-
7/27/2019 age.pdf
1/4
International Journal of Epidemiology 2002;31:715718
Will you still need me, will you still feed me, when Im 64?
Lennon and McCartney wrote this line in 1967. Average life
expectancy at birth for a man in England was 68, but it is
now
75 years and rising at the rate of 2 months every year. The
rise
in the oldest old has been even more dramatic amongst very
old people and is best exemplified by the number of people
reaching 100 years of age. In the UK, it is the custom for
the
Queen to send these people a congratulatory telegram (Table
1).
The Queen now sends a card by express mail as the telegram
service no longer exists. How long before she just sends an
e-mail?
This issue of the International Journal of Epidemiology
containsa series of papers concerned with ageing. For each of us
indi-
vidually, having survived long enough to be reading this,
our
chances of reaching old age are high. And yet, the myths
surrounding ageing are legion. Our commentators make an
excellent job of highlighting and demolishing many of them.
Demographic alarmism
The ticking of the demographic time-bomb and associated
chaos
for public services has been a prevalent theme. Averting the
crisis of very large numbers of older people has been used as
a
lever to promote questionable policy changes,1 which have
failed. Gee contextualizes current concerns about the ageing
of
populations with earlier eras of demographic alarmism:
fertilitycontrol in Canada in an attempt to preserve and improve
the
White race; massive western (largely US) funding for birth
control to slow the population bomb of the rapidly growing
populations of the South, which still continues.2 Both were
misguided and ultimately such policies fail. In commenting
on
the impact of demographic change on health and social care,
both US and European perspectives highlight the fact that it
is
not demographic factors that will determine the affordability
of
care, but rather it is politics and social organization.3,4
While the whole world is ageing, there is marked hetero-
geneity between countries in the rate of ageing. Palacios
suggests,
controversially, that the differences in both the numbers of
aged
and the economic status of different countries may promote
migration that would enable the long-term care needs of
elderlypeople in high-income countries to be met and would lead
to
the economic growth of poorer countries.5 Although it is
frequently emphasized that the majority of the worlds
elderly
people live in low- to middle-income countries, it is the
speed
with which these populations are ageing that is of greater
significance. In the rich North, a century of economic
growth
change enabled slow and steady development of the
infrastructure necessary to support the health and social
needs
of growing numbers of elderly people. It took over 100 years
for
Belgium to double the proportion of its 60+ population from
9% to 18%. China will take 34 years and Singapore only
20 years to achieve the same population ageing.
Projectionssuggest that the net world monthly gain in people aged
65 years
and over by 2010 will be 1.1 million every month,6 from a
current level of about 800 000 every month. In the poor
South,
it will be difficult to implement adequate support systems,
given
their economic status and the lack of political will.
A new social contract?
In Latin America, Palloni et al. feel that the chances of
achieving
successful public policies are bleak, citing the causes as
untamed
inflationary pressures, recessionary set backs, high
unemploy-
ment, increasing absolute poverty and growing social and
economic inequalities.7 It seems likely that in all countries
there
will be a need to re-define the role of the state in welfarism
assuggested by Lloyd-Sherlock, who also emphasizes the changing
economic, social and cultural contexts in which social
policies
for older people are enacted.8 The social contract between
individuals, families and the state requires re-definition.
But
this re-definition needs to be done explicitly, starting with
a
statement of our social values from which our policies
should
grow. In the UK, the issue of long-term care has only
recently
become the subject of review in the form of a Royal Com-
mission.9 While unanimous conclusions could not be reached
on who should pay for certain aspects of long-term care,
that
independent, explicit and reasoned debate has occurred will
make for better understanding of our social contract.
Political denial, empoweringthe disenfranchised
In poorer countries, as both Evans and Gorman note, it is
much
more likely that politicians will simply neglect to consider
their
responsibilities to older people or, worse, remain in a state
of
denial in which it is assumed that traditional values will
ensure
that the family will cope.10,11 In an effort to understand
the nature of health and social care needs associated with
the
ageing of populations, the Association of South East Asian
Nations (ASEAN) decided to establish a focus on ageing. A
field
International Epidemiological Association 2002 Printed in Great
Britain
Department of Social Medicine, University of Bristol, Canynge
Hall,
Whiteladies Road, Bristol BS8 2PR, UK.
715
EDITORIAL
Ageing, health and societyShah Ebrahim
Table 1 Birthday greetings telegrams sent by Queen Elizabeth II
to
people on their 100th birthday, 19522001
1952 1962 1972 1982 1992 2001
255 590 1283 2759 3382 3898
Source: Buckingham Palace Anniversaries Office, 2002.18
-
7/27/2019 age.pdf
2/4
review of policies revealed marked variation, largely deter-
mined by the prevailing system of political organization and
wealth (Tables 2, 3).
Evans considers it unlikely that international aid donors
will
create social support systems to replace the traditions
destroyed
by development money.10 While it is commonplace for donors
to consider the effects of funding on women and the poor,
similar considerations for old age are currently
non-existent,but could be implemented. Non-governmental
organizations,
which might be expected to play a leading role in such
advocacy, are said by Gorman to lack the necessary
resources.11
They are however, often better placed to deal with the dis-
empowerment of poor elderly people through community
action schemes, such as the community banking and income
generation initiatives.12
Avoiding differential challenge
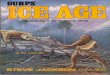
Evans defines the process of ageing as one of loss of
adaptability
of the individual and of differential challenge, such that
older
people are faced with greater performance requirements
relative to their capacity.10 For example, road crossing
timers
that are too short for older people to cross the road safely;
high
steps to get onto public transport; and poor quality housing
(Figure 1). Many of these problems could be improved by
better design, but in the case of disabled access in the UK,
legislation was required to ensure that new buildings were
designed appropriately. Such design is often of benefit not
justto disabled older people but also to mothers laden with
shopping and children.
A common link running through several of the articles in
this
issue is the need to ensure income security in old age.
Differential challenge due to poverty is the most pressing
problem in the countries of the South. Our common stereotype
is of intergenerational money transfers flowing from children
to
parents or grandparents in these countries. However, recent
work in Indonesia among poor rural people has demonstrated
that the majority of transfers are from older to younger
people
(Philip Kraeger, University of Oxford, personal communi-
cation). Futhermore, the picture is complex, with many
elders
716 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
Table 2 Health policies of relevance to health care for elderly
people in Association of South East Asian Nations (ASEAN), 1997
Health policy Brunei Cambodia Indonesia Laos Malaysia Myanmar
Philippines Singapore Thailand Vietnam
Free primary health care Yes Yesa Yes Yesa Yes Yesa Some Some
Yes Yes
Free hospital care Yes Yesa Yes Yesa Yes Yesa Some No Yes
Yes
Training in geriatrics No Medicine No Nursing No No No Medicine,
Nursing Medicine
nursing
Geriatric services No No No Abandoned University No Some Yes Yes
Yes
Community rehabilitation No Amputees No Projects Projects
Projects Projects Yes Projects Some
Preventive services Yes No No No No Projects Yes Yes Projects
No
Nursing homes Yes No Private and No Private and Private Private
and Private and Private and No
Public Public Public Public Public
a User charges currently under investigation.
Source: Ebrahim S. Report to Association of South East Asian
Nations Task Force on Ageing , 1997.19
Table 3 Social policies of relevance to elderly people in
Association of South East Asian Nations (ASEAN), 1997
Social policy Brunei Cambodia Indonesia Laos Malaysia Myanmar
Philippines Singapore Thailand Vietnam
Pensions All citizens Civil Civil servants, Civil Civil Civil
Civil servants, Civil Civil Civil
servants Widows servants servants, servants self-employed
servants, servants servants
pensions restricted employed
Housing Some No No Very limited: Rural NGOa No Group homes
Limited No No
civil servants housing
scheme
Caring
allowances On No No No Tax relief No Tax relief Tax relief No
No
application for carers for carers for carers
Disability
allowances On No No No No No Workers No Yes Limited
application compensationTransport None None Subsidized None
Subsidized None Subsidized Subsidized None None
fares fares fares fares
Respite care None None None None None None Institutional
Institutional None Social
and day and day centres
centres centres
Organizations None Senior None National Senior None Senior
Citizens Singapore Senior Senior
for elderly Citizens Front for Citizens Federations/ Action
Citizens Citizens
people Association Construction Association Associations Group
Association Association
of Elders
a Non-governmental organization.
Source: Ebrahim S. Report to Association of South East Asian
Nations Task Force on Ageing , 1997.19
-
7/27/2019 age.pdf
3/4
being without children or any obvious means of immediate
support.
Social policies should be complemented by adequate health
care policies. Good health care for all ages is likely to play
amajor role in improving the peak capacity of older people, and
reducing the rate of decline of physical and mental function
associated with old age, such that we reach thresholds for
maintaining independent life at a much later age. When
disease
strikes, accurate diagnosis and prompt treatment, coupled
with
rehabilitation, will be needed to move the individual above
dependency thresholds. In the UK a National Service Frame-
workor blueprintfor health services for older people has
been implemented which attempts to define the standard of
care that should be expected.13 It remains to be seen
whether
initiatives of this nature will work. Hospital services for
elderly
people are becoming widespread in China14 and many
countries of the South, but without adequate community out-
reach and support for family carers it is doubtful that they
willachieve the aim of allowing older people to maintain
independence for as long as possible.
The World Assembly on Ageing, Madrid
Many of these issuesincluding health, nutrition, protection
of
elderly consumers, housing and environment, family, social
welfare, income security, employment and educationwere
the priorities of the First World Assembly on Ageing in
Vienna
in 1982. It is now acknowledged that much of the work
proposed never happened.15 Member states of the United
Nations, organs of the United Nations and non-governmental
organizations, research institutions and the private sector
wereinvolved. During 812 April 2002 a second World Assembly met
in Madrid with the aim of reviewing the outcome of the first
World Assembly and then adopting a revised plan of action on
ageing that is aligned to the sociocultural, economic and
demographic realities of the new century, with particular
attention to the needs and perspectives of developing
countries.
At the Assembly, the World Health Organization launched its
life course approach to healthy ageing. This builds on the
notion
that industrialized countries have been able to postpone the
onset of disability and diseaseand while the latter is
certainly
true, there is much less evidence to be sure about the
postponement of disability. Actions are recommended in three
essential areas: health, participation and security (Box 1).
It would be easy to quibble with these rather glib recom-
mendations, but in the face of political inertia it is important
to
make the point clearly that much can be done, and in some of
the areas listed in Box 1 we have a fair idea of how to
proceed.There is clearly a major research agenda for ageing
identified
by these recommendations: we simply do not know how to
promote mental health or physical activity. To make matters
worse, it is likely that information gleaned from the rich
North
is unlikely to be applicable to the poor South.
The World Assembly strategy stresses the need for action,
for
linkages between ageing and development programmes, and for
the needs and perspectives of developing countries to be
taken
into account. Not surprisingly, publicprivate partnerships
are
promoted and measures to promote intergenerational
solidarity
emphasized. Topics covered by the strategy are shown in Box
2.
The international media attention for this World Assembly
has
been muted, and has emphasized ageing as an international
problem16 rather than the Assemblys more positive slogan
asociety for all ages.
The notion that a World Assembly is capable of providing a
blueprint that is relevant to such diverse member countries
is
rather surprising and it seems likely that the interests of
the
powerful countriesprobably through the publicprivate
partnerships proposedwill prevail despite initiatives like
this.
The complexity and breadth of topics covered by the Assembly
may be its undoing given the short attention span of
politicians.
By contrast HelpAge International, a non-governmental organ-
ization, has adopted a more focussed strategy, emphasizing
the
discrimination against older people in health care, legal
services
and education.17 However, the importance of international
meetings is in the symbolism and hope they provide to those
who are attempting, often in small ways, to make improve-ments
to the care of older people, to advocate the need for
politicians to take an interest, and as a rallying call to
older
people themselvesmany of whom do have votes, money and
informal modes of ensuring intergenerational influence.
Almost
everyone will become oldthese are issues that will affect
us all.
AGEING, HEALTH AND SOCIETY 717
Figure 1: Profile of physical capacity changes with age
indicating a
threshold for independent life and possible means of reducing
the
consequences of age-related changes in physical capacity.
Box 1: WHOAgeing: A Policy Framework
(http://www.who.int/hpr/ageing)
Address factors that contribute to the onset of disease
and disabilities like poverty, low literacy levels and lack
of education. Control tobacco use and alcohol abuse throughout
the
life course.
Ensure appropriate nutrition and healthy eating
starting at an early age.
Promote physical activity at all ages.
Create age-friendly, safe environments by making walk-
ing safe and implementing fall prevention programmes.
Increase affordable access to essential, safe medications
and assistive devices such as eyeglasses or walkers.
-
7/27/2019 age.pdf
4/4
References1 World Bank. Averting the Old Age Crisis. Policies to
Protect the Old and
Promote Growth. Oxford: Oxford University Press, 1994.
2 Gee EM. Misconceptions and misapprehensions about
population
ageing. Int J Epidemiol2002;31:75053.
3 Wiener JM, Tilly J. Population ageing in the United States
of
America: implications for public programmes. Int J Epidemiol
2002;31:77681.
4 Walker A. Ageing in Europe: policies in harmony or discord?
Int J
Epidemiol2002;31:75861.
5 Palacios R. The future of global ageing. Int J Epidemiol
2002;
31:78691.
6 Kinsella K. Demographic aspects. In: Ebrahim S, Kalache A
(eds).Epidemiology in Old Age. London: BMJ Publishing, 1996, pp.
3240.
7 Palloni A, Pinto-Aguirre G, Pelaez M. Demographic and
health
conditions of ageing in Latin America and the Caribbean. Int
J
Epidemiol2002;31:76271.
8 Lloyd-Sherlock P. Social policy and population ageing:
challenges for
north and south. Int J Epidemiol2002;31:75457.
9 Royal Commission on Long Term Care. With Respect to Old
Age.
London: Stationery Office, 1999.
10 Evans JG. The gifts reserved for age. Int J
Epidemiol2002;31:79295.
11 Gorman M. Global ageingthe non-governmental organization
role
in the developing world. Int J Epidemiol2002;31:78285.
12 Randel J, German T, Ewing D, for HelpAge International. The
Ageing
& Development Report 1999. Poverty, Independence & the
Worlds Older
People. London: Earthscan Publications, 1999.13 Secretary of
State for Health. National Service Framework. Older People.
London: Department of Health, 2001.
14 Woo J, Kwok T, Sze FKH, Yuan HJ. Ageing in China: health and
social
consequences and responses. Int J Epidemiol2002;31:77275.
15 Bosch X. Two billion people older than 60 years by 2050,
warns UN
Secretary General. Lancet2002;359:1321.
16 BBC World News.
http://news.bbc.co.uk/hi/english/health/newsid_
1913000/1913515.stm
17 HelpAge International. The State of the Worlds Older People.
2002.
http://www.helpage.org. Accessed 16 April 2002.
18 Buckingham Palace, Anniversaries Office, London UK (+44 20
793
04832).
19 Ebrahim S. Report to Association of South East Asian Nations
Task Force on
Ageing. Jakarta: ASEAN Secretariat, 1997.
20 Ebrahim S. Health of Elderly People. In: Detels R, McEwan
J,
Beaglehole R, Tanaka H (eds). Oxford Textbook of Public Health,
4th Edn,
2002, Vol. 3, Ch. 11.8, p. 1712.
718 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
Box 2: International Strategy for Action on Ageing.
2nd World Assembly on Ageing April 2002
(http://www.un.org/ageing/coverage/
Empowerment of older persons to fully and effectively
participate in the social, economic and political lives of
their societies, including through income-generating
and voluntary work;
Provision of opportunities for individual development,
self-fulfilment and well-being throughout life as well as
in late life, through, for example, access to life-long
learning;
Guaranteeing the economic, social and cultural rights
of older persons as well as their civil and political
rights,
including the elimination of all forms of discrimination
on the basis of age;
Commitment to gender equality in older persons
through elimination of all gender-based discrimination,
as well as all other forms of discrimination;
Recognition of the crucial importance of inter-
generational interdependence, solidarity and reciprocity
for social development;
Provision of health care and support for older people,
as needed;
Facilitating partnership between all levels of govern-
ment, civil society, the private sector and older persons
themselves in translating the International Strategy
into practical action;
Harnessing of scientific research and expertise to focus
on the individual, social and health implications of
ageing, in particular within developing countries.