Embed Size (px)
Citation preview
TINA VANDECASTEELE
AGGRESSION AND TRANSGRESSIVE BEHAVIOUR IN CARE RELATIONSHIPS
BETWEEN NURSES AND PATIENTS
Supervisor: Prof. dr. Sofie VerhaegheCo-supervisor: Prof. dr. Ann Van Hecke
THAT’S HOW THE LIGHT GETS IN.
Leonard Cohen
THERE IS A CRACK IN EVERYTHING.

xxx
Opgedragen aan mémé, Julia D’Haene
xxx
2
AGGRESSION AND TRANSGRESSIVE BEHAVIOUR IN CARE RELATIONSHIPS:
Influencing factors and underlying processes in nurses’ and patients’
perceptions
PhD thesis Ghent University
Copyright © 2018, Tina Vandecasteele
Verschenen in de reeks monografieën van de Vakgroep Maatschappelijke Gezondheidkunde,
Universiteit Gent
All rights reserved. No parts of this book may be reproduced or transmitted in any form or by any means,
electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the authors.
ISBN: 9789073626874D/2018/3988/8
TINA VANDECASTEELE
AGGRESSION AND TRANSGRESSIVE BEHAVIOUR IN CARE RELATIONSHIPS:
Influencing factors and underlying processes in nurses’ and patients’ perceptions
Supervisor: Prof. dr. Sofie VerhaegheCo-supervisor: Prof. dr. Ann Van Hecke
Dissertation submitted in fulfilment of the requirements for the degree of PhD in Health Sciences.
Academic Year 2017-2018
xxx
4
Supervisor
Professor Dr. Sofie Verhaeghe
University Centre for Nursing and Midwifery
Department of Public Health - Faculty of Medicine and Health Sciences
Ghent University, Belgium
Co-supervisor
Professor Dr. Ann Van Hecke
University Centre for Nursing and Midwifery
Department of Public Health - Faculty of Medicine and Health Sciences
Ghent University, Belgium
Other members of the guidance committee
Professor Dr. Dimitri Beeckman
University Centre for Nursing and Midwifery
Department of Public Health - Faculty of Medicine and Health Sciences
Ghent University, Belgium
Professor Dr. Em. Maria Grypdonck
University Centre for Nursing and Midwifery
Department of Public Health - Faculty of Medicine and Health Sciences
Ghent University, Belgium
xxx
5
Examination committee
Professor Dr. Ruth Piers
Department of Internal Medicine
Faculty of Medicine and Health Sciences
Ghent University, Belgium
Professor Dr. Kurt Audeanert
Department of Psychiatry and Medical Psychology
Faculty of Medicine and Health Sciences
Ghent University, Belgium
Dr. Els Steeman
Department of Geriatrics
AZ Nikolaas, Belgium
Dr. Peter Pype
Department of General practice and primary health care
Faculty of Medicine and Health Sciences
Ghent University, Belgium
Professor Dr. Wilfried Schnepp
Department for Family-Oriented and Community-Based Nursing
Institute of Nursing Science
University of Witten/Herdecke
Professor Dr. Rudy Van den Broecke - chairman
Department of Uro-gynaecology
Faculty of Medicine and Health Sciences
Ghent University, Belgium

xxx
6
xxx
7
TABLE OF CONTENTS
Chapter I.
INTRODUCTION 13
1 | General introduction 15
1.1. | The problem of aggression in healthcare 16
1.2. | Challenges in addressing aggression in healthcare 22
1.3. | General objectives and outline of this dissertation 25
Chapter II.
ASSESSMENT OF AGGRESSION IN CARE RELATIONSHIPS: VALIDATION OF
THREE INSTRUMENTS 37
1. | Introduction 40
1.1. | Background 40
1.2. | Assessment of patients’ and family members’ aggression in general hospitals 41
2. | The study 43
2.1. | Aims 43
3. | Results 45
3.1. | Phase I: Translation and adaption of the SOVES, POAS-s and POIS 45
3.2. | Phase II: Assessment of psychometric properties of the Dutch version of the
SOVES, POAS-s and POIS 45
4. | Discussion 48
4.1. | Implications for nursing management 50
5. | Conclusion 51
Chapter III.
EXPERIENCES AND PERCEPTIONS OF AGGRESSION OF NURSES WORKING
IN PRIMARY CARE AND GENERAL HOSPITAL SETTINGS 59
1. | Introduction 63
2. | The study 65
2.1. | Aims 65
2.2. | Design 65
2.3. | Participants 65
xxx
8
2.4. | Data collection 66
2.5. | Data analysis 67
2.6. | Ethical considerations 68
3. | Results 68
3.1. | Comparison of nurses’ experiences and perceptions of patient aggression and aggression by patients’ family members in primary care and general hospital setting 69
3.2. | Identifying associations between nurses’ characteristics and perceptions regarding aggression and its management 75
4. | Discussion 79
4.1. | Methodological considerations 82
5. | Conclusion 83
Chapter IV.
PATIENTS’ PERCEPTIONS OF TRANSGRESSIVE BEHAVIOUR IN CARE
RELATIONSHIPS WITH NURSES 91
1. | Introduction 95
2. | The study 97
2.1. | Aim 97
2.2. | Design 97
2.3. | Participants 97
2.4. | Data collection 97
2.5. | Ethical considerations 98
2.6. | Data analysis 98
2.7. | Rigour 99
3. | Results 100
3.1. | Framework of suppositions: ‘Competent care and human interaction, surely that is self-evident?’ 100
3.2. | Experiencing discrepancies: ‘Competent care and human interaction, is it not self-evident after all?’ 101
3.3. | And now what?: ‘Apparently, competent care and human interactions are not self-evident’ 103
3.4. | Integration: What (exactly) is transgressive (behaviour)? 106
4. | Discussion 107
4.1. | Interpretation and context of the results 108
4.2. | Limitations 109
5. | Conclusion 110
xxx
9
Chapter V.
NURSES’ PERCEPTIONS OF TRANSGRESSIVE BEHAVIOUR IN CARE
RELATIONSHIPS WITH PATIENTS 115
1. | Introduction 118
1.1. | Background 118
2. | The study 120
2.1. | Aim 120
2.2. | Design 120
2.3. | Sample 120
2.4. | Data collection 121
2.5. | Ethical considerations 122
2.6. | Data analysis 122
2.7. | Rigour 122
3. | Results 123
3.1. | Determining factors 123
3.2. | Regulating factors 125
4. | Discussion 128
4.1. | Interpretation and context of the results 129
4.2. | Limitations 131
4.3. | Implications for practice 131
4.4. | Implications for further research 132
5. | Conclusion 133
Chapter VI.
INFLUENCE OF TEAM MEMBERS ON NURSES’ PERCEPTIONS OF
TRANSGRESSIVE BEHAVIOUR 139
1. | Introduction 142
1.2. | Background 142
2. | The Study 144
2.1. | Aim 144
2.2. | Design 144
2.3. | Sample and participants 144
2.4. | Data collection 145
2.5. | Ethical considerations 146
xxx
10
2.6. | Data analysis 147
2.7. | Rigour 147
3. | Results 147
4. | Discussion 154
4.1. | Interpretation and discussion of the findings 155
4.2. | Implications for policy and practice 157
4.3. | Study limitations 157
5. | Conclusion 158
Chapter VII.
GENERAL DISCUSSION 165
1. | Introduction 167
2. | The merit of adopting the concept of ‘transgressive behaviour’ 167
3. | Connecting the nurses’ and the patients’ perspective on transgressive behaviour in care relationships 171
4. | Care relationships in a broader perspective and challenges for healthcare practice 175
5. | Implications and recommendations for nursing practice 179
6. | Recommendations for management 186
7. | Methodological considerations 188
8. | Recommendations for further research 191
SUMMARY 207
SAMENVATTING 213
CURRICULUM VITAE 221
DANKWOORD 229

xxx
11

xxx
12
Introduction
13
Chapter I.
INTRODUCTION

Chapter I
14
Introduction
15
1 | General introduction
It is two o’clock in the afternoon. You are a patient at the orthopaedics department. Your neighbour has
been complaining of pain for the entire morning and finally asks you to call a nurse. You call a nurse,
but nobody shows up. After half an hour you get out of bed and walk to the nurse station. A few nurses
approach while they are talking and laughing. You get angry, how dare they make you wait for so long,
all the while your neighbour is in pain. In a loud and angry voice you tell them that you need a nurse
right now as your neighbour is in severe pain. One of the nurses replies she will come in a minute. You
return to your room, and wait. After another ten minutes, a nurse enters your room and tells you you
ought to be more polite in the future.1
The focus of this dissertation is broadly portrayed in this example. This example highlights different
aspects of aggression in healthcare, referring to the different perspectives in aggressive incidents and
the interactional component of aggression in care relationships. Compared to general workers,
healthcare workers have been identified as the group of employees most at risk of aggression, with
nurses prominent on the at-risk list (Wells & Bowers 2002; Estryn-Behar 2008; Wei, Chiou, Chien, &
Huang, 2016). Aggression towards nurses can arise from different sources. Research focused on
aggression of patients to nurses (Farrell & Shafiei 2012; Waschgler et al., 2013; Arnetz et al., 2015), of
family members to nurses (Lin & Liu, 2005; Hahn et al., 2012; Pich, Hazelton, & Kable 2013), of nurses
to nurses (Rowe & Sherlock, 2005; Johnson, 2009; Trépanier, Fernet, Austin, & Boudrias, 2016), and
of doctors or allied health professionals to nurses (Sofield & Salmond, 2003; Farrell & Shafiei, 2012;
Hamblin et al., 2016). This dissertation will primarily focus on the first source, namely aggression
towards nurses perpetrated by patients.
In this introduction, aggression in interpersonal relationships in healthcare including the problem of
aggression in healthcare, and the challenges in addressing aggression in healthcare will be touched
upon. Further on, the aim of the dissertation, the research objectives and an overview of the different
chapters of this dissertation will be given.
1 An experience brought by a participant (chapter IV)
Chapter I
16
1.1. | The problem of aggression in healthcare
Aggression in healthcare is not a new phenomenon, and not a new problem. When exploring aspects
of aggression in healthcare, it is important to define the concept of aggression. The word aggression
origins from the early 17th century from the Latin word aggressio(n-), from aggredi ‘to attack’ (Edward,
Ousey, Warelow, & Liu, 2014). Transferring the concept of aggression to a healthcare context has
induced a lot of different definitions of aggression, and a great deal of ambiguity and inconsistency in
defining this concept. This difficulty in defining aggression is related to the subjective aspects of
aggression (Rippon, 2000) and the multidimensionality and complex multifactorial nature of this concept
(Cutcliffe & Riahi, 2013). A cursory review of the used definitions of aggression in general literature
demonstrates diversity in defining this concept. On a more conventional or general level, the Oxford
Dictionary defines aggression as ‘feelings of anger or antipathy resulting in hostile or violent behaviour,
a readiness to attack or confront’. In earlier and rather general definitions, aggression is described as
‘an act whose goal-response is injury to another organism’ (Dollard et al., 1939 in Berkowitz 1989) or
‘any form of behaviour directed towards the goal of harming or injuring another living being who is
motivated to avoid such treatment’ (DeWall, Anderson, & Bushman, 2011). And another definition of
aggression is ‘behaviour that harms regardless of the intention of the aggressor’ (Richardson &
Hammock 2011; Edward et al., 2014). These definitions refer to ‘human aggression’ on a somewhat
general level. More recently, in defining aggression in a more specific healthcare context, aggression is
comprehensively described as ‘a negative expression of inner anxiety, which can adopt a physically
violent form, aimed at oneself, others or the material environment, or can have a verbal nature which
amounts to insulting, provocation or threatening behaviour’ (Wittouck, Audenaert & Vander Laenen,
2015) . Rippon (2000) proclaims a clear and agreed upon definition of aggression needs to be
established and compared different definitions across different contexts and studies. He concluded that
certain factors appeared to be constant in research and publications on the subject of aggression. These
factors include intent on the part of the aggressor, a cognitive process, and physical, psychological
and/or emotional harm resulting from the behaviour (Rippon, 2000). Despite the notion that there is no
universal definition of aggression and therefore no common comprehension of what constitutes
aggression, there is a plethora of research on the topic of aggression in healthcare. In addressing
aggression in healthcare, research has focused on the exposure of nurses to aggression and its
Introduction
17
prevalence, the consequences of experiencing aggression and the causes of aggression in care
relationships.
In focusing on nurses exposure to aggression, a recent review of Spector, Zhou, and Che (2014),
which provided data on 151.347 nurses from 160 samples, reported overall exposure rates of 36.4% for
physical aggression, 66.9% for nonphysical aggression, and 25% for sexual harassment (Spector et al.,
2014). Rates of exposure appeared to vary by world region, and varied in the source of aggression, with
patients accounting for most of it in Anglo (Gerberich et al., 2004; Hegney, Tuckett, Parker, & Eley,
2010) and European regions (Estryn-Behar et al., 2008; Gascón et al. 2009), whereas patients’ families
or friends were the most common source of aggression towards nurses in the Middle East (Esmaeilpour,
Salsali, & Ahmadi, 2001). These nurses exposure rates are broadly similar to those reported in other,
albeit smaller samples in European studies (Camerino et al., 2008; Estryn-Behar et al. 2008; Hahn et
al., 2010; Magnavita & Heponiemi, 2011).
The majority of studies focusing on nurses’ exposure to patient aggression were conducted in mental
health (Duxbury, 2002; Edward et al., 2015), geriatric (Zeller et al., 2009; Duxbury, Pulsford, Hadi, &
Sykes, 2013) or emergency departments (Campbell et al., 2011; Hahn et al., 2013; Wei et al., 2016).
Other settings like general hospital wards (Hahn et al., 2008; Hahn et al., 2011), paediatrics (Pich,
Hazelton, Sundin, & Kable, 2011; Pich et al., 2013), community (Geiger-Brown et al., 2007; da Silva et
al., 2015) or ambulatory care (Hahn et al., 2013) have been studied to a lesser extent. Nevertheless,
across different countries, different studies, and different contexts, research on aggression in nursing
suggests patient aggression is a problem in most -if not all- nursing settings. This particular vulnerability
of nurses is believed to be related to the frequent and longer contacts with patients and their families as
nurses are responsible for providing direct care (Catlette, 2005). Consequently, the nature, the duration
and the intensity of the care relationship with patients or their families appears to make nurses more
prone to experience aggression during their occupation (Gerberich et al., 2004; Abderhalden et al.,
2007; Waschgler et al., 2013).
Because of the increased risk that nurses face in encountering aggression during their occupation, there
has been an interest in research to understand the consequences of experiencing aggression. A
number of documented consequences have been linked to aggression in healthcare, pointing out how
the occurrence of aggression causes harm to the individual nurses, the quality of patient care, and the
organisation as a whole. Individual nurses are placed at an increased risk of injury, low morale, feelings

Chapter I
18
of vulnerability (Arnetz & Arnetz, 2001; Fry, O’ Riordan, Turner, & Mills, 2002), sleep disturbances, loss
of self-confidence (May & Grubbs, 2002), and other consequences that compromise the physical and
psychological well-being of nurses (Needham et al., 2005; Hahn et al., 2008). These consequences
even affect caregiving for future patients as research points out how nurses experience a loss of
empathy towards patients (Pich et al., 2011), increase avoidance with fewer contacts with patients
(Luckhoff et al., 2013), adopt a passive role (Needham et al., 2005), become less eager to spend time
with patients or become less willing to answer patient’s call lights (Gates, Fitzwater, & Meyer, 1999).
Consequences of experiencing aggression on the quality of patient care have been studied in a cross-
sectional study of Roche et al. (2010), pointing out how patient aggression was associated with falls,
medication errors and late administration of medications. However, Roche et al. (2010) also observed
how tensions in the work environment attributed to this observed association and hypothesised how
aggression is also related to specific unit circumstances, like for instance ward instability. Moreover,
consequences of patient aggression have also been studied on an organisational level. Several
studies have pointed out how organisations are faced with increased absenteeism (Foster, Bowers, &
Nijman, 2007; Nijman, Bowers, Oud, & Jansen, 2005), reduced job motivation (Arnetz & Arnetz, 2001;
Hahn et al., 2010; Needham et al., 2005), and increased staff turnover rates (Sofield & Salmond, 2003,
Clausen, Hogh, Carneiro, & Borg, 2013; Luckhoff et al., 2013) when being confronted with patient
aggression. These consequences are all detrimental especially in current times of nursing shortage
(Jackson, Clare, & Mannix, 2002; Camerino et al., 2008).
Alongside and inspired by research on the consequences of patient aggression on nurses, patient care
and the organisation, there has been an increased interest in understanding what causes patient
aggression. Irrespective of a healthcare context, psychologists have proposed a variety of theories to
understand why people sometimes behave aggressively. Five main theories of aggression guide most
research, and include the cognitive neoassociation theory (Berkowitz, 1989, 1990, 1993), social learning
theory (Bandura 1983, 2001), script theory (Huesmann 1986, 1988), excitation transfer theory (Zillmann
1983), and social interaction theory (Tedeschi & Felson 1994). With regard to the specific healthcare
research in this area, different theories have been developed that endeavour to explain what causes
patients to behave aggressively in a healthcare context. To provide a first general overview, three broad
conceptual models on the causation of patient aggression will be introduced: the internal, external,
and situational or interactional model (Nijman, 2002; Duxbury, 2002; Duxbury & Whittington, 2005). The
Introduction
19
main suppositions of these models explaining causes of patient aggression are discussed, connecting
these to identified risk factors for caregivers to encounter aggression. Subsequently, several theoretical
frameworks which recognise the multifactorial nature of aggression encompassing the three conceptual
models, will be briefly presented.
Internal model. According to Duxbury and Whittington (2005), research studies examining patient
aggression that are underpinned by this model are prevalent. In this particular model, individual patient
variables are believed to be the cause of aggression. This perspective has induced a lot of research to
focus on the link between aggression and particular (demographic) features of perpetrators of
aggression. Risk factors for aggression on the patients’ level have been identified, e.g. health disorders,
severe psychopathology or thought disorders (Nijman, 2002; Ayranci et al., 2006; Podubinski, Lee,
Hollander, & Daffern, 2017), intoxication because of drug and/or alcohol use (Gacki-Smith et al., 2009;
Pompeii et al., 2013), cognitive problems with advanced age (Gacki-Smith et al., 2009; Gates, Ross, &
McQueen, 2006; Hahn et al., 2013), repeated hospital admissions (James, Madeley, & Dove, 2006), or
a history of aggression towards caregivers (Reed, 1997). As a result, diagnosis and age are by far the
most frequently researched demographic variables to explain the causes of patient aggression. Whilst
features of the internal model are attractive because of the relatively fixed nature of these variables, the
predictive value of such variables keeps being called into question (Duxbury & Whittington, 2005).
External model. The external model opposes the internal model and asserts that environmental factors
contribute to the occurrence of patient aggression. Accordingly, issues that have been explored include
building deficits such as limited space or provisions of privacy, time of the day, type of regime,
overcrowding, and the impact of unit design (Duxbury, 2002; Gates et al., 2006; Gillespie, Gates, Miller,
& Howard, 2010). For instance, Pompeii et al. (2013) pointed out how long waiting times (Ayranci et al.,
2006; Gacki-Smith et al., 2009; Gates et al., 2006) and overcrowding (El-Gilany et al., 2010; Gacki-
Smith et al., 2009) were environmental conditions present at the time of an aggressive incident. External
factors as staff characteristics are also believed to have an impact upon the incidence of patient
aggression. A review of Gillespie et al. (2010) pointed out how caregivers’ gender (Ayranci et al., 2006;
Hegney et al., 2006; Camerino et al., 2008), age (Ayranci et al., 2006; Camerino et al., 2008; Thomas
et al., 2006), years of working experience (Ergün & Karadakovan, 2005), hours worked (Thomas et al.,
2006; Hegney et al., 2006), marital status (Lin & Liu, 2005), and previous workplace aggression training
(Ergün & Karadakovan, 2005) have been found to increase the risk of caregivers being targets of
Chapter I
20
aggression. However, Gillespie and colleagues (2010) do conclude that identifying healthcare workers
most at risk of experiencing aggressive events based on their characteristics is difficult because
research findings on these external factors are inconsistent.
Interactional/situational model. This model supposes it is important to examine the interaction
between groups of variants that incorporate both internal and external factors when exploring the
problem of patient aggression in healthcare. The impact of combined factors that have a negative
influence on staff-patient relationships is recognized in the situational model. A number of studies
support the view that negative staff and patient relationships might lead to patient aggression (Nijman,
2002; Duxbury, 2002). In examining research on ecologic factors influencing the likelihood of inpatient
unit aggression, Hamrin, Iennaco, & Olser, (2009) pointed out how staff who were more authoritative
and detached towards patients were more prone to aggressive encounters. Whereas staff who engaged
with patients in early intervention, were psychologically available to patients, understood patients’
perspectives and demonstrated compassionate attitudes, encountered fewer aggressive incidents
(Hamrin et al., 2009). In Duxbury et al. (2013) nurses’ perspectives towards aggressive behaviour of
older people with dementia were explored, pointing out how aggressive behaviour is largely an
interpersonal phenomenon and interactions between staff and patients are a significant cause for
patients’ aggressive responses. When aggressive behaviour arose, nurses attributed this to interactions
with other residents, or the person being denied something by staff. This perspective encompassing
situational factors as significant triggers for aggression has also been observed in other studies (Almvik,
Rasmussen, & Woods, 2006; Whall et al., 2008).
The division in these three models is interesting as it provides a tentative overview of beliefs about the
complex reasons leading to patient aggression. An understanding of beliefs towards patient aggression
is important as the way patient aggression is understood influences the way aggression is managed. As
Duxbury (2002) proclaims, the internal perspective in the internal model prevails which may contribute
to the perpetuated use of medical interventions (f.i. chemical restraint) to manage patient aggression.
Whereas if aggression is perceived as an interpersonal and situational phenomenon, a response by
interpersonal means might be preferred, in being aware of own contributions in triggering aggression
(MacDonald et al., 2007). Nevertheless, one can criticise it is difficult to make distinctions between what
is internal and external to the individual or part of the overall situation and subsequent interactions
(Duxbury & Whittington, 2005). Even though these three models are presented as distinct models, it is
Introduction
21
imperative to note there is an important interaction between these models. Risk factors for aggression
identified in the internal model might make a person more likely to engage in aggressive behaviour.
However, an individual propensity for aggression still needs to be triggered. Immediately, this points
towards the range of situational factors, identified in the conceptualization of the external and
interactional model. For example, in a study about aggression towards healthcare workers in a paediatric
emergency department, Gillespie et al. (2008) identified patients’ and families’ inability to deal with a
crisis situation to be a risk factor for aggression. However, in considering the context and characteristics
of paediatric emergencies, it is important to understand patients’ or families’ behaviour, even if it is
aggressive, from both an internal, external and situational model. Consequently, the division in three
broad conceptual models is interesting, but an interrelation between these models needs to be
acknowledged to generate a comprehensive understanding of patient aggression. This
acknowledgement of different factors contributing to patient aggression is present in the existing
theoretical frameworks regarding patient aggression in healthcare. These frameworks acknowledge the
complexity of the interrelation of different risk factors in explaining why patients behave aggressively in
a healthcare context. Most theoretical frameworks on aggression in healthcare consider aggression to
be a complex and multi-faceted phenomenon, with a variety of triggering factors, behaviours, and
consequences beyond the individual perpetrator. For instance, Nijman’s model, in trying to shed light
on the mechanisms that lead to aggression, elucidates how certain patient, staff and ward characteristics
may interact in causing patient aggression (Nijman, 2002). Likewise, Hamrin and colleagues pointed out
how aggression in inpatient mental health units results from a multitude of factors, including individual
patient and staff factors, the complex interaction between patients and staff, and the unit and
organizational culture (Hamrin et al., 2009). The Safewards model of Bowers (2014) also uses a
comprehensive structure in referring to a dynamic interaction between staff modifiers and patient
modifiers, which may lead to conflict and containment on mental health wards. Even though most of
these theoretical frameworks have been developed in specific settings like the mental healthcare setting
(Nijman, 2002; Hamrin et al., 2009; Bowers, 2014), they provide a set of explicable principles about
patient aggression which could be transferred to other healthcare settings. Although there are inherent
differences among various healthcare settings, transferring insights can be based on the similarity that
care is provided for patients in vulnerable situations. And in addition, the notion that patient aggression
occurs in interpersonal care relationships, irrespective of the context of the specific healthcare setting.

Chapter I
22
1.2. | Challenges in addressing aggression in healthcare
Despite the important insights generated through the extant research on aggression in healthcare, some
issues regarding aggression in care relationships remain unclear or under-researched. These
issues induce challenges in understanding aggressive behaviour in care relationships. These issues
pertain to a scarcity of knowledge on aggression in more general hospital settings, a paucity of insight
into patients’ perspectives of aggression, a limited to no insight into perceptions or meanings of
aggression, and a lack of insight into team dynamics in nursing teams in processing patient aggression.
These issues will be elaborated upon below.
Knowledge on the occurrence of patient aggression in more general settings. As mentioned
before, the problem of aggression towards nurses has been a subject of research for decades. Most
studies have focused on geriatric (Almvik et al., 2006; Duxbury et al., 2013), emergency (Gerdtz et al.,
2013), and mental healthcare settings (Abderhalden et al., 2007). Little knowledge is available about
patient aggression in more general medical and surgical care units or in primary care. Because of some
differences, self-evidently generalizing results from for instance emergency settings to general hospitals
or primary care might induce challenges (Winstanley & Whittington, 2004). For example, the specific
nurses’ work climate in primary care might influence the occurrence of patient aggression as nurses
often perform activities outside health centres (such as private home visits), generally work alone (da
Silva et al., 2015) and cannot rely on the protection that is present in hospital settings (e.g. the presence
of colleagues, alarm systems) (Geiger-Brown et al., 2007). Likewise, according to Roche et al. (2010),
general hospital settings are increasingly regarded to be vulnerable for aggressive incidents. Few
studies focused on the occurrence of patient aggression in general hospital settings (Hahn et al., 2013;
Heckemann et al., 2015). Although the work of Hahn (2011) has made a significant contribution to the
understanding of patient and visitor violence in general hospital settings in Switzerland and other
German-speaking countries, much can still be learned about the occurrence of patient aggression in the
former settings (Winstanley & Whittington 2004; Wei et al., 2016). So far, scarce initiatives have been
undertaken to focus on patient aggression in a general hospital setting or in primary care in Belgium.
Insight into patients’ perspectives of aggression. Even though there is a plethora of research on
aggression in healthcare, surprisingly little is known about the patient’s perspective regarding
aggression in care relationships. Despite concerns about ethical dilemmas associated with exploring
patient perspectives (Duxbury & Whittington, 2005), it is necessary to understand how patients construe

Introduction
23
care relationships with caregivers and how they experience aggressive or negative interactions with
caregivers. The focus in research on aggression in healthcare is rather unilateral as the majority of
research starts off with the caregivers’ perspective and explores caregivers’ experiences of patient
aggression (Jansen, Dassen, Groot, & Jebbink, 2005; Gale et al., 2009; Farrell & Shafiei, 2012). Few
studies adopt the patients’ perspective (Duxbury, 2002; Duxbury & Whittington, 2005) to understand
how patients might experience negative, aggressive or untoward behaviour of caregivers. Exploration
of patients’ perspectives is important as professional staff and researchers will tend to see the world in
a particular way, and thus are likely to be more or less ignorant of how patients experience the world
(Gudde, Olso, Whittington, & Vatne, 2015). Directly comparing both patients’ and staff’ perspectives on
the causes of aggression, Duxbury and Whittington (2005) pointed out how both perspectives differ
significantly.
On a more general level, patients’ views of healthcare are considered an essential component of health
service evaluations. They are used to assess how well services are provided at a local level (McPherson,
Kayes, Moloczij, & Commins, 2014), to obtain feedback to healthcare workers to improve quality of care
(Cominskey, Coyne, Lalor, & Begley, 2014), or as an outcome measure to evaluate organizational
changes (Metzelthin et al., 2013). In literature and in practice, patient satisfaction surveys are regarded
as a valid method to obtain patients’ views of healthcare and are as such frequently used (You et al.,
2013; Lehto, Helander, Taari, & Aromaa, 2014). Alongside the reservations that exist about the validity
of patient satisfaction as a concept and the instruments used to measure it (William 1994), patient
satisfaction surveys do not seem sensitive enough in eliciting disappointment, negative experiences or
untoward and aggressive behaviour of caregivers (Coyle & Williams, 2001). Therefore, it is important to
gain insight into the patient’s perspective regarding aggressive or negative interactions with healthcare
staff. And in literature, the importance of drawing on experiences of both staff and patients if one wishes
to understand aggression in care relationships in a comprehensive way, is acknowledged (Gudde et al.,
2015).
Insight into perceptions and the meaning of aggression. As previously mentioned, the internal,
external and interactional model on causes of aggression refers to reasons as to why patients can
behave aggressively in a healthcare context (Nijman, 2002; Duxbury, 2002; Duxbury & Whittington,
2005). These entailed different viewpoints of aggression and aggressive behaviour which impact the
nature of the approach to managing aggressive incidents (Jansen et al., 2005; Duxbury, Hahn,
Chapter I
24
Needham, & Pulsford, 2008). Although this relation between perceptions of aggression and intervention
strategies in managing aggression is acknowledged, little is known about how nurses perceive and think
about patient aggression (Winstanley & Whittington, 2004; Catlette, 2005; Needham et al., 2005). Just
a few instruments are available to assess perceptions of aggression. For instance, the (shortened
version of the) Perception of Aggression Scale (Jansen, Dassen, & Moorer, 1997; Needham et al.,
2004), the Attitude towards Aggression Scale (Jansen et al., 2005), and the Management of Aggression
and Violence Attitude Scale (Duxbury, 2002) are some instruments to assess perceptions, attitudes or
beliefs towards aggression. These kind of instruments typically adopt statements about or definitions of
aggression as starting-points to explore participants’ perceptions about aggression. Although this
approach renders relevant information in assessing perceptions of aggression, a discernible difficulty
arises. When statements or definitions of aggression are used, the concept of aggression is represented
as a measurable, uniform phenomenon, free of context and meaning. There is a basic assumption that
the same statements about the phenomenon of aggression have the same meaning for all subjects,
which can be understood as way of objectifying the phenomenon of aggression. However, surveying
the phenomenon of aggression in this objectifying approach sidesteps the notion that perceptions of
what aggression means, vary between persons. Aggression means something that is different for
various individuals as the specific context, and assigned meaning of aggression take on a crucial role
in how aggression is perceived (O’Connell et al., 2000; Duxbury, 2003). This means that the subjective
experience of aggression, with an inherent diversity among individuals, cannot easily be integrated in
statements, measurement instruments or definitions of aggression. However, at present, no insight
exists on the subjective meaning of aggression in care relationships between nurses and patients.
Insight into team dynamics in nursing teams in addressing patient aggression. In addressing
nurses’ perspectives of aggression in care relationships, most studies focus on the perspective of
singular nurses. Group dynamics and interactions with other team members that can influence individual
nurse’s experiences are scarcely taken into consideration. The influence of team members and group
interactions can be essential as research has noted how peer pressure from other nursing staff appears
to be one of the reasons incidents are not reported (Rippon, 2000, Sato, Wakabayashi, Kiyoshi-Teo, &
Fukahori, 2013). This finding suggests nurses can be affected or even swayed by colleagues with
regards to perceiving, managing or eventually reporting aggression. Reasons as to why and how nurses
are influenced by colleagues can be found in literature on socializing processes in nursing teams
Introduction
25
(Bisholt, 2012; Feng & Tsai, 2012; Thrysou, Hounsgaard, Dohn, & Wagner, 2012). The concept
‘professional socialization’ (Mooney, 2007; Bisholt, 2012) refers to processes through which
practitioners are merged into the profession (Mooney, 2007). This process entails that newcomers
gradually acquire attitudes, values, and norms of professional clinical practitioners (Mooney, 2007; Feng
& Tsai, 2012) while learning (in)formal rules of the organisation (Maben, Latter, & Clark, 2006). These
studies commonly focus on experiences of recently qualified nurses (Bisholt, 2012) or Baccalaureate
nursing students (Secrest, Norwood, & Keatley, 2002). It can be hypothesized that similar processes of
socialisation remain present in nurses who have been working for some time in nursing practice
(Yarbrough, Martin, Alfred, & McNeill, 2016). Likewise, it remains unclear how these processes influence
patient’s care or the conduct towards patients following experiences of patient aggression. There is little
knowledge at hand surrounding nurses’ interactions and team dynamics in perceiving and addressing
patients’ aggressive behaviour.
1.3. | General objectives and outline of this dissertation
This dissertation aims to contribute to the literature on aggression in care relationships by providing
tentative answers to these various presented challenges. This dissertation will focus on under-
researched nurses’ work settings, use both an objectifying and a subjectifying approach in
understanding aggression in care relationships, adopt both the nurses’ and patients’ perspective in
perceiving aggression, and examine group dynamics in nursing teams in perceiving and addressing
patient aggression. The studies discussed in this dissertation are divided into two major parts, and
guided by different research objectives. These will be further explained below.
To gain knowledge on the occurrence of patient aggression in more general settings and nurses ’
perceptions of aggression, the first part of this dissertation focuses on gaining a broad indication of
nurses’ experiences of aggression in the general hospital setting and in primary care in Belgium. An
assessment instrument was needed to provide information on frequencies and characteristics of patient
aggression, and nurses’ perceptions of aggression working in these settings. In chapter II, the
translation and psychometric validation of three assessment instruments is addressed, formulating
following research objectives:
To translate the Survey of Violence Experienced by Staff (SOVES), the shortened Perception
of Aggression Scale (POAS-s) and the Perception of Importance of Intervention Skills Scale
(POIS) and adapt these instruments for use in general hospital settings.
Chapter I
26
To assess psychometric properties (content validity, construct validity, stability, and internal
consistency) of the translated versions of these instruments in general hospital settings.
Following the translation and psychometric validation of these assessment instruments, chapter III
outlines the results of a cross-sectional study. This cross-sectional study focuses on nurses’ experiences
of patient aggression and aggression by patients’ family members in primary care and in general hospital
settings. In addition, factors associated with nurses’ perceptions of aggression and its management
were identified through a sample of 769 nurses working in primary care and in general hospital settings.
Following research objectives were formulated:
To compare nurses’ experiences of patient aggression and aggression by patients’ family
members in both primary care and general hospital settings.
To identify associations between patient-related, nurse-related and work-related characteristics
and nurses’ perceptions of aggression and its management.
In the second part of this dissertation, an understanding of the meaning of aggression was sought. In
contrast to the rather objectifying approach towards aggression that was adopted in the previous
chapters, following chapters adopt a more subjectifying approach of the concept of aggression. A
subjectifying approach focuses on a form of inductive reasoning to understand aggression in healthcare,
and consequently, how perceptions of aggression can emerge. In order to reach understanding of the
meaning of aggression, the term ‘transgressive behaviour’ was adopted. The use of this term allows
returning to the ‘essence’ of experiencing aggression, namely a crossing of own limits, standards or
norms. This encompasses a subjective interpretation of when and what limits are exceeded for situations
to be experienced as transgressive. In contrast to a more objectifying approach, a subjectifying approach
does not determine in advance which behavioural acts count as aggression, or which ethical or moral
principles are at stake when perceiving transgressive behaviour. As such, the specific context and
assigned meaning of aggression are integrated in trying to understand the meaning of aggression. This
means that both nurses’ and patients’ own experiences of transgressive behaviour provided the starting-
point to gain an understanding of the meaning of aggression and the explanatory underlying processes
of how these perceptions emerge. Chapter IV addresses the meaning of transgressive behaviour in
care relationships with nurses from the patient’s perspective in a general hospital ward setting,
formulating following research objectives:
Introduction
27
To gain insight into what it is like for patients to experience transgressive behaviour in care
relationships with nurses.
To gain insight into processes or mechanisms that influence perceived seriousness of
transgressive behaviour from the patients’ perspective.
As it was important to gain an understanding of the dynamics of the nurse-patient care relationship, the
nurses’ perspective regarding the onset and meaning of patients’ transgressive behaviour is outlined in
chapter V, which is guided by the following research objectives:
To gain insight into behaviour in the patient-nurse relationship that is perceived as transgressive
from the nurses’ perspective.
To gain insight into processes or mechanisms that influence perceived seriousness of patients’
transgressive behaviour.
As these results pointed out the necessity to understand group dynamics in nursing teams in
perceiving and handling transgressive behaviour, a final chapter VI provides an understanding of the
influence of team members in how nurses perceive and address patients’ transgressive behaviour.
Following broad research objective was formulated:
To explore and understand group dynamics and the influence of team members on how
nurses perceive and deal with transgressive behaviour in care relationships with patients.
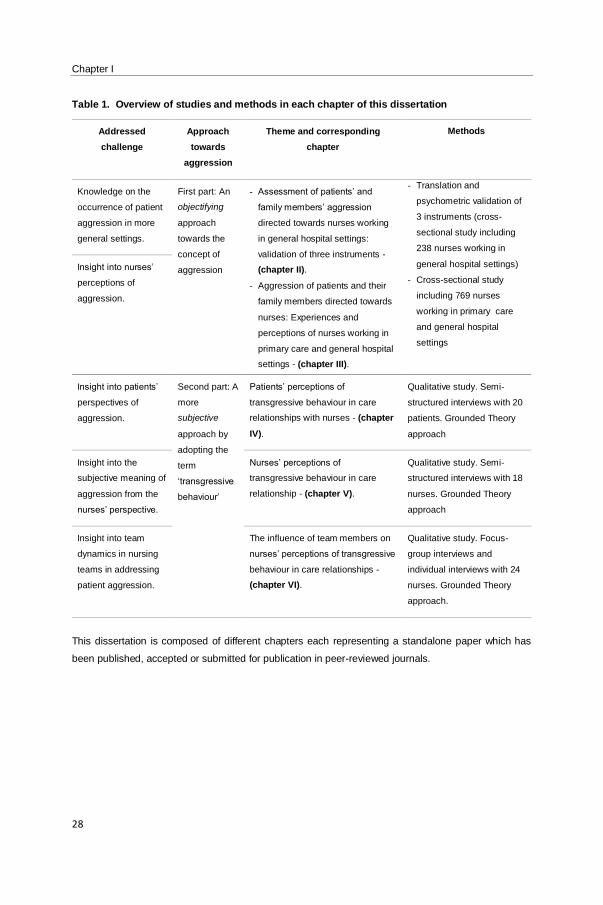
A brief overview of the addressed challenges, the used approach of aggression, and the methods
employed in each study is included in table 1, and described in more detail in the subsequent chapters.
The third part of this dissertation, chapter VII, provides a general discussion of the findings of this
dissertation. In addition, the relevance of these findings for nursing practice and nursing management
are outlined. Finally, recommendations for further research are presented.
Chapter I
28
Table 1. Overview of studies and methods in each chapter of this dissertation
Addressed
challenge
Approach
towards
aggression
Theme and corresponding
chapter
Methods
Knowledge on the
occurrence of patient
aggression in more
general settings.
First part: An
objectifying
approach
towards the
concept of
aggression
- Assessment of patients’ and
family members’ aggression
directed towards nurses working
in general hospital settings:
validation of three instruments -
(chapter II).
- Aggression of patients and their
family members directed towards
nurses: Experiences and
perceptions of nurses working in
primary care and general hospital
settings - (chapter III).
- Translation and
psychometric validation of
3 instruments (cross-
sectional study including
238 nurses working in
general hospital settings)
- Cross-sectional study
including 769 nurses
working in primary care
and general hospital
settings
Insight into nurses’
perceptions of
aggression.
Insight into patients’
perspectives of
aggression.
Second part: A
more
subjective
approach by
adopting the
term
‘transgressive
behaviour’
Patients’ perceptions of
transgressive behaviour in care
relationships with nurses - (chapter
IV).
Qualitative study. Semi-
structured interviews with 20
patients. Grounded Theory
approach
Insight into the
subjective meaning of
aggression from the
nurses’ perspective.
Nurses’ perceptions of
transgressive behaviour in care
relationship - (chapter V).
Qualitative study. Semi-
structured interviews with 18
nurses. Grounded Theory
approach
Insight into team
dynamics in nursing
teams in addressing
patient aggression.
The influence of team members on
nurses’ perceptions of transgressive
behaviour in care relationships -
(chapter VI).
Qualitative study. Focus-
group interviews and
individual interviews with 24
nurses. Grounded Theory
approach.
This dissertation is composed of different chapters each representing a standalone paper which has
been published, accepted or submitted for publication in peer-reviewed journals.
Introduction
29
REFERENCES
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Fischer, J.E., & Haug, H.J. (2007). Frequency and
severity of aggressive incidents in acute psychiatric wards in Switzerland. Clinical Practice and Epidemiology in
Mental Health, 4, 3–30.
Almvik, R., Rasmussen, K., & Woods, P. (2006). Challenging behaviour in the elderly-monitoring violent incidents.
Internal Journal of Geriatric Psychiatry, 21(4), 368-74.
Arnetz, J. E., & Arnetz, B. B. (2001). Violence towards health care staff and possible effects on the quality of
patient care. Social Science & Medicine, 52(3), 417-27.
Arnetz, J. E., Hamblin, L., Essenmacher, L., Upfal, M. J., Ager, J., & Luborsky, M. (2015). Understanding patient-
to-worker violence in hospitals: a qualitative analysis of documented incident reports. Journal of Advanced
Nursing, 71(2), 338-48.
Ayranci, U., Yenilmez, C., Balci, Y., & Kaptanoglu, C. (2006). Identification of violence in Turkish health care
settings. Journal of Interpersonal Violence, 21(2), 276-96.
Bandura, A. (1983). Psychological mechanisms of aggression. In R. G. Geen & E. Donnerstein (Eds.),
Aggression: Theoretical and empirical reviews (pp. 1-40). New York: Academic Press.
Bandura, A. (2001). Social cognitive theory: an agentic perspective. Annual Review of Psychology, 52, 1–26.
Berkowitz, L. (1989). Frustration-aggression hypothesis: examination and reformulation. Psychological Bulletin,
106(1), 59-73.
Berkowitz, L. (1990). On the formation and regulation of anger and aggression: a cognitive neo associationistic
analysis. The American Psychologist, 45, 494-503.
Berkowitz, L. (1993). Pain and aggression: some findings and implications. Motivation and Emotion, 17, 277-93.
Bisholt, B. K. (2012). The professional socialization of recently graduated nurses–experiences of an introduction
program. Nurse Education Today, 32(3), 278–282.
Bowers, L. (2014). Safewards: a new model of conflict and containment on psychiatric wards. Journal of
Psychiatric and Mental Health Nursing, 21(6), 499-508).
Camerino, D., Estryn-Behar, M., Conway, P. M., van Der Heijden, B. I. & Hasselhorn, H. M. (2008). Work-related
factors and violence among nursing staff in the European NEXT study: a longitudinal cohort study. International
Journal of Nursing Studies, 45(1), 35–50.
Campbell, J. C., Messing, J. T., Kub, J., Agnew, J., Fitzgerald, S., Fowler, B., Sheridan, D., Lindauer, C., Deaton,
J., & Bolyard, R. (2011). Workplace violence: prevalence and risk factors in the safe at work study. Journal of
Occupational and Environmental Medicine, 53(1), 82-9.
Chapter I
30
Catlette, M. (2005). A descriptive study of the perceptions of workplace violence and safety strategies of nurses
working in level I trauma centers. Journal of Emergency Nursing, 31(6), 519-25.
Clausen, T., Hogh, A., Carneiro, I. G., & Borg, V. (2013). Does psychological well-being mediate the association
between experiences of acts of offensive behaviour and turnover among care workers? A longitudinal analysis.
Journal of Advanced Nursing, 69(6), 1301-13.
Cominskey, C., Coyne, I., Lalor, J., & Begley, C. (2014). A national cross-sectional study measuring predictors for
improved service user outcomes across clinical nurse or midwife specialist, advanced nurse practitioner and
control sites. Journal of Advanced Nursing 70(5), 1128–1137.
Coyle, J., & Williams, B. (2001). Valuing people as individuals: development of an instrument through a survey of
person-centredness in secondary care. Methodological Issues in Nursing Research, 36(3), 450–459.
Cutcliffe, J. R., & Riahi, S. (2013). Systemic perspective of violence and aggression in mental health care:
Towards a more comprehensive understanding and conceptualization: Part 1. International Journal of Mental
Health Nursing, 22, 558–567.
Da Silva, A. T., Peres, M. F., Lopes, Cde S., Schraiber, L. B., Susser, E., & Menezes, P. R. (2015). Violence at
work and depressive symptoms in primary health care teams: a cross-sectional study in Brazil. Social psychiatry
and psychiatric epidemiology, 50(9), 1347-55.
DeWall, C. N., Anderson, C. A., & Bushman, B. J. (2011). The general aggression model: Theoretical extensions
to violence. Psychology of Violence, 1(3), 245-258.
Dollard, J., Doob, L., Miller, N., Mowrer, O., & Sears, R. (1939). Frustration and aggression. New Haven, CT: Yale
University Press.
Duxbury, J. (2002). An evaluation of staff and patient views of and strategies employed to manage inpatient
aggression and violence on one mental health unit: A pluralistic design. Journal of Psychiatric and Mental Health
Nursing, 9(3), 325–337.
Duxbury, J. (2003). Testing a new tool: the Management of Aggression and Violence Attitude Scale (MAVAS).
Nurse Researcher, 10(4), 39-52.
Duxbury, J., & Whittington, R. (2005). Causes and management of patient aggression and violence: Staff and
patient perspectives. Journal of Advanced Nursing, 50(5), 469–478.
Duxbury, J., Hahn, S., Needham, I., & Pulsford, D. (2008). The Management of Aggression and Violence Attitude
Scale (MAVAS): a cross-national comparative study. Journal of Advanced Nursing, 62(5), 596-606.
Duxbury, J., Pulsford, D., Hadi, M., & Sykes, S. (2013). Staff and relatives' perspectives on the aggressive behaviour
of older people with dementia in residential care: a qualitative study. Journal of Psychiatric and Mental Health
Nursing, 20(9), 792-800.
Introduction
31
Edward, K. L., Ousey, K., Warelow, P., & Lui, S. (2014). Nursing and aggression in the workplace: A systematic
review. British Journal of Nursing, 23(12), 653–659.
Edward, K. L., Stephenson, J., Ousey, K., Lui, S., Warelow, P., & Giandinoto, J.A. (2016). A systematic review
and meta-analysis of factors that relate to aggression perpetrated against nurses by patients/relatives or staff.
Journal of Clinical Nursing, 25(3-4), 289-99.
El-Gilany, A. H., El-Wehady, A., & Amr, M. (2010). Violence against primary health care workers in Al-Hassa,
Saudi Arabia. Journal of Interpersonal Violence, 25(4), 716-34.
Ergün, F. S., & Karadakovan, A. (2005). Violence towards nursing staff in emergency departments in one Turkish
city. International Nursing Review, 52, 154–160.
Esmaeilpour, M., Salsali, M., & Ahmadi, F. (2011). Workplace violence against Iranian nurses working in
emergency departments. International Nursing Review, 58, 130–137.
Estryn-Behar, M., van der Heijden, B., Camerino, D., Fry, C., Le Nezet, O., Conway, P.M., Hasselhorn, H.M., &
NEXT Study Group. (2008). Violence risk in nursing – results from the European ‘NEXT’ study. Occupational
Medicine, 58(2), 107–114.
Farrell, G. A., & Shafiei, T. (2012). Workplace aggression, including bullying in nursing and midwifery: a
descriptive survey (the SWAB study). International Journal of Nursing Studies, 49(11), 1423-31.
Feng, R. F., & Tsai, Y. F. (2012). Socialisation of new graduate nurses to practicing nurses. Journal of Clinical
Nursing, 21(13–14), 2064–2071.
Foster, C., Bowers, L., & Nijman H. (2007). Aggressive behavior on acute psychiatric wards: prevalence, severity
and management. Journal of Advanced Nursing, 58(2), 140–149.
Fry, A. J., O'Riordan, D., Turner, M., & Mills K. L. (2002). Survey of aggressive incidents experienced by
community mental health staff. International Journal of Mental Health Nursing, 11(2), 112-20.
Gacki-Smith, J., Juarez, A. M., Boyett, L., Homeyer. C., Robinson. L., & MacLean, S.L. (2009). Violence against
nurses working in US emergency departments. Journal of Nursing Administration, 39(7), 340-9.
Gale, C., Hannah, A., Swain, N., Gray, A., Coverdale, J., & Oud, N. (2009). Patient aggression perceived by
community support workers. Australasian Psychiatry, 17(6), 497-501.
Gascón, S., Martinez-Jarreta, B., González-Andrade, J. F., Santed, M. A., Casalod, Y., & Rueda, M. A. (2009).
Aggression towards health care workers in Spain: A multi-facility study to evaluate the distribution of growing
violence among professionals, health facilities and departments. International Journal of Occupational &
Environmental Health, 15, 29–35.
Gates, D. M., Fitzwater, E., & Meyer, U. (1999). Violence against caregivers in nursing homes: Expected,
tolerated, and accepted. Journal of Gerontological Nursing, 25(4), 12–22.
Chapter I
32
Gates, D. M., Ross, C. S., & McQueen, L. (2006). Violence against emergency department workers. The Journal
of Emergency Medicine, 31(3), 331–337.
Geiger-Brown, J., Muntaner, C., McPhaul, K., Lipscomb, J., & Trinkoff, A. (2007). Abuse and violence during
home care work as predictor of worker depression. Home health care services quarterly, 26(1), 59-77.
Gerberich, S. G., Church, T. R., McGovern, P. M., Hansen, H. E., Nachreiner, N. M., Geisser, M. S., Ryan, A. D.,
Mongin, S. J. & Watt, G. D. (2004). An epidemiological study of the magnitude and consequences of work related
violence: the Minnesota Nurses’ Study. Occupational and Environmental Medicine, 61(6), 495–503.
Gerdtz, M. F., Daniel, C., Dearie, V., Permatunga, R., Bamert, M., & Duxbury, J. (2013). The outcome of a rapid
training program on nurses’ attitudes regarding the prevention of aggression in emergency departments: a multi -
site evaluation. International Journal of Nursing Studies, 50(11), 1434–45.
Gillespie, G. L. (2008). Violence against healthcare workers in a pediatric emergency department. Unpublished
dissertation, University of Cincinnati.
Gillespie, G. L., Gates, D. M., Miller, M., & Howard, P. K. (2010). Workplace violence in healthcare settings: risk
factors and protective strategies. Rehabilitation Nursing, 35(5), 177-84.
Gudde, C. B., Olsø, T. M., Whittington, R., & Vatne S. (2015). Service users' experiences and views of aggressive
situations in mental health care: a systematic review and thematic synthesis of qualitative studies. Journal of
Multidisciplinary Healthcare, 3(8),449-62.
Hahn, S., Zeller, A., Needham, I., Kok, G., Dassen, T., & Halfens, R. J. G. (2008). Patient and visitor violence in
general hospitals: a systematic review of the literature. Aggression and Violent Behavior, 13, 431–441.
Hahn, S., Müller, M., Needham, I., Dassen, T., Kok, G., & Halfens, R. J. G. (2010). Factors associated with
patient and visitor violence experienced by nurses in general hospitals in Switzerland: a cross-sectional survey.
Journal of Clinical Nursing, 19(23–24), 3535–3546.
Hahn, S., Müller, M., Needham, I., Dassen, T., Kok, G., & Halfens, R. J. (2011). Measuring patient and visitor
violence in general hospitals: feasibility of the SOVES-G-R, internal consistency and construct validity of the
POAS-S and the POIS. Journal of Clinical Nursing, 20(17-18), 2519-30.
Hahn, S. (2011). Patient and visitor violence against health care staff in general hospitals. Unpublished
dissertation. Maastricht University.
Hahn, S., Hantikainen, V., Needham, I., Kok, G., Dassen, T., & Halfens, R. J. G. (2012). Patient and visitor
violence in the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey.
Journal of Advanced Nursing, 68(12), 2685–2699.
Hahn, S., Müller, M., Hantikainen, V., Kok, G., Dassen, T., & Halfens R. J. G. (2013). Risk factors associated with
patient and visitor violence in general hospitals: results of a multiple regression analysis. International Journal of
Nursing Studies, 50(3), 374–385.
Introduction
33
Hamblin, L. E., Essenmacher, L., Ager, J., Upfal, M., Luborsky, M., Russell, J., & Arnetz, J. (2016). Worker-to-
Worker Violence in Hospitals: Perpetrator Characteristics and Common Dyads. Workplace Health & Safety, 64(2),
51-6.
Hamrin, V., Iennaco, J., & Olsen, D. (2009). A review of ecological factors affecting inpatient psychiatric unit
violence: implications for relational and unit cultural improvements. Issues in Mental Health Nursing, 30(4), 214-
26.
Heckemann, B., Zeller, A., Hahn, S., Dassen, T., Schols, J. M., & Halfens, R. J. (2015). The effect of aggression
management training programmes for nursing staff and students working in an acute hospital setting. A narrative
review of current literature. Nurse Education Today, 35(1), 212–219.
Hegney, D., Eley, R., Plank, A., Buikstra, E., & Parker, V. (2006). Workplace violence in Queensland, Australia:
The results of a comparative study. International Journal of Nursing Practice, 12, 220–231.
Hegney, D., Tuckett, A., Parker, D., & Eley, R. M. (2010). Workplace violence: Differences in perceptions of
nursing work between those exposed and those not exposed: A cross-sector analysis. International Journal of
Nursing Practice, 16, 188–202.
Huesmann, L. R. (1986). Psychological processes promoting the relation between exposure to media violence
and aggressive behavior by the viewer. Journal of Social Issues, 42, 125-40.
Huesmann, L. R. (1988). An information processing model for the development of aggression. Aggressive
Behavior, 14, 13–24.
Jackson, D., Clare, J., & Mannix, J. (2002). Who would want to be a nurse? Violence in the workplace--a factor in
recruitment and retention. Journal of Nursing Management, 10(1), 13-20.
James, A., Madeley, R., & Dove, A. (2006). Violence and aggression in the emergency department. Emergency
Medicine Journal, 23(6), 431–434.
Jansen, G., Dassen, T., & Moorer, P. (1997). The perception of aggression. Scandinavian Journal of Caring
Sciences, 11(1), 51-5.
Jansen, G. J., Dassen, T. W., & Groot Jebbink, G. (2005). Staff attitudes towards aggression in health care: A
review of the literature. Journal of Psychiatric and Mental Health Nursing, 12(1), 3–13.
Johnson, S. L. (2009). International perspectives on workplace bullying among nurses: a review. International
Nursing Review, 56(1), 34-40.
Lehto, U., Helander, S., Taari, K., & Aromaa, A. (2014). Patient experiences at diagnosis and psychological well -
being in prostate cancer: a Finnish national survey. European Journal of Oncology Nursing, 19(3), 220–229.
Lin, Y. H., & Liu, H. E. (2005). The impact of workplace violence on nurses in South Taiwan. International Journal
of Nursing Studies, 42, 773–778.
Chapter I
34
Luckhoff, M., Jordaan, E., Swart, Y., Cloete, K. J., Koen, L., & Niehaus, D. J. (2013). Retrospective review of
trends in assaults and seclusion at an acute psychiatric ward over a 5-year period. Journal of Psychiatric and
Mental Health Nursing, 20(8), 687-95.
Maben, J., Latter, S., & Clark, J. M. (2006). The theory–practice gap: Impact of professional–bureaucratic work
conflict on newly-qualified nurses. Journal of Advanced Nursing, 55(4), 465–477.
MacDonald, C. (2007). Care assistants’ views and experience of ‘challenging behaviour’ in dementia. Journal of
Dementia Care, 14, 33–38.
Magnavita, N., & Heponiemi, T. (2011). Workplace violence against nursing students and nurses: An Italian
experience. Journal of Nursing Scholarship, 43, 203–210.
May, D. D., & Grubbs, L. M. (2002). The extent, nature, and precipitating factors of nurse assault among three
groups of registered nurses in a regional medical center. Journal of Emergency Nursing, 28(1); 11-7.
Metzelthin, S. F., Danïels, R., van Rossum, E., Cox, K., Habets, H., de Witte, L. P. & Kempen, G. I. (2013). A
nurse-led interdisciplinary primary care approach to prevent disability among community dwelling frail older
people: a large-scale process evaluation. International Journal of Nursing Studies, 50(9), 1184–1196.
McPherson, K. M., Kayes, N. K., Moloczij, N., & Commins, C. (2014). Improving the interface between informal
carers and formal health and social services: a qualitative study. International Journal of Nursing Studies, 51(3),
418–429.
Mooney, M. (2007). Professional socialization: The key to survival as a newly qualified nurse. International
Journal of Nursing Practice, 13(2), 75–80.
Needham, I., Abderhalden, C., Dassen, T., Haug, H. J., & Fischer, J. E. (2004). The perception of aggression by
nurses: psychometric scale testing and derivation of a short instrument. Journal of Psychiatric and Mental Health
Nursing, 11(1), 36-42.
Needham, I., Abderhalden, C., Halfens, R. J. G., Fischer, J. E., & Dassen, T. (2005). Non-somatic effects of
patient aggression on nurses: a systematic review. Journal of Advanced Nursing, 49(3), 283–296.
Nijman, H. L. I. (2002). A model of aggression in psychiatric hospitals. Acta Psychiatrica Scandinavica, 106, 142–
143.
Nijman, H., Bowers, L., Oud, N., & Jansen, G. (2005). Psychiatric nurses’ experiences with inpatient aggression.
Aggressive Behaviour, 31(3), 217–227.
O’Connell, B., Young, J., Brooks, J., Hutchings, J., & Lofthouse, J. (2000). Nurses’ perceptions of the nature and
frequency of aggression in general ward settings and high dependency areas. Journal of Clinical Nursing, 9(4),
602–610.
Pich, J., Hazelton, M., Sundin, D., & Kable, A. (2011). Patient-related violence at triage: A qualitative descriptive
study. International Emergency Nursing, 19(1), 12–19.
Introduction
35
Pich, J., Hazelton, M., & Kable, A. (2013). Violent behaviour from young adults and the parents of paediatric
patients in the emergency department. International Emergency Nursing, 21(3), 157-62.
Podubinski, T., Lee, S., Hollander, Y., & Daffern, M. (2017). Patient characteristics associated with aggression in
mental health units. Psychiatry Research, 250, 141-145.
Pompeii, L., Dement, J., Schoenfisch, A., Lavery, A., Souder, M., Smith, C., & Lipscomb, H. (2013). Perpetrator,
worker and workplace characteristics associated with patient and visitor perpetrated violence (Type II) on hospital
workers: a review of the literature and existing occupational injury data. Journal of Safety Research, 44, 57-64.
Reed, J. (1997). Risk assessment and clinical risk management: the lessons from recent inquiries. British Journal
of Psychiatry, 170 (32), 4-7.
Richardson, D.S., & Hammock, G. S. (2011). Is it aggression? Perceptions of and motivations for passive and
psychological aggression. In Forgas J.P, Arie W. Kruglanski A.W., & Williams K.P. - The Psychology of Social
Conflict and Aggression. New York – London: Psychology Press, Taylor & Francis Group.
Rippon, T. J. (2000). Aggression and violence in health care professions. Journal of Advanced Nursing, 31(2),
452–460.
Roche, M., Diers, D., Duffield, C., & Catling-Paull, C. (2010). Violence toward nurses, the work fenvironment, and
patient outcomes. Journal of Nursing Scholarship, 42(1), 13-22.
Rowe, M. M., & Sherlock H. (2005). Stress and verbal abuse in nursing: do burned out nurses eat their young?
Journal of Nursing Management, 13(3), 242-8.
Sato, K., Wakabayashi, T., Kiyoshi-Teo, H., & Fukahori, H. (2013). Factors associated with nurses’ reporting of
patients’ aggressive behavior: A cross-sectional survey. International Journal of Nursing Studies, 50(10), 1368–
1376.
Secrest, J. A., Norwood, B. R., & Keatley, V. M. (2003). ‘I was actually a nurse’: The meaning of professionalism
for baccalaureate nursing students. The Journal of Nursing Education, 42(2), 77–82.
Spector, P. E., Zhou, Z. E., & Che, X. X. (2014). Nurse exposure to physical and nonphysical violence, bullying
and sexual harassment: a quantitative review. International Journal of Nursing Studies, 51(1), 72–84.
Sofield, L., & Salmond, S. W. (2003). Workplace violence. A focus on verbal abuse and intent to leave the
organization. Orthopedic Nursing, 22(4), 274-83.
Tedeschi, J. T., & Felson, R. B. (1994). Violence, Aggression, & Coercive Actions. Washington DC: American
Psychological Association.
Thomas, N. I., Brown, N. D., Hodges, L. C., Gandy, J., Lawson, L. Lord, J. E., & Williams, D. K. (2006). Risk
profiles for four types of work-related injury among hospital employees. AAOHN Journal, 54(2), 61–68.
Chapter I
36
Trépanier, S. G., Fernet, C., Austin, S., & Boudrias, V. (2016). Work environment antecedents of bullying: A
review and integrative model applied to registered nurses. International Journal of Nursing Studies, 55, 85-97.
Trysoe, L., Hounsgaard, L., Dohn, N. B., & Wagner, L. (2012). Newly qualified nurses–experiences of interaction
with members of a community of practice. Nurse Education Today, 32(5), 551–555.
Waschgler, K., Ruiz-Hernandez, J. A., Llor-Esteban, B., & Garcıa-Izquierdo, M. (2013). Patients’ aggressive
behaviors towards nurses: development and psychometric properties of the hospital aggressive behavior scale-
users. Journal of Advanced Nursing, 69(6), 1418–1427.
Wells, J., & Bowers, L. (2002). How prevalent is violence towards nurses working in general hospitals in the UK?
Journal of Advanced Nursing, 39(3), 230–240.
Wei, C. Y., Chiou, S. T., Chien, L. Y., & Huang, N. (2016). Workplace violence against nurses - Prevalence and
association with hospital organizational characteristics and health-promotion efforts: Cross-sectional study.
International Journal of Nursing Studies, 56, 63–70.
Whall, A. L., Colling, K. B., Kolanowski, A., Kim, H., Son Hong, G. R., DeCicco, B., Ronis, D. L., Richards, K. C.,
Algase, D., & Beck, C. (2008). Factors associated with aggressive behavior among nursing home residents with
dementia. Gerontologist, 48(6), 721-31.
Winstanley, S., & Whittington, R. (2004). Aggressive encounters between patients and general hospital staff: Staff
perceptions of the context and assailants’ levels of cognitive processing. Aggressive Behavior, 30(6), 534–543.
Wittouck, C., Audenaert, K. & Vander Laenen, F. (2015). Hoofdstuk 7: Omgaan met agressie en suïcidaal gedrag.
In Handboek forensische gedragswetenschappen. Antwewrpen: Maklu-Uitgevers nv.
Yarbrough, S., Martin, P., Alfred, D., & McNeill, C. (2016). Professional values, job satisfaction, career
development and intent to stay. Nursing Ethics. 1-11.
You, L. M., Aiken, L. H., Sloane, D. M., Liu, K., He, G. P., Hu, Y., Jiang, X. L., Li, X. H., Li X. M., Liu, H. P., Shang,
S. M., Kutney-Lee, A., & Sermeus, W. (2013). Hospital nursing, care quality and patient satisfaction: cross-
sectional surveys of nurses and patients in hospitals in China and Europe. International Journal of Nursing
Studies, 50(2), 154–161.
Zeller, A., Hahn, S., Needham, I., Kok, G., Dassen, T., & Halfens, R. J. G. (2009). Aggressive behavior of nursing
home residents toward caregivers: a systematic literature review. Geriatric Nursing, 30(3), 174–187.
Zillmann D. 1983. Arousal and aggression. In Green R.G. & Donnerstein E. (Eds.) Aggression: theoretical and
empirical reviews (vol. 1, pp 75-102). New York: Academia Press.
Assessment of aggression: validation of instruments
37
Chapter II.
ASSESSMENT OF AGGRESSION IN CARE
RELATIONSHIPS: VALIDATION OF THREE INSTRUMENTS
Tina Vandecasteele1.2, Ann Van Hecke1,3, Bart Debyser2, Tine Vanderplancke4,
Tine De Backer2, Dimitri Beeckman1, Sofie Verhaeghe1,2
1 Department of Public Health, Faculty of Medicine and Health Sciences, University Centre for Nursing &
Midwifery, Ghent University, Ghent, Belgium.
2 Department Health care, VIVES University College, Roeselare, Belgium.
3 University Hospital Ghent, Ghent, Belgium.
4 Department Health care, VIVES University College, Kortrijk, Belgium.
Based on a manuscript submitted to the Journal of Nursing Management

Chapter II
38

Assessment of aggression: instrument validation
39
Assessment of patients’ and family members’ aggression directed towards nurses
working in general hospital settings: Validation of three instruments
Abstract
Aim. To psychometrically test the Dutch version of the Survey of Violence Experienced by Staff
(SOVES), the shortened Perception of Aggression Scale (POAS-s) and the Perception of Importance of
Intervention Skills Scale (POIS) for use in general hospital wards.
Background. Experiencing aggression has an important impact on both the professional and personal
lives of nurses. Minimal research focuses on patient aggression in general hospital settings. The
SOVES, POAS-S and POIS are validated instruments to study multiple dimensions of patient violence
at the clinical level in a variety of general hospital settings.
Method. Psychometric properties (content- and construct validity, stability, and internal consistency)
were determined in a cross-sectional study including 238 nurses working in general hospital settings.
Results. The instruments showed good content validity and test-retest reliability. Significant
relationships between encountering patient aggression and patient contact time, patients’ ages, and
nurses’ degrees were observed, suggesting construct validity of the SOVES. Factor analysis of the
POAS-s and POIS identified two-factor structures, explaining 46.7% and 68.5% of the variance.
Cronbach’s alpha of the POAS-s was 0.64 and 0.70, alpha-value of the POIS was 0.88 and 0.84.
Conclusions. The instruments showed acceptable to good psychometric properties, and are
recommended to be used in practice to assess patient aggression in general hospitals.
Implications for nursing management. Nurse managers can use these instruments to assess patient
aggression in particular settings, to analyse factors contributing to patient aggression and consequently
design interventions to support nurses in managing patient aggression.
Keywords. Aggression, general hospital setting, instrument, nursing, psychometrics.
Chapter II
40
1. | Introduction
Patient aggression towards nurses occurs frequently (Spector, Zhou, & Che, 2014). Assessment
instruments are needed to provide specific information on frequencies and differences among places
and times of patient aggression. This article addresses the Dutch translation and psychometric testing
of three instruments to assess patients’ and/or family members’ aggression in general hospitals. Data
were obtained in preparation of a larger assessment of aggression using these instruments in general
hospital settings.
1.1. | Background
Aggression by patients towards healthcare workers is a complex and significant occupational hazard in
hospitals worldwide (Hahn et al., 2008; McPhaul, London, & Lipscomb, 2013). Compared to other
healthcare providers, nurses are at a higher risk of experiencing aggression (International Council of
Nurses, 2006; Arnetz et al., 2015). Substantial research on aggression towards nurses has been
conducted, focusing on prevalence (Camerino et al., 2008; Wei, Chiou, Chien, & Huang, 2016),
determinants (Adib et al., 2002; Hahn et al., 2013), risk factors (Gillespie, Gates, Miller, & Howard,
2010), and consequences (Wells & Bowers, 2002; Sofield & Salmond, 2003). Subsequently, several
factors have been identified to contribute to the occurrence of patients’ and family members’ aggression.
These factors account for particular patients’ and/or family members’ characteristics (Hahn et al., 2013),
staff characteristics (Duxbury, 2002; Jansen, Dassen, & Groot Jebbink, 2005), staff-patient and families
interactions (Winstanley & Whittington, 2004; Winstanley, 2005), and organizational characteristics
(Farrell, Bobrowski, & Bobrowski, 2006). With regard to the latter, some specific clinical areas seem to
be at a particular risk of patient and visitor aggression (Spector et al., 2014). Settings like emergency
departments (Gacki-Smith et al., 2009), geriatric care (Franz et al., 2010) and mental health (Foster,
Bowers, & Nijman, 2007) have been exposed to high frequencies of aggression. However, also general
inpatient settings, like medical and surgical wards, are increasingly regarded to be vulnerable for
aggressive incidents (Roche, Diers, Duffield, & Catling-Paull, 2010). Whilst a number of studies have
addressed aggression in the former specific healthcare settings, only a few have done so for nursing in
general hospital settings (Hahn et al., 2013; Heckemann et al., 2015).
Assessment of aggression: instrument validation
41
1.2. | Assessment of patients’ and family members’ aggression in general hospitals
As classifications, scales and standardized assessment instruments form an integral part of nursing
research and nursing practice (Streiner & Kottner, 2014), an instrument is required to study aggression
towards nurses objectively. A variety of instruments exists to assess aggression in healthcare. Examples
of validated instruments are the Staff Observation Aggression Scale (Palmstierna & Widstedt, 1987),
the Management of Aggression and Violence Attitude Scale (Duxbury, 2003), the Attitudes Toward
Physical Assault Questionnaire (Poster & Ryan, 1989), and the Overt Aggression Scale (Yudofsky et
al., 1986). However, current instruments reflect the aforementioned focus on specific clinical areas as
these instruments have primarily been validated in mental health settings (Nijman et al., 2002; Jansen
et al., 2005), emergency (Barzman et al., 2012), or geriatric settings (Ryser, Duxbury, & Hahn, 2015).
Validated instruments to assess patients’ and/or family members’ aggression in general hospital settings
are scarce. Accordingly, Hahn et al. (2011) formulated a conceptual model encompassing relevant
factors related to patients’ and/or family members’ aggression in general hospitals. Based on this model,
three instruments can been combined to provide a comprehensive representation of patients’ and/or
family members’ aggression in general hospital settings.
The Survey of Violence experienced by Staff (SOVES). The SOVES was originally developed by
McKenna (2004) to gather information on workplace aggression, and to acquire data on involved
healthcare staff, patients and the broader workplace environment. The SOVES explores five themes:
(1) prevalence of aggression, (2) consequences of aggression, (3) reporting of aggression, (4) support
after experiencing aggression, and (5) training in managing aggression; as each of these themes is
related to three manifestations of aggression: verbal aggression, threats and physical aggression.
‘Verbal aggression’ is understood as abusive or offensive language, personally derogatory remarks,
profanity or obscene comments. ‘Threats’ are explained as warnings of intent to injure, harassment,
physical intimidation or threat with a weapon. ‘Physical aggression’ comprises slapping, pinching,
pushing, shoving, spitting, kicking or the use of a weapon. The SOVES provides a comprehensive
representation of aggression as several variables (nurses’ characteristics, patients’ characteristics,
nurses’ experiences of different types of aggression, practice characteristics and broader organizational
characteristics) are assessed. Close-ended questions and Visual Analogue Scales (VAS) are used to
assess these variables. Content validity and internal consistency have been assessed by McKenna
(2004), while feasibility and face validity of the German version of the SOVES have been appraised by
Chapter II
42
Hahn et al. (2011), showing good psychometric properties. The SOVES provides important information
on aggressive incidents in nursing practice. However, literature has emphasized attitude towards patient
aggression to be influential towards intervention strategies in handling patient aggression (Duxbury,
2002). Nurses’ beliefs about causation of aggression influence their approach to manage incidents
(Duxbury, Hahn, Needham, & Pulsford, 2008). As this influential and mediating factor is not included in
the SOVES, both the POAS-s and POIS are important to add to gain a more accurate representation of
aggression in nursing practice.
The shortened Perception of Aggression Scale (POAS-s). The POAS, originally developed by
Jansen et al. (1997), consisted of 30 Likert-scaled statements which express various views regarding
aggression. In 2004, Needham and colleagues derived a shortened version, the POAS-s, consisting of
12 items on a 5-point Likert scale, encompassing two dimensions in perceiving aggression: aggression
as a more dysfunctional/undesirable phenomenon (dimension 1) or as a more
functional/comprehensible phenomenon (dimension 2). Validation of the POAS-s has been assessed
through construct validity (Abderhalden et al., 2002), test-retest reliability, internal consistency
(Needham et al., 2004; Hahn et al., 2011), and content validity (Hahn et al., 2011), providing satisfactory
psychometric properties.
The Perception of Importance of Intervention Skills Scale (POIS). The POIS was developed by
Hahn et al. (2011) to measure perceptions of the importance of intervention skills in managing patient
aggression in a general hospital setting. The instrument consists of nine items reflecting common
prevention and intervention strategies (e.g. verbal communications, setting limits, intervening as a
team), measured on a 10-point VAS-scale. In 2011, a psychometric evaluation was conducted in
assessing internal consistency and construct validity in general hospital settings (Hahn et al., 2011),
emphasizing two dimensions in perceptions about aggression management: structured interventions,
evaluation and reflection to manage aggression (dimension 1), and preventive measures to manage
aggression (dimension 2).
As a combination of these three instruments provide access to relevant factors in assessing patients’
and family members’ aggression in general hospital settings, this study aims to translate and validate
these instruments in general hospital settings.
Assessment of aggression: instrument validation
43
2. | The study
2.1. | Aims
This study aims
to translate the SOVES, POAS-s and POIS and adapt it for use in a general hospital setting and
to assess psychometric properties of the translated version in general hospital settings.
2.2. | Methods
2.2.1. Phase I: Translation and adaption of the SOVES, POAS-s and POIS
Three certified translators, with medical-language translation experience, individually translated the
instruments from German to Dutch. Translations were compared and discussed by the translators,
analysing different proposals until reaching consensus. As a control measure of the translation of the
SOVES and the POAS-S, the English validated version of the SOVES and POAS-S was translated by
a translator with a Master’s degree in Linguistics and Literature, Dutch-English. The researcher expert
panel (TV-AVH-SV) and two Masters of Nursing Science students thoroughly reviewed every item while
comparing translations to the original instruments. Difficulties in translating and discrepancies were
discussed with the translators.
Face and content validity of the instruments was assessed by a panel of seven experts (stage 1). Five
had extensive experience in nursing practice in general hospital settings, four were researchers in the
field of aggression in the healthcare system, and two were very familiar with the theoretical basis of
aggression in care relationships. These experts assessed the content, clarity, feasibility and
comprehensibility of the instruments, the technical and semantic equivalence of the translations, and
discussed the cross-cultural relevance of questions ensuring its relevance to the nursing practice and
healthcare context in Belgium. Subtle differences in the conceptual meaning of words were assessed
and discussed.
The semi-final version of the instruments was then pilot-tested for clarity, feasibility and user-friendliness
in a sample of 13 practicing nurses (stage 2). By being cognitively interviewed, nurses elaborated on
how they interpreted and answered the questions of the questionnaire. They judged the construct and
content of the questions for relevance in their nursing practice or clinical setting. Finally, the researcher
expert panel (stage 3) thoroughly discussed all the proposed changes to the instruments.
2.2.2. Phase II: Psychometric properties of the Dutch version of the SOVES, POAS-s and POIS
Design. A cross-sectional validation study was conducted.
Data collection. Ten general medical and surgical wards in two general hospitals and one teaching
hospital were invited to participate. Data were collected from September 2014 to September 2015. The
researcher explained the study to the head of departments and the head nurses. Each head nurse was
consulted to make practical arrangements to distribute the instruments. Nurses were invited to take part,
Chapter II
44
and were informed through a presentation during team meetings. The instruments had to be completed
within six weeks. To ensure anonymity, instruments were returned in secured boxes at the wards. Every
two weeks, a researcher collected the instruments and provided reminders.
To assess test-retest reliability of the instruments, nursing students, obtaining their Master’s degree
(n=34) and licensed practice students obtaining their Bachelor’s degree (n=47) with both experience in
nursing practice were invited to participate. The interval between the test and retest was four to five
hours.
Ethical considerations. Nurses were informed participation was voluntary and responses were treated
anonymous. The study was approved by the Ethical Committee of the Ghent University Hospital
(B/670201421265) and the local Ethical Committees of the hospitals.
Statistical analysis. Descriptive statistics were used to describe nurses’ demographic and professional
characteristics. Negatively worded items of the POAS-s and POIS were reversed before analysis.
Construct validity of the SOVES was assessed by the known-groups technique (Polit & Beck, 2017).
Literature suggests different groups can be expected to differ on the frequency of experiencing
aggression (table 1). Although the SOVES encompasses several major themes, only the frequency of
encountering aggression was chosen to provide an indication of construct validity. Chi-square tests were
used to compare group scores because of the dichotomous character of having encountered aggression
within the past year. Construct validity of the POAS-s and POIS was assessed by an exploratory factor
analysis using principal component analysis (Polit & Beck, 2017). The varimax rotation with Kaiser
normalisation was used. The Kaiser-Meyer-Olkin (KMO) Measure of Sampling Adequacy over 0.50,
Bartlett’s test of sphericity and scree plots were evaluated. A requirement of at least 10 participants per
variable of the POAS-s and POIS was intended (Norman & Streiner, 2014). Internal consistency of the
POAS-s and POIS was studied by calculating inter-item correlations Cronbach’s alpha (Polit & Beck,
2017). Cronbach’s alphas were interpreted as described by Streiner and Norman (2003): 0.70 <
Cronbach’s α < 0.90. To assess stability reliability, intraclass correlation coefficients were calculated for
each item of the POAS-s and POIS (Shrout & Fleiss, 1979). Due to the stable nature of the items of the
SOVES, a reliability assessment did not seem appropriate. Reliability coefficients ≥0.70 were considered
as satisfactory (Polit & Beck, 2017). All statistical analyses were performed using SPSS version 22.0
(SPSS Inc., Chicago, IL, USA)
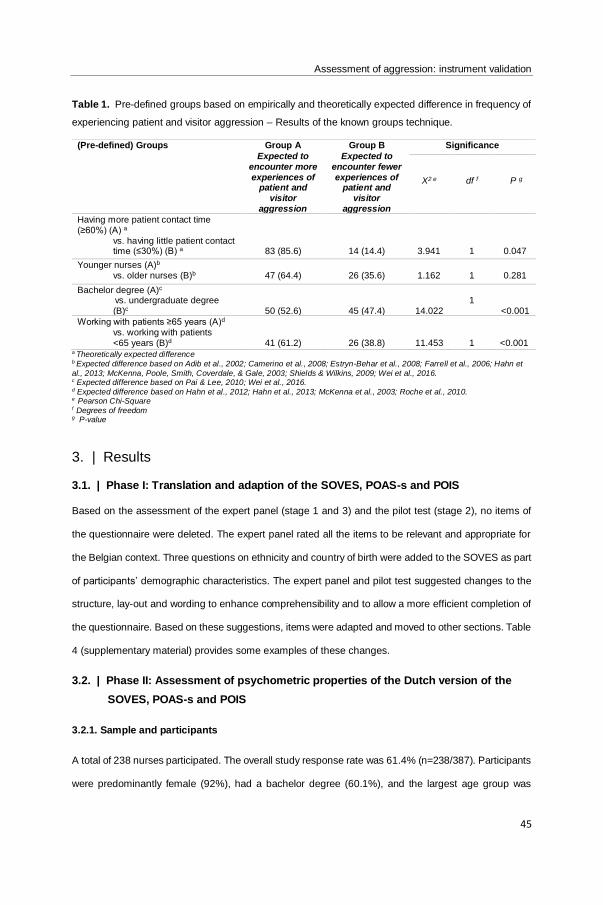
Assessment of aggression: instrument validation
45
Table 1. Pre-defined groups based on empirically and theoretically expected difference in frequency of
experiencing patient and visitor aggression – Results of the known groups technique.
(Pre-defined) Groups Group A
Expected to encounter more experiences of
patient and visitor
aggression
Group B
Expected to encounter fewer experiences of
patient and visitor
aggression
Significance
X2 e
df f
P g
Having more patient contact time (≥60%) (A) a
vs. having little patient contact time (≤30%) (B) a
83 (85.6)
14 (14.4)
3.941
1
0.047
Younger nurses (A)b vs. older nurses (B)b
47 (64.4)
26 (35.6)
1.162
1
0.281
Bachelor degree (A)c vs. undergraduate degree (B)c
50 (52.6)
45 (47.4)
14.022
1
<0.001
Working with patients ≥65 years (A)d vs. working with patients <65 years (B)d
41 (61.2)
26 (38.8)
11.453
1
<0.001 a Theoretically expected difference b Expected difference based on Adib et al., 2002; Camerino et al., 2008; Estryn-Behar et al., 2008; Farrell et al., 2006; Hahn et
al., 2013; McKenna, Poole, Smith, Coverdale, & Gale, 2003; Shields & Wilkins, 2009; Wei et al., 2016. c Expected difference based on Pai & Lee, 2010; Wei et al., 2016. d Expected difference based on Hahn et al., 2012; Hahn et al., 2013; McKenna et al., 2003; Roche et al., 2010. e Pearson Chi-Square f Degrees of freedom g P-value
3. | Results
3.1. | Phase I: Translation and adaption of the SOVES, POAS-s and POIS
Based on the assessment of the expert panel (stage 1 and 3) and the pilot test (stage 2), no items of
the questionnaire were deleted. The expert panel rated all the items to be relevant and appropriate for
the Belgian context. Three questions on ethnicity and country of birth were added to the SOVES as part
of participants’ demographic characteristics. The expert panel and pilot test suggested changes to the
structure, lay-out and wording to enhance comprehensibility and to allow a more efficient completion of
the questionnaire. Based on these suggestions, items were adapted and moved to other sections. Table
4 (supplementary material) provides some examples of these changes.
3.2. | Phase II: Assessment of psychometric properties of the Dutch version of the
SOVES, POAS-s and POIS
3.2.1. Sample and participants
A total of 238 nurses participated. The overall study response rate was 61.4% (n=238/387). Participants
were predominantly female (92%), had a bachelor degree (60.1%), and the largest age group was
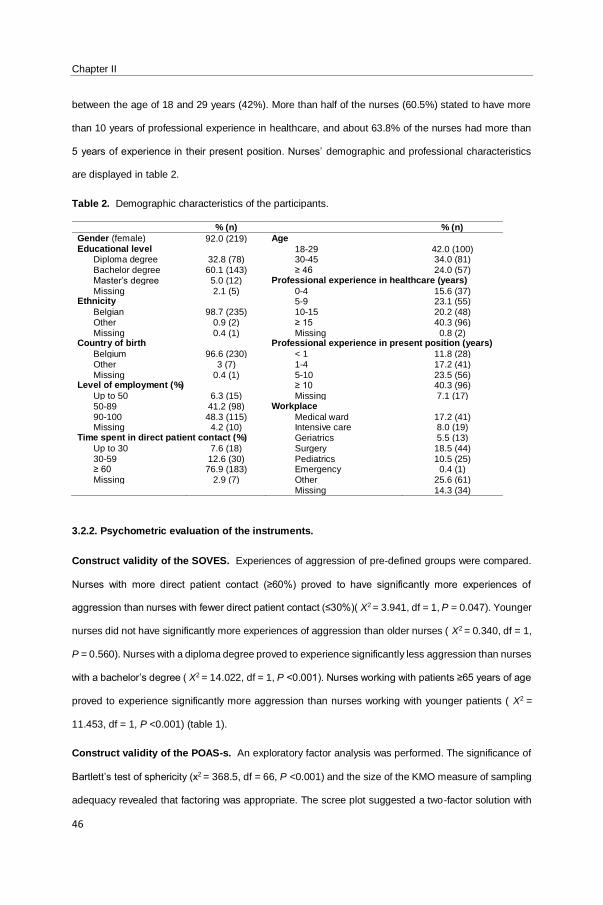
Chapter II
46
between the age of 18 and 29 years (42%). More than half of the nurses (60.5%) stated to have more
than 10 years of professional experience in healthcare, and about 63.8% of the nurses had more than
5 years of experience in their present position. Nurses’ demographic and professional characteristics
are displayed in table 2.
Table 2. Demographic characteristics of the participants.
% (n) % (n)
Gender (female) 92.0 (219) Age Educational level 18-29 42.0 (100)
Diploma degree 32.8 (78) 30-45 34.0 (81) Bachelor degree 60.1 (143) ≥ 46 24.0 (57) Master’s degree 5.0 (12) Professional experience in healthcare (years)
Missing 2.1 (5) 0-4 15.6 (37) Ethnicity 5-9 23.1 (55)
Belgian 98.7 (235) 10-15 20.2 (48) Other 0.9 (2) ≥ 15 40.3 (96) Missing 0.4 (1) Missing 0.8 (2)
Country of birth Professional experience in present position (years)
Belgium 96.6 (230) < 1 11.8 (28) Other 3 (7) 1-4 17.2 (41) Missing 0.4 (1) 5-10 23.5 (56)
Level of employment (%) ≥ 10 40.3 (96) Up to 50 6.3 (15) Missing 7.1 (17) 50-89 41.2 (98) Workplace 90-100 48.3 (115) Medical ward 17.2 (41) Missing 4.2 (10) Intensive care 8.0 (19)
Time spent in direct patient contact (%) Geriatrics 5.5 (13) Up to 30 7.6 (18) Surgery 18.5 (44) 30-59 12.6 (30) Pediatrics 10.5 (25) ≥ 60 76.9 (183) Emergency 0.4 (1) Missing 2.9 (7) Other 25.6 (61)
Missing 14.3 (34)
3.2.2. Psychometric evaluation of the instruments.
Construct validity of the SOVES. Experiences of aggression of pre-defined groups were compared.
Nurses with more direct patient contact (≥60%) proved to have significantly more experiences of
aggression than nurses with fewer direct patient contact (≤30%)( X2 = 3.941, df = 1, P = 0.047). Younger
nurses did not have significantly more experiences of aggression than older nurses ( X2 = 0.340, df = 1,
P = 0.560). Nurses with a diploma degree proved to experience significantly less aggression than nurses
with a bachelor’s degree ( X2 = 14.022, df = 1, P <0.001). Nurses working with patients ≥65 years of age
proved to experience significantly more aggression than nurses working with younger patients ( X2 =
11.453, df = 1, P <0.001) (table 1).
Construct validity of the POAS-s. An exploratory factor analysis was performed. The significance of
Bartlett’s test of sphericity (x2 = 368.5, df = 66, P <0.001) and the size of the KMO measure of sampling
adequacy revealed that factoring was appropriate. The scree plot suggested a two-factor solution with
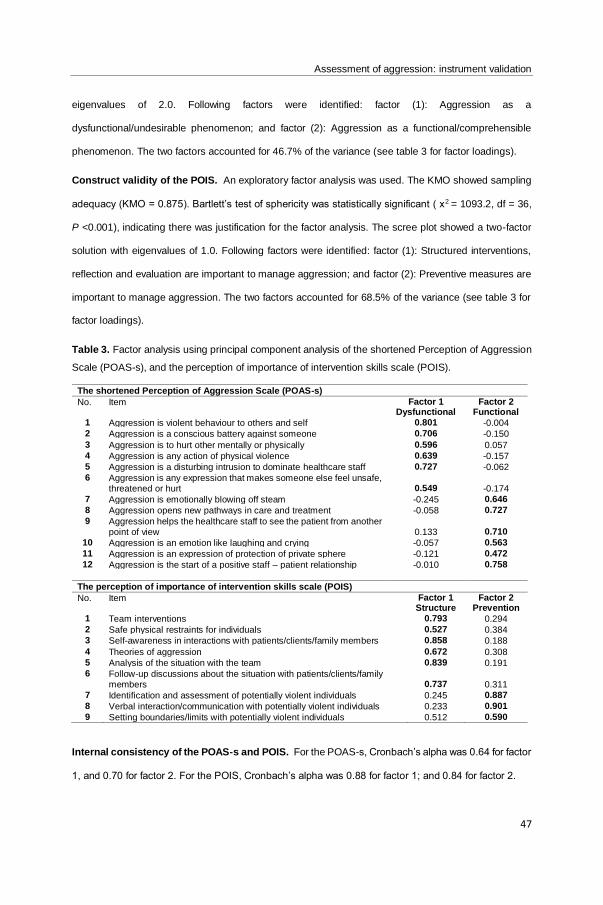
Assessment of aggression: instrument validation
47
eigenvalues of 2.0. Following factors were identified: factor (1): Aggression as a
dysfunctional/undesirable phenomenon; and factor (2): Aggression as a functional/comprehensible
phenomenon. The two factors accounted for 46.7% of the variance (see table 3 for factor loadings).
Construct validity of the POIS. An exploratory factor analysis was used. The KMO showed sampling
adequacy (KMO = 0.875). Bartlett’s test of sphericity was statistically significant ( x2 = 1093.2, df = 36,
P <0.001), indicating there was justification for the factor analysis. The scree plot showed a two-factor
solution with eigenvalues of 1.0. Following factors were identified: factor (1): Structured interventions,
reflection and evaluation are important to manage aggression; and factor (2): Preventive measures are
important to manage aggression. The two factors accounted for 68.5% of the variance (see table 3 for
factor loadings).
Table 3. Factor analysis using principal component analysis of the shortened Perception of Aggression
Scale (POAS-s), and the perception of importance of intervention skills scale (POIS).
The shortened Perception of Aggression Scale (POAS-s)
No. Item Factor 1 Dysfunctional
Factor 2 Functional
1 Aggression is violent behaviour to others and self 0.801 -0.004 2 Aggression is a conscious battery against someone 0.706 -0.150
3 Aggression is to hurt other mentally or physically 0.596 0.057 4 Aggression is any action of physical violence 0.639 -0.157 5 Aggression is a disturbing intrusion to dominate healthcare staff 0.727 -0.062 6 Aggression is any expression that makes someone else feel unsafe,
threatened or hurt
0.549
-0.174
7 Aggression is emotionally blowing off steam -0.245 0.646
8 Aggression opens new pathways in care and treatment -0.058 0.727
9 Aggression helps the healthcare staff to see the patient from another point of view
0.133
0.710
10 Aggression is an emotion like laughing and crying -0.057 0.563
11 Aggression is an expression of protection of private sphere -0.121 0.472
12 Aggression is the start of a positive staff – patient relationship -0.010 0.758
The perception of importance of intervention skills scale (POIS)
No. Item Factor 1 Structure
Factor 2 Prevention
1 Team interventions 0.793 0.294 2 Safe physical restraints for individuals 0.527 0.384 3 Self-awareness in interactions with patients/clients/family members 0.858 0.188
4 Theories of aggression 0.672 0.308 5 Analysis of the situation with the team 0.839 0.191 6 Follow-up discussions about the situation with patients/clients/family
members
0.737
0.311
7 Identification and assessment of potentially violent individuals 0.245 0.887
8 Verbal interaction/communication with potentially violent individuals 0.233 0.901
9 Setting boundaries/limits with potentially violent individuals 0.512 0.590
Internal consistency of the POAS-s and POIS. For the POAS-s, Cronbach’s alpha was 0.64 for factor
1, and 0.70 for factor 2. For the POIS, Cronbach’s alpha was 0.88 for factor 1; and 0.84 for factor 2.
Chapter II
48
Stability reliability of the POAS-s and POIS. A total of 81 nursing students completed the instruments
twice. The intraclass correlation coefficient for the POAS-s ranged between 0.71 (95% CI = 0.53–0.82,
P <0.001) and 0.88 (95% CI = 0.80–0.93, P <0.001). The intraclass correlation coefficient for the POIS
ranged between 0.81 (95% CI = 0.69–0.88, P <0.001) and 0.93 (95% CI = 0.89–0.96, P <0.001).
4. | Discussion
An accurate assessment of patients’ and/or family members’ aggression in general hospital settings is
an important step in developing and implementing strategies to prevent and manage patients’ and/or
family members’ aggression. The purpose of this study was to translate and evaluate psychometric
properties of three assessment instruments regarding aggression for use in general hospital settings.
These instruments are the Survey of Violence Experienced by Staff (SOVES); the shortened Perception
of Aggression Scale (POAS-s) and the Perception of Importance of Intervention Skills Scale (POIS).
The findings support the validity and reliability of the Dutch version of the three instruments.
Construct validity of the SOVES was assessed by the known-group technique. Different groups of
nurses that were empirically and theoretically expected to encounter more or fewer experiences of
aggression were compared. As expected, nurses who worked with patients over 65 years, nurses who
had more patient contact time ( ≥60%), and nurses with a bachelor’s degree seemed to have significantly
more experiences of patient aggression within the past year in comparison to nurses working with
younger patients, nurses having little patient contact time ( ≤30%), or nurses having a diploma degree.
However, younger nurses did not seem to have significantly more experiences of patient aggression
than older nurses. This finding might partially be explained by the lack of sensitivity in the categorical
group comparison, nurses under the age of 30 were compared to nurses over the age of 46 years.
Nurses’ ages were not assessed as a continuous variable. And as there were only three categories
regarding nurses’ ages ( <30, 30-45, and >46), this division might be too broad to render a significant
difference.
Construct validity of the POAS-s and POIS were assessed in factor analyses. Conform previous studies
(Abderhalden et al., 2002; Needham et al., 2004; Hahn et al., 2011), the data confirmed two-factor
structures in both the POAS-s and POIS. Both two-factor solutions explained 47% and 69% of the
variance respectively. Subsequently, internal consistency in the construct of the POAS-s with a
Cronbach’s alpha of 0.64 for factor 1 (‘aggression perceived as a dysfunctional/undesirable
Assessment of aggression: instrument validation
49
phenomena’) and 0.70 for factor 2 (‘aggression perceived as a functional/comprehensible phenomena’)
appeared to be rather moderate to acceptable. These alpha-values are comparable to those obtained
in other studies (Needham et al., 2004; Hahn et al., 2011). The moderate explained variance and internal
consistency might be ascribed to the complexity of the construct the items of the POAS-s are measuring.
Perceptions of aggression constitute a multidimensional construct. And perceptions are related to the
extent of exposure to aggression experienced, the causes and types of aggression, the perpetrators,
the management of aggression and the severity of injuries sustained (Jansen et al., 2005). This
complexity of the construct of perceptions suggests a multidimensionality of perceiving aggression which
challenges assessment of internal consistency. A comprehensive understanding of perceptions of
aggression might be acquired by integrating the dimensions Jansen et al. (2005) envisioned in the
Attitude of Aggression Scale. This instrument constitutes five dimensions rather than the two-
dimensional POAS-s, and is validated in mental health nurses (Jansen et al., 2005). Further research
could transfer and adapt these dimensions for use in general hospital settings.
Internal consistency in the construct of the POIS was found to be relatively high. A Cronbach’s alpha of
0.88 was found for factor 1 (perceiving structured interventions, reflection and evaluation as important
in managing aggression) and an alpha-value of 0.84 for factor 2 (perceiving preventive measures as
important in managing aggression). These values and the explained variance are higher than the ones
found in the original development and validation study of the POIS (Hahn et al., 2011). Consequently,
the POIS can be considered to be a promising instrument to acquire nurses’ perceptions on the
importance of intervention skills in managing aggression in general hospital settings. Insight into nurses’
perceptions about which skills they address in managing aggression can inspire intervention strategies
to support nurses in managing aggression.
The psychometric assessment supported the test-retest reliability of the instruments as the intraclass
correlations of the POAS-s and POIS reached the established recommendations. However, these
results have to be interpreted with caution because of the short interval between the two administrations.
Besides this limitation, the study was subject to other limitations. The sample comprised 238 nurses,
which can be considered to be rather limited. As the study focused on the psychometric properties of
instruments, and KMO measures in preparation of factor analyses indicated sampling adequacy, this
limited sample proved sufficient. Moreover, ten respondents per item is commonly recommended as a
minimum to support factor analysis (Polit & Beck, 2017).
Chapter II
50
Another limitation pertains the assessment of content validity. As no systematic quantification was
produced, this might be considered to be a limitation. However, various discussions on relevance,
meaning and appropriateness of the content of the instruments were conducted by a diverse researcher
expert panel in the field of aggression in healthcare systems. In these continued discussions, the
consistency of the content of the instruments with literature (f.e. Hahn et al., 2013) was taken into
consideration. This researcher expert panel thoroughly reviewed the translation process. This measure
was taken instead of performing back-translations. In discussing translations and considering technical
and semantic equivalence, and cultural relevance of questions, a good method of cross-cultural
translation and adaption of the instruments was sought (Squires et al., 2013). As no gold standard for
translation techniques exists (Cha, Kim, & Erlen, 2007), the method used in this study can be considered
as valuable because of the agreement that was reached among the expert panel, and the sound
adaptions and rather modest changes that were administered to the instruments. Finally, as validation
of instruments is considered to be a continuous process, further research should obtain a larger sample,
and procure a multidimensional assessment of perceptions of aggression.
4.1. | Implications for nursing management
Patient aggression is a problem for nurses. Consequently, this topic is on the agenda of many hospitals
in many countries. Because of the risk that nurses face, there is an interest to understand the
consequences of experiencing aggression. A number of consequences have been linked to aggression
in healthcare, pointing out how the occurrence of aggression causes harm to individual nurses, quality
of patientcare, and organisations as a whole. Individual nurses are placed at an increased risk of injury,
low morale, sleep disturbances, loss of self-confidence, etc. that compromise the physical and
psychological well-being of nurses (Gerberich et al., 2004; Roche et al., 2010). These consequences
affect caregiving for future patients as research points out how nurses experience a loss of empathy
towards patients, increase avoidance with fewer contacts with patients or adopt passive roles (Needham
et al., 2005). Moreover, patient aggression is associated with falls, medication errors and late
administration of medication, which signifies a striking impact of experiencing patient aggression on the
quality of patientcare (Roche et al., 2010). On an organizational level, organisations are faced with
reduced job motivation (Needham et al. 2005), and increased absenteeism (Foster et al., 2007), and
staff turnover rates (Luckhoff et al., 2013). These consequences are all detrimental especially in current
times of nursing shortage (Estryn-Behar et al., 2008). Gaining an accurate and validated measure of

Assessment of aggression: instrument validation
51
patients’ aggression and/or family members’ aggression allows tailoring of interventions to prevent, and
manage aggression issues in general hospital settings.
5. | Conclusion
An objective measure to study aggression in nursing practice is important. The Survey of Violence
Experienced by Staff, the shortened Perception of Aggression Scale and the Perception of Importance
of Intervention Skills Scale showed acceptable to good psychometric properties. The combination of
these assessment instruments can provide and advance knowledge on manifestations of patients’
and/or family members’ aggression on general hospital wards. This kind of representation can inform
intervention strategies in managing aggression that take into consideration the needs of the specific
setting, the involved patients and the professional caregivers.
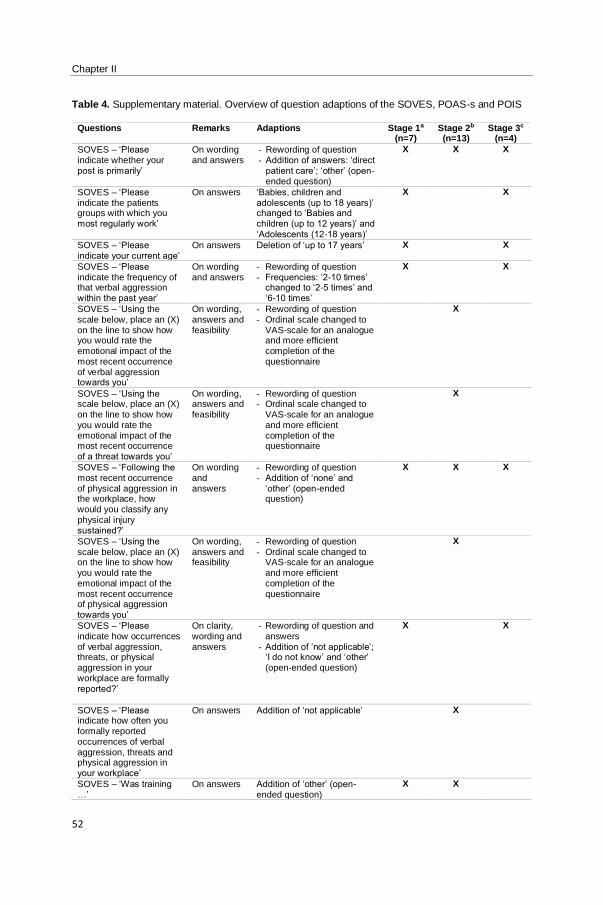
Chapter II
52
Table 4. Supplementary material. Overview of question adaptions of the SOVES, POAS-s and POIS
Questions Remarks Adaptions Stage 1a (n=7)
Stage 2b (n=13)
Stage 3c (n=4)
SOVES – ‘Please indicate whether your post is primarily’
On wording and answers
- Rewording of question - Addition of answers: ‘direct
patient care’; ‘other’ (open-ended question)
X X X
SOVES – ‘Please indicate the patients groups with which you most regularly work’
On answers ‘Babies, children and adolescents (up to 18 years)’ changed to ‘Babies and children (up to 12 years)’ and ‘Adolescents (12-18 years)’
X X
SOVES – ‘Please indicate your current age’
On answers Deletion of ‘up to 17 years’ X X
SOVES – ‘Please indicate the frequency of that verbal aggression within the past year’
On wording and answers
- Rewording of question - Frequencies: ‘2-10 times’
changed to ‘2-5 times’ and ‘6-10 times’
X X
SOVES – ‘Using the scale below, place an (X) on the line to show how you would rate the emotional impact of the most recent occurrence of verbal aggression towards you’
On wording, answers and feasibility
- Rewording of question - Ordinal scale changed to
VAS-scale for an analogue and more efficient completion of the questionnaire
X
SOVES – ‘Using the scale below, place an (X) on the line to show how you would rate the emotional impact of the most recent occurrence of a threat towards you’
On wording, answers and feasibility
- Rewording of question - Ordinal scale changed to
VAS-scale for an analogue and more efficient completion of the questionnaire
X
SOVES – ‘Following the most recent occurrence of physical aggression in the workplace, how would you classify any physical injury sustained?’
On wording and answers
- Rewording of question - Addition of ‘none’ and
‘other’ (open-ended question)
X X X
SOVES – ‘Using the scale below, place an (X) on the line to show how you would rate the emotional impact of the most recent occurrence of physical aggression towards you’
On wording, answers and feasibility
- Rewording of question - Ordinal scale changed to
VAS-scale for an analogue and more efficient completion of the questionnaire
X
SOVES – ‘Please indicate how occurrences of verbal aggression, threats, or physical aggression in your workplace are formally reported?’
On clarity, wording and answers
- Rewording of question and answers
- Addition of ‘not applicable’; ‘I do not know’ and ‘other’ (open-ended question)
X X
SOVES – ‘Please indicate how often you formally reported occurrences of verbal aggression, threats and physical aggression in your workplace’
On answers Addition of ‘not applicable’ X
SOVES – ‘Was training …’
On answers Addition of ‘other’ (open-ended question)
X X
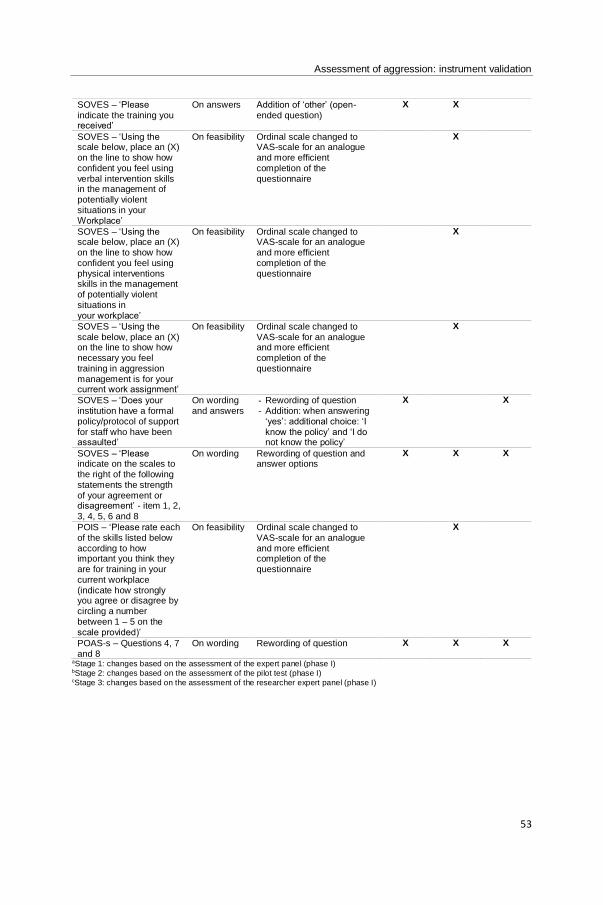
Assessment of aggression: instrument validation
53
SOVES – ‘Please indicate the training you received’
On answers Addition of ‘other’ (open-ended question)
X X
SOVES – ‘Using the scale below, place an (X) on the line to show how confident you feel using verbal intervention skills in the management of potentially violent situations in your Workplace’
On feasibility Ordinal scale changed to VAS-scale for an analogue and more efficient completion of the questionnaire
X
SOVES – ‘Using the scale below, place an (X) on the line to show how confident you feel using physical interventions skills in the management of potentially violent situations in your workplace’
On feasibility Ordinal scale changed to VAS-scale for an analogue and more efficient completion of the questionnaire
X
SOVES – ‘Using the scale below, place an (X) on the line to show how necessary you feel training in aggression management is for your current work assignment’
On feasibility Ordinal scale changed to VAS-scale for an analogue and more efficient completion of the questionnaire
X
SOVES – ‘Does your institution have a formal policy/protocol of support for staff who have been assaulted’
On wording and answers
- Rewording of question - Addition: when answering
‘yes’: additional choice: ‘I know the policy’ and ‘I do not know the policy’
X X
SOVES – ‘Please indicate on the scales to the right of the following statements the strength of your agreement or disagreement’ - item 1, 2, 3, 4, 5, 6 and 8
On wording Rewording of question and answer options
X X X
POIS – ‘Please rate each of the skills listed below according to how important you think they are for training in your current workplace (indicate how strongly you agree or disagree by circling a number between 1 – 5 on the scale provided)’
On feasibility Ordinal scale changed to VAS-scale for an analogue and more efficient completion of the questionnaire
X
POAS-s – Questions 4, 7 and 8
On wording Rewording of question X X X
aStage 1: changes based on the assessment of the expert panel (phase I) bStage 2: changes based on the assessment of the pilot test (phase I) cStage 3: changes based on the assessment of the researcher expert panel (phase I)
Chapter II
54
REFERENCES
Abderhalden, C., Needham, I., Friedli, T. K., Poelmans, J., & Dassen, T. (2002). Perception of aggression among
psychiatric nurses in Switzerland. Acta Psychiatrica Scandinavica, 412, 110-7.
Adib, S.M., Al-Shatti, A.K., Kamal, S., El-Gerges, N., & Al-Raqem, M. (2002). Violence against nurses in healthcare
facilities in Kuwait. International Journal of Nursing Studies, 39(4), 469-478.
Arnetz, J.E., Hamblin, L., Essenmacher, L., Upfal, M.J., Ager, J., & Luborsky, M. (2015). Understanding patient-to-
worker violence in hospitals: a qualitative analysis of documented incident reports. Journal of Advanced Nursing,
71(2), 338–348.
Barzman, D., Mossman, D., Sonnier, L., & Sorter, M. (2012). Brief Rating of Aggression by Children and
Adolescents (BRACHA): a reliability study. The journal of the American Academy of Psychiatry and the Law, 40(3),
374-82.
Camerino, D., Estryn-Behar, M., Conway, P. M., van Der Heijden, B. I., & Hasselhorn, H. M. (2008). Work-related
factors and violence among nursing staff in the European NEXT study: a longitudinal cohort study. International
Journal of Nursing Studies, 45(1), 35–50.
Cha, E.S., Kim, K.H., & Erlen, J.A. (2007). Translation of scales in cross-cultural research: issues and techniques.
Journal of Advanced Nursing, 58(4), 386-95.
Duxbury, J. (2002). An evaluation of staff and patient views of and strategies employed to manage inpatient
aggression and violence on one mental health unit: A pluralistic design. Journal of Psychiatric and Mental Health
Nursing, 9(3), 325–337.
Duxbury, J. (2003). Testing a new tool: the Management of Aggression and Violence Attitude Scale (MAVAS).
Nurse Researcher, 10(4), 39-52.
Duxbury, J., Hahn, S., Needham, I., & Pulsford, D. (2008). The Management of Aggression and Violence Attitude
Scale (MAVAS): a cross-national comparative study. Journal of Advanced Nursing, 62(5), 596-606.
Estryn-Behar, M., van der Heijden, B., Camerino, D., Fry, C., Le Nezet, O., Conway, P.M., Hasselhorn, H.M., &
NEXT Study Group (2008). Violence risks in nursing-results from the European 'NEXT' Study. Occupational
medicine, 58(2) 107-14.
Farrell, G.A., Bobrowski, C., & Bobrowski, P. (2006). Scoping workplace aggression in nursing: findings from an
Australian study. Journal of Advanced Nursing, 55(6), 778-87.
Franz, S., Zeh, A., Schablon, A., Kuhnert, S., & Nienhaus, A. (2010). Aggression and violence against healthcare
workers in Germany: a cross sectional retrospective survey. BMC Health services research 10(51).
Foster, C., Bowers, L., & Nijman, H. (2007). Aggressive behaviour on acute psychiatric wards: prevalence, severity
and management. Journal of Advanced Nursing, 58(2), 140-9.
Assessment of aggression: instrument validation
55
Gacki-Smith, J., Juarez, A.M., Boyett, L., Homeyer, C., Robinson, L., & MacLean, S.L. (2009). Violence against
nurses working in US emergency departments. Journal of nursing administration, 39(7-8), 340-9.
Gerberich, S.G., Church, T.R., McGovern, P.M., Hansen, H.E., Nachreiner, N.M., Geisser, M.S., Ryan, A.D.,
Mongin, S.J., & Watt, G.D. (2004). An epidemiological study of the magnitude and consequences of work related
violence: the Minnesota Nurses' Study. Occupational and environmental medicine, 61(6), 495-503.
Gillespie, G.L., Gates, D.M., Miller, M., & Howard, P.K. (2010). Workplace violence in healthcare settings: risk
factors and protective strategies. Rehabilitation Nursing, 35(5), 177–184.
Hahn, S., Zeller, A., Needham, I., Kok, G., Dassen, T., & Halfens, R. J. G. (2008). Patient and visitor violence in
general hospitals: a systematic review of the literature. Aggression and Violent Behavior, 13, 431–441.
Hahn, S., Müller, M., Needham, I., Dassen, T., Kok, G., & Halfens, T.J. (2011). Measuring patient and visitor
violence in general hospitals: feasibility of the SOVES-G-R, internal consistency and construct validity of the POAS-
S and the POIS. Journal of Clinical Nursing, 20(17-18), 2519-30.
Hahn, S., Müller, M., Hantikainen, V., Kok, G., Dassen, T., & Halfens, R.J.G. (2013). Risk factors associated with
patient and visitor violence in general hospitals: results of a multiple regression analysis. International Journal of
Nursing Studies 50(3), 374-85.
Heckemann, B., Zeller, A., Hahn, S., Dassen, T., Scholas, J.M., & Halfens, R.J. (2015). The effect of aggression
management training programmes for nursing staff and students working in an acute hospital setting. A narrative
review of current literature. Nurse Education Today, 35(1), 212-9.
International Council of Nurses, 2006. United Against Violence. International Council of Nurses, Geneva,
Switzerland.
Jansen, G., Dassen, T., & Moorer, P. (1997). The perception of aggression. Scandinavian journal of caring sciences,
11(1), 51-5.
Jansen, G.J., Dassen, T.W. & Groot Jebbink, G. (2005). Staff attitudes towards aggression in healthcare: a review
of the literature. Journal of Psychiatric and Mental Health Nursing, 12(1), 3-13.
Luckhoff, M., Jordaan, E., Swart, Y., Cloete, K. J., Koen, L., & Niehaus, D. J. (2013). Retrospective review of trends
in assaults and seclusion at an acute psychiatric ward over a 5-year period. Journal of Psychiatric and Mental Health
Nursing, 20(8), 687-95.
McKenna, B.G., Poole, S.J., Smith, N.A., Coverdale, J.H., & Gale, C.K. (2003). A survey of threats and violent
behaviour by patients against registered nurses in their first year of practice. International Journal of Mental Health
Nursing, 12(1), 56-63.
McKenna, K. (2004). Study of Work-Related Violence. Committee on Workplace Violence, North Eastern Health
Board, Ireland, pp. 1–121.
Chapter II
56
McPhaul, K.M., London, M., & Lipscomb, J.A. (2013). A framework for translating workplace violence intervention
research into evidence-based programs. The Online Journal of Issues in Nursing, 18(1).
Nijman, H. L. I. (2002). A model of aggression in psychiatric hospitals. Acta Psychiatrica Scandinavica, 106, 142–
143.
Needham, I., Abderhalden, C., Dassen, T., Haug, H.J., & Fischer, J.E. (2004). The perception ofaggression by
nurses: psychometric scale testing and derivation of a short instrument. Journal of psychiatric and mental health
nursing, 11(1), 36-42.
Needham, I., Abderhalden, C., Halfens, R. J. G., Fischer, J. E., & Dassen, T. (2005). Non-somatic effects of patient
aggression on nurses: a systematic review. Journal of Advanced Nursing, 49(3), 283–296.
Norman, G.R., & Streiner, D.L. (2014). Biostatistics: The Bare Essentials, 4th edn. PMPH USA, Shelton, CT. Poster,
E.C., & Ryan, J.A. (1989). Nurses' attitudes toward physical assaults by patients. Archives of psychiatric nursing,
3(6), 315-22.
Pai, H.C., & Lee, S. (2010). Risk factors for workplace violence in clinical registered nurses in Taiwan. Journal of
Clinical Nursing, 20(9-10), 1405-12.
Palmstierna, T., & Wistedt, B. (1987). Staff observation aggression scale, SOAS: presentation and evaluation. Acta
Psychiatrica Scandinavica, 76(6), 657-63.
Polit, D., & Beck, C. (2017). Nursing Research: Generating and Assessing Evidence for Nursing Practice. Tenth
edition. Lippincott Williams & Wilkins, Philadelphia.
Roche, M., Diers, D., Duffield, C., & Catling-Paull, C. (2010). Violence toward nurses, the work environment, and
patient outcomes. Journal of nursing scholarship, 42(1), 13-22.
Ryser, A.E., Duxbury, J., & Hahn, S. (2015). [Content validation of the quest ionnaire “The Management of
Aggression in People with Dementia Attitude Questionnaire German Version” (MAPDAQ-G)]. Pflege, 28(3), 157-
68.
Shields M. & Wilkins K. (2009). Factors related to on-the-job abuse of nurses by patients. Health reports 20(2), 7-
19.
Shrout, P.E., & Fleiss, J.L. (1979). Intraclass correlations: uses in assessing rater reliability. Psychological Bulletin,
86(2), 420–428.
Spector, P.E., Zhou, Z.E., & Che, X.X. (2014). Nurse exposure to physical and nonphysical violence, bullying, and
sexual harassment: a quantitative review. International Journal of Nursing Studies, 51(1), 72-84.
Streiner, L., & Norman, R. (2003). Health Measurement Scales. A Practical Guide to Their Development and Use.
Oxford University Press, New York.
Assessment of aggression: instrument validation
57
Streiner, D.L., & Kottner, J. (2014). Recommendations for reporting the results of studies of instrument and scale
development and testing. Journal of Advanced Nursing, 70(9), 1970-9.
Squires, A., Aiken, L.H., van den Heede, K., Sermeus, W., Bruyneel, L., Lindqvist, R., Schoonhoven, L., Stromseng,
I., Busse, R., Brzostek, T., Ensio, A., Moreno-Casbas, M., Rafferty, A.M., Schubert, M., Zikos, D., & Matthews, A.
(2013). A systematic survey instrument translation process for multi-country, comparative health workforce studies.
International journal of nursing studies, 50(2), 264-73.
Wei, C.Y., Chiou, S.T., Chien, L.Y., & Huang, N. (2016). Workplace violence against nurses: Prevalence and
association with hospital organizational characteristics and health-promotion efforts: Cross-sectional study.
International Journal of Nursing Studies, 56, 63-70.
Wells, J., & Bowers, L. (2002). How prevalent is violence towards nurses working in general hospitals in the UK?
Journal of Advanced Nursing, 39(3), 230-240.
Winstanley, S., & Whittington, R. (2004). Aggressive encounters between patients and general hospital staff: Staff
perceptions of the context and assailants’ levels of cognitive processing. Aggressive Behavior, 30(6), 534–543.
Winstanley, S. (2005). Cognitive model of patient aggression towards healthcare staff: The patient's perspective.
Work & Stress: An International Journal of Work, Health & Organisations, 19(4), 340-350.
Yudofsky, S.C., Silver, J.M., Jackson, W., Endicott, J., & Williams, D. (1986). The Overt Aggression Scale for the
objective rating of verbal and physical aggression. The American Journal of Psychiatry, 143(1), 35-9.

Assessment of aggression: validation of instAssessment of aggression: Experiences and perceptions
58
Assessment of aggression: validation of instAssessment of aggression: experiences and perceptions
59
Chapter III.
EXPERIENCES AND PERCEPTIONS OF AGGRESSION OF
NURSES WORKING IN PRIMARY CARE AND GENERAL
HOSPITAL SETTINGS
Tina Vandecasteele1,2, Ann Van Hecke1,3, Veerle Duprez1, Dimitri Beeckman1, Sofie Verhaeghe1,2
1 Department of Public Health, Faculty of Medicine and Health Sciences, University Centre for Nursing &
Midwifery, Ghent University, Ghent, Belgium.
2 Department Health care, VIVES University College, Roeselare, Belgium.
3 University Hospital Ghent, Ghent, Belgium.
Based on a manuscript submitted to the Journal of Advanced Nursing, under revision.

Chapter III
60
Assessment of aggression: experiences and perceptions
61
Aggression of patients and their family members directed towards nurses: Experiences
and perceptions of nurses working in primary care and general hospital settings
ABSTRACT
Aims. To assess nurses’ experiences of aggression by patients and their family members in primary
care and general hospital settings; and to identify factors associated with nurses’ perceptions of
aggression and its management.
Background. Even though a lot of research focused on nurses’ exposure to aggression, little is known
about nurses working in primary care. Understanding how nurses perceive aggression is important as
perceptions influence strategies used to manage aggression.
Design. Cross-sectional study (September 2014-December 2016).
Methods. Three validated instruments were used (the Survey of Violence Experienced by Staff; the
shortened Perception of Aggression Scale; and the Perception of Importance of Intervention Skills
Scale). The sample comprised 769 nurses from 24 general wards and one primary care organisation.
Descriptive statistics, Chi square and Independent-Samples t-test were performed. Multiple logistic
regression analyses were used to determine factors associated with perceptions of aggression and its
management.
Results. The majority of hospital nurses (89.2%) and primary care nurses (77.9%) indicated to have
experienced aggression. Primary care nurses were more emotionally burdened because of verbal
aggression (p=0.002), threats (p<0.001) and physical aggression (p<0.001) than hospital nurses.
Different factors were associated with perceiving aggression as a dysfunctional or as a functional
phenomenon. More working experience (OR 2.8), having duties in predominantly direct patient care (OR
6.3) or in education (OR 8.0), experiencing threats (OR 10.9) and having contact with patients’ parents
(OR 3.6) were associated with increased odds of perceiving aggression as a dysfunctional phenomenon.
The likelihood to perceive aggression as a functional phenomenon increased when nurses were male
(OR 3.9), worked in primary care (OR 2.4), were fulltime employed (OR 5.1), and had contact with
patients’ parents (OR 9.1) or patients’ partners (2.4).
Conclusion. Aggression is a major problem for nurses, irrespective of work setting. Aggression of
patients’ family members is highly prevalent. This study identified patient-related, nurse-related and

Chapter III
62
work-related characteristics associated with nurses’ perceptions of aggression suggesting crucial points
for developing interventions to support the understanding and management of aggression in nursing
practice. Future research should focus on further exploring the processes at play in perceiving specific
patients’ behaviour or patient’s family member’s behaviour as aggressive.
Key words. Aggression, general hospital, nurses, POAS-s, POIS, primary care, SOVES, violence.
Assessment of aggression: experiences and perceptions
63
1. | Introduction
Aggression in care relationships is internationally acknowledged as a serious problem for nurses
(Camerino et al., 2008), and the reported increase of patient aggression has been of interest to
researchers across countries in recent years (Spector, Zhou, & Che, 2014).
In addressing the problem of aggression in healthcare, research has focused on prevalence (Camerino
et al. 2008; Wei, Chiou, Chien, & Huang, 2016), determinants (Adib et al. 2002; Hahn et al., 2013), risk
factors (Amore et al., 2008; Gillespie, Gates, Miller, & Howard, 2010), and consequences (Sofield &
Salmond, 2003; Wells & Bowers, 2002), contributing to a greater understanding of aggression in care
relationships. On the level of patients’ characteristics (Hahn et al., 2013), staff characteristics (Duxbury,
2002; Jansen, Dassen, & Groot Jebbink, 2005), staff-patient and visitor interactions (Winstanley &
Whittington, 2004; Winstanley, 2005), and organizational characteristics (Farrell, Bobrowski, &
Bobrowski, 2006), different factors have been identified to contribute to the occurrence of patient
aggression. Research also indicates that -when being compared to other caregivers- nurses appear to
be at especial risk to encounter patient aggression due to the nature, duration and intensity of care
relationships with patients (Abderhalden et al., 2007; Camerino et al., 2008; Waschgler et al., 2013).
With regard to nurses’ working contexts, most of the research on aggression relates to geriatric (Almvik,
Rasmussen, & Woods, 2006; Duxbury, Pulsford, Hadi, & Sykes, 2013), emergency (Gerdtz et al., 2013),
and mental health settings (Abderhalden et al., 2007). Few attempts have been made to examine
aggression in general hospital settings (Winstanley & Whittington, 2004; Hahn et al., 2013; Heckemann
et al., 2015). However, research indicates that general hospital settings are increasingly regarded to be
vulnerable for aggressive incidents (Roche, Diers, Duffield, & Catling-Paull, 2010).
Moreover, with regard to nurses’ experiences of aggression in care relationships, surprisingly little is
known about nurses working in primary healthcare or community care. Research on aggression in
primary care generally focuses on patients experiencing domestic violence (Malpass et al. 2014; Pal,
2016), abuse (Williamson et al., 2015), or intimate partner violence (Higgins, Manhire, & Marshall, 2015;
Sawyer, Coles, Williams, & Williams, 2016). Few studies assessed patient aggression against general
practitioners (Magin et al., 2005) or nurses (Geiger-Brown et al. 2007; Da Silva et al., 2015). The few
existing studies focusing on primary care workers agree that aggression is common in primary care,
Chapter III
64
entailing the potential to be very stressful for caregivers (Barling, Rogers, & Kelloway, 2001; Büssing &
Höge, 2004).
Regarding the primary care context, some assumptions can be made about nurses’ work climate which
makes them more prone to experience patient aggression in comparison to hospital nurses. Primary
care nurses often act directly within communities, perform activities outside health centres (such as
private home visits) and generally work alone (Da Silva et al., 2015). The protection that nurses have in
hospital settings (e.g. presence of colleagues, security guards or alarm systems) is not present in
primary care (Geiger-Brown et al., 2007) which implies that nurses have to rely on their own resources
to manage aggression (Barling et al., 2001). This might result in primary care nurses being more
vulnerable to patient aggression than hospital nurses. However, experiences of patient aggression have
not been compared across both nurses’ work settings.
In addition, scarce literature is available about nurses’ perceptions of aggression. Literature has
emphasized nurses’ attitude towards patient aggression to be influential towards intervention strategies
in handling patient aggression (Duxbury, 2002; Vandecasteele et al., 2015). This link is acknowledged
in the Theory of Reasoned Action (Fishbein & Ajzen, 1975). Nurses’ perceptions about causation of
aggression may influence their approach to manage incidents (Jansen et al., 2005; Duxbury, Hahn,
Needham, & Pulsford, 2008). Research on perceptions of aggression primarily focused on nurses
working in mental health settings (Needham et al., 2005; Verhaeghe et al., 2016), in emergency settings
(Morken, Alsaker, & Johansen, 2016), or in residential care settings when caring for patients with
dementia (Duxbury, Pulsford, Hadi, & Sykes, 2012). However, generalizing results from these settings
to a more general setting of primary healthcare or general hospital wards is difficult. To our knowledge,
there is no literature focusing on nurses’ perceptions of patient aggression when working in a general
hospital setting, or in primary healthcare. We can assume these nurses, especially nurses in primary
healthcare, perceive patient aggression in a different way than nurses working in other contexts. They
generally know patients for a longer time as they contribute to continuity of care (Griffiths, Maben, &
Murrell, 2011), they guide patients in their daily living (Fletcher & Dahl, 2013), and get acquainted with
contextual factors which might explain patients’ behaviour.
Assessment of aggression: experiences and perceptions
65
2. | The study
2.1. | Aims
This study aims:
To compare nurses’ experiences of patient aggression and aggression by patients’ family
members in both primary care and general hospital settings.
To identify associations between patient-related, nurse-related and work-related characteristics
and nurses’ perceptions about (the management of) aggression.
2.2. | Design
A cross-sectional study was conducted.
2.3. | Participants
Data were collected in three general hospitals, a University hospital and a primary care organization in
Belgium between September 2014 and December 2016. In the hospital settings, all nursing officers
were invited to be involved in this study. Twenty-four general wards were invited to participate.
Emergency, geriatric and mental health departments were excluded. Each nurse manager, head of
department and head nurse was informed and invited to include their ward. All twenty-four wards
participated. Nurses working on these wards were invited to take part. The researchers informed the
nurses through a short presentation during team meetings. To ensure anonymity, completed
questionnaires were returned in secured boxes on the ward. The researchers collected these once a
week, returning to each ward to provide reminders and maximize participation.
In the primary care context, two departments of one primary care organization were included. In
Belgium, nurses who work in primary care are most often part of a larger primary care organization
which mainly involves nursing care during home visits. These nurses work in close collaboration with
general practitioners and other professional caregivers, but they are not necessarily directly employed
in general practice. Nurse officers of both departments were informed about the study, and invited to
participate.
In one of the departments, a convenience sample was recruited. Nurses were informed about the study
through a short video on the website of this department, and were able to complete the questionnaire
through a web-based link. In the second department, data were collected in 300 randomly selected
nurses. The nurse officer provided an anonymous list of all nurses. A random sample generated by
Chapter III
66
SPSS version 22.0 was obtained from this list. These nurses were informed about the study and invited
to participate through a short video which was sent via e-mail. Through a web-based link, nurses could
anonymously answer the questionnaire. Reminders were sent via e-mail, and were provided once every
two weeks between November to December 2016.
2.4. | Data collection
Nurses’ experiences and perceptions regarding patient aggression and aggression of patients’ family
members were assessed using three instruments.
The Survey of Violence experienced by Staff (SOVES). The SOVES was originally developed by
McKenna (2003) to gather information on workplace aggression, and to acquire data on involved
healthcare staff, patients and the broader workplace environment. The SOVES explores five themes:
(1) prevalence of aggression, (2) consequences of aggression, (3) reporting of aggression, (4) support
after experiencing aggression, and (5) training in managing aggression; as each of these themes is
related to three manifestations of aggression: verbal aggression, threats and physical aggression.
‘Verbal aggression’ is understood as abusive or offensive language, personally derogatory remarks,
profanity or obscene comments. ‘Threats’ are explained as warnings of intent to injure, harassment,
physical intimidation or threat with a weapon. ‘Physical aggression’ comprises slapping, pinching,
pushing, shoving, spitting, kicking or the use of a weapon. The SOVES provides a comprehensive
representation of aggression as several variables (nurses’ characteristics, patients’ characteristics,
nurses’ experiences of different types of aggression, practice characteristics and broader organizational
characteristics) are assessed. Close-ended questions and Visual Analogue Scales (VAS) are used to
assess these variables. Content validity and internal consistency have been assessed by McKenna
(2004), while feasibility and face validity of the German version of the SOVES have been appraised by
Hahn et al. (2011), showing good psychometric properties. The SOVES was translated into Dutch and
tested for use in the Belgian general hospital setting in a sample of 237 nurses. Face validity, content
validity and construct validity have been assessed showing acceptable to good psychometric properties
(Vandecasteele et al., (2017) - Submitted manuscript). Limited adjustments on sociodemographic
characteristics were made to suit the use in a primary care context.
The shortened Perception of Aggression Scale (POAS-s). The POAS, originally developed by
Jansen, Dassen, & Moorer (1997), consisted of 30 Likert-scaled statements which express various
views regarding aggression. In 2004, Needham et al. derived a shortened version, the POAS-s,
Assessment of aggression: experiences and perceptions
67
consisting of 12 items on a 5-point Likert scale, encompassing two dimensions in perceiving aggression:
aggression as a more dysfunctional and undesirable phenomenon (dimension 1) or as a more functional
and comprehensible phenomenon (dimension 2). Validation of the POAS-s has been assessed through
construct validity (Abderhalden et al., 2002), test-retest reliability, internal consistency (Needham et al.,
2004; Hahn et al., 2011), and content validity (Hahn et al., 2011), providing satisfactory psychometric
properties. The Dutch version of the POAS-s appraised construct validity and internal consistency,
procuring acceptable psychometric properties (Vandecasteele et al., (2017) - Submitted manuscript).
The Perception of Importance of Intervention Skills Scale (POIS). The POIS was developed by
Hahn et al. (2011) to measure perceptions of the importance of intervention skills in managing patient
aggression in a general hospital setting. The instrument consists of nine items reflecting common
prevention and intervention strategies (e.g. verbal communications, setting limits, intervening as a
team), measured on a 10-point VAS-scale. In 2011, a psychometric evaluation was conducted in
assessing internal consistency and construct validity in general hospital settings (Hahn et al., 2011),
emphasizing two dimensions in perceptions about aggression management: structured interventions,
evaluation and reflection to manage aggression (dimension 1), and preventive measures to manage
aggression (dimension 2). Good psychometric properties of the Dutch version were obtained in
assessing construct validity and internal consistency (Vandecasteele et al., (2017) - Submitted
manuscript).
2.5. | Data analysis
Frequencies were determined to describe participants’ demographic and professional characteristics.
Chi-square and Independent-Samples t-tests were used to test for differences among the two samples
regarding experiences of patient aggression and aggression caused by patients’ family members, and
different factors related to aggression (e.g. training in managing aggression). Chi-square tests were
used for categorical variables (e.g. utilized support mechanism following an occurrence of aggression),
while t-tests were used for continuous variables (e.g. emotional impact of verbal/physical aggression or
threats).
Logistic regression models were used to investigate factors associated with nurses’ perceptions of
aggression and its management. Multiple regression models were run with the two dimensions of the
POAS-s (‘perceiving aggression as a dysfunctional and undesirable phenomenon’ and ‘perceiving
aggression as a functional and comprehensible phenomenon’) and the two dimensions of the POIS
Chapter III
68
(‘perceiving structured interventions/reflection as important to manage aggression’ and ‘perceiving
preventive measures as important’) as dependent variables. Dependent variables were dichotomized.
A mean score on the statements constituting e.g. the perception that aggression is a
dysfunctional/undesirable phenomenon was computed per participant. Subsequently, mean scores
were categorized as ‘do not agree’ (range [1-2.4] = 0) and ‘agree’ (range [3.6-5] = 1). Neutral scores,
referring to an undecided opinion whether or not one agreed with e.g. the perception that aggression is
a dysfunctional phenomenon, were removed from analysis. Independent variables were selected based
on (1) a p<0.10 between the independent and dependent variable in univariate analyses, (2) an
empirically expected relationship between the independent and dependent variable based on literature,
or (3) a theoretical and logically expected relationship between the independent and dependent variable.
All independent variables were dichotomized. Independent variables were presented as odds ratios
(OR) with 95% confidence intervals. The significance level was held at α <0.05. Previous to regression
modelling, interrelation among independent variables was explored using Chi-square tests. All statistical
analyses were performed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA).
2.6. | Ethical considerations
The study was approved by the Ethical Committee of the Ghent University Hospital (B/670201421265)
and the Ethical Committees of the participating hospitals. The Institutional Review Board of the primary
care organization approved the study. Participation was voluntary. Hospital nurses provided consent by
signing an informed consent. Primary care nurses consented by completing the questionnaire.
3. | Results
The study population included 769 nurses (hospital setting: 271 nurses and primary care setting: 498
nurses). Response rate was 55% for the sample of hospital nurses, 55.3% and 27.8% for the sample of
nurses working in the two departments of primary care. Participants were predominantly female (94.6%),
had a diploma degree (50%), worked less than fulltime (56.9%) and the largest age group was older
than 46 years (43.5%). More than half of the nurses (76.3% and 72.6%) stated to have more than 10
years of professional experience in healthcare and more than 10 years of professional experience in
their present position. Nurses’ demographic and professional characteristics are displayed in table 1.
Several significant demographic and professional differences were observed among the two samples.
Primary care nurses are characterized by a high percentage of older nurses with a diploma degree, who
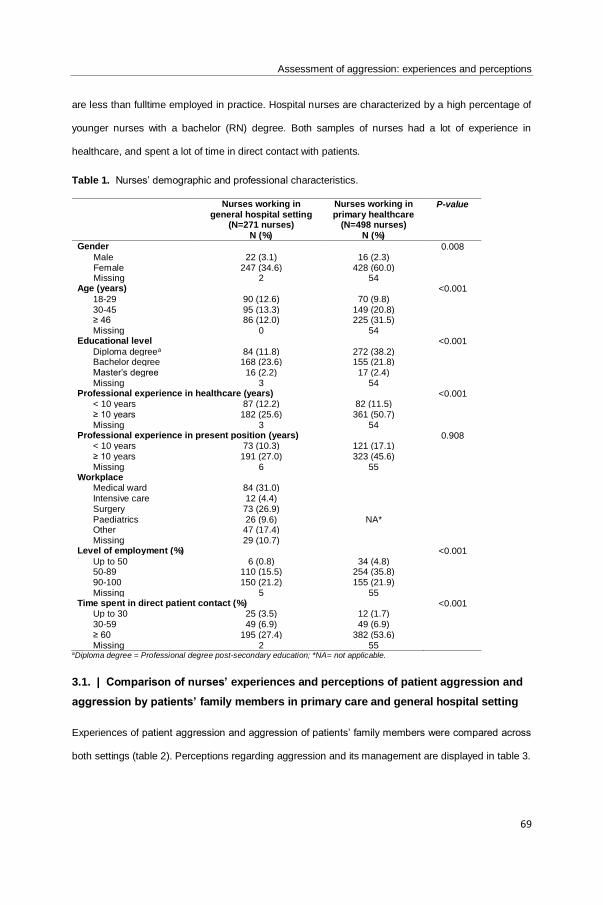
Assessment of aggression: experiences and perceptions
69
are less than fulltime employed in practice. Hospital nurses are characterized by a high percentage of
younger nurses with a bachelor (RN) degree. Both samples of nurses had a lot of experience in
healthcare, and spent a lot of time in direct contact with patients.
Table 1. Nurses’ demographic and professional characteristics.
Nurses working in general hospital setting
(N=271 nurses) N (%)
Nurses working in primary healthcare
(N=498 nurses) N (%)
P-value
Gender 0.008 Male 22 (3.1) 16 (2.3)
Female 247 (34.6) 428 (60.0) Missing 2 54
Age (years) <0.001 18-29 90 (12.6) 70 (9.8)
30-45 95 (13.3) 149 (20.8) ≥ 46 86 (12.0) 225 (31.5) Missing 0 54
Educational level <0.001 Diploma degreea 84 (11.8) 272 (38.2)
Bachelor degree 168 (23.6) 155 (21.8) Master’s degree 16 (2.2) 17 (2.4) Missing 3 54
Professional experience in healthcare (years) <0.001 < 10 years 87 (12.2) 82 (11.5)
≥ 10 years 182 (25.6) 361 (50.7) Missing 3 54
Professional experience in present position (years) 0.908 < 10 years 73 (10.3) 121 (17.1)
≥ 10 years 191 (27.0) 323 (45.6) Missing 6 55
Workplace Medical ward 84 (31.0)
NA*
Intensive care 12 (4.4) Surgery 73 (26.9) Paediatrics 26 (9.6) Other 47 (17.4) Missing 29 (10.7)
Level of employment (%) <0.001 Up to 50 6 (0.8) 34 (4.8)
50-89 110 (15.5) 254 (35.8) 90-100 150 (21.2) 155 (21.9) Missing 5 55
Time spent in direct patient contact (%) <0.001 Up to 30 25 (3.5) 12 (1.7)
30-59 49 (6.9) 49 (6.9) ≥ 60 195 (27.4) 382 (53.6) Missing 2 55
aDiploma degree = Professional degree post-secondary education; *NA= not applicable.
3.1. | Comparison of nurses’ experiences and perceptions of patient aggression and
aggression by patients’ family members in primary care and general hospital setting
Experiences of patient aggression and aggression of patients’ family members were compared across
both settings (table 2). Perceptions regarding aggression and its management are displayed in table 3.
Chapter III
70
Prevalence of patient aggression and aggression of patients’ family members. About 89.2% of
hospital nurses and 77.9% of primary care nurses experienced aggression during their professional
nursing career. Of this group, 62.8% of hospital nurses and 54.1% of primary care nurses experienced
aggression during the past 12 months. Of these hospital nurses, 94,1% had experienced verbal
aggression, 45.3% had experienced physical aggression and 36.1% had experienced threats. In
comparison, 91.9% of primary care nurses indicated to have experienced verbal aggression, 29%
experienced physical aggression and threats were experienced by 40% in the past 12 months. Hospital
nurses experienced more aggression during the past 12 months (p=0.044), and more verbal aggression
of patients or their family members than primary care nurses (p=0.012). More than half (69.0%) of
primary care nurses were exposed to verbal aggression of patients’ family members once, whereas
32.9% of hospital nurses experienced verbal aggression by patients’ family members once.
Consequences of patient aggression and aggression of patients’ family members. Eight primary
care nurses, and two hospital nurses had to take time off duty due to an aggressive incident. Primary
care nurses were more emotionally burdened because of verbal aggression (p=0.002), threats (p<0.001)
and physical aggression (p<0.001) in comparison to hospital nurses.
Support mechanisms used following experiences of aggression. No differences were observed
regarding support mechanisms (e.g. discussions with supervisors, colleagues, partners, friends or
family) following aggressive incidents. The majority of nurses across both samples gained support by
discussing the incident with their colleagues.
Training in the management of aggression. No differences were observed in the number of nurses
following training in aggression management (p=0.297). However, primary care nurses perceived
training as more important than hospital nurses (p<0.001). Primary care nurses appeared to have more
training in identifying and assessing potentially violent individuals (p=0.017), analysing situations within
the team (p=0.003), setting boundaries with potentially violent individuals (p<0.001), being self-aware in
interactions with patients (p=0.015), and having follow-up discussions about situations with patients
(p=0.003). Primary care nurses indicated to be more confident in using verbal (p<0.001) and physical
(p<0.001) intervention skills in managing aggression in comparison to hospital nurses.
Reporting of aggression. More hospital nurses indicated not to report aggressive incidents to
supervisors or line managers in comparison to primary care nurses (p<0.001). More primary care nurses

Assessment of aggression: experiences and perceptions
71
indicated to report ‘almost all to all’ incidents in comparison to hospital nurses (p=0.035). However,
irrespective of work setting, the majority of nurses indicated to report none to a few of the aggressive
incidents they encountered in the past 12 months.
Perceptions regarding aggression and its management. Overall and irrespective of work setting,
nurses were more inclined to agree that aggression is a dysfunctional phenomenon in comparison to
perceiving aggression as a functional/comprehensible phenomenon (table 3). No differences among the
two samples were observed related to perceiving aggression as a dysfunctional phenomenon (p=0.983),
nor as a functional phenomenon (p=0.149). However, primary care nurses perceived both intervention
(p<0.001) and preventive (p<0.001) strategies as more important to manage aggression than the
hospital nurses.
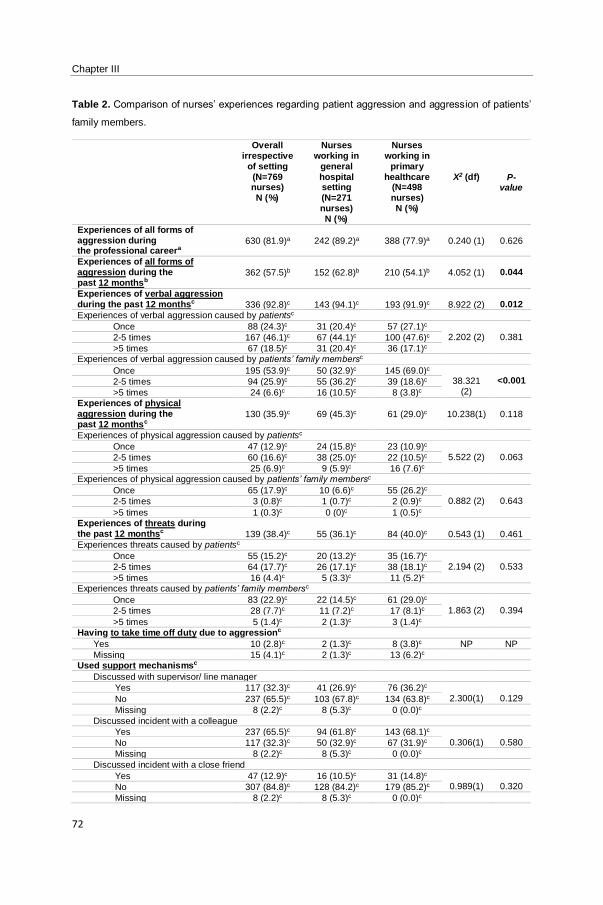
Chapter III
72
Table 2. Comparison of nurses’ experiences regarding patient aggression and aggression of patients’
family members.
Overall irrespective
of setting (N=769 nurses) N (%)
Nurses working in
general hospital setting (N=271 nurses) N (%)
Nurses working in
primary healthcare
(N=498 nurses) N (%)
X2 (df)
P-value
Experiences of all forms of aggression during the professional careera
630 (81.9)a
242 (89.2)a
388 (77.9)a
0.240 (1)
0.626
Experiences of all forms of aggression during the past 12 monthsb
362 (57.5)b
152 (62.8)b
210 (54.1)b
4.052 (1)
0.044
Experiences of verbal aggression during the past 12 monthsc
336 (92.8)c
143 (94.1)c
193 (91.9)c
8.922 (2)
0.012
Experiences of verbal aggression caused by patientsc
Once 88 (24.3)c 31 (20.4)c 57 (27.1)c 2.202 (2)
0.381 2-5 times 167 (46.1)c 67 (44.1)c 100 (47.6)c
>5 times 67 (18.5)c 31 (20.4)c 36 (17.1)c Experiences of verbal aggression caused by patients’ family membersc
Once 195 (53.9)c 50 (32.9)c 145 (69.0)c 38.321
(2)
<0.001 2-5 times 94 (25.9)c 55 (36.2)c 39 (18.6)c
>5 times 24 (6.6)c 16 (10.5)c 8 (3.8)c Experiences of physical aggression during the past 12 monthsc
130 (35.9)c
69 (45.3)c
61 (29.0)c
10.238(1)
0.118
Experiences of physical aggression caused by patientsc
Once 47 (12.9)c 24 (15.8)c 23 (10.9)c 5.522 (2)
0.063 2-5 times 60 (16.6)c 38 (25.0)c 22 (10.5)c
>5 times 25 (6.9)c 9 (5.9)c 16 (7.6)c Experiences of physical aggression caused by patients’ family membersc
Once 65 (17.9)c 10 (6.6)c 55 (26.2)c 0.882 (2)
0.643 2-5 times 3 (0.8)c 1 (0.7)c 2 (0.9)c
>5 times 1 (0.3)c 0 (0)c 1 (0.5)c Experiences of threats during the past 12 monthsc
139 (38.4)c
55 (36.1)c
84 (40.0)c
0.543 (1)
0.461
Experiences threats caused by patientsc
Once 55 (15.2)c 20 (13.2)c 35 (16.7)c 2.194 (2)
0.533 2-5 times 64 (17.7)c 26 (17.1)c 38 (18.1)c
>5 times 16 (4.4)c 5 (3.3)c 11 (5.2)c Experiences threats caused by patients’ family membersc
Once 83 (22.9)c 22 (14.5)c 61 (29.0)c 1.863 (2)
0.394 2-5 times 28 (7.7)c 11 (7.2)c 17 (8.1)c
>5 times 5 (1.4)c 2 (1.3)c 3 (1.4)c Having to take time off duty due to aggressionc
Yes 10 (2.8)c 2 (1.3)c 8 (3.8)c NP NP
Missing 15 (4.1)c 2 (1.3)c 13 (6.2)c Used support mechanismsc
Discussed with supervisor/ line manager
Yes 117 (32.3)c 41 (26.9)c 76 (36.2)c 2.300(1)
0.129 No 237 (65.5)c 103 (67.8)c 134 (63.8)c
Missing 8 (2.2)c 8 (5.3)c 0 (0.0)c
Discussed incident with a colleague
Yes 237 (65.5)c 94 (61.8)c 143 (68.1)c 0.306(1)
0.580 No 117 (32.3)c 50 (32.9)c 67 (31.9)c
Missing 8 (2.2)c 8 (5.3)c 0 (0.0)c
Discussed incident with a close friend
Yes 47 (12.9)c 16 (10.5)c 31 (14.8)c 0.989(1)
0.320 No 307 (84.8)c 128 (84.2)c 179 (85.2)c
Missing 8 (2.2)c 8 (5.3)c 0 (0.0)c
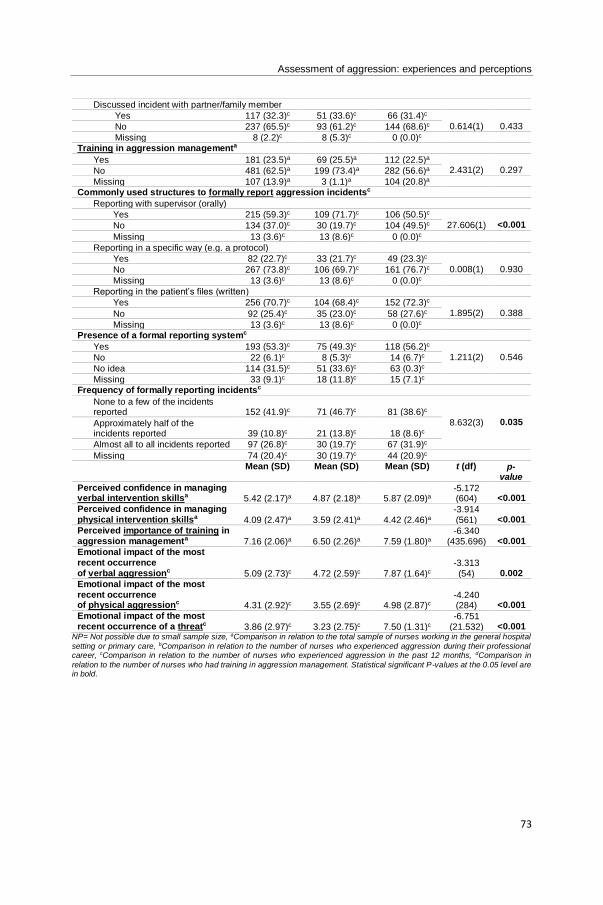
Assessment of aggression: experiences and perceptions
73
Discussed incident with partner/family member
Yes 117 (32.3)c 51 (33.6)c 66 (31.4)c 0.614(1)
0.433 No 237 (65.5)c 93 (61.2)c 144 (68.6)c
Missing 8 (2.2)c 8 (5.3)c 0 (0.0)c Training in aggression managementa
Yes 181 (23.5)a 69 (25.5)a 112 (22.5)a 2.431(2)
0.297 No 481 (62.5)a 199 (73.4)a 282 (56.6)a
Missing 107 (13.9)a 3 (1.1)a 104 (20.8)a Commonly used structures to formally report aggression incidentsc
Reporting with supervisor (orally)
Yes 215 (59.3)c 109 (71.7)c 106 (50.5)c 27.606(1)
<0.001 No 134 (37.0)c 30 (19.7)c 104 (49.5)c
Missing 13 (3.6)c 13 (8.6)c 0 (0.0)c
Reporting in a specific way (e.g. a protocol)
Yes 82 (22.7)c 33 (21.7)c 49 (23.3)c 0.008(1)
0.930 No 267 (73.8)c 106 (69.7)c 161 (76.7)c
Missing 13 (3.6)c 13 (8.6)c 0 (0.0)c
Reporting in the patient’s files (written)
Yes 256 (70.7)c 104 (68.4)c 152 (72.3)c 1.895(2)
0.388 No 92 (25.4)c 35 (23.0)c 58 (27.6)c
Missing 13 (3.6)c 13 (8.6)c 0 (0.0)c Presence of a formal reporting systemc
Yes 193 (53.3)c 75 (49.3)c 118 (56.2)c 1.211(2)
0.546 No 22 (6.1)c 8 (5.3)c 14 (6.7)c
No idea 114 (31.5)c 51 (33.6)c 63 (0.3)c
Missing 33 (9.1)c 18 (11.8)c 15 (7.1)c Frequency of formally reporting incidentsc
None to a few of the incidents reported
152 (41.9)c
71 (46.7)c
81 (38.6)c
8.632(3)
0.035 Approximately half of the incidents reported
39 (10.8)c
21 (13.8)c
18 (8.6)c
Almost all to all incidents reported 97 (26.8)c 30 (19.7)c 67 (31.9)c
Missing 74 (20.4)c 30 (19.7)c 44 (20.9)c
Mean (SD) Mean (SD) Mean (SD) t (df) p-value
Perceived confidence in managing verbal intervention skillsa
5.42 (2.17)a
4.87 (2.18)a
5.87 (2.09)a
-5.172 (604)
<0.001
Perceived confidence in managing physical intervention skillsa
4.09 (2.47)a
3.59 (2.41)a
4.42 (2.46)a
-3.914 (561)
<0.001
Perceived importance of training in aggression managementa
7.16 (2.06)a
6.50 (2.26)a
7.59 (1.80)a
-6.340 (435.696)
<0.001
Emotional impact of the most recent occurrence of verbal aggressionc
5.09 (2.73)c
4.72 (2.59)c
7.87 (1.64)c
-3.313 (54)
0.002
Emotional impact of the most recent occurrence of physical aggressionc
4.31 (2.92)c
3.55 (2.69)c
4.98 (2.87)c
-4.240 (284)
<0.001
Emotional impact of the most recent occurrence of a threatc
3.86 (2.97)c
3.23 (2.75)c
7.50 (1.31)c
-6.751 (21.532)
<0.001
NP= Not possible due to small sample size, aComparison in relation to the total sample of nurses working in the general hospital
setting or primary care, bComparison in relation to the number of nurses who experienced aggression during their professional career, cComparison in relation to the number of nurses who experienced aggression in the past 12 months, dComparison in
relation to the number of nurses who had training in aggression management. Statistical significant P-values at the 0.05 level are in bold.
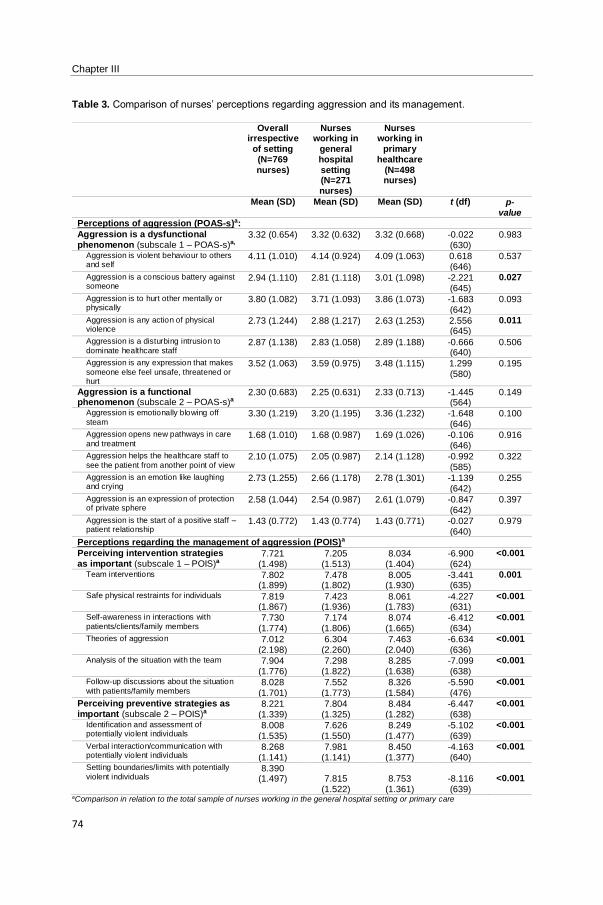
Chapter III
74
Table 3. Comparison of nurses’ perceptions regarding aggression and its management.
Overall irrespective
of setting (N=769 nurses)
Nurses working in
general hospital setting (N=271 nurses)
Nurses working in
primary healthcare
(N=498 nurses)
Mean (SD) Mean (SD) Mean (SD) t (df) p-value
Perceptions of aggression (POAS-s)a:
Aggression is a dysfunctional phenomenon (subscale 1 – POAS-s)a,
3.32 (0.654) 3.32 (0.632) 3.32 (0.668) -0.022 (630)
0.983
Aggression is violent behaviour to others and self
4.11 (1.010) 4.14 (0.924) 4.09 (1.063) 0.618 (646)
0.537
Aggression is a conscious battery against someone
2.94 (1.110) 2.81 (1.118) 3.01 (1.098) -2.221 (645)
0.027
Aggression is to hurt other mentally or physically
3.80 (1.082) 3.71 (1.093) 3.86 (1.073) -1.683 (642)
0.093
Aggression is any action of physical violence
2.73 (1.244) 2.88 (1.217) 2.63 (1.253) 2.556 (645)
0.011
Aggression is a disturbing intrusion to
dominate healthcare staff 2.87 (1.138) 2.83 (1.058) 2.89 (1.188) -0.666
(640) 0.506
Aggression is any expression that makes
someone else feel unsafe, threatened or hurt
3.52 (1.063) 3.59 (0.975) 3.48 (1.115) 1.299 (580)
0.195
Aggression is a functional phenomenon (subscale 2 – POAS-s)a
2.30 (0.683) 2.25 (0.631) 2.33 (0.713) -1.445 (564)
0.149
Aggression is emotionally blowing off
steam 3.30 (1.219) 3.20 (1.195) 3.36 (1.232) -1.648
(646) 0.100
Aggression opens new pathways in care
and treatment 1.68 (1.010) 1.68 (0.987) 1.69 (1.026) -0.106
(646) 0.916
Aggression helps the healthcare staff to
see the patient from another point of view 2.10 (1.075) 2.05 (0.987) 2.14 (1.128) -0.992
(585) 0.322
Aggression is an emotion like laughing and crying
2.73 (1.255) 2.66 (1.178) 2.78 (1.301) -1.139 (642)
0.255
Aggression is an expression of protection of private sphere
2.58 (1.044) 2.54 (0.987) 2.61 (1.079) -0.847 (642)
0.397
Aggression is the start of a positive staff – patient relationship
1.43 (0.772) 1.43 (0.774) 1.43 (0.771) -0.027 (640)
0.979
Perceptions regarding the management of aggression (POIS)a
Perceiving intervention strategies as important (subscale 1 – POIS)a
7.721 (1.498)
7.205 (1.513)
8.034 (1.404)
-6.900 (624)
<0.001
Team interventions 7.802 (1.899)
7.478 (1.802)
8.005 (1.930)
-3.441 (635)
0.001
Safe physical restraints for individuals 7.819 (1.867)
7.423 (1.936)
8.061 (1.783)
-4.227 (631)
<0.001
Self-awareness in interactions with
patients/clients/family members 7.730
(1.774) 7.174
(1.806) 8.074
(1.665) -6.412 (634)
<0.001
Theories of aggression 7.012 (2.198)
6.304 (2.260)
7.463 (2.040)
-6.634 (636)
<0.001
Analysis of the situation with the team 7.904 (1.776)
7.298 (1.822)
8.285 (1.638)
-7.099 (638)
<0.001
Follow-up discussions about the situation
with patients/family members 8.028
(1.701) 7.552
(1.773) 8.326
(1.584) -5.590 (476)
<0.001
Perceiving preventive strategies as important (subscale 2 – POIS)a
8.221 (1.339)
7.804 (1.325)
8.484 (1.282)
-6.447 (638)
<0.001
Identification and assessment of potentially violent individuals
8.008 (1.535)
7.626 (1.550)
8.249 (1.477)
-5.102 (639)
<0.001
Verbal interaction/communication with potentially violent individuals
8.268 (1.141)
7.981 (1.141)
8.450 (1.377)
-4.163 (640)
<0.001
Setting boundaries/limits with potentially
violent individuals 8.390
(1.497)
7.815 (1.522)
8.753
(1.361)
-8.116 (639)
<0.001
aComparison in relation to the total sample of nurses working in the general hospital setting or primary care
Assessment of aggression: experiences and perceptions
75
3.2. | Identifying associations between nurses’ characteristics and perceptions
regarding aggression and its management
Statistical modelling. Independent variables were:
Nurses’ characteristics: demographic (gender) and professional characteristics (work setting,
educational degree, level of employment, job experience, training level in aggression
management, perceived importance of training in aggression management, perceived
confidence in managing verbal or physical intervention skills in managing aggression)
Nurses’ accounts of experiences of patient aggression or family members’ aggression:
prevalence (having encountered different forms of aggression during the past 12 months
perpetuated by patients or their family members), consequences (taking time of duty due to
aggressive incidents, emotional impact of verbal or physical aggression or threats, …), reporting
(frequency of formally reporting aggressive incidents), support mechanism following an
aggressive incident (discussion with supervisor, colleague, friend or family), and perceptions
regarding aggression and its management.
Patients’ characteristics and family members’ characteristics: patients’ ages, frequency of
contact with patients’ family members.
Practice characteristics: direct patient contact time, nurses’ primary tasks.
Organizational characteristics: reporting systems regarding experiences of aggression,
commonly used systems to report aggression.
Univariate analyses examined relationships between independent and dependent variables (table 4,
additional files). Multiple regression analyses were run to identify associations between independent
variables and different perceptions regarding aggression and its management (table 5).
Factors associated with perceiving aggression as a dysfunctional and undesirable phenomenon.
Nurses with more experience in their current position had a higher chance to perceive aggression as
dysfunctional than nurses with less experience in their current position (p=0.006). When nurses mostly
work with patients’ parents (p=0.022), or they are mostly involved in direct patient care (p=0.046), or in
the education of nursing students (p=0.032), these factors increased the estimated odds of perceiving
aggression as dysfunctional. Nurses who had experienced threats in the past 12 months were more
likely to perceive aggression as dysfunctional (p=0.021). However, if nurses gained support following
an aggressive incident by discussing the incident with their supervisor, the likelihood to perceive
Chapter III
76
aggression as dysfunctional decreased (p=0.026). The likelihood to perceive aggression as
dysfunctional also decreased with nurses who primarily work with patients over 65 years of age
(p=0.031).
Factors associated with perceiving aggression as a functional and comprehensible
phenomenon. Male nurses had higher estimated odds to perceive aggression as functional than
female nurses (p=0.038). Primary care nurses (p=0.034), and nurses who work fulltime (p=0.048) had
a higher chance to perceive aggression as functional in comparison to hospital nurses or nurses holding
less than a fulltime employment. Nurses who mainly have contact with patients’ partners (p=0.037) or
patients’ parents (p=0.013) had a higher chance to perceive aggression as comprehensible. In contrast,
predominantly caring for patients over 65 years of age decreased the estimated chance to perceive
aggression as comprehensible (p=0.041). The likelihood to perceive aggression as functional decreased
when the commonly used system to report aggression was the verbal report with the supervisor
(p=0.045).
Factors associated with perceiving structured intervention strategies, evaluation and reflection
as important. Nurses with training in aggression management (p=0.007) and nurses with their primary
task in education of nursing students (p=0.017) had an increased estimated chance to perceive
structured interventions, evaluation or reflection as important.
Factors associated with perceiving preventive strategies as important. A logistic regression
analysis was not applicable due to a lack of variance in this dependent variable, and therefore these
results are not displayed in table 5. Two nurses (0.2%) perceived preventive measures as ‘not to
moderately important’, and 162 nurses (21.1%) indicated to be rather neutral regarding the importance
of preventive measures. Whereas, the majority of nurses (n=605, 78.7%) perceived preventive
measures to manage aggression as ‘important to very important’.
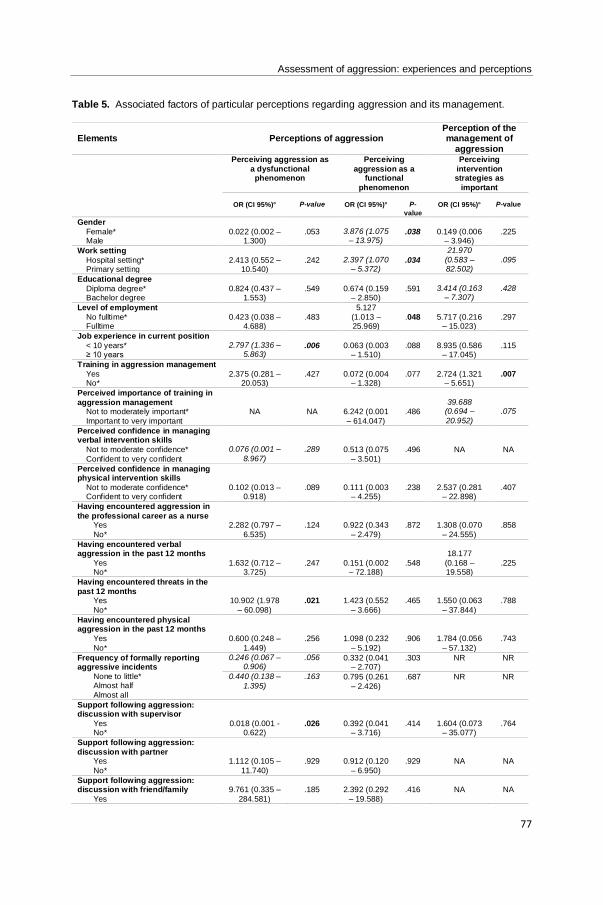
Assessment of aggression: experiences and perceptions
77
Table 5. Associated factors of particular perceptions regarding aggression and its management.
Elements
Perceptions of aggression
Perception of the management of
aggression
Perceiving aggression as
a dysfunctional phenomenon
Perceiving
aggression as a functional
phenomenon
Perceiving
intervention strategies as
important
OR (CI 95%)°
P-value
OR (CI 95%)°
P-
value
OR (CI 95%)°
P-value
Gender
Female* Male
0.022 (0.002 – 1.300)
.053
3.876 (1.075 – 13.975)
.038
0.149 (0.006 – 3.946)
.225
Work setting
Hospital setting* Primary setting
2.413 (0.552 – 10.540)
.242
2.397 (1.070 – 5.372)
.034
21.970
(0.583 – 82.502)
.095
Educational degree
Diploma degree* Bachelor degree
0.824 (0.437 – 1.553)
.549
0.674 (0.159 – 2.850)
.591
3.414 (0.163 – 7.307)
.428
Level of employment
No fulltime* Fulltime
0.423 (0.038 – 4.688)
.483
5.127
(1.013 – 25.969)
.048
5.717 (0.216 – 15.023)
.297
Job experience in current position
< 10 years* ≥ 10 years
2.797 (1.336 – 5.863)
.006
0.063 (0.003 – 1.510)
.088
8.935 (0.586 – 17.045)
.115
Training in aggression management
Yes No*
2.375 (0.281 – 20.053)
.427
0.072 (0.004 – 1.328)
.077
2.724 (1.321 – 5.651)
.007
Perceived importance of training in
aggression management Not to moderately important*
Important to very important
NA
NA
6.242 (0.001
– 614.047)
.486
39.688 (0.694 –
20.952)
.075
Perceived confidence in managing verbal intervention skills
Not to moderate confidence*
Confident to very confident
0.076 (0.001 –
8.967)
.289
0.513 (0.075
– 3.501)
.496
NA
NA
Perceived confidence in managing physical intervention skills
Not to moderate confidence* Confident to very confident
0.102 (0.013 – 0.918)
.089
0.111 (0.003 – 4.255)
.238
2.537 (0.281 – 22.898)
.407
Having encountered aggression in
the professional career as a nurse Yes
No*
2.282 (0.797 –
6.535)
.124
0.922 (0.343
– 2.479)
.872
1.308 (0.070
– 24.555)
.858
Having encountered verbal aggression in the past 12 months
Yes No*
1.632 (0.712 – 3.725)
.247
0.151 (0.002 – 72.188)
.548
18.177
(0.168 – 19.558)
.225
Having encountered threats in the
past 12 months Yes
No*
10.902 (1.978
– 60.098)
.021
1.423 (0.552
– 3.666)
.465
1.550 (0.063
– 37.844)
.788
Having encountered physical aggression in the past 12 months
Yes
No*
0.600 (0.248 –
1.449)
.256
1.098 (0.232
– 5.192)
.906
1.784 (0.056
– 57.132)
.743
Frequency of formally reporting aggressive incidents
None to little* Almost half
Almost all
0.246 (0.067 – 0.906)
.056 0.332 (0.041 – 2.707)
.303 NR NR
0.440 (0.138 –
1.395)
.163 0.795 (0.261
– 2.426)
.687 NR NR
Support following aggression: discussion with supervisor
Yes No*
0.018 (0.001 -0.622)
.026
0.392 (0.041 – 3.716)
.414
1.604 (0.073 – 35.077)
.764
Support following aggression:
discussion with partner Yes
No*
1.112 (0.105 –
11.740)
.929
0.912 (0.120
– 6.950)
.929
NA
NA
Support following aggression: discussion with friend/family
Yes
9.761 (0.335 –
284.581)
.185
2.392 (0.292
– 19.588)
.416
NA
NA
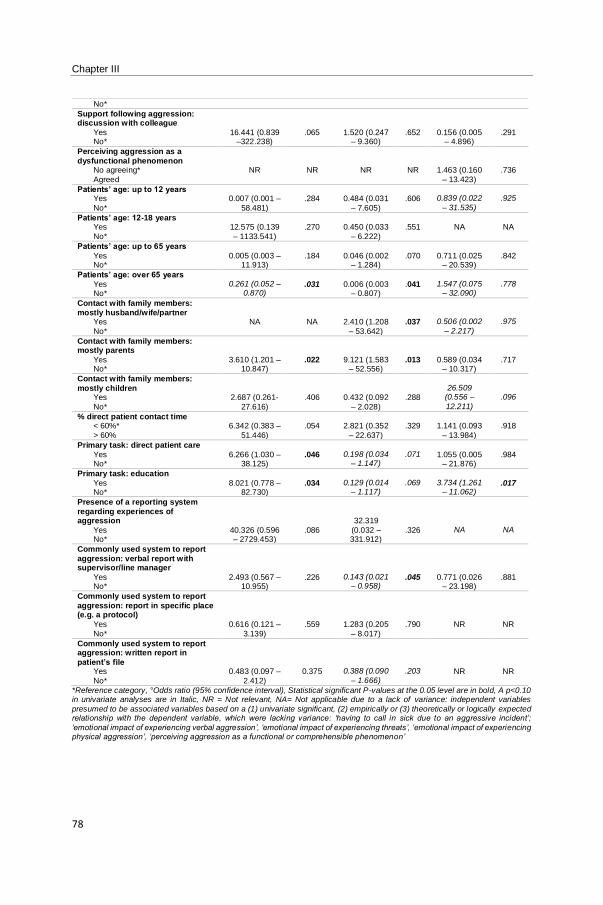
Chapter III
78
No*
Support following aggression: discussion with colleague
Yes No*
16.441 (0.839 –322.238)
.065
1.520 (0.247 – 9.360)
.652
0.156 (0.005 – 4.896)
.291
Perceiving aggression as a
dysfunctional phenomenon No agreeing*
Agreed
NR
NR
NR
NR
1.463 (0.160
– 13.423)
.736
Patients’ age: up to 12 years Yes
No*
0.007 (0.001 –
58.481)
.284
0.484 (0.031
– 7.605)
.606
0.839 (0.022
– 31.535)
.925
Patients’ age: 12-18 years Yes
No*
12.575 (0.139
– 1133.541)
.270
0.450 (0.033
– 6.222)
.551
NA
NA
Patients’ age: up to 65 years
Yes No*
0.005 (0.003 – 11.913)
.184
0.046 (0.002 – 1.284)
.070
0.711 (0.025 – 20.539)
.842
Patients’ age: over 65 years
Yes No*
0.261 (0.052 – 0.870)
.031
0.006 (0.003 – 0.807)
.041
1.547 (0.075 – 32.090)
.778
Contact with family members:
mostly husband/wife/partner Yes
No*
NA
NA
2.410 (1.208
– 53.642)
.037
0.506 (0.002
– 2.217)
.975
Contact with family members: mostly parents
Yes No*
3.610 (1.201 – 10.847)
.022
9.121 (1.583 – 52.556)
.013
0.589 (0.034 – 10.317)
.717
Contact with family members:
mostly children Yes
No*
2.687 (0.261-
27.616)
.406
0.432 (0.092
– 2.028)
.288
26.509 (0.556 –
12.211)
.096
% direct patient contact time < 60%*
> 60%
6.342 (0.383 –
51.446)
.054
2.821 (0.352
– 22.637)
.329
1.141 (0.093
– 13.984)
.918
Primary task: direct patient care
Yes No*
6.266 (1.030 – 38.125)
.046
0.198 (0.034 – 1.147)
.071
1.055 (0.005 – 21.876)
.984
Primary task: education
Yes No*
8.021 (0.778 – 82.730)
.034
0.129 (0.014 – 1.117)
.069
3.734 (1.261 – 11.062)
.017
Presence of a reporting system
regarding experiences of aggression
Yes No*
40.326 (0.596 – 2729.453)
.086
32.319
(0.032 – 331.912)
.326
NA
NA
Commonly used system to report
aggression: verbal report with supervisor/line manager
Yes No*
2.493 (0.567 – 10.955)
.226
0.143 (0.021 – 0.958)
.045
0.771 (0.026 – 23.198)
.881
Commonly used system to report
aggression: report in specific place (e.g. a protocol)
Yes
No*
0.616 (0.121 –
3.139)
.559
1.283 (0.205
– 8.017)
.790
NR
NR
Commonly used system to report aggression: written report in
patient’s file Yes
No*
0.483 (0.097 –
2.412)
0.375
0.388 (0.090
– 1.666)
.203
NR
NR
*Reference category, °Odds ratio (95% confidence interval), Statistical significant P-values at the 0.05 level are in bold, A p<0.10 in univariate analyses are in Italic, NR = Not relevant, NA= Not applicable due to a lack of variance: independent variables
presumed to be associated variables based on a (1) univariate significant, (2) empirically or (3) theoretically or logically expected relationship with the dependent variable, which were lacking variance: ‘having to call in sick due to an aggressive incident’;
‘emotional impact of experiencing verbal aggression’, ‘emotional impact of experiencing threats’, ‘emotional impact of experiencing physical aggression’, ‘perceiving aggression as a functional or comprehensible phenomenon’
Assessment of aggression: experiences and perceptions
79
4. | Discussion
Our findings provide a comparison of nurses’ experiences of patient aggression and aggression of
patients’ family members across two different nurses’ work settings: the general hospital setting and the
primary care setting or community care setting. Significant differences were observed regarding the
prevalence of aggression, consequences of experiencing aggression, used support mechanisms
following experiences of aggression, training in the management of aggression, reporting of aggressive
incidents and perceptions regarding aggression and its management.
In line with other research, this study confirms and stresses how aggression is an important concern for
nurses irrespective of their work setting (Spector et al., 2014). Our findings on the prevalence of
aggression are similar to those reported in other studies (Hahn et al., 2013; Hanson et al., 2015) in the
same way as verbal aggression appears to be the most prevalent form experienced (Edward, Ousey,
Warelow, & Lui, 2014). Except for hospital nurses’ experiences of physical aggression by patients, all
forms of aggression were perpetuated more by patients’ family members than by patients. This
difference was more pronounced in primary care nurses than in hospital nurses. Primary care nurses
encountered significantly more verbal aggression of patients’ family members in comparison to hospital
nurses. This difference might be explained by work contexts as primary care nurses interact more with
family members in the private home setting (Geiger-Brown et al., 2007; Nakaishi et al., 2013). Moreover,
primary care nurses described a significant higher emotional impact of experiencing verbal aggression,
physical aggression and threats than hospital nurses. The private and sometimes isolated home setting,
or the lack of direct contact with colleagues (Da Silva et al., 2015) might explain this difference. Although
there were no differences in the types of support mechanisms used by both samples of nurses following
an aggressive incident, we did not assess the perceived meaning or impact of support of colleagues,
supervisors, etc. Even though primary care nurses gained support from colleagues following an
aggressive incident, the lack of direct contact with colleagues when aggressive incidents occur might
explain the higher emotional impact of aggressive incidents. As Barling et al. (2001) established, primary
care nurses have to rely on their own resources to manage aggressive incidents. The prominent
emotional impact of aggression is important to acknowledge since research indicates that a long lasting
overwhelming of one’s coping resources might result in prolonged stress (Denton et al., 2002) which
might lead to poorer mental and physical health outcomes of professionals (Hanson et al., 2015).
Hanson et al. (2015) adopt the transactional stress and coping theory (Lazarus & Folkman, 1982) and
Chapter III
80
the social-learning theory (Bandura, 1982) to presume that nurses’ confidence in preventing and
responding to aggression mitigates the negative impact of aggression on one’s health. Our study
provides mixed evidence as primary care nurses described a significant higher emotional impact of
aggression in comparison to hospital nurses, while they also indicated to be significantly more confident
in using verbal and physical interventions to manage aggression. However, overall confidence levels of
both samples of nurses in managing aggression appear rather low to moderate. This finding warrants
further research to understand relationships between nurses’ confidence in managing aggression and
the emotional impact of experiencing aggressive incidents when they occur. This understanding would
generate insight to fine-tune interventions to support nurses in managing aggression.
In addition, associations between patient-related, nurse-related and work-related characteristics, and
nurses’ perceptions about aggression were examined. Having more working experience was associated
with perceiving aggression as a dysfunctional phenomenon, a finding confirmed in literature
(Abderhalden et al., 2002; Verhaeghe et al., 2016). When nurses’ primary task was the education of
nursing students, a higher likelihood of perceiving aggression as dysfunctional was observed. This
association might be explained by the higher workload of these nurses (McIntosh, Gidman, & Smith,
2014), or the protective role these nurses might adopt towards students, making them more prone to
perceive aggression as undesirable and disturbing. However, these are merely assumptions as there is
no literature to support these presumptions. Future work should explore relationships between nurses’
characteristics as working experience or organisational factors as workload and their influence on
perceiving patient’s behaviour as aggressive.
Predominantly working in direct patient care was associated with perceiving aggression as
dysfunctional. This association seems logical. More direct patient contact might result in nurses being
more exposed to patient aggression, leading to the perception that aggression is dysfunctional (Jansen
et al., 2005). Despite this presumption, other associations regarding the perception that aggression is a
functional phenomenon provide an additional understanding. Primary care nurses and nurses who
predominantly have contact with patient’s husbands or partners were more inclined to perceive
aggression as a functional phenomenon. Working in the patient’s home environment and interacting
with people close to the patient, might result in an understanding of patient’s behaviour even if it is
aggressive (Winstanley, 2005). This personal and long-term nature of caregiving is considered to be a
typical feature of community nursing (van Iersel et al., 2016).
Assessment of aggression: experiences and perceptions
81
Findings revealed how male nurses were more inclined to agree that aggression is comprehensible than
female nurses. Research on strategies male nurses use to manage emotions in nursing points out how
male nurses control own emotions as instrumental to the management of patients’ emotions. For
instance, remaining calm avoids adding to the emotions already present among patients (Cottingham,
2015). The de-escalating effect of managing own emotions to pre-empt patient’s belligerence might
influence perceptions of what patients’ aggression means. This can explain male nurse’s perception that
patient aggression is comprehensible.
It appears to be striking that predominantly working with patients over 65 years of age, and working with
patients’ parents are two factors associated with both perceiving aggression as a dysfunctional and as
a functional phenomenon. This finding seems quiet ambiguous, as it could be expected that nurses in
favour of the items constituting the perception that aggression is a dysfunctional phenomenon would
disagree with the items constituting the perception that aggression is a functional phenomenon. In line
with Abderhalden et al. (2002), nurses could have agreed to the two dimensions simultaneously. This
could demonstrate that the way aggression is perceived is more complex, encompassing agreement
with the notion that aggression can be both a functional and a dysfunctional phenomenon
(Vandecasteele et al., 2015). The perception of aggression might depend on specific clinical situations
(Jansen et al., 2005). For instance, when nurses have contact with predominantly patients’ parents,
parents might provide a contextual understanding of patients’ aggressive behaviour, which might lead
to the perception that aggressive behaviour can be functional. In contrast, research also identified
parents of paediatric patients to be a significant source of aggression (Pich, Hazelton, & Kable, 2013),
which might lead to circumstances in which aggression is perceived as dysfunctional. The same ‘double’
stand can be present in caring for older patients. Literature suggests aggression is highly prevalent in
geriatric settings, which might lead to the perception that aggression in is dysfunctional as a result of
the high exposure to aggression (Jansen et al., 2005). However, when caring for older patients some
contextual factors (e.g. the cognitive status of patients expressing aggressive behaviour) might be taken
into account leading to the perception that aggressive behaviour can be comprehensible and
understandable (Winstanley & Whittington, 2004; Vandecasteele et al., 2015). This ambiguity might be
a limitation of using the POAS-s. In this instrument, aggression is assessed on very general levels
whereas the specificity of particular aggressive incidents might have a more profound influence on how
Chapter III
82
aggression is perceived (Abderhalden et al., 2002). Future research is required to determine what
underlying processes are at play in perceiving patient’s behaviour as aggressive.
As an implication for practice, the findings on the reporting of aggressive incidents ought to be
considered. The majority of nurses indicated they did not, or only limitedly, formally report aggressive
incidents. The finding that a lot of nurses did not know whether formal reporting systems were present
has to be taken into account. The finding of underreporting aggressive incidents is internationally
acknowledged (Sato et al., 2013). Present findings contribute to this literature as an association was
found between commonly used structures to formally report aggression and the perception that
aggression is a comprehensible or functional phenomenon. When it was common to report with the
supervisor, the likelihood that aggression was perceived as functional decreased. This finding can be
contrasted with the finding that nurses, when they gained support from supervisors following aggression,
the chance that aggression was perceived as dysfunctional decreased. This finding emphasises that
mere reporting of incidents to supervisors is insufficient, a supportive context and a tenet to search for
what makes aggression understandable seems to be important to decrease the risk that the experience
and seriousness of aggression will be amplified. As an implication for research, it would be interesting
to understand nurses’ perceptions regarding different types of aggression. When nurses experienced
threats in the past 12 months, they were more inclined to perceive aggression as a dysfunctional and
undesirable phenomenon. This finding seems straightforward as direct experiences of aggression can
have a profound influence on perceptions of aggression (Jansen et al., 2005). However, experiencing
verbal or physical aggression did not seem to influence nurses’ perceptions of aggression. This finding
warrants exploration through research. Qualitative inquiry into the meaning of different types of
aggression would enable greater understanding of the (lack of) associations found here.
4.1. | Methodological considerations
A limitation is the cross-sectional nature of the study which does not allow to determine causality. This
is important in interpreting results of regression analyses. Another limitation pertains to the low response
rate in one of the departments in primary care (27.8%) where nurses were conveniently sampled. This
can introduce bias (Polit & Beck, 2017). Comparing both departments in primary care rendered no
significant differences in nurses’ experiences of patient aggression or aggression of patients’ family
members. In addition, recall bias can be present as the instruments adopt a 12 month time frame to
assess experiences of aggression. This induces the risk that one extreme aggressive incident

Assessment of aggression: experiences and perceptions
83
profoundly influences recollections of aggression. As the 12 months’ time frame is a commonly used
time frame to assess aggression in healthcare (Hahn et al., 2013), this time frame was adopted to allow
international comparison of findings.
5. | Conclusion
Aggression in healthcare is not a new problem. The findings from this study present a unique insight
into experiences of aggression of nurses working in primary care and general hospital settings, and into
the factors associated with nurses’ perceptions regarding aggression and its management. Irrespective
of work setting, the study confirms how aggression in nursing is highly prevalent, suggesting a negative
impact on nurses’ work, professional practice and overall well-being. Different factors (nurses’ gender
job experience, level of employment, work setting, primary tasks and exposure to aggression; contact
with patients’ family members and patients’ ages) were found to be associated with nurses’ perceptions
of aggression. There is a need for closer investigation of associations between nurses’ working
experience, nurses’ workload and the perception that aggression is a dysfunctional phenomenon. As
we cannot assume the cross-sectional associations we observed are causal, further work is warranted
to understand how certain perceptions of aggression emerge, how they influence nurse’s behaviour,
and what underlying processes are present in perceiving patient’s behaviour as aggressive.
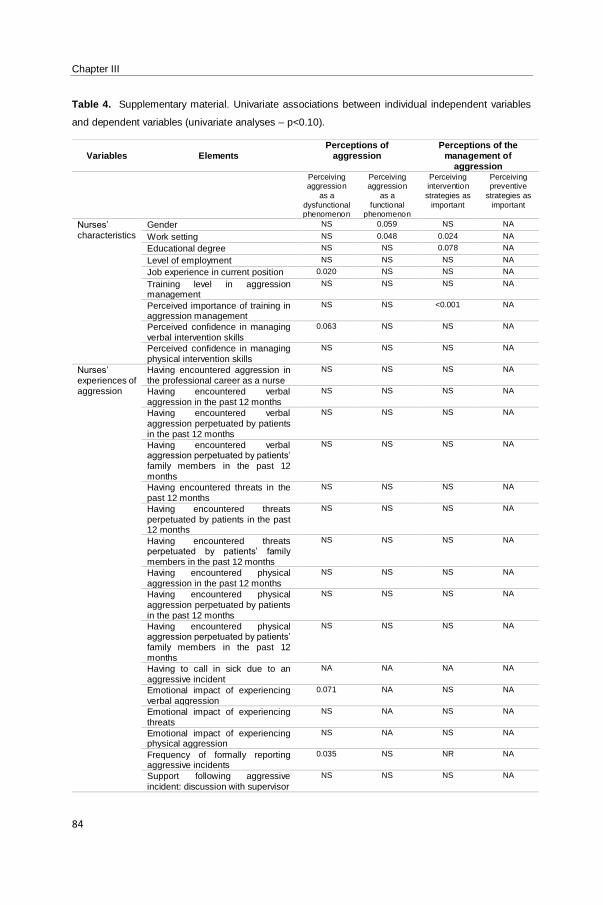
Chapter III
84
Table 4. Supplementary material. Univariate associations between individual independent variables
and dependent variables (univariate analyses – p<0.10).
Variables
Elements
Perceptions of aggression
Perceptions of the management of
aggression
Perceiving aggression
as a
dysfunctional phenomenon
Perceiving aggression
as a
functional phenomenon
Perceiving intervention
strategies as
important
Perceiving preventive
strategies as
important
Nurses’ characteristics
Gender NS 0.059 NS NA
Work setting NS 0.048 0.024 NA
Educational degree NS NS 0.078 NA
Level of employment NS NS NS NA
Job experience in current position 0.020 NS NS NA
Training level in aggression management
NS NS NS NA
Perceived importance of training in aggression management
NS NS <0.001 NA
Perceived confidence in managing verbal intervention skills
0.063 NS NS NA
Perceived confidence in managing physical intervention skills
NS NS NS NA
Nurses’ experiences of aggression
Having encountered aggression in the professional career as a nurse
NS NS NS NA
Having encountered verbal aggression in the past 12 months
NS NS NS NA
Having encountered verbal aggression perpetuated by patients in the past 12 months
NS NS NS NA
Having encountered verbal aggression perpetuated by patients’ family members in the past 12 months
NS NS NS NA
Having encountered threats in the past 12 months
NS NS NS NA
Having encountered threats perpetuated by patients in the past 12 months
NS NS NS NA
Having encountered threats perpetuated by patients’ family members in the past 12 months
NS NS NS NA
Having encountered physical aggression in the past 12 months
NS NS NS NA
Having encountered physical aggression perpetuated by patients in the past 12 months
NS NS NS NA
Having encountered physical aggression perpetuated by patients’ family members in the past 12 months
NS NS NS NA
Having to call in sick due to an aggressive incident
NA NA NA NA
Emotional impact of experiencing verbal aggression
0.071 NA NS NA
Emotional impact of experiencing threats
NS NA NS NA
Emotional impact of experiencing physical aggression
NS NA NS NA
Frequency of formally reporting aggressive incidents
0.035 NS NR NA
Support following aggressive incident: discussion with supervisor
NS NS NS NA
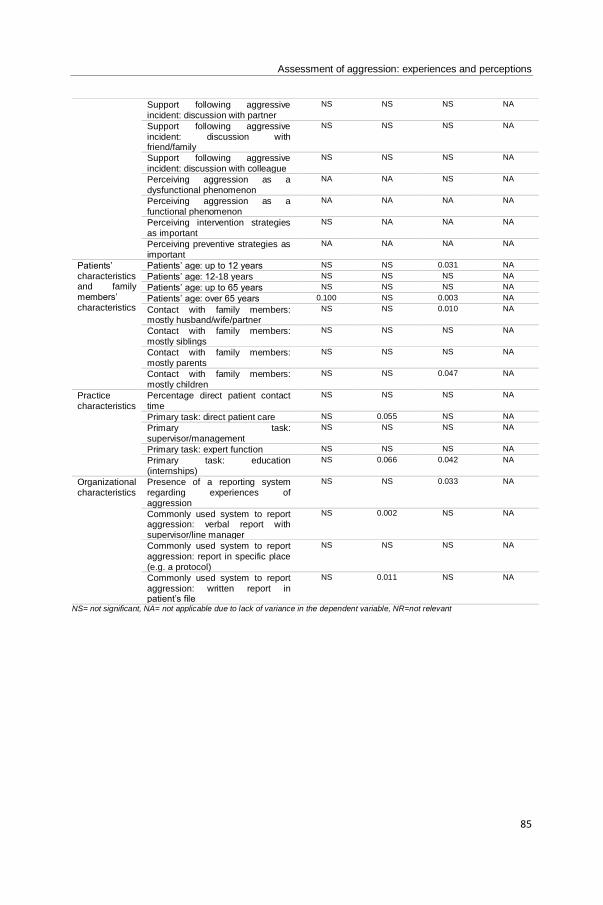
Assessment of aggression: experiences and perceptions
85
Support following aggressive incident: discussion with partner
NS NS NS NA
Support following aggressive incident: discussion with friend/family
NS NS NS NA
Support following aggressive incident: discussion with colleague
NS NS NS NA
Perceiving aggression as a dysfunctional phenomenon
NA NA NS NA
Perceiving aggression as a functional phenomenon
NA NA NA NA
Perceiving intervention strategies as important
NS NA NA NA
Perceiving preventive strategies as important
NA NA NA NA
Patients’ characteristics and family members’ characteristics
Patients’ age: up to 12 years NS NS 0.031 NA
Patients’ age: 12-18 years NS NS NS NA
Patients’ age: up to 65 years NS NS NS NA
Patients’ age: over 65 years 0.100 NS 0.003 NA
Contact with family members: mostly husband/wife/partner
NS NS 0.010 NA
Contact with family members: mostly siblings
NS NS NS NA
Contact with family members: mostly parents
NS NS NS NA
Contact with family members: mostly children
NS NS 0.047 NA
Practice characteristics
Percentage direct patient contact time
NS NS NS NA
Primary task: direct patient care NS 0.055 NS NA
Primary task: supervisor/management
NS NS NS NA
Primary task: expert function NS NS NS NA
Primary task: education (internships)
NS 0.066 0.042 NA
Organizational characteristics
Presence of a reporting system regarding experiences of aggression
NS NS 0.033 NA
Commonly used system to report aggression: verbal report with supervisor/line manager
NS 0.002 NS NA
Commonly used system to report aggression: report in specific place (e.g. a protocol)
NS NS NS NA
Commonly used system to report aggression: written report in patient’s file
NS 0.011 NS NA
NS= not significant, NA= not applicable due to lack of variance in the dependent variable, NR=not relevant
Chapter III
86
REFERENCES
Abderhalden, C., Needham, I., Friedli, T. K., Poelmans, J., & Dassen, T. (2002). Perception of aggression among
psychiatric nurses in Switzerland. Acta Psychiatrica Scandinavica, 412, 110-7.
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Fischer, J.E., & Haug H.J. (2007). Frequency and severity
of aggressive incidents in acute psychiatric wards in Switzerland. Clinical Practice and Epidemiology in Mental
Health, 4, 3-30.
Adib, S.M., Al-Shatti, A.K., Kamal, S., El-Gerges, N., & Al-Raqem, M. (2002). Violence against nurses in healthcare
facilities in Kuwait. International Journal of Nursing Studies, 39(4), 469-478.
Almvik, R., Rasmussen, K., & Woods, P. (2006). Challenging behaviour in the elderly: Monitoring violent incidents.
International Journal of Geriatric Psychiatry, 21(4), 368-74.
Amore, M., Menchetti, M., Tonti, C., Scarlatti, F., Lundgren, E., Esposito, W., & Berardi, D. (2008). Predictors of
violent behavior among acute psychiatric patients: clinical study. Psychiatry and Clinical Neurosciences, 62, 247–
55.
Barling, J., Rogers, A.G., & Kelloway, E.K. (2001). Behind closed doors: in-home workers' experience of sexual
harassment and workplace violence. Journal of occupational health psychology, 6(3), 255-69.
Bandura, A. (1982). Self-efficacy mechanism in human agency. American Psychologist, 37(2), 122-47.
Büssing, A., & Höge, T. (2004). Aggression and violence against home care workers. Journal of occupational health
psychology, 9(3), 206-19.
Camerino, D., Estryn-Behar, M., Conway, P.M., van Der Heijden, B.I., & Hasselhorn, H.M. (2008). Work-related
factors and violence among nursing staff in the European NEXT study: a longitudinal cohort study. International
Journal of Nursing Studies, 45, 35-50.
Cottingham, M.D. (2015). Learning to “Deal” and “De-escalate”: How Men in Nursing Manage Self and Patient
Emotions. Sociological Inquiry, 85(1), 75-99.
Da Silva, A.T., Peres, M.F., Lopes, C. de S., Schraiber, L.B., Susser, E., & Menezes, P.R. (2015). Violence at work
and depressive symptoms in primary health care teams: a cross-sectional study in Brazil. Social psychiatry and
psychiatric epidemiology, 50(9), 1347-55.
Denton, M.A., Zeytinoğlu, I.U., & Davies, S. (2002). Working in clients' homes: the impact on the mental health and
well-being of visiting home care workers. Home health care services quarterly, 21(1), 1-27.
Duxbury, J. (2002). An evaluation of staff and patient views of and strategies employed to manage inpatient
aggression and violence on one mental health unit: a pluralistic design. Journal of Psychiatric and Mental Health
Nursing, 9(3), 325-37.
Duxbury, J., Hahn, S., Needham, I., & Pulsford, D. (2008). The Management of Aggression and Violence Attitude
Scale (MAVAS): a cross-national comparative study. Journal of Advanced Nursing, 62(5), 596-606.
Assessment of aggression: experiences and perceptions
87
Duxbury, J., Pulsford, D., Hadi, M., & Sykes, S. (2012). Staff and relatives' perspectives on the aggressive behaviour
of older people with dementia in residential care: a qualitative study. Journal of psychiatric and mental health
nursing, 20(9), 792-800.
Duxbury, J., Pulsford, D., Hadi, M., & Sykes, S. (2013). Staff and relatives' perspective on the aggressive behavior
of older people with dementia in residential care: A qualitative study. Journal of Psychiatric and Mental Health
Nursing, 20(9), 792-800.
Edward, K.L., Ousey, K., Warelow, P., & Lui, S. (2014). Nursing and aggression in the workplace: a systematic
review. British journal of nursing, 23(12).
Farrell, G.A., Bobrowski, C., & Bobrowski, P. (2006). Scoping workplace aggression in nursing: findings from an
Australian study. Journal of Advanced Nursing, 55(6), 778-87.
Fishbein, M., & Ajzen, I. (1975). Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research.
Reading, MA: Addison-Wesley.
Fletcher, M.J., & Dahl, B.H. (2013). Expanding nurse practice in COPD: is it key to providing high quality, effective
and safe patient care? Primary care respiratory journal, 22(2), 230-3.
Geiger-Brown, J., Muntaner, C., McPhaul, K., Lipscomb, J., & Trinkoff, A. (2007). Abuse and violence during home
care work as predictor of worker depression. Home health care services quarterly, 26(1), 59-77.
Gerdtz, M.F., Daniel, C., Dearie, V., Prematunga, R., Bamert, M., & Duxbury, J. (2013). The outcome of a rapid
training program on nurses' attitudes regarding the prevention of aggression in emergency departments: A multi -
site evaluation. International Journal of Nursing Studies, 50(11), 1434-45.
Gillespie, G.L., Gates, D.M., Miller, M., & Howard, P.K. (2010). Workplace violence in healthcare settings: risk
factors and protective strategies. Rehabilitation Nursing, 35, 177–84.
Griffiths, P., Maben, J., & Murrells, T. (2011). Organisational quality, nurse staffing and the quality of chronic disease
management in primary care: observational study using routinely collected data. International Journal of Nursing
Studies, 48(10), 1199-210.
Hahn, S., Müller, M., Needham, I., Dassen, T., Kok, G, & Halfens, T.J. (2011). Measuring patient and visitor violence
in general hospitals: feasibility of the SOVES-G-R, internal consistency and construct validity of the POAS-S and
the POIS. Journal of Clinical Nursing, 20, 2519-30.
Hahn, S., Müller, M., Hantikainen, V., Kok, G., Dassen, T., & Halfens, R.J.G. (2013). Risk factors associated with
patient and visitor violence in general hospitals: results of a multiple regression analysis. International Journal of
Nursing Studies, 50(3), 374-85.
Hanson, G.C., Perrin, N.A., Moss, H., Laharnar, N., & Glass, N. (2015). Workplace violence against homecare
workers and its relationship with workers health outcomes: a cross-sectional study. BMC Public Health, 15(11).
Chapter III
88
Heckemann, B., Zeller, A., Hahn, S., Dassen, T., Schols, J. M., & Halfens, R. J. (2015). The effect of aggression
management training programmes for nursing staff and students working in an acute hospital setting. A narrative
review of current literature. Nurse Education Today, 35(1), 212–219.
Higgins, D., Manhire, K., & Marshall, B. (2015). Prevalence of intimate partner violence disclosed during routine
screening in a large general practice. Journal of primary health care, 7(2), 102-8.
Jansen, G., Dassen, T., & Moorer, P. (1997). The perception of aggression. Scandinavian Journal of Caring
Sciences, 11(1), 51-5.
Jansen, G.J., Dassen, T.W., & Groot Jebbink, G. (2005). Staff attitudes towards aggression in health care: a review
of the literature. Journal of Psychiatric and Mental Health Nursing, 12(1), 3-13.
Lazarus, R.S., & Folkman, S. (1984). Stress, Appraisal, and Coping. New York, NY: Springer Publishing Company.
Magin, P.J., Adams, J., Sibbritt, D.W., Joy, E., & Ireland, M.C. (2005). Experiences of occupational violence in
Australian urban general practice: a cross-sectional study of GPs. The Medical journal of Australia, 183(7), 352-6.
Malpass, A., Sales, K., Johnson, M., Howell, A., Agnew-Davies, R., & Feder, G. (2014). Women's experiences of
referral to a domestic violence advocate in UK primary care settings: a service-user collaborative study. The British
journal of general practice, 64(620), 151-158.
McIntosh, A., Gidman, J., & Smith, D. (2014). Mentors' perceptions and experiences of supporting student nurses
in practice. International Journal of Nursing Practice, 20(4), 360-5.
McKenna, B.G., Poole, S.J., Smith, N.A., Coverdale, J.H., & Gale, C.K. (2003). A survey of threats and violent
behaviour by patients against registered nurses in their first year of practice. International Journal of Mental Health
Nursing, 12(1), 56-63.
McKenna, K. (2004). Study of Work-Related Violence. Committee on Workplace Violence, North Eastern Health
Board, Ireland, 1–121.
Morken, T., Alsaker, K., & Johansen, I.H. (2016). Emergency primary care personnel's perception of professional-
patient interaction in aggressive incidents - a qualitative study. BMC Family practice 17(54).
Nakaishi, L., Moss, H., Weinstein, M., Perrin, N., Rose, L., Anger, W.K., Hanson, G.C., Christian, M., & Glass, N.
(2013). Exploring workplace violence among home care workers in a consumer-driven home health care program.
Workplace health & safety, 61(10), 441-50.
Needham, I., Abderhalden, C., Dassen, T., Haug, H.J., & Fischer, J.E. (2004). The perception of aggression by
nurses: psychometric scale testing and derivation of a short instrument. Journal of psychiatric and mental health
nursing, 11(1), 36-42.
Needham, I., Abderhalden, C., Halfens, R.J.G., Fischer, J.E., & Dassen, T. (2005). Non-somatic effects of patient
aggression on nurses: a systematic review. Journal of Advanced Nursing 49(3), 283-296.
Assessment of aggression: experiences and perceptions
89
Pal, K. (2016). Could you wait a second? Lancet 387, 1900-1.
Pich, J., Hazelton, M., & Kable, A. (2013). Violent behaviour from young adults and the parents of paediatric patients
in the emergency department. International Emergency Nursing, 21(3), 157-62.
Polit, D., & Beck, C. (2017). Nursing Research: Generating and Assessing Evidence for Nursing Practice. Lippincott
Williams & Wilkins, Philadelphia.
Roche, M., Diers, D., Duffield, C., & Catling-Paull, C. (2010). Violence toward nurses, the work environment, and
patient outcomes. Journal of nursing scholarschip, 42(1), 13-22.
Sato, K., Wakabayashi, T., Kiyoshi-Teo, H., & Fukahori, H. (2013). Factors associated with nurses' reporting of
patients' aggressive behavior: a cross-sectional survey. International Journal of Nursing Studies, 50(10), 1368-76.
Sawyer, S., Coles, J., Williams, A., & Williams, B. (2016). A systematic review of intimate partner violence
educational interventions delivered to allied health care practitioners. Medical Education, 50(11), 1107-1121.
Sofield, L., & Salmond, S.W. (2003). Workplace violence. A focus on verbal abuse and intent to leave the
organization. Orthopedic Nursing, 22, 274-83.
Spector, P.E., Zhou, Z.E., & Che, X.X. (2014). Nurse exposure to physical and nonphysical violence, bullying, and
sexual harassment: a quantitative review. International Journal of Nursing Studies 51(1), 72-84.
van Iersel, M., Latour, C.H., de Vos, R., Kirschner, P.A., & Scholte Op Reimer, W.J. (2016). Nursing students'
perceptions of community care and other areas of nursing practice: A review of the literature. International Journal
of Nursing Studies, 61, 1-19.
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D., & Verhaeghe, S. (2015). Nurses'
perceptions of transgressive behaviour in care relationships: a qualitative study. Journal of Advanced Nursing,
71(12), 2786-98.
Vandecasteele T., Van Hecke A., Debyser B., Vanderplancke T., Beeckman D. & Verhaeghe S. (2017) Assessment
of patients’ and family members’ aggression directed towards nurses working in general hospital settings: validation
of three instruments. Submitted manuscript.
Verhaeghe, S., Duprez, V., Beeckman, D., Leys, J., Van Meijel, B., & Van Hecke, A. (2016). Mental Health Nurses'
Attitudes and Perceived Self-Efficacy Toward Inpatient Aggression: A Cross-Sectional Study of Associations With
Nurse-Related Characteristics. Perspectives in psychiatric care, 52(1), 12-24.
Waschgler, K., Ruiz-Hernández, J.A., Llor-Esteban, B., & García-Izquierdo, M. (2013). Patients’ aggressive
behaviors towards nurses: development and psychometric properties of the hospital aggressive behavior scale-
users. Journal of Advanced Nursing, 69, 1418–27.
Wei, C.Y., Chiou, S.T., Chien, L.Y., & Huang, N. (2016). Workplace violence against nurses – Prevalence and
association with hospital organizational characteristics and health-promotion efforts: Cross-sectional study.
International Journal of Nursing Studies, 56, 63-70.
Chapter III
90
Wells, J., & Bowers, L. (2002). How prevalent is violence towards nurses working in general hospitals in the UK?
Journal of Advanced Nursing, 39, 230-40.
Whittington, R. (2002). Attitudes toward patient aggression amongst mental health nurses in the 'zero tolerance'
era: associations with burnout and length of experience. Journal of Clinical Nursing, 11(6), 819-25.
Williamson, E., Jones, S.K., Ferrari, G., Debbonaire, T., Feder, G., & Hester, M. (2015). Health professionals
responding to men for safety (HERMES): feasibility of a general practice training intervention to improve the
response to male patients who have experienced or perpetrated domestic violence and abuse. Primary health care
research & development, 16(3), 281-8.
Winstanley, S., & Whittington, R. (2004). Aggressive encounters between patients and general hospital staff: Staff
perceptions of the context and assailants' levels of cognitive processing. Aggressive behaviour, 30(6), 534-543.
Winstanley, S. (2005). Cognitive model of patient aggression towards health care staff: The patient's perspective.
Work & Stress: An International Journal of Work, Health & Organisations, 19(4), 340-350.
Patients’ perceptions of transgressive behaviour
91
Chapter IV.
PATIENTS’ PERCEPTIONS OF TRANSGRESSIVE
BEHAVIOUR IN CARE RELATIONSHIPS WITH NURSES
Tina Vandecasteele1,2, Bart Debyser2, Ann Van Hecke1,3, Tineke De Backer2, Dimitri Beeckman1,
Sofie Verhaeghe1,2
1 Department of Public Health, Faculty of Medicine and Health Sciences, University Centre for Nursing &
Midwifery, Ghent University, Ghent, Belgium.
2 Department Health care, VIVES University College, Roeselare, Belgium.
3 University Hospital Ghent, Ghent, Belgium.
Based on the article of Vandecasteele T., Debyser B., Van Hecke A., De Backer T., Beeckman D. &
Verhaeghe S. (2015) Patients’ perceptions of transgressive behaviour in care relationships with nurses:
a qualitative study. Journal of Advanced Nursing. 71(12), 2822–2833.

Chapter IV
92
Patients’ perceptions of transgressive behaviour
93
Patients’ perceptions of transgressive behaviour in care relationships with nurses: a
qualitative study
ABSTRACT
Aim. To gain insight in the onset and meaning of transgressive behaviour in care relationships with
nurses, from the perspective of patients.
Background. Aggression and transgressive behaviour in healthcare have been a focus of research
over the last decades. Most studies describe staff experiences on patient aggression. Patient’
perspectives on aggression and transgressive behaviour in interactions with nurses are rarely sought.
There is a need to better understand the meaning of transgressive behaviour from the patient’
perspective.
Design. Qualitative interview study.
Methods. Twenty patients were purposefully sampled from six wards of two general hospitals. Semi-
structured interviews were carried out in 2011. Data were analysed using the constant comparative
method inspired by the grounded theory approach.
Findings. On elaborating on what constitutes experiences of transgressive behaviour, patients employ
a framework of suppositions towards hospital care and nurse–patient relationships. This framework
leads to implicit ideas on how competent professional caregivers will be and on how relationships with
nurses will be characterized as normal human interactions. When these anticipated ideas are not met,
patients feel obliged to address this discrepancy by adjusting their expectations or behaviour. Patients
become more vigilant with regard to care given by nurses; search for own solutions; make excuses for
nurses or reprioritize their expectations. Because of this adjustment, perceptions of transgressive
behaviour are reinforced, mitigated or put into perspective.
Conclusion. This study offers an understanding of what underlying process patients go through when
interacting with nurses and how perceptions of transgressive behaviour can take place or evolve in these
interactions. Patients appear to adjust their own expectations or behaviour based on what they
experience in care relationships with nurses or the professional care in the hospital. It is crucial that
patients feel free to discuss their expectations or untoward needs, and nurses learn to understand and
reflect on those experiences.

Chapter IV
94
Keywords. Aggression, general hospital, nurse–patient relationship, nurses, nursing, patient, patients’
experiences, qualitative research, transgressive behaviour, violence.
Patients’ perceptions of transgressive behaviour
95
1. | Introduction
The article addresses the meaning of transgressive behaviour from the patient’s perspective in a general
hospital ward setting. Data are reported where patients describe in their own words their perceptions of
transgressive behaviour in care relationships with nurses. Data were obtained as part of a larger
qualitative study exploring the onset and meaning of transgressive behaviour in the dynamics of nurse–
patient care relationships.
1.1. | Background
Aggression in healthcare have been a focus of research over the last decades (Spector, Zhou, & Che,
2014). Extensive research has been conducted to understand the phenomenon of aggression in care
relationships between caregivers and patients (Hahn et al., 2008; Hahn et al., 2012). Most of the
research relates to geriatric (Almvik, Rasmussen, & Woods, 2006; Duxbury, Pulsford, Hadi, & Sykes,
2013), emergency (Gerdtz et al., 2013) and mental health settings (Abderhalden et al., 2007). Relatively
few attempts have been made to examine aggression in general healthcare settings (Winstanley &
Whittington, 2004; Hahn et al., 2008).
This study has two distinct presuppositions. The first is the focus in literature on staff experiences with
different types of patient aggression. Most of the studies investigate precursors or antecedents of
aggressive behaviour. These are performed by measuring risk factors associated with patient
aggression (Hahn et al., 2010; Hahn et al., 2013) or by retrospective surveys where healthcare providers
indicate to what extent they are exposed to specific physical, verbal and non-verbal aggressive
behaviours (Foster, Bowers, & Nijman, 2007; Abderhalden et al., 2008; Yang et al., 2012). Several
patient characteristics, workplace characteristics and characteristics of patient and healthcare provider
interactions have thus been identified to contribute to patient aggression (Hahn et al., 2008). The
majority of studies describe staff experiences in relation to patient aggression or difficult patient’
behaviour (Koekkoek, Hutschemaekers, van Meijel, & Schene, 2011). The patient’s perspective on
aggressive or difficult nurses’ behaviour is rarely sought. However, on a more general level, patients’
views of healthcare are considered an essential component of health service evaluations. They are used
to assess how well services are provided at a local level (McPherson, Kayes, Moloczij, & Commins,
2014); to obtain feedback to healthcare workers to improve quality of care (Cominskey, Coyne, Lalor &
Begley, 2014), or as an outcome measure to evaluate organizational changes (Metzelthin et al., 2013).
In literature, patient satisfaction surveys are regarded as a valid method to obtain patients’ views of
Chapter IV
96
healthcare and are as such frequently used (You et al., 2013; Lehto, Helander, Taari, & Aromaa, 2014).
Nevertheless, reservations exist about the validity of patient satisfaction as a concept and instruments
to measure it (Williams, 1994; Bruyneet et al., 2017). In recent years, the focus has shifted from patient
satisfaction to exploring dissatisfaction with healthcare (Söderberg, Olsson, & Skär, 2012; Howard,
Fleming, & Parker, 2013). The concept of dissatisfaction is believed to redirect attention to problems
experienced by patients and has mainly been explored by analysing formal complaints (Veneau &
Chariot, 2013; Zengin et al., 2014). However, these studies exclude negative experiences that are not
translated into formal complaint and as such do not seem sensitive enough in eliciting disappointment
or negative experiences with healthcare (Coyle & Williams, 2001).
The second presupposition of this study is related to the operationalization of aggressive or difficult
nurses’ behaviour. The broader term ‘transgressive behaviour’ was used. In literature, different
definitions of the concept of aggression exist, highlighting different elements (Liu, 2004; Nijman, Bowers,
Oud, & Jansen, 2005; Liu, Lewis, & Evans, 2013). These elements were merged into the following broad
definition of aggression: ‘Inflicting harm to material or to another person by transgressing the other
person’s limits, standards, or norms’. This study drew on the latter part of this definition: ‘transgressing
of limits, standards, or norms’. This notion assumes that experiences of transgressive behaviour can
vary from person to person as perceptions of an aggressive act is an internal personal construct
(O’Connell et al., 2000). Use of this term allows an individual interpretation of when and what limits are
exceeded for situations to be experienced as transgressive and which factors influence this process. In
literature, ‘transgression’ is commonly combined with moral or ethical values or principles as boundaries.
This particular conceptualization presumes certain moral or ethical suppositions which have to be
crossed for a moral or ethical transgression to occur. In this study, particular ethical or moral principles
were not defined or expected to be at stake when perceiving transgressive behaviour. Furthermore,
transgressive behaviour is situated in patient–nurse relationships and patient–nurse interactions. The
interpretation of limits, how they are exceeded, the perceived seriousness of the situation and the
processes involved in this interpretation, were not determined in advance. The overall aim of the study
is to provide a better understanding of perceptions of transgressive behaviour in care relationships from
the perspective of patients.
Patients’ perceptions of transgressive behaviour
97
2. | The study
2.1. | Aim
The aim of the study was to provide a better understanding in which cases nurse behaviour is perceived
as transgressive and what it is like for patients to experience transgressive behaviour in patient–nurse
relationships. The long-term goal is to combine the patient perspective with the nurse perspective
(reported in another publication) in an integrative analysis to provide an overall perspective of
transgressive behaviour in the dynamics of patient–nurse care relationships.
2.2. | Design
A qualitative study according to the grounded theory was conducted as this study focused on clarifying
and understanding patient perceptions of transgressive behaviour (Glaser & Strauss, 1967; Morse &
Field, 1996; Hallberg, 2006).
2.3. | Participants
Participants were recruited in 2011 in six wards located in two general hospitals in Belgium. These
hospitals serve both rural and urban communities situated in West Flanders, a Dutch-speaking Belgian
province. To recruit patients, student nurses were informed about the study and asked to distribute
closed envelopes with an information letter to patients of different wards. Included wards had a
diagnostic, medical, geriatric or surgical focus. Patients had to be admitted for a minimum of three days
which meant each patient had communicated regularly with nurses during their stay. When patients
gave their consent, a researcher visited the patient to answer questions and to get acquainted. Twenty
patients participated. Patients’ characteristics are presented in Table 1. The sample comprised a range
of participants in terms of age, educational level and reasons for hospital admission.
2.4. | Data collection
Data were collected using semi-structured interviews with open-ended questions. The interviewers
adopted a conversational and emphatic approach, guided by a topic list and patients’ answers. Patients
were encouraged to tell their story. Each interview started by asking the patient to describe an incident
he or she perceived as transgressive. From that point on, interview techniques elicited more details
about these perceptions. Table 2 provides examples of frequently asked questions. The topic list was
initially guided by sensitizing concepts derived from literature and was gradually adjusted to new insights
gained from analysis of interviews. To broaden initial insights and to select participants for subsequent
Chapter IV
98
interviews, theoretical sampling was used (Draucker, Martsolf, Ratchneewan, & Rusk, 2007). After 14
interviews, interviews were held with four patients who were labelled ‘difficult patients’ by several nurses.
These patients were sought to understand how they perceive care relationships and how they thought
they were perceived by nurses. Interviews were held shortly before hospital discharge or during the first
weeks afterwards and took place in the hospital or in the patients’ home. Each interview lasted between
20–81 minutes (average duration: 40 minutes). During and immediately after each interview, the
interviewer made field notes about patient’s non-verbal expressions and wrote down initial ideas about
the story of the patient or own perceptions of the interview. All interviews were tape-recorded. Audio
recordings were transcribed verbatim by a professional transcription service. Identifying data mentioned
in the interviews were deleted. Two analysts checked each transcript against the recording for accuracy.
Hence, they immersed themselves in the data and became sensitive to issues of importance. These
analysts uncovered and added information on reflection about participants’ expressions and reactions.
2.5. | Ethical considerations
Approval by the Ethical commission of the VIVES University College was provided. Written informed
consent was obtained. As patients were asked about nurses’ behaviour, confidentiality and anonymity
were stressed. The researchers were not known to any of the participants.
2.6. | Data analysis
Interviews were read and re-read entirely to obtain an overall picture of the interview and to get
familiarized with the data. Meaningful content of the interviews was comprehensively described and
subsequently coded using the NVIVO software package (QSR International). Fragments with the same
code were compared using the constant comparative method. By using initial inductive coding, by
comparing interviews and coded fragments and by considering possible meanings of the data, initial
ideas about conceptual constructs emerged. The process of data analysis occurred simultaneously with
data collection. This approach allowed to guide data collection based on emerging theoretical insights
and allowed to reach data saturation (Charmaz, 2008).
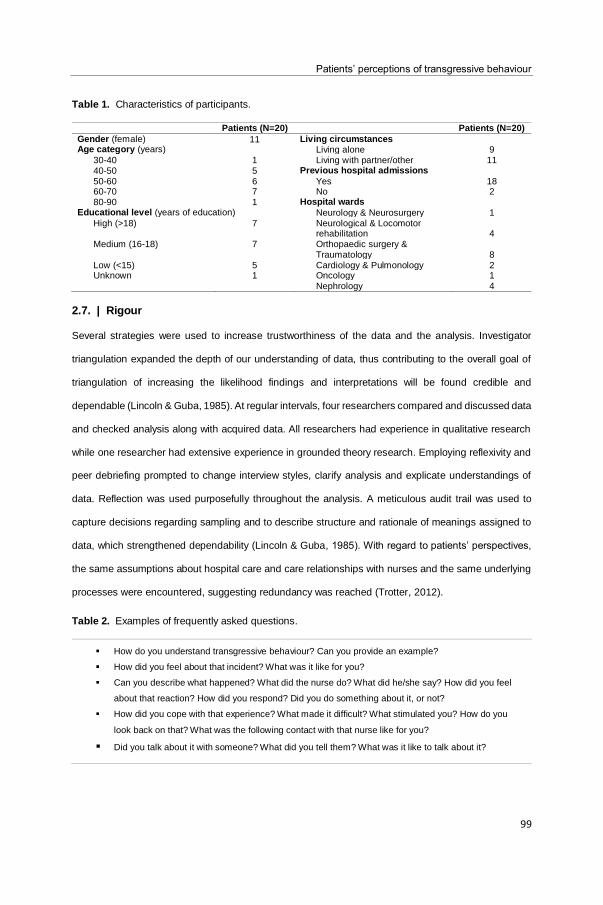
Patients’ perceptions of transgressive behaviour
99
Table 1. Characteristics of participants.
Patients (N=20) Patients (N=20)
Gender (female) 11 Living circumstances Age category (years) Living alone 9
30-40 1 Living with partner/other 11 40-50 5 Previous hospital admissions
50-60 6 Yes 18 60-70 7 No 2 80-90 1 Hospital wards
Educational level (years of education) Neurology & Neurosurgery 1 High (>18) 7 Neurological & Locomotor
rehabilitation
4 Medium (16-18) 7 Orthopaedic surgery &
Traumatology
8 Low (<15) 5 Cardiology & Pulmonology 2 Unknown 1 Oncology 1
Nephrology 4
2.7. | Rigour
Several strategies were used to increase trustworthiness of the data and the analysis. Investigator
triangulation expanded the depth of our understanding of data, thus contributing to the overall goal of
triangulation of increasing the likelihood findings and interpretations will be found credible and
dependable (Lincoln & Guba, 1985). At regular intervals, four researchers compared and discussed data
and checked analysis along with acquired data. All researchers had experience in qualitative research
while one researcher had extensive experience in grounded theory research. Employing reflexivity and
peer debriefing prompted to change interview styles, clarify analysis and explicate understandings of
data. Reflection was used purposefully throughout the analysis. A meticulous audit trail was used to
capture decisions regarding sampling and to describe structure and rationale of meanings assigned to
data, which strengthened dependability (Lincoln & Guba, 1985). With regard to patients’ perspectives,
the same assumptions about hospital care and care relationships with nurses and the same underlying
processes were encountered, suggesting redundancy was reached (Trotter, 2012).
Table 2. Examples of frequently asked questions.
How do you understand transgressive behaviour? Can you provide an example?
How did you feel about that incident? What was it like for you?
Can you describe what happened? What did the nurse do? What did he/she say? How did you feel
about that reaction? How did you respond? Did you do something about it, or not?
How did you cope with that experience? What made it difficult? What stimulated you? How do you
look back on that? What was the following contact with that nurse like for you?
Did you talk about it with someone? What did you tell them? What was it like to talk about it?
Chapter IV
100
3. | Results
During the interviews, all patients originally declared to be satisfied with the care they were given in the
hospital, and with the nurse – patient relationships. Patients stated that nurses were friendly, that they
did not have important remarks and that, overall, they did not have complaints:
“… Generally speaking, it’s all right. I don’t have complaints, really. No, overall, I don’t have any
complaints about the hospital, no complaints, so generally…”
Patients uttered that the experienced care generally meets their expectations. The most important
problem patients can initially think of is that hospital food is not nice. However, as patients gave a more
detailed account of their specific experiences, their satisfaction became less pronounced. Very
cautiously, perceived satisfaction was toned down.
“… There was the occasional nurse who was not as friendly…”
“…The thing I could come up with is that the people who are working there have too much to
do, to the point where they don’t have enough time to take care of you properly…”
Gradually, patients spontaneously started to tell stories about experiences with nurses that were not as
positive and interactions they felt were transgressive. The nature of these examples varied greatly.
Some stories concerned medical or health-related matters, while others concerned communication and
interactions. Some patients told about how a nurse did not know how to fit a prosthesis and hurt the
patient in the attempt; another nurse did not recognize a patient was having an epileptic seizure; nurses
took up to 30 minutes to answer calls; a nurse refused to administer pain relief; a nurse made the remark
that the patient was addicted to a type of medication; dinner was taken away by the nurse while the
patient was not given the time to finish it, etcetera.
As patients were describing these various incidents, they went into further detail about what exactly
made it a bad or transgressive experience. An explanatory process of how experiences of transgressive
behaviour emerge is described below.
3.1. | Framework of suppositions: ‘Competent care and human interaction, surely that
is self-evident?’
When patients are admitted to the hospital, they envisage what care and nurse – patient relationships
are going to be like. They have general ideas or suppositions about what it is like to be hospitalized.
Patients’ perceptions of transgressive behaviour
101
[Author’s note: The term supposition is understood as: ‘An idea or notion sufficiently probable to be
practically assumed as true, or to be at least admitted as possibly true, on account of consistency with
known facts’ (English Oxford Dictionary)] These general ideas concern two domains. The first domain
pertains ideas about hospital care. Patients feel they will be in competent and capable hands in a
hospital. Because of patients’ specific circumstances of illness or rehabilitation, they need hospital care.
From this perspective, they expect care providers who are able to give adequate and competent
responses to their illness and care related needs:
“…I assume they know how to do their job. They know all this stuff, I don’t, so I need to listen to
them. It’s their job, they went to school for these things, I assume it’s their area of expertise, I
assume they know about this…”
The second domain of patients’ visualization concerns ideas about the nurse – patient relationship.
Patients think about how they will have normal human contact or normal human interactions with nurses.
They have the idea they will be heard and seen as human beings, despite the fact they are in a hospital
as patients:
“…that they act completely normal, it should all be very normal, (. . .) human, acting normal,
have some respect, a little compassion...”
“…You assume they know their job, but you also expect a little more than that...”
These two suppositions are considered to be self-evident and logical. These are thought to be normal
ideas about what hospital care and nurse – patient relationships are going to be like. These assumptions
add a factor of predictability to a patient’s stay in the hospital. The assumptions are not considered
special or exceptional, they are part of a natural framework of suppositions.
3.2. | Experiencing discrepancies: ‘Competent care and human interaction, is it not
self-evident after all?’
Those two suppositions are tacit and rather implicit. Patients are not always aware they have these
suppositions. This realization hits them when their assumptions are not met. When patients do not feel
they are getting competent care or human interactions, they become aware they initially formed ideas
about care and care relationships. It is only then patients become aware of these previously made
suppositions. Non-fulfilment of suppositions causes them to experience indignation. There is a
Chapter IV
102
discrepancy between self-evident assumptions and the perceived reality. Subsequently, competent care
and human interactions are no longer perceived as self-evident.
When it comes to competent care, some patients told stories in which the expertise of the care providers
was questioned. One patient described a nurse provided pain relieving medication while he is allergic
to that product. In response, the patient’s daughter attached a list to her father’s bed listing products he
is allergic to. Despite this list, every time her father asked for pain relief, that same product he is allergic
to was brought to him. Another patient described a nurse accompanied him for an examination. He
asked where she was taking him to and when she said it was to Nuclear Magnetic Resonance, he said
he was not allowed to because of his pacemaker. He indicated the nurse had not gone through his
medical file and was putting him in danger.
“…I can see something’s going on with that man, she just leaves and ignored him and all of a
sudden I can see him shaking, an actual epileptic seizure. . . they don’t even recognize it. What
have they gone to school for? I think that’s really sad…”
The second supposition made by patients concerns the nurse – patient relationship and the human
interactions patients envision as part of that relationship. Patients told stories of how they were ignored
by nurses or not treated as human beings. One woman described the nurse criticized her for not having
to have worked a day in her life because of her long-term illness. Another man described dinner was
put in front of him without a single word, no ‘good afternoon’ or ‘enjoy’. Patients also provided examples
of a lack of genuine involvement of nurses in the nurse – patient contact. Various patients mentioned
they felt they were just a “number”:
“…One thing that is very annoying is when two nurses are caring for you and they are conversing
with each other over your head. That’s so annoying, you really feel like just a number…”
Furthermore, various patients indicated nurses are more concerned about the way care is organized
than they are about the patient’s request. Patients mentioned that nurses stick to their routine and are
reluctant to deviate from it. One nurse distributes medication while another checks parameters of all
patients. Patients describe they cannot approach the nurse about matters that are not part of his or her
task at that moment:
“…But when it comes to organization as such, they all have their own task.. Don’t bother asking
a nurse to do this or that, because someone who’s serving dinner is then going to collect the
Patients’ perceptions of transgressive behaviour
103
trays. It’s often something small. ‘Could you switch on my nebulizer?’. They’re doing their
rounds, it’s a strict routine. They refuse to deviate from it…”
Various patients gave examples of situations in which they were not acknowledged or heard with regard
to their own appraisal or expertise concerning their illness and health. Patients stated that they
themselves felt what they could or could not do, but nurses kept emphasizing and imposing things,
according to guidelines and protocols, they should be able to do at a certain point in time. Several
patients felt they were not heard.
“…I had two surgeries on my back. So the first day after the surgery, they said, ‘roll to the side
and sit up’, of course that’s difficult. On the second day, they demand you get out of bed. But I
felt worse, I couldn’t get out. And they didn’t believe me, the nurse didn’t believe it. ‘You’ve had
surgery and according to the text-book, you should be able to get out of bed on the second day’.
On the third day, they made a new scan and saw that those nerves had not been unblocked
and on the fourth day I had another surgery. So they don’t listen, because that’s not possible,
according to the ‘textbook’ you should be able to do this…”
Because of these experiences, patients develop a different view of hospital care and nurse – patient
relationships. Receiving competent care and having human interactions with nurses are no longer
considered self-evident or logical. The trust patients used to have in hospital care and nurse – patient
relationships is still present, but carefully toned down.
3.3. | And now what?: ‘Apparently, competent care and human interactions are not
self-evident’
When patients gradually realize that hospital care and nurse – patient relationships are not what they
thought it would be, they become distressed. Receiving competent care and having human interactions
are no longer self-evident, which forces patients to adapt to these new perceptions. These experiences
have different effects. Several patterns are put into action: patients become more vigilant with regard to
care given by nurses; they search for their own solutions; they make excuses for the nurses or they
reprioritize their expectations.
Dealing with perceived discrepancies: ‘You do pay more attention’. When patients realize it is not
self-evident to receive adequate care or do not feel in competent and capable hands, they become more
Chapter IV
104
observant and vigilant. Patients describe they observe nurses carefully, check their medication and ask
which examinations they are having and why. The care they receive is more outspokenly questioned.
“…They came to collect me for my hip. Ah, you’ve got a scanner appointment. She says: ‘it’s an
MR scan’. I say: ‘an MR scan? I can’t do that because I’ve got a pacemaker.’ And she says ‘And
now you tell me?’ ‘Listen here, missy, you walk in here and tell me to come.’ You’d be in there
if you wouldn’t have said something, wouldn’t you! The battery can generate voltage which could
burn your heart, destroying your pacemaker. If you’re not paying attention, you’re done for. You
constantly have to be on your guard…”
Numerous patients mention that they have become more vigilant when they are in hospitals because of
experiences during previous hospitalizations. Previous experiences taught people what competent care
is or what is to be expected from care providers. Patients acknowledge their attitude towards nurses
became sterner. They report to have learnt to be assertive and vocal when it comes to expressing their
dissatisfaction.
“…I know that, when you’re in hospital, you’re supposed to keep quiet. It’s not the first time I’ve
been in hospital. If you’re good and you’re afraid to say anything, it’s not going to help you. You
have to advance and then you’ll get what you need. If you don’t stand your ground and you
never say anything, they’ll think you’re an easy-going patient, but they’ll also ignore you…”
Dealing with perceived discrepancies: ‘I take care of it myself’. Some patients look for solutions on
their own when hospital care and nurse – patient relationships do not meet their expectations. They no
longer expect to receive certain aspects of caregiving in nurse – patient care relationships. They search
for other solutions. One woman described her neighbour helped her out of bed every time she needed
to use the bathroom. Otherwise, she had to wait too long for nurses to come. As this solution worked
perfectly well, she no longer called nurses.
“…You’re in pain, trying to find a comfortable position and you can’t and you ask for a simple
painkiller, just some paracetamol, not morphine or something and they won’t give it to you. Well,
I said, you know what, I won’t ask anymore and I didn’t. I asked the boys to bring some
paracetamol from home. I had some in the cupboard. That’s me, taking care of myself...”
Dealing with perceived discrepancies: ‘It is annoying, but not their fault’. Some patients adapt or
adjust their expectations. They realize their assumptions do not correspond with the reality of hospital
Patients’ perceptions of transgressive behaviour
105
care so they adapt their expectations from nurses or keep them to a minimum. They start calling nurses
less and only do so when it is urgent, or try to understand when medication errors are made when
several patients with the same surname are on the same ward, or they know it can take long for nurses
to answer calls so they call in advance if they need to use the bathroom.
“…I didn’t ask a lot, I waited until they came around and if it was urgent, I called out when
someone was passing in the hallway and I asked for someone to come around...”
“…No, they never addressed me by my name. But I don’t expect them to. You can’t expect them
to know every patient’s name, can you. With all those patients coming and going, how can
they…”
Other patients minimize their needs by taking into account the needs of their fellow patients. They
consider the fact they are not alone and that the nurses’ time has to be divided among all patients. Since
nurses have a lot of patients to care for, patients adjust their expectations of care that can be provided
to them:
“…We weren’t difficult patients. I know that everyone in there is ill too. You can never think
you’re the only one there. I keep that in mind…”
Various patients take the nurses’ working context into consideration. The perceived discrepancy
between their suppositions of hospital care and the reality is thus minimized. This discrepancy is linked
to matters that do not fall within the nurses’ responsibilities. The way care is organized, or shortage of
staff is given as reasons for why patients feel they are not treated as human beings. Nurses themselves
are not viewed as the cause of discrepancies. Although care relationships may not meet patients’
expectations, it does not appear to be the nurses’ fault. They can-not help it either.
“…Well, the problem is they don’t have enough staff. There’d be less problems if there was more
staff, they’d be less cranky...”
“…If you have to use the bathroom or something like that, it can take quite a while for someone
to come and help you. But I know that there’s a shortage of staff everywhere, it’s not their fault…”
Dealing with perceived discrepancies: establishing priorities. Some patients discover both their
suppositions of competent hospital care and human interactions with nurses are not met. One patient
declares he called the nurse because his neighbour was unwell. The nurse did not answer the call until
Chapter IV
106
half an hour later and when he talked to her about the long waiting time, she told him to be more polite.
When he discussed this experience further, he said he found the long waiting time worse than the
nurse’s retort. The fact it took half an hour to answer calls, was more important and serious to him.
Another patient told a nurse her drip kept getting infected. She knew from a previous stay on another
ward that a special lock could avoid needing a new drip every time it got infected. She further narrates
the nurse waved her aside and said they did not have time for it. The patient described she feels more
strongly about not getting the special lock than she does about the nurse’s rude reply. When judging
what is worst, patients consider what has the biggest impact or is most relevant to them personally. Not
having human interactions is thought to be less important than not receiving competent care. The worst
is whatever is most threatening on a personal level. A quadriplegic woman illustrates this.
“…If they’re late or cranky or whatever. Well, small things like that, I won’t react, but if it concerns
me personally, I will do something, if I know it’s not right…”
Patients feel annoyed when they do not experience human interactions in nurse – patient relationships
but they consider it inconceivable when they feel nurses’ expertise is of a questionable level.
3.4. | Integration: What (exactly) is transgressive (behaviour)?
Patients can report to be ‘satisfied’ while there is a complex underlying process of being confronted and
dealing with negative experiences about hospital care and nurse – patient relationships. Patients have
an implicit framework of suppositions. Based on this framework, hospital care and nurse – patient
relationships are evaluated. The framework generates implicit assumptions or ideas about hospital care
and nurse – patient relationships. Patients envisage receiving competent care and having human
interactions with nurses. These suppositions are considered to be self-evident and logical. Patients do
not have second thoughts about these suppositions. Both the framework and suppositions appear to be
implicit. They are not discussed with nurses and patients are not aware of these assumptions until they
experience envisaged care or nurse – patient relationships are not met in the perceived reality.
Experiencing these discrepancies gives rise to a process of adaptation. Consciously or otherwise,
patients feel bound to act on those discrepancies. It is both a cognitive and emotional process where
discrepancies give rise to an adjustment of assumptions or behaviour. This adjustment results in patients
becoming more vigilant or assertive to bring up questionable expertise in contact with nurses. Other
patients are more likely to adjust their expectations and no longer think human interactions with nurses
Patients’ perceptions of transgressive behaviour
107
are self-evident. These patients make excuses or look outside the nurses’ responsibility for causes of
negative experiences. Consequently, when pointing out the ‘worst’ part of a negative experience,
patients attach great importance to nurses’ expertise. They find it annoying to feel not treated in a human
way but it is minimized and put into perspective more quickly. Errors or questionable competencies of
nurses are considered to be inconceivable and are not as easily minimized or excused. A comparative
assessment is made to decide which factor affects patients most, personally or health-wise. Although
rude replies are annoying, they are less disturbing than professional errors with potentially major
consequences.
Due to the framework of suppositions and the process of adjustment in case experiences do not
correspond with assumptions, experiences of transgressive behaviour are put into perspective.
Whenever patients describe experiences of transgressive behaviour, the transgressive aspect of it is
mostly subjective. It is difficult to make objective determinations of what can and cannot be classified as
transgressive behaviour. Because of the process of adjustment, patients will tone down their opinion
about incidents that were experienced as transgressive. By making excuses, nurses are no longer the
cause of problems. By searching for solutions on their own, patients no longer need to address nurses
in case of problems. Experiences of transgressive behaviour are ‘addressed’ by the patient. This might
explain why patients’ ‘satisfaction’ was emphasized at the beginning of the interviews and incidents of
transgressive behaviour were voiced only gradually.
4. | Discussion
The study sought to better understand which nurse behaviour is experienced as transgressive by
patients and what constitutes this perception. The findings demonstrate that behaviour in itself does not
determine ‘what’ is experienced as transgressive. We described an underlying process patients go
through when interacting with nurses and how perceptions of transgressive behaviour can take place or
evolve in these interactions. Present findings demonstrate that patients employ a framework which leads
to implicit suppositions about professional care in the hospital and personal care relationships with
nurses. This framework generates ideas on how competent and skilled professional caregivers will be
and how relationships with nurses will be normal human interactions. Subsequently, a process of
adaption is employed when discrepancies are felt between these suppositions and the experienced care
or care relationship.
Chapter IV
108
4.1. | Interpretation and context of the results
The first major supposition to encounter competent and skilled professional caregivers might be
underpinned by a feeling of basic trust in nurses as professionals. A conceptual understanding of trust
and trustworthiness in nursing is provided by Dinç and Gastmans (2012). As a relational phenomenon,
impersonal trust in nurses is understood as having trust in nurses because institutions regulate practices
and endorse trustworthiness of professional activities (Dinç & Gastmans, 2012). Hence, expecting
competent professional care might be based on trust in nurses’ professional dispositions and
competencies as they are part of professional institutions. Likewise, competence adequacy of nurses
was identified as a normative expectation of patients in a grounded theory study on the meaning of
dissatisfaction of healthcare (Coyle, 1999a; Coyle, 1999b). Competence inadequacy, suggested as a
professionals’ lack of training, knowledge and expertise, accounted for an important untoward
experience of healthcare (Coyle, 1999a; Coyle, 1999b). Our findings demonstrate how perceiving
nurses’ competence inadequacy brought some patients to become alert or to adopt a sceptical attitude
towards nurses’ professional competences. Furthermore, experiences of competence inadequacy seem
to influence impressions of subsequent healthcare encounters. This notion is emphasized by our
findings as patients who had previous experience in healthcare, found their experiences empowering to
bring up untoward needs in contact with nurses.
The second major supposition is obtaining normal human interactions in care relationships with nurses.
When patients are admitted to a hospital, it is plausible they feel anxious and vulnerable. These feelings
are likely to increase because of unpleasant anxiety-provoking experiences commonly encountered in
hospitals (Winstanley, 2005). Hospitalization usually involves enforced confinement, a loss of privacy
and embarrassing situations, all of which might induce or exacerbate anxiety (Winstanley, 2005).
Inherent asymmetry in nurse – patient relationships might influence patients’ vulnerability and anxiety.
Power imbalances in nurse – patient relationships are found to contribute and increase patients’
vulnerability and dependency (Carter, 2009). Experiencing vulnerability and anxiety might impinge why
patients search for normal human interactions with nurses. Being seen as individuals or as human
beings might alleviate feelings of vulnerability of people who are or become recipients of healthcare
(Sellman, 2005).
Our findings demonstrate how patients deal with an untoward need for normal human interactions with
nurses. Although patients described nurses to have a primarily task-oriented approach, little attending

Patients’ perceptions of transgressive behaviour
109
behaviour and little acknowledgement of patients’ appraisal about illness or health; they were not
inclined to blame nurses. They adjusted and lowered their expectations towards nurses. A qualitative
study on patients’ experiences of nurse–patient communication confirms this notion partially. Patients
described nurses to be more concerned with completing tasks than talking to them and some patients
were frustrated and felt nurses did not care about them as individuals (McCabe, 2004). However, as our
findings also indicate, nurses were not blamed for this. Our findings show how patients make excuses
or minimize their expectations towards nurses. McCabe (2004) found similar results. Although patients
indicated they would like to be treated as individuals, they did not blame nurses and attributed nurses’
poor communication skills to the idea nurses were ‘too busy’ (McCabe, 2004). Blaming factors outside
of nurses’ responsibility or minimizing expectations towards nurses, is also seen in acutely ill older
patients. Patients ‘managed’ their relationship with nurses by showing concern for the busy, time-
pushed, emotionally exhausted nurses, by being grateful, and by trying to be a ‘good patient’ (Maben et
al., 2012). Maben et al. (2012) posit how this results in a lack of complaint, and satisfaction with care
based on low expectations. As a patient in the study of Maben et al. (2012) explained, ‘she did not want
to be seen as someone who is complaining’. Our finding that patients were inclined to emphasize
satisfaction with care during the first moments of interviews might be a similar finding. Patients adjust
and lower expectations, thus avoiding the need to complain. Stories of transgressive behaviour were
only gradually and cautiously formulated when asked to elaborate on experiences in care relationships.
This finding might show the relative meaning of patient satisfaction surveys. Patients can give positive
evaluations of quality of care while they have negative experiences in healthcare. Consequently, there
are differences between experiences reported in public accounts (for instance in questionnaires) and
those reported in personal accounts (during an interview). Moreover, the process of adjusting
expectations and searching for own solutions for untoward needs, might mitigate or diminish the need
for formal reporting of complaints. Simultaneously, the complex process of perceiving transgressive
behaviour demonstrates how these experiences are not easily articulated as formal complaints as they
are primarily grounded in nurse – patient interactions and dynamics of care relationships.
4.2. | Limitations
A limitation is the cross-sectional design. Patients were interviewed during or shortly after their hospital
admission. A longitudinal approach by interviewing patients multiple times during hospital admissions,
would allow an understanding of how perceptions might alter during hospital admissions. Further
Chapter IV
110
research could adopt a longitudinal design which would elicit more clearly processes of adapting
cognitions and emotions in interactions with nurses.
5. | Conclusion
We gained an indication on how patients perceive transgressive behaviour and what processes underpin
these perceptions. Patients employ a framework of suppositions when they are admitted to the hospital.
They have certain ideas about professional care in the hospital and personal care relationships with
nurses. Due to patient’s adjustment of behaviour or expectations when assumptions are not met, it is
difficult for nurses to ascertain what problems patients experience. It is crucial that patients feel free to
talk about experienced discrepancies so these experiences might be explained, clarified or resolved. As
a nurse, it is vital to understand that patients might bring negative ‘baggage’ because of previous hospital
experiences. This entails the risk patients are more reluctant to access hospital care, trust nurses’
caregiving or talk about previous negative experiences. The findings also point out how some
expectations are ‘not negotiable’. Patients make efforts to understand and cope with experiencing not
being treated as human beings, but they are indignant when professional caregiving is experienced as
inadequate or of questionable expertise. Professional incompetence in a professional institution as a
hospital is inconceivable. This finding is important for nursing education as it points out interpersonal
communication skills and professional technical competences are both crucial. In addition, this study
shows that even in a topic as transgressive behaviour, usually associated with interpersonal
communication, professional technical nursing competencies cannot be seen as less important.
Patients’ perceptions of transgressive behaviour
111
REFERENCES
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Fischer, J.E., & Haug, H.J. (2007). Frequency and severity
of aggressive incidents in acute psychiatric wards in Switzerland. Clinical Practice and Epidemiology in Mental
Health, 3(30).
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Haug, H.J., & Fischer, J.E. (2008). Structured risk
assessment and violence in acute psychiatric wards: randomised controlled trial. The British Journal of Psychiatry,
193(1), 44–50.
Almvik, R., Rasmussen, K., & Woods, P. (2006). Challenging behaviour in the elderly: monitoring violent incidents.
International Journal of Geriatric Psychiatry, 21(4), 368–374.
Bruyneel, L., Tambuyzer, E., Coeckelberghs, E., De Wachter, D., Sermeus, W., De Ridder, D., Ramaekers, D.,
Weeghmans, I., & Vanhaecht, K. (2017). New Instrument to Measure Hospital Patient Experiences in Flanders.
International Journal of environmental research and public health, 14(11).
Carter, M.A. (2009). Trust, power and vulnerability: a discourse on helping in nursing. Nursing Clinic of North
America, 44(4), 393– 405.
Charmaz, K. (2008) Constructing Grounded Theory: A Practical Guide through Qualitative Analysis. Sage,
Thousand Oaks, CA.
Cominskey, C., Coyne, I., Lalor, J., & Begley, C. (2014). A national cross-sectional study measuring predictors for
improved service user outcomes across clinical nurse or midwife specialist, advanced nurse practitioner and control
sites. Journal of Advanced Nursing, 70(5), 1128–1137.
Coyle, J. (1999a). Understanding dissatisfied users: developing a framework for comprehending criticisms of health
care work. Journal of Advanced Nursing, 30(3), 723–731.
Coyle, J. (1999b). Exploring the meaning of ‘dissatisfaction’ with health care: the importance of ‘personal identity
treat’. Sociology of Health & Illness, 21(1), 95–124.
Coyle, J., & Williams B. (2001). Valuing people as individuals: development of an instrument through a survey of
person-centredness in secondary care. Methodological Issues in Nursing Research, 36(3), 450–459.
Dinç, L. & Gastmans, C. (2012). Trust and trustworthiness in nursing: an argument-based literature review. Nursing
Inquiry, 19(3), 223–237.
Draucker, C.B., Martsolf, D.S., Ratchneewan, R., & Rusk, T.B. (2007). Theoretical sampling and category
development in grounded theory. Qualitative Health Research, 17(8), 1137–1148.
Duxbury, J., Pulsford, D., Hadi, M., & Sykes, S. (2013). Staff and relatives’ perspective on the aggressive behavior
of older people with dementia in residential care: a qualitative study. Journal of Psychiatric and Mental Health
Nursing, 20(9), 792–800.
Chapter IV
112
Foster, C., Bowers, L., & Nijman, H. (2007). Aggressive behaviour on acute psychiatric wards: prevalence, severity
and management. Journal of Advanced Nursing, 58(2), 140–149.
Gerdtz, M.F., Daniel, C., Dearie, V., Permatunga, R., Bamert, M., & Duxbury, J. (2013). The outcome of a rapid
training program on nurses’ attitudes regarding the prevention of aggression in emergency departments: a multi -
site evaluation. International Journal of Nursing Studies, 50(11), 1434–1445.
Glaser, B.G., & Strauss, A. (1967). The Discovery of Grounded Theory. Adline Atherton, Chicago, IL.
Hahn, S., Zeller, A., Needham, I., Kok, G., Dassen, T., & Halfens, R.J.G. (2008). Patient and visitor violence in
general hospitals: a systematic review of the literature. Aggression and Violent Behavior, 13(6), 431–441.
Hahn, S., Müller, M., Needham, I., Dassen, T., Kok, G., & Halfens, R.J.G. (2010). Factors associated with patient
and visitor violence experienced by nurses in general hospitals in Switzerland: a cross-sectional survey. Journal of
Clinical Nursing, 19(23–24), 3535–3546.
Hahn, S., Hantikainen, V., Needham, I., Kok, G., Dassen, T., & Halfens, R.J.G. (2012). Patient and visitor violence
in the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey. Journal of
Advanced Nursing, 68(12), 2685–2699.
Hahn, S., Müller, M., Hantikainen, V., Kok, G., Dassen, T., & Halfens, R.J.G. (2013). Risk factors associated with
patient and visitor violence in general hospitals: results of a multiple regression analysis. International Journal of
Nursing Studies, 50(3), 374–385.
Hallberg, L.R.M. (2006). The ‘core category’ of grounded theory: making constant comparisons. International
Journal of Qualitative Studies on Health and Well-Being, 1(3), 141–148.
Howard, M., Fleming, M.L. & Parker, E. (2013). Patients do not always complain when they are dissatisfied:
implications for service quality and patient safety. Journal of Patient Safety, 9(4), 224–231.
Koekkoek, B., Hutschemaekers, G., van Meijel, B., & Schene, A. (2011). How do patients come to be seen as
‘difficult’?: a mixed-methods study in community mental health care. Social Science & Medicine, 72(4), 504–512.
Lehto, U., Helander, S., Taari, K., & Aromaa, A. (2014). Patient experiences at diagnosis and psychological well-
being in prostate cancer: a Finnish national survey. European Journal of Oncology Nursing, 19(3), 220–229.
Lincoln, Y.S., & Guba, E.G. (1985). Naturalistic inquiry. Sage, Beverly Hills, CA.
Liu, J. (2004). Concept analysis: aggression. Issues in Mental Health Nursing, 25(7), 693–714.
Liu, J., Lewis, G., & Evans, L. (2013). Understanding aggressive behaviour across the lifespan. Journal of
Psychiatric and Mental Health Nursing, 20(2), 156–168.
Maben, J., Adams, M., Peccei, R., Murrells, T., & Robert, G. (2012). ‘Poppets and parcels’: the links between staff
experiences of work and acutely ill older peoples’ experience of hospital care. International Journal of Older People
Nursing, 7(2), 83–94.
Patients’ perceptions of transgressive behaviour
113
McCabe, C. (2004). Nurse-patient communication: an exploration of patients’ experiences. Journal of Clinical
Nursing, 13(1), 41– 49.
McPherson, K.M., Kayes, N.K., Moloczij, N., & Commins, C. (2014). Improving the interface between informal carers
and formal health and social services: a qualitative study. International Journal of Nursing Studies, 51(3), 418–429.
Metzelthin, S.F., Daniëls, R., van Rossum, E., Cox, K., Habets, H., de Witte, L.P., & Kempen, G.I. (2013). A nurse-
led interdisciplinary primary care approach to prevent disability among community-dwelling frail older people: a
large-scale process evaluation. International Journal of Nursing Studies, 50(9), 1184–1196.
Morse, J.M., & Field, P.A. (1996). Nursing Research: The Application of Qualitative Approaches. London: Chapman
& Hall.
Nijman, H., Bowers, L., Oud, N., & Jansen, G. (2005). Psychiatric nurses’ experiences with inpatient aggression.
Aggressive Behaviour, 31(3), 217–227.
O’Connell, B., Young, J., Brooks, J., Hutchings, J., & Lofthouse, J. (2000). Nurses’ perceptions of the nature and
frequency of aggression in general ward settings and high dependency areas. Journal of Clinical Nursing, 9(4),
602–610.
Sellman, D. (2005). Towards an understanding of nursing as a response to human vulnerability. Nursing Philosophy,
6(1), 2–10.
Söderberg, S., Olsson, M., & Skär, L. (2012). A hidden kind of suffering: female patient’s complaints to Patient’s
Advisory Committee. Scandinavian Journal of Caring Sciences, 26(1), 144–150.
Spector, P.E., Zhou, Z.E., & Che, X.X. (2014). Nurse exposure to physical and nonphysical violence, bullying and
sexual harassment: a quantitative review. International Journal of Nursing Studies, 51(1), 72–84.
Trotter, R.T. (2012). Qualitative research sample design and sample size: resolving and unresolved issues and
inferential imperatives. Preventive Medicine, 55(5), 398–400.
Veneau, L., & Chariot, L. (2013). How do hospitals handle patients complaints? An overview from the Paris area.
Journal of Forensic and Legal Medicine, 20(4), 242–247.
Williams, B. (1994). Patient satisfaction: a valid concept? Social Science & Medicine, 38(4), 509–516.
Winstanley, S. (2005). Cognitive model of patient aggression towards health care staff: the patient’s perspective.
Work & Stress, 19(4), 340–350.
Winstanley, S., & Whittington, R. (2004). Aggression towards health care staff in a UK general hospital: variation
among professions and departments. Journal of Clinical Nursing, 13(1), 3–10.
Yang, L.Q., Spector, P.E., Chang, C.H., Gallant-Roman, M., & Powell, J. (2012). Psychosocial precursors and
physical consequences of workplace violence towards nurses: a longitudinal examination with naturally occurring
groups in hospital settings. International Journal of Nursing Studies, 49(4), 1091–1102.

Chapter IV
114
You, L.M., Aiken, L.H., Sloane, D.M., Liu, K., He, G.P., Hu, Y., Jiang, X.L., Li, X.H., Li, X.M., Liu, H.P., Shang, S.M.,
Kutney-Lee, A., & Sermeus, W. (2013). Hospital nursing, care quality and patient satisfaction: cross-sectional
surveys of nurses and patients in hospitals in China and Europe. International Journal of Nursing Studies, 50(2),
154–161.
Zengin, S., Al B., Yavuz, E., Kursunkoseler, G., Guzel, R., Sabak, M., & Yildirim, C. (2014). Analysis of complaints
lodged by patients attending a university hospital: a 4-year analysis. Journal of Forensic and Legal Medicine, 22,
121–124.
Nurses’ perceptions of transgressive behaviour
115
Chapter V.
NURSES’ PERCEPTIONS OF TRANSGRESSIVE BEHAVIOUR
IN CARE RELATIONSHIPS WITH PATIENTS
Tina Vandecasteele1,2, Bart Debyser2, Ann Van Hecke1,3, Tineke De Backer2, Dimitri Beeckman1,
Sofie Verhaeghe1,2
1 Department of Public Health, Faculty of Medicine and Health Sciences, University Centre for Nursing &
Midwifery, Ghent University, Ghent, Belgium.
2 Department Health care, VIVES University College, Roeselare, Belgium.
3 University Hospital Ghent, Ghent, Belgium.
Based on the article of Vandecasteele T., Debyser B., Van Hecke A., De Backer T., Beeckman D. &
Verhaeghe S. (2015) Nurses’ perceptions of transgressive behaviour in care relationsh ips: a qualitative
study. Journal of Advanced Nursing 71(12), 2786–2798.

Chapter V
116
Nurses’ perceptions of transgressive behaviour
117
Nurses’ perceptions of transgressive behaviour in care relationships: a qualitative
study
ABSTRACT
Aim. To acquire insight into the onset and meaning of transgressive behaviour from the perspective of
nurses.
Background. Patient aggression towards healthcare providers occurs frequently. Nurses in particular
are at risk of encountering aggressive or transgressive behaviour due to the nature, duration and
intensity of care relationships with patients. This study analysed nurses’ perspectives with regard to the
onset and meaning of transgressive patient behaviour in a general hospital setting.
Design. Qualitative research according to the grounded theory method.
Methods. Data were collected in 2011 through individual interviews with 18 nurses who were selected
using purposive and theoretical sampling.
Findings. Findings revealed that various nurse - patient interactions can result in episodes of
transgressive behaviour, depending on the interplay of determining and regulating factors which have
been identified at the patient, nurse and ward level. Experiences of transgressive behaviour are
influenced by the degree of control nurses experience over the provision of care; the degree of patient
acceptance of organizational and ward rules, the degree of gratitude and recognition expressed by the
patient and the extent of patient regard for the nurse as a person. Factors affecting transgressive
experiences were a trusting relationship between the patient and the nurse; the extent to which patient
perspectives are understood; the methods of managing transgressive behaviour; and the influence of
the team, head nurse and ward culture and habits.
Conclusions. The results of this study can support the development of nurses’ coping ability and self-
confidence to mitigate or prevent experiences of transgressive behaviour.
Keywords. Aggression, care relationship, general hospital, nurse–patient relationship, nurses, nursing,
qualitative research, transgressive behaviour, violence.
Chapter V
118
1. | Introduction
Patient aggression towards healthcare providers occurs frequently (Hahn et al., 2008; Hahn et al., 2012;
Spector, Zhou, & Che, 2014). Nurses are at especial risk due to the nature, duration and intensity of the
care relationship with patients (Gerberich et al., 2004; Abderhalden et al., 2007; Waschgler et al., 2013).
Reports on prevalence and incidence indicate that high percentages of nurses have been subjected to
patient aggression at some time (Hahn et al., 2012; Spector et al., 2014). Literature suggests there may
be substantial consequences from aggressive encounters, with negative implications for the personal
well-being and professional performance of care providers, patient outcomes and the quality of care
(Needham et al., 2005; Hahn et al., 2008).
1.1. | Background
Although patient aggression has been widely studied in recent decades, most of the research relates to
geriatric (Almvik, Rasmussen, & Woods, 2006; Duxbury, Pulsford, Hadi, & Sykes, 2013), emergency
(Gerdtz et al., 2013) and mental health settings (Abderhalden et al., 2007). Research on aggression in
general hospitals is limited (O’Connell et al., 2000; Wells & Bowers, 2002) and generalizing from specific
to universal settings is difficult.
Research on aggression in healthcare usually reports occurrence of aggression. This is performed by
measuring risk factors associated with patient aggression or violence (Hahn et al., 2010; Hahn et al.,
2013) or by surveys where nurses indicate to what extent they are exposed to specific physical, verbal
and non-verbal behaviours (Foster, Bowers, & Nijman, 2007; Abderhalden et al., 2008, Yang, Spector,
Chang, & Gallant-Roman, 2012). Comparing these results is challenging due to some methodological
and theoretical difficulties. For example, in several studies, the researchers assume that specific
behaviours are perceived as aggressive by definition. However, perceptions of what constitutes an
aggressive act can vary from person to person. There is little insight into how aggression is perceived,
what limits are exceeded for a situation to be experienced as aggressive and which factors influence
this process. Few studies situate aggression in the patient-nurse interaction (Nijman, Bowers, Oud, &
Jansen, 2005) or in relational environments in which aggression takes place. Furthermore, several
articles illustrate the problem of under-reporting of aggressive incidents (Chapman, Styles, Perry, &
Combs, 2010; Gates, Gillespie, & Succop, 2011). This indicates that the aetiology and seriousness of
the phenomenon of aggression is not yet fully understood, making generalizations about the
Nurses’ perceptions of transgressive behaviour
119
phenomenon of aggression in nursing care on general hospital wards difficult. This study attempts to
meet present difficulties in existing literature.
As a first step, an unambiguous operationalization of aggression was necessary. In the literature,
different definitions exist, highlighting different elements of the concept of aggression (Liu, 2004; Nijman
et al., 2005; Liu, Lewis, & Evans, 2013). These elements have been merged into the following broad
definition of aggression: Inflicting harm to material or to another person by transgressing the other
person’s limits, standards or norms. This is expressed by verbal or physical aggression, intimidation, or
threats to objects. This study focused on the “transgressing of limits, standards, or norms”. The concept
of aggression was operationalized using the broader term ‘transgressive behaviour’, since the
perception of an aggressive act is an internal personal construct and varies among individuals
(O’Connell et al., 2000). Use of this term allows an individual interpretation of when and what limits are
exceeded without defining them in advance. In literature, ‘transgression’ is common ly combined with
moral or ethical values or principles as boundaries. However, this conceptualization already presumes
certain moral or ethical suppositions which have to be crossed for a moral of ethical transgression to
occur. In the present study, we did not define or expect particular ethical or moral principles to be at
stake when perceiving transgressive behaviour. We started inductively with exploring the understanding
of what is transgressive and what are underlying processes in this perception. The interpretation of
limits, how they are exceeded, the perceived seriousness of the situation and the processes involved in
this interpretation, were not determined in advance. Furthermore, transgressive behaviour is situated in
the nurse - patient relationship and the nurse – patient interaction. To fully understand this interaction,
both nurses and patients were included in the overall study. The overall aim of the study is to provide a
better understanding of perceptions of transgressive behaviour in care relationships from the
perspective of nurses. This study is part of a larger study where patients were also interviewed regarding
experiences related to transgressive behaviour. These results will be described in another manuscript.
Subsequent combining both perspectives in an integrative analysis will provide an overall perspective
of transgressive behaviour in care relationships.
Chapter V
120
2. | The study
2.1. | Aim
This study sought to answer two questions from a nurse’s perspective:
What behaviour in the patient–nurse relationship is perceived as transgressive? and;
What processes or mechanisms influence perceived seriousness of transgressive behaviour?
2.2. | Design
A qualitative study according to the grounded theory with constant comparison was conducted to
understand and explain nurses’ perceptions of transgressive behaviour in care relationships with
patients (Glaser & Strauss, 1967; Morse & Field, 1996; Hallberg, 2006).
2.3. | Sample
Participants were recruited in December 2011. The study was conducted in six wards located in two
general hospitals in Belgium. These hospitals serve both rural and urban communities situated in West
Flanders, a Dutch-speaking Belgian province. Included wards had a diagnostic, medical, geriatric, or
surgical focus. Heads of departments and head nurses were informed about the study. The researchers
informed the nurses about the study aim, the procedure of the study, and talked about the practical
considerations.
A purposive sample of experienced nurses who agreed to participate was selected for variety in age,
educational degree and work experience. This recruitment procedure was designed to lead to situational
diversity in experiences with regard to transgressive behaviour. To broaden initial insights and to select
participants for subsequent interviews, theoretical sampling was used (Draucker, Martsolf,
Ratchneewan, & Rusk, 2007). After nine interviews, further interviews were thus carried out with male
and female nurses from another hospital to assess the influence of hospital culture on perceptions of
transgressive behaviour. Theoretical sampling was also adopted to search for wards with a strict regime
or with a loosely structure to assess the influence of ward organization on perceptions of transgressive
behaviour.
Eighteen nurses were interviewed. Sample size was determined by data saturation, when no further
information was obtained and when connections among emerging concepts were clear. Saturation was
reached after 15 interviews. A subsequent three interviews did not lead to further deepening of the
analysis and as such validated the saturation. Table 1 summarizes the characteristics of the 18 nurses
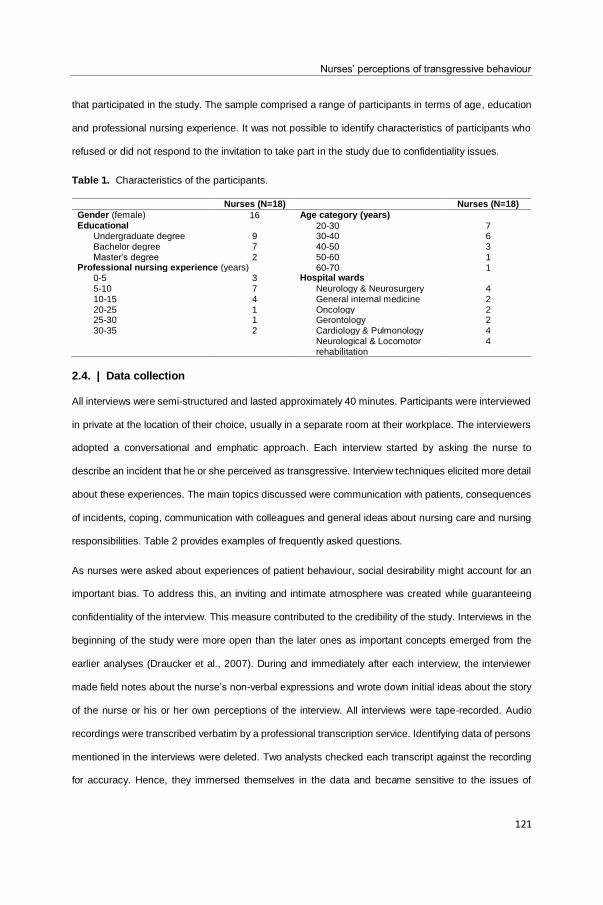
Nurses’ perceptions of transgressive behaviour
121
that participated in the study. The sample comprised a range of participants in terms of age, education
and professional nursing experience. It was not possible to identify characteristics of participants who
refused or did not respond to the invitation to take part in the study due to confidentiality issues.
Table 1. Characteristics of the participants.
Nurses (N=18) Nurses (N=18)
Gender (female) 16 Age category (years) Educational 20-30 7
Undergraduate degree 9 30-40 6 Bachelor degree 7 40-50 3 Master’s degree 2 50-60 1
Professional nursing experience (years) 60-70 1 0-5 3 Hospital wards
5-10 7 Neurology & Neurosurgery 4 10-15 4 General internal medicine 2 20-25 1 Oncology 2 25-30 1 Gerontology 2 30-35 2 Cardiology & Pulmonology 4
Neurological & Locomotor rehabilitation
4
2.4. | Data collection
All interviews were semi-structured and lasted approximately 40 minutes. Participants were interviewed
in private at the location of their choice, usually in a separate room at their workplace. The interviewers
adopted a conversational and emphatic approach. Each interview started by asking the nurse to
describe an incident that he or she perceived as transgressive. Interview techniques elicited more detail
about these experiences. The main topics discussed were communication with patients, consequences
of incidents, coping, communication with colleagues and general ideas about nursing care and nursing
responsibilities. Table 2 provides examples of frequently asked questions.
As nurses were asked about experiences of patient behaviour, social desirability might account for an
important bias. To address this, an inviting and intimate atmosphere was created while guaranteeing
confidentiality of the interview. This measure contributed to the credibility of the study. Interviews in the
beginning of the study were more open than the later ones as important concepts emerged from the
earlier analyses (Draucker et al., 2007). During and immediately after each interview, the interviewer
made field notes about the nurse’s non-verbal expressions and wrote down initial ideas about the story
of the nurse or his or her own perceptions of the interview. All interviews were tape-recorded. Audio
recordings were transcribed verbatim by a professional transcription service. Identifying data of persons
mentioned in the interviews were deleted. Two analysts checked each transcript against the recording
for accuracy. Hence, they immersed themselves in the data and became sensitive to the issues of
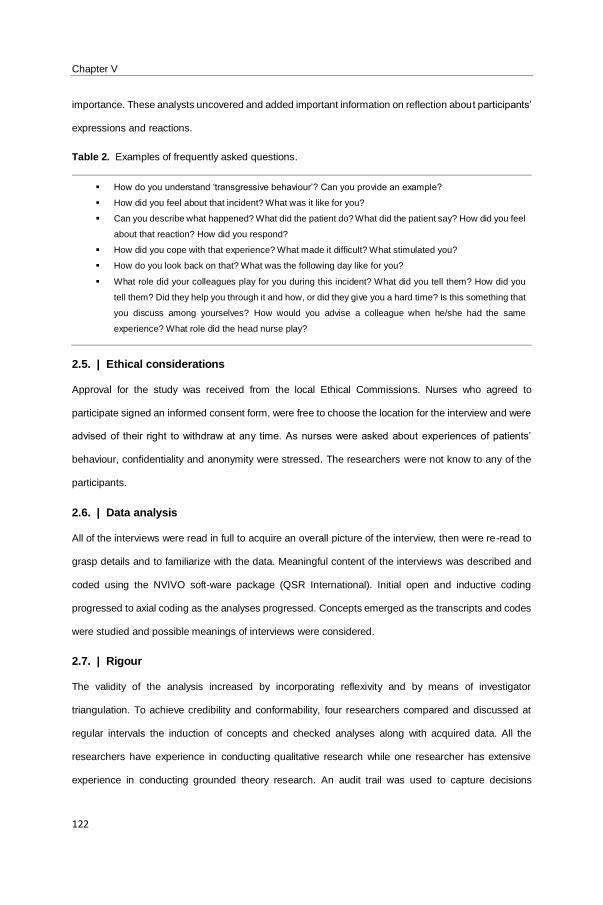
Chapter V
122
importance. These analysts uncovered and added important information on reflection about participants’
expressions and reactions.
Table 2. Examples of frequently asked questions.
How do you understand ‘transgressive behaviour’? Can you provide an example?
How did you feel about that incident? What was it like for you?
Can you describe what happened? What did the patient do? What did the patient say? How did you feel
about that reaction? How did you respond?
How did you cope with that experience? What made it difficult? What stimulated you?
How do you look back on that? What was the following day like for you?
What role did your colleagues play for you during this incident? What did you tell them? How did you
tell them? Did they help you through it and how, or did they give you a hard time? Is this something that
you discuss among yourselves? How would you advise a colleague when he/she had the same
experience? What role did the head nurse play?
2.5. | Ethical considerations
Approval for the study was received from the local Ethical Commissions. Nurses who agreed to
participate signed an informed consent form, were free to choose the location for the interview and were
advised of their right to withdraw at any time. As nurses were asked about experiences of patients’
behaviour, confidentiality and anonymity were stressed. The researchers were not know to any of the
participants.
2.6. | Data analysis
All of the interviews were read in full to acquire an overall picture of the interview, then were re-read to
grasp details and to familiarize with the data. Meaningful content of the interviews was described and
coded using the NVIVO soft-ware package (QSR International). Initial open and inductive coding
progressed to axial coding as the analyses progressed. Concepts emerged as the transcripts and codes
were studied and possible meanings of interviews were considered.
2.7. | Rigour
The validity of the analysis increased by incorporating reflexivity and by means of investigator
triangulation. To achieve credibility and conformability, four researchers compared and discussed at
regular intervals the induction of concepts and checked analyses along with acquired data. All the
researchers have experience in conducting qualitative research while one researcher has extensive
experience in conducting grounded theory research. An audit trail was used to capture decisions
Nurses’ perceptions of transgressive behaviour
123
regarding sampling and to describe the structure and rationale of meanings assigned to data, which
strengthened dependability (Lincoln & Guba, 1985). Data collection and data processing were executed
iteratively until data saturation was reached (Charmaz, 2008).
3. | Results
Nurses described and elaborated on diverse incidents in patient contact which were experienced as
transgressive behaviour. Although nurses described different experiences of perceived transgressive
behaviour, the analysis converged around a consistent set of factors that impinged the perception of
transgressive behaviour. Nine factors were identified. These factors work in two distinct manners. Four
factors have an outspoken influence on the onset of the perception of transgressive behaviour
(determining factors), five factors indirectly determined the perceived seriousness of transgressive
behaviour (regulating factors). These nine factors will be described to construct how perceptions of
transgressive behaviour emerge.
3.1. | Determining factors
The first four factors are determining factors. These factors are factors which, at a given moment and in
a particular situation, encompass a limit to be exceeded, causing specific behaviour to be perceived as
transgressive. The following dimensions were identified as determining factors: The degree of control
that nurses experience over the provision of care, the perceived degree of patient acceptance of
organizational and ward rules, the perceived degree of gratitude and recognition expressed by the
patient and the perceived extent of patient regard for the nurse as a person.
The perceived degree of control that nurses experience over the provision of care and perceived
degree of patient acceptance of organizational and ward rules. Nurses regard the role of a good
nurse as providing proper care to patients. Consequently, they consider it their responsibility to ensure
that the patient receives proper care. To achieve this within a limited time frame, nurses feel the need
to control the organization of care.
“…What is it that makes you satisfied about your work? [interviewee]: The feeling that you can
provide the care like you want to provide, because that is not always possible due to lack of
time…”
Chapter V
124
Subsequently, the need to control provision of care leads to the expectation of a complementary attitude
from patients and their acceptance of organizational and ward rules. Patient behaviour perceived as
difficult or unpredictable is experienced by nurses as transgressive because it disturbs the performance
of care activities and results in a sense of loss of control over the provision of care:
“…People claim and expect too much. There are things they can do themselves, they call to get
their glasses filled with water and you have to go quickly whilst they can do it themselves…”
“…They expect you to be there immediately because they feel a little pain. You don’t get any
time while we already work so fast. There is no patience. And they expect us to do things they
can do themselves…”
The organizational and ward rules that nurses define as important and use as a framework for the
performance of their care activities, appear to be mostly self-imposed. They are not described as a
prerequisite or as dictated in a ward policy. Nurses describe how they try to maintain a planning of their
provision of care. One nurse described she wanted to finish hygienic patient care by 10 o’clock in the
morning, so she would have time to drink some coffee and subsequently have a quiet moment to fill in
patient files. This planning was not imposed by the ward or the organization. However, when patients
asked something interrupting this self-imposed planning, perceptions of transgressive behaviour
appeared to emerge more rapidly.
The perceived degree of gratitude and recognition expressed by the patient and the perceived
extent of patient regard for the nurse as a person. In their personal interpretation of the care
relationship, nurses expressed a need for implicit and explicit recognition of their personal and
professional roles. Situations were perceived as transgressive when nurses felt undervalued for their
position and expertise:
“…I do my best and the family and patient think, I don’t work enough. I’m not fast enough,
patients are not well cared for, they have to sit up for a long time… While you know you did
everything you could do… That really hurts...”
Several nurses described how they wanted to be seen by patients as a person without being connected
to professional tasks. Caregiving provided nurses a feeling of self-worth and satisfaction, a feeling that
was threatened when patients did not provide confirmation of proper care. Obtaining gratitude and
Nurses’ perceptions of transgressive behaviour
125
recognition from patients can thus be part of the expectation of patient respect for the way nurses provide
care:
“…Particularly the way people state things, it is demeaning: ‘You are paid to do this’…”
“…Sometimes, we do have patients who are grateful. A woman for example said this morning
that we were so kind. That experience is lovely, it makes the whole day better...”
The lack of recognition of the personal and professional role of the nurse was a determining factor for
the onset of perceived transgressive behaviour. Nurses reported that when they did not feel appreciated
in their personal and professional roles, they valued the caring aspect of the relationship to a lesser
degree, distancing themselves from the patient. As a consequence, simply completing the expected
tasks and maintaining control over the provision of care became more important.
3.2. | Regulating factors
Although these determining factors can result in an experience of transgressive behaviour, several
factors regulate the meaning of these experiences. These factors are regulating factors. Regulating
factors reinforce or mitigate a nurse’s experience and the perceived seriousness of transgressive
behaviour. Two levels were identified at which these factors manifest: The nurse level and the
organizational level. At the nurse level, a trusting relationship between patients and nurses, the extent
to which patient perspectives were understood and the way transgressive behaviour was managed,
were directly regulating factors influencing experiences of transgressive behaviour. At the organizational
level, the role of the team and head nurse and the influence of ward culture and habits, were indirectly
regulating factors influencing experiences of transgressive behaviour.
Nurse level – trusting relationship between patients and nurses and the extent to which patient
perspectives are understood. When nurses knew the patient in a more personal way and understood
individual needs, they perceived transgressive behaviour as less serious. The existence of a trusting
relationship mitigated the experience. Likewise, when patient behaviour could be attributed to external
factors, transgressive behaviour was experienced as less serious:
“…You build a band, family members and patients tell you something and you tell something.
By opening yourself up, you experience less transgressive behaviour…”
“…You won’t experience transgressive behaviour of patients when you have a good connection
with them…”
Chapter V
126
The existence of a trusting relationship with the patient implies the ability to understand patients’
perspectives and needs. Subsequently, nurses perceived patient behaviour in a contextual manner
which ‘normalized’ the meaning or mitigated the seriousness of potentially transgressive behaviour:
“…To us, 5 minutes is not long, but if you urgently need to go to the toilet and you have to wait
five minutes, I imagine it is absolutely not pleasant…”
Nurse level – the way transgressive behaviour is managed. The way nurses managed experiences
of transgressive behaviour was a third regulating factor. Different methods are employed to prevent or
respond to transgressive behaviour to provide proper care. Nurses had preferred, individual ways of
dealing with transgressive behaviour, which were employed in every situation and not differentiated
according to patients. Nurses who felt they lacked the ability to deal with transgressive behaviour
perceived it as more serious and disturbing. Consequently, coping styles had an impact on the
perception of seriousness of transgressive behaviour. The most common style was to avoid interaction
with the patient. Nurses reported that they knew what they should not do when confronted with
transgressive behaviour, but did not know what they were supposed to do. As a result, they remained
silent, left the room, avoided the patients, or tried not to enter the patient’s room alone:
“…It is creativity. A patient did not want to take his medication and got angry, so I tried to tempt
him with a pudding or a drink. It is a way of avoiding contact about his medication by using
concrete things, in order not to provoke…”
“…She was always angry with us. So I washed her as early as possible so she was still half-
asleep. So by the time she’s fully awake, I was already gone…”
Organizational level – the role of the team and head nurse. The influence of nursing team members
and the head nurse was a regulating factor that mitigated or exacerbated experiences of transgressive
behaviour. Nurses felt supported by venting their experiences with colleagues. Colleagues might look
for solutions or offer to take over care tasks so that the nurse was no longer confronted with
transgressive behaviour. Because of this support, incidents were perceived as less oppressive. Head
nurses were also considered to be in a supportive role since they were perceived as more empowered
to put an end to transgressive behaviour of patients. Support from the team and head nurse took on a
regulating role regarding experiences of transgressive behaviour consistent with the commonly used
method of evading interaction at the nurses’ level:
Nurses’ perceptions of transgressive behaviour
127
“…I did not know what to do. So I went to my colleague and she said she would handle it. So
she addressed the patient and his family…”
Organizational level – influence of ward culture and habits. Ward standards and habits were a
second regulating factor in experiencing transgressive behaviour. In general, nurses tried to avert
transgressive encounters and in wards or organizational settings where a task-oriented approach was
valued, this method of handling transgressive experiences seemed justified. Individual nurse’s
perceptions concerning transgressive behaviour were shaped by and became similar to the perceptions
of other nurses in the same ward, including behaviour perceived as transgressive, aspects influencing
these perceptions and consequences of these perceptions on relationships with patients:
“…So I said it to my colleague and she asked me what I said to the patient. And she responded
saying ‘you were right to act like that, there was no other way’. So I knew I did the right thing…”
Although different wards were included in the study, no influence of the specific ward characteristics
was found on perceptions of transgressive behaviour. However, nurses did seem to adapt their coping
styles to the culture of a particular ward. New nurses who start working on a ward go through a
socialization process where ward culture and habits influenced personal perspectives on transgressive
behaviour and how to deal with it. New nurses even renounced their own, perhaps more effective, coping
styles to adapt to ward habits:
“…Here we can witness this ¨[author’s note: On some wards, nurses’ names could not be
mentioned in patient contact]: ‘I do not say my name,’ we are afraid that we would be held
accountable if something goes wrong. But I do not really understand, how can it hurt somebody
if they were to know my name?...”
“…This patient got sedatives quickly when he was restless. But the reason for his behaviour is
the fact that he is in a hospital. He doesn’t know anybody and sees white aprons. He does not
see that at home. So medication is administered too quickly. But that is common here…”
The process extending throughout this study and connecting these factors, follows a three-phase model.
Chronologically, phase I starts with an incident that may induce an experience of transgressive
behaviour. Four factors determined this perceived exceeding of a limit. The exceeding of a limit is
followed by phase II, ‘Giving meaning to the incident’. In the second phase, nurses acknowledge the
exceeded limit and give meaning to this perception. Five factors regulate the perceived seriousness
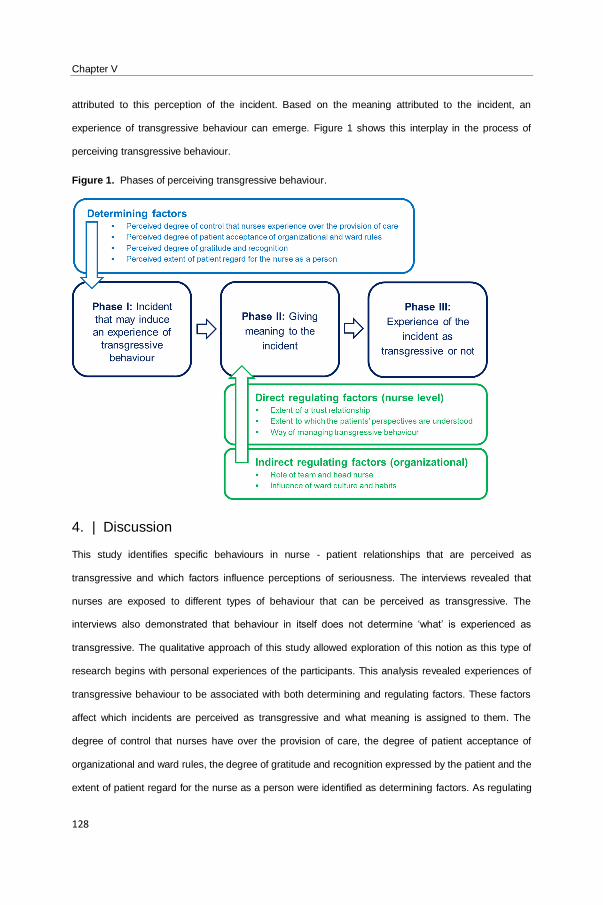
Chapter V
128
attributed to this perception of the incident. Based on the meaning attributed to the incident, an
experience of transgressive behaviour can emerge. Figure 1 shows this interplay in the process of
perceiving transgressive behaviour.
Figure 1. Phases of perceiving transgressive behaviour.
4. | Discussion
This study identifies specific behaviours in nurse - patient relationships that are perceived as
transgressive and which factors influence perceptions of seriousness. The interviews revealed that
nurses are exposed to different types of behaviour that can be perceived as transgressive. The
interviews also demonstrated that behaviour in itself does not determine ‘what’ is experienced as
transgressive. The qualitative approach of this study allowed exploration of this notion as this type of
research begins with personal experiences of the participants. This analysis revealed experiences of
transgressive behaviour to be associated with both determining and regulating factors. These factors
affect which incidents are perceived as transgressive and what meaning is assigned to them. The
degree of control that nurses have over the provision of care, the degree of patient acceptance of
organizational and ward rules, the degree of gratitude and recognition expressed by the patient and the
extent of patient regard for the nurse as a person were identified as determining factors. As regulating

Nurses’ perceptions of transgressive behaviour
129
factors, the extent of the trusting relationship between patients and nurses, the extent to which the
patient’s perspective is understood and honoured, the way transgressive behaviour is managed by
nurses and the roles of the nursing team and head nurse and ward culture and habits, were identified.
These factors are connected to one another and are responsible for dynamics in maintaining, reinforcing
or decreasing experiences of transgressive behaviour.
4.1. | Interpretation and context of the results
Nurses consider it their duty to provide good care. As a consequence, nurses strive to establish and
maintain control over the provision of care. This striving seems to imply a dedication to finalize tasks
that form a direct requirement for the continuation of care. This striving seems to have two effects. On
the one hand, patients are expected to conform to ward rules and the task division. On the other hand,
more specific nursing tasks or demands (e.g. patient administration, distribution of meals, administration
of medication) are experienced as more important than prevention, recognition, or management of
transgressive behaviour. This task-oriented working context might exacerbate experiences of
transgressive behaviour since transgressive behaviour is a disruptive event interfering with the feeling
of control over the care organization. Previous studies have confirmed this idea, as heavy workloads
and consequent lack of time on the part of nurses can contribute to patient aggression (Zernike &
Sharpe, 1998; Camerino et al., 2008; Morgan et al., 2008). Both factors can reinforce the need for nurses
to feel in control of the provision of care.
Participants reported that their self-esteem was associated with job identity. Lack of confirmation of
professional performance had a negative impact on personal well-being. Similar findings were described
in a qualitative study exploring satisfaction in nursing in the context of staffing shortages. Two of the
intrinsic dimensions of work satisfaction were found to be ‘touching the lives of patients through their
caring work,’ and ‘having pride in acquired skills and competencies’ (Morgan & Lynn, 2009). Nurses
want to feel valued by patients in a personal way and want to be respected for their professional
contribution to patient care at the same time. This finding suggests that dependence on patient
confirmation increases the risk that experiences of transgressive behaviour are perceived more readily
when confirmation is lacking.
Participants in this study responded to experiences of transgressive behaviour with avoidance. A study
on the interpersonal skills that nurses adopt, identified different types of communication styles, including
authoritative interventions (e.g. prescribing, instructing, confronting) and facilitating interventions (e.g.
Chapter V
130
catharsis and stimulating reflection, offering support) (Burnard & Morrison, 2005). Nurses in that study
primarily employed authoritative interventions and rarely attempted facilitating interventions (Burnard &
Morrison, 2005). The current study findings are comparable, as participants scarcely used facilitating
communication styles; there were few attempts to understand (the context of) patient behaviours and
the nurse’s own share in incidents was not considered. This might be explained by the way in which
nurses perceive aggressive behaviour. Dunn, Elsom, & Cross (2007) argue that psychological
constructs of self-efficacy and locus of control are closely related to the nurses’ ability to effectively
manage aggressive incidents. Locus of control concerns personal attributions of life events to either
internal or self-directed actions, or to external or environmental factors. In this study, nurse perceptions
of transgressive behaviour might be influenced by their locus of control. Nurses with a strong external
locus of control might believe experiences of transgressive behaviour derive primarily from patient
behaviour and feel victimized because of these experiences. This notion might justify authoritative
interventions. Likewise, nurses with a strong internal locus of control who believe experiences derive
from their own actions, might be inclined to perceive transgressive behaviour as a normal human
reaction arising from a specific interaction. Subsequently, more facilitative interventions might be used.
When there is no catharsis, no exploration or reflection on transgressive behaviour, or when avoidance
is used, it increases the risk that the experience and seriousness of transgressive behaviour will be
amplified.
There is an additional risk that nurses alienate from the patient’s perspective, illustrated by the
identification of a regulating factor: nurse understanding of the patient’s perspective mitigated
perceptions of transgressive behaviour. When patients’ perspectives are not understood, an ‘us and
them’ viewpoint might be adopted, increasing the risk of alienation and perceptions of transgressive
behaviour.
The findings indicate that nurses rarely give feedback to patients on experiences of transgressive
behaviour. Nurses must acquire the appropriate communication skills to do so. Although literature points
out that education and professional experience influence the perceived prevalence of patient and visitor
violence (Estryn-Behar et al., 2008; Hahn et al., 2010; Hahn et al., 2012), present analysis of findings
did not demonstrate a major influence of experience and education on the perception of transgressive
behaviour. However, present findings indicate how the perception of having a ‘good’ way of managing
transgressive behaviour mitigated perceived seriousness of transgressive behaviour. As this is a

Nurses’ perceptions of transgressive behaviour
131
perception, it is not clear whether perceived ‘good’ ways of managing transgressive behaviour is a result
of the professional nursing experience or education.
Supporting language and communication skills of nurses are aspects frequently researched, both on
the level of the individual nurse (Boscart, 2009), and on the level of wards (Björkdahl, Hansebo, &
Palmstierna, 2013; McLaughlin, Pearce, & Trenoweth, 2013). Our findings support the notion to
intervene on the level of the ward since colleagues and ward culture influenced individual nurse’s
perceptions. Together with colleagues, nurses searched for ways to avoid perceived transgressive
behaviour or sought confirmation for their reactions. The team encouraged nurses to vent emotions or
find support in other ways. This finding is consistent with literature (Estryn-Behar et al., 2008; Zeller et
al., 2011).
4.2. | Limitations
There might exist a selection bias in that we only interviewed Dutch-speaking nurses and we recruited
in two large general hospitals. Therefore, we do not know whether our results can be generalized to not
native Dutch-speaking nurses or nurses working in University hospitals.
4.3. | Implications for practice
Present findings reveal self-imposed rules and standards nurses use to plan their own care leading to a
specific expected accepting attitude of patients of this self-imposed care planning. It is important that
head nurses or nurse managers support nurses in making these self-imposed rules or standards more
explicit and support nurses to become more aware of the consequences and risks of these self-imposed
planning. It is also of particular importance that new graduate nurses are vigilantly empowered and
stimulated to reflect on the nurse - patient relationship, understand the patient perspective and provide
patient-oriented care. Literature on the transition process of new graduate nurses to practicing nurses
demonstrates how this is a major challenge (Feng & Tsai, 2012). However, literature suggests that short-
term education sessions where nurses are supported in reflecting on the interaction with patients and
encouraged to understand the patient’s perspective can be sufficient to obtain a reflective and patient-
oriented interaction (Boscart, 2009). Reflecting in group on experiences of transgressive behaviour while
contemplating the interaction with patients, understanding the patient’s behaviour and the regulation of
personal emotions, are interventions described in the mental health setting (Björkdahl et al., 2013) and
the geriatric setting (Zeller et al., 2009). These interventions suggest the importance of intervening on a

Chapter V
132
group level when designing programs to support individual nurses. This is important as these
interventions can take the culture of the team and the ward into account. Dackert (2010) reports a
positive relationship between perceived team climate that supports innovation and individual well-being
of nurses and a negative relationship between perceived team climate and stress reactions. A team
climate supporting innovative processes incorporates for example a shared concern about the quality of
work, communication and interaction, the encouragement of nurses to improve their work, etc. (Dackert,
2010). An innovative team climate might imply that nurses are empowered and stimulated to develop
their competences in interacting with patients which might alter and amend nurses’ perceptions of
transgressive behaviour.
Likewise, it would be interesting to examine whether lived experiences of patients and nurses receive
sufficient attention during training and postgraduate courses. For a professional to develop new
competencies, the way of understanding needs to be challenged. Understanding the patient’s
perspective and acknowledging personal feelings and sharing in care relationships, might support
nurses in perceiving and dealing with transgressive behaviour. An increasing tendency to objectify and
standardize nursing care might increase the risk that behaviour in a specific situation is prescribed,
rather than for individuals to evaluate care in a reflective manner.
4.4. | Implications for further research
In this study transgressive behaviour was operationalized based on nurse’s perceptions. Nurses
experienced transgressive behaviour when personal limits, standards, or norms were crossed. No
standard on transgressive or aggressive behaviour was imposed. However, personal boundaries are
different from professional boundaries. Personal experiences of transgressive behaviour do not imply
that professional boundaries are exceeded. However, present findings indicate that nurses’ personal
boundaries coincide with their professional boundaries, whereas a distinction between individual
normativity and professional nursing normativity appears of paramount importance. When personal
limits are crossed, professional limits are not necessarily violated. Future research might explore how
personal and professional standards interact and what professional normativity means for the perception
of the relationship with the patient.
Since colleagues, ward culture and ward habits influenced perception of and reaction to transgressive
behaviour, it would be interesting to examine the effect of individual experiences of transgressive
Nurses’ perceptions of transgressive behaviour
133
behaviour on staff mentality of transgressive behaviour. Group processes and socialization can be
further explored to design tailored support on a group level for nurses working in general hospital wards.
Likewise, the setting was limited to general medical wards in general hospitals. It would be interesting
to replicate this study in other settings such as residential or home care because in these settings, nurse
interaction with patients and position in relation to patients differs greatly in nature, which could affect
perceptions of transgressive behaviour.
This study revealed dimensions that affect nurse perceptions of transgressive behaviour in general
hospitals. Connecting these findings to the analysis of patients’ interviews will deepen the dynamics of
professional relationships in the context of perceiving transgressive behaviour.
5. | Conclusion
The findings of this study suggest that perceptions of transgressive behaviour are determined and
regulated by several factors on the level of the patient, the individual nurse and the hospital. The findings
demonstrate how nurses’ experiences largely rely on the interaction with patients and thus reveal the
complexity of nurses’ perceptions of transgressive behaviour in care relationships with patients. The
notion that experiences of nurses and patients cannot be separated and contribute equally to
perceptions of transgressive behaviour is a theorem of ‘the interactional model’ (Pervin , 1988, in
Duxbury, 1999). This approach examines violence and aggression in the combined context of both the
individual and their environment and as such recognizes both factors as equally important (Duxbury,
1999). Consequently, if transgressive behaviour can be perceived by nurses as an experience largely
reliant on the interaction with patients, then the care that follows could reflect this approach. Nurses
would thus be inclined to reflect on their own behaviour in the interaction with patients. Present findings
demonstrate how nurses primarily perceive the relationship with and the behaviour of the patient from
their own frame of reference or viewpoint. The specific context or the individual perspective of the patient
is not necessarily inserted in the nurses’ assessment of the interaction with patients, resulting in possible
perceptions of transgressive behaviour. Engaging nurses in ‘reflective practice’ during their working day
might enable them to examine their work and gain insight and awareness from their work. Reflecting on
their work enables nurses to connect with their implicit needs and might challenge them to understand
their patients’ perspectives and experiences (Markey & Farvis, 2014). In turn, implementing ‘reflective

Chapter V
134
practice’ can benefit personal and professional development (Williams & Walker, 2003; Gustafsson &
Fagerberg, 2004; Tishelman et al., 2004).
Nurses’ perceptions of transgressive behaviour
135
REFERENCES
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Fischer, J.E., & Haug, H.J. (2007). Frequency and severity
of aggressive incidents in acute psychiatric wards in Switzerland. Clinical Practice and Epidemiology in Mental
Health, 4, 3–30.
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Haug, H.J., & Fischer, J.E. (2008). Structured risk
assessment and violence in acute psychiatric wards: randomised controlled trial. The British Journal of Psychiatry,
193(1), 44–50.
Almvik, R., Rasmussen, K., & Woods, P. (2006). Challenging behaviour in the elderly: monitoring violent incidents.
International Journal of Geriatric Psychiatry, 21(4), 368–374.
Björkdahl, A., Hansebo, G., & Palmstierna, T. (2013). The influence of staff training on the violence prevention and
management climate in psychiatric inpatient units. Journal of Psychiatric and Mental Health Nursing, 20(5), 396–
404.
Boscart, V.M. (2009). A communication intervention for nursing staff in chronic care. Journal of Advanced Nursing,
65(9), 1823– 1832.
Burnard, P., & Morrison, P. (2005). Nurses’ perceptions of their interpersonal skills: a descriptive study using six
category intervention analysis. Nurse Education Today, 25(8), 612–617.
Camerino, D., Estryn-Behar, M., Conway, P.M., van Der Heijden, B.I., & Hasselhorn, H.M. (2008). Work-related
factors and violence among nursing staff in the European NEXT study: a longitudinal cohort study. International
Journal of Nursing Studies, 45(1), 35–50.
Chapman, R., Styles, I., Perry, L., & Combs, S. (2010). Nurses’ experience of adjusting to workplace violence: a
theory of adaptation. International Journal of Mental Health Nursing, 19(3), 186–194.
Charmaz, K. (2008). Constructing Grounded Theory: A Practical Guide through Qualitative Analysis . Sage,
Thousand Oaks, CA.
Dackert, I. (2010). The impact of team climate for innovation on well-being and stress in elderly care. Journal of
Nursing Management, 18(3), 302–310.
Draucker, C.B., Martsolf, D.S., Ratchneewan, R., & Rusk, T.B. (2007). Theoretical sampling and category
development in grounded theory. Qualitative Health Research, 17(8), 1137–1148.
Dunn, K., Elsom, S., & Cross, W. (2007). Self-efficacy and locus of control affect management of aggression by
mental health nurses. Issues in Mental Health Nursing, 28(2), 201–217.
Duxbury, J. (1999). An exploratory account of registered nurses’ experience of patient aggression in both mental
health and general nursing settings. Journal of Psychiatric and Mental Health Nursing, 6(2), 107–114.
Duxbury, J., Pulsford, D., Hadi, M., & Sykes, S. (2013). Staff and relatives’ perspective on the aggressive behavior
of older people with dementia in residential care: a qualitative study. Journal of Psychiatric and Mental Health
Nursing, 20(9), 792–800.
Estryn-Behar, M., van der Heijden, B., Camerino, D., Fry, C., Le Nezet, O., Conway, P.M., Hasselhorn, H.M., &
NEXT Study Group (2008). Violence risk in nursing: results from the European ‘NEXT’ study. Occupational
Medicine, 58(2), 107– 114.
Feng, R.F., & Tsai, Y.F. (2012). Socialisation of new graduate nurses to practising nurses. Journal of Clinical
Nursing, 21(13–14), 2064–2071.
Chapter V
136
Foster, C., Bowers, L., & Nijman, H. (2007). Aggressive behavior on acute psychiatric wards: prevalence, severity
and management. Journal of Advanced Nursing, 58(2), 140–149.
Gates, D.M., Gillespie, G.L., & Succop, P. (2011). Violence against nurses and its impact on stress and productivity.
Nursing Economics, 29(2), 59–67.
Gerberich, S.G., Church, T.R., McGovern, P.M., Hansen, H.E., Nachreiner, N.M., Geisser, M.S., Ryan, A.D.,
Mongin, S.J., & Watt, G.D. (2004). An epidemiological study of the magnitude and consequences of work related
violence: the Minnesota Nurses’ Study. Occupational and Environmental Medicine, 61(6), 495–503.
Gerdtz, M.F., Daniel, C., Dearie, V., Permatunga, R., Bamert, M., & Duxbury, J. (2013). The outcome of a rapid
training program on nurses’ attitudes regarding the prevention of aggression in emergency departments: a multi -
site evaluation. International Journal of Nursing Studies, 50(11), 1434–1445.
Glaser, B.G., & Strauss, A. (1967). The Discovery of Grounded Theory. Adline Atherton, Chicago, IL.
Gustafsson, C., & Fagerberg, I. (2004). Reflection, the way to professional development? Journal of Clinical
Nursing, 13(3), 271–280.
Hahn, S., Zeller, A., Needham, I., Kok, G., Dassen, T., & Halfens, R.J.G. (2008). Patient and visitor violence in
general hospitals: a systematic review of the literature. Aggression and Violent Behavior, 13, 431–441.
Hahn, S., Müller, M., Needham, I., Dassen, T., Kok, G., & Halfens, R.J.G. (2010). Factors associated with patient
and visitor violence experienced by nurses in general hospitals in Switzerland: a cross-sectional survey. Journal of
Clinical Nursing, 19(23–24), 3535–3546.
Hahn, S., Hantikainen, V., Needham, I., Kok, G., Dassen, T., & Halfens, R.J.G. (2012). Patient and visitor violence
in the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey. Journal of
Advanced Nursing, 68(12), 2685–2699.
Hahn, S., Müller, M., Hantikainen, V., Kok, G., Dassen, T., & Halfens, R.J.G. (2013). Risk factors associated with
patient and visitor violence in general hospitals: results of a multiple regression analysis. International Journal of
Nursing Studies, 50(3), 374–385.
Hallberg, L.R.M. (2006). The ‘core category’ of grounded theory: making constant comparisons. International
Journal of Qualitative Studies on Health and Well-Being, 1(3), 141–148.
Lincoln, Y.S., & Guba, E.G. (1985). Naturalistic Inquiry. Sage, Beverly Hills, CA.
Liu, J. (2004). Concept analysis: aggression. Issues in Mental Health Nursing, 25(7), 693–714.
Liu, J., Lewis, G., & Evans, L. (2013). Understanding aggressive behaviour across the lifespan. Journal of
Psychiatric and Mental Health Nursing, 20(2), 156–168.
Markey, L., & Farvis, R. (2014). Reflective practice in an acute setting. Nursing Times, 110(24), 16–18.
McLaughlin, S., Pearce, R., & Trenoweth, S. (2013). Reducing conflict on wards by improving team communication.
Mental Health Practice, 16(5), 29–31.
Morgan, J.C., & Lynn, M.R. (2009). Satisfaction in nursing in the context of shortage. Journal of Nursing
Management, 17(3), 401– 410.
Morgan, D.G., Crossley, M.F., Stewart, N.J., D’Arcy, C., Forbes, D.A., Normand, S.A., & Cammer, A.L. (2008).
Taking the hit: focusing on caregiver ‘error’ masks organizational-level risk factors for nursing aide assault.
Qualitative Health Research, 18(3), 334–346.
Nurses’ perceptions of transgressive behaviour
137
Morse, J., & Field, P.A. (1996). Nursing Research. The Application of Qualitative Approaches. London: Chapman
& Hall.
Needham, I., Abderhalden, C., Halfens, R.J.G., Fischer, J.E., & Dassen, T. (2005). Non-somatic effects of patient
aggression on nurses: a systematic review. Journal of Advanced Nursing, 49(3), 283–296.
Nijman, H., Bowers, L., Oud, N., & Jansen, G. (2005). Psychiatric nurses’ experiences with inpatient aggression.
Aggressive Behaviour, 31(3), 217–227.
O’Connell, B., Young, J., Brooks, J., Hutchings, J., & Lofthouse, J. (2000). Nurses’ perceptions of the nature and
frequency of aggression in general ward settings and high dependency areas. Journal of Clinical Nursing, 9(4),
602–610.
Spector, P.E., Zhou, Z.E., & Che, X.X. (2014). Nurse exposure to physical and nonphysical violence, bullying and
sexual harassment: a quantitative review. International Journal of Nursing Studies, 51(1), 72–84.
Tishelman, C., Bernhardson, B.M., Blomberg, K., Borjeson, S., Franklin, L., Johansson, E., Levealahti, H., Sahlberg-
Blom, E., & Ternestedt, B.M. (2004). Complexity in caring for patients with advanced cancer. Journal of Advanced
Nursing, 45(4), 420–429.
Waschgler, K., Ruiz-Hernandez, J.A., Llor-Esteban, B., & Garçıa-Izquierdo, M. (2013). Patients’ aggressive
behaviors towards nurses: development and psychometric properties of the hospital aggressive behavior scale-
users. Journal of Advanced Nursing, 69(6), 1418–1427.
Wells, J., & Bowers, L. (2002). How prevalent is violence towards nurses working in general hospitals in the UK?
Journal of Advanced Nursing, 39(3), 230–240.
Williams, B., & Walker, L. (2003). Facilitating perception and imagination in generating change through reflective
practice groups. Nurse Education Today, 23(2), 131–137.
Yang, L.Q., Spector, P.E., Chang, C.H., Gallant-Roman, M., & Powell, J. (2012). Psychosocial precursors and
physical consequences of workplace violence towards nurses: a longitudinal examination with naturally occurring
groups in hospital settings. International Journal of Nursing Studies, 49(9), 1091–1102.
Zeller, A., Hahn, S., Needham, I., Kok, G., Dassen, T., & Halfens, R.J.G. (2009). Aggressive behavior of nursing
home residents toward caregivers: a systematic literature review. Geriatric Nursing, 30(3), 174–187.
Zeller, A., Dassen, T., Kok, G., Needham, I., & Halfens, R.J.G. (2011). Nursing home caregivers’ explanations for
and coping strategies with residents’ aggression: a qualitative study. Journal of Clinical Nursing, 20(17–18), 2469–
2478.
Zernike, W., & Sharpe, P. (1998). Patient aggression in a general hospital setting: do nurses perceive it to be a
problem? International Journal of Nursing Practice, 4(2), 126–133.

Influence of team members on perceptions of transgressive behaviour
138
Influence of team members on perceptions of transgressive behaviour
139
Chapter VI.
INFLUENCE OF TEAM MEMBERS ON NURSES’
PERCEPTIONS OF TRANSGRESSIVE BEHAVIOUR
Tina Vandecasteele1,2, Ann Van Hecke1,3, Veerle Duprez1, Dimitri Beeckman1, Bart Debyser2,
Maria Grypdonck1, Sofie Verhaeghe1,2
1 Department of Public Health, Faculty of Medicine and Health Sciences, University Centre for Nursing &
Midwifery, Ghent University, Ghent, Belgium.
2 Department Health care, VIVES University College, Roeselare, Belgium.
3 University Hospital Ghent, Ghent, Belgium.
Based on the article of Vandecasteele T, Van Hecke A, Duprez V, Beeckman D, Debyser B, Grypdonck
M, & Verhaeghe S. The influence of team members on nurses’perceptions of transgressive behaviour
in care relationships: A qualitative study. Journal of Advanced Nursing. 2017;00:1–12.
https://doi.org/10.1111/jan.13315.

Chapter VI
140

Influence of team members on perceptions of transgressive behaviour
141
The influence of team members on nurses’ perceptions of transgressive behaviour in
care relationships: A qualitative study
ABSTRACT
Aim. The aim of this study was to gain insight into the influence of team members in how nurses
perceive and address patients’ transgressive behaviour.
Background. Aggression and transgressive behaviour in healthcare have been a focus of research
over the past few decades. Most studies have focused on individual nurses’ experiences with
aggression and transgressive behaviour. Literature examining group dynamics in nursing teams and
team members’ interactions in handling patients’ transgressive behaviour is scarce.
Design. Qualitative interview study.
Methods. Seven focus-group interviews and two individual interviews were carried out in 2014-2016.
Twenty-four nurses were drawn from eight wards in three general hospitals. Interviews were analysed
using the constant comparative method influenced by the grounded theory approach.
Findings. While elaborating how they perceived and addressed transgressive behaviour, nurses
disclosed how interactions with team members occurred. Several patterns arose. Nurses talk to one
another, excuse one another, fill in for one another, warn one another and protect and safeguard one
another. In these patterns in reaction to patients’ transgressive behaviour, implicit group norms
transpire, causing nursing teams to acquire their specific identity “as a group”. Consequently, these
informal group norms in nursing teams impinge how nurses feel threatened by patients’ potential
transgressive behaviour; gain protection from the group of nurses and conform to informal ward rules.
Conclusion. The findings of this study can support intervention strategies aimed at supporting nurses
and nursing teams in managing patient aggression and transgressive behaviour by identifying and
explicating these group dynamics and team members’ interactions.
Keywords. Aggression, care relationship, general hospital, nurse–patient relationship, nurses, nursing
teams, qualitative research, transgressive behaviour, violence.
Chapter VI
142
1. | Introduction
This article addresses the influence of nursing team members on nurses’ perceptions of transgressive
behaviour in care relationships with patients and how they deal with these perceptions. It is imperative
to understand these group dynamics in nursing teams to develop effective organizational interventions
to address transgressive behaviour in care relationships between nurses and patients.
1.2. | Background
Aggression in health care is not a new problem. Aggression towards healthcare workers is prevalent
and well recognized internationally (Wei, Chiou, Chien, & Huang, 2016). The extensive consequences
of aggression in care relationships on nurses, patients, patient care and the organization as a whole,
have induced a large amount of research on aggression in health care. Hence, this research has noted
that aggression is most prevalent in emergency departments, geriatric and mental healthcare settings
(Spector, Zhou, & Che, 2014). Its contributing risk factors have been well documented and have been
identified on the level of patients’ characteristics (Hahn et al., 2013), staff characteristics (Duxbury, 2002;
Jansen, Dassen, & Groot Jebbink, 2005), staff–patient interactions (Winstanley, 2005; Winstanley &
Whittington, 2004) and organizational characteristics (Farrell, Bobrowski, & Bobrowski, 2006; May &
Grubbs, 2002). Much has been learnt about the consequences of encountering aggression regarding
both the physical and psychological well-being of caregivers (Mantzouranis, Fafliora, Bampalis, &
Christopoulou, 2015; Needham, Abderhalden, Halfens, Fischer, & Dassen, 2005) and different
aetiological models on aggression have been described (Duxbury & Whittington, 2005; Wahl, 2009).
This extensive amount of research fosters a greater understanding of aggression in different settings,
patient populations and organizational structures.
However, despite these important insights, some issues regarding aggression in care relationships
remain unclear or under-researched. These issues are related to the specific focus in research on
particular settings and on the perspective of individual caregivers as well as the particular
operationalization of the concept of aggression.
Most studies have focused on geriatric (Almvik, Rasmussen, & Woods, 2006; Duxbury, Pulsford, Hadi,
& Sykes, 2013), emergency (Gerdtz et al., 2013) and mental healthcare settings (Abderhalden et al.,
2007), creating a gap in knowledge about nurses’ experiences in general medical and surgical care
units. However, according to Roche, Diers, Duffield, & Catling-Paull (2010), general hospital settings
Influence of team members on perceptions of transgressive behaviour
143
are increasingly regarded to be vulnerable for aggressive incidents (Roche et al., 2010). For instance,
Pich, Hazelton, Sundin, & Kable (2011) identified parents of paediatric patients as a potential significant
group as a source of aggression. Although there have been a few studies focusing on patient aggression
in general hospital settings (Hahn et al., 2013; Heckemann et al., 2015), much can still be learnt about
experiences of nurses working in the former settings (Wei et al., 2016; Winstanley & Whittington, 2004).
Moreover, most studies focus on the perspective of singular nurses on patient aggression (Luck,
Jackson, & Usher, 2008; Stevenson, Jack, O’Mara, & LeGris, 2015). Group dynamics and interactions
with other team members that can influence individual nurse’s experiences are scarcely taken into
consideration (Cox, 2001). Group interactions and the influence of team members can be rather
profound because research on why aggressive incidents are under-reported has noted how peer
pressure from other nursing staff appears to be one of the reasons incidents are not reported (Rippon,
2000; Sato, Wakabayashi, Kiyoshi-Teo, & Fukahori, 2013). This finding suggests that nurses can be
affected or even swayed by colleagues with regards to perceiving, managing or eventually reporting
aggression. Reasons as to why and how nurses are influenced by colleagues, can be partially found in
literature on socializing processes in nursing teams (Bisholt, 2012; Feng & Tsai, 2012; Trysoe,
Hounsgaard, Dohn, & Wagner, 2012). In particular, the concept “professional socialization” (Bisholt,
2012; Mooney, 2007) refers to processes through which new practitioners are merged into the
profession (Mooney, 2007). This process entails that newcomers gradually acquire attitudes, values and
norms of professional clinical practitioners (Feng & Tsai, 2012; Mooney, 2007) while learning (in)formal
rules of the organization (Maben, Latter, & Clark, 2006). These studies focus on experiences of recently
qualified nurses (Bisholt, 2012) or Baccalaureate nursing students (Secrest et al., 2003). It can be
hypothesized that similar processes of socialization remain present in nurses who have been working
for some time in nursing practice (Yarbrough, Martin, Alfred, & McNeill, 2016). Like-wise, it remains
unclear how these processes might influence patient’s care or the conduct towards patients. There is
little knowledge at hand surrounding nurses’ interactions and team dynamics in perceiving and
addressing patients’ transgressive behaviour.
A third issue regarding existing literature on aggression in care relationships pertains to
operationalisations of “aggression”. Several researchers have noted how comparison of research
findings is hampered by adopting different definitions of “aggression” (Hahn et al., 2008; Rippon, 2000).
In addition, addressing related concepts, such as “challenging behaviour” (Almvik et al., 2006) or
Chapter VI
144
“assault” (Gerberich et al., 2005; May & Grubbs, 2002), made discussions on aggression in healthcare
more thorough and intriguing but at the same time more complex. However, when using definitions of
“aggression”, an assumption that specific behaviours are perceived as aggressive by definition is made.
However, perceptions of what constitutes aggressive acts can vary from person to person. Little insight
is available on how aggression is perceived, what limits must be exceeded for situations to be
experienced as aggressive and which factors might influence this process. In this study, the broader
term “transgressive behaviour” was used because its use allows returning to the “essence” of
experiencing aggression, namely the crossing of one’s limits, standards or norms. Use of this term
allows an individual interpretation of when and what limits are exceeded for situations to be experienced
as transgressive and which factors influence this process. This study strives to use an inductive
approach because the interpretation of limits, how they are exceeded, the perceived seriousness of the
situation and the processes involved in this interpretation were not determined in advance.
Consequently, this study tries to contribute to the literature on aggression in care relationships by
focusing on group dynamics in nursing teams in general hospital settings regarding transgressive
behaviour.
2. | The Study
2.1. | Aim
The purpose of this study was to explore and understand group dynamics and the influence of team
members on how nurses perceive and deal with transgressive behaviour in care relationships with
patients.
2.2. | Design
This study adopted principles of the Grounded Theory to examine reasoning processes used by nurses
for interacting with team members in perceiving and dealing with transgressive patients’ behaviour. This
design facilitated the understanding of nurses’ perceptions regarding complex and potentially sensitive
work-related issues (Glaser & Strauss, 1967; Hallberg, 2006; Morse & Field, 1996).
2.3. | Sample and participants
The study occurred in six hospital wards located in three general hospitals in Belgium. These hospitals
serve both rural and urban communities. Included wards had a medical, geriatric, or surgical focus.
Recruitment and data collection occurred over 2 years from 2014–2016. Study aim and procedures were
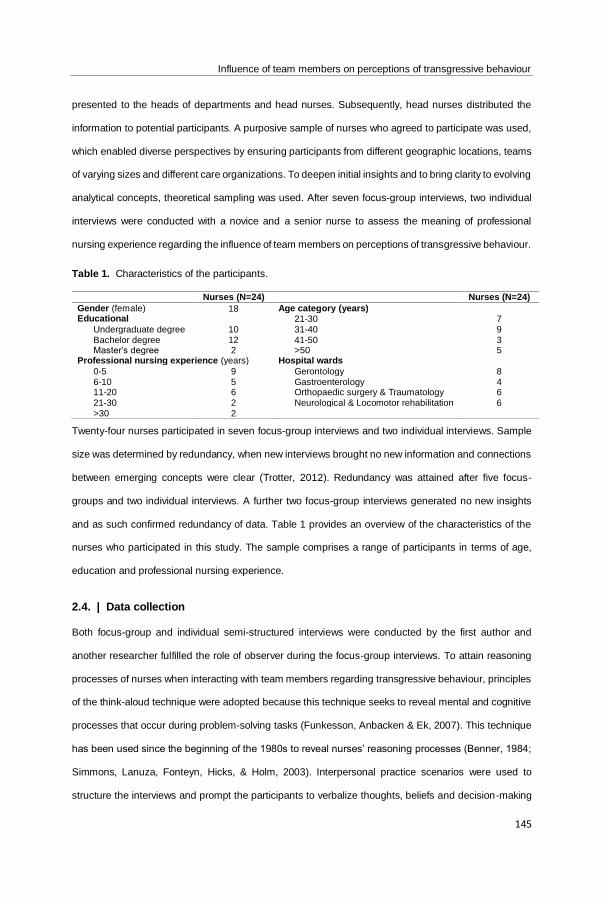
Influence of team members on perceptions of transgressive behaviour
145
presented to the heads of departments and head nurses. Subsequently, head nurses distributed the
information to potential participants. A purposive sample of nurses who agreed to participate was used,
which enabled diverse perspectives by ensuring participants from different geographic locations, teams
of varying sizes and different care organizations. To deepen initial insights and to bring clarity to evolving
analytical concepts, theoretical sampling was used. After seven focus-group interviews, two individual
interviews were conducted with a novice and a senior nurse to assess the meaning of professional
nursing experience regarding the influence of team members on perceptions of transgressive behaviour.
Table 1. Characteristics of the participants.
Nurses (N=24) Nurses (N=24)
Gender (female) 18 Age category (years) Educational 21-30 7
Undergraduate degree 10 31-40 9 Bachelor degree 12 41-50 3 Master’s degree 2 >50 5
Professional nursing experience (years) Hospital wards
0-5 9 Gerontology 8 6-10 5 Gastroenterology 4 11-20 6 Orthopaedic surgery & Traumatology 6 21-30 2 Neurological & Locomotor rehabilitation 6 >30 2
Twenty-four nurses participated in seven focus-group interviews and two individual interviews. Sample
size was determined by redundancy, when new interviews brought no new information and connections
between emerging concepts were clear (Trotter, 2012). Redundancy was attained after five focus-
groups and two individual interviews. A further two focus-group interviews generated no new insights
and as such confirmed redundancy of data. Table 1 provides an overview of the characteristics of the
nurses who participated in this study. The sample comprises a range of participants in terms of age,
education and professional nursing experience.
2.4. | Data collection
Both focus-group and individual semi-structured interviews were conducted by the first author and
another researcher fulfilled the role of observer during the focus-group interviews. To attain reasoning
processes of nurses when interacting with team members regarding transgressive behaviour, principles
of the think-aloud technique were adopted because this technique seeks to reveal mental and cognitive
processes that occur during problem-solving tasks (Funkesson, Anbacken & Ek, 2007). This technique
has been used since the beginning of the 1980s to reveal nurses’ reasoning processes (Benner, 1984;
Simmons, Lanuza, Fonteyn, Hicks, & Holm, 2003). Interpersonal practice scenarios were used to
structure the interviews and prompt the participants to verbalize thoughts, beliefs and decision-making
Chapter VI
146
in explaining responses to these real-world scenarios. These practice scenarios were collected in a prior
pilot study and provided examples of transgressive patients’ behaviour as experienced by nurses
working in general hospital settings. In addition to these practice scenarios, nurses were encouraged to
recollect own experiences in practice regarding transgressive patients’ behaviour and the meaning of
team members in experiencing or handling this behaviour. As stated in the introduction, “transgressive
behaviour” was not defined in advance prior to the interviews with nurses. The inductive approach
allowed an individual interpretation of when and what limits were exceeded for situations to be
experienced as transgressive. The first scenarios described situations where nurses reflected at a more
individual level on how they would perceive and respond to patient’s transgressive behaviour. Gradually
scenarios were provided which encompassed interactions between team members. Table 2 provides
examples of fragments of interpersonal practice scenarios. Interviews were conducted in a location
convenient to the participants. All the participants chose a separate room at their place of employment,
ensuring their privacy. Focus-group interviews lasted between 65 – 120 minutes and individual
interviews were approximately 60 minutes in length. Field notes were made capturing impressions and
thoughts during and after the interviews, with attention to thick description. During the interviews, these
notes were about that was verbalized, including points that needed clarification. After consent, each
interview was audiotaped. Digital recordings were transcribed to create verbatim accounts. All the
identifiers of the participants were removed from the transcripts prior to analysis.
Table 2. Examples of fragments of interpersonal practice scenarios
“[…] You have to administer an intramuscular injection to a patient. The patients responds by saying
she wants the doctor to administer the injection as ‘you are not competent’[…]”
“[…] You are using the passive patient lift to transfer the patient to his chair. The patient responds by
saying that you are very lazy for using the passive lift […]”
“[…] You are walking in the hallway. You pass a room and witness how a colleague is very rude to a
patient. The response of your colleague provokes an angry reaction of the patient […]”.
“[…] A patient complains about a dirty mobile toilet which was left in his room. It is not the first time
your colleague forgot to remove and clean the mobile toilets. The patient accuses you and says
‘everything is very filthy on this ward’[…]”
2.5. | Ethical considerations
Research Ethics Committee approval for the study was obtained from the University Hospital Ethics
Committee prior to commencement. All the participants were given informational leaflets and were
informed of the procedure and objectives of the study. Written consent of every participant was obtained.

Influence of team members on perceptions of transgressive behaviour
147
The participants were assured they could withdraw at any time and confidentiality was stressed. The
researchers were not known to any of the participants.
2.6. | Data analysis
An iterative approach was undertaken as analysis was performed simultaneously with data collection.
At first, the authors read the transcripts several times to gain an overall picture of the interviews, to
familiarize themselves with the data and to gather initial ideas on the possible meaning of the data. In
search for understanding, probing reflective questions were generated (e.g. in elaborating on
experiences, when do nurses use the term “we” and when do they use the term “I”?) Subsequently,
initial open codes were assigned capturing meaningful content of the interviews using the NVIVO
Software package (QSR International). Without losing the context and attributes of each interview,
constant comparison of interviews allowed the gradual emergence of conceptual insights. Progressively,
more abstract and conceptual insights were constructed and added to these initial understandings. This
approach informed further data collection on theoretical insights and enabled data saturation.
2.7. | Rigour
Several strategies were applied in every phase of the research to ensure trustworthiness of the data
and analysis. The framework of Lincoln and Guba (1985), through the meaning of credibility,
confirmability and dependability, underpinned the study. A thorough form of investigator triangulation
was adopted, ensuring both credibility and dependability of the findings and data (Lincoln & Guba, 1985).
All the researchers had experience in conducting qualitative research and four researchers had
extensive experience in grounded theory research and the thinking-aloud method. The interpretative
process of analysis was underpinned by reflexivity, ensuring openness to the meaning of the data and
a general tenet to question, criticize and explicate understandings of the data (Malterud, 2001). An audit
trail provided a thorough description of the structure and rationale of meaning assigned to data, which
strengthened dependability (Lincoln & Guba, 1985).
3. | Results
During the interviews, nurses explained how they perceived and dealt with transgressive patient
behaviour. Nurses were generally found to prefer a particular way of reacting to transgressive behaviour
and they especially described a rather evasive way of dealing with it. They described how they ignored
transgressive behaviour, how they avoided contact by handing over the patient’s care to colleagues,
Chapter VI
148
how they limited contact to that was strictly necessary, or how they sought solutions to no longer take
care of the patient themselves.
"...Or not going in alone. We do that very often, entering the room with a colleague. And then
we say: ‘Well, we are going to wash him together right away’. That way we get our work done
faster..."
The interviews demonstrated that nurses are strongly influenced by the interaction with colleagues when
deciding how to address transgressive behaviour. In this interaction, four concrete actions can be
distinguished: (1) talking to colleagues and excusing each other; (2) filling in for each other; (3) informing
and warning each other and (4) defending, protecting and safeguarding each other. These dynamics
will be further elaborated below.
Talking to colleagues and excusing each other (“Tell me what happened… It is not your fault”).
When perceiving transgressive behaviour, nurses approach a colleague. During this first contact, they
usually explain what occurred. They inform their colleague about what the patient said or did. Nurses
mentioned they felt offended and indignant about transgressive behaviour. Communicating with a
colleague served as a form of recuperation. Nurses noted it is very important to communicate with
colleagues to vent or to let go of the incident. Sharing what occurred seems to have a healing effect.
Nurses mainly expected their colleagues to show solidarity. Therefore, it was not necessary to keep on
talking about the incident. Colleagues seemed to adopt an “excusing” attitude. Nurses stated how their
colleagues said they were not to be blamed for the patient’s transgressive behaviour, the incident had
nothing to do with them personally, it was the patient’s fault and they experienced a similar situation
themselves. Because of this “excusing” attitude, nurses did not take the incident personally. Indicating
it was the patient’s fault or noting that other nurses experienced the same thing helped nurses to not
blame themselves.
"...Just tell what the patient said and then that colleague will react ‘Let it be, that’s how that
patient is’, or something similar. ‘That happens a lot and everyone has to deal with that.’ So yes.
‘It also happens to me, so don’t dwell on it’..."
Several nurses noted that it did not matter which colleague they told their story to. They even addressed
colleagues with whom they did not have a good personal bond. Some nurses added that everyone
Influence of team members on perceptions of transgressive behaviour
149
knows it is important to let go of the experience at that moment and to talk about it. The bond with the
colleague addressed is of no importance.
"...Nurse 4: I think it is the first person you encounter in the corridor that you. ...// Nurse 3: To
whom you vent. Nurse 4: To whom you can let off steam. Nurse 3: You vent your feelings, and
then the experience is in the past. Nurse 1: Yes, then it’s in the past...."
Talking to colleagues and excusing each other often results in colleagues taking over each other’s care
assignments.
Filling in for each other (“I will take over from you”). Most nurses said they avoided contact with
the patient after they experienced transgressive behaviour. They remarked it would be of no use to
argue or to talk about the problem. They added it would only make matters worse if they were to talk
with the patient about transgressive behaviour. Several nurses said they then handed over care
assignments to colleagues so they either no longer had to see the patient that often, or no longer had
to see them at all.
"...It often happens that someone says ‘Look, I won't enter that room anymore.’ Then someone
else will go. That is the best thing to do. Because eventually you may enter into a discussion
you would rather avoid...”
Furthermore, nurses noted they quickly came to the solution to fill in for each other and to take over
each other’s care assignments. All the nurses said no one has to explain why this arrangement was
made. Filling in for each other is not necessarily further discussed among colleagues. Some nurses said
that this solution is generally believed to be the right one to assure the patient’s care.
"...She kept on shouting, and I said [to a colleague]: ‘You can leave the bathroom, I will carry
on.’ I: And did you discuss that with that colleague afterwards? P: "No, but usually you know
each other well enough. I don’t have to say, I don’t think I should start ‘You should’ve done that
or that.’ I wouldn’t do that"..."
Addressing colleagues about transgressive behaviour and taking over care assignments also results in
fellow nurses being informed and warned about patients.
Informing and warning each other (“You should be on your guard”). Several nurses said that
talking to colleagues about transgressive behaviour allowed them to tell their side of the story. As such,
Chapter VI
150
colleagues were informed about what occurred in an objective way, nurses said. Some nurses
suggested that the patient himself could indeed tell what occurred to colleagues, which made it important
for nurses to tell their side of the story first.
"...And make clear to your colleagues what happened. If that patient should talk about the
incident to your colleagues... Then your colleagues also know your point of view, what actually
happened..."
When nurses informed their colleagues about patient’s behaviour, these colleagues are warned. That
way, other nurses can prepare themselves when meeting the patient.
“…And if we know that certain people quickly become aggressive or verbally aggressive, we
often say when passing on the patient's care to a colleague: "You have to take extra care with
that patient, be very gentle, because..."
Informing and warning colleagues about patients’ behaviour also led to patients being labelled.
Experiences and impressions of one nurse were shared, which inclined other nurses to adopt the same
judgement. Several nurses stated they already had certain expectations regarding the patient’s
behaviour before actually meeting them.
"...Sometimes, we do influence each other. That’s true. If one nurse says that a patient is a
difficult person, the next colleague who enters the patient's room will often also think he is a
difficult person. 4: "That’s just because it’s passed on like that." 2: "You sometimes think
someone is a difficult person just because you expect them to be difficult. Even though that
might actually not be the case in reality, you start seeing things which indicate that they are
indeed a difficult patient ..." 1: "Yes that’s true. Yes, when you enter the room of a patient your
colleague finds difficult, you will take that expectation into account when you approach the
patient." 2: "Ah, yes" 3: "Yes, you are indeed prepared when you enter the room." 4: "Yes, yes."
3: "You already react differently, don't you?" 2: "Yes you are already ..."//4: "Yes, you can’t
endure that much anymore..."
Labelling patients influenced the concrete contact that nurses subsequently had with the patient. Nurses
said they were already prepared when they entered the room and they were immediately less tolerant
and firmer. They also said they thought in advance about what they would say if the patient was difficult.
Influence of team members on perceptions of transgressive behaviour
151
If nurses adopted a colleague’s judgement on a patient’s behaviour, they seemed to approach the
patient (or their family) the same way their colleague did. Some nurses described how a patient’s
husband interfered too much in the care for his wife. They explained that this man always took care of
his wife at home and he wanted to continue taking care of her in the hospital. These nurses then told
how they, together with their colleagues, made sure the husband did not hinder the patient’s care.
"...Oh, yes. The patient's husband who was intrusive. He always wanted to help and explain to
us how we should do our jobs. Because we also had to place her in the armchair with the hoist,
and then ... <<laughs>>. And then we actually made sure she was already in the armchair when
he arrived. <laughs>> Just to make things easier for us, yes. So he did not ... have to interfere,
you know..."
These implicit agreements on how to approach patients also seemed to have an influence on a fourth
dynamic: defending, protecting and safeguarding each other.
Defending, protecting and safeguarding each other (“You have to protect the team”). When a
patient exhibited transgressive behaviour towards a colleague, all the nurses described how they stood
by their colleague. Nurses quoted several examples of how they witnessed colleagues being insulted or
not knowing how to react to a patient’s reproaches. Most nurses said they joined in the conversation
with the patient and literally stood by their colleague. Several nurses then clarified they wanted to do
this to show they supported their colleague.
"...If I see something is going on ... If a colleague is involved, I’ll immediately go there. I: "And
what would you do then?" P: "First, I’ll ask what’s going on. Then my colleague no longer stands
there alone. ... They [the patients] usually start to falter then. And then you listen to what your
colleague says, and you just agree..."
All the nurses said it was logical and obvious to assist their colleagues. Some nurses added that the
bond with colleagues was of no importance. Even if there was not a good personal bond, it was obvious
to support and defend colleagues when they experienced difficulties.
"...Then you’ll defend that colleague, even if you don’t like them. You’ll defend them anyway. I
do believe we all have it in us. Everyone does it, yes. Actually, we all agree on it? We can all
rely on each other. That's what I feel. No matter what happens... "
Chapter VI
152
Several nurses referred to incidents where a patient reproached them for a mistake a colleague had
made. All the nurses said they dealt with these reproaches by correcting the situation, soothing the
patient, solving the problem and leaving the situation alone. Then, they usually told the patient they
would immediately solve the problem and that everyone makes mistakes.
"...Say that it was so busy it was forgotten. I would apologize for my colleague and I wouldn't
react to it. 1: "Actually, avoid a discussion with the patient. Just ignore it"..."
All the nurses said they did not further react to the patient’s personal reproaches to express their
displeasure afterwards. They no longer talked about the incident. Some nurses explained they did not
want to talk to patients about a mistake a colleague made. They added that the patient might pass on
what they said about the colleague who made a mistake. They wanted to avoid patients talking to other
colleagues about that.
"...If you think what the patient says about that colleague is true, you do not have to admit it to
the patient. You keep it to yourself. I would certainly not react to it. Because they could use it
against you. They could even ask that particular colleague ‘Do you know what your colleague
says about you?’ You never know. No, no. Hear all, see all, say nothing. That’s what you should
do..."
Furthermore, nurses talked about how they communicated with their colleague when a patient
reproached them for a “mistake” they made. A difference was observed regarding the kind of “mistake”
the colleague made. Nurses described examples of mistakes relating to nursing tasks, for instance,
leaving a bedpan which was not emptied in the room or serving dishes wrongly, as well as mistakes
related to communication with patients, for instance, a patient was berated, or insulted by a nurse. When
the mistake was related to nursing tasks, nurses said they usually used “humour” to talk to a colleague
about that mistake. They made a witty remark or joke about the incident.
"...When I saw her in the corridor, I said ‘Did you forget to remove that bedpan? I will tuck them
in now, okay?’ I said this while laughing. But <<laughs>> Yes, I said that while laughing"..."
Most of the nurses tended to spare colleagues or tried to avoid talking directly about the “mistake”. This
indirect communication was also used for incidents, where a colleague made a “mistake” relating to
communication with patients. Several nurses said especially in those situations it was difficult to talk
about “mistakes” with the colleague involved. Nurses explained that talking to colleagues about mistakes
Influence of team members on perceptions of transgressive behaviour
153
would create tension and this causes problems because they still had to collaborate. Most of the nurses
said they informed the head nurse in such situations and asked them to clear up the incident with the
colleague. Some nurses added it was the head nurse’s task to discuss such matters and as a result,
nurses tended to talk about their experiences with the head nurse instead of with colleagues.
"...I didn’t say that directly to my colleague, but I told the head nurse. I mentioned it in passing
and said: ‘When you have the time, you should talk to that colleague about the incident, to calm
them down.’ If the situation is really delicate, I will speak with my head nurse... "
3.1. | Integration: To what end are these actions towards colleagues directed?
The four abovementioned actions in the interaction with nursing’ team members display an underlying
dynamic. This dynamic will be further explained and clarified in a cyclic process.
A certain vigilance appears to be present in nurses’ dealings with patients. Essentially, perceptions of
transgressive behaviour occur individually with personal contact between the patient and the nurse. As
such, transgressive behaviour is connected to the individual vulnerability of nurses. The nurse feels
insulted, accused or hurt by the transgressive behaviour of the patient. This experience causes the
nurse to search for a colleague to be able to vent, find support and not blame herself, or to let a colleague
fill in for her in providing care for the patient. At the same time, patient’s transgressive behaviour causes
the nurse to feel insulted “as a person” but, simultaneously, feel threatened “as a group of nurses”.
Nurses seem to transfer or picture themselves in two congruent perspectives: their own perspective and
the perspective of the nursing team. Moreover, both perspectives exist in parallel. This means that
experiences of individual nurses virtually “become” experiences of the nursing team which means that
experiences of transgressive behaviour are both shared and transferred. That way, experiences of
colleagues are regarded as each nurse’s very own experiences. Sharing, transferring and adopting
experiences results in the labelling of patients or the adoption of the same kind of approach towards
patients. Simultaneously, it results in nurses self-evidently venting among themselves, self-evidently
excusing one another, self-evidently filling in for one another, informing and warning one another, etc.
Accordingly, in these dynamics, the group of nurses acquires its identity “as a group”. Protecting the
group and subsequently gaining protection of the group, becomes an important implicit focus of
individual nurses; meanwhile protecting and preserving the group becomes a shared unspoken focus of
nursing teams. Protecting the group and putting the group at the forefront also implies that nurses
conform for the sake of preserving the proper functioning of the group. This implies the avoidance of
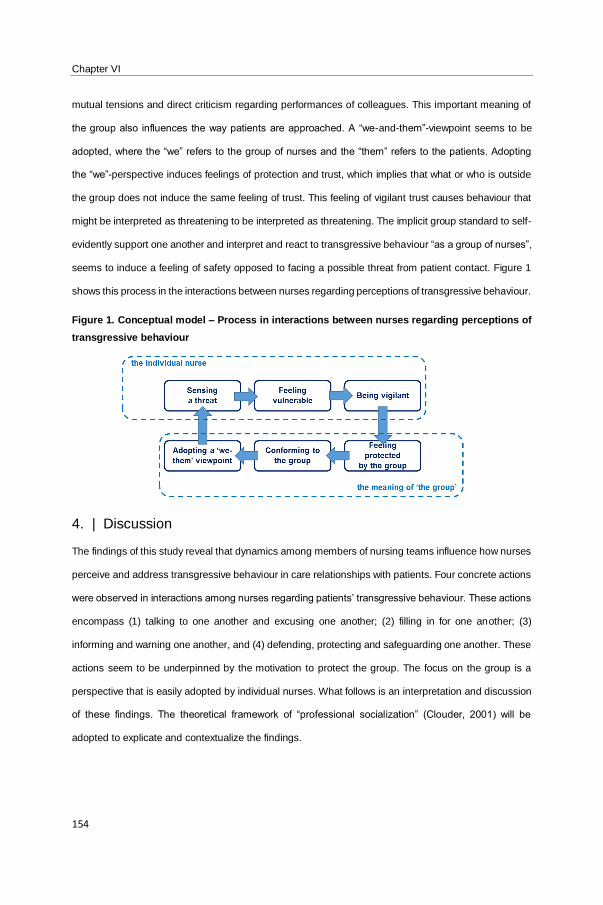
Chapter VI
154
mutual tensions and direct criticism regarding performances of colleagues. This important meaning of
the group also influences the way patients are approached. A “we-and-them”-viewpoint seems to be
adopted, where the “we” refers to the group of nurses and the “them” refers to the patients. Adopting
the “we”-perspective induces feelings of protection and trust, which implies that what or who is outside
the group does not induce the same feeling of trust. This feeling of vigilant trust causes behaviour that
might be interpreted as threatening to be interpreted as threatening. The implicit group standard to self-
evidently support one another and interpret and react to transgressive behaviour “as a group of nurses”,
seems to induce a feeling of safety opposed to facing a possible threat from patient contact. Figure 1
shows this process in the interactions between nurses regarding perceptions of transgressive behaviour.
Figure 1. Conceptual model – Process in interactions between nurses regarding perceptions of
transgressive behaviour
4. | Discussion
The findings of this study reveal that dynamics among members of nursing teams influence how nurses
perceive and address transgressive behaviour in care relationships with patients. Four concrete actions
were observed in interactions among nurses regarding patients’ transgressive behaviour. These actions
encompass (1) talking to one another and excusing one another; (2) filling in for one another; (3)
informing and warning one another, and (4) defending, protecting and safeguarding one another. These
actions seem to be underpinned by the motivation to protect the group. The focus on the group is a
perspective that is easily adopted by individual nurses. What follows is an interpretation and discussion
of these findings. The theoretical framework of “professional socialization” (Clouder, 2001) will be
adopted to explicate and contextualize the findings.
Influence of team members on perceptions of transgressive behaviour
155
4.1. | Interpretation and discussion of the findings
When nurses encounter transgressive behaviour, they are inclined to approach a colleague to express
their emotions. In addressing the feeling of threat or insult caused by patient’s transgressive behaviour,
nurses seek out a colleague to find support and vent, thus bringing these taxing emotions back to
manageable levels. This example of social coping encompasses the search for social support in solving
problems (Lazarus & Folkman, 1984; Schreuder et al., 2011). Searching social support has been
described in a review on coping strategies of victims of aggression in healthcare (Edward, Ousey,
Warelow, & Lui, 2014). Edward et al. (2014) concluded it is important for nurses to feel safe and
supported when they experience aggression. Present findings confirmed this kind of support is obtained
by interacting with colleagues. In a context of professional socialization, this interaction can be
understood as a form of “attachment” as colleagues represent figures to turn to during times of stress to
find comfort and support, who diminish anxiety (Clouder, 2001). Colleagues respond by telling the nurse
it is not their fault, as she or he did nothing wrong, the patient is to blame or they themselves experienced
similar incidents. However, this kind of interaction induces certain group dynamics and even group
“norms”. For instance, the inclination of nurses to react to transgressive behaviour in a rather evasive
way, is reinforced by easily finding support in interacting with colleagues. While on the other hand, by
excusing and praising one another after transgressive behaviour, colleagues support the evasive way
of handling transgressive behaviour. This interaction induces or maintains a certain professional norm,
asserting it is alright to avoid patients after incidents, not blame oneself, nor feel personally responsible.
Furthermore, a colleague’s approach of self-evidently filling in for another nurse, dismissing and avoiding
exploration of incidents induces a professional norm suggesting it is important not to dwell on such
incidents and to let go of one’s own feelings of vulnerability. Steege and Rainbow (2017) suggest this
interaction might be part of the nursing professional culture because of the value placed on portraying
an image of strength and invulnerability to colleagues and patients. These group norms can also be
understood from a social constructionist perspective on professional socialization as they refer to shared
understandings of what it means to be a professional person (Clouder, 2001). The idea that a nurse
should not react to transgressive behaviour because it may lead to an escalation of the incident seems
to be a shared notion in nursing teams. Communicating with patients about transgressive behaviour is
not considered to be a solution, a finding confirmed in literature (Vandecasteele et al., 2015). Literature
on socializing processes in nursing teams might add to this finding, as appearing to be busy seems to
Chapter VI
156
be part of the ward culture, while talking to patients is not considered to constitute working (Mooney,
2007). Moreover, the belief that communication can only make things worse suggests an appraisal of
the kind of communication suitable for responding to transgressive behaviour. Burnard and Morrison
(2005) studied different communication styles used by nurses, differentiating between authoritative (i.e.
prescribing, confronting, instructing) and facilitative interventions (catharsis, stimulating reflection,
offering support). Nurses mostly adopted authoritative interventions (Burnard & Morrison, 2005). If
nurses feel most comfortable adopting an authoritative communication style, the belief that
communication about transgressive behaviour can only lead to an escalation appears logical. This
perception might explain why reactions to transgressive behaviour occur as short-term interventions,
that is, avoiding the patient, venting among colleagues, or filling in for one another. These interactions
and the group norms that arise from them, seem to suggest a specific meaning of “the group” for nursing
teams. The need to belong to a team (Secrest, Norwood, & Keatley, 2003), become an insider (Feng &
Tsai 2012), or become accepted in the profession (Bisholt 2012) has been described in literature on
professional socialization. In this study, these needs imply that nurses, on encountering transgressive
behaviour, feel threatened as an individual and at the same time, as a group of nurses. This threat as a
group of nurses generates the adoption of an “us-vs.-them” perspective that reinforces perceptions of
patients as “outsiders” when they display transgressive behaviour. This construction of the “us”
perspective can be a result of the process of socialization into the profession (Clouder, 2001). This
interaction is seen in this study’s findings on labelling of patients. Labels of “difficult patient” were
adopted, shared and transferred. This labelling can suggest a form of moral disengagement (Bandura,
2002), a process which has been studied in the context of nurses (Fida et al., 2016). In Koekkoek,
Hutschemaekers, van Meijel, & Schene (2011), the process of labelling patients as “difficult” is described
in mental healthcare and can be understood in the context of influential research on “the unpopular
patient” (Johnson & Webb, 1995; Stockwell, 1972). Adopting the perspective of the group of nurses and
hence protecting one another, also seems to motivate nurses to conform to informal group rules. For
instance, not criticizing one another regarding interpersonal communication with patients seems to be
an informal rule. This process of conformity is an aspect of professional socialization as internalizing
values and beliefs of members of the profession subjects individuals to social control (Clouder, 2001).
Batch and Windsor (2015) found similar results, as speaking out or reacting in any way other than the
expected manner carried the risk of being identified as a troublemaker and resulted in poor

Influence of team members on perceptions of transgressive behaviour
157
communication among nurses (Batch & Windsor, 2015). Similarly, avoiding one another was identified
as the most commonly used conflict management style of nurses in nursing conflict (Cavanagh, 1991;
Valentine, 2001), a style presumed to maintain harmony and preserve interpersonal relationships
(Valentine, 2001).
4.2. | Implications for policy and practice
It appears imperative that a better understanding and a specific acknowledgement of these team
dynamics might lead organizations to consider these interactions when planning interventions to support
nurses in perceiving and handling transgressive behaviour. Such acknowledgement is important, as
these dynamics presumably have an impact on the quality of patient care. Although these findings were
generated based on nurses’ perspectives, consequences of such team dynamics for patient care can
be hypothesized. Koekkoek et al. (2011) described a tentative model showing how patients and
professionals can reinforce each other’s ineffective behaviour based on their previous attributions and
enter vicious circles of ineffective communication. Similarly, when nurses avoid contact with patients or
label patients, patients might feel frustrated, ignored and hurt, which might cause them to escalate their
behaviour to gain nurses’ attention (Brunero & Lamont, 2010). At the same time, these interactions in
nursing teams include no exploration of what makes transgressive behaviour “understandable” (Stone,
McMillan, & Hazelton, 2015) which increases the risk experiences and seriousness of the transgressive
behaviour will be amplified. As an implication for practice, interventions to support nurses and nursing
teams in processing transgressive behaviour in care relationships should be implemented on a team
level, incorporating the culture of the ward and the dynamics of teams. In the geriatric (Zeller et al.,
2009) and mental healthcare setting (Björkdahl, Hansebo, & Palmstierna, 2013; Bowers, 2014),
initiatives and interventions have been carried out on this group level. Reflecting in group on experiences
of transgressive behaviour while contemplating interactions and communication with patients,
apprehending patient’s behaviour and becoming aware of one’s own implicit personal emotions seem
to be very important in achieving a reflective nursing practice.
4.3. | Study limitations
There were some limitations in relation to data collection. Data collection was limited to individual and
focus-group interviews only. Observations of nursing teams might have generated an additional
understanding of the dynamics of perceiving transgressive behaviour in care relationships with patients,
as it would have provided access to the ways nurses act and interact (Aitken, Marshall, Elliott, &

Chapter VI
158
McKinley, 2011). However, verbal accounts of nurses proved to provide an in-depth and comprehensive
representation of how nurses perceive and address transgressive behaviour. Similarly, conducting
focus-group interviews allowed to gain tentative access to interactions of nurses in conversing with one
another regarding experiences of transgressive behaviour.
5. | Conclusion
This study complements existing knowledge on nurses’ experiences regarding aggression and
transgressive behaviour in healthcare. The study notes how nurses are influenced by team members in
perceiving and handling patients’ transgressive behaviour. Certain group dynamics and the emergence
of group norms have been identified to impinge these interactions. An important finding of this study
relates to the shared focus among nurses on the protection and preservation of the group. The latter
focus among nurses is underpinned by a process of professional socialization in nursing teams
regarding the conduct towards patients.
Influence of team members on perceptions of transgressive behaviour
159
REFERENCES
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Fischer, J. E., & Haug, H. J. (2007). Frequency and severity
of aggressive incidents in acute psychiatric wards in Switzerland. Clinical Practice and Epidemiology in Mental
Health, 4, 3–30.
Aitken, L. M., Marshall, A., Elliott, R., & McKinley, S. (2011). Comparison of ‘think aloud’ and observation as data
collection methods in the study of decision making regarding sedation in intensive care patients. International
Journal of Nursing Studies, 48(3), 318–325.
Almvik, R., Rasmussen, K., & Woods, P. (2006). Challenging behaviour in the elderly: Monitoring violent incidents.
International Journal of Geriatric Psychiatry, 21(4), 368–374.
Bandura, A. (2002). Selective moral disengagement in the exercise of moral agency. Journal of Moral Education,
32(2), 101–119.
Batch, M., & Windsor, C. (2015). Nursing casualization and communication: A critical ethnography. Journal of
Advanced Nursing, 71(4), 870–880.
Benner, P. (1984). From novice to expert: Excellence and power in clinical nursing practice. Menlo Park: Addison-
Wesley Publishing Company.
Bisholt, B. K. (2012). The professional socialization of recently graduated nurses–experiences of an introduction
program. Nurse Education Today, 32(3), 278–282.
Björkdahl, A., Hansebo, G., & Palmstierna, T. (2013). The influence of staff training on the violence prevention and
management climate in psychiatric inpatient units. Journal of Psychiatric and Mental Health Nursing, 20(5), 396–
404.
Bowers, L. (2014). Safewards: A new model of conflict and containment on psychiatric wards. Journal of Psychiatric
and Mental Health Nursing, 21(6), 499–508.
Brunero, S., & Lamont, S. (2010). The ‘difficult’ nurse-patient relationship: Development and evaluation of an e-
learning package. Contemporary Nurse, 35(2), 136–146.
Burnard, P., & Morrison, P. (2005). Nurses’ perceptions of their interpersonal skills: A descriptive study using six
category intervention analysis. Nurse Education Today, 25(8), 612–617.
Cavanagh, S. J. (1991). Conflict management style of staff nurses and nurse managers. Journal of Advanced
Nursing, 16(10), 1254–1260.
Clouder, D. L. (2001) Becoming professional: An exploration of the social construction of identity. Thesis Submitted
for the Degree of PhD at the University of Warwick.
Cox, K. B. (2001). The effects of unit morale and interpersonal relations on conflict in the nursing unit. Journal of
Advanced Nursing, 35(1), 17– 25.
Chapter VI
160
Duxbury, J. (2002). An evaluation of staff and patient views of and strategies employed to manage inpatient
aggression and violence on one mental health unit: A pluralistic design. Journal of Psychiatric and Mental Health
Nursing, 9(3), 325–337.
Duxbury, J., Pulsford, D., Hadi, M., & Sykes, S. (2013). Staff and relatives’ perspective on the aggressive behavior
of older people with dementia in residential care: A qualitative study. Journal of Psychiatric and Mental Health
Nursing, 20(9), 792–800.
Duxbury, J., & Whittington, R. (2005). Causes and management of patient aggression and violence: Staff and
patient perspectives. Journal of Advanced Nursing, 50(5), 469–478.
Edward, K. L., Ousey, K., Warelow, P., & Lui, S. (2014), Nursing and aggression in the workplace: A systematic
review. British Journal of Nursing, 23(12), 653–654, 656-9.
Farrell, G. A., Bobrowski, C., & Bobrowski, P. (2006). Scoping workplace aggression in nursing: Findings from an
Australian study. Journal of Advanced Nursing, 55(6), 778–787.
Feng, R. F., & Tsai, Y. F. (2012). Socialisation of new graduate nurses to practising nurses. Journal of Clinical
Nursing, 21(13–14), 2064–2071.
Fida, R., Tramontano, C., Paciello, M., Kangasniemi, M., Sili, A., Bobbio, A., & Barbaranelli, C. (2016). Nurse moral
disengagement. Nursing Ethics, 23(5), 547–564.
Funkesson, K. H., Anbäcken, E. M., & Ek, A. C. (2007). Nurses’ reasoning process during care planning taking
pressure ulcer prevention as an example. A think-aloud study. International Journal of Nursing Studies, 44(7), 1109–
1119.
Gerberich, S. G., Church, T. R., McGovern, P. M., Hansen, H., Nachreiner, N. M., Geisser, M. S., Jurek, A. (2005).
Risk factors for work-related assaults on nurses. Epidemiology, 16(5), 704–709.
Gerdtz, M. F., Daniel, C., Dearie, V., Prematunga, R., Bamert, M., & Duxbury, J. (2013). The outcome of a rapid
training program on nurses’ attitudes regarding the prevention of aggression in emergency departments: A multi -
site evaluation. International Journal of Nursing Studies, 50(11), 1434–1445.
Glaser, B. G., & Strauss, A. (1967). The discovery of grounded theory. Chicago, IL: Adline Atherton.
Hahn, S., Müller, M., Hantikainen, V., Kok, G., Dassen, T., & Halfens, R. J. G. (2013). Risk factors associated with
patient and visitor violence in general hospitals: Results of a multiple regression analysis. International Journal of
Nursing Studies, 50(3), 374–385.
Hahn, S., Zeller, A., Needham, I., Kok, G., Dassen, T., & Halfens, R. J. G. (2008). Patient and visitor violence in
general hospitals: A systematic review of the literature. Aggression and Violent Behavior, 13(6), 431–441.
Hallberg, L. R. M. (2006). The ‘core category’ of grounded theory: Making constant comparisons. International
Journal of Qualitative Studies on Health and Well-Being, 1(3), 141–148.
Influence of team members on perceptions of transgressive behaviour
161
Heckemann, B., Zeller, A., Hahn, S., Dassen, T., Schols, J. M., & Halfens, R. J. (2015). The effect of aggression
management training programmes for nursing staff and students working in an acute hospital setting. A narrative
review of current literature. Nurse Education Today, 35(1), 212–219.
Jansen, G. J., Dassen, T. W., & Groot Jebbink, G. (2005). Staff attitudes towards aggression in health care: A
review of the literature. Journal of Psychiatric and Mental Health Nursing, 12(1), 3–13.
Johnson, M., & Webb, C. (1995). Rediscovering unpopular patients: The concept of social judgement. Journal of
Advanced Nursing, 21(3), 466–475.
Koekkoek, B., Hutschemaekers, G., van Meijel, B., & Schene, A. (2011). How do patients come to be seen as
‘difficult’?: A mixed-methods study in community mental health care. Social Science & Medicine, 72(4), 504–512.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer.
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Beverly Hills, CA: Sage.
Luck, L., Jackson, D., & Usher, K. (2008). Innocent or culpable? Meanings that emergency department nurses
ascribe to individual acts of violence. Journal of Clinical Nursing, 17(8), 1071–1078.
Maben, J., Latter, S., & Clark, J. M. (2006). The theory–practice gap: Impact of professional–bureaucratic work
conflict on newly-qualified nurses. Journal of Advanced Nursing, 55(4), 465–477.
Malterud, K. (2001). Qualitative research: Standards, challenges and guidelines. The Lancet, 358(9280), 483–488.
Mantzouranis, G., Fafliora, E., Bampalis, V. G., & Christopoulou, I. (2015). Assessment and analysis of workplace
violence in a Greek Tertiary Hospital. Archives of Environmental & Occupational Health, 70(5), 256–264.
May, D. D., & Grubbs, L. M. (2002). The extent, nature and precipitating factors of nurse assault among three
groups of registered nurses in a regional medical center. Journal of Emergency Nursing, 28(1), 11–17.
Mooney, M. (2007). Professional socialization: The key to survival as a newly qualified nurse. International Journal
of Nursing Practice, 13(2), 75–80.
Morse, J., & Field, P. A. (1996). Nursing research. The application of qualitative approaches. London, UK: Chapman
& Hall.
Needham, I., Abderhalden, C., Halfens, R. J. G., Fischer, J. E., & Dassen, T. (2005). Non-somatic effects of patient
aggression on nurses: A systematic review. Journal of Advanced Nursing, 49(3), 283–296.
Pich, J., Hazelton, M., Sundin, D., & Kable, A. (2011). Patient-related violence at triage: A qualitative descriptive
study. International Emergency Nursing, 19(1), 12–19.
Rippon, T. J. (2000). Aggression and violence in health care professions. Journal of Advanced Nursing, 31(2), 452–
460.
Chapter VI
162
Roche, M., Diers, D., Duffield, C., & Catling-Paull, C. (2010). Violence toward nurses, the work environment and
patient outcomes. Journal of Nursing Scholarship, 42(1), 13–22.
Sato, K., Wakabayashi, T., Kiyoshi-Teo, H., & Fukahori, H. (2013). Factors associated with nurses’ reporting of
patients’ aggressive behavior: A cross-sectional survey. International Journal of Nursing Studies, 50(10), 1368–
1376.
Schreuder, J. A., Plat, N., Magerøy, N., Moen, B. E., van der Klink, J. J., Groothoff, J. W., & Roelen, C. A. (2011).
Self-rated coping styles and registered sickness absence among nurses working in hospital care: A prospective 1-
year cohort study. International Journal of Nursing Studies, 48(7), 838–846.
Secrest, J. A., Norwood, B. R., & Keatley, V. M. (2003). ‘I was actually a nurse’: The meaning of professionalism
for baccalaureate nursing students. The Journal of Nursing Education, 42(2), 77–82.
Simmons, B., Lanuza, D., Fonteyn, M., Hicks, F., & Holm, K. (2003). Clinical reasoning in experienced nurses.
Western Journal of Nursing Research, 25(6), 701–719.
Spector, P. E., Zhou, Z. E., & Che, X. X. (2014). Nurse exposure to physical and nonphysical violence, bullying and
sexual harassment: A quantitative review. International Journal of Nursing Studies, 51(1), 72–84.
Steege, L. M., & Rainbow, J. G. (2017). Fatigue in hospital nurses - ‘Supernurse’ culture is a barrier to addressing
problems: A qualitative interview study. International Journal of Nursing Studies, 67, 20–28.
Stevenson, K. N., Jack, S. M., O’Mara, L., & LeGris, J. (2015). Registered nurses’ experiences of patient violence
on acute care psychiatric inpatient units: An interpretive descriptive study. BMC Nursing, 17, 14–35.
Stockwell, F. (1972). The unpopular patient. London: RCN.
Stone, T. E., McMillan, M., & Hazelton, M. (2015). Back to swear one: A review of English language literature on
swearing and cursing in Western health settings. Aggression and Violent Behavior, 25(Part A), 65–74.
Trotter, R. T. (2012). Qualitative research sample design and sample size: Resolving and unresolved issues and
inferential imperatives. Preventive Medicine, 55(5), 398–400.
Trysoe, L., Hounsgaard, L., Dohn, N. B., & Wagner, L. (2012). Newly qualified nurses–experiences of interaction
with members of a community of practice. Nurse Education Today, 32(5), 551–555.
Valentine, P. E. B. (2001). A gender perspective on conflict management strategies of nurses. Journal of Nursing
Scholarship, 33(1), 69–74.
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D., & Verhaeghe, S. (2015). Nurses’
perceptions of transgressive behaviour in care relationships: A qualitative study. Journal of Advanced Nursing,
71(12), 2786–2798.
Wahl, K. (2009) Aggression und Gewalt. Ein biologischer, psychologischer und sozialwissenschaftlicher Uberblick.
Heidelberg: Spektrum Akademischer Verlag.

Influence of team members on perceptions of transgressive behaviour
163
Wei, C. Y., Chiou, S. T., Chien, L. Y., & Huang, N. (2016). Workplace violence against nurses - Prevalence and
association with hospital organizational characteristics and health-promotion efforts: Cross-sectional study.
International Journal of Nursing Studies, 56, 63–70.
Winstanley, S. (2005). Cognitive model of patient aggression towards health care staff: The patient’s perspective.
Work & Stress: An International Journal of Work, Health & Organisations, 19(4), 340–350.
Winstanley, S., & Whittington, R. (2004). Aggressive encounters between patients and general hospital staff: Staff
perceptions of the context and assailants’ levels of cognitive processing. Aggressive Behavior, 30(6), 534–543.
Yarbrough, S., Martin, P., Alfred, D., & McNeill, C. (2016), Professional values, job satisfaction, career development
and intent to stay. Nursing Ethics, 1-11.
Zeller, A., Hahn, S., Needham, I., Kok, G., Dassen, T., & Halfens, R. J. G. (2009). Aggressive behavior of nursing
home residents toward care-givers: A systematic literature review. Geriatric Nursing, 30(3), 174–187.

General discussion
164
General discussion
165
Chapter VII.
GENERAL DISCUSSION
Ring the bells that still can ring.
Forget your perfect offering.
There is a crack in everything.
That's how the light gets in.
L. Cohen

Chapter VII
166
General discussion
167
1. | Introduction
This dissertation addressed how nurses and patients experience the care relationship with one another
in a context of experiencing and perceiving aggression and transgressive behaviour. In addition, the
influence of team members on nurses’ perceptions of aggression and transgressive behaviour was
explored.
This general discussion will start with an introduction on the concept of ‘transgressive behaviour’ as an
important aspect or starting-point in understanding aggression in care relationships. Subsequently,
some key findings of this dissertation will be addressed. Reiterating discussion points of previous
chapters shall be limited to a minimum to avoid duplication. Some reflections on a wider context of care
relationships between nurses and patients will be presented to situate the findings in a broader
perspective. Implications and recommendations for nursing practice and nursing management will be
addressed, and methodological considerations and recommendations for further research will complete
this general discussion.
2. | The merit of adopting the concept of ‘transgressive behaviour’
In the introduction of this dissertation, a distinction between a more objectifying and a subjectifying
approach towards aggression was made. The strongest difference between both approaches lies in the
way aggression is understood and conceptualized. Using an objectifying approach, aggression would
be defined which definition would allow discrimination between that which is aggressive behaviour and
that which is non-aggressive behaviour (Voyer et al., 2005; Hahn et al., 2013; Swain & Gale, 2014).
Whereas a subjectifying approach of aggression tries to take into account the specific context and
assigned meaning of aggression by using the perspectives of the persons involved as starting-points.
In the studies described in chapter II and III, an objectifying approach was adopted in examining nurses’
experiences of patient aggression and aggression by patients’ family members in primary care and in
general hospital settings. Different aspects of aggression in nursing practice were addressed by using
a translated and validated version of the Survey of Violence experienced by Staff (McKenna, 2004;
Hahn et al., 2011). Three manifestations of aggression in nursing practice were explored: verbal
aggression, physical aggression and threats, and in line with other research, these studies emphasized
and stressed how aggression is an important problem and concern for nurses irrespective of their work
setting (Hahn et al., 2013; Spector, Zhou, & Che, 2014; Hanson et al., 2015). In these studies, there
Chapter VII
168
was not only a focus on the prevalence and manifestation of aggression, but also on nurses’ perceptions
of aggression and its management. To examine perceptions of aggression, two translated and validated
instruments, the shortened Perception of Aggression Scale (Jansen, Dassen, & Moorer, 1997;
Abderhalden et al., 2002; Needham et al., 2004; Hahn et al., 2011), and the Perception of Importance
of Intervention Skills Scale (Hahn et al., 2011), were used. Based on these instruments, most nurses
were inclined to perceive aggression as a dysfunctional and as an undesirable phenomenon. Several
factors on the level of nurses’ characteristics, nurses’ exposure to aggression, patients’ and family
members’ characteristics, practice characteristics and organisational characteristics were identified to
be associated with nurses’ perceptions of aggression and its management. These different associations
suggest a complicated underlying process in how aggression is perceived as the rationale for some
associations were assumptions in absence of explanatory evidence (Abderhalden et al., 2002). The
objectifying approach towards the concept of aggression was valuable to gain an indication and
description of aggression in care relationships, but restrictive in understanding how perceptions of
aggression occur or take place in interactions with patients or their family members. A critical question
concerns the extent to which a complex and contextually bound concept such as perceptions of
aggression can be operationalized into measurement instruments. The division between perceiving
aggression as a functional or as a dysfunctional phenomenon is too limited, and underestimates the
complexity and contextual dependency of how perceptions of aggression emerge. Consequently, it is
important to enable an understanding of the underlying processes that are present in perceiving
aggression. A more subjectifying approach in trying to understand rather than explain aggression was
found in adopting the concept of transgressive behaviour. This concept allowed an individual
interpretation by both nurses and patients of when and what limits are exceeded in the interaction with
one another without defining these limits in advance. The concept transgressive behaviour emerges
from the different studies as a complex, contextually dependent and relational process in which both
nurses and patients participate in their unique way. All studies point out how behaviour in itself does not
determine ‘what’ is experienced as transgressive. Interviewing nurses and patients concerning their
perceptions of transgressive behaviour, and adopting their representations of their experiences captured
how both nurses and patients give meaning to transgressive behaviour. An underlying process in both
nurses’ and patients’ perceptions of transgressive behaviour emerged and was identified.
General discussion
169
Adopting the concept of transgressive behaviour allowed to address the meaning of transgressive
behaviour from the patient’s perspective (chapter IV). Patients appeared to adopt a framework of
suppositions which generates implicit ideas or assumptions about hospital care and nurse-patient
relationships. Hence, patients envisage receiving competent care and having human interactions with
nurses. These assumptions are implicit, and awareness of these assumptions occurs when patients
experience envisaged care or nurse-patient relationships are not met in their perceived reality.
Experiencing these discrepancies gives rise to a process of adaption, and several patterns are put into
action: patients become more vigilant with regard to care given by nurses; they search for own solutions;
they make excuses for nurses or they reprioritize their expectations. As such, patients go through both
a cognitive and emotional process in adjusting their assumptions or behaviour. Due to these processes,
experiences of transgressive behaviour are put into perspective. The transgressive aspect of
experiencing transgressive behaviour is ‘addressed’ by patients themselves by adopting different
patterns of adjustment.
Subsequently, the onset and meaning of transgressive behaviour from the nurses’ perspective was
explored (chapter V). These findings revealed that nurses’ experiences of transgressive behaviour were
associated with determining and regulating factors. These factors affect which incidents are perceived
as transgressive and what meaning is assigned to them. The degree of control that nurses experience
over the provision of care, the degree of patient acceptance of organizational and ward rules, the degree
of gratitude and recognition expressed by the patient and the extent of patient regard for the nurse as a
person were identified as determining factors. As regulating factors, the extent of a trusting relationship
between patients and nurses, the extent to which the patient’s perspective is understood, the way
transgressive behaviour is managed by nurses and the roles of the nursing team and head nurse and
ward culture and habits, were identified. These different factors appeared to be connected to one
another and were responsible for particular dynamics in maintaining, reinforcing, or decreasing
experiences of transgressive behaviour.
In putting these findings on the nurses’ perspective in a broader perspective, the group dynamics in
nursing teams regarding patients’ transgressive behaviour were examined (chapter VI). Different
patterns of interactions were observed in nursing teams following experiences of transgressive
behaviour: nurses talked to and excused one another; filled in for one another; informed and warned
one another; and defended, protected and safeguarded one another. These patterns in reaction to

Chapter VII
170
patients’ transgressive behaviour seem to be underpinned by the motivation to protect the group. In
these interactions, implicit group norms transpire, causing nursing teams to acquire their specific identity
“as a group”. These informal group norms in nursing teams appeared to impinge how nurses feel
threatened by patients’ potential transgressive behaviour; gain protection from the group of nurses and
conform to informal ward rules.
These insights into nurses’ and patients’ experiences, and dynamics in nursing teams allowed to obtain
a tentative, but reasonable representation of what occurs in care relationships in a context of
transgressive behaviour. One can question whether these insights render the possibility to formulate a
precise definition of transgressive behaviour as it is customary in research to comprehensively define
the phenomenon under research since a definition can function as a basis for further research and
theory construction (Brüggemann, 2012). Our insights on the concept of transgressive behaviour do not
result in a theoretical definition, nor in an autonomous theory. Our insights make up a theoretical
framework, amenable to modification, which situates transgressive behaviour in a context of care
relationships between nurses and patients. This theoretical framework entails an abstract notion and
understanding of what transgressive behaviour is or constitutes, and this abstract notion of a concept
does induce additional challenges. It can be argued that highly abstract concepts may overlap with other
concepts to a large extent, which makes it difficult to identify the uniqueness of such concepts (Benzein
& Saveman, 1998). For instance, the concept of transgressive behaviour might be expected to overlap
to concepts as abuse (Brüggemann, 2012) and assault (May & Grubbs, 2002; Winstanley & Whittington,
2002; Renwick et al., 2016). However, as Brüggemann (2012) states, trying to obtain uniformity in
defining concepts might dismiss any kind of contradiction or exception which may actually hamper
theoretical development within the field. Therefore it seems to be more interesting to, instead of defining
transgressive behaviour which is an exclusive process, describe transgressive behaviour which is an
inclusive process (Benzein & Saveman, 1998). This approach allowed us in our studies to describe
transgressive behaviour from both the patients’ and nurses’ perspective without defining in advance
what or what not constituted transgressive behaviour. This meant that patients’ and nurses’ experiences
of transgressive behaviour provided the starting-point in our analyses. Because of this -rather inductive-
starting-point, a large diversity was observed in the nature of the experiences of transgressive behaviour
from both the nurses’ and the patients’ perspective. Focusing on specific behaviour that was reported
as an experience of transgressive behaviour would not had rendered an understanding of why and how
General discussion
171
something was experienced as a transgression. As such, it was important to explore the explanatory
underlying processes of how experiences of transgressive behaviour emerge and search for an
understanding of what transgressive behaviour means in care relationships. What follows are some
findings on the connection between the nurses’ and the patients’ perspective in perceiving transgressive
behaviour in care relationships.
3. | Connecting the nurses’ and the patients’ perspective on
transgressive behaviour in care relationships
There are some findings that seem to take on a prominent role from both the nurses’ and the patients’
perspective. These findings pertain to the process of adapting to one’s environment, the importance of
maintaining the organisation of care, and -on a more abstract level- a reciprocal reinforcing process in
nurses’ and patients’ perceptions of transgressive behaviour.
The process of adapting to one’s environment. Findings on nurses’ and patients’ experiences and
perceptions of transgressive behaviour indicate that both nurses and patients appear to adapt or
conform to their specific environment and context. This process of adaptation is characterized by an
alteration of own behaviour or cognitions based on what both patients and nurses experience in their
interactions with others. Consequently, this alteration of behaviour or cognitions presumes an
interpretation of what someone else expects or imposes. Nurses’ perceptions of transgressive behaviour
were shaped by and became similar to the perceptions of other nurses on the same ward, including
patients’ behaviour perceived as transgressive, aspects influencing these perceptions and
consequences of these perceptions on care relationships with patients. Nurses adapted their coping
styles with patient’s transgressive behaviour to the culture of their particular ward. This identified
alteration on the nurses’ level was contextualized in a process of professional socialisation (Clouder,
2001), which entails processes in which nurses adapt to what is common practice in the nursing team
they are part of. Dynamics in the interactions between nurses appear to be underpinned by a shared
focus on the protection and proper functioning of ‘the group’. For the sake of the group, nurses
conformed to implicit group norms and standards.
In addition, the ways in which patients adapted to their environment were quite prominent. Different
patterns were observed, and these patterns display different manners in which patients adapt to their
Chapter VII
172
context on the nursing ward. Patients adopted a more vigilant, alert and sceptical attitude as an
adaptation or answer to the perception that nurses’ professional competencies were questionable.
When patients encountered untoward needs in contact with nurses during previous hospital admissions,
patients appeared to become more vigilant and stern in subsequent contacts with nurses. On a similar
level, the pattern of finding own solutions is another example of the ways in which patients adapt to their
context. Experiencing untoward needs in contact with nurses entailed this adjustment. They no longer
expected nurses to respond to their specific needs as they themselves already took care of their own.
Another pattern that was observed in patients was the minimizing of expectations and the ‘excusing’
attitude towards nurses. The processes underpinning these patients’ responses to what they experience
in care relationships with nurses, have been acknowledged in literature (Price, 2011; Maben et al., 2012;
McCabe, 2004).
The motives or reasons to adapt to one’s specific environment differ according to the nurses’ and the
patients’ perspective. From the nurses’ perspective, conforming to group norms and standards in the
nursing team ensures they gain protection. Adhering to the common ways of thinking about the conduct
towards patients in a context of transgressive behaviour induces feelings of safety as this conventional
thinking and acting according to the group identity generates a ‘safe haven’ for nurses. In contrast,
patients’ motives to adapt to their specific context appears to be connected to a motivation ‘to weather
through’ the hospital admission. In literature, this process is also described as ‘surviving the hospital
stay’ (Jacelon, 2004). The pattern of establishing priorities in response to untoward needs in contact
with nurses can be understood in this regard. Patients established priorities when both their expectations
to receive competent care and to experience normal human interactions with nurses were not met. As
a consequence, patients judged nurse’s professional competencies to be more important than
interpersonal contacts with nurses. In judging what was worst, patients considered what was most
relevant to them personally, or was most threatening on a personal level. Actively focusing on personal
health as of primary importance in a context of impaired dignity, is recognized in literature (Jacelon,
2004). This particular pattern of minimizing expectations of encountering normal human interactions with
nurses, and focusing on receiving at least adequate professional competencies, was a prominent pattern
observed in the ways in which patients adapt or conform to what they experience during their hospital
admission.
General discussion
173
As part of this process of adapting and conforming to their context, both nurses and patients grew to
focus their attention to the organisation of care.
The importance of maintaining the organisation of care. In exploring both nurses’ and patients’
recollections of transgressive behaviour in care relationships, nurses and patients were found to put the
organisation of care in the foreground. The organisation of care is understood here as the proper
sequence or process of care tasks for all patients on the nursing ward to receive proper care.
Nurses’ considerations start off with the desire to be a ‘good nurse’, a motive that is recognized in
literature (Peter, Simmonds, & Liashenko, 2016). Being a good nurse means that care tasks are finished
in a limited time frame, which brings about a focus in everyday practice on more concrete tasks and the
rather technical side of nurses’ work. Appropriately completing these concrete care tasks seems to be
the nurses’ objective, and the nurses’ framework to assess own performances as a professional person
and as a ‘good nurse’. In this perspective, striving to be a good nurse gives rise to the expectation that
gratitude and recognition is yielded by the patients they care for. Recognition is sought for the proper
completion of care tasks. As such, nurses easily perceived patient’s behaviour as transgressive when
this recognition was lacking. Being interrupted in the execution of care tasks, being told they took too
long to answer patients’ call lights, not being acknowledged in striving to be a good nurse, easily induced
perceptions of patient’s transgressive behaviour. When patients’ recognition for nurses’ professional
role was lacking, which gives rise to a perception of transgressive behaviour, nurses were inclined to
search for recognition and confirmation in the contact with colleagues. In this interaction, colleagues
adopted an excusing attitude towards the nurse and confirmed his or her conduct towards the patient.
Colleagues commonly solved the incident by simply taking over care tasks and filling in for each other.
This solution is easily adopted as nurses seemed to share the focus on the proper completion of care
tasks and the proper maintenance of the organisation of care. The proper organisation of care thus
becomes a shared focus and a justification for their actions. These actions, in simply completing the
expected care tasks with the patient, can also be understood in the ‘we-and-them’-perspective that is
adopted, where the ‘we’ refers to the group of nurses, and the ‘them’ refers to the patients. Because of
this perspective, a focus on the organisation of care is justified, and there is no encouragement to try to
talk to patients about transgressive incidents. Short-term interventions in avoiding the patient, venting
among colleagues and filling in for one another as thus preferred, and a shared focus on the preservation
of the organisation of care is thus shared and consolidated. This approach in nursing teams in solving
Chapter VII
174
difficult incidents by adopting short-term interventions, might also explain why the majority of nurses
indicated to report none to a few of the aggressive incidents they encountered. The influence of group
dynamics might generate an additional understanding of the reasons why underreporting of aggressive
behaviour is prevalent (Sato et al. 2013).
These identified dynamics in nursing teams appeared to influence the patient’s perspective. As nurses
were focused on the proper organization of care, a conforming attitude of patients and family members
was expected. This meant that patients and family members were expected to conform and adapt to
informal and implicit rules and regulations of the ward and the organisation. As a consequence, patients
were likewise inclined to attach meaning to conforming to these implicit norms and consequently, to the
importance of maintaining the care organization. Finding own solutions and avoiding the need to call the
nurse, being grateful and obliging, minimizing expectations, only calling when it was absolutely
necessary, .. are examples of patients’ behaviour that can be understood in this perspective. As such,
the nurses’ focus on the importance of maintaining the care organisation seems to be shared, and even
imposed upon patients and their family members.
A reciprocal reinforcing process in nurses’ and patients’ perceptions of transgressive
behaviour. The dynamics of adapting to one’s environment, and the focus on maintaining the
organisation of care suggest that nurses’ and patients’ perspectives should not be seen as perspectives
that are constant. Both perspectives are constructed in an interaction between the nurse and the patient;
the nursing team and the nurse; and the nursing team and the patient. This notion comprises well with
the interactional or situational model on the causation of aggression in care relationships (Nijman, 2002;
Duxbury, 2002; Duxbury & Whittington, 2005). Both nurses and patients appear to be responsive and
sensitive to what they experience in interactions with one another, and the underlying processes of
perceiving transgressive behaviour in these interactions were identified. Even though these processes
were studied as separate perspectives, different reinforcing processes in both perspectives seem to be
present. For instance, it can be assumed that the adaptive behaviour in some patients provides an
indirect answer to the nurses’ desire to be in control of the care organisation or the nurses’ focus on the
organisation of care. These patients adopt an excusing attitude towards the nurse, and take into account
the needs of fellow patients or the nurses’ working context in appraising the interaction with nurses. It
can be assumed these patients are also more inclined to be grateful for the nurses’ caregiving as they
are responsive to this need of nurses for implicit and explicit recognition. In contrast, when patients were
General discussion
175
more inclined to be more observant, more stern or more vigilant, it can be assumed their behaviour is
easily perceived as transgressive behaviour. Openly questioning the care they receive, might provoke
nurses to no longer feel in control of the care organisation, which entails the risk that patient’s vigilant
behaviour is easily perceived as transgressive. As such, nurses’ responses might comprise avoidance
of these patients or labelling these patients as ‘difficult’, which in return might provoke a negative cyclic
process wherein perceptions of transgressive behaviour in both perspectives are consolidated.
4. | Care relationships in a broader perspective and challenges for
healthcare practice
Present findings focus on care relationships between nurses and patients. Notwithstanding the particular
interaction between the nurse and the patient, it is important to adopt an ecological -and therefore
broader- perspective acknowledging how experiences of aggression and transgressive behaviour
involve an interaction between the nurse, the patient and the broader context in which this interaction
occurs. This ecological approach comprises well with Paterson, Leadbetter, and Miller (2005)
suggesting a misperception of the problem of aggression as principally a function of interpersonal
conflict. Paterson et al. (2005) argue a recognition of organisational and societal roots of aggression is
important. This encompasses the influence of aspects of the prevalent culture of the ward and
organisation (on a meso-level) and various evolutions in healthcare in specific and society in general
(on a macro-level). What follows is a cursory overview of some contextual aspects and a few reflections
on the presumed influence of these aspects on experiences of aggression and transgressive behaviour
in care relationships between nurses and patients.
On a meso-level, attention is directed towards the culture of the ward and the organisation. The findings
on the group norms in nursing teams highlight how nurses are substantially influenced by the commonly
existing standards among nursing team members regarding aggression and transgressive behaviour.
These group norms influence nurse’s behaviour towards patients and the concrete contact with patients
following perceptions of transgressive behaviour. For instance, easily finding support in interacting with
colleagues reinforces the rather evasive way of individual nurses in handling transgressive behaviour.
Moreover, a colleague’s approach of self-evidently filling in for another nurse, dismissing and avoiding
exploration of incidents induces a certain group norm suggesting it is important not to dwell on incidents
Chapter VII
176
of transgressive behaviour. In addition, by excusing and praising one another after incidents of
transgressive behaviour, a certain group norm appears to be established that patients are primarily to
blame for perceptions of transgressive behaviour and nurses are not personally responsible. As
mentioned before, being part of this culture of the ward might provoke nurses to adapt to the values,
beliefs, and standards put forth by their nursing team members, processes which can be explicated by
the framework of ‘professional socialisation’ (Clouder, 2001). By focusing on dynamics in nursing teams
regarding patients’ transgressive behaviour (chapter VI), an influence of these dynamics on nurse’s
individual conduct towards patient’s transgressive behaviour was identified. Furthermore, present
findings do not point out that the specificity or the specialisation of the ward, nor the characteristics of
the patient populations admitted to these wards, profoundly influence perceptions of transgressive
behaviour. This is an argument for the transferability of the findings (Lincoln & Guba, 1985) on the
broader dynamics of these influences on this meso-level irrespective of the setting of the general
hospital wards.
The culture of the organisation (the hospital) is also part of this meso-level, which is expected to be
influenced by general evolutions on a macro-level. This macro-level encompasses some broad
developments in society and in healthcare in specific. For instance, there is a global recognition that
hospitals around the world are under tremendous pressure (Karanikolos et al., 2013). This pressure has
to do with the treatment of massively increased volumes of patients, the continuous expansion in size,
the reduction in staffing levels (European federation of Nurses, 2012), the ever-increasing specialisation
of medicine and nursing, the continuous drives for increased productivity and efficiency (Seys et al.,
2017), and the continual pressure to reduce errors (Bargagliotti, 2012), improve patient outcomes (Aiken
et al., 2003; Kane et al., 2007), and quality of care (Mainz, 2003; Ball et al., 2014). Moreover, the contact
time between patients and members of staff has been sharply reduced (Bruyneel et al., 2015), the
average lengths of stay are falling (Buchan, O’ May, & Dussault, 2013), and there is a greater throughput
of patients (Maben, Cornwell, & Sweeney, 2009). In addition, a shortage of nurses is globally recognized
(WHO 2006; Buchan & Aiken, 2008; European Commission, 2012; Bargagliotti, 2012). All these
evolutions pose significant challenges to health systems and governments around the world (Keyko,
Cummings, Yonge, & Wong, 2016). Against this backdrop, different developments on the level of
healthcare institutions and on a societal level have been observed which influence the delivering of
nursing care and the nature of care relationships between nurses and patients. Just a few of these
General discussion
177
developments are the evolution of quality monitoring and quality assessment (O’Reilly, Courtney, &
Edwards, 2007), the digital revolution (Maben et al., 2009; Desmet, 2009), and the audit culture which
is linked to the digital revolution (Maben et al., 2009). In many ways, these developments bring benefit
in producing vastly increased transparency in medical affairs generally (Maben et al., 2009), or by
providing individual facilities with reports indicating their progress in terms of clinical care benchmarks,
enabling them to determine areas for attention in their quality improvement cycles (O’Reilly et al., 2007).
However, these evolutions encompass an inherent focus on the measurability of quality of care or
caregivers’ performance. And even though it is acknowledged that quality of care is not easily defined
nor measured (Donabedian 1988; Marquis, 2002; Mor, Angelelli, Gifford, Morris, & Moore, 2003), the
risk arises that measurable activities in caregiving are privileged over non-measurable activities (Maben
et al., 2009). Moreover, the caring part of nursing, comprising the ‘whole’ package of activities that
include technical and emotional competence, demonstrated interest, giving comfort, and the
acknowledgement of vulnerability (Corbin, 2008), comprehends non-measurable activities. Maben
(2008) hypothesizes this caring part of nursing might become marginalized and subordinated in an
increasingly managerial discourse in healthcare focusing on outcome evaluations and benchmarking.
As such, the focus on standardised organisational practices can have a profound impact on the nature
of nurses’ caregiving (Ranking & Campbell, 2006). It can be hypothesised the ‘caring part’ of nursing is
particularly important in a context of aggression and transgressive behaviour in care relationships.
Although the findings of this dissertation cannot support decided statements on the influence of these
processes on nurse-patient care relationships, it can be assumed that these processes are part of a
larger context affecting the way nurses’ caregiving is constructed or expected to be performed. The
findings on the importance of maintaining the care organisation (chapter V and VI), and the patients’
assessment of the importance nurses attach to guidelines and protocols (chapter IV) can be put in this
perspective. As a consequence, it can be hypothesized that behaviour of some patients is easily
perceived as transgressive because their needs and requirements fir poorly with services available to
them. For example, patients with a chronic illness, patients with multi-comorbities, older patients, etc.
might be easily seen as ‘difficult’ or challenging patients because of the complexity of their essential
requirements and the idea they do not easily fit in standardized organisational practices. As such, these
developments on a meso- and macro-level might increase the risk that more depersonalised or detached
nurse-patient relationships transpire. This presumed remoteness (distance) in care relationships can
Chapter VII
178
lead to the situation wherein patients are no longer personally known or understood by nurses, which
carries the additional risk that patient’s behaviour is easily perceived as transgressive behaviour.
In considering the effects of these evolutions on nurses themselves, Maben (2008) and Corbin (2008)
point out the difference between how nurses ideally would like to care for patients, and the reality they
face in practice. Restrictions in their care context might induce nurses to feel they are being limited or
constrained in their caregiving, which can result in nurses feeling powerless, burnt-out, frustrated or
morally distressed (Maben, 2008). ‘Moral distress’ is understood as ‘failing to convert personal ideas on
what good care is, into practice’, and can arise when caregivers know what would be the right thing to
do, but experience restrictions to act according to their notion of the right thing to do (Vanlaere &
Burggrave, 2014). In addition to aforementioned restrictions in care organisations, present findings on
group norms in nursing teams also suggest that nurses might feel restricted based on what is common
practice in their nursing team. Even though nurses knew what would be the right thing to do, they
adapted to certain ward habits and renounced their own ideas on handling patient’s transgressive
behaviour. As such, it can be hypothesized that adhering to specific group norms in addressing patient’s
transgressive behaviour might also induce a form of moral distress in nurses. Alongside moral distress,
‘burnouts’ in nursing have also been mentioned as a result of the inability to give perceived ideal care
(Aiken, Clarke, Cheung, Sloane, & Silber, 2002; Reeves, West & Baron, 2005). Burnouts, which
components are emotional exhaustion, depersonalization and reduced personal accomplishment
(Maslach & Jackson, 1986), have been studied in relation to workplace aggression in hospital staff
(Winstanley & Whittington, 2002), suggesting how aggressive encounters were likely to lead to elevated
levels of emotional exhaustion, subsequently causing an increase in depersonalization (Winstanley &
Whittington, 2002). However, elevated levels of burnout originating from workload or other workplace
conditions might also result in staff being more vulnerable to encounter aggression (Winstanley &
Whittington, 2002). Present findings on transgressive behaviour in care relationships appear to suggest
a similar association between experiences of transgressive behaviour and the components of burnouts.
As perceiving patient’s behaviour as transgressive appeared to generate a depersonalised attitude of
nurses, and an emotional remoteness towards the patient. However, it can also be hypothesized that
restrictive working climates, and possible moral distress or burnout as a result, make nurses more prone
or vulnerable to experience and perceive transgressive behaviour in care relationships with patients.
General discussion
179
5. | Implications and recommendations for nursing practice
Translating research findings into clear-cut implications for nursing practice is difficult. Present findings
highlight the complexity of experiencing transgressive behaviour in care relationships between nurses
and patients, which entail a likewise complex solution or answer as to what can be ‘done’ about
(perceptions of) aggressive or transgressive behaviour in care relationships. What follows are basic
principles to consider in addressing transgressive behaviour in care relationships between nurses and
patients. Far from being in any way prescriptive, these basic principles should be considered a basic
reference tool for stimulating the development of interventions or initiatives to aid nurses in (1) reflecting
on perceptions of transgressive behaviour, (2) addressing personal feelings of discomfort based on
perceptions of transgressive behaviour, (3) communicating with patients about perceptions of
transgressive behaviour, and (4) adopting a reflexive stance towards transgressive behaviour in nursing
teams.
Reflecting on perceptions of transgressive behaviour. How nurses perceive transgressive
behaviour made up the starting point of the research. This starting point is important to consider as it
holds the straightforward premise that perceptions of transgressive behaviour are ‘perceptions’ of one
person interpreting certain behaviour or certain words of another person as ‘transgressive’. Hence, it is
important that nurses acknowledge that what they perceive as transgressive is in fact a perception, and
not a given situation. Subsequently, reflecting on own perceptions of transgressive behaviour, how those
perceptions emerge and how own vulnerabilities might impinge these perceptions, is important. As a
nurse, it is of vital importance to recognize the unique disposition and trajectory of patients. This implies
that nurses should recognize that patient’s values and beliefs might differ significantly from the nurse’s
values and beliefs. In this context, the need to be person-centred and compassionate as caregivers is
of foundational importance, and has always followed a parallel stream when historically treatment and
patient caregiving has been institutionalized (O’Toole & Welt, 1989; Koene, Grypdonck, Rodenbach,
and Windey, 1988; Van Heijst, 2006). Person-centred care is defined as the recognition of “the patient
as the source of control and full partner in providing compassionate and coordinated care based on
respect for patient's preferences, values, and needs” (Cronenwett et al., 2007). Person-centred care
requires that nurses value and respect the patient's perspective as well as recognize and explore their
own values (Lusk & Fater, 2013). Further, literature suggests that person-centred care requires nurses
Chapter VII
180
to individualize care, encourage patient autonomy, and display a caring attitude through therapeutic
communication and respect for uniqueness (Lusk & Fater, 2013). In this description of what person-
centred care entails, three major points are important in the context of transgressive behaviour in care
relationships. First, the necessity of understanding the patients’ frame of reference or context. When
patient’s behaviour is perceived as aggressive or transgressive, it is important to position specific
behaviour in the context of the patient’s illness, illness trajectory or biography in general. It seems
elementary to keep in mind that patients have developed a lot of experience, narratives and skills to
cope with situations throughout their lives. These strategies also influence the way they deal with their
illness or their hospital admission. As such, if patient’s behaviour is perceived as aggressive or
transgressive, it is important see ‘beyond’ specific behaviour. Second, it is important that nurses are
sensitive and responsive to patients in exploring what it is like for them to be in the hospital, what is it
like for them to communicate and interact with caregivers, and how patients give meaning to their
experiences in the hospital. As patients adopted different strategies to adapt to their circumstances in
the hospital, it appears to be of paramount importance that nurses are accessible and willing to listen
more closely to what patients are going through. Third, the notion that nurses need to recognize and
explore their own values and beliefs. As such, the expressed need for patients to be grateful and obliging
could be recognized and dealt with by nurses. Reflecting on these implicit needs, and the consequences
when these needs are not gratified ought be addressed in nurse’s reflective practice (Markey & Farvis,
2014; Williams & Walker, 2003; Gustafsson & Fagerberg, 2004; Tishelman et al., 2004). In addition, a
critical point needs to be raised concerning the difference between personal normativity and professional
normativity. Nurses need to acknowledge the additional risks in avoiding the patient following
perceptions of transgressive behaviour, or ‘getting the work done faster’ by bringing in another colleague
to finish the patient’s care. These ways of coping with patient’s transgressive behaviour encompass the
risk that specific essential signals, symptoms or signs of patient’s distress, patient’s illness, or patient’s
general condition are not noticed or observed. Moreover, according to the patient’s perspective, some
patients are inclined to search for own solutions, like bringing their own pain medication to the hospital
when they do not get their pain medication fast enough, helping other patients get up when nurses take
too long to answer call lights, etc. encompassing an additional risk that important aspects of patient’s
care are not known to or observed by nurses. These examples refer to the importance of the difference
between personal normativity and professional nursing normativity. When personal limits, standards or
General discussion
181
norms are crossed, professional limits are not necessarily violated. However, when nurses were inclined
to avoid patients following perceptions of transgressive behaviour, it can be assumed nurses no longer
succeed at that time in acting as a professional nurse. This distinction between personal and
professional normativity is important to acknowledge and recognize for nurses in reflecting on
perceptions of transgressive behaviour. That way, nurses can perceive transgressive behaviour,
recognize the tendency to avoid the patient as a consequence, and realize additional risks emerge when
patients are avoided. ‘Risks’ can be understood here as potential harm to the integral patient. As such,
avoiding patients following transgressive behaviour would not be recognized as behaviour fitting the role
of a professional nurse. Subsequently, the challenge or task arises to maintain good professional care
irrespective of perceiving patient’s behaviour as transgressive. However, this nurses’ task is demanding
as it involves the emotional labour of managing both personal and patient’s emotions (Delgado, Upton,
Ranse, Furness, & Foster, 2017).
Addressing personal feelings of discomfort based on perceptions of transgressive behaviour.
When nurses perceived patients’ transgressive behaviour, they felt insulted, accused, threatened, hurt,
and even angry. Although nurses were inclined to seek rapid solutions for these feelings by avoiding the
patient, by focusing on completing expected care tasks, or by contacting and ventilating their emotions
among colleagues, it seems to be imperative that nurses acknowledge these taxing emotions, address
them, and try to accept them. When these emotions are accepted and acknowledged, nurses gain an
option on how they care to process or deal with these feelings (Vanlaere & Burggraeve, 2014). A first
normalisation of experiencing these taxing emotions appears to be important. Caregiving entails an
intersubjective interaction, rather than an interaction between an object and a subject (Van Heijst, 2006).
This notion encompasses an acknowledgement of the personal vulnerability and fallibility of caregivers,
and as such, the recognition that it is normal that feelings of irritation or anger transpire in situations in
which different people interact and work together. Feeling irritated or angry might even be a form of self-
preservation, in the sense that own limits or boundaries are preserved and defended (Vanlaere &
Burggraeve, 2014). As such, acknowledging taxing emotions, and exploring how and why specific
interactions with patients are hurtful or distressing, appears to be of particular importance when an
individual nurse perceives transgressive behaviour. The installed group norm not to dwell on incidents,
to let go of incidents, and to let it pass entails the risk that nurses who feel hurt by perceived
transgressive behaviour, feel more alone or more vulnerable. Steege and Rainbow (2016) use the
Chapter VII
182
metaphor of the ‘cloak of invulnerability’ as a way of referring to the nursing professional culture of
putting value on portraying an image of strength and invulnerability to colleagues and to patients. As
such, the risk arises that nurses might be inclined to cover up frustrations or concerns out of fear of
being judged by their nursing team members as too sensitive or not relentless enough (Roose, 2015).
In exploring how nurses deal with the emotional labour that is part of nurse-patient/family and collegial
interpersonal interactions, Delgado et al. (2017) focused on the concept of ‘resilience’. Resilience in
nursing has been identified as a personal capacity that aids nurses in dealing with workplace adversity
and demands (Hart, Brannan, & De Chesnay, 2014; McDonald, Jackson, Wilkes, & Vickers, 2013), and
is understood as the ability of individuals to bounce back or to cope successfully despite adverse
circumstances (Rutter, 2008; Hart et al., 2014). Building nurses’ resilience has potential to strengthen
their capacity to address the effects of emotional labour on their well-being and work (McDonald,
Jackson, Wilkes, & Vickers, 2012; 2016; Sorensen and Iedema, 2009), and consequently, exploring
possibilities to strengthen nurses’ resilience appears to be important in a context of aggressive and
transgressive behaviour. Furthermore, professing personal vulnerability as a nurse might also create
sensitivity for the vulnerability of the patient. A sensitivity that is part of the Human Condition (Arendt
1998), and part of the ethics of caregiving (Van Heijst 2005). As mentioned before, indirect forms of
relief were used to deal with difficult emotions in contact with patients following perceptions of
transgressive behaviour. Acknowledging the own use of indirect forms of relief, might be constructive to
realise that patients might also adopt indirect forms of relief to deal with difficult emotions. This indirect
relief of emotions might transpire or appear in aggressive or transgressive behaviour of patients. This
realisation might prove to be important in the subsequent contact with the patient following perceptions
of aggressive or transgressive behaviour.
Communicating with patients about perceptions of transgressive behaviour. Following the
previous important principles of reflecting on own perceptions of transgressive behaviour, and
addressing personal feelings of discomfort following perceptions of transgressive behaviour, there is a
subsequent principle of communicating about perceptions of transgressive behaviour. When nurses
perceived transgressive behaviour, communication with patients about the nurse’s perceptions was
avoided. Nurses even narrated that things definitely would get worse if they were to talk about
perceptions of transgressive behaviour with patients themselves. Nurses pointed out how some things
are better left unsaid. This attitude to avoid communication with patients about transgressive behaviour

General discussion
183
appeared to be self-evident and logical, and particularly common among nursing team members. The
observed stance and notion of nurses towards communication about transgressive behaviour can be
contrasted with general guidelines in addressing aggressive patient’s behaviour. Some principles of
treatment protocols of aggression in a hospital setting can be transferred to a context of transgressive
behaviour. An important principle is the notion that aggression ought to be understood as a form of
communication (Audenaert, Meesen, Jannes, & Van Heeringen, 2001). Patients might want to pose an
awkwardly worded question or adopt a rather negative, prominent or harsh way of conveying the
message that something might be wrong or difficult for them. As such, interpreting patients’ behaviour
or patients’ words as ‘merely’ difficult or transgressive or as ‘merely’ harsh words is not enough. An
interpretation as such does not render the possibility to find a connection to the reason why the patient
expresses a certain something in a certain way. Consequently, rather than avoiding communication
following perceptions of transgressive behaviour, an attitude should be adopted showing that the
message (the patient might want to convey) is understood. As such, in perceiving patient’s behaviour
as transgressive, it is important to try to understand how the patient experiences and gives meaning to
his/her specific situation, and to establish whether the patient’s context includes anxiety-provoking
experiences in the eyes of the patient (Winstanley, 2005). As a nurse, it is important to be able to move
beyond literal words or behaviour in order to explore and understand which message the patient wants
to convey. This notion is of particular importance in caring for patients with cognitive problems, such as
Alzheimer’s disease. Looking beyond actual behaviour, being attentive, and trying to correctly interpret
and understand (non)verbal communication and signals (Gaydos, 2005; Steeman, 2013; Grypdonck &
Sermeus, 2016) is a first and crucial step in caring for this vulnerable patient group. When patient’s
behaviour is perceived as transgressive, it is more challenging but ever so important to listen more
closely to the message the patient might want to convey (Gaydos, 2005). If the patients notices that his
or her message is conveyed to the nurse, even though harsh, impolite or vulgar words were used, then
an openness to create a mutual understanding between the nurse and the patient might be triggered
(Keirse, 2014).
Adopting a reflexive and flexible stance in nursing teams in addressing transgressive behaviour.
In addressing perceptions and experiences of transgressive behaviour, nurses were strongly influenced
by their nursing team members. Nurses’ tendency to find support by discussing incidents with primarily
colleagues was also apparent in chapter II when nurses were asked to indicate their primary support
Chapter VII
184
mechanism when aggressive incidents occur. Consequently, it is important to devise initiatives in
handling patients’ transgressive behaviour on the level of the ward or the nursing team. The findings
suggested there is a common ‘language’ among nurses team members, a language that appears to
connect nurses. Focusing on the proper completing of care tasks, and on the organisation of care
emerges as this shared and consolidated focus among nursing team members. This should encourage
nurses to consider the impact of this shared focus. And this focus also appears to generate certain
implicit rules in nursing teams which need explicitating. As an example, in focusing on the importance
of the organisation of care, Jukema (2011) questions in a context of ‘preservative care’ whether it is
more important that the ‘work’ is finished by 10 o’clock, or that the patients are left in charge of their own
care and decide themselves when they want to be washed? This is simply a tentative example of
considerations that can be made on the level of a nursing team. To extend this example on the
necessary considerations regarding the impact of care organisation, Winstanley and Whittington’s study
(2004) focused on situational variables and patient cognitions in studying patient aggression. They
conclude that the extent to which the encroachment upon patients’ autonomy is seen as anxiety-
provoking by the patient -illustrating how seemingly minor issues such as the timing of personal care-
can be perceived as provocative, which can lead to patient aggression. For instance, not all patients
want to be washed exactly when nurses’ work schedules dictate (Winstanley, 2005). However, it nurses
primarily focus on completing care tasks, this very focus on the organisation of care might induce
aggressive and transgressive behaviour. These policies can be reviewed to determine in what way is it
possible to accommodate the meaning of compassionate care, holistic care, or patient-centered care,
in an organisational structure and context structuring and dictating how, when and in what way service
deliveries (like basic hygienic care) take place (Barclay, 2016). Adopting a flexible and reflexive stance
as a nursing team might make nurses more aware of the patient’s perspective (Dierckx de Casterlé,
2015) which would enable them to take into account patient’s experiences and difficulties, possibly
leading to a reduction in perceptions of transgressive behaviour or possible conflicts. Moreover, terms
and concepts as holistic care, compassionate care (Maben et al., 2009; Blomberg, Griffiths, Wengström,
May, & Bridges, 2016), person-centred care (McCormack et al., 2015; Dewing & McCormack, 2017), ..
are terms that most nurses are familiar with, and these terms are often used or referred to in nursing
practice and nursing education (Maben et al., 2009). Even though these concepts can transpire in
everyday practical acts and decisions (Molewijk & Widdershoven, 2006), the implication and translation
General discussion
185
of these concepts into nursing practice can be quite challenging and difficult. In the nursing team, it
would be quite interesting to discuss, compare and reflect on the meaning of these concepts in everyday
nursing practice. Disagreement in understandings may produce fertile ground for reflective progress. As
such, moral case deliberations (Molewijk & Widdershoven, 2006) could offer possibilities to configure
these discussions since the own (moral) expertise of healthcare professionals forms the starting-point
of these discussions. This would appear to be an interesting focus for nurse specialists in adopting a
role of clinical leader in guiding nurses and nursing teams in these discussions (Hamric, Spross &
Hanson 2005). Moreover, these kind of discussions and reflections are of particular importance in a
context of aggression and transgressive behaviour in care relationships as the translation of these
concepts into practice will be particularly ‘challenging’ when nurses (or nursing teams) feel threatened,
hurt, or insulted by the perception of aggressive or transgressive behaviour. Facilitating reflective
practice in nursing teams might be interesting. In posing different statements regarding what aggression
is or entails, the POAS-s might provide a good starting-point or outline to support this reflective practice.
The different statements - f.i. ‘aggression is to hurt other mentally or physically’, ‘aggression helps the
healthcare staff to see the patient from another point of view’, or ‘aggression is the start of a positive
staff – patient relationship’ – display different cognitions towards aggression, which can prove to be a
good starting-point for discussions among team members. In nursing teams, experiences of aggression
and transgressive behaviour might be deconstructed and explored, which would enable nurses to
identify and consider different perspectives (the perspective of the patient, his/her family, the nurse, etc.)
which might reduce elements of subjectivity (Williams & Walker, 2003). Individual nurses and nursing
teams should be encouraged to examine experiences of aggression and transgressive behaviour and
the impact of management approaches employed. For example, if nursing teams do not reflect on
perceptions of transgressive behaviour, or disregard the patient’s context, the patient’s illness or their
own share in incidents, the strategies employed will not address the problem. As such, the risk emerges
that care may be given with the best of intentions by the nurse, but in real terms may not suit the patient
at all. In other words, the very perception of patient’s transgressive behaviour might emphasize the
‘difference’ between nurse’s values and beliefs and the patient’s values and beliefs, and this difference
in itself should encourage communication between nurses and patients so that nurses can correctly
interpret and understand (non)verbal communication or signals of patients.
Chapter VII
186
6. | Recommendations for management
Considering management and policies towards aggression and transgressive behaviour in healthcare,
it is important to name the ‘zero tolerance’-policy towards aggression in healthcare, which was adopted
in 1999 by the UK Government’s Department of Health (Whittington, 2002) and to some degree in some
Australian states (Holmes, 2006) to tackle aggression and violence to healthcare staff. A policy of ‘zero
tolerance’ entails that specific behaviour, like aggression, will not be tolerated under any circumstances,
and that there will be a non-negotiable sanction imposed whenever that behaviour occurs (Holmes,
2006). The policy of ‘zero tolerance’ might even entail a red card system where staff issues red cards
when patients’ behaviour is unacceptable encompassing the right to withhold treatment from aggressive
patients. This is but one -albeit rather extreme- example of a hardened attitude, and consequently a
policy, towards patient aggression in healthcare. This ‘zero tolerance’-policy can be criticized based on
present findings, and has been strongly criticized throughout literature. The policy of ‘zero tolerance’
does not allow for consideration of particular circumstances or the motivations of the patient, nor the
nurse interpreting or perceiving specific behaviour. Furthermore, blame is attributed to patients,
intolerance by healthcare workers is encouraged (Duxbury & Whittington, 2005, Paterson et al., 2005;
Holmes, 2006), the complexity of the issue of aggression is ignored (Brockmann, 2002), and the
opportunity to build rapport and understand patients’ emotional needs is hindered (Farrell & Salmon,
2014). Contemplating about policies on and management of aggression and transgressive behaviour in
healthcare is important as present findings suggest that the work environment and context are key to
good nurse and patient experiences. Based on present findings, some considerations for (nursing)
management can be formulated.
The dynamic that was observed in nursing teams in protecting and safeguarding ‘the group’ of nurses
warrants further attention. These dynamics in the interprofessional relationships of nurses was assumed
to be a consequence of the interactions with patients and the perceptions of patient’s transgressive
behaviour that occur in this interaction. Literature suggests however that this dynamic might also be
linked to nurse managers’ reactions when aggressive or transgressive behaviour of patients is brought
up or reported. It is possible that nurses perceived nursing managers to take the patient’s side and
favour customer friendliness over staff protection (Renker, Scribner, & Huff, 2015; Gates et al., 2011).
Even though the interaction between nurses and nursing managers on the topic of patient aggression
or transgressive behaviour was not studied, it is plausible that nurses in the present studies also

General discussion
187
experienced it that way. As such, searching for and receiving protection from the group of nurses might
gain its particular importance as the group becomes the primary source of support. As a consequence
for nursing managers, creating and conserving a supporting climate which fosters open dialogue
between nurse managers of all levels and nursing staff to share and discuss mutual expectations and
support needs seems to be important (Heckemann et al., 2017).
Another recommendation for (nursing) management pertains to the finding that nurses expected patients
to display a form of gratitude and recognition from patients and their families. As a nurse manager, it is
important to acknowledge and identify this need, and encourage practice wherein nurses feel valued by
the organization in which they work (Maben, 2008). Gaining recognition from nursing management might
prevent nurses from searching for recognition in care relationships with patients or their family members.
As a consequence for nurse managers, producing a supporting work environment with individualized
considerations (Avolio, Bass, & Jung, 1999) which focus on understanding the needs of the nurses
appears to be important. Moreover, a review of Cummings et al. (2010) pointed out how a leadership
style focused on people and relationships (f.e. supportive, transformational (Bass & Avolio, 1994) and
resonant (Boyatzis & McKee, 2005; Goleman, Boyatzis, & McKee, 2002) leadership styles) is associated
with staff satisfaction with work, role and pay, staff relationships with work, staff health and wellbeing,
work environment factors, and productivity and effectiveness (Cummings et al., 2010). In contrast, a
negative association was observed between the former outcomes and leadership styles focusing on
tasks to be accomplished (f.e. dissonant (Goleman et al., 2002), instrumental (Antonakis & House, 2002)
and management by exception (Avolio et al., 1999) leadership styles). The authors conclude that by
investing energy into relationships with nurses, relational leaders positively affect the health and well-
being of their nurses, and, ultimately, the outcomes for patients (Cummings et al., 2010). Creating a
work environment which displays concern for its caregivers as persons and which builds trust through
responding to staff concerns seems to be very important. Moreover, leadership styles which focus
primarily on the task to be completed may not be tuned to the emotional needs of staff as they provide
complex care, and as such, might not understand the difficult times caregivers go through. Especially in
a context of experiencing and perceiving aggression and transgressive behaviour, nurse leaders who
are relationally focused seem to be important.
A final recommendation for nursing management pertains to an important part of the results of the
interviews with patients regarding their perceptions of transgressive behaviour. Patients expressed the
Chapter VII
188
expectation to encounter competent and skilled professionals during their hospital stay. This expectation
was presumed to be part of a basic trust in professionals because they are part of professional
institutions which regulate practices and endorse trustworthiness of professional activities (Dinç &
Gastmans, 2012). Patients perceived receiving competent care as self-evident. Despite this expectation,
several patients referred to experiences where the nurses’ professional expertise was questionable and
even inadequate. For example, patients narrated about nurses not recognizing an epileptic seizure,
about getting the wrong medication, repeatedly getting medication they were allergic to despite their
own warning, not getting their pain medication, etc. These recollections of patients can serve to be a
considerable sort of ‘wake-up’ call for management, as these examples pertain to a core process of
caregiving: the very quality of care that ‘users’ of a hospital receive. Professional competences and
expertise have a considerable impact on the quality of care, and realizing the quality policy is an
important objective of nursing management (Glouberman & Mintzberg, 2001). The findings on the
patients’ experiences of their hospital admission underline the importance of drawing on the perspective
of people ‘undergoing’ diverse and intricate processes of caregiving in hospitals. Even though patients
in this dissertation’s study talked about just a few personal –and easily articulated- experiences, similar
experiences do not become ‘visible’ if the patients’ perspective regarding the care they receive is not
considered to be a valid and valuable representation of what occurs in basic caregiving processes (Ross
et al., 2014). This recommendation fits with the general recognition of patient participation as a key
component in the redesign of healthcare processes, and as a means to improve patient safety (World
Health Organisation, 2005; Longtin et al., 2010). In literature, there are some initiatives on the
involvement of stakeholders (in particular patients and their representatives) in hosp ital’s decision
structures (Longtin et al., 2010; Ross et al., 2014; Malfait, Van Hecke, Hellings, De Bodt, & Eeckloo,
2017) pointing out how the involvement of stakeholders proves to be an important method to address
the quality of care and client-centeredness in an organization (Malfait et al., 2017).
7. | Methodological considerations
Each separate study of this dissertation has methodological limitations which have been described and
discussed in the previous chapters. What follows are more general methodological considerations that
pertain to several studies at once.
General discussion
189
A transversal representation of nurses’ and patients’ perceptions of transgressive behaviour
was gained. Both nurses and patients were interviewed only once, which makes it difficult to ascertain
whether nurses’ and patients’ perceptions of transgressive behaviour change over time based on
subsequent interactions with patients or with nurses. In subsequent interactions, it is possible that there
are experiences in the interpersonal contact that ‘counterbalance’ experiences or perceptions of
aggression or transgressive behaviour. This possibility is described further as a recommendation for
further research (please see recommendations for further research).
Patients were approached as solitary people. In exploring patients’ perspectives of transgressive
behaviour in care relationships, their individual perspective was examined. This means there is no data
on the interaction between patients and their family members or network regarding experiences or
perceptions of transgressive behaviour. As the perspective of family members regarding transgressive
behaviour in care relationships was not in the scope of this dissertation, this is not considered to be a
methodological limitation. However, insight into interactions between patients and their network
concerning transgressive behaviour in care relationships would have rendered an additional
understanding as one can presume that the patients’ perspective regarding transgressive behaviour in
care relationships is profoundly influenced by the meaning family members attribute to specific incidents.
As such, adopting the family members’ perspective is suggested as a recommendation for further
research (please see recommendations for further research).
Recollections of experiences of aggression and transgressive behaviour were gathered. Both
questionnaires and interviews were used to collect data. The questionnaire that was used collects data
on nurses’ experiences of aggression that occurred in the past year. This time frame induces the risk
that past experiences of aggression are forgotten, or one extreme aggressive incident profoundly
influences recollections of experiences of aggression. Moreover, recollections of past experiences of
aggression and transgressive behaviour –collected through both the questionnaire and the interviews-
might be subject to a form of cognitive coping. This means that experiences are already processed, and
that the emotional meaning or impact of experiences is no longer present. As such, the emotions that
were present in experiencing incidents no longer overwhelm participants in recollecting their
experiences of aggression or transgressive behaviour. Given the ways in which both patients and nurses
adopt strategies to overcome or deal with incidents of aggression and transgressive behaviour, it is

Chapter VII
190
important to acknowledge that experiences might already be reframed by the participant. This is a
limitation of the studies.
An abstraction of experiences of aggression and transgressive behaviour was required. Nurses
and patients were interviewed regarding their experiences of aggression and transgressive behaviour.
In addition to the circumstances where nurses and patients were asked to recollect past experiences,
they were invited to ‘give words’ to their experiences. This has induced additional challenges for analysis
since the usage of words imposes a restriction. Using words requires an abstract representation of
experiences and perceptions. For example, stating that an experience was ‘emotionally difficult’, ‘very
distressing’ or ‘quite painful’ is a very abstract representation of the real emotions and cognitions that
are involved in particular situations. Hence, an extensive form of investigator triangulation was important
to compensate for this abstraction and reconstruction in words. By involving different researchers,
different perspectives were obtained which helped recover implicit data hidden behind words. This
approach in analysis helped to elicit nuance in the understanding of the data (Rubin & Rubin, 1995).
Homogeneity in patients’ characteristics. The findings mainly pertain to Caucasian, Dutch-speaking
patients. Patients who were not able to speak Dutch were excluded from the study. As such, it is not
known whether non-Dutch speaking patients experience or perceive aggression or transgressive
behaviour the same way as was noted in present study’s findings on the patients’ perspective.
Furthermore, one can question whether primarily articulate and self-reflexive patients participated in the
interviews. Even though no patients refused to take part in the study, it might be possible that patients
who are articulate about their experiences in care relationships were more inclined to participate. As
such, there is a risk that present findings mainly represent the experiences of ‘articulate patients’. Even
if this were the case, the representation of ‘articulate patients’ on what occurs in care relationships with
nurses in a context of transgressive behaviour, can still be valuable for patients who cannot easily voice
what they experience in care relationships with nurses in a context of transgressive behaviour. The
concept that underpins this notion, is the authenticity of the study. Lincoln & Guba (1989) add
authenticity to the criteria for methodological adequacy, and describe how a study is (ontological)
authentic when participants and similar groups are helped to understand their world. As such, a study
is authentic when the findings help participants -or other patients in case of this dissertation- to
understand their social world, or human condition (Lincoln & Guba 1989).
General discussion
191
Involved researchers were mainly nurses. The different studies were conducted by a team of
researchers which mainly consisted of nurses. It is reasonable to believe that this professional
background entails preconceived ideas about care relationships between nurses and patients. This is
important to consider as researchers co-construct and affect data collection as well as the results, and
these considerations are particularly important in conducting grounded theory research. How
researchers should address their preconceived ideas on the phenomenon under research is a
discussion point in grounded theory, with a substantial difference between traditional or objectivist
grounded theory approaches and constructivist grounded theory approaches (Charmaz, 2008).
According to the former approach, based on the Glaserian and Straussian schools of grounded theory,
the researcher should ideally be unbiased and know very little of the phenomenon under research so
as not to disturb the analysis and understanding of the phenomenon of interest by preconceived ideas.
But according to a more constructivist grounded theory approach, the researcher is a ‘situated
knowledge producer’ (Charmaz, 2009) who does not only acknowledge preconceived ideas but uses
them in order to better understand the phenomenon of interest. In this dissertation, this meant that the
researchers’ preconceived ideas about care relationships in general were acknowledged, critically
appraised and used as gradually developing theoretical sensitivity (Charmaz, 2008). Moreover,
researcher triangulation was adopted which safeguarded controlled usage of subjectivity, and avoided
premature stranding in theoretical concepts. Critical reasoning, a general openness to the unexpected
and the constructed interpretations of the various researchers expanded the understanding of
theoretical possibilities and the emerging theoretical constructs.
8. | Recommendations for further research
A few recommendations for further research will be addressed and described based on the
methodological approaches in this dissertation, the findings and the limitations of the separate studies.
Transgressive behaviour in care relationships between patients and caregivers that are not
nurses. Aggression and transgressive behaviour in care relationships between nurses and patients
made up the starting-point of this dissertation. However, experiences of aggression and transgressive
behaviour in care relationships do not occur solely in the disciplinary group of nurses (Stubbs,
Winstanley, Alderman, & Birkett-Swan, 2009; Wu et al., 2015; Kowalczuk & Krajewska-Kulak, 2017).
Hahn et al. (2013), in studying risk factors of patient and visitor violence in different disciplinary groups,

Chapter VII
192
pointed out how out of all staff groups, only medical doctors had a significant lower rate of experiencing
patient and visitor violence. When the care relationship with patients or clients is characterized by long-
term support, patients or clients are actively involved in their treatment regime or in short, there is a
interpersonal relationship between the caregiver and the patient; chances are experiences of aggression
of transgressive behaviour will transpire in these treating or guiding care relationships. Insights gained
from this dissertation’s studies might be transferred to disciplinary groups other than nurses. As such,
the findings and insights might be adopted to support (student)caregivers in their attitude-forming in care
relationships, in further developing social or communicative skills, and in gaining an indication of what it
is like for people to ‘become’ a patient or a client in a healthcare system. Further research could explore
whether the observed dynamics in nurse-patient care relationships are specific to the nursing profession,
or additional theoretical concepts play a crucial role in the interaction between patients and other
caregivers in a context of aggressive or transgressive behaviour. For instance, the very notion of what
aggressive or transgressive behaviour is, means or entails; might be different for other disciplinary
groups. Furthermore, the dynamics that were observed in nursing teams influenced nurses’ perceptions
of transgressive behaviour. It would be interesting to explore the dynamics in teams of other disciplinary
groups regarding transgressive behaviour, and whether or not similar group processes emerge.
Processes and dynamics in care relationships that might counterbalance experiences and
perceptions of aggression and transgressive behaviour. This dissertation focused on experiences
and perceptions of aggression and transgressive behaviour in care relationships between nurses and
patients. Even though this focus was an essential starting-point of this research, this focus entails an
inherent focus on ‘negative’ aspects in care relationships between nurses and patients. A focus on what
‘goes wrong’ in care relationships does not necessarily provide insight into processes that might
counterbalance certain experiences of transgressive behaviour. A longitudinal approach in exploring
what occurs in care relationships in a context of aggression and transgressive behaviour could render
an additional understanding. Present findings, in adopting a transversal approach, provide a mere
indication on what might occur in subsequent contacts following transgressive behaviour. For instance,
the ‘labelling’ of patients as difficult patients appeared to result in subsequent strained interactions
between nurses and patients, a finding confirmed in literature (Koekkoek, Hutschemaekers, van Meijel,
& Schene, 2011; Price, 2013). However, the perceived seriousness of transgressive behaviour was
regulated and mitigated by the existence of a trusting relationship between the nurse and the patient.

General discussion
193
The extent to which the patient’s perspective was understood by the nurse, also mitigated the
seriousness of perceived transgressive behaviour. These aspects in care relationships would be
interesting to examine in further research. A longitudinal approach in this research is deemed
appropriate as it can be presumed that a trusting relationship or the ability to understand the patient’s
perspective are aspects that develop over time.
The significance of complexity theory in understanding interactions and relationships among
nursing team members. A central notion of complexity theory is the idea that groups of living people
or organisations can be described as complex adaptive systems (Holden, 2005). A complex adaptive
system is a collection of individual agents with freedom to act in ways that are not always totally
predictable, and whose actions are interconnected so that one agent's actions changes the context for
other agents (Plsek & Greenhalgh, 2001). A perspective as such in focusing on systems thinking has a
long tradition in nursing (Fawcett, 2000). Present findings on nursing team interactions (chapter VI)
suggest that nursing teams can be conceptualised as complex adaptive systems. Attributes of complex
adaptive systems emerge in the nursing team interactions. For example, the self-imposed rules among
nurses can be conceptualized as internalised rules (Wilson, Holt, & Greenhalgh 2001). Conforming to
informal group norms and gaining protection from the group can be conceptualised as attractor
behaviour of nurses (Plsek & Wilson, 2001). Professional socialising processes can be conceptualised
as an adaption of agents within the system (Plsek & Greenhalgh, 2001). Research on the meaning of
complexity theory for health care research is increasing (McDaniel, Lanham, & Anderson, 2009; Pype
et al., 2017) as complexity theory appears particularly applicable for studying relationships and
interactions between health care professionals (Thompson et al., 2016). Future research could adopt
complexity theory as the conceptual framework and design to understand nursing teams as complex
adaptive systems.
Nurses’ and patients’ perspectives of aggression and transgressive behaviour, based on the
‘same’ incidents. In exploring nurses’ and patients’ perceptions of transgressive behaviour, their own
individual perspective was adopted. This starting-point was self-evident as an objective of this
dissertation was obtaining an understanding of the meaning of aggression and transgressive behaviour
in care relationships. In order to gain insight into the meaning nurses and patients attributed to incidents,
it was important not to impose standards or norms which had to be at stake to experience aggression
or transgressive behaviour. The individual and subjectifying approach made sure the meaning of
Chapter VII
194
aggression and transgressive behaviour was reached and clarified. This approach also entailed that
nurses and patients were not elaborating on the same incidents of aggression or transgressive
behaviour, implying that both perspectives were not explored regarding one singular incident or
interaction. Using such an approach would have implied that ‘what’ is an incident would have been
imposed already by the researchers. Nevertheless, a direct comparison of both perspectives on the
same incidents of aggression and transgressive behaviour can render an additional understanding of
how both perspectives influence each other regarding concrete incidents in nursing practice. As such,
different versions of the same incident could be presented, allowing an analysis of why in these
circumstances contradictory understandings can be held by nurses and patients (Rubin & Rubin, 1995).
Initiatives to guide and prepare pregraduate-nurses for professional socialisation in nursing
practice. In exploring associations between different patient-related, nurse-related and work-related
characteristics and nurses’ perceptions of aggression, an association was observed between nurses’
primary tasks and their perceptions regarding aggression. When nurses’ primary task was the education
of nursing students, a higher likelihood of perceiving aggression as a dysfunctional phenomenon was
observed. This association was presumed to exist because of the protective role these nurses might
adopt towards students, making them more prone to perceive aggression as undesirable and disturbing.
The protective role nurses adopt towards their colleagues was also observed in the group dynamics in
nursing teams on account of experiences of transgressive behaviour. In this interaction among
colleagues, a tendency to adopt a hardened attitude towards patients’ transgressive behaviour was also
observed in reaction to an incident where a colleague experiences transgressive behaviour. These
dynamics were framed in a process of professional socialisation (Clouder, 2001; Mooney, 2007; Bisholt,
2012). A similar process might exist in the perception of nurses in practice who educate and guide
nursing students. This finding warrants further exploration to understand how pregraduate-nurses can
be guided or prepared for these socialisation processes. Different studies have pointed out that there is
a tension between the academic environment of the nursing education, and the professional
environment (Bisholt, 2012; Thrysoe, 2012). A high degree of adaption of student nurses or novice
nurses is requested in facing differences between the professional values that are learned in nursing
school, and the organisational values that are acquired in the workplace. The professional value in
nursing education is patient-oriented, while the organisational value in nursing practice is task-oriented
(Feng & Tsai, 2012). Further research could explore how pregraduate-nurses can be prepared and
General discussion
195
guided in dealing with these socialisation processes without feeling restrained in their daily practices in
working within confined limitations (Mooney, 2007).
Family member’s perspective regarding aggression and transgressive behaviour in care
relationships. As mentioned before, the patient’s perspective was approached as an individual
perspective. There is no insight into the family member’s perspective, or the interaction between the
patient and his/her family members. Further research might focus on how experiences of aggression or
transgressive behaviour of patients and their family members’ are subject to a dynamic interaction, and
mutually influence each other. Family members for instance, might be inclined to validate and support
the patient’s perspective regarding transgressive behaviour of nurses, or might be inclined to soothe the
patient’s interpretation of nurse’s transgressive behaviour. The pattern that was observed in patients’
response to transgressive behaviour of searching for own solutions and asking family members to bring
medication from home, provides a mere indication of the interaction between the patient and his/her
family members. Present findings do not provide insight into what exactly goes on in this interaction.
However, in exploring aggression and transgressive behaviour in care relationships, a complex social
situation is studied which warrants a multidimensional approach (Duxbury, 2002). As such,
understanding the family members’ perspective and influence on the patients’ perspective is important.
In this context, it is also important to refer to the results about the prevalence of aggression caused by
patients’ family members. A lot of hospital nurses and primary care nurses indicated to experience verbal
aggression, physical aggression and threats by patients’ family members. In only considering the ‘one
time’- exposure of nurses to aggression, nurses marked that almost all forms of aggression were more
frequently caused by patients’ family members than by patients themselves. These results demonstrate
it is important to understand which underlying processes explain why and how aggression or
transgressive behaviour occurs in the relationships between nurses and patients’ family members.
Extant literature on aggression in care relationships primarily focuses on nurse-patient relationships,
and only marginally considers aggression or transgressive behaviour of patients’ family members.
Moreover, when family members or relatives are involved in research on aggression in care
relationships, they are mostly conglomerated with the occurrence of patient aggression (Lepping, Lanka,
Turner, Stanaway, & Krishna, 2013; Wei, Chiou, Chien, & Huang, 2016; Najafi et al., 2017). Further
research could focus on gaining the perspective of family members on aggression and transgressive
behaviour in care relationships, and focus on what occurs in the interaction between nurses and family

Chapter VII
196
members. Especially in primary care, where family members shoulder significant responsibilities and
concern for the patient’s care, additional insight into dynamics in interactions between nurses and family
members appears to be very important.
General discussion
197
REFERENCES
Abderhalden, C., Needham, I., Friedli, T. K., Poelmans, J., & Dassen, T. (2002). Perception of aggression among
psychiatric nurses in Switzerland. Acta Psychiatrica Scandinavica, 412, 110-7.
Aiken, L. H., Clarke, S. P., Sloane, D. M., Sochalski, J., & Silber, J. H. (2002). Hospital nurse staffing and patient
mortality, nurse burnout and job dissatisfaction. Journal of the American Medical Association, 288(16), 1987-93.
Aiken, L. H., Clarke, S. P., Cheung, R. B., Sloane, D. M., & Silber, J. H. (2003). Educational levels of hospital
nurses and surgical patient mortality. Journal of the American Medical Association, 290, 1617-23.
Antonakis, J., & House, R. J. (2002). An analysis of the full-range leadership theory: the way forward. In: Avolio,
B.J., Yammarino, F.J. (Eds.), Transformational and Charismatic Leadership: The Road Ahead. JAI Press,
Amsterdam, pp. 3–33.
Arendt H. (1998). The human condition. With an introduction by Margaret Canovan. The University of Chicago.
Audenaert, K., Meesen, D., Jannes, C., & Van Heeringen, C. (2001). Voorstel tot een behandelprotocol bij
agressie in het ziekenhuis. Tijdschrift voor Geneeskunde. Nr 23.
Avolio, B. J., Bass, B. M., & Jung, D. I. (1999). Re-examining the components of transformational and
transactional leadership using the multifactor leadership questionnaire. Journal of Occupational and
Organizational Psychology, 72(4), 441–462.
Ball, J., Murrells, T., Rafferty, A. M., Morrow, E., & Griffiths, P. (2014). ‘Care left undone’ during nursing shifts:
Associations with workload and perceived quality of care. British Medical Journal Quality and Safety, 23, 116-125.
Barclay, L. (2016). In sickness and in dignity: A philosophical account of the meaning of dignity in health care.
International Journal of Nursing Studies, 61, 136-41.
Bargagliotti, L. A. (2012). Work engagement in nursing: a concept analysis. Journal of Advanced Nursing, 68(6),
1414–1428.
Bass, B. M., & Avolio, B. J. (1994). Improving Organizational Effectiveness through Transformational Leadership.
SAGE Publications, London.
Benzein, E., & Saveman, B. I. (1998). One step towards the understanding of hope: a concept analysis.
International Journal of Nursing Studies, 35, 322-9.
Bisholt, B. K. (2012). The professional socialization of recently graduated nurses–experiences of an introduction
program. Nurse Education Today, 32(3), 278–282.
Blomberg, K., Griffiths, P., Wengstrom, Y., May, C., & Bridges, J. (2016). Interventions for compassionate nursing
care: a systematic review. International Journal of Nursing Studies, 62, 137-55.
Boyatzis, R., & McKee, A. (2005). Resonant Leadership. Harvard Business School Press, Boston.
Chapter VII
198
Brockmann, M. (2002). New perspectives on violence in social care. Journal of Social Work 1(2), 29–44.
Brüggemann, A. J. (2012). Toward an Understanding of Abuse in Health Care: A Female Patient Perspective.
Linköping University Medical Dissertations, No. 1318.
Bruyneel, L., Li, B., Ausserhofer, D., Lesaffre, E., Dumitrescu, I., Smith, H. L., Sloane, D. M., Aiken, L. H., &
Sermeus, W. (2015). Organization of Hospital Nursing, Provision of Nursing Care, and Patient Experiences With
Care in Europe. Medical Care Research and Review, 72, 643-64.
Buchan, J., & Aiken, L. (2008). Solving nursing shortages: A common priority. Journal of Clinical Nursing, 17(24),
3262–3268.
Buchan, J., O'May, F., & Dussault, G. (2013). Nursing workforce policy and the economic crisis: a global overview.
Journal of Nursing Scholarship, 45(3), 298-307.
Charmaz, K. (2008). Constructing Grounded Theory. A practical guide through qualitative analysis. London: Sage.
Charmaz, K. (2009). Shifting the ground: Constructivist grounded theory methods. In J.M. Morse (Eds.),
Developing Grounded Theory: the Second Generation (pp. 127-154). Walnut Creek, CA: Left Coast Press.
Clouder, D. L. (2001) Becoming professional: An exploration of the social construction of identity. Thesis
Submitted for the Degree of PhD at the University of Warwick
Corbin, J. (2008). Is caring a lost art in nursing? International Journal of Nursing Studies, 45(2), 163–165.
Cronenwett, L., Sherwood, G., Barnsteiner, J., Disch, J., Johnson, J., Mitchell, P., Sullivan, D. T., & Warren, J.
(2007). Quality and safety education for nurses. Nursing Outlook, 55(3), 122–131.
Cummings, G. G., MacGregor, T., Davey, M., Lee, H., Wong, C. A., Lo, E., Muise, M., & Stafford, E. (2010).
Leadership styles and outcome patterns for the nursing workforce and work environment: a systematic review.
International Journal of Nursing Studies, 47(3), 363-85.
Dewing, J., & McCormack, B. (2017). Editorial: Tell me, how do you define person-centredness? Journal of
Clinical Nursing, 26(17-18), 2509-2510.
Dierckx de Casterlé, B. (2015). Realising skilled companionship in nursing: a utopian idea or difficult challenge?
Journal of Clinical Nursing, 24(21-22), 3327-35.
Dinç, L., & Gastmans C. (2012). Trust and trustworthiness in nursing: an argument-based literature review.
Nursing Inquiry, 19(3), 223–237.
Delgado, C., Upton, D., Ranse, K., Furness, T., & Foster, K. (2017). Nurses' resilience and the emotional labour
of nursing work: An integrative review of empirical literature. International Journal of Nursing Studies, 70, 71-88.
Desmet, M. (2009). Liefde voor het werk in tijden van management. Open brief van een arts. Uitgeverij Lannoo,
Tielt
General discussion
199
Donabedian, A. (1988). The quality of care. How can it be assessed? Journal of the American Medical
Association, 260(12), 1743–8.
Duxbury, J. (2002). An evaluation of staff and patient views of and strategies employed to manage inpatient
aggression and violence on one mental health unit: a pluralistic design. Journal of Psychiatric and Mental Health
Nursing, 9(3), 325-37.
Duxbury, J., & Whittington, R. (2005). Causes and management of patient aggression and violence: Staff and
patient perspectives. Journal of Advanced Nursing, 50(5), 469–478.
European Commission. Commission Staff Working Document on an Action Plan for the EU Health Workforce. In
Report No.: Contract NO.: SWD (2012) 93 final. Strasbourg: European Commission: 2012, 18.4.12.
European Federation of Nurses. (2012). Caring in crisis: The impact of the financial crisis on nurses and nursing.
Brussels
Farrell, G. A., & Salmon, P. (2014). Do zero tolerance policies deskill nurses? Nursing Times, 110(6), 14-6.
Feng, R. F., & Tsai, Y. F. (2012). Socialisation of new graduate nurses to practising nurses. Journal of Clinical
Nursing, 21(13–14), 2064–2071.
Fawcett, J. (2000). Analysis and evaluation of contemporary nursing knowledge: Nursing models and theories .
F.A. Davis, Philadelphia, P.A.
Gates, D., Gillespie, G., Smith, C., Rode, J., Kowalenko, T., & Smith, B. (2011). Using action research to plan a
violence prevention program for emergency departments. Journal of Emergency Nursing, 37(1), 32–39.
Gaydos, H. L. (2005). Understanding personal narratives: an approach to practice. Journal of Advanced Nursing,
49(3), 254-9.
Glouberman, S., & Mintzberg, H. (2001). Managing the care of health and the cure of disease--Part I:
Differentiation. - Health Care Manage Rev. 2001 Winter;26(1):56-69; discussion 87-9.
Goleman, D., Boyatzis, R., McKee, A. (2002). The New Leaders: Transforming the Art of Leadership into the
Science of Results. Little, Brown, London, England.
Grypdonck, M. & Sermeus, W. (2016). Integrerende verpleegkunde revisited. Hefboom tot integrale zorg.
Uitgeverij Acco: Leuven
Gustafsson, C., & Fagerberg, I. (2004). Reflection, the way to professional development? Journal of Clinical
Nursing, 13(3), 271-80.
Hahn, S., Müller, M., Needham, I., Dassen, T., Kok, G., & Halfens, T. J. (2011). Measuring patient and visitor
violence in general hospitals: feasibility of the SOVES-G-R, internal consistency and construct validity of the
POAS-S and the POIS. Journal of Clinical Nursing, 20, 2519-30.
Chapter VII
200
Hahn, S., Müller, M., Hantikainen, V., Kok, G., Dassen, T., & Halfens, R. J. G. (2013). Risk factors associated with
patient and visitor violence in general hospitals: Results of a multiple regression analysis. International Journal of
Nursing Studies, 50(3), 374–385.
Hamric, A.B., Spross, J.A., & Hanson, C.M. (2005). Advanced Practice Nursing: An Integrative Approach.
Saunders.
Hanson, G. C., Perrin, N. A., Moss, H., Laharnar, N., & Glass, N. (2015). Workplace violence against homecare
workers and its relationship with workers health outcomes: a cross-sectional study. BMC Public Health, 15(11).
Hart, P. L., Brannan, J. D., De Chesnay, M. (2014). Resilience in nurses: an integrative review. Journal of Nursing
Management, 22(6), 720-34.
Heckemann, B., Peter, K. A., Halfens, R. J., Schols, J. M., Kok, G.5, & Hahn, S. (2017). Nurse managers:
Determinants and behaviours in relation to patient and visitor aggression in general hospitals. A qualitative study.
Journal of Advanced Nursing, Jun 21.
Holden, L.M. (2005). Complex adaptive systems: concept analysis. Journal of Advanced Nursing, 52(6), 651-657.
Holmes, C. A. (2006). Violence, zero tolerance and the subversion of professional practice. Contemporary Nurse,
21(2), 212-27.
Jacelon, C. S. (2004). Managing personal integrity: the process of hospitalization for elders. Journal of Advanced
Nursing, 46(5), 549-57.
Jansen, G., Dassen, T., & Moorer, P. (1997). The perception of aggression. Scandinavian Journal of Caring
Sciences, 11(1), 51-5.
Jukema, J. S. (2011). Bewarende zorg. Een visie voor verzorgenden en verpleegkundigen. Proefschrift aan de
Universiteit Utrecht.
Karanikolos, M., Mladovsky, P., Cylus, J., Thomson, S., Basu, S., Stuckler, D., Mackenbach, J. P., & McKee, M.
(2013). Financial crisis, austerity, and health in Europe. The Lancet, 13, 381(9874), 1323-31.
Keirse, M. (2014). Zie de mens. Pleidooi om anders naar elkaar te kijken. Uitgeverij Lannoo: Tielt.
Keyko, K., Cummings, G. G., Yonge, O., & Wong, C. A. (2016). Work engagement in professional nursing
practice: A systematic review. International Journal of Nursing Studies, 61, 142-64.
Koekkoek, B., Hutschemaekers, G., van Meijel, B., & Schene, A. (2011). How do patients come to be seen as
‘difficult’? A mixed-methods study in community mental health care. Social Science & Medicine, 72(4), 504–512.
Koene, G. B. M. L., Grypdonck, M., Rodenbach, M. T., & Windey, T. (1982). Integrerende Verpleegkunde.
Wetenschap in praktijk. Lochem: De Tijdstroom.
General discussion
201
Kowalczuk, K., & Krajewska-Kułak, E. (2017). Patient aggression towards different professional groups of
healthcare workers. Annals of Agricultural and Environmental Medicine, 24(1), 113-116.
Lepping, P., Lanka, S. V., Turner, J., Stanaway, S. E., & Krishna, M. (2013). Percentage prevalence of patient
and visitor violence against staff in high-risk UK medical wards. Clinical Medicine (London, England), 13(6), 543-
6.
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Beverly Hills, CA: Sage.
Longtin, Y., Sax, H., Leape, L. L., Sheridan, S. E., Donaldson, L., & Pittet, D. (2010). Patient participation: current
knowledge and applicability to patient safety. May Clinic Proceedings, 85(1), 53-62.
Lusk, J. M., & Fater, K. (2013). A concept analysis of patient-centered care. Nursing Forum, 48(2), 89-98.
Maben, J. (2008). The art of caring: invisible and subordinated? A response to Juliet Corbin: 'is caring a lost art in
nursing?'. International Journal of Nursing Studies, 45(3), 335-8.
Maben, J., Cornwell, J. & Sweeney, K. (2009). In praise of compassion. Journal of Research in Nursing, 15(1), 9–
13.
Maben, J., Adams, M., Peccei, R., Murrells, T., & Robert, G. (2012). ‘Poppets and parcels’: the links between staff
experiences of work and acutely ill older peoples’ experience of hospital care. International Journal of Older
People Nursing, 7(2), 83–94.
Mainz, J. (2003). Defining and classifying clinical indicators for quality improvement. International Journal for
Quality in Health Care, 15, 523–530.
Malfait, S., Van Hecke, A., Hellings, J., De Bodt, G., & Eeckloo, K. (2017). The impact of stakeholder involvement
in hospital policy decision-making: a study of the hospital’s business processes. Acta Clinica Belgica, 72(1), 63-
71.
Markey, L., & Farvis, R. (2014). Reflective practice in an acute setting. Nursing Times, 110(24), 16-8.
Marquis, R. (2002). Quality in aged care: A question of relational ethics. Australasian Journal on Ageing, 21, 25–
29.
Maslach, C., & Jackson, S. E. (1986). Maslach Burnout Inventory Manual, 2nd edn. Palo Alto, CA: Consulting
Psychologists Press.
May, D. D., & Grubbs, L. M. (2002). The extent, nature and precipitating factors of nurse assault among three
groups of registered nurses in a regional medical center. Journal of Emergency Nursing, 28(1), 11–17.
McCabe, C. (2004). Nurse-patient communication: an exploration of patients’ experiences. Journal of Clinical
Nursing, 13(1), 41–49.
Chapter VII
202
McCormack, B., Borg, M., Cardiff, S., Dewing, J., Jacobs, G., Janes, N., Karlsson, B., McCance, T., Elin, T.,
Mekki, E., Porock, D., Van Lieshout, F., & Wilson, V. (2015). Person-centredness – the ‘state’ of the art.
International Practice Development Journal, 5.
McDaniel, R.R., Lanham, H.J., &, Anderson, R.A. (2009). Implications of complex adaptive systems theory for the
design of research on health care organizations. Health Care Management Review, 34(2), 191-199.
McDonald, G., Jackson, D., Wilkes, L., & Vickers, M. A. (2012). A work-based educational intervention to support
the development of personal resilience in nurses and midwives. Nurse Education Today, 32(4), 378–384.
McDonald, G., Jackson, D., Wilkes, L., & Vickers, M. (2013). Personal resilience in nurses and midwives: effects
of a work-based educational intervention. Contemporary Nurse, 45(1), 134–143.
McDonald, G., Jackson, D., Wilkes, L., & Vickers, M. (2016). Surviving workplace adversity: a qualitative study of
nurses and midwives and their strategies to increase personal resilience. Journal of Nursing Management, 24(1),
123–131.
McKenna, K. (2004). Study of Work-Related Violence. Committee on Workplace Violence, North Eastern Health
Board, Ireland, 1–121.
Molewijk, B. & Widdershoven, G. (2006). Moreel beraad en goede zorg voor ouderen veronderstellen én
versterken elkaar. Tijdschrift voor Geneeskunde. 62, nr. 23.
Mooney, M. (2007). Professional socialization: The key to survival as a newly qualified nurse. International
Journal of Nursing Practice, 13(2), 75–80.
Mor, V., Angelelli, J., Gifford, D., Morris, J., & Moore, T. (2003). Benchmarking and quality in residential and
nursing homes: lessons from the US. International Journal of Geriatric Psychiatry, 18, 258–266.
Najafi, F., Fallahi-Khoshknab, M., Ahmadi, F., Dalvandi, A., Rahgozar, M. (2017). Antecedents and consequences
of workplace violence against nurses: A qualitative study. Journal of Clinical Nursing, 6 May 2017.
Needham, I., Abderhalden, C., Dassen, T., Haug, H. J., & Fischer, J. E. (2004). The perception of aggression by
nurses: psychometric scale testing and derivation of a short instrument. Journal of psychiatric and mental health
nursing, 11(1), 36-42.
Nijman, H. L. I. (2002). A model of aggression in psychiatric hospitals. Acta Psychiatrica Scandinavica, 106, 142–
143.
O'Reilly, M., Courtney, M., & Edwards, H. (2007). How is quality being monitored in Australian residential aged
care facilities? A narrative review. International Journal for Quality in Health Care, 19(3), 177-82.
O’Toole, A. W., Welt, S. R. (Eds.) (1989). Interpersonal theory in nursing practice. Selected works of Hildegard E.
Peplau. New York, Springer.
General discussion
203
Paterson, B., Leadbetter, D., & Miller, G. (2005). Beyond Zero Tolerance: a varied approach to workplace
violence. British Journal of Nursing, 14(15), 810-5.
Peter, E., Simmonds, A., & Liaschenko, J. (2016). Nurses' narratives of moral identity: Making a difference and
reciprocal holding. Nursing Ethics. 2016 May 24.
Plsek, P.E., & Greenhalgh, T. (2001). Complexity science: The challenge of complexity in health care. BMJ, 15,
625-628.
Plsek, P.E., & Wilson, T. (2001). Complexity, leadership, and management in healthcare organisations. BMJ,
323(7315), 746-749.
Price, B. (2011). Making better use of older people’s narratives. Nursing Older People, 23(6), 31-37.
Price, B. (2013). Countering the stereotype of the unpopular patient. Nursing Older People, 25(6), 27-34.
Pype, P., Krystallidou, D., Deveugele, M., Mertens, F., Rubinelli, S., & Devisch I. (2017). Healthcare teams as
complex adaptive systems: Focus on interpersonal interaction. Patient education and counseling, 100(11), 2028-
2034.
Reeves, R., West, E., & Baron, D. (2005). The impact of barriers to providing high-quality care on nurses’
intentions to leave London Hospitals. Journal of Health Services Research & Policy, 10(1), 5-9.
Renker, P., Scribner, S. A., & Huff, P. (2015). Staff perspectives of violence in the emergency department:
Appeals for consequences, collaboration and consistency. Work, 51, 5–18.
Renwick, L., Lavelle, M., Brennan, G., Stewart, D., James, K., Richardson, M., Williams, H., Price, O., & Bowers,
L. (2016). Physical injury and workplace assault in UK mental health trusts: An analysis of formal reports.
International Journal of Mental Health Nursing, 25(4), 355-66.
Roose, J. (2015). Moeilijke mensen bestaan niet. Iedereen fantastig. Praktische werkwijze in de benadering van
mensen met negatief gedrag, in de hulpverlening en daarbuiten. Drukkerij - Uitgeverij Jan Verhoeven nv
Ross, F., Smith, P., Byng, R., Christian, S., Allan, H., Price, L., & Brearley, S. (2014). Learning from people with
long-term conditions: new insights for governance in primary healthcare. Health & Social Care in the Community,
22(4), 405-16.
Rubin, H. J. & Rubin, I.S. (1995). Qualitative interviewing. The art of hearing data. Sage Publications: London.
Rutter, M. (2008). Developing concepts in developmental psychopathology. In Developmental Psychopathology
and Wellness: Genetic and Environmental Influences (J.J. Hudziak ed.), pp. 3–22. American Psychiatric
Publishing, Washington, DC.
Sato, K., Wakabayashi, T., Kiyoshi-Teo, H., & Fukahori, H. (2013). Factors associated with nurses’ reporting of
patients’ aggressive behavior: A cross-sectional survey. International Journal of Nursing Studies, 50(10), 1368–
1376.
Chapter VII
204
Seys, D., Bruyneel, L., Deneckere, S., Kul, S., Van der Veken, L., van Zelm, R., Sermeus, W., Panella, M., &
Vanhaecht, K. (2017). Better organized care via care pathways: A multicenter study. PLoS One, 12(7).
Sorensen, R., & Iedema, R. (2009). Emotional labour: clinicians' attitudes to death and dying. Journal of Health
Organization and Management, 23(1), 5–22.
Spector, P. E., Zhou, Z. E. & Che, X. X. (2014). Nurse exposure to physical and nonphysical violence, bullying
and sexual harassment: a quantitative review. International Journal of Nursing Studies, 51(1), 72–84.
Steege, L. M., & Rainbow, J. G. (2017). Fatigue in hospital nurses - ‘Supernurse’ culture is a barrier to addressing
problems: A qualitative interview study. International Journal of Nursing Studies, 67, 20–28.
Steeman, E. (2013). The lived experience of older people living with early-stage dementia. Doctoral thesis in
Biomedical Sciences.
Stubbs, B., Winstanley, S., Alderman, N., & Birkett-Swan, L. (2009). The risk of assault to physiotherapists:
beyond zero tolerance? Physiotherapy, 95, 134-139.
Swain, N., & Gale, C. (2014). A communication skills intervention for community healthcare workers reduces
perceived patient aggression: a pretest-posttest study. International Journal of Nursing studies, 51(9), 1241-5.
Thompson, D.S., Fazio, X., Kustra, E., Patrick, L., & Stanley, D. (2016). Scoping review of complexity theory in
health services research. BMC Health Services Researh, 16.
Tishelman, C., Bernhardson, B. M., Blomberg, K., Börjeson, S., Franklin, L., Johansson, E., Leveälahti, H.,
Sahlberg-Blom, E., & Ternestedt, B. M. (2004). Complexity in caring for patients with advanced cancer. Journal of
Advanced Nursing, 45(4), 420-9.
Trysoe, L., Hounsgaard, L., Dohn, N. B., & Wagner, L. (2012). Newly qualified nurses–experiences of interaction
with members of a community of practice. Nurse Education Today, 32(5), 551–555.
Van Heijst, A. (2006). Menslievende zorg: Een ethische kijk op professionaliteit. Kampen: Uitgeverij Klement.
Vanlaere, L. & Burggraeve, R. (2014). Gekkenwerk. Kleine ondeugden voor zorgdragers. Uitgeverij Lannoo, Tielt.
Voyer, P., Verreault, R., Azizah, G. M., Desrosiers, J., Champoux, N., & Bédard, A. (2005). Prevalence of
physical and verbal aggressive behaviours and associated factors among older adults in long-term care facilities.
BMC Geriatrics, 10, 5-13.
Wei, C. Y., Chiou, S. T., Chien, L. Y., & Huang, N. (2016). Workplace violence against nurses - Prevalence and
association with hospital organizational characteristics and health-promotion efforts: Crosssectional study.
International Journal of Nursing Studies, 56, 63–70.
World Health Organisation. World Alliance for Patient Safety. Global Patient Safety Challenge. 2005-2006: Clean
care is safer care. Geneva. Switzerland: World Health Organisation; 2005:1-25.
General discussion
205
World Health Organization (WHO). (2006). Working together for health: The World Health Report 2006. Geneva:
WHO.
Whittington, R. (2002). Attitudes toward patient aggression amongst mental health nurses in the 'zero tolerance'
era: associations with burnout and length of experience. Journal of Clinical Nursing, 11(6), 819-25.
Winstanley, S. (2005). Cognitive model of patient aggression towards health care staff: The patient's perspective.
Work & Stress: An International Journal of Work, Health & Organisations, 19(4), 340-350.
Williams, B., & Walker, L. (2003). Facilitating perception and imagination in generating change through reflective
practice groups. Nurse Education Today, 23(2), 131-7.
Wilson, T., Holt, T., & Greenhalgh, T. (2001). Complexity science: complexity and clinical care. BMJ, 22, 285-288.
Winstanley, S., Whittington, R. (2002). Violence in a general hospital: comparison of assailant and other assault-
related factors on accident and emergency and inpatient wards. Acta Psychiatrica Scandinavica Supplementum,
412, 144-7.
Winstanley, S., & Whittington, R. (2004). Aggressive encounters between patients and general hospital staff: Staff
perceptions of the context and assailants’ levels of cognitive processing. Aggressive Behavior, 30(6), 534–543.
Wu, J. C., Tung, T. H., Chen, P. Y., Chen, Y. L., Lin, Y. W., & Chen, F. L. (2015). Determinants of workplace
violence against clinical physicians in hospitals. Journal of Occupational Health, 57(6), 540-7.

206

Summary
207
SUMMARY

208
Summary
209
SUMMARY
Aggression in health care is not a new problem. Aggression towards healthcare workers is prevalent
and well recognized internationally as a complex problem. This complexity is related to the subjective
aspects of aggression, and the multidimensional and multifactorial nature of the occurrence of
aggression in care relationships. When compared to other caregivers, nurses appear to be at especial
risk to encounter aggression due to the nature, duration and intensity of their care relationships with
patients. Research pointed out that aggression in care relationships generates several negative
consequences for nurses, for patients, for the quality of care, and for the organisation as a whole.
Despite these important insights generated through the extant research, some gaps in current
knowledge on aggression in care relationships exist. Most studies focus on specific settings, like geriatric
settings, emergency or mental health settings. Little knowledge is available about patient aggression in
more general medical and surgical care units or in primary care. Furthermore, little is known about the
perceptions or the subjective meaning of aggression from the perspective of nurses, nor from the
perspective of patients. In addition, as most studies focus on the individual perspective of nurses
regarding aggression, scarce knowledge is available on the group dynamics or –processes in nursing
team following aggressive incidents. These gaps in extant research induced a research trajectory that
–in the form of a doctoral dissertation- tried to contribute to the literature on aggression in care
relationships by providing tentative answers to these various presented challenges.
To gain knowledge on the occurrence of patient aggression in more general settings and nurses’
perceptions of aggression, the first part of this dissertation focuses on gaining a broad indication of
nurses’ experiences of aggression in the general hospital setting and in primary care in Belgium. An
assessment instrument was needed to provide information on frequencies and characteristics of patient
aggression, and nurses’ perceptions of aggression working in these settings. As such, chapter II
addresses the translation and psychometric validation of tree assessment instruments. These three
instruments are the Survey of Violence Experienced by Staff (SOVES), the shortened Perception of
Aggression Scale (POAS-s) and the Perception of Importance of Intervention Skills Scale (POIS). This
psychometric evaluation addressed the content- and construct validity, stability, and internal
consistency, and concluded that the Dutch version of these instruments demonstrated acceptable to
good psychometric properties. Consequently, chapter III outlines the results of a cross-sectional study
adopting the three assessment instruments. This cross-sectional study including 769 nurses focuses on
210
nurses’ experiences of patient aggression and aggression by patients’ family members in primary care
and in general hospital settings. About 89.2% of hospital nurses and 77.9% of primary care nurses had
experienced aggression, and verbal aggression appeared to be most prevalent in both groups.
Aggression by patients’ family members turned out to be common among primary care nurses.
Especially primary care nurses were more emotionally burdened because of verbal aggression, physical
aggression and threats. Most nurses across both groups appealed to colleagues when aggressive
incidents occurred in order to gain support. The majority in hospital nurses and primary care nurses
indicated to report none to a few of the aggressive incidents they encountered. In addition, nurses’
perceptions of aggression were addressed. Most nurses across both groups agreed that aggression is
a dysfunctional and undesirable phenomenon. A subsequent regression-analysis revealed which factors
on the level of nurses, patients or the organization were associated with different perceptions of
aggression.
The second part of this dissertation focuses on gaining an understanding of the meaning of aggression
by adopting a more subjectifying approach of the concept of aggression. A subjectifying approach
focuses on a form of inductive reasoning to understand aggression in healthcare, and consequently,
how perceptions of aggression can emerge. In order to reach understanding of the meaning of
aggression, the term ‘transgressive behaviour’ was adopted. The use of this term allows returning to the
‘essence’ of experiencing aggression, namely a crossing of own limits, standards or norms. This
encompasses a subjective interpretation of when and what limits are exceeded for situations to be
experienced as transgressive. This means that both nurses’ and patients’ own experiences of
transgressive behaviour provided the starting-point to gain an understanding of the meaning of
aggression and the explanatory underlying processes of how these perceptions emerge. In chapter IV,
the meaning of nurses’ transgressive behaviour from the patients’ perspective is addressed. Twenty
interviews were conducted with patients that were admitted to general hospital wards. Patients appeared
to adopt a framework of suppositions which generates implicit ideas or assumptions about hospital care
and nurse-patient relationships. Hence, patients envisage how competent professional caregivers will
be and on how relationships with nurses will be characterized as normal human interactions. These
assumptions are implicit, and awareness of these assumptions occurs when patients experience
envisaged care or nurse-patient relationships are not met in their perceived reality. Experiencing these
discrepancies gives rise to a process of adaption, and several patterns are put into action: patients
Summary
211
become more vigilant with regard to care given by nurses; they search for own solutions; they make
excuses for nurses or they reprioritize their expectations. As such, patients go through both a cognitive
and emotional process in adjusting their assumptions or behaviour. Due to these processes,
experiences of transgressive behaviour are put into perspective. The transgressive aspect of
experiencing transgressive behaviour is ‘addressed’ by patients themselves by adopting different
patterns of adjustment. Subsequently, chapter V explores the onset and meaning of transgressive
behaviour from the nurses’ perspective. Eighteen nurses, working on general hospital wards were
interviewed regarding their perceptions of patients’ transgressive behaviour. These findings revealed
that nurses’ experiences of transgressive behaviour were associated with a complex interplay of both
determining and regulating factors. These factors affect which incidents are perceived as transgressive
and what meaning is assigned to them. The degree of control that nurses experience over the provision
of care, the degree of patient acceptance of organizational and ward rules, the degree of gratitude and
recognition expressed by the patient and the extent of patient regard for the nurse as a person were
identified as determining factors. As regulating factors, the extent of a trusting relationship between
patients and nurses, the extent to which the patient’s perspective is understood, the way transgressive
behaviour is managed by nurses and the roles of the nursing team and head nurse and ward culture
and habits, were identified. These different factors appeared to be connected to one another and were
responsible for particular dynamics in maintaining, reinforcing, or decreasing experiences of
transgressive behaviour. To frame these findings in a broader perspective, the group dynamics in
nursing teams on account of transgressive behaviour were examined. Twenty-four nurses, working in
general hospital settings, were interviewed. Chapter VI outlines these results. Different patterns of
interactions were observed in nursing teams following experiences of transgressive behaviour: nurses
talked to and excused one another; filled in for one another; informed and warned one another; and
defended, protected and safeguarded one another. These patterns in reaction to patients’ transgressive
behaviour seem to be underpinned by the motivation to protect the group. In these interactions, implicit
group norms transpire, causing nursing teams to acquire their specific identity “as a group”. These
informal group norms in nursing teams appeared to impinge how nurses feel threatened by patients’
potential transgressive behaviour; gain protection from the group of nurses and conform to informal ward
rules.

212
The findings of this dissertation contribute to the extant knowledge on what occurs in nurse-patient care
relationships in a context of aggression and transgressive behaviour. Even though aggression as a
phenomenon in care relationships has been the subject of abundant research, a ‘novel’ approach was
adopted for this dissertation. The onset and meaning of ‘transgressive behaviour’ in care relationships
was explored. This was done by quantitatively examining nurses’ experiences and perceptions of
aggression, and by qualitatively studying what transgressive behaviour is for patients, means for nurses,
and causes in nursing teams. The findings underline the complexity and multidimensional nature of
aggression and transgressive behaviour in care relationships. In addition, behaviour in itself does not
determine ‘what’ is experienced as aggressive or transgressive behaviour. Underlying dynamic
processes in patients’ and nurses’ perceptions were identified that determine the meaning that is
attributed to specific interactions in care relationships. The findings of this dissertation offer patients,
student-nurses, nurses and nursing managers a comprehensible framework of what occurs in nurse-
patient care relationships when aggression or transgressive behaviour is experienced or perceived. The
findings can provide content (or form the basis) of a policy to clarify, understand and remedy aggression
and transgressive behaviour in practice.

Samenvatting
213
SAMENVATTING

214
Samenvatting
215
SAMENVATTING
Agressie vormt geen nieuw probleem in de zorgverlening. Nationale en internationale literatuur erkent
agressie als een complex probleem in ziekenhuizen wereldwijd. Deze complexiteit heeft te maken met
de subjectieve aspecten van agressie, en het multidimensionale en multifactoriële karakter van het
voorvallen van agressie in zorgrelaties. Van alle zorgverleners blijken verpleegkundigen in het bijzonder
een risico te lopen op het ervaren van agressie omwille van de aard, de duur en de intensiteit van hun
zorgrelaties met patiënten. Bestaand onderzoek heeft verder ook aangetoond dat het voorkomen van
agressie in zorgrelaties een aantal negatieve gevolgen genereert voor verpleegkundigen, voor
patiënten, en voor de kwaliteit van de zorgverlening. Ook op het niveau van de organisatie worden een
aantal belangrijke overkoepelende negatieve gevolgen geïdentificeerd van agressie in
zorgverleningsrelaties. Niettegenstaande deze belangrijke inzichten uit bestaand onderzoek, zijn er een
aantal hiaten aanwezig in de bestaande kennis over agressie in zorgrelaties. De meeste literatuur over
agressie richt zich bijvoorbeeld vooral op een aantal specifieke settings, zoals geriatrische settings, en
spoed- en psychiatrische afdelingen. Over het voorkomen van agressie in meer generieke settings,
zoals algemene ziekenhuisafdelingen of de eerstelijnszorg, is niet veel geweten. Er is verder ook weinig
literatuur voorhanden over de percepties en de subjectieve betekenis van agressie vanuit het
perspectief van verpleegkundigen, of vanuit het perspectief van patiënten. Doordat bestaande literatuur
zich bovendien vooral richt op het individuele perspectief van verpleegkundigen ten aanzien van
agressie, is er ook nog erg weinig kennis beschikbaar over de groepsdynamieken en -processen in
verpleegkundige teams naar aanleiding van agressie-incidenten. Deze hiaten in bestaand onderzoek
over agressie in zorgrelaties vormden de aanleiding voor een onderzoekstraject dat -onder de vorm van
een doctoraatsonderzoek- op verschillende domeinen antwoorden probeerde te formuleren.
Om meer te weten over het voorvallen van agressie in meer generieke settings, en de percepties van
verpleegkundigen over agressie, richt het eerste deel van dit onderzoekstraject zich op het verkrijgen
van een brede indicatie van agressie-ervaringen van verpleegkundigen op algemene
ziekenhuisafdelingen en in de eerstelijnszorg. Het verkrijgen van een gevalideerd assessment
instrument was vervolgens belangrijk om informatie in te winnen over de frequenties en karakteristieken
van agressie, en de percepties over agressie van deze verpleegkundigen. Hoofdstuk II richt zich
daarom op de vertaling en psychometrische validering van drie assessment instrumenten. Deze drie
instrumenten zijn de Survey of Violence Experienced by Staff (SOVES), the shortened Perception of
216
Aggression Scale (POAS-s) en the Perception of Importance of Intervention Skills Scale (POIS). Bij
deze psychometrische evaluatie werd de inhoudsvaliditeit, construct validiteit, stabiliteit en interne
consistentie nagegaan, waaruit bleek dat de Nederlandstalige versies van deze instrumenten
acceptabele tot goede psychometrische kenmerken hadden. In hoofdstuk III worden vervolgens de
resultaten toegelicht van een cross-sectionele studie waarbij de drie assessment instrumenten gebruikt
werden. Deze cross-sectionele studie bij 769 verpleegkundigen (werkzaam op algemene
ziekenhuisafdelingen en in de thuiszorg) richtte zich op hun ervaringen met agressie van patiënten en
van de familieleden van patiënten. Uit deze resultaten blijkt dat 89.2% van de
ziekenhuisverpleegkundigen, en 77.9% van de thuisverpleegkundigen al agressie ervaren had, en
verbale agressie bleek bij beide groepen verpleegkundigen het vaakst voor te komen. Agressie door de
familieleden van patiënten bleek frequent voor te komen bij thuisverpleegkundigen. Vooral
thuisverpleegkundigen ervoeren ook een belangrijke emotionele impact van het ervaren van verbale
agressie, fysieke agressie of bedreigingen. De meeste verpleegkundigen in beide groepen deden
overwegend beroep op collega’s wanneer agressie-incidenten zich voordeden om ondersteund te
worden. De meeste ziekenhuisverpleegkundigen en thuisverpleegkundigen gaven daarbij ook aan dat
agressie-incidenten niet tot slechts heel beperkt gerapporteerd werden. Daarnaast werd ook bekeken
op welke manier verpleegkundigen agressie percipieerden. De meeste verpleegkundigen uit beide
groepen waren het eens met het idee dat agressie een erg dysfunctioneel en ongewenst fenomeen is.
Bovendien werd via een regressie-analyse ook gekeken naar welke factoren geassocieerd zijn met
verschillende percepties over agressie.
Het tweede deel van het onderzoekstraject richt zich vooral op het verkrijgen van inzicht in de
subjectieve betekenis van agressie. Het zoeken naar deze subjectieve betekenis ging uit van een vorm
van inductief redeneren om agressie in zorgrelaties te begrijpen, en om te begrijpen hoe percepties over
agressie zich vormen. Om inzicht te krijgen in de subjectieve betekenis van agressie werd gebruik
gemaakt van de term ‘grensoverschrijdend gedrag’. Het hanteren van deze term laat toe om terug te
keren naar de essentie van het ervaren van agressie, namelijk het overschrijden van bepaalde grenzen,
normen of waarden. Dit veronderstelt verder een subjectieve interpretatie over wanneer en welke
grenzen overschreden worden om bepaalde interacties of situaties als grensoverschrijdend te ervaren.
Bij het hanteren van de term ‘grensoverschrijdend gedrag’ werd vooral uitgegaan van de eigen
ervaringen en percepties van verpleegkundigen en patiënten over wat zij in het contact met elkaar
Samenvatting
217
grensoverschrijdend vonden. Door kwalitatieve theorievormende onderzoeken werd gezocht naar de
ontstaansmechanismen en de onderliggende processen in het percipiëren van grensoverschrijdend
gedrag in zorgrelaties. In hoofdstuk IV wordt het perspectief van patiënten over grensoverschrijdend
gedrag door verpleegkundigen toegelicht. Daarbij werden 20 interviews afgenomen met patiënten die
opgenomen waren op algemene ziekenhuisafdelingen. Patiënten blijken een impliciet referentiekader
te hanteren waarbinnen ze de zorg in het ziekenhuis en de zorgrelaties met verpleegkundigen plaatsen.
Dit kader creëert de verwachting dat ze zich in het ziekenhuis in deskundige en capabele handen zullen
bevinden, en de zorgrelaties met verpleegkundigen zich zullen voordoen als normale, menselijke
interacties. Wanneer patiënten gewaar worden dat deze verwachtingen op beide domeinen niet
vanzelfsprekend en logisch zijn, ervaren ze een discrepantie tussen hun verwachtingen en de ervaren
zorgrealiteit. Het ervaren van deze discrepantie zorgt ervoor dat patiënten zich gaan aanpassen, en vier
patronen konden geïdentificeerd worden: patiënten werden meer waakzaam, kritisch en controlerend
over de zorg; patiënten zochten naar eigen oplossingen; patiënten waren geneigd verpleegkundigen te
verontschuldigen; of patiënten passen verregaand hun verwachtingen aan. Op deze manier gaan
patiënten door zowel een cognitief als emotioneel proces in het aanpassen van hun verwachtingen of
hun gedrag. Door deze verschillende processen, worden hun ervaringen van grensoverschrijdend
gedrag gerelativeerd. Het ‘grensoverschrijdende’ aspect wordt aangepakt door patiënten zelf door het
hanteren van verschillende aanpassingsprocessen.
In hoofdstuk V wordt vervolgens het perspectief van verpleegkundigen toegelicht. Achttien
verpleegkundigen, werkzaam op algemene ziekenhuisafdelingen, werden over hun percepties van
grensoverschrijdend gedrag door patiënten bevraagd. De beleving en betekenisgeving van
verpleegkundigen blijkt samen te hangen met een complex samenspel van bepalende en regulerende
factoren in het percipiëren van grensoverschrijdend gedrag. Deze factoren bepalen welke situaties als
grensoverschrijdend ervaren worden, en welke betekenis deze vervolgens toebedeeld worden. De mate
van ervaren controle op de zorgorganisatie, de mate van conformerend gedrag van de patiënt en diens
familie, de mate van diskwalificatie van de eigen persoon, en de mate van gekregen dankbaarheid en
erkenning werden als bepalende factoren geïdentificeerd. Als regulerende factoren werd de mate
waarin een vertrouwensrelatie bestond tussen de patiënt en de verpleegkundige, de mate waarin het
perspectief van de patiënt gezien werd, de manier waarop met grensoverschrijdend gedrag omgegaan
werd, en de beïnvloeding van het verpleegkundig team, en de invloed van de afdelingscultuur- en
218
gewoontes geïdentificeerd. Deze factoren bleken met elkaar verbonden te zijn, en zijn verantwoordelijk
voor een eigen dynamiek in het onderhouden, versterken of verminderen van ervaringen van
grensoverschrijdend gedrag. Om deze bevindingen in een breder perspectief te plaatsen, werden ook
de groepsdynamieken in verpleegkundige teams naar aanleiding van grensoverschrijdend gedrag
verder onderzocht. Om zicht te krijgen op deze groepsdynamieken werden 24 verpleegkundigen
bevraagd. In hoofdstuk VI worden deze resultaten toegelicht. Verschillende patronen werden
geobserveerd in de interacties tussen verpleegkundigen onderling na ervaringen van
grensoverschrijdend gedrag: verpleegkundigen spraken elkaar aan en verontschuldigden elkaar;
namen zorgtaken bij elkaar over; informeerden en waarschuwden elkaar; en beschermen, verdedigden
en vrijwaarden elkaar. Deze patronen naar aanleiding van grensoverschrijdend gedag van patiënten of
familieleden lijken voort te vloeien vanuit een motivatie om de groep verpleegkundigen te beschermen.
In deze interactie blijken impliciete groepsnormen op te treden waardoor verpleegkundige teams hun
specifieke betekenis en identiteit ‘als groep’ ontwikkelen. Deze informele groepsnormen in
verpleegkundige teams bleken een invloed uit te oefenen op de manier waarop verpleegkundigen zich
bedreigd voelden door potentieel grensoverschrijdend gedrag van patiënten, vervolgens bescherming
genoten in de groep verpleegkundigen en zich hierdoor ook conformeerden aan informele
afdelingsregels.
De bevindingen uit dit doctoraatsonderzoek vormen een aanvulling op de bestaande kennis over wat
zich afspeelt in zorgrelaties tussen verpleegkundigen en patiënten in een context van agressie en
grensoverschrijdend gedrag. Alhoewel agressie als fenomeen in zorgrelaties al vaak onderzocht is,
werd voor het doctoraatsonderzoek een ‘vernieuwende’ benadering gehanteerd. De betekenis van
‘grensoverschrijdend gedrag’ in zorgrelaties werd geëxploreerd. Dit gebeurde door het kwantitatief
bekijken van de ervaringen en percepties van verpleegkundigen over agressie, en het kwalitatief
onderzoeken van wat grensoverschrijdend gedrag is voor patiënten, betekent voor verpleegkundigen
en vervolgens teweegbrengt in verpleegkundige teams. De bevindingen onderschrijven de complexiteit
en het multidimensionale karakter van agressie en grensoverschrijdend gedrag in zorgrelaties. Daarbij
komt dat gedrag op zich niet bepaalt ‘wat’ als agressief of als grensoverschrijdend gedrag ervaren wordt.
Onderliggende dynamische processen bij zowel patiënten als verpleegkundigen werden geïdentificeerd
die bepalen welke betekenis toebedeeld wordt aan bepaalde interacties in zorgrelaties. De bevindingen
van dit proefschrift bieden patiënten, student-verpleegkundigen, verpleegkundigen en verpleegkundig

Samenvatting
219
managers een inzichtelijk referentiekader over wat zich afspeelt in zorgrelaties tussen verpleegkundigen
en patiënten wanneer agressie of grensoverschrijdend ervaren of gepercipieerd wordt. Ze kunnen mee
inhoud geven (of de basis vormen) aan een beleid dat agressie en grensoverschrijdend gedrag in de
praktijk begrijpelijk maakt, en remedieert.

Curriculum Vitae
220

Curriculum Vitae
221
CURRICULUM VITAE

222
Curriculum Vitae
223
CURRICULUM VITAE
PERSONAL DATA
Date and place of birth December 2nd 1987, Torhout (Belgium)
Married to Filiep Taverniers
Address Kleine Heirenthoek 18, 9880 Landegem, Nevele
Contact [email protected]
EDUCATION
2005-2008 Bachelor of Nursing – University College Brugge-Oostende
2008-2011 Master of Science in Nursing and Midwifery – Ghent University
Thesis: Caregiving for older people with cancer: a qualitative study on the
experiences of family members
WORK EXPERIENCE
10.2010-12.2010 Scientific staff – University Centre for Nursing & Midwifery, Department of Public Health,
Ghent University
10.2009-06.2012 Scientific staff – Research in oncology and geriatrics, federal government project,
Geriatrics department, University Hospital Ghent
07.2008-current Primary care nurse, independent practice
03.2011-current PhD student - University Centre for Nursing & Midwifery, Department of Public Health,
Ghent University
12.2011-current Researcher – University college VIVES, Department of Health, Roeselare
ADDITIONAL TRAINING
2011 Basic assistant training, Ghent University
2014 Medical & Scientific writing, Doctoral Schools, Ghent University
2014, 2015 & 2016 Summer School for Doctoral Studies - European Academy of Nursing Science
2016 Kwalitatief onderzoek in de gezondheidszorg: basiskaders voor de meest gebruikte
kwalitatieve onderzoeksmethoden, Doctoral Schools, Ghent University
2017 Workshop Discourse analysis, European Congress of Qualitative Inquiry
2017 Workshop Qualitative evidence synthesis, European Congress of Qualitative Inquiry
2017 Kwalitatief onderzoek in de gezondheidszorg: specifieke designs en -methoden voor
gevorderden, Doctoral Schools, Ghent University
2017 Argumentation and debating techniques – Summer School Let’s talk Science, Doctoral
Schools, Ghent University
224
PUBLICATIONS
Publications in international journals included in the science citation index
Vandecasteele, T., Van Hecke, A., Duprez, V., Beeckman, D., Debyser, B., Grypdonck, M., & Verhaeghe, S.
(2017). The influence of team members on nurses’ perceptions of transgressive behaviour in care relationships: A
qualitative study. Journal of Advanced Nursing, 00, 1-12.
Vandewalle, J., Debyser, B., Beeckman, D., Vandecasteele, T., Deproost, E., Van Hecke, A., & Verhaeghe, S.
(2017). Constructing a positive identity: A qualitative study of the driving forces of peer workers in mental health-
care systems, International Journal of Mental Health Nursing.
Duprez, V., Vandecasteele, T., Beeckman, D., Verhaeghe, S., & Van Hecke, A. (2016). The effectiveness of
interventions to enhance self-management support competencies in the nursing profession: a systematic review.
Journal of Advanced Nursing, 73(8), 1807-1824.
Vandewalle, J., Debyser, B., Beeckman, D., Vandecasteele, T., Van Hecke, A., & Verhaeghe, S. (2016) Peer
workers' perceptions and experiences of barriers to implementation of peer worker roles in mental health services:
A literature review. International Journal of Nursing Studies, 60, 234-250.
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D., & Verhaeghe, S. (2015). Patients’
perceptions of transgressive behaviour in care relationships with nurses: a qualitative study. Journal of Advanced
Nursing, 71(12), 2822–2833.
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D., & Verhaeghe, S. (2015). Nurses’
perceptions of transgressive behaviour in care relationships: a qualitative study. Journal of Advanced Nursing,
71(12), 2786–2798.
Vandecasteele, T., Senden, C. (joint first authorship), Vandenberghe, E., Versluys, K., Piers, R., Grypdonck, M.,
& Van Den Noortgate, N. (2014). The interaction between lived experiences of older patients and their family
caregivers confronted with a cancer diagnosis and treatment: A qualitative study. International Journal of Nursing
Studies, 52(1), 197-206.
Publications in national journals
Debyser, B., De Backer, T., Vandecasteele, T., Demuynck, E., & Verhaeghe, S. (2013). Grensoverschrijdend
gedrag in de zorgrelatie: het perspectief van algemeen ziekenhuisverpleegkundigen. Verpleegkunde, 3, 4 – 11.
Chapters in books
Senden, C., Vandecasteele, T., Vandenberghe, E., Versluys, K., Grypdonck, M., Deveugele, M. & Van Den
Noortgate, N. Ziekte- en zorgbeleving bij ouderen met kanker. In Senden, C., Versluys, K., Piers, R., Grypdonck,
M., Van Den Noortgate, N. (2014) Zorgen voor zieke ouderen tot het einde. Levensverhalen tonen de weg. Tielt:
Uitgeverij Lannoo
Curriculum Vitae
225
PRESENTATIONS
Presentations at international conferences
Vandecasteele, T., Van Hecke, A., Debyser, B., Vanderplancke, T., Beeckman, D., & Verhaeghe, S. (2017). The
Dutch version of the SOVES, the POAS-s and the POIS to measure patient aggression in general hospitals: A
validation study. Oral presentation at CARE4 - International Scientific Nursing and Midwifery Congress. Antwerp,
Belgium.
Verhaeghe, S., & Vandecasteele, T. (2017). Thinking aloud in qualitative interviews: thinking and reasoning
processes in praxis. Oral presentation at the European congress of Qualitative Inquiry. Leuven, Belgium.
Bastiaens, H., Verhaeghe, S., Van Hecke, A., Anthierens, S., & Vandecasteele, T. (2016). Workshop: Match your
research question with the appropriate qualitative approach. Workshop at Interuniversity symposium on Qualitative
Research in Medical and Health Sciences. Leuven, Belgium.
Verhaeghe, S., & Vandecasteele T. (2016). Applying qualitative research in various health care domains. Oral
presentation at Interuniversity symposium on Qualitative Research in Medical and Health Sciences. Leuven,
Belgium.
Vandecasteele, T., Grypdonck, M., Debyser, B., Beeckman, D., Van Hecke, A., & Verhaeghe, S. (2016). Influence
of team members on nurses’ perceptions of transgressive behaviour in care relationships: A qualitative study. Oral
presentation at The 5th International Conference on Violence in the Health Sector, Dublin, Ireland.
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D., & Verhaeghe, S. (2016). Nurses’
perceptions of transgressive behaviour in care relationships: A qualitative study. Oral presentation at The 5th
International Conference on Violence in the Health Sector, Dublin, Ireland.
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D., & Verhaeghe, S. (2016). Patients’
perceptions of transgressive behaviour in care relationships with nurses: a qualitative study. Oral presentation at
The 5th International Conference on Violence in the Health Sector, Dublin, Ireland.
Vandecasteele, T., Debyser, B., Van Hecke, A. De Backer, T., Beeckman, D., & Verhaeghe, S. (2016). Patients’
perceptions of transgressive behaviour in care relationships with nurses: a qualitative study. Poster Presentation at
Summer School 2016, European Academy of Nursing Science, Halle (Saale), Germany.
Masquelier, E., Vandecasteele, T., & Verhaeghe, S. (2015). Family presence during resuscitation: perspective of
family members and emergency care providers. Oral presentation at Congress of the European Resuscitation
Council (Resuscitation 2015): ERC symposium on guidelines. Prague, Czech Republic.
Vandecasteele, T., Debyser, B., De Backer, T., Van Hecke, A., Beeckman, D., & Verhaeghe, S. (2014).
Transgressive behavior in health care: insight into the onset, meaning and implications for nursing practice. Oral
presentation at Summer School 2015, European Academy of Nursing Science, Barcelona, Spain.
226
Vandecasteele, T., Debyser, B., De Backer, T., Van Hecke, A., Beeckman, D., & Verhaeghe, S. (2015).
Transgressive Behaviour in Care Relationships: Perspectives of Nurses Working in a General Hospital. Oral
presentation at CARE4 – International Scientific Nursing and Midwifery Congress, Antwerp, Belgium.
Vandecasteele, T., Debyser, B., De Backer, T., Van Hecke, A., Beeckman, D., & Verhaeghe, S. (2014).
Transgressive behavior in health care: insight into the onset, meaning and implications for nursing practice. Oral
presentation at Summer School 2014, European Academy of Nursing Science, Rennes, France.
Vandecasteele, T. , Van Hecke, A., Grypdonck, M., van Zuuren, F., Beeckman, D., & Verhaeghe, S. (2012). Lived
experiences and underlying processes of patients with refractory epilepsy and their family when referred to a
Refractory Epilepsy center: a grounded theory study. Oral presentation at 13th European Doctoral Conference in
Nursing Science, Graz, Austria.
Senden, C. , Vandecasteele, T., Vandenberghe, E., Versluys, K., Piers, R., Decoene, E., Grypdonck, M.,
Deveugele, M. & Van Den Noortgate, N. (2012). The experiences and the need for support of older cancer patients
(70+) and their family caregivers: Recommendations for nursing practice, Oral presentation at European Oncology
Nursing Society, Genève, Switzerland.
Vandecasteele, T., Versluys, K., Vandenberghe, E., Piers, R., Decoene, E., Deveugele, M., Grypdonck, M., & Van
Den Noortgate, N. (2011). The lived experience of family members of older cancer patients during a treatment with
chemotherapy and/or radiotherapy, Oral presentation at 15th International Nursing Research Conference, Madrid,
Spain.
Vandenberghe, E., Versluys, K., Vandecasteele, T., Piers, R., Decoene, E., Deveugele, M., Grypdonck, M., & Van
Den Noortgate, N. (2011). The lived experience of older cancer patients during a treatment with chemotherapy
and/or radiotherapy. Oral presentation at 15th International Nursing Research Conference, Madrid, Spain.
Vandecasteele, T., Vandenberghe, E., Senden, C., Versluys, K., Grypdonck, M., Deveugele, M., & Van Den
Noortgate, N. (2011). Experiences of older cancer patients and informal caregivers during treatment with
chemotherapie and/or radiotherapy, Poster presentation at the European Union Geriatric Medicine Society, Malaga,
Spain.
Presentations at Belgian conferences
Vandecasteele, T., Van Hecke, A., Debyser, B., Loncke, P., Verschoren, H., Patoor, I., Verkest, A., Beeckman, D.,
& Verhaeghe, S. (2016). Studienamiddag ‘Zorg zonder grenzen’: Agressie en grensoverschrijdend gedrag in
zorgrelaties. Is het een zorg in de zorg? In samenwerking met VIVES Hogeschool Roeselare. Roeselare, België.
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D. & Verhaeghe, S. (2016).
Grensoverschrijdend gedrag in zorgrelaties: Wat betekent het voor patiënten? Orale presentatie tijdens
avondsymposium ‘Zorg zonder grenzen: Agressie en grensoverschrijdend gedrag in zorgrelaties: Wat betekent het
voor de zorgorganisatie? Gent, België.
Curriculum Vitae
227
Vandecasteele, T., Debyser, B., Van Hecke, A., De Backer, T., Beeckman, D. & Verhaeghe, S. (2016).
Grensoverschrijdend gedrag in zorgrelaties: Wat is het voor verpleegkundigen? Orale presentatie tijdens
avondsymposium ‘Zorg zonder grenzen: Agressie en grensoverschrijdend gedrag in zorgrelaties: Wa t betekent het
voor de zorgorganisatie? Gent, België.
Vandecasteele, T., Grypdonck, M., Debyser, B., Beeckman, D., Van Hecke, A., & Verhaeghe, S. (2016).
Grensoverschrijdend gedrag in zorgrelaties: Wat brengt het teweeg in verpleegkundige teams? Orale presentatie
tijdens avondsymposium ‘Zorg zonder grenzen: Agressie en grensoverschrijdend gedrag in zorgrelaties: Wat
betekent het voor de zorgorganisatie? Gent, België.
Vandecasteele, T., Debyser, B., De Backer, T., Van Hecke, A., Beeckman, D., & Verhaeghe, S. (2015).
Grensoverschrijdend gedrag (GOG) in de gezondheidszorg: Inzicht in de beleving, ontstaansmechanismen en
implicaties voor de verpleegkundige praktijk. Poster presentatie op 5de editie van het Studenten
Onderzoekssymposium – Studentenraad Geneeskunde en Gezondheidswetenschappen. Gent, België.
Vandecasteele, T., Debyser, B., De Backer, T., Van Hecke, A., Beeckman, D., Verhaeghe, S. (2015).
Grensoverschrijdend gedrag (GOG) in de zorgrelatie: het perspectief van verpleegkundigen werkzaam op
algemene ziekenhuisafdelingen. Poster presentatie op 5de editie van het Studenten Onderzoekssymposium –
Studentenraad Geneeskunde en Gezondheidswetenschappen. Gent, België.
Debyser, B., De Backer, T., Vandecasteele, T., Demuynck, E., Verhaeghe, S. (2013). Grensoverschrijdend gedrag
in de gezondheidszorg: Inzicht in de ontstaansmechanismen en de betekenis. Presentatie op 39ste week van de
Verpleegkundigen en Vroedkundigen, Nieuwpoort, België.
Vandecasteele, T., & Senden, C. (2013). Beleving en ondersteuningsnoden van oudere kankerpatiënten en hun
familie: aanbevelingen voor de verpleegkundige praktijk. Presentatie op het symposium ‘Afgestemde zorg voor de
ouderen patiënt – waar onderzoek en zorg elkaar ontmoeten’. Gent, België.
Vandenberghe, E., Versluys, K., Vandecasteele, T., Piers, R., Decoene, E., Deveugele, M., Grypdonck, M., & Van
Den Noortgate, N. (2011). Beleving van oudere mensen met kanker die behandeld worden met chemotherapie
en/of radiotherapie, Orale presentatie op Congres in de psychosociale oncologie, Cédric Hèle Instituut, Mechelen,
België.
Vandecasteele, T., Versluys, K., Vandenberghe, E., Piers, R., Decoene, E., Deveugele, M., Grypdonck, M., & Van
Den Noortgate, N. (2011). Beleving van familieleden van oudere mensen met kanker die behandeld worden met
chemotherapie en/of radiotherapie, Orale presentatie op Congres in de psychosociale oncologie, Cédric Hèle
Instituut, Mechelen, België.
Vandecasteele, T., Versluys, K., Vandenberghe, E., Piers, R., Decoene, E., Deveugele, M., Grypdonck, M., Van
Den Noortgate, N. - Beleving van familieleden van oudere mensen met kanker die behandeld worden met
chemotherapie en/of radiotherapie, Orale presentatie op 30ste oncologiedagen voor verpleegkundigen, Ede, 36-28
oktober 2011.
Vandenberghe, E., Versluys, K., Vandecasteele, T., Piers, R., Decoene, E., Deveugele, M., Grypdonck, M., & Van
Den Noortgate, N. (2011). Beleving van oudere mensen met kanker die behandeld worden met chemotherapie
en/of radiotherapie, Orale presentatie op 30ste oncologiedagen voor verpleegkundigen, Ede, Nederland.

228
REVIEWER
Journal of Advanced Nursing
SCIENTIFIC MEMBERSHIP
Student member of the European Academy of Nursing Science

Dankwoord
229
DANKWOORD

230
Dankwoord
231
DANKWOORD
Aan het einde van een doctoraatstraject is het goed om de tijd te nemen om terug te kijken naar alle
kleine successen en grotere mislukkingen in het ganse traject van het doctoreren, en te beseffen dat
het eigenlijk wel heel mooi geweest is. Doctoreren zie ik als een avontuur. Als een gedegen leerproces,
met successen die gevierd worden, en fouten die subtiel vergeten worden. Het is een kans om met
inhoudelijke vragen op een wetenschappelijke wijze bezig te zijn. Het is dan ook een enorme luxe om
op een grondige manier een onderzoeksthema te mogen verkennen, en dat je wat eigen te maken. Ik
had daarbij ook het grote geluk dat ik me mocht omringd weten door een heleboel mensen die stuk voor
stuk op één of andere manier bewust of onbewust geholpen hebben om alles tot een goed eind te
brengen. Het past hier dan ook om deze mensen uitdrukkelijk te bedanken.
Eerst en vooral ben ik zeer dankbaar voor mijn promotor, Professor Dr. Sofie Verhaeghe. Sofie, dit
proefschrift was er zonder jou niet geweest. Je hebt me wegwijs gemaakt in de wondere wereld van
kwalitatief onderzoek, in visie-ontwikkeling, in het doceren, en het begeleiden van studenten. Ik mocht
geweldig veel van jou leren. Je vermogen om soms tegen de stroom in een heldere visie weer te geven
die onderbouwd, doordacht en compleet terecht is, is indrukwekkend. Bedankt voor de vele leuke (al
dan niet wetenschappelijke) gesprekken, onze gezellige speurtochten naar wat er in de data vervat zit,
je nuchtere kijk op de dingen, je Socratische begeleiding, je gedrevenheid, je kritische verbeteringen
van ideeën en teksten, je goede raad en je geduld, ... . Bedankt, ik mag me gelukkig prijzen met een
promotor zoals jij. Jouw vertrouwen heeft heel veel voor mij betekend.
Mijn co-promotor, Professor Dr. Ann Van Hecke, wil ik ook oprecht bedanken. Ann, je gedegen,
zorgvuldige, optimistische, en kritische blik hebben me vaak en veel verder geholpen, zowel wat betreft
de analyses, als wat betreft de publicaties. Je hebt een indrukwekkend vermogen om met het nodige
inzicht en flair een (letterlijk) einde te maken aan mijn neiging om veel te lange zinnen te maken, met
onnodig veel komma’s’, die dan nog niet eens een samenhang hebben, en dan nog daarnaast extra
ideeën bevatten die afleiden van de kerngedachte die eigenlijk al lang moest duidelijk zijn in het eerste
deel van de zin, maar die dan gewoon ook nog ondergesneeuwd wordt door die extra ideeën die er op
het einde van het verhaal niet eens zoveel meer toe doen. Bedankt om komaf te maken met die neiging
van mij ;-).
232
Mijn dank gaat ook uit naar Professor Dr. Dimitri Beeckman. Bedankt om ook een rol op te nemen in de
begeleidingscommissie van dit doctoraat. Bedankt voor jouw no-nonsense aanpak, je nauwkeurig
naleeswerk, en je steuntjes in de rug. Jullie drieën samen leiden het UCVV. Het is opmerkelijk hoe jullie
voor een groot aantal erg diverse medewerkers individuele condities creëren waarbinnen medewerkers
het best kunnen werken, en tot hun recht komen. Jullie verbinden wetenschappelijke normen en
vereisten met menselijkheid over hoe het is om je doorheen een moeilijk doctoraatstraject te begeven.
Bedankt om mij de kans te geven dit doctoraatsonderzoek tot een goed eind te brengen. Ik kijk terug op
een zeer leerzaam proces en dank jullie voor jullie rol daarin.
Een speciaal woord van dank aan Professor Mieke Grypdonck. Beste Mieke, met u is voor mij alles
gestart. Ik herinner me nog goed het gesprek met u tijdens mijn masteropleiding, en de overwegingen
over welke weg nu de ‘juiste’ zou zijn. U gaf me moed en vertrouwen om de sprong naar een doctoraat
te wagen. U leerde me ook hoe belangrijk het is om authentiek te zijn, en hoe nieuwsgierigheid als
onderzoeker erg belangrijk is. U leerde me ook hoe je een puzzel niet altijd bij de randjes hoeft te
beginnen. Bedankt voor uw inspirerende steun!
Ook de leden van de jury wil ik graag bedanken: Professor Kurt Audenaert, Dr. Els Steeman, Professor
Ruth Piers, Dr. Peter Pype, Professor Wilfried Schnepp, en Professor Rudy Van den Broecke als
voorzitter. Bedankt voor uw betrokkenheid, uw waardevolle opmerkingen en goede suggesties die het
proefschrift echt verbeterden.
Ik wil ook heel graag mijn collega’s van het UCVV en onze vakgroep van nu en van vroeger bedanken.
Eén voor één zijn jullie fantastische mensen die met een gedrevenheid, nieuwsgierigheid en ambitie
zoeken naar inzichten en oplossingen voor erg diverse en indrukwekkende probleemstellingen. Een
bijzonder woord van dank gaat daarbij uit naar mijn directe bureaugenoten van het eerste uur (toen nog
in blok A), Joline, Ineke, Aurélie, Mathieu, en Veerle, en van het laatste uur (nu op 5K3), Veerle, Katrin
en Elien. Bedankt voor de manier waarop we altijd met de nodige humor de lastigste situaties aangepakt
hebben, hoe we oplossingen ‘uitdoctorden’, hoe we op elkaar rekenden voor ‘reality checks’, hoe jullie
konden appreciëren welke enorme culturele verrijking de aanwezigheid van een West-Vlaming met zich
meebrengt, en hoe we voor elkaar kleine fanclubs konden vormen.
Ik wil ook graag mijn collega’s van de VIVES Hogeschool, campus Roeselare, bedanken. Ik ben
dankbaar dat ik een deeltje mag uitmaken van een mooi team dat met een heldere visie over wie we
Dankwoord
233
zijn als verpleegkundigen en wat we kunnen betekenen als verpleegkundigen, haar bacheloropleiding
vormgeeft. Een bijzonder woord van dank gaat daarbij naar Bart Debyser en Tineke De Backer. Het
onderzoek over Grensoverschrijdend Gedrag is bij jullie gestart. Ik mocht meewerken en verder werken
met jullie ideeën over grensoverschrijdend gedrag en wat zich dan afspeelt in zorgrelaties. Bedankt dat
ik hiertoe de kans kreeg, en bedankt voor jullie vertrouwen.
Ook mijn collega’s in de thuisverpleging wil ik heel graag bedanken: mama, Carine, en collega’s.
Bedankt dat ik ook een deeltje van jullie team mag uitmaken. Mijn betrokkenheid in de thuisverpleging
is de laatste tijd verminderd. Het neemt niet weg dat het zorgdragen voor de mensen van onze rondes,
en het rondrijden in onze streek altijd een beetje voelt als thuiskomen. Bedankt voor jullie impliciete en
expliciete steun.
In het bijzonder wil ik ook alle betrokken patiënten, hun naasten, en de betrokken verpleegkundigen,
danken dat zij hun gevoelens, gedachten en ervaringen met ons hebben willen delen. Praten over
ervaringen en percepties van agressie en grensoverschrijdend gedrag is niet vanzelfsprekend. Bedankt
dat jullie jullie verhalen met ons wilden delen.
De studenten uit de masteropleiding Verpleegkunde en Vroedkunde wil ik ook graag bedanken. Bedankt
voor jullie insteek, jullie feedback, jullie kritische vragen, … tijdens de jaren van mijn
assistentenmandaat. Een speciaal woord van dank gaat daarbij ook uit naar de studenten die op een
mooie manier zijlijnen uitwerken of uitwerkten van dit doctoraatsonderzoek.
Mijn vrienden en vriendinnen wil ik ook graag bedanken voor de nodige afleiding en het amusement.
Bedankt voor de vele leuke en knettergekke momenten samen. Bedankt voor het tonen van
belangstelling ookal was mijn relaas soms geweldig saai, bedankt voor het meeleven met mij, en jullie
steun!
Dan wil ik ook graag mijn familie bedanken. Bedankt lieve pepe, nichten, neven, tantes en nonkels!
Bedankt voor alle babbels, begrip, ontspanning, plezier, steun, en aanmoedigingen. Ik mag me gelukkig
prijzen in onze gezellige familie. Mijn dank is groot!
Mijn schoonfamilie wil ik ook graag bedanken. Ik heb veel geluk om me te mogen omringd weten door
stuk voor stuk fantastische mensen. Bedankt, lieve schoonmama, lieve schoonzussen en –broers, lieve
neefjes en nichtjes. Het is een eer om een deeltje uit te maken van jullie warme en grote familie. Bedankt
voor jullie ondersteuning gedurende dit ganse proces.
234
Een heel speciaal woord voor onze mémé, Julia D’Haene. Lieve meme, elke dag nog ben je in onze
gedachten. Elke dag nog voorzie jij inspiratie, moed en kracht om verder te zetten. Herinneringen aan
jou doen ons verder doen met een gemis in ons hart maar met een kracht die alleen jij kon
teweegbrengen.
Een bijzonder woord ook voor mijn ouders. Lieve mama en papa, met enkele woorden hier kan ik niet
genoeg uitdrukken hoe dankbaar ik ben. Jullie hebben ons opgevoed met een respect voor traditie en
waardigheid. Met een gezonde portie zelfrelativering, en een nog gezondere portie geweldig droge
humor. Dat ik hier mag staan, heb ik aan jullie te danken. Jullie zetten ons op weg, kijken toe hoe we
dat doen, in een vertrouwen dat we onze weg vinden. Bedankt voor jullie steun bij de avonturen die wij
aangaan, en voor jullie meeleven met alle grote en kleine dingen in ons leven!
Mijn broers, Bram en Martijn, en Sofie als fantastische vriendin van Bram, wil ik ook graag bedanken.
Mijn broers en partners in crime. Het is een feit dat we zo van elkaar verschillen dat we perfect bij elkaar
passen. Bedankt voor jullie steun, jullie grapjes, jullie betrokkenheid!
Een laatste woord van dank is voor Filiep. Lieve Filiep, mocht ik je minder graag zien, dan zou het vast
makkelijker zijn om er over te babbelen. Bedankt voor de moed en kracht die je gaf, voor de
ondersteuning die je voorzag, om er te zijn wanneer ik je het meest nodig had, voor het geduld dat je
had, voor het doorgeven van discipline en veerkracht, en voor de rust die je bracht. Bedankt, Iepje!
Door de ondersteuning van velen mocht ik vandaag een droom verwezenlijken. Ik hoop nu dat ik zelf
kan bijdragen om anderen te helpen hun dromen te verwezenlijken. Ik wens u allen te bedanken voor
uw aanwezigheid, voor uw steun, en voor uw interesse!
Tina Vandecasteele, 18 januari 2018

Dankwoord
235

Dankwoord
236
AGGRESSION AND TRANSGRESSIVE BEHAVIOUR IN CARE RELATIONSHIPSInfluencing factors and underlying processes in nurses’ and patients’ perceptions
Tina Vandecasteele
Aggression in health care is not a new problem. Aggression towards healthcare workers is prevalent and well recognized internationally as a complex problem. When compared to other caregivers, nurses appear to be at especial risk to encounter aggression due to the nature, duration and intensity of their care relationships with patients. Research pointed out that aggression in care relationships generates several negative consequences for nurses, for patients, for the quality of care, and for the organisation as a whole.
This doctoral dissertation tried to contribute to the extant knowledge on what occurs in nurse-patient care relationships in a context of aggression and transgressive behaviour. Even though aggression as a phenomenon in care relationships has been the subject of abundant research, a ‘novel’ approach was adopted for this dissertation. The onset and meaning of ‘transgressive behaviour’ in care relationships was explored. This was done by quantitatively examining nurses’ experiences and perceptions of aggression, and by qualitatively studying what transgressive behaviour is for patients, means for nurses, and causes in nursing teams. The findings underline the complexity and multidimensional nature of aggression and transgressive behaviour in care relationships. In addition, behaviour in itself does not determine ‘what’ is experienced as aggressive or transgressive behaviour. Underlying dynamic processes in patients’ and nurses’ perceptions were identified that determine the meaning that is attributed to specific interactions in care relationships.
The findings of this dissertation offer patients, student-nurses, nurses and nursing managers a comprehensible framework of what occurs in nurse-patient care relationships when aggression or transgressive behaviour is experienced or perceived. The findings can provide content (or form the basis) of a policy to clarify, understand and remedy aggression and transgressive behaviour in practice.
Aggression and transgressive behaviour in care relationships between nurses and patientswas written as a PhD-thesis by Tina Vandecasteele at the Ghent University, Department of
Public Health, University Centre for Nursing and Midwifery.





























