Embed Size (px)
Citation preview
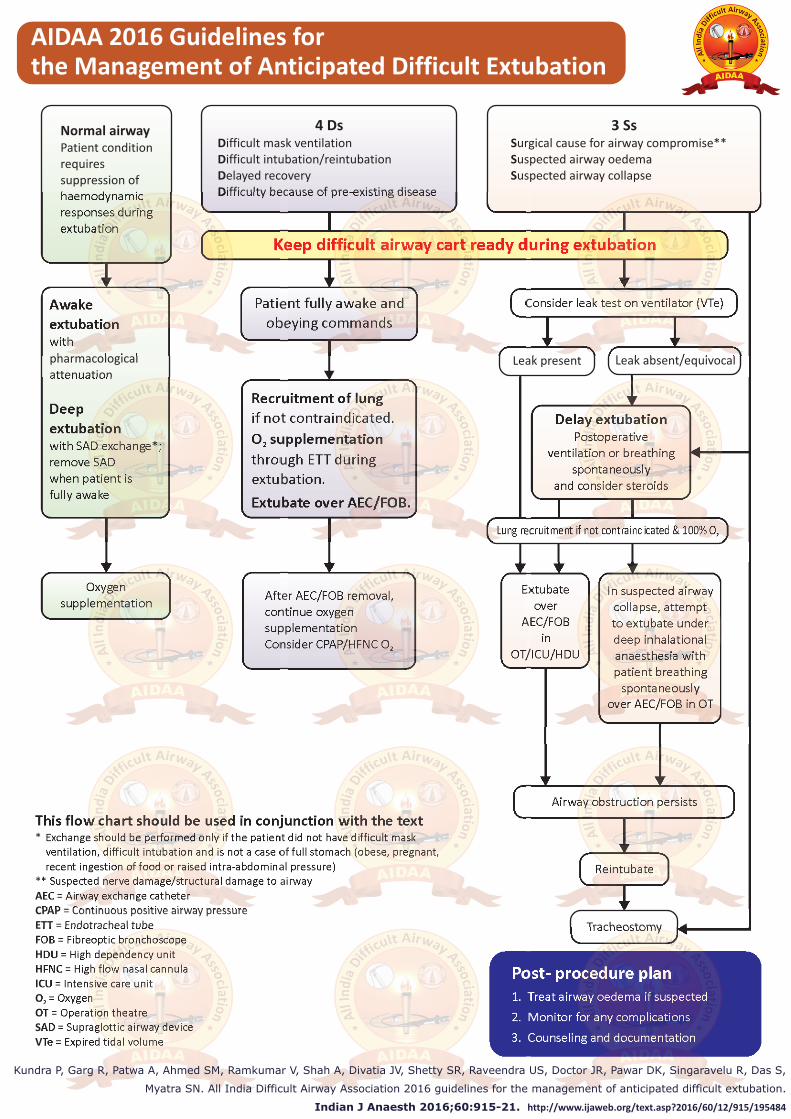
AIDAA 2016 Guidelines for the Management of Anticipated Difficult Extubation
This flow chart should be used in conjunction with the text * Exchange should be performed only if the patient did not have difficult mask ventilation, difficult intubation and is not a case of full stomach (obese, pregnant, recent ingestion of food or raised intra-abdominal pressure)** Suspected nerve damage/structural damage to airway AEC = Airway exchange catheterCPAP = Continuous positive airway pressure ETT = Endotracheal tubeFOB = Fibreoptic bronchoscope HDU = High dependency unitHFNC = High flow nasal cannulaICU = Intensive care unitO = Oxygen 2
OT = Operation theatreSAD = Supraglottic airway device VTe = Expired tidal volume
Normal airwayPatient condition requires suppression of haemodynamic responses during extubation
After AEC/FOB removal,continue oxygen supplementationConsider CPAP/HFNC O2
In suspected airway collapse, attempt to extubate under deep inhalational anaesthesia with patient breathing
spontaneously over AEC/FOB in OT
Recruitment of lung if not contraindicated.
O supplementation 2
through ETT during extubation.
Extubate over AEC/FOB.
Awake extubation with pharmacological attenuation
Deep extubation with SAD exchange*; remove SAD when patient is fully awake
3 SsSurgical cause for airway compromise**Suspected airway oedemaSuspected airway collapse
4 DsDifficult mask ventilationDifficult intubation/reintubationDelayed recoveryDifficulty because of pre-existing disease
Keep difficult airway cart ready during extubation
Leak absent/equivocalLeak present
Airway obstruction persists
Tracheostomy
Reintubate
Extubate over
AEC/FOB in
OT/ICU/HDU
Oxygensupplementation
Patient fully awake and obeying commands
Consider leak test on ventilator (VTe)
Delay extubationPostoperative
ventilation or breathing spontaneously
and consider steroids
Lung recruitment if not contraindicated & 100% O2
Post- procedure plan1. Treat airway oedema if suspected
2. Monitor for any complications
3. Counseling and documentation
Kundra P, Garg R, Patwa A, Ahmed SM, Ramkumar V, Shah A, Divatia JV, Shetty SR, Raveendra US, Doctor JR, Pawar DK, Singaravelu R, Das S,
Myatra SN. All India Difficult Airway Association 2016 guidelines for the management of anticipated difficult extubation.
Indian J Anaesth 2016;60:915-21. http://www.ijaweb.org/text.asp?2016/60/12/915/195484





























