Embed Size (px)
Citation preview

Talk to Me Teamwork and Communication as Best Practices for
Patient Safety
September 29, 2015
Aileen R. Killen
Head of Casualty Risk Consulting
Healthcare
+1 646 857 0261
International Forum on Quality and Safety in Healthcare

Freedom from accidental injury (IOM)
Discipline in health care sector that applies safety science methods
toward the goal of achieving a trustworthy system of health care
delivery…an attribute of health care systems; it minimizes the
incidence and impact of, and maximizes recovery from, adverse
events (AHRQ).
The avoidance, prevention, and amelioration of adverse outcomes or
injuries stemming from the processes of health care. These events
include “errors”, “deviations”, and “accidents”. Safety emerges from
the interaction of components of the system; it does not reside in a
person, device or department (NPSF)
The absence of preventable harm to a patient during the process of
health care (WHO)
2
What is patient safety? Key definitions
Two or more individuals
Meaningful task interdependence
Have a leader
Have specialized member roles
and responsibilities
Intensive communication
3
Characteristics of all teams
What makes a team?

Posses specialized and
complimentary knowledge and
skills
Know their role and roles of
others on the team
Make decisions
Often function under high-
workload conditions
Act as a collective unit as a
result of interdisciplinary tasks
performed by team members
4
Characteristics
What is a health care team?
World Health Organization (2012)

Core teams
– Direct care providers
Coordinating teams
– Provide operational management and resource management for core
teams
Contingency teams
– Formed for emergent or specific events
Ancillary services
– Provide services that facilitate patient care
Support services and administration
– Leadership
5
Types of teams found in healthcare World Health Organization
World Health Organization (2012)

Team leadership
– Task Coordination and Planning
– Development and Motivation of team
Mutual performance monitoring
– Understand environment to identify lapses in task assignment or task overload
– Situational Awareness
Backup behavior
– Understand tasks of other team members to in order to redistribute work or support others
Adaptability
– Respond to changes in the environment
Team orientation
– Take others ideas into account
– Team goals more important than individual goals
6
Key dimensions of effective teams
Salas, E., Simms, D.E., & Burke, C.S. (2005).

Respect and trust in order to debrief and give feedback
Good communication skills to accurately convey information
Shared mental model (Situational awareness)
– Be on same page
– Be in same movie
Is your team
– Team of experts ?
or
– An expert team ?
7
Requirements for effective teams

What teamwork is
– Set of interrelated behaviors, cognitions and attitudes
– Distinct from task work
– Members anticipate each others needs
– Collective set of efficacy and “teamness”
– Provide back-up behaviors
What teamwork is NOT
– Not automatic response to putting people together
– You do not need to like all members of your team
– No need to work with team members on a permanent basis
8
Teamwork and patient safety
Salas (2008)

9
What’s different?
Action teams
– Conditions change frequently
– May be assembled ad hoc
– Have a dynamically changing
team membership
– May work together for short
periods of time
– Consist of specialists
– Have to integrate different
professional cultures
Teamwork in healthcare
Manser, T. (2009)

Transfer of information, idea, feelings
Functions of communication in a healthcare system
– Provides knowledge
– Establishes relationships
– Supports leaderships and team co-ordination
Model of communication
– Sender convert an idea into a message
– using medium (written, verbal) to transmit message to one or more
receivers
– who then translate the message back to the original idea
10
What is communication? World Health Organization (WHO)
World Health Organization (2009)

Transmission failures
– Information not transmitted – message is unclear
Ambiguity of message
Problem with medium
Reception failures
– Information not received
– Information with sent but misrepresented, ignored, etc.
11
What is communication? How can it fail?
Knowing the game plan
Getting in the huddle
Giving signals
Listening to the coach
Revising the game plan
Sitting on the bench
12
Team huddle
Effective communication

What we know about teamwork and communication
13
And the literature says….

Retrospective analysis of incident and adverse events found
communication and teamwork issues to be among the most frequent
contributing factors
Observational studies and retrospective analysis show that many
factors that contribute to incidents or adverse events come from
inadequate teamwork and NOT lack of clinical skills
Healthcare providers place a great deal of importance on aspects of
teamwork such as communication and collaboration
Studies identified differences in perceived quality of teamwork
between professional groups
Studies indicate staff perceptions of teamwork are related to quality
and safety of patient care
14
Key concepts about teamwork and safety From review of the literature (1998-2007)
Manser, T. (2009)

Patient safety; Hospital risk
WHO HOW MANY WHEN HOW
Hospital C-Suite
Executives and
Risk Managers
from hospitals
representative of
the US landscape
N=250 Hospital C-Suite
Executives
N=100 Risk Managers
46% CNO
40% COO
Remainder CEO, CMO
and CFO
Data collection
occurred
November 13 –
December 20, 2012
Computer-Assisted
Telephone
Interviews
Perspectives of hospital C-Suite and Risk Managers
AIG (2013)

Four core themes emerged…
1 Patient safety and financial sustainability challenge hospital C-Suite and
Risk Managers for their time and attention
2 Who is “responsible for” patient safety and who “owns” patient safety do
not fall within the same role at the hospital.
3 “Lack of teamwork, negative culture and poor communication” is
the number one barrier to ensuring a safe environment for patients.
4 Perceived “enhancements” to patient safety—such as technology, regulation
and metrics —can have the opposite effect.
AIG (2013)

17 17
Lack of teamwork, negative culture and communication are
seen as the top barrier to patient safety.
B5. In your own words, what do you feel are the barriers to improving patient safety in your hospital? (split sample;
n=125 C-Suite, n=96 Risk Managers)
*Statistically significant difference between C-Suite and Risk Managers
The culture between the nurses
and the physicians. The lack of
autonomy the nurses have. The
amount of control medical staff
have.
– C-Suite
“ “ The barriers are the
communication with the
healthcare team. The handoff from
one unit to another and from one
physician to another physician or
nurse is a hard transition for the
patient.
– Risk Manager
“ “ Barriers to Improving Patient Safety
42%
22%
18%
10%
8%
7%
13%
4%
3%
55%
10%
4%
3%
9%
14%
15%
10%
28%*
Lack of team work /
negative culture and
Lack of staff
Financial issues
Tim e
Resources/equipm ent
Training/education
O ther
Nothing
DK/Refused
C-suite
Risk M anagers
communication

18 18
Teamwork and communication problems are at the core of
patient safety risk.
B4. Which of the following contribute to patient safety risk? (n=250 C-Suite, n=100 risk managers)
*Statistically significant difference between C-Suite and Risk Managers
Prospective intervention study in Oxford, UK
Using models from Formula 1 and aviation to improve handovers from
surgery to ICU
Results
– Mean decrease in technical errors during handovers from 5.42 to 3.15
– Mean decrease in omissions 2.09 to 1.07
– Duration of handover reduced 10.8 to 9.4 minutes
39% of patients pre-intervention had more than one error in handover;
11.5 % of patients with new protocol
19
Effective communication Patient handover
Catchpole, KR, De Leval, MR, McEwan, A, Pigott, et al (2007)

Survey of 60 hospitals
Use of Safety Attitudes
Questionnaire
Response rate 77.1 %
(2,135 / 2,769)
20
In the eye of the beholder
Operating Room teamwork
Makary, MA, Sexton, JB, Freischlag, JA, Holzmulueller, et al (2006)

Differing perceptions
From members of the healthcare team
Anesth
.
Nurse
Surgeon
CRNA
Makary, MA, Sexton, JB, Freischlag, JA, Holzmulueller, et al (2006)

From the view of the surgeon
Makary, MA, Sexton, JB, Freischlag, JA, Holzmulueller, et al (2006)
Anesth
84%
Nurse
88%
Surgeon
85%
CRNA
87%
Differing perceptions

From view of anesthesiologist
Anesth
96%
Nurse
89%
Surgeon
70%
CRNA
92 %
Makary, MA, Sexton, JB, Freischlag, JA, Holzmulueller, et al (2006)
Differing perceptions
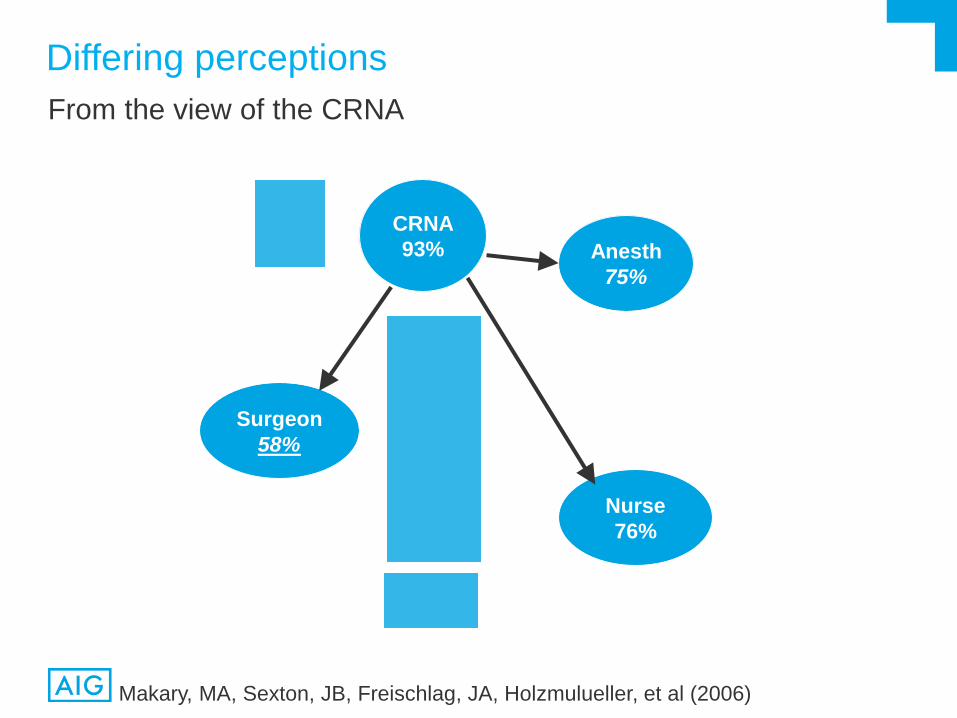
From the view of the CRNA
Makary, MA, Sexton, JB, Freischlag, JA, Holzmulueller, et al (2006)
Anesth
75%
Nurse
76%
Surgeon
58%
CRNA
93%
Differing perceptions

From the view of the OR nurse
Anesth
63%
Nurse
81%
Surgeon
48%
CRNA
68%
Differing perceptions
Makary, MA, Sexton, JB, Freischlag, JA, Holzmulueller, et al (2006)

Do not delay operating room start times ( Ali,et al , 2011) – 5-10 minute safety briefing between surgeons, anesthesia staff and
nursing staff to discuss operating list
– Great Western Hospital, UK
Reduce nonroutine events ( Einav, et al 2010)
– Reduction (25%) in number of nonroutine events with briefing;
– increase in number of surgeries with no nonroutine events ( Einav, et al 2010)
– Haifa Israel
Do not take a long time (Berenholtz,et al 2009) – 2.9 minutes for briefing
– 2.5 minutes for debriefing
– Baltimore, MD , USA
Improve compliance with antibiotic and DVT prophylaxis ( Lingard, et al (2011; (Paull, et al 2010) – Ontario, Canada
– USA
26
Briefings as a communication tool Preoperative briefings and huddles
Strategies from around the globe
27
International Experiences

Program developed to respond to areas identified as needing improvement in
culture surveys over several year
– Teamwork across hospital units
– Handover
Based on “ideal” communication and teamwork of Formula 1 car racing pit
crew
– Mind your Ps - 4 “P’s”
Presider : leadership
Player: role of each member
Process: vital steps
Purpose: common goal
28
An effective approach to patient safety National University Hospital Singapore
Mujumdar,S. & Santos, D (2014)

Need effective communication of the 4 Ps to execute the patient safety task at
hand
What else gets in the way?
– Number of lines of communication in complex patient care scenarios
– Mode of communication – oral, written, electronic
– Cultural factors
Nurses are narrative and descriptive
Physicians prefer brevity
Strategies
– Practice, Practice, Practice
Assertion
Empathy
SBAR
TeamSTEPPS®
29
An effective approach to patient safety National University Hospital Singapore

“Between the Flags” program in NSW Public Hospitals (2010)
– Over 200 facilities
Role of High reliability teams in responding to clinical deterioration
Based on work in 1980’s in UK to identify patients who were
deteriorating
– Vital signs thresholds
– Criteria for escalation
Evaluation under way
– Also role of culture on implementation
of program (with University of NSW)
30
Keeping patients safe New South Wales, Australia
www.cec.health.nsw.gov.au/programs/between-the-flags

Doing what we already know how to do
Create conditions that prompt, reward and facilitate appropriate
behaviors
7 step plan Overcoming educational barriers
1. Teach effective communication strategies e.g. SBAR
2. Train teams together
3. Train teams using simulation
– Overcoming psychological barriers
4. Define inclusive teams
5. Create democratic teams
– Overcoming organizational barriers
6. Support teamwork with protocols and procedures
7. Develop an organizational culture supporting healthcare teams
31
Overcoming barriers to effective communication University of Auckland, New Zealand
Weller, J., Boyd, M., & Cumin, D. (2014)

Means to reduce the authority gradient
– Among different professional groups
– Among senior and junior staff in the same professional groups
– Reluctance to speak up often related to previous rudeness or intimidation
Overcome ineffective communication due to differences in communication styles
Strategies
– Team Briefings and debriefings
You cant debrief it you did not brief (ark)
Huddles
– Structured Communication Tools
SBAR
CUS
Memory Joggers (checklists)
32
Strategies to improve communication University of Mandurah, Western Australia
Gluyas (2015)

A different methodology to study handoffs
Use of philosophy and methodology of Appreciative Inquiry (AI)
– Change management technique that looks at what works well
– Positive cousin of root cause analysis
Because most handoffs go well
– Structured interviews with 29 nurses, 5 ward clerks, 2 home health
coordinators, 9 allied health clinicians, 2 patients, 1 family member
– Key Themes
Identified situational variables necessary for perfect transfer
Mode and transfer –related communication
Important factors with patient and family
33
Building teamwork and trust University of Manitoba, Canada
Clarke, D., Werestiuk, K., Schoffner, A., Gerard, J., et al (2012)

What do “we” all need to do?
34
So what does it all mean?

Know thy self
– What kind of clinician am I?
Do I take shortcuts
– Be mindful
Do I have it right?
What is the worst it could
be?
– Develop Internal Alarms
Know when you are drifting
– What is drift?
Gradually downgrade the
significance of risk until it is
accepted as normal part of
work
35
How to be safe
Picture here
Patient Safety

Know thy Colleagues
– Teamwork
Who is on your team?
Do your know their names?
– Formal leaders
Board
C-suite
– Informal leaders
– Patients
36
How to be safe
Patient Safety

TeamSTEPPS®
– Developed by Agency for Healthcare Research and Quality
– Incorporated by WHO in Patient Safety Curriculum
– Strategies & Tools to Enhance Performance and Patient Safety
Key Principles
– Team Structure
– Leadership
– Situation Monitoring
– Mutual Support
– Communication
37
Team Training It takes practice, practice, practice
www.ahrq.gov/health-care-information/topics/topic-teamstepps

Organize and lead team events
– Brief
– Huddle
– Debrief
Effective Leadership
– Flat hierarchy
– Share the plan
– Invite others into the conversation
– Explicitly ask people to share questions and concerns
38
TeamSTEPPS® Leadership
www.ahrq.gov/health-care-information/topics/topic-teamstepps

Continually scanning and assessing the environment to maintain
situational awareness
Ensure all team members are “on the same page” and “have each
others back”
Loss of Situational Awareness
– Trying to do something new under pressure
– Doesn’t feel right
– Boredom
– Being rushed being behind schedule
39
TeamSTEPPS® Situation Monitoring
www.ahrq.gov/health-care-information/topics/topic-teamstepps

Foster climate where it is expected that assistance will be actively
sought and offered
– Go from “I am not sure but this must be right” to “ I will assume this is not
right until I get proof otherwise”
Provide feedback to improve team performance – Timely, respectful, specific, directed towards improvement, considerate
Advocate for the patient when team member viewpoint do not agree
with decision maker
Assert a correction action
– Two- Challenge Rule
– “Stop the line”
– It’s okay to CUS
40
TeamSTEPPS®
Mutual Support
www.ahrq.gov/health-care-information/topics/topic-teamstepps

SBAR
– Situation
– Background
– Assessment
– Recommendation
Call Outs for critical information
– Informs all at same time in emergency
– Airway status? Airway clear
Closed- Loop Communication
Critical Language
Handoff
41
TeamSTEPPS® Communication
www.ahrq.gov/health-care-information/topics/topic-teamstepps

42
Final Thoughts

Questions, please!
43
Discussion

44
References
AIG (2013). Patient Safety; Hospital Risk – Perspectives of Hospital C-suite
and Risk Managers.
Ali, M., Osborne, A., Bethune, R., & Pullyblank, A. (2011). Preoperative
surgical briefings do not delay operating room start times and are popular with
surgical team members. Journal of Patient Safety, 7 (3): 139-43.
Berenholtz, B.M., Shumacher, K., Hayanga, A.J., Simon, M. Goeschel, C.,
Pronovost, P.J., Shanley, C.J., & Welsh, R.j. (2009). Implementing
standardized operating room briefings and debriefings at a large regional
medical center. Joint Commission Journal of Quality and Patient Safety, 35 (8):
391-7.
Cathchpole, K.R., De Leval, M.R.. McEwan, A., Pigott, N., Elliot, M.J.,
McQuillan, A., MacDonald, C., & Goldman, A.J. (2007). Patient handover from
surgery to intensive care: using Formula 1 pit-stop and aviation models to
improve safety and quality. Pediatric Anesthesia, 17: 470-478.

45
References
Einav, Y. Gopher, D. Kara, I. Ben-Yosef, O. Lawn, M., Laufer, N. Lievergall,
M. Donchin, Y. (2010). Preoperative Briefing in the operating room: shared
cognition, teamwork and patient safety. Chest. 137 (2): 443-9.
Lingard, l., Reghr, G. Cartmill, C. Orser, B. Espin, S., Bohen, J., Reznick, R.
Baker, R. Rotstein, L., & Doran, D. (2011). BMJ Quality and Safety, 20 (6): 475-
82.
Makary, MA, Sexton, JB, Freischlag, JA, Holzmulueller, et al (2006).
Operating Room Teamwork among Physicians and Nurses: Teamwork is in the
Eye of the Beholder. Journal of the American of Surgeons, 202 (5), 746-752.
Manser, T. (2009) Teamwork and patient safety in dynamic domains of
healthcare: a review of the literature. Acta Anaesthesiologica Scandinavica, 53,
143-151.

46
References
Mujumdar, S. & Santos, D. (2014). Teamwork and communication: An
effective approach to patient safety. World Hospitals and Health Services, 50
(1), 19-22.
Salas, E., Sims, D, Klein, C. & Burke, C.S. (2003). Can Teamwork enhance
safety?. Risk Management Foundation Forum, 5-9.
Salas, E., Simms, D.E., & Burke, C.S. (2005). Is there a “Big Five” in
teamwork? Small Group Research, 36, 555-99.
Weller, J., Boyd, M., & Cumin, D. (2014) Teams, tribes and patient safety:
overcoming barriers to effective teamwork in healthcare. Postgraduate
Medicine Journal,90,149-154

47
References – Websites
www.ahrq.gov/health-care-information/topics/topic-teamstepps
www.cec.health.nsw.gov.au/programs/between-the-flags
World Health Organization (2009). Human Factors in patient safety: review of
topic and tools. Report for methods and measures working group of WHO
patient safety. Retrieved from
www.who.int/patientsafety/research/methods_measures/human_factors/hum
an_factors_review.pdf
World Health Organization (2012). Being a team player. To Err is Human
Course, 1-5. Retrieved from
www.who.int/patientsafety/education/curriculum/course4_handout.pdf

American International Group, Inc. (AIG) is a leading international insurance organization serving customers in more than 100 countries and jurisdictions. AIG companies serve commercial, institutional,
and individual customers through one of the most extensive worldwide property-casualty networks of any insurer. In addition, AIG companies are leading providers of life insurance and retirement services
in the United States. AIG common stock is listed on the New York Stock Exchange and the Tokyo Stock Exchange.
Additional information about AIG can be found at www.aig.com | YouTube: www.youtube.com/aig | Twitter: @AIGInsurance | LinkedIn: http://www.linkedin.com/company/aig
AIG is the marketing name for the worldwide property-casualty, life and retirement, and general insurance operations of American International Group, Inc. For additional information, please visit our
website at www.aig.com. All products and services are written or provided by subsidiaries or affiliates of American International Group, Inc. Products or services may not be available in all countries, and
coverage is subject to actual policy language. Non-insurance products and services may be provided by independent third parties. Certain property-casualty coverages may be provided by a surplus lines
insurer. Surplus lines insurers do not generally participate in state guaranty funds, and insureds are therefore not protected by such funds.