Embed Size (px)
Citation preview

Ai Ling TanGynaecological OncologistAscot Clinic/ADHB
NCSP UPDATE & PRIMARY HPV SCREENING


NCSP annual monitoring report 2010-11
Since 2005 cancer rates stable

Coverage rates by age

Coverage rates by ethnicity

Ethnic Disparities=WORK REQUIRED!!
• Participation, retention and follow up of abnormalities
• 3 year coverage – Maori, Pacific Island and Asian women <50% compared to European women > 77%
• Adjustment for hysterectomies, coverage goal is 75%
• Incidence and mortality rates in European women is 30% lower

Changes to the Standards 2013

Future direction of NCSP
Challenges •Improve coverage •Achieve equity in coverage and incidence •Implement the Parliamentary review report recommendations
•Accurate electronic colposcopy data transfer•Linkage to immunisation register•2015 Audit cycle

The Sun is setting on the Pap Smear

Wright and Schiffman (2003) NEJM
Natural History of HPV Infections

Natural History of Cervical Carcinogenesis
NormalCervix
Mild Cytologic and/orHistologic Abnormalities
PrecancerCervicalCancer
HPV=human papillomavirus.Schiffman M, Kjaer SK. J Natl Cancer Inst Monogr. 2003;(31):14-19.
HPV
Progression
RegressionClearance
Infection InvasionHPV- Infecte
d Cervix
Primary prevention
Secondary prevention
Triage strategies with HPV testing, P16INK4a, others
HPV
Test

CvC
x Cases/100,000
0
5
10
15
20
25
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 >65
Age (years)
HP
V P
reva
len
ce (
%)
0
2
4
6
8
10
12
14
16
18
20
HPV
Cervical Cancer
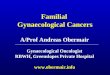
Sources: NCI SEER Data, 1990-94; Melkert et al., 1993. Int J Canc 53:919.
Relationship of Age to HPV Prevalence and Incidence of Cervical Cancer

Central/South America
Northern Africa
North America/Europe
South Asia
16
18
45
31
33
HPV Type
52
Others
Prevalence of HPV Types in Cervical Cancer
58
57
12.6
69.7
14.6
67.6
1752.5
25.7

HPV is detectable in over 90% of cervical cancers in NZ

Cytology
HPV DNA
Biomarkers
[p16/Ki67]
HPV mRNA
NO
WF
UT
UR
EChanging Cervical Screening

Cytology versus HPV testing
Subjective Objective

HPV DNA testsCobas 4800 HPV [Roche]
Digene HC-2 [Qiagen]Cervista HPV HR
[Hologic]Cervista HPV16/18
[Hologic]
FDA approved HPV tests[for clinical use]
HPV RNA testsAptima HPV assay [Hologic/ GenProbe]

Introduction of HPV testing
• Triage of low grade smears• Test of cure post LLETZ• Historical test of cure
• Primary HPV screening

HPV triage of ASCUS/LSIL
Women > 30 years ASCUS / LSIL
HrHPV reflex test
Repeat cytology at 12 months
HrHPV negative
Refer to colposcopyReturn to 3 yearly
screening
HrHPV positive
Cytology > ASC-US Cytology negative
HPV Testing Guidance 1
Triage of women 30 years and over with ASC-US or LSIL(who have not had an abnormal smear within the last 5 years)
Refer to colposcopy

Risk for CIN 3+
25%
15%
0.0%
HPV 16 positive
Any high-risk HPV(+) other than HPV 16
Castle P et al J Natl Cancer Inst 2005;97:1066-71
35%
7.5%
32.5%
39.5%
8.4% 9.5%
ASC-US LSIL LSILASC-US

Post treatment HPV testing
• Substitutes for annual smears for life
SMEAR + HPVNEGATIVE
SMEAR +HPV NEGATIVE
NORMAL SCREENING
+

Cancer Res; November 1 2006

Test of cure studyIf cytology and HPV testing are negative at six months then the risk of CIN 2+ over the next two years was less than 0.5%
Kitchener et al Lancet Onc 2009
HPV testing using HC2 is the most sensitive test of cure and is superior to either cytology or colposcopy Paraskevaidis et al Cancer Treat Rev, 2004
The addition of cytology to HPV testing improves the sensitivity of sampling. The optimum time for the double test (cytology and HC2) is probably at 18–24 months
Coupe et al BJOG, 2007

Post Treatment

Previous Treatment

Why change now?
High-Risk HPV DNA Testing is more sensitive in detecting high grade disease than a Pap test Clavel C, et al. Brit J Cancer, 2001;89:1616-1623
A positive high-risk HPV result is an objective risk indicator for the development of high-grade disease and cancer
Screening is less effective with reduced prevalence
Lorincz A., Richart, R. Arch Pathol Lab Med, 2003;127: 959-968.

HPV Vaccination

Confidence in new test with longer screening interval

• Over 60,000 women in analysis• All North American and European
studies where cytology is used as the primary screen and where HR HPV was run in parallel

Comparison of HPV DNA vs Cytology: Europe / USA Combined Results
# Screened: >60,000: HC2 + Cytology Age: 30-60 (majority)
CIN 3+ CIN 2+
HPV DNA
Cytology
207 125 33 365 313 183 38 534Cases:
Se
ns
itiv
ity
(%
)
Cuzick et al. Int J Cancer, April 2006

Dillner et al 2008 BMJ
www.canserforum.com (Cuzick et al, 2006)
Performance characteristics:cytology and HPV testing[meta analysis]

Cumulative incidence of Cancer in women with negative entry test
3.5 years 5.5 years
Experimental arm (HPV-based)
4.6 per 105 (1.1 – 12.1)
8.7 per 105 (3.3 – 18.6)
Control arm (cytology based)
15.4 per 105 (7.9 – 27.0)
36.0 per 105 (23.2 – 53.5)
Rate ratio was 0.30 (0.15 – 0.60)
Guglielmo Ronco et al Lancet 2014;383:524-532
HPV-based screening provides 60 – 70% greater protection against invasive cervical carcinomas compared with
cytology

Detection of cancer using HPV vs cytology
Ronco et al Lancet 2014

HPV analysis – primary screening
•Primary screening with HPV may be effective in women over 30
• Arbyn meta-analysis of 49 studies
HPV testing showed a higher sensitivity for CIN 2+ and CIN 3+ relative to cytology
HPV negative women had a significantly lower cumulative incidence of CIN 3+ in the second round of screening compared with cytology negative women

HPV analysis – primary screeningKitchener et al Eur J Cancer 2011
ARTISTIC screening trial
negative HPV test provides the same degree of ‘protection’ over two screening rounds as negative cytology for one screening round
allows screening interval to be increased to 5-6 years or longer in women over 30 Yr

Summary
Sensitivity Specificity
HPV (primarily HC2) 96% 92%
CYTOLOGY 53% 96%
Management Problems•Similar positive predictive value for CIN3 detection BUT•Too many women with HPV positive normal smears

ADVANTAGES OF USING HPV TESTING AS THE SOLE PRIMARY SCREENING TEST
Automated, Objective, Very Sensitive Test
Quality controlMedico-legal
Cytology reserved for 6-10% of women
High qualityFewer, more focused cyto-screenersAvoids triage of HPV negative ASCUS/LSIL
Longer screening interval
CostConvenience

So why not just use HPV alone?
• Use of HPV testing alone as primary screening test will yield too many positives
• Would generate too many colposcopy referrals
• Not practical <30 as prevalence too high
• Triage further with use of cytology• Possible alternative triage with genotyping

•Rijkaart et al. concluded that referral for cytology followed by repeat cytology led to an acceptable colposcopy referral rate [33.4% of positives] and a high negative predictive value [99.3%]

Vaccin
e, V
ol x
x S
up
ple
men
t x, 2
00
8. ©
20
06
Else
vie
r Limite
d. A
ll righ
ts rese
rved
. Ch
ap
ter 0
3. F
igu
re 3
POTENTIAL NEW SCREENING ALGORITHM
Use of HPV TESTING as the primary screening test and of CYTOLOGY to triage HPV positive women
WOMEN AGED 35 - 64 YEARSHPV TEST
Negative Positive
Normal orASCUS
≥ LSIL
Cytology Negative
HPV Negative
Cytology ≥
LSILHPV Positive & Cytology < LSIL
HPV Negative & CytologyASCUS
CYTOLOGY
COLPOSCOPYHPV & CYTOLOGYat 6 – 12 months
COLPOSCOPYNORMAL
5 YEAR RECALLHPV & CYTOLOGYat 6 – 12 months
NORMAL 5 YEAR RECALL

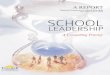
HC2=Hybrid Capture 2 HPV Test.Khan M. et al. J Natl Cancer Inst. 2005;97:1072-1079.
Cumulative Incidence of CIN 3+ in 20,512 Women: 10-year Follow-up
0
5
10
15
20
4.5 15.0 27.0 39.0 51.0 63.0 75.0 87.0 99.0111.0119.5Follow-up time (months)
Cu
mu
lati
ve in
cid
en
ce r
ate
(%
)
Positive for HPV 16
Positive for HPV 18
Positive for non-HPV 16/18oncogenic types in HC2Oncogenic HPV negative

Vacc
ine,
Vol xx S
up
ple
men
t x,
20
08
. ©
20
06
Els
evie
r Li
mit
ed
. A
ll ri
gh
ts r
ese
rved
. C
hap
ter
03.
Fig
ure
4
POTENTIAL FUTURE SCREENING ALGORITHM
Use of HPV TESTING as the primary screening test and of CYTOLOGY and HPV TYPING to triage HPV positive women to eliminate a ‘short follow up’ group. Triage with P16
AND MRNA may also be useful, but this is less well established
WOMEN AGED 35 - 64 YEARSHPV TEST
Negative Positive
</= LSIL > LSIL
Negative
Positive
NORMAL 5 YEAR RECALL
CYTOLOGY
COLPOSCOPY3 – 5 YEAR
RECALL
COLPOSCOPYHPV 16/18 Typing

Screening Age….
P Sasieni BMJ 2009
High incidence hpv and CINLow risk of cancer
Spontaneous regression
Impact of HPV vaccination
Odds of developing cancer between screened and unscreened as a function of age

Later age of onset of screeningIncidence HPV in young women
Age HrHPV Pos Cyto Pos
> 35 5.8% 2.5%
< 35 13% 3.6%
< 25 34 – 47 %

Self Collection for the under- and never -screened women


Primary HPV Screening
USA - Co-testing (Cytology and HPV testing) - Primary HPV screening with genotyping for women 25yo and older
Intention to commence in 2016
Netherlands - HPV testing with reflex LBC from 30
Australia - HPV testing with partial genotyping and reflex LBC

Conclusion
• Primary HPV screening more sensitive• Negative HPV test confers greater protection
• Longer screening intervals• Raise screening age
• Need to triage with cytology +/- genotyping
• Need to raise vaccination rates to be most effective

A new dawn is rising…….
The Era of Primary HPV Cervical Screening