wte International Recruit *
Night 100% 116.7%
Ward 31 General Medicine
Day 88.4% 99.4% • 2.0wte International Recruit *
• 2.8wte RN vacancies
• 0.82wte RN sickness Night 93.3% 106.7%
MAU General Medicine
Day 98.1% 96.2%
Night 91.4% 95.3%
CCU General Medicine
Day 99.4% 87.3% 1.74wte Care Staff vacancies
Night 100% Not
Applicable
Ward 40 General Medicine
Day 96.9% 128.7% 2.0wte International Recruit * 1.2wte RN vacancies
Night 87.8% 155%

7
May-14 Planned Staff Vs Actual
Comments WARD SPECIALTY SHIFT
Registered Staff
Care Staff
Ward 41 General Medicine
Day 90.1% 130.8% • AP in-post bridges RN/Care Staff requirements, inc in Care Staff %
• 2.0wte International Recruit *
• 0.7wte RN vacancies
• 1.98wte RN Sickness/Mat Leave
Night 85.6% 160%
Ward 42 General Medicine
Day 96.2% 110.9% 2.0wte International Recruit * 1.4wte RN vacancies 0.53wte RN sickness Night 84.4% 123.3%
Ward 43 General Medicine
Day 79.7% 132.2% • 2.0wte International Recruit *
• 3.0wte RN vacancies
• 1.54wte RN sickness Night 100% 108.3%
Ward 44 General Medicine
Day 80.4% 151.2% • 1:1’s for patient safety (dementia ward) & supporting RN shortfall
• 2.0wte International Recruit *
• 3.3wte RN vacancies
• 1.16wte RN sickness
Night 98.3% 130%
Ward 45 General Medicine
Day 85.8% 98.4% • 0.7wte RN vacancies
• 1.97wte RN sickness
Night 100% 110%
Ward 46 General Medicine
Day 80.4% 143% • 2.0wte International Recruit *
• 1.5wte RN vacancies
• 1.01wte RN sickness Night 100% 156.7%
Maternity Ward 27
Obstetrics Day 100.4% 89.9%
• 2.89wte care staff vacancies
• 1.17wte care staff sickness
Night 95.2% 96.7%
Women’s Health Unit
Gynaecology Day 81.4% 128.9% • 0.63wte Maternity Leave
Establishment currently under review
Night 96.7% Not
Applicable
NICU Obstetrics Day 91.7% 80.4% • 0.56wte RN vacancies
• 2.54wte RN sickness
Night 100% Not
Applicable
Children’s Ward
Paediatrics Day 98.8% 92.2%
Night 102.7% Not
Applicable

PART 1
AGENDA ITEM 13
Title of Board paper
Patient Experience Update
Board meeting date Thursday 31st July 2014
Purpose
To provide the Board with an update and an overview of the work to date that is focusing upon the Patient Experience.
Actions Recommended
Discussion / Noting / Decision
Publication
This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms FFT – Friends and Family Test
Any communications actions after the meeting
Cascade to divisional and operational forum as appropriate.
Report of Mr John Goodenough, Director of Nursing
Paper prepared by
Lindsay Stewart, Interim Deputy Director of Nursing Helen Howard, Head of Patient Experience
2
Patient Experience Update Purpose
To provide Trust Board with an update and overview of the work to date that is
focusing upon the Patient Experience.
Discussion
Delivering a high-quality experience for patients should, without question, be a
priority for all NHS organisations. This will become increasingly important as the NHS
operates in an ever-more dynamic environment, with patients’ expectations
increasing.
Patients, carers and families utilising our services at TGH have a right to experience
the best care by a Trust that listens to their voice and demonstrates that patient and
family experience is at the heart of the care we provide and is a key measure of
patient care.
As part of the Trusts Quality Improvement Strategy, patient experience forms one of
the quality drivers with the aim that all patients will receive high quality care that is
tailored to their individual needs, which we will be monitored through the delivery of
the Patient Experience Strategy.
This paper will provide an update on how we are monitoring the experiences of our
patients though the following processes.
The Friends and Family test
This is measured by asking patients across A&E, inpatient areas and Maternity a set
question;
“How likely are you to recommend our ward, department or service to your friends
and family if they needed similar care or treatment?”

3
Responses are collected in various ways, cards, volunteers – tablet, internet, SMS
texting service (piloted for 3 months) and are collated on a monthly basis. There is a
2014/15 FFT national CQUIN which requires a response rate for A&E of 15% to be
achieved by the end of Quarter 1 and to maintain improvement.
Table 1 below shows our current position for all areas A&E, Inpatient, Combined (IP
& A&E) and Maternity.
A&E FFT
In May the response rate for A&E reached 26.4% Table 2 shows how we are
performing in A&E in relation to the specific questions, with 82.7% scoring extremely
likely or likely to recommend the department.

4
The chart below demonstrates our position for A & E across Greater Manchester and
England. It is clear work needs to continue to ensure we are capturing feedback for
A&E.
Friends and Family Test - A&E Departments (Type 1 and 2)Friends and Family Test submissions by trust
May 2014
NameTotal
Responses
Total
Eligible
Response
Rate
Friends
and Family
Test Score
Extremely
LikelyLikely Neither Unlikely
Extremely
Unlikely
Don't
Know
England 137,471 721,251 19.1% 54
(63.4%)87
286 31,003 6,030 3,698 5,762 3,692
BOLTON NHS FOUNDATION TRUST 1,155 6,185 18.7% 56 (66.9%)773 227 59 30 46 20
CENTRAL MANCHESTER UNIVERSITY HOSPITALS NHS FOUNDATION TRUST 1,892 9,741 19.4% 60 (69.9%)1324 331 68 50 90 29
PENNINE ACUTE HOSPITALS NHS TRUST 4,205 12,499 33.6% 51 (57.2%)2409 1,123 198 75 133 267
SALFORD ROYAL NHS FOUNDATION TRUST 1,169 4,136 28.3% 59 (68.7%)804 215 63 27 39 21
STOCKPORT NHS FOUNDATION TRUST 722 4,172 17.3% 41 (55.4%)400 203 54 22 32 11
TAMESIDE HOSPITAL NHS FOUNDATION TRUST 1,101 4,165 26.4% 38 (53.4%)589 322 74 46 57 13
UNIVERSITY HOSPITAL OF SOUTH MANCHESTER NHS FOUNDATION TRUST 770 4,440 17.3% 58 (69.3%)534 109 35 33 36 23
Breakdown of Responses

5
Thematic analysis for A&E FFT.
As part of the feedback process there is a free text component. The analysis has
identified themes and feedback has been given to the Divisions for them to
implement changes as appropriate. This month the feedback has been very positive
with key themes being caring; professional, friendly, courteous, staff; prompt
treatment; helpful, supportive and informative staff; excellent doctors and
nurses; porter and all staff fantastic; first class, excellent service. The areas of
concern are generally waiting times but an acknowledgement form the department
that May had a particularly high number of attendees to the department.
Inpatient FFT Survey analysis.
The inpatient survey response rates no longer remain a CQUIN target for 2014/15,
although the FFT element of the survey remains in place with a target of 25% by the
end of quarter 1. Table 3 highlights the inpatient response rate for May was 42.3%.
The chart below demonstrates our inpatient position in comparison to Greater
Manchester and the England FFT results. When calculating the combined responses

6
of extremely likely and likely scores, TGH achieved 93.9% compared to 94.4% for
England and 94.2% for Greater Manchester.
Analysis of the themes from the heat maps for inpatients continues to demonstrate
that noise at night remains a key theme. All areas have been reminded to discuss at
ward meetings the findings from the feedback.
The heat map below represents the question asked with Q19 identifying a consistent
theme relating to noise at night.
Friends and Family Test - InpatientFriends and Family Test submissions by area
team
May 2014Unify2 Data Collection - FFT_IP
NameTotal
Responses
Total
Eligible
Response
Rate
Friends and
Family Test
Score
Extremely
LikelyLikely Neither Unlikely
Extremely
Unlikely
Don't
Know
England (including Independent Sector Providers) 124,169 346,223 35.9% 74 (75.6%)93973 23,228 2,572 880 984 2,532
England (without Independent Sector Providers) 118,552 334,095 35.5% 73 88,899 22,748 2,545 876 961 2,523
Greater Manchester Area Team 7,266 18,855 38.5% 77 (77.4%)5630 1,215 120 51 42 208
Tameside Hospital Foundation Trust 459 1,086 42.3% 66 (70.5%)324 107 13 5 6 4
Breakdown of Responses

7

8
Maternity service FFT Maternity Services response rates have remained static in May, with an overall
response of 24.9%. Further work needs to continue in increasing the response rates
for Maternity. The card redesign is being discussed with the division to ensure it
meets the needs of the service.

9
Maternity services has comparison with England and Greater Manchester
demonstrates an improved position with an improved response rate, an improved net
promoter score and combined responses of extremely likely and likely scores,
achieving 97.4% compared to 94.1 % for England and 97.2% for Greater
Manchester.
Friends and Family Test - Maternity Friends and Family Test
submissions by area team
MAY 2014
NameTotal
ResponsesTotal Eligible
Response
Rate
Friends and
Family Test
Score
Extremel
y LikelyLikely Neither Unlikely
Extremely
Unlikely
Don't
Know
England 8,573 51,905 16.5% 67
(69.3%)
5946 2,128 177 83 58 181
Greater Manchester Area Team 481 2,912 16.5% 70 (70.6%)340 128 5 0 1 7
Tameside Hospital Foundation Trust 189 760 24.9% 80 (81.4%)154 30 4 0 0 1
Breakdown of Responses

10
Additional Surveys
A number of additional surveys have been created within the Meridian real time
monitoring system to further gather patient experience relating to this month. These
include :
• audiology,
• breast care services,
• learning disabilities services,
• children’s community nursing team,
• hospital alcohol liaison service.
The individual departments are able to access the data from the system and the plan
going forward, is for these to be monitored at local level through the clinical
governance structures with divisional representatives to report the outcomes and
learning to the patient experience group.
Voluntary Services THFT have a large number of volunteers who contribute on a daily basis to the
operational aspects of the hospital. There are currently 420 volunteers registered
with the hospital.
The voluntary services have implemented the Dining Companions project with formal
training taking place in May. Volunteers are now on two wards in Ladysmith who are
piloting the project.
The plan going forward is to increase the number of Dining Companions to give
every ward access to this service.

11
Ward bed side booklet Plans are in progress to develop an up to date bedside booklet that provides relevant
information for all our inpatients across the Trust. This A5 wipe able booklet will be
available for every in patient and it is hoped this project will be supported by the
League of Friends.
Open and Honest care
The Trust continues to report as part of the open and honest care programme which
publishes on monthly basis information relating to three key categories: safety,
experience and improvement. As well as publishing data relating to FFT, HCAI‟s,
Safety Thermometer, pressure Ulcers and Falls we also use patient stories as an
essential tool to improving the care received by the patients and their families. Each
month a patient story is published alongside an improvement story for the Trust. As
the programme has developed we have tried to link the two together and last month
we used the Hospital Alcohol Liaison service with a patient who had received care
from the team. Formal evaluation of the programme has been commissioned by
NHS England, and THFT will be part of the evaluation with the research being
undertaken by Edge Hill University. The proposed start date is June 2014 with
completion scheduled for December 2014
Local College Engagement
The Trust has been working with Tameside College to facilitate placements for the
year 2 Health and Social Care students. The first cohort of students will commence in
September 2014.
Design and creation of a Dementia friendly garden located in Ladysmith courtyard
area has commenced in partnership with Cofley and Tameside College – art
students. The plan is shown below. It is hoped this will be open in early summer.

12
Ladysmith Building – Sensory Garden Plan
• Trellises / Hanging Baskets - to be placed between the green plant pots (alternately) on each section of brickwork.
• Where green plant pots go the paving slabs will be removed and pots lowered in with stone placed around the bases.
• Refurbished benches will be positioned in the seating areas.
• The centre piece will be a piece of imitation grass and possibly a central feature.
• Gaps between pathways can be filled at a later date.
Patient and Carer feedback from Carer’s supporting a relative with Dementia
The Dementia Strategy supports the ongoing work with Carers of patients with
Dementia. To develop our partnership working going forward with the Tameside
Carers Action group, the Dementia Specialist nurse attends their meetings on a
Concrete pots
Trellis
Hanging
baskets
Grassed area
Sitting areas
Defined path
ways (wheel
chair width+)

13
quarterly basis to gain feedback around the care and support we provide to patients
with dementia from a Carers perspective. We continue to undertake the Carer’s
survey following the discharge of a family member as another method of obtaining
feedback.
Although the responses continue to be small in number it is important to monitor the
returns and continue supporting carer engagement.
Date Chann
el
Pleas
e tell
us
how
old
the
patie
nt is:
Please
tell us
how
old you
are:
What
ward(s
) were
they
on?
Did they
always
have the
help they
needed
to eat
and
drink?
Were you
involved
as much as
you
wanted to
be in
decisions
about
their care
and
treatment?
Did you feel
that the
patient was
treated with
dignity and
respect?
Did you
know who
to speak to
about their
care and
treatment?
Was
the
hospita
l
enviro
nment
clean
and
tidy?
As a carer of a
person with
Dementia who
is in hospital,
did you feel
adequately
supported
during their
hospital stay?
06/05/2
014 Web 80+ 40 - 64
Ward
41 No No
Yes,
sometimes
Yes,
sometimes Good No
12/05/2
014 Web 80+ 80+
Ward
41
Yes,
always
Yes,
always Yes, always
Yes,
always
Very
good Yes, always
27/05/2
014 Tablet 80+ 65 - 69
Ward
44
Yes,
always
Yes,
sometime
s Yes, always
Yes,
always
Very
good Yes, always
29/05/2
014 Tablet 80+ 65 - 69
Ward
41
Yes,
sometim
es
Yes,
sometime
s
Yes,
sometimes
Yes,
sometimes Good
Yes,
sometimes
Tameside Safety and Quality Accreditation Standards
The Accreditation standards assessment process has now been rolled out in a
phased approach. A team of Senior Nurses and representatives from the Quality &
Governance unit have supported the assessment process across all the wards with
the exception of NICU. The outcomes of the Children’s assessment is currently being
validated

14
Tameside Safety and Quality Accreditation Heat map
Org
an
isa
tio
n
an
d
Ma
na
ge
me
nt
of
the
Cli
nic
al
Are
a
Sa
feg
ua
rdin
g p
ati
en
ts
Pa
in M
an
ag
em
en
t
Pa
tie
nt
Sa
fety
En
vir
on
me
nta
l S
afe
ty
Nu
trit
ion
a
nd
Hy
dra
tio
n
En
d o
f L
ife
Ca
re
Me
dic
ine
s
Ma
na
ge
me
nt
Pe
rso
n C
en
tere
d C
are
Pre
ssu
re U
lce
rs
Eli
min
ati
on
Co
mm
un
ica
tio
n
Infe
ctio
n C
on
tro
l
Ov
era
ll S
core
Ward 1 2 3 4 5 6 7 8 9 10 11 12 13
Ward 30 Ambe
r
Ward 31 Red
Ward 40 Red
Ward 41 Ambe
r
Ward 42 Red
Ward 43 Red
Ward 44 Red
Ward 45 Red
Ward 46 Red
Ward 5 (ASU) Red
MAU Red
Elective Unit Ambe
r
Surgical Unit Ambe
r
Trauma unit Ambe
r
WHU Ambe
r
CCU Ambe
r
ITU Ambe
r
A&E Ambe
r
Maternity Ambe
r
Children’s Unit
The heat map identifies the outcome against the 13 standards for all areas that have
been assessed. Discussion at the Nursing and Midwifery Leaders Forum will review
the learning from the assessment programme and start planning the next
reassessment.

15
The Ward Leaders all have action plans for their wards and it is expected that
improvement across all areas should be demonstrated. The Accreditation
programme will now have a rolling timeframe for assessment and reassessment
based on the wards overall level of achievement. The aim is to have “Elite” wards by
end of 2015.
This work now provides a ward accreditation scheme that gives assurance to the
Trust Board, Commissioners and other external inspectors that the provision of
quality care delivered to our patients is assessed and monitored using the Tameside
Safety and Quality accreditation standards as a mechanism to drive up quality.
Summary
Patient experience is so much more than just undertaking surveys and seeking
opinion it is about a way of monitoring the quality of care we give to our patients
through the feedback that we collect. The themes that are identified via the feedback
together with the information we collect in relation to complaints and PALS will give
clinical areas, wards and departments a broader spectrum of information which
together with the performance data will allow them to enhance and improve the
quality of care our patients at TGH receive.
Recommendation
The Trust Board is requested to receive this update and note the processes that are
in place to support the delivery of a high quality experience for patients, families and
carers at TGH.
John Goodenough
Executive Director of Nursing
July 2014

16

1
PART 1 AGENDA ITEM 14
Title of Board paper
Mandatory Training
Board meeting date 31st July 2014
Purpose
To appraise the Board of the position with regards Mandatory Training and improvements in order to ensure compliance against the Trust target of 95%
Actions Recommended
To note the contents of the paper.
Publication
This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms DOL’s – Deprivation of Liberty
Any communications actions after the meeting
To communicate any comments from the Board to the Divisional Teams. TO follow up with Divisions achievement against plans submitted.
Report of Amanda Bromley, HR Director
Paper prepared by Amanda Bromley, HR Director

2
Mandatory Training
Introduction
The purpose of this Board report is to inform the Board of improvements to the
Mandatory Training target.
The current target for Mandatory training is 95%. Mandatory Training is made up of 3
elements – each with an individual target of 95%.
These elements include:
1) The Work Book which includes
• Information Governance, • Infection Prevention and Control for non-clinical staff • Health and Safety, • Safeguarding Children Level 1 • Safeguarding Adults Level 1, • Moving and Handling Level 1, • Equality & Diversity
2) Face to Face Sessions – Manual Handling, Infection Prevention, Resuscitation,
Fire, Conflict Resolution
3) E-Learning – a mixture of national e-learning packages and local packages are in place
The Work Book is a paper based workbook designed to offer a flexible way in which to meet the necessary levels of mandatory training required by Tameside Hospital NHS Foundation Trust. It is recognised by the Trust that releasing staff for face to face sessions on an annual basis is increasingly difficult. The Work Book therefore replaces the need for some staff to attend the face to face Mandatory Training sessions. In principle the workbook is an ideal mechanism for meeting the required levels of mandatory training however in practice the quality of the workbook is poor and training and learning outcomes cannot be measured. Whilst e-learning is proving a useful tool to aid the completion of Mandatory Training,
there are issues with not all staff having access to a Trust e-mail account and access
to a computer.
Known Challenges
At a time when assurance and compliance with standards are required there are
many competing demands for what is known as ‘Mandatory’ training. The list of
training for staff groups to complete training on either an annual or bi-annual basis in

3
associated fields is ever growing e.g. DOLs, Falls, Dementia, Prevent, Conflict
Resolution,
The many Mandatory training elements are not all managed by the Education Team
and therefore the processes for ensuring Mandatory training is recorded on the
central OLM system are not always in place and therefore the issue of data capture
and accuracy is a known challenge.
Currently the Education and Training team are reviewing the process of identifying
who needs what training, the OLM system can capture the ‘competencies’ required
so that accurate systems can be put in place to ensure reminders can be sent to
Managers to identify which staff need the training and when.
Managers receive a monthly email detailing each staff member and the dates their
Mandatory Training is required – staff are RAG (Red, Amber, Green) rated as to their
compliance. Any staff member deemed as Amber is recognised as needing to book
on a session or complete an e-learning package or the workbook. A staff member
showing red is deemed to be non-compliant. Managers are asked to focus on the
staff showing as amber.
As the reports are circulated a month behind the current month, the reports are often
challenged by Managers as not being accurate – real-time recording and reports is
not available unless the Trust chooses to implement Manager/Employee self-service.
The current rates for Mandatory training are identified in the table below:
Mandatory Training
Workbook Target Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Jun-14
Emergency
Services &
Critical Care
95% 86.5
%
87.6% 90.8% 87.8% 90.5% 88.6% 81.4% 77.0% 81.3% 79.9% 84.2% 80.5%
Elective
Services
95% 81.4
%
84.0% 85.3% 91.5% 93.2% 92.2% 87.2% 84.4% 83.9% 79.9% 82.9% 84.4%
Womens
Services
95% 70.9
%
73.5% 79.6% 86.1% 93.8% 95.1% 90.8% 88.1% 91.6% 84.9% 88.0% 88.5%
Childrens
Services
95% 74.6
%
76.6% 81.3% 83.0% 86.1% 87.2% 88.1% 85.9% 81.5% 87.6% 87.6% 87.8%
Diagnostic &
Therapeutic
95% 92.0
%
88.5% 89.1% 89.7% 92.9% 90.6% 90.9% 91.8% 91.2% 88.8% 91.6% 92.2%
Facilities 95% 91.2
%
95.6% 94.6% 98.3% 99.1% 98.3% 87.7% 93.1% 92.2% 97.5% 99.2% 93.0%
Corporate 95% 92.5
%
92.4% 95.3% 94.4% 94.2% 94.2% 91.7% 94.0% 91.3% 91.4% 91.1% 90.9%
Tameside
NHS Trust
95% 84.7
%
85.6% 88.2% 89.5% 92.0% 91.0% 86.7% 85.2% 85.9% 84.4% 86.9% 85.9%
Manual Handling
Target Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Jun-14
Emergency 95% 92.1 90.8% 88.2% 89.3% 89.6% 90.2% 89.6% 89.8% 90.1% 89.1% 88.2% 87.8%

4
Services &
Critical Care
%
Elective
Services
95% 92.1
%
91.7% 85.5% 88.7% 88.8% 90.9% 90.9% 91.7% 91.5% 92.7% 91.7% 90.4%
Womens
Services
95% 90.2
%
90.5% 92.0% 90.0% 91.6% 83.5% 87.5% 91.7% 88.8% 89.7% 88.5% 88.5%
Childrens
Services
95% 87.1
%
88.7% 84.1% 84.4% 84.8% 87.9% 88.1% 88.9% 86.1% 85.6% 80.4% 80.4%
Diagnostic &
Therapeutic
95% 96.6
%
94.2% 93.1% 92.7% 93.7% 92.9% 92.6% 95.8% 96.1% 94.7% 95.2% 93.5%
Facilities 95% 100.
0%
100.0
%
100.0
%
100.0
%
100.0
%
100.0
%
100.0
%
100.0
%
100.0
%
100.0
%
99.2% 99.1%
Corporate 95% 98.9
%
97.8% 98.2% 98.6% 99.0% 99.0% 99.0% 98.1% 99.7% 98.2% 98.1% 96.6%
Tameside
NHS Trust
95% 93.4
%
92.5% 90.1% 91.0% 91.6% 91.6% 91.7% 92.6% 92.5% 92.2% 91.1% 90.3%
Resus Target Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Jun-14
Emergency
Services &
Critical Care
95% 92.0
%
89.2% 90.3% 88.3% 88.8% 89.3% 90.4% 91.2% 90.4% 90.0% 85.2% 83.1%
Elective
Services
95% 91.2
%
87.1% 88.3% 85.3% 88.3% 88.3% 87.5% 89.0% 86.8% 88.5% 84.8% 82.7%
Womens
Services
95% 91.7
%
90.1% 91.8% 87.9% 89.0% 83.7% 82.8% 88.5% 78.2% 82.5% 82.4% 78.4%
Childrens
Services
95% 86.7
%
83.0% 80.2% 78.8% 77.4% 77.7% 81.6% 78.1% 79.8% 76.3% 69.3% 66.7%
Tameside
NHS Trust
95% 91.3
%
88.1% 89.1% 86.4% 87.5% 87.1% 87.8% 89.1% 86.6% 87.6% 83.9% 82.0%
Overall
Compliance
95% 89.6
%
88.8% 89.1% 89.2% 90.7% 90.7% 88.8% 89.0% 88.5% 88.1% 87.7% 86.6%
Improvements Made
In order to achieve the Trust’s target a number of changes have been made centrally
to aid Divisions in achieving the target, these include:
• Education and Training Bulletin has been produced detailing all the
Mandatory training face to face sessions
• Dates have been advertised for the next 6 months following feedback about
unavailability of dates and dates not being available
• More e-learning packages have been developed, development sessions have
been provided to provide guidance to staff not familiar with the e-learning
packages
• A dedicated mandatory training email has been developed so staff can book
on courses more easily using the dedicated email. An on-line booking facility
is currently under development.
• A monthly email highlighting the staff who did not attend sessions (DNA’s) is
to be sent to Managers from next month. Currently this is not provided.

5
Divisional Trajectories
Following a request at the last Board, the Divisional teams were asked to provide
trajectories detailing the improvement to the Mandatory training rates for their areas.
Detailed plans have been supplied outlining how the Divisions plan to achieve the
target of 95%, the majority have plans in place to achieve the target by December
2014. These plans will be monitored through the Operational Board.
Where tables have been supplied these have been attached in appendices 1-3.

Appendix 1
Elective Division Mandatory Training Improvement Plan
Mandatory Compliance 31st May 2014 WB MH Resus Conflict
recovery trajectory for areas where not
95% compliant
% % % % Aug-14 Sep-14 Oct-14
Anaesthetic Recovery Theatres L5 90% 90% 98% 95% 95%
Anaesthetics - Medical L5 77% 81% 65% 90% 75% 85% 95%
Audiology Services L5 100% 100% 100% 100%
Cancer Data Service L5 81% 100% 50% 100% 75% 85% 95%
Day Endoscopy Unit L5 95% 90% 94% 81% 85% 95%
Day Surg Endoscopy Ward L5 89% 95% 78% 78% 85% 95%
Dental Specialties - Medical L5 17% 83% 100% 67% 75% 85% 95%
Dental Surgery Services L5 100% 100% 88% 88% 95%
Elective - Nursing & support L5 40% 100% 75% 50% 75% 85% 95%
Elective Services - Managers & support L5 82% 96% 50% 0% 75% 85% 95%
Elective Unit L5 93% 96% 80% 76%
ENT Medical L5 40% 60% 20% 60% 75% 85% 95%
ENT Nurse Practitioner-Elective L5 50% 100% 50% 0% 75% 85% 95%
General Outpatients L5 77% 91% 92% 88% 85% 95%
General Surgery Medical L5 71% 82% 76% 82% 85% 95%
Hartshead Theatres 1-10 L5 86% 88% 95% 97% 95%
ITU / Surgical HDU L5 95% 88% 93% 90% 95%
Orthopaedic Nursing Support L5 50% 100% 100% 100% 75% 85% 95%
Orthopaedics - Medical L5 74% 95% 68% 74% 75% 85% 95%
Phlebotomy service L5 77% 100% 46% 31% 75% 85% 95%
Surgical Unit L5 86% 89% 78% 63% 75% 85% 95%
Theatres Support L5 0% 100% 100% 100% 75% 85% 95%
Trauma Unit L5 81% 96% 94% 88% 85% 95%
Urology L5 100% 100% 50% 75% 75% 85% 95%
Vascular L5 100% 100% 100% 100%

Appendix 2
Medicine & Urgent Care Division Mandatory Training Improvement Plan
INDICATOR
CURRENT
PERFORMANCE
30th
June 2014
Mandatory Training
(target 95%)
Manual Handling 88%
Resus 83%
Workbook Completion 80%
Conflict 74%
0
10
20
30
40
50
60
70
80
90
100
Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14
PDR
Manual Handling
Resus
Workbook
Conflict

Appendix 3
Children’s Services Mandatory Training Improvement Plan
Workbook Manual Handling Resus
Current position 88% 80% 69% By end of August. 90% 85% 70% By end of Sept 95% 91% 80% By end of Oct 95% 92% 90% By end of December 95% 95% 95%

PART 1
AGENDA ITEM 15a
Title of paper
Summary Paper of the June 2014 meeting of Quality and Governance Committee including Summarised Aggregated Learning Report ( May 2014)
Meeting date 31st July 2014
Purpose Provided for review and awareness
Actions Recommended
Discussion / Noting / Decision
Publication This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms If present explained in document
Any communication actions after meeting
Dissemination and communication
Report of Tricia Kalloo – Non Executive Director
Paper prepared by Peter Weller Director of Quality and Governance

2
Quality and Governance Committee
26th June 2014
Summary of discussions The Committee received and accepted the minutes of the last meeting and reviewed the actions arising from these which were all covered on the agenda. At the request of the committee the Head of Patient Flow was in attendance to provide an update and assurance on the changes being implemented to the Discharge process as part of the work programme. An update was provided on changes and integration of the team and progress on more effective use of Intermediate care provision including the quality of handover and transfer. The early commencement of discharge planning from the point of admission was stressed as being key to success in planning early discharge. It was identified that the work programme had been informed by the Keogh review and ECIST review. It was identified that the work was part of the Trust CQUIN for 2014/15 and the impact of changes would be reviewed at the end of Q1 14/15, using Q4 13/14 as the baseline monitoring position. An update of the CQC Inspection to date was received. It was confirmed that the 1st two phases of the inspection had been completed and the CQC were now in the process of compiling the report. It was identified that we were expecting the report by July 2014. The Committee received the Patient Experience update which included the progress with the Friends and Family Test results and the improved response rates for A&E. The development work engaging voluntary services were highlighted and the relationship with the local education college including the potential this may offer was explained. The Dining companion’s project was identified as working well on two wards in the Ladysmith block which was provided for 3 meals a day, and had received positive feedback. It was also highlighted that the Trust were one of two in the North West that were piloting the Macmillan Value based standards which link closely to the Trust Values and Behaviours. A gap analysis was currently being undertaken as a baseline to allow progress to be monitored. Progress was reported against the planned ward accreditation programme and reported that all general and acute wards would have been through an initial review by end of June as expected. The report also identified that the Trust had received the annual organ donation report, and the Initial review identified that the Trust had made good progress with respect to these requirements. It was noted that a full review of the report and outcomes would be undertaken by the HTA and Organ Donation committee to inform the future progression with the requirements. The Serious Incident Update Report was received with discussion, scrutiny and challenge by members on information provided. The strengthened process for sharing and dissemination of the outcome was emphasised. An update was provided in relation to the section 28 Letter from the Coroner in respect of the Emergency Department and Critical Care pathway that related to an event prior to the changes

3
implemented within the service. The issues and themes apparent within the mortality reviews were also discussed and questioned by the NED’s. An update was received on the Significant Risk Report and Board Assurance Framework which is also reported to Trust Board but for assurance monitoring and scrutiny reported to this committee. An update was provided on Mortality and the progress with Mortality Reviews. It was identified that the Trust SHMI was gradually reducing and there was better alignment of this with the HSMR. It was identified that reports and analysis requested and received from Dr Foster on specific speciality areas had been shared with the Divisions for review and understanding and for Divisions to provide assurance to the Mortality Steering Group on actions being taken. The Committee received a presentation on the requested summary aggregated learning report to provide a dashboard view into the current issues related to Incidents, Complaints, and Claims, Safeguarding concerns, Inquests and mortality reviews. The committee discussed the dashboard overview, and emerging or apparent trends. Members welcomed the level of detail and analysis in the presentation and considered what level of detail would be appropriate for routine Trust Board reporting to provide assurance and also ensure the Trust Board had sight of key issues and themes. It was agreed that a revised summary report be produced and was presented to the June Trust Board by the Chair of the meeting along with the summary notes of the May Quality and Governance meeting for review and discussion. Minutes of reporting committees were received and reviewed for assurance and awareness. Under any other business members were made aware of the Risk summit being held that afternoon. It was understood this had been requested by the Deanery following the recent planned review, and also in the context of the THAG (Tameside Hospital Action Group) report which had been circulated to other stakeholders. This event was noted by members of the meeting. Ms T Kalloo Non-Executive Director July 2014

4
Summary Aggregated Learning information – June 2014 **still being validated
Incidents reported Apr 14 May 14 June 14** 4 month
avg trend 12 month avg trend
New incidents (reported in month- includes delayed reports) 761 794 802 � �
Reported with Moderate harm 16 13 32 � �
Reported with Major harm 0 3 4 � �
Reported with Catastrophic harm 1 1 0 � � Never Event 0 0 0 n/a n/a
RIDDOR reported incidents 1 2 0 � �
Complaints and PALS issues Apr 14 May 14 June 14 4 month
avg trend 12 month avg trend
New Complaints 39 39 39 � � New MP enquiry 4 0 4 � �
New External complaint 0 1 3 � �
New Enquiry 6 5 5 � �
New PALS issues 167 177 246 � �
Total issues received 217 222 299 � �
Re opened Complaints 3 9 8 � �
Issues /cases responded to 203 209 196 � �
Complaints %age closed in agreed timescale 68% 51% 85% � �
Average time to close issues/cases (days) 18 27 26 � �
Number issues on-going @ time of monthly report 246
Ombudsman Cases upheld 1 0 0
New issues in Month by Division
Indicators Apr 14 May 14 June 14 4 month
avg trend 12 month avg trend
0 20 40 60
Facilities
Nursing
Diagnostic & Therapeutic
Womens & Childrens
Elective Services
Emergency & Critical Care
3 months June 14 - Moderate or greater harm by reported Division
3 Moderate
4 Major
5 Catastrophic
0 10 20 30 40 50 60 70
Emergency & Critical Care
Elective Services
Womens & Childrens
Diagnostic & Therapeutic
Planning & Service Impr.
Emergency &
Critical CareElective Services
Womens &
Childrens
Diagnostic &
Therapeutic
Planning &
Service Impr.
Apr 24 11 2 1 1
May 21 12 3 2 1
Jun 17 21 1
Complaints by Division
Top Incident Causes reported with Moderate harm and above (June 2014) Clinical Management issues
Potential Delayed Treatment
Infection Control - HCAI Associated Death
Infection Control - Tested Positive For CDIFF
Pressure Ulcer - Grade 2 Hospital Acquired
Pressure Ulcer - Grade 2 Non Hospital Acquire
Top issues reported (June 2014) related to Medical Care And Treatment
Nursing Care
Communication - Written
Cancellation Of Operations
Medical Care
Diagnosis - Wrong
Waiting List - OP Consultant
Appointment (OP) Cancellation
Appointment (OP) Delay
Discharge Arrangements
Top issues reported (June 2014) related to Appointment (OP) Delay
Communication - Written
Medical Care And Treatment
Appointment (OP) Cancellation
Communication - Verbal
Compliment - Staff
Communication - Admin Staff
Communication/Info to Patients
Waiting List - OP Consultant
Delay In Diagnosis (Results)

5
Mortality reviews required 75 57 81 n/a n/a
Mortality reviews undertaken (@07/0/7/14 73 56 38 n/a n/a
Inquests with TGH involvement closed /heard 10 13 9 n/a n/a
Coroner-Prevention of Future Death report (Rule 43 ) 1 0 1 n/a n/a
Themes reported (June 2014) • Morality – themed feedback to Division for learning from reviews
o Record keeping standards
o Frequency of patient review
o Re-assessment and of patients
o Consistent use of PARS
• Inquest and Coroner
o n/a
Indicators Apr 14 May 14 June 14 4 month
avg trend 12 month avg trend
StEIS reports
Internal issue 4 6 2 n/a n/a
External issue 2 4 2 n/a n/a
Never events 0 0 0 n/a n/a
Safeguarding - Adult cases reported
Allegation on hospital care 19 7 6 n/a n/a
Allegation on other care 29 8 9 n/a n/a
Themes reported (June 2014) StEIS
• Related to Infection control and patients admitted with Pressure ulcers
Adult Safeguarding
• Related to issues already identified in Incident reporting and complaints

PART 1 AGENDA ITEM 15b
Title of Board paper
Finance and Performance Committee Minutes: Meeting held on the 24th June 2014
Board meeting date 31st July 2014
Purpose
To inform the Board about matters discussed at the Finance and Performance Committee
Actions Recommended
Discussion/Noting/Decision
Publication
This paper will be published in line with the Tameside Hospital NHS Foundation Trust publication scheme, subject to any redactions approved by the Board.
Unusual acronyms
CYE – Current Year Effect EDG – Executive Delivery Group FYE – Full Year Effect
Any communications actions after the meeting
None
Report of Anne Dray – Chair of the Finance and Performance Committee
Paper prepared by Barbara Herring, Director of Finance

1
FINANCE AND PERFORMANCE COMMITTEE Agenda item 2
Date of Meeting: 24th June 2014 Time: 10.00 am Location: Meeting Room, Silver Springs Present Position Initial Mrs A Dray Non-Executive Director (Chair) AD Mr T Ward Non-Executive Director TW Mrs B Herring Director of Finance BH Miss S Holroyd Deputy Director of Finance SH Mrs G Parker Director of Estate and Facilities GP Mr P Williams Chief Operating Officer PW Mr C Porter Turnaround Director CP In Attendance Mr T Sivner Chief Pharmacist TS
Item No
Description Action
66/2014 Apologies Paul Williams, Suzanne Holroyd
67/2014 Minutes of the previous meeting 27th May 2014
The minutes were accepted as a correct record with the following amendments: 54/2014 – the following sentence should be reworded to read “the report should have, as in the divisional reports, a note of the actions being taken”. The report should also include divisional reports which give details of actions being taken. 56/2014 – second paragraph SH to provide further details of the pressures of £3.8m to be added to the action log. 56/2014 – b) second paragraph Typographical error – are – should read area. 57/2014 – final sentence Post meeting note – BH advised that the telephone contact information is correct as the actual service does not start until July/August. 57/2014 – sentence beginning “CP stated that” – should read – reprioritise for the EDG agenda – not reprioritise the EDG agenda. 58/2014 – sixth paragraph Typographical error – ace – should read face
SH

2
58/2014 – eighth paragraph Typographical error – wo – should read two 58/2014 – ninth paragraph Typographical error – of – should read also 59/2014 Post meeting note – GP confirmed that the final costs of the scanner has been agreed and it is within the £1.5m budget. 59/2014 – eleventh paragraph Amend the minute to read – …. reviewing the case six months after the new Radiology Manager commences in post. It was agreed that an update on the project management will come to the meeting in August and an overall update will be available in July 2015. 60/2014 AD/BH/TW to clarify actions.
68/2014 Matters arising: There were no matters arising.
69/2014 Action log
3.1 Tier 1 Report BH introduced the report and highlighted the following: The Executive Team have agreed to continue with reduced contracted support for Lorenzo until August. A plan is being drawn up to facilitate moving to business as usual A restructure of corporate services is planned and this will be implemented as soon as possible. BH is to cost the restructure within the existing resources and identify any potential savings. A bid has been submitted to HSCIC for additional funding and a response regarding additional funding of around £500k from Tim Donahue is awaited. A restructure of IM&T is planned to stabilise the infrastructure and systems. Considerable investment has been made in Corporate Nursing and Governance Department which has been funded from Keogh costs. CP to meet with John Goodenough to discuss the Nursing element of the report.
Until appointments are made in the senior interim positions UHSM are recharging at a premium rate. If we come out of special measures the Department of Health will award £500k which UHSM have agreed to refund to the Trust.
CP

3
CP expressed concern regarding the overspend in the communications budget and that stated processes are not being followed. A paper is to be presented to EDG regarding the need for a substantive transformation team to support the agenda over the next few years. CP stressed that additional contracts should not be offered to staff without going through the VAR process. CP to provide an update for the next meeting. A review of the current divisional structure is being undertaken and this will help identify true levels of accountability.
CP
70/2014 Finance and Activity Performance 31st May 2014 BH presented the report to the Committee, highlighting the following areas. AD expressed concern regarding low activity levels. BH advised this issue has been discussed at length with the Executive Team, and it was identified that deflections that are being made in A&E and reduction in length of stay are contributing to the reduction of activity levels. BH is reviewing the conversation rate from A&E activity into non-
elective admissions and once the review has been completed, the possibility of additional funding will be discussed with the CCG. Waiting lists are being validated, and hold files are being look into to determine the exact number of patients waiting for appointments. Length of stay in Trauma and Orthopaedics has increased over the past six months and the reasons for this are being investigated. CP advised that the financial position has deteriorated and meetings have been arranged to review the situation. A Business Case for two additional T&O Consultants is being presented at the next Executive Team meeting. GP referrals have been included into the report and demand is showing a slight upward trend. The level of coding has reduced at month end to 70%; this is due to staffing pressures, the availability of records to code, and clinical outcome sheets not being recorded in real time. The recording of outcomes has been addressed and work is ongoing to ensure this is sustained.
There is still a concern that not all the activity is being collected. A company is to be appointed to ensure every point of activity is being captured correctly. Internal Audit and Cymbio are also reviewing the systems and processes. The Heading for Home project is looking at the cohort of patients who are awaiting intervention from Social Services and moving on a sub-contractual basis into the private sector. This will ensure beds are available and the income is classed as excess bed days where appropriate and the activity will be recorded on our systems. The additional funding from the Department of Health was received on 23rd June and will become permanent funding at the end of July.

4
BH agreed to provide a separate forecast paper for the June position and each month after. To be added to the work programme.
BH
71/2014 Diagnostic Division – Position at 31st May 2014
TS gave an update on the financial position as at 31st May 2014, he reported that the headline figures in terms of the division are:
• Expenditure of the division is £23/24m per annum and off-set by income of about £12/13m. The overall budget is £10.8m per annum.
• The division is showing a £113k over spend plus £50k shortfall in CIP which makes of total of £153k overspent.
• Pathology is effectively underspent at end of Month 2 by £50k.
• Blood product usage is lower than expected, but it is unpredictable to plan for, this is being monitored to see if any CIPs can be identified.
Radiology
• The overspend is predominantly driven by overspend in the Radiology budget which equates to over 90%. The majority of the £153k overspend is due to pay budgets for additional sessions and WLI’s.
• There are issues in the variation of the existing workload for Radiologists. Job planning and productivity issues are being addressed. CP to meet with TS regarding use of agency staff. The long term strategy is to look at partnership with other organisations.
• A Radiologist of the day has been introduced which will look at different ways of working to ensure the service is as effective as possible. They will also review requests to ensure they are appropriate.
• Activity has reduced but demand has increased, and MR scanning is predicted to increase by 13%. TS agreed to provide the figures to CP.
• Ways of educating staff as to the cost of each investigation are being considered.
• Savings have been identified by the use of external reporting partners and once the MR scanner has been installed it will no longer be necessary to hire external scanners.
• Meridian undertook a review which identified capacity; this was disputed by the Radiologists. Dr Brett is conducting a further review to ensure maximum productivity. TS agreed to forward the report to CP.
• CP to share the data with EDG to gain a collaborative understanding.
Pharmacy
• Pharmacy have a slight overspend of £11k which was due to an under achievement on PbR tariff which can vary from month to month.
• Staffing pressures have been experienced as a result of the on-going issues with the prescribing model on Lorenzo. The most critical issues have mostly been resolved, talks are ongoing regarding the timescale for resolving the outstanding 70/80 issues.
CP
TS
TS
5
• A judgement whether or not to continue to use the prescribing model on Lorenzo will be taken next week, once a position statement has been received.
CIP
• Pharmacy is expected to post another £45/50k in Month 3. Some areas in the planned CIP around the collaboration are going to be extremely challenging. CP stressed that divisions need to manage budgets within the resources and this should be the message that is given to front line managers.
• Pharmacy is now opening over the weekend and opening hours have been increased to ensure prescription charges are collected.
• The option of selling over the counter medicines is being considered.
72/2014 Cost Improvement Programme: 31st May 2014 CP presented the report to the Committee, highlighting the following: 97% against the Monitor plan has been achieved for Month 2 accumulative leaves around 80 behind and around 88/89% deliver accumulative in the first two months. There are a number of schemes which are challenged whereby the leads are leaving or additional costs are being incurred to retain staff. A paper detailing the increased posts for the Transformation Team has been produced which includes a Financial band 8b to ensure turnaround work is continued. The meeting of the Controls Group has identified issues with the use of agency staff, and action is being taken to tighten up the processes. Discussions are to take place with Agencies in order to renegotiate commission and headline rates for doctors. Re-admissions are unlikely to reach £300k this year, but there is an opportunities to bring into the length of stay and right sizing beds project. It was agreed to leave the rating for this action as red. The divisional CIP had a target of 1.06 in month and delivered a total of 1.67, of which a significant amount is non-recurrent. Recurrent CIPs are being sought. Length of stay is to remain red as ward 30 has not closed on 1st June as anticipated. The contract with NHSP is due to be reviewed in October. One or two major projects have been identified from the initial meeting of the Innovation and Ideas workstream and the next meeting is scheduled to take place on the 7th July. Focussed meeting are taking place by exception in order to hold colleagues to account for overspend on budgets.

6
73/2014 Banking Arrangements The Committee noted the paper
74/2014 Service Line Reporting BH presented the paper which was taken to Board in November for information only as the 13/14 figures are not available. Once the information is available an updated report will be provided.
75/2014 Minutes of reporting Committees: 9.1 Executive Delivery Group The minutes were noted 9.2 Capital Planning and Estates Committee Deferred until next meeting
76/2014 Committee Workplan The workplan was noted and the following changes and additions agreed.
1. Service Line Reporting – November 2. Deloitte Governance Action Plans – July 3. Risks for BAF – July 4. Forecast Paper – August/September 5. QIA – Q1
BH
77/2014 Any other Business
AD advised that she has been invited to the CCG along with Julie Soboljew to meet with the Dr Alan Dow.
78/2014 Date of Next Meeting 25th July at 2.00 pm Silver Springs Meeting Room