Embed Size (px)
Citation preview

Aid Stagnation, Shifting Disease Burdens, and the SDGs:
How Will Global Health Meet the Challenges?
Gavin Yamey MD MPH
Professor of the Practice of Global Health & Public PolicyDirector, Center for Policy Impact in Global Health
Associate Director for Policy, Duke Global Health Institute
July 4, 2016


Editorial: wjm, PLOS Medicine, PLOS NTDsJournalism: KFF Global Health Reporting Fellow
Policy research: Evidence to Policy initiative (E2Pi), UCSFTeaching: Global health policy


This is my 7th Geneva trip

Aims of the course
3 key lenses:
- transitions
- SDGs
- GH2035
What will it take to reach GH2035 goals?
How the course addresses post-2015 challenges
Agenda

Aims of the course
3 key lenses:
- transitions
- SDGs
- GH2035
What will it take to reach GH2035 goals?
How the course addresses post-2015 challenges
Agenda

Aims of the Course: the 4Cs
CRASH COURSE• Global health landscape: actors, architecture,
governance, financing• Evolution of our global health challenges:
what lies ahead• Policy options for the next era and beyond
CONTEXT• Where do the Geneva-based global health
organizations fit into this picture?• What role do they play in meeting the health
needs of the world’s most vulnerable people?
CONNECTIONS • Build personal networks of friends, colleagues, and mentors
CURIOSITY • Ask questions of the world’s leading voices in global health

Aims of the course
3 key lenses:
- transitions
- SDGs
- GH2035
What will it take to reach GH2035 goals?
How the course addresses post-2015 challenges
Agenda

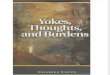
1993-2013: Extraordinary Health Progress
Female life expectancy at birth for select countries compared to the frontierThe frontier line indicates female life expectancy in the best-performing country in that year, which has been Japan for the past 20 years.
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

MDGs Were Catalytic
“Substantial progress since the Millennium Declaration is an encouraging sign of the effect of global action”
Murray CJ et al, Lancet 2014, Jul 21
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

Unprecedented Mobilization of Aid for Health
Figure from Financing Global Health 2013, IHME
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

Scientific Innovations Played a RoleLens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

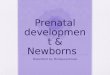
1993-2013: Extraordinary Economic Progress
Movement of populations from low income to higher income between 1990 and 2011
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

Epidemiological & demographic
Financing
Governance
MDGs to SDGs
1
2
3
4
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

The MDGs: Simplicity and Clarity
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

The 17 SDGs: An Expansive Agenda
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

SDG 3: The Global Health Goal
“Ensure healthy lives and promote wellbeing for all at all ages”
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

9 TARGETS
4 MEANS OF IMPLEMENTATION
SDG 3: Targets and Approaches
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

3.1 Reduce global maternal mortality ratio to under 70 per 100,000 live births 3.2 End preventable deaths of newborns and under-five children 3.3 End the epidemics of AIDS, tuberculosis, malaria, and neglected tropical diseases and combat hepatitis, water-borne diseases, and other communicable diseases 3.4 Reduce by one-third pre-mature mortality from NCDs3.5 Strengthen prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol 3.6 Halve global deaths and injuries from road traffic accidents 3.7 Ensure universal access to sexual and reproductive health care services3.8 Achieve universal health coverage, including financial risk protection, access to quality essential health care services, and access to safe, effective, quality, and affordable essential medicines and vaccines for all 3.9 Substantially reduce number of deaths and illnesses from hazardous chemicals and air, water, and soil pollution and contamination
SDG 3: The Nine Targets (2030 End Date)Numeric targets
Zero targets
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

SDG 3: The 4 Means of Implementation
3.a Strengthen implementation of Framework Convention on Tobacco Control 3.b Support R&D of vaccines and medicines for the communicable diseases/NCDs that primarily affect developing countries, provide access to affordable essential medicines and vaccines, provide access to medicines for all 3.c Increase substantially health financing and the recruitment, development and training and retention of the health workforce in developing countries, especially in LDCs and SIDS 3.d Strengthen capacity of all countries, particularly developing countries, for early warning, risk reduction, and management of national and global health risks
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

Global Health 2035: WDR 1993 @20 Years
The World Bank’s World Development Report 1993
• Evidence-based health expenditures are an investment not only in health but in economic prosperity
• Additional resources should be spent on cost-effective interventions to address high-burden diseases
The Lancet Commission on Investing in Health (chaired by Lawrence Summers and Dean Jamison)
• Re-examines the case for investing in health
• Proposes a health investment framework for low- and middle-income countries
• Provides a roadmap to achieving dramatic gains in global health by 2035
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

2015-2035: Three Domains of Health Challenges
High rates of avertable infectious, child, and
maternal deaths
Unfinished agenda
Global shift towards non-communicable diseases
(NCDs) and injuries
Emerging agenda
Impoverishing medical expenses, unproductive
cost increases
Cost agenda
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

Global Health 2035: 4 Key Findings
The returns from investing in health are extremely impressive
A grand convergence in health is achievable within our lifetime
Fiscal policies are a powerful, underused lever for curbing non-
communicable diseases and injuries
Pro-poor pathways to universal health
coverage are an efficient way to achieve health
and financial protection
Lens 1: Transitions Lens 2: SDGs Lens 3: Global Health 2035

Aims of the course
3 key lenses:
- transitions
- SDGs
- GH2035
What will it take to reach GH2035 goals?
How the course addresses post-2015 challenges
Agenda

The returns from investing in health are extremely impressive
A grand convergence in health is achievable within our lifetime
Fiscal policies are a powerful, underused lever for curbing non-
communicable diseases and injuries
Pro-poor pathways to universal health
coverage are an efficient way to achieve health
and financial protection
The Global Health 2035 Goals

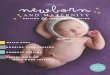
Two Centuries of Divergence; ‘4C Countries’ Then Converged
1750 1800 1850 1900 1950 2000
01
00
200
30
04
00
Under-five mortality, China and Sweden, 1751-2008
Year
5q0
pe
r 1
,00
0 liv
e b
irth
s
Sweden
China
Gap between China and Sweden

Now on Cusp of a Historical Achievement:Nearly All Countries Could Converge by 2035

Convergence to Which Countries?
Diverse group of middle-income
countries showed the way
Previously had high death rates
Low- or lower middle-income in
1991
Achieved high level of health status by
2011 largely because of scale-up of health sector interventions
“4C Countries”
Costa Rica, Cuba, Chile, China
We show that nearly all countries could
reach the same health status by
2035

Strategy 1: Aggressive Scale-Up of Today’s Tools
Accelerated scale-up of coverage
Global Investment Framework for Women's & Children's Health
• RMNCH, including family planning, pregnancy-related interventions, safe abortion and complications, and maternal nutrition
• HIV• Malaria• Tuberculosis• Neglected tropical diseases

Strategy 2: Strengthen Health Delivery Systems
Photo: GAVI, the Vaccine Alliance

Strategy 3: Develop Tomorrow’s Tools

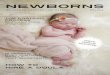
Factors Accounting for Decline in Child Mortality, LICs and MICs, 1970-2000
Jamison, Murphy, Sandbu. Why Has Under-5 Mortality Decreased at Such Different Rates inDifferent Countries? Health Economics 2016;48:16-25

Impact and Cost of Convergence
Low-income countries Lower middle-income countries
Annual deaths averted from 2035 onwards
4.5 million 5.8 million
Approximate incremental cost per year, 2016-2035
$25 billion $45 billion
Proportion of costs devoted to structural investments in health system
60-70% 30-40%
Proportion of health gap closed by existing tools (rest closed by new tools)
2/3 4/5

New Global Map of Disease: “Pockets of Poverty”
Under-5 deaths in rural versus urban India

Global Health 2035: 4 Key Findings
The returns from investing in health are extremely impressive
A grand convergence in health is achievable within our lifetime
Fiscal policies are a powerful, underused lever for curbing non-
communicable diseases and injuries
Pro-poor pathways to universal health
coverage are an efficient way to achieve health
and financial protection

Convergence Has Impressive Benefit: Cost Ratio
“Further proof that improvements in human
survival have economic value well beyond their direct links
to GDP”
Jim KimWorld Bank President

Sources of Income to Fund Convergence
Economic growth
• IMF: low- and lower middle-income countries to add $9.6 trillion/y to GDP from 2015-2035
• Cost of convergence ($70 billion/y) is about 1% of anticipated growth
Mobilization of domestic resources
• Taxation of tobacco, alcohol, sugar, extractive industries
Inter-sectoral reallocations and efficiency gains
• Removal of fossil fuel subsidies, health sector efficiency
• Subsidies account for 6.5% of global GDP
Development assistance for
health
• Will still be crucial for achieving convergence
• Health aid will need to evolve to support global functions

The returns from investing in health are extremely impressive
A grand convergence in health is achievable within our lifetime
Fiscal policies are a powerful, underused lever for curbing non-
communicable diseases and injuries
Pro-poor pathways to universal health
coverage are an efficient way to achieve health
and financial protection
The Global Health 2035 Goals

Single Greatest Opportunity To Curb NCDs is Tobacco Taxation
50% rise in tobacco price from tax increases in China
prevents 20 million deaths + generates extra $20 billion/y in next 50 y
additional tax revenue would fall over time but would be higher than current levels even after 50 y
largest share of life-years gained is in bottom income quintile

Essential Package of Clinical Interventions
WHO “best buys”
NCD Intervention
Liver cancer Hepatitis B vaccine
Cervical cancer VIA and treatment of pre-cancerous lesions
CVD and diabetes Counselling and multi-drug therapy for high-risk patients
Heart attack Aspirin

We Recommend Scale-up in All Countries
Cost-effective
80% coverage by 2020 would avert 37% of global burden of cardiovascular disease
Low coverage
Except for hepatitis B vaccine, very low coverage across LICs/MICs
Feasible
1st step for all countries; costs $9bn/y; we argue that HPV
vaccine & morphine should be included

Phased Expansion Pathways
Choice of packages and expansion pathway will vary with pattern of disease, delivery capacity, domestic health spending

Sudden Price Drops Affect Expansion Pathway
For drugs, diagnostics, and vaccines, which can usually be delivered without complex infrastructure, price reductions can sometimes occur very rapidly
Price drop might be large enough for intervention to be used earlier in expansion pathway
Price

Global Health 2035: 4 Key Findings
The returns from investing in health are extremely impressive
A grand convergence in health is achievable within our lifetime
Fiscal policies are a powerful, underused lever for curbing non-
communicable diseases and injuries
Pro-poor pathways to universal health
coverage are an efficient way to achieve health
and financial protection

Our Recommendation on UHC:Pro-Poor Pathway (Blue Shading)
+ essential package for NCDIs

Benefits to Countries of Adopting Pro-Poor UHC
1 • Poor gain the most in terms of health and financial risk protection
2 • Approach yields high health gains per $ spent
3 • Public money is used to address negative externalities of infectious disease transmission
4 • Implementation success in many low- and middle-income countries has shown feasibility

Aims of the course
3 key lenses:
- transitions
- SDGs
- GH2035
What will it take to reach GH2035 goals?
How the course addresses post-2015 challenges
Agenda

The returns from investing in health are extremely impressive
A grand convergence in health is achievable within our lifetime
Fiscal policies are a powerful, underused lever for curbing non-
communicable diseases and injuries
Pro-poor pathways to universal health
coverage are an efficient way to achieve health
and financial protection
Lecture: Women’s, Children’s and Adolescents’ Health in the SDG eraSite visits: Global Fund, GAVI, WHO SHOC room, FIND & MMVPolicy competition: malaria vaccine
Lecture: Global health financing
Lecture: Global mental healthPanels: Tobacco control, violence and injuries
Panel: UHC
COURSE ROADMAP1

The returns from investing in health are extremely impressive
A grand convergence in health is achievable within our lifetime
Fiscal policies are a powerful, underused lever for curbing non-
communicable diseases and injuries
Pro-poor pathways to universal health
coverage are an efficient way to achieve health
and financial protection
COURSE ROADMAP2
Cross-cutting issues: governance, trade, humanitarian intervention
Panel: Governance for global healthSite visits: MSF, WTO