Embed Size (px)
Citation preview
Community Mental Health Journal, Vol. 29, No. 5, October 1993
CLINICAL CARE UPDATE
"Aggressive" and "Problem-Focused" Models of Case Management for the Severely Mentally Ill
Patrick W. Corrigan, Psy.D. Donna Kayton-Weinberg, MS
ABSTRACT: In this paper, the relative merits and limitations of two models of case management (CM) are compared: "aggressive" and ~problem-focused". Although aggres- sive CM has a well-established history of improving the community tenure of deinstitu- tionalized patients, individuals participating in this treatment are likely to become dependent on health care providers and hence require indeterminate assistance. Problem-focused CM teaches patients how to identify and resolve community-based predicaments thereby making them relatively more independent of the mental health system. Patients receiving problem-focused CM, however, need reasonably competent cognitive functions thereby ruling out participation of the most severely disabled individuals. An interaction of the two approaches is proposed in which aggressive and problem-focused CM is selected depending on the patient's current needs, cognitive deficit, and level of social support.
As more and more severely mentally ill patients have been released from long term psychiatric hospitals, clinical investigators have searched for and developed treatment strategies that meet patients' multi-faceted needs. After two decades of work, it now seems apparent that competent community support programs (CSPs) that include long
Patrick W. Corrigan is Director of the University of Chicago Center for Psychiatric Rehabilita- tion. Donna Kayton-Weinberg is affiliated with the Illinois School of Professional Psychology.
Address correspondence to Patrick W. Corrigan, Psy. D., University of Chicago Center for Psychiatric Rehabilitation, 7230 Arbor Drive, Tinley Park, IL 60430.
4 4 9 �9 1993 Human Sciences Press, l~c.
450 Community Mental Health Journal
term case management (CM) provide a better quality of life than contin- ued inpatient care. Traditionally, CM has been viewed as an "aggres- sive" endeavor in which case managers assume responsibility for the comprehensive treatment needs of their patients. However, aggressive CM that occurs over the long term is very expensive, especially with other, equally costly, interventions. With severe restrictions on mental health budgets common in most states, t reatment strategies are needed that augment aggressive CM and produce a more efficient and cost- effective intervention. In this paper, the pros and cons of problem- focused CM are reviewed for this purpose. Before discussing the com- parative strengths and weaknesses of these two forms of CM, however, the community needs of severely mentally ill patients are discussed.
THE NEED FOR COMMUNITY CARE
With the convergence of several independent movements in the early sixties, (e.g., wide spread use of neuroleptic medication, the institution of Aid to the Disabled (now Supplemental Security Income), and pas- sage of the Community Mental Heal th Centers Act of 1963), large numbers of institutionalized psychiatric patients were released from the hospital (Bachrach, 1981; Goldman, Gatozzi, & Taube, 1981; Lamb, 1982; Mechanic & Rochefort, 1990). Although the quality and organiza- tion of community care in the years immediately after deinstitutional- ization have been widely regarded as lacking (General Accounting Office, 1978; Intagliata, 1982; Mechanic & Aiken, 1989), CSPs for a subsample of patients emerged where the quality of care was satisfac- tory. Several studies have shown that patients treated in well- administered CSPs for a discrete period of time have better outcomes than patients who remain in the hospital during the same period of time and then are released. Specifically, patients in CSPs report more satisfaction with treatment and greater a t ta inment of personal goals than inpatient comparison groups (Test & Stein, 1978). Despite the decrease in institutional structure, CSP patients dem(~nstrate less symptomatology (Herz, Endicott, Spitzer, & Mesnikoff, 1971; Stein & Test, 1978; Mosher & Menn, 1978) and fewer relapses (Mosher & Menn, 1978; Mueller & Hopp, 1983) than patients treated at inpatient settings and then released.
Other studies have indicated that quality of community care and improvement in mental status vary with the intensity of the CSP
Patrick W. Corrigan, Psy.D. and Donna Kayton-Weinberg, MS 451
(Modrcin, Rapp, & Poertner, 1988). Anthony and Blanch (1989) identi- fied twelve need domains including outreach, rehabilitation, health care, crisis intervention, housing, income support, family care, and advocacy. Programs that address more areas of community need yield greater outcomes. CM plays a central role in coordinating services for these domains and assuring that quality and continuity of care re- mains.
HOW TO CASE MANAGE." A G G R E S S I V E A N D PROBLEM- FOCUSED A P P R O A C H E S
Depending on the way in which CM is construed overall, specific duties may include discharge planning from the inpatient setting, estab- lishing linkages with community programs, networking with these programs to confirm that linkages have occurred, assurance that qual- ity community care is proffered, and advocacy when sufficient quality is not provided (Kanter, 1989). Two models have developed that provide a framework for carrying out these duties: ~aggressive" CM (Johnson & Rubin, 1983; Schwartz, Goldman, & Churgin, 1982) and problem- focused (or ~'clinical") CM (Bachrach, 1989; Kanter, 1989; Lamb, 1980). As we will show in this paper, these two CM models do not entail mutually exclusive interventions nor pose independent goals. Rather, an interaction of the two strategies over the course of the disorder may provide the most effective CM for severely mentally ill adults.
In aggressive CM, case managers assume the role of responsible caretakers. Their goal is to actively assist patients in at taining service goals such as housing, financial aid, and vocational rehabilitation. For example, the aggressive case manager for Ed, a patient who has lost his Medicaid benefits, will call the Public Aid worker, obtain all necessary documentation to substantiate Ed's claims, travel with the patient to the Medicaid office, and follow-up with Ed to assure that Medicaid is eventually received. Sometimes extraordinary efforts may be needed to help accomplish these goals (e.g., work evening hours, travel across town for appointments, venture into dangerous neighborhoods), efforts tha t are assumed to be part of the aggressive case manager's standard duties. Proponents of aggressive CM assume that case managers are more skillful than patients in navigating the various services and agencies. As a result, patients often are relegated to passive roles with relatively little opportunity for learning new skills. For example, Ed

452 Community Mental Health Journal
might not say much, instead deferring to his case manager who would iron out the problem.
Good aggressive CM has been described as longitudinal, cross sec- tional, and accessible (Baker & Intagliata, 1992; Caragonne, 1981; Intagliata, 1982; Test & Stein, 1978). Such CM is ongoing, beginning at discharge and continuing with patients as they move through various community services. Longitudinal CM does not end if the patient suf- fers a relapse and is rehospitalized. Instead, a spot remains vacant in the case load for the patient's eventual return to the community. Cross sectional CM implies that the case manager addresses all of the pa- tient's need domains. Hence, case managers must have a broad network of service ~contacts" available to meet the changing spectrum of patient needs. By being accessible, case managers reach out to patients to serve them at their home, work place, or day treatment program rather than wait for them to meet at the office.
Rather than viewing the fulfillment of community needs as the ulti- mate goal of CM, '~clinical" case managers envision the work towards fulfillment as a therapeutic opportunity in which individuals with chronic mental illness may learn to cope with their disorder better. As a result, patients become more self-reliant and less dependent on the mental health system. In this light, the practice of CM is more akin to a therapeutic experience in which the mental health professional is reluc- tant to assume total responsibility for the patients' problems. Clinical case managers play an active role in helping patients to cope with community difficulties.
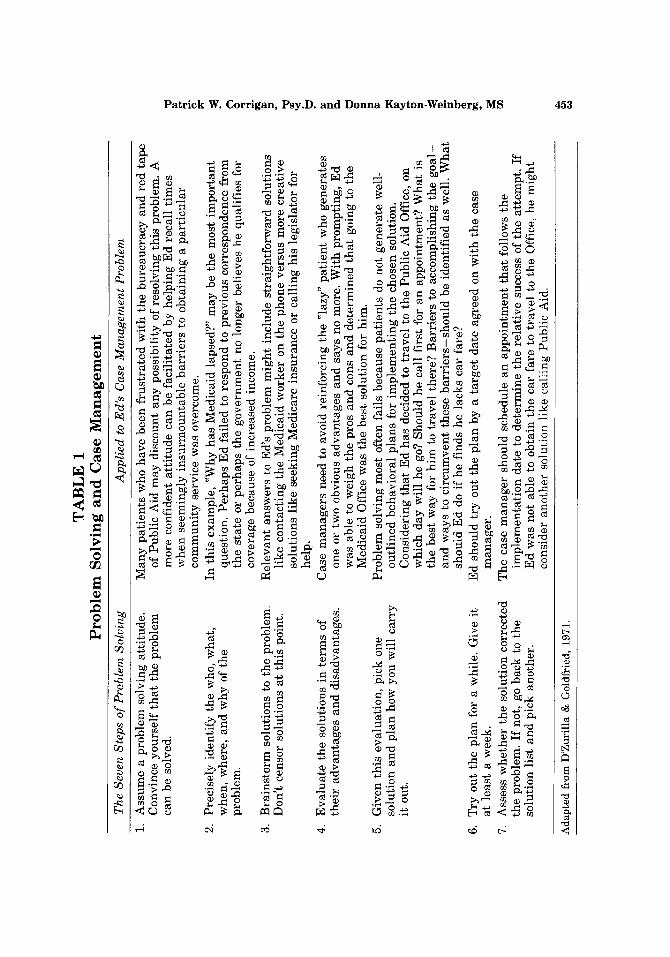
Problem solving provides a useful paradigm for clinical case man- agers. Seven steps in problem solving are reviewed in Table 1. The manner in which a case manager might adopt this strategy to resolve, for example, Ed's problem with Public Aid is also outlined in this table. Problem solving affords a stepwise clinical outline with which patients learn to resolve their community needs. Problem-focused case man- agers first teach the i r patients the steps of problem solving and then encourage them to independently resolve future community dilemmas, perhaps prompting patients when they are stuck at one of the steps or serving as a resource in generating solutions to esoteric community predicaments. Research on problem solving in inpatient settings has shown that severely mentally ill patients can learn this stepwise method and competently apply it to meet life problems (Hansen, St. Lawrence, & Christoff, 1985; Liberman, Mueser, & Wallace, 1986; Siegel & Spivack, 1976a,b; Wallace & Liberman, 1985).
TA
BL
E
1 P
rob
lem
Sol
vin
g an
d C
ase
Man
agem
ent
The
Sev
en S
teps
of
Pro
blem
Sol
ving
A
ppli
ed t
o E
d's
Cas
e M
anag
emen
t P
robl
em
1.
Ass
um
e a
pro
ble
m s
olvi
ng a
ttit
ud
e.
Man
y p
atie
nts
who
hav
e b
een
fru
stra
ted
wit
h t
he
bu
reau
crac
y a
nd
red
tap
e C
onvi
nce
yo
urs
elf
that
th
e pr
oble
m
of P
ub
lic
Aid
may
dis
coun
t an
y p
ossi
bili
ty o
f re
solv
ing
th
is p
robl
em.
A
can
be
solv
ed,
mo
re c
onfi
dent
att
itu
de
can
be
faci
lita
ted
by
hel
pin
g E
d r
ecal
l ti
mes
2.
3.
Pre
cise
ly i
den
tify
th
e w
ho,
wh
at,
whe
n, w
here
, an
d w
hy
of
the
prob
lem
.
Bra
inst
orm
sol
utio
ns t
o th
e pr
oble
m.
Do
n't
cen
sor
solu
tion
s at
thi
s po
int.
4.
Ev
alu
ate
the
solu
tion
s in
ter
ms
of
thei
r ad
van
tag
es a
nd
dis
adv
anta
ges
.
5.
Giv
en t
his
ev
alu
atio
n,
pick
one
so
luti
on
an
d p
lan
how
yo
u w
ill
carr
y
it o
ut.
6.
Try
ou
t th
e p
lan
for
a w
hile
. G
ive
it
at l
east
a w
eek.
7.
A
sses
s w
het
her
th
e so
luti
on c
orre
cted
th
e pr
oble
m.
If n
ot,
go b
ack
to
the
solu
tio
n l
ist
and
pic
k an
oth
er.
wh
en s
eem
ing
ly i
nsu
rmo
un
tab
le b
arri
ers
to o
bta
inin
g a
par
ticu
lar
com
mu
nit
y s
ervi
ce w
as o
verc
ome.
In
th
is e
xam
ple,
~W
hy h
as M
edic
aid
laps
ed?"
may
be
the
mo
st i
mp
ort
ant
ques
tion
. P
erh
aps
Ed
fai
led
to r
esp
on
d t
o p
rev
iou
s co
rres
pond
ence
fro
m
the
stat
e or
per
hap
s th
e g
ov
ern
men
t no
lo
ng
er b
elie
ves
he q
uali
fies
for
co
ver
age
beca
use
of i
ncr
ease
d i
ncom
e.
Rel
evan
t an
swer
s to
Ed
's p
rob
lem
mig
ht
incl
ude
stra
igh
tfo
rwar
d s
olu
tio
ns
like
co
nta
ctin
g t
he
Med
icai
d w
ork
er o
n th
e ph
one
ver
sus
mo
re c
reat
ive
solu
tion
s li
ke s
eeki
ng M
edic
are
insu
ran
ce o
r ca
llin
g hi
s le
gis
lato
r fo
r he
lp.
Cas
e m
anag
ers
need
to
avoi
d re
info
rcin
g t
he
~la
zy"
pat
ien
t w
ho g
ener
ates
on
e or
tw
o ob
viou
s ad
van
tag
es a
nd
say
s no
mor
e. W
ith
pro
mp
tin
g,
Ed
w
as a
ble
to w
eigh
th
e pr
os a
nd
con
s an
d d
eter
min
ed t
hat
goi
ng t
o th
e M
edic
aid
Off
ice
was
th
e be
st s
olu
tio
n f
or h
im.
Pro
ble
m s
olvi
ng m
ost
oft
en f
ails
bec
ause
pat
ien
ts d
o no
t g
ener
ate
wel
l-
ou
tlin
ed b
ehav
iora
l p
lan
s fo
r im
ple
men
tin
g t
he
chos
en s
olut
ion.
C
on
sid
erin
g t
hat
Ed
has
dec
ided
to
trav
el t
o th
e P
ubli
c A
id O
ffic
e, o
n w
hic
h d
ay w
ill
he g
o? S
houl
d h
e ca
ll f
irst
for
an
ap
po
intm
ent?
Wh
at i
s th
e b
est
way
for
him
to
trav
el t
her
e? B
arri
ers
to a
ccom
plis
hing
th
e g
oa
l-
and
way
s to
cir
cum
ven
t th
ese
bar
rier
s-sh
ou
ld b
e id
enti
fied
as
wel
l. W
hat
sh
ou
ld E
d do
if
he f
inds
he
lack
s ca
r fa
re?
Ed
sh
ou
ld t
ry o
ut t
he
pla
n b
y a
targ
et d
ate
agre
ed o
n w
ith
th
e ca
se
man
ager
. T
he c
ase
man
ager
sho
uld
sche
dule
an
ap
po
intm
ent
that
fol
low
s th
e im
ple
men
tati
on
dat
e to
det
erm
ine
the
rela
tiv
e su
cces
s of
th
e at
tem
pt.
If
Ed
was
no
t ab
le t
o o
bta
in t
he
car
fare
to
trav
el t
o th
e O
ffic
e, h
e m
igh
t co
nsid
er a
no
ther
sol
utio
n li
ke c
alli
ng
Pub
lic
Aid
.
o o o o0
Ad
apte
d f
rom
D'Z
uri
lla
& G
old
frie
d,
1971
.
454 Community Mental Health Journal
LIMITATIONS OF AGGRESSIVE AND PROBLEM-FOCUSED CM
Both aggressive and problem-focused CM have limitations in their effectiveness which suggest that an interaction of the two approaches serves CM and the patient best. Because the case manager is responsi- ble for most service goals in aggressive CM, the patient is likely to become dependent on the professional such that CM services occur in never ending fashion. This form of CM is very expensive. Recent aware- ness about dwindling mental health budgets has driven legislators and mental health administrators alike to search for more cost efficient t reatment strategies. Still, some might argue tha t services like aggres- sive CM need to be ongoing to address the waxing and waning course of the severely mentally ill patient (Test & Stein, 1978). Is such lengthy and costly CM justified?
Research is mixed regarding the necessity for longitudinal case man- agement. Bond (1984) showed that the length of time in CSP treatment was positively correlated with the rate of patient self-sufficiency. How- ever, others have argued that the need for specific CM services such as linkage planning diminishes soon after community reentry (Harris & Bergman, 1988; Surles & McGurrin, 1987). As patients adjust to other community care programs, CM can be curtailed. Aggressive CM that includes problem solving may help these patients become more inde- pendent and decrease the need for longitudinal care.
What limitations exist to the problem solving approach? Bellack, Morrison, and Mueser (1990) have criticized the stepwise approach of problem solving as not being representative of the actual process by which people confront day to day problems. Rather than being strategic in their approach towards common problems, individuals tend to draw on responses automatically with little cognitive mediation. People ad- dress novel problems in which they lack well-rehearsed responses intu- itively rather than using means-end logical analysis (Kitchener, 1983).
Whether problem solving is a stepwise process in normal individuals has not been resolved empirically. However, as a technique, the seven steps provide a useful prosthesis for guiding socially disordered pa- tients in resolving interpersonal difficulties. This prosthesis may not totally approximate normative problem solving; artificial limbs do not always look exactly like arms and legs. However, the clearly specified steps of problem solving assist cognitively limited patients in better understanding their problems and in figuring out solutions. Still there are some patients with sufficiently severe cognitive and intellectual impairments who are unable to readily learn these skills (Corrigan et
Patrick W. Corrigan, Psy.D. and Donna Kayton-Weinberg, MS 455
al., 1991; Massel et al., 1991). As a result, the cognitive requirements of problem-focused CM may preclude a segment of the severely disturbed population from benefiting from this approach.
Problem-focused CM differs from aggressive CM in another signifi- cant way. Where aggressive CM requires extraordinary efforts to as- sure that community goals are accomplished, practitioners of problem- focused CM view errors in the at ta inment of community goals as oppor- tunities to learn to fine tune problem solving skills. Hence, problem- focused case managers are more likely to permit their patients to fumble with at taining community needs and to make mistakes. As a result, patient goals are not likely to be as quickly resolved as peers par taking in aggressive interventions. Given the immediacy and neces- sity of some patients' goals, this approach may have grave implications. For example, the homeless patient in the middle of winter needs to find emergency shelter at once. In this situation, a more aggressive ap- proach is indicated. Alternately, the case manager may decide to inter- vene aggressively in situations where the problem-focused approach causes patients to become discouraged with frequent wrong decisions.
The immediacy and necessity of patients' goals is moderated by their support network. Individuals with a large and satisfactory network of family and friends are better able to address needs tha t occur in their lives (Sarason & Sarason, 1986; Sarason, Sarason, & Shearin, 1986). The support network of many patients with severe mental illness is smaller and less intimate than their peers (Tolsdorf, 1976). Neverthe- less, case managers may adopt problem-focused strategies for highly demanding life needs if the patient has family or friends that can lend support.
INTEGRATING A GGRESSIVE AND PROBLEM-FOCUSED CM
Kanter (1989) has called for development of a CM system in which the intensity of work with an individual patient is t i trated with that per- son's changing needs; the lability of patients' state and needs is espe- cially marked in light of recent advances in psychopharmacology. Im- plicit in Kanter's recommendation is that individual differences exist in patients' need for various CM services. For example, research suggests that the course of severe mental illness within a patient may vary widely from a progressively worsening downhill trend at one extreme to total remission and performance of relatively "normal" social goals at the other (Harding, 1988). Hence, case managers need to use strategies
456 Community Mental Health Journal
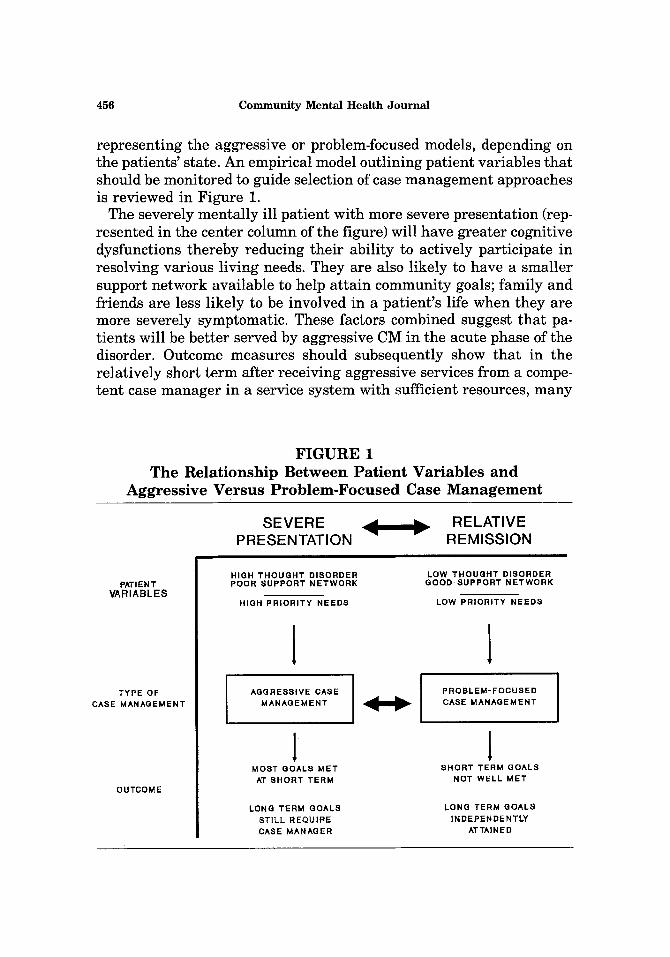
representing the aggressive or problem-focused models, depending on the patients' state. An empirical model outlining patient variables that should be monitored to guide selection of case management approaches is reviewed in Figure 1.
The severely mentally ill patient with more severe presentation (rep- resented in the center column of the figure) will have greater cognitive dysfunctions thereby reducing their ability to actively participate in resolving various living needs. They are also likely to have a smaller support network available to help at tain community goals; family and friends are less likely to be involved in a patient's life when they are more severely symptomatic. These factors combined suggest that pa- tients will be better served by aggressive CM in the acute phase of the disorder. Outcome measures should subsequently show that in the relatively short term after receiving aggressive services from a compe- tent case manager in a service system with sufficient resources, many
FIGURE 1 The Relationship Between Patient Variables and
Aggressive Versus Problem-Focused Case Management
SEVERE PRESENTATION
RELATIVE REMISSION
P~IENT VARIABLES
TYPE OF CASE MANAGEMENT
OUTCOME
HIGH THOUGHT DISORDER POOR SUPPORT NETWORK
HIGH PRIORITY NEEDS
LOW THOUGHT DISORDER GOOD SUPPORT NETWORK
LOW PRIORITY NEEDS
l 1 AGGRESSIVE CASE
MANAGEMENT I PROBLEM-FOCUSED
CASE MANAGEMENT
1 l MOST GOALS MET SHORT TERM GOALS AT SHORT TERM NOT WELL MET
LONG TERM GOALS STILL REQUIRE CASE MANAGER
LONG TERM GOALS |NDEPENDENTLY
ATTAINED

Patrick W. Corrigan, Psy.D. and Donna Kayton-Weinberg, MS 457
of the patient's needs will be met. However, problem-focused strategies should be introduced as patients improve.
Patients are better able to participate in CM planning and are more likely to learn the components of problem solving when they are in a relatively stable stage of their illness where cognitive deficits are di- minished. Case managers should introduce problem-focused strategies slowly by demonstrating the process around a specific, low priority problem with which the patient is struggling. In the beginning, the case manager assumes responsibility for guiding the patient through the seven problem solving steps. As the patient masters these steps, the case manager plays a less essential role so that eventually, the input of the professional is not needed to resolve some life difficulties.
When starting the problem-focused approach, specific problems are not likely to be quickly resolved. As a result, the priority of presenting problems and needs should be regularly assessed. The case manager may decide to include more aggressive approaches for some life prob- lems. A dynamic mix of aggressive and problem-focused approaches will help patients learn how to better meet their life demands and become less dependent on the mental health system.
REFERENCES
Anthony, W. A., & Blanch, A. (1989). Research on community support services: What have we learned. Psychosocial Rehabilitation Journal, 12, 55-81.
Bachrach, L. L. (1981). Deinstitutionalization: Development and theoretical perspectives. In I. D. Rutman (Ed.). Planning for deinstitutionalization: A review of principles, methods, and appli- cations (pp. 5-23). Atlanta, GA: Project Share.
Bachrach, L. L. (1989). Case management: Toward a shared definition. Hospital and Community Psychiatry, 40, 883-884.
Baker, F., & Intagliata, J. (1992). Case management. In R.P. Liberman (Ed.), Handbook of psychiatric rehabilitation, (pp. 213-244). New York: Pergamon.
Bellack, A. S., Morrison, R. L., & Mueser, K. T. (1990). Social problem solving in schizophrenia. Schizophrenia Bulletin, 15, 101-116.
Bond, G. R. (1984). An economic analysis of psychosocial rehabilitation. Hospital and Community Psychiatry, 35, 356-362.
Caragonne, P. (1981). A twenty-two site analysis of case management work activity components. Austin, TX: Case Management Center.
Corrigan, P.W., Wallace, C.J., Green, M.F., & Schade, M.L. (1991). Cognition and social function- ing in schizophrenia. Presentation at the Annual Meeting of the American Psychiatric Associa- tion.
D'Zurilla, T.J. (1986). Problem solving therapy: A social competence approach to clinical interven- tion. New York: Springer.
Emerson, E., & Emerson, C. (1987). Barriers to the effective implementation of habilitative behavioral programs in an institutional setting. Mental Retardation, 25, 101-106.
Essock-Vitale, S. (1987). Patient characteristics predictive of treatment costs on inpatient psychi- atric wards. Hospital and Community Psychiatry, 38, 263-269.
458 Community Mental Health Journal
General Accounting Office. (1978). Returning the mentally disabled to the community: Govern- ment needs to do more. Comptroller General's Report to the Congress. Washington, D.C.
Goldman, H. H., Gatozzi, A. A., & Taube, C. A. (1981). Defining and counting the chronically mentally ill. Hospital and Community Psychiatry, 32, 22.
Hansen, D.J., St. Lawrence, J.S., & Christoff, K.A. (1985). Effects of interpersonal problem-solving training with chronic aftercare patients on problem-solving component skills and effective- ness of solution. Journal of Consulting and Clinical Psychology, 53, 167-174.
Harding, C.M. (1988). Course types in schizophrenia. Schizophrenia Bulletin, 14, 633-644. Harris, M., & Bergman, H. C. (1988). Misconceptions about use of case management services by
the chronic mentally ill: A utilization analysis. Hospital and Community Psychiatry, 39, 1276-1280.
Herz, M. I., Endicott, J., Spitzer, R. L., & Mesnikoff, A. (1971). Day versus inpatient hospitaliza- tion: A controlled study. American Journal of Psychiatry, 127, 1371-1382.
Intagliata, J. (1982). Improving the quality of community care for the chronically mentally disabled: The role of case management. Schizophrenia Bulletin, 8, 655-674.
Johnson, P. J., & Rubin, A. (1983). Case management in mental health: A social work domain? Social Work, Jan.-Feb., 49-53.
Kanter, J. (1989). Clinical case management: Definition, principles, components. Hospital and Community Psychiatry, 40, 361-368.
Kitchener, K.S. (1983). Cognition, metacognition, and epistemic cognition: A three-level model of cognitive processing. Human Development, 26, 222-232.
Lamb, H. R. (1980). Therapist-case managers: More than brokers of services. Hospital and Commu- nity Psychiatry, 31, 762-764.
Lamb, H. R. (1982). Young adult chronic patients: The new drifters. Hospital and Community Psychiatry, 33, 465-468.
Liberman, R. P., Mueser, K. T., & Wallace, C. J. (1986). Social skills training for schizophrenic individuals at risk for relapse. American Journal of Psychiatry, 143, 523-526.
Massel, H.K., Corrigan, P.W., Liberman, R.P., & Milan, M. (1991). Conversation Skills Training in Thought-Disordered Schizophrenics Through Attention Focusing. Psychiatry Research, 38, 51-61.
Mechanic, D., & Aiken, L. H. (Eds.). (1989). Paying for Services: Promises and Pitfalls of Capitation. San Francisco: Jossey-Bass.
Mechanic, D., & Rochefort, D. A. (1990). Deinstitutionalization: An appraisal of reform. Annual Review of Sociology, 16, 301-327.
Modrcin, M., Rapp, C. A., & Poertner, J. (1988). The evaluation of case management services with the chronically mentally ill. Evaluation and Program Planning, 11, 307-314.
Mosher, L. R., & Menn, A. Z. (1978). Community residential treatment for schizophrenia: Two-year follow-up. Hospital and Community Psychiatry, 29, 715-723.
Mueller, J., & Hopp, M. (1983). A demonstration of the cost benefits of case management services for discharged mental patients. Psychiatric Quarterly, Spring, 17-24.
Sarason, I.G., & Sarason, B.R. (1986). Experimentally provided social support. Journal of Person- ality and Social Psychology, 50, 1222-1225.
Sarason, I.G., Sarason, B.R., & Shearin, E.N. (1986). Social support as an individual difference variable: Its stability, origins, and relational aspects. Journal of Personality and Social Psychology, 50, 845-855.
Schwartz, S. R., Goldman, H. H., & Churgin, S. (1982). Case management for the chronic mentally ill: Models and dimensions. Hospital and Community Psychiatry, 33, 1006-1009.
Siegel, J. M., & Spivack, G. (1976a). A new therapy program for chronic patients. Behavior Therapy,. 7, 129-130.
Siegel, J. M., & Spivack, G. (1976b). Problem solving therapy: The description of a new program for chronic psychiatric patients. Psychotherapy Theory, Research, and Practice, 13, 368-373.
Stein, L. I., & Test, M. A. (1978). An alternative to mental hospital treatment. In L. I. Stein & M. A. Test (Eds.). Alternatives to Mental Hospital Treatment. New York: Plenum.
Surles, R. C., & McGurrin, M. C. (1987). Increased use of psychiatric services by young chronic mentally ill patients. Hospital and Community Psychiatry, 38, 401-405.
Test, M. A., & Stein, L. I. (1978). Community treatment of the chronic patient: Research overview. Schizophrenia Bulletin, 4, 350-364.
Tolsdorf, C.C. (1976). Social networks, support, and coping. Family Process, 15, 407-418. Wallace, C. J., & Liberman, R. P. (1985). Social skills training for patients with schizophrenia: A
controlled clinical trial. Psychiatry Research, 15, 239-247.