Embed Size (px)
Citation preview

Air Pollution andPublic Health inNorth Carolina

Air Pollution and Public Healthin North Carolina
Travis MadsenElizabeth Ouzts
February 2006

The authors greatly appreciate the timely input and insightful review offered by Dr. J.C.Chen and Dr. David Richardson of the University of North Carolina School of PublicHealth, Department of Epidemiology; Dr. David Leith of the University of North Caro-lina Department of Environmental Sciences and Engineering; and Dr. David Bates, Pro-fessor Emeritus of Medicine, University of British Columbia. Tony Dutzik and ElizabethRidlington of the Frontier Group generously provided editorial and research assistance.
The financial support of the Z. Smith Reynolds Foundation and the Energy Foundationmade this project possible.
The views and opinions expressed here are those of the authors and do not necessarilyreflect the views of our funders or of individuals who provided review. The recommenda-tions are those of the Environment North Carolina Research & Policy Center. Any factualerrors are strictly the responsibility of the authors.
© Environment North Carolina Research & Policy Center
In 2006, Environment North Carolina Research & Policy Center became the new home ofNorth Carolina Public Interest Research Group (NCPIRG) Education Fund's environ-mental work.
Environment North Carolina Research & Policy Center is a 501(c)(3) organization. Weare dedicated to protecting North Carolina’s air, water and open spaces. We investigateproblems, craft solutions, educate the public and decision makers, and help North Carolin-ians make their voices heard in local, state and national debates over the quality of ourenvironment and our lives.
For more information about Environment North Carolina and Environment North Caro-lina Research & Policy Center, see our Web site at www.environmentnorthcarolina.org orcontact our offices at (919) 833-0015 or by email at [email protected].
Additional copies of this report can be obtained online at www.environmentnorthcarolina.orgor in print by sending $10 per copy to:
Environment North Carolina Research & Policy Center112 South Blount Street, Suite 102Raleigh, NC 27601
Acknowledgments

Table of Contents
Executive Summary 4
Introduction 8
Exposure to Air Pollution and How it Causes Harm 9Air Pollution in North Carolina 10Soot (Particulate Matter) 11Smog (Ground-Level Ozone) 13
Health Damage Caused by Air Pollutionin North Carolina 15Premature Death 16Hospital Stays and Emergency Room Visits 18New Cases of Chronic Disease—Asthma and Bronchitis 20Asthma Attacks 22Missed Work Days and Sick Days 22
Air Pollution and North Carolina’s Children 23Infant Death 24Asthma Attacks, Acute Bronchitis and Missed School Days 24
Clean Air Policy Recommendations 27Sources of Dirty Air 27Policies Aimed at the Largest Pollution Sources 27
Methodology 30Sources of Uncertainty 34
Notes 36

4 Air Pollution and Public Health in North Carolina
Executive Summary
A ir pollution in North Carolina makespeople sick and cuts lives short.Air pollution triggers heart attacks
and strokes. It causes diseases like chronicbronchitis, asthma and lung cancer. It sendspeople to the emergency room with respi-ratory problems, causes asthma attacks, andcontributes to respiratory illness in other-wise healthy people. At the root of all ofthese problems, air pollution irreparablydamages lung tissues in ways similar to sec-ond-hand tobacco smoke.
In this report, we estimate the healthimpact of air pollution above natural back-ground levels in North Carolina. The esti-mates cover particulate pollution (or soot),which comes from smokestacks and vehicleexhaust, and ground-level ozone (or smog),which develops across much of the state onhot summer days as a result of emissionsfrom cars, trucks, smokestacks and othersources. The estimates rely on a numberof information sources: 2003 air pollutionmonitoring data from the U.S. Environ-mental Protection Agency (EPA); statisticsabout the frequency of health problemsfrom the North Carolina State Center forHealth Statistics and the U.S. EPA; scien-tific studies linking air pollution and healthproblems; and methodology based on simi-lar work from the U.S. EPA and the World
Health Organization. Taken together, thesesources reveal that air pollution places a sig-nificant burden on the health of all NorthCarolinians.
Many North Carolina residents suf-fer health problems caused by pollutioneven at levels that meet air pollutionstandards.
• Despite the fact that air pollutionlevels in North Carolina meet healthstandards during much of the year,even “safe” levels of pollution cancause damage. Scientific experimentsshow no threshold below whichpollution does not have an effect.
Air pollution causes illness in other-wise healthy people.
• Air pollution causes in the range of ahalf-million missed work days eachyear, and millions of cases whereNorth Carolinians experiencesymptoms like shortness of breath orrunny nose.
Air pollution causes thousands ofpeople to be admitted to area hospitalsevery year and increases the burden ofchronic disease.

Executive Summary 5
• Air pollution leads to an estimated6,000 hospital admissions forrespiratory disease and 2,000 forcardiovascular disease annually.
• In addition, air pollution causesapproximately 1,500 new cases ofasthma and 2,500 new cases of chronicbronchitis in adults every year.
• Among asthmatics, soot pollutioncauses an estimated 200,000 asthmaattacks annually, with an additional200,000 caused by smog.
Every year, air pollution kills thousandsof people in North Carolina.
• Air pollution causes about 3,000premature deaths in North Carolinaannually, accounting for between 3 and7 percent of all deaths not caused byviolence or accidents.
• Compared to national statistics, airpollution ranks as the third highest riskfactor for premature death, behindsmoking and poor diet/physicalinactivity.
• Tables ES-1 and ES-2 provide asummary of the health impacts of airpollution in North Carolina, includingcentral estimates as well as upper andlower boundaries of statistical precision.
Children are especially vulnerable tothe effects of air pollution.
• Every year, air pollution causes dozensof infant deaths and hundreds ofthousands of school absences due toillness. (See Table ES-3.)
• Injuries caused by air pollution in earlyin life can have permanent consequences.
Aggressive action to reduce air pol-lution can improve public health andreduce the societal cost of pollution-caused illness.
In 1999, the two largest sources of NorthCarolina’s air pollution were coal-firedpower plants and automobiles. In 2002, the
state Legislature passed the Clean Smoke-stacks law, which will reduce power plantpollution in-state by more than 70 percentover the next seven years. Reducing pollu-tion from vehicles is the next priority steptoward healthy air at the state level. Becauseemissions from vehicles and industrial fa-cilities located upwind from North Caro-lina also contribute to the overall problem,action at the regional and federal level willalso be required.
State Level Actions:
• Strengthen limits on automobile airpollution in line with New York,Massachusetts, New Jersey, Connecti-cut, Rhode Island, Maine, Vermont,California, Oregon and Washington.
• Require retrofitting of diesel engineswith particulate filtration systems,including school bus fleets and con-struction equipment.
• Reduce car-dependent land usepractices and sprawl.
• Increase transportation funding fortransit, rail freight, and other alterna-tive transportation projects.
Federal and Regional Level Actions:
• Fully enforce the Clean SmokestacksAct, pursuing all available means toreduce pollution in neighboring states.
• Restore the New Source Reviewprovision of the federal Clean Air Actand require the oldest coal-fired powerplants and other industrial facilities inthe country to install modern emis-sions control technology.
• Limit nationwide industrial emissionsof sulfur dioxide, nitrogen oxides, andmercury to between 10 percent and 30percent of 2000 levels.
• Strengthen national emission standardsfor cars and trucks to match or exceedstandards adopted by California andother states.

6 Air Pollution and Public Health in North Carolina
Table ES-1: Annual Public Health Damage from Smog (Ground-Level Ozone)in North Carolina
Health Effect Estimated Cases Range
Adult Onset Asthma (Males, 25+) 1,500 900 –1,900Respiratory Hospital Admissions 4,000 3,000 – 5,000Asthma Attacks 200,000 100,000 – 300,000Restricted Activity Days 1 million 800,000 – 1.4 millionIncreased Symptom Days 4 million 2 million – 6 million
Table ES-2: Annual Public Health Impact of Soot (PM10) in North Carolina
Health Effect Estimated Cases Range
Premature Death (Adults) 3,000 2,000 – 4,600Respiratory Hospital Admissions 2,000 1,700 – 2,600Cardiovascular Hospital Admissions 2,000 900 – 2,500New Cases of Chronic Bronchitis 2,500 260 – 4,400Asthma Attacks 200,000 100,000 – 390,000Missed Work Days 500,000 440,000 – 520,000Restricted Activity Days 5 million 4.1 million – 5.5 millionIncreased Symptom Days 15 million 7 million – 23 million
Table ES-3: Annual Air Pollution Damage to Children’s Health in NorthCarolina
Health Effect Estimated Cases Range
Infant Deaths 50 30 – 60Asthma ER Visits 1,500 200 – 3,500Acute Bronchitis 20,000 13,000 – 33,000Asthma Attacks 100,000 90,000 – 120,000Missed School Days 300,000 NA

Executive Summary 7
How to Interpret Health Effect Estimates
The numbers reported here are an illustration of the likely health impacts of airpollution commonly found in North Carolina. The estimates are subject to sev-
eral sources of scientific uncertainty, which could make the actual numbers higheror lower. Where possible, we attempted to make conservative assumptions—mean-ing the scope and scale of the impacts of air pollution may be larger than reportedhere. Sources of uncertainty include:
• The report does not capture or quantify all the effects of air pollution—forexample, air pollution could affect development before birth, predisposingadults to disability or disease.
• The scientific studies that form the foundation of the estimates rely on statisti-cal models that are sensitive to input assumptions.
• Health systems do not track events like asthma attacks, making frequencyestimates necessary. These estimates may not reflect local conditions perfectly.
• Population exposures to air pollution are estimated based on readings at fixedmonitors. Errors in extrapolating exposure to the whole population, either inthis report or in published scientific literature, could affect the accuracy of ourestimates.
See the methodology section on page 30 for a more complete discussion.

8 Air Pollution and Public Health in North Carolina
Introduction
A ir pollution in North Carolina is a ser-ious and persistent problem.
The American Lung Association givesCharlotte, the Triad, the Triangle and theAsheville region an “F” for air quality—andthat’s just for smog pollution.1 Particulatepollution also poses major health risks forNorth Carolinians, especially children andthe elderly.
Air pollution shortens lives, sends peopleto the hospital and the emergency room,and triggers asthma attacks. These aremerely the most visible signs of the healththreat posed by polluted air. Air pollutionaffects every individual, reducing lung func-tion and increasing the risk of illness.
Nor are we safe on days when air pollu-tion levels are below those recognized bygovernment as meeting federal standards.Ozone smog and particulate soot can af-fect health even on days when an air pollu-tion alert is not in effect.
This is especially true for people wholive, work or play near busy roadways. TheWorld Health Organization and theAmerican Academy of Pediatrics recom-mend that communities take action to
reduce pollution—especially traffic-relatedpollution—to improve public health.2
It wasn’t supposed to be this way—notin 2006. When Congress adopted the fed-eral Clean Air Act in 1970, it establishedthe goal of setting and achieving air qual-ity standards protective of human health by1975. Nearly three decades later, NorthCarolina’s air still fails to meet establishedhealth standards—standards that may notbe fully protective of human health.
With the rollback of key air pollutionpolicies at the federal level—and with in-creased motor vehicle traffic, population,and overall energy use threatening to un-dermine the progress we have made towardcleaner air—North Carolina has reached acritical juncture. Solutions do exist. Frommodern emission controls for cars andpower plants to effective transit systems, wehave the technological know-how to sig-nificantly cut the amounts of air pollutionin North Carolina air.
By adopting public policies that put thesetechnologies to work, North Carolina canreduce air pollution and help millions ofits citizens to live longer and healthier lives.

Exposure to Air Pollution 9
Most people think of air pollutiononly on days when the news an-nounces an air quality alert, warn-
ing of high levels of smog. Unfortunately,people in North Carolina aren’t exposed toair pollution just a few dozen times a yearon bad air days. North Carolinians breatheair pollution day in and day out through-out their entire lives.
Much of the pollution comes from burn-ing fossil fuels for energy—in cars, trucks,power plants, industrial facilities, and en-gines. Many of these pollutants are invis-ible, and they are everywhere. They mixtogether in the atmosphere and react incomplicated ways to form a toxic soup.
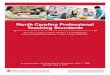
On bad air days, visibility plummets andthe air looks thick and hazy. (See Figure 1.)Sometimes the sun even looks red as it setsdue to pollutants in the air. These cloudsof haze contain hundreds of toxic chemicals.
Two of the most harmful air pollutantsare soot and smog. Soot, or particulate pol-lution, contaminates the air year-round.Power plants, engines and motor vehiclesemit soot directly into the air. Chemicalreactions between gaseous pollutants in theair can also create fine particles. Smog
plagues summer days when intense sunlighttransforms air pollutants and oxygen intotoxic gases such as ozone.
Exposure to Air Pollutionand How it Causes Harm
These two photos depict good and bad airquality days in North Carolina. Each photodepicts the same view from the WRAL toweroff US 70 southeast of Raleigh near Clayton.However, in the second photo, visibility isgreatly reduced by a cloud of smog containingground level ozone and particulates.
Figure 1: Clear and Polluted Days inRaleigh
Phot
o co
urte
sy o
f N.C
. Div
ision
of A
ir Q
ualit
y

10 Air Pollution and Public Health in North Carolina
Air Pollution inNorth CarolinaSmog and soot reach unhealthy levels regu-larly in North Carolina. Annual averagesoot concentrations in the state (measuredas particulate matter (PM) less than 2.5micrometers in diameter) range from about8 micrograms per cubic meter in the leastpolluted parts of the state to 16 microgramsper cubic meter in the most polluted areas.3
(See Figure 2.)During the summertime ozone season
from April through October, the averagedaily peak one-hour ozone levels reach
47-61 ppb across the state. (See Figure 3.)On hot summer days, ozone levels routinelyexceed EPA health standards in the centralpart of the state.
If there were no human-induced air pol-lution emitted in North America, PM10 lev-els would be between 5 and 10 microgramsper cubic meter, and afternoon smog levelsin the spring, summer and fall would be 15to 30 ppb.6 If pollution were not emittedfrom other countries in the world as well,natural background levels would be evenlower.7
Soot and smog cause damage when theycome in contact with lungs. Ozone quickly
Figure 3: Average Smog Levels in North Carolina, April to October 20035
Figure 2: Average Soot Levels in North Carolina, 2003 (PM2.5)4
High: 17
Low: 8
Microgramsper cubicmeter
High: 68
Low: 46
Parts perbillion

Exposure to Air Pollution 11
reacts with airway tissues and produces in-flammation similar to a sunburn on the in-side of the lungs. Particulates travel deepinto the lower passages of the lungs andbecome trapped there, delivering a payloadof toxic chemicals. Constant exposure tothese pollutants over time permanentlydamages lung tissues, decreases the abilityto breathe normally, and exacerbates oreven causes chronic disease.
Soot (Particulate Matter)Back in the early days of the industrialrevolution, thick black smoke pouredfrom factories and coal-fired furnaces. Dur-ing the 1952 “Great Fog,” one of the mostnotorious pollution events in history,
Strengthening National Air Quality Standards
The Environmental Protection Agency (EPA) sets national air quality standardsunder the authority of the federal Clean Air Act. Under the law, the EPA is
supposed to review the standards every five years and adjust them based on thelatest scientific knowledge of what will protect public health with an adequate mar-gin of safety.8
Because of industry resistance, the standards trail scientific understanding of howdangerous air pollution really is. For example, EPA tightened standards for bothsoot and smog in 1997, based on accumulating evidence that soot and smog weremore harmful than previously believed. However, the American Trucking Associa-tion led a coalition of industries in a lawsuit against the new standards. Ultimately,the Supreme Court rejected industry arguments and upheld the standards in 2001.9The process delayed implementation of the new standards for years.
Researchers have published more than 2,000 studies on particle pollution sincethe last standard-setting review in 1997, showing serious health risks at pollutionlevels well below current standards.10 In 2005, the independent Clean Air ScientificAdvisory Committee and staff scientists at the U.S. EPA both concluded that thestandards for particulate matter were not adequate and recommended strengthen-ing them.11
However, the Bush administration disregarded the advice of these experts. InDecember 2005, the administration proposed standards weaker than recommendedby its own scientists—ignoring their advice for the first time in history. As a result,the standards would leave millions of Americans exposed to particulate pollution atlevels that pose clear risks to health.
12,000 Londoners died from intense pol-lution exposure.12
Today, the thick, black smoke character-istic of uncontrolled pollution has been re-placed with the more subtle and insidiousdirty haze that can almost look natural be-cause of its frequent presence over the east-ern United States. However, this pollutionis anything but natural. It comes from fuelburning, and mostly consists of fine soot,or extremely small and practically invisibleparticles in the air.
Some types of soot are simply unburnedfuel particles. Other types of soot are cre-ated when pollutants react with each otherin the atmosphere. Particles can containhundreds of different chemicals from can-cer-causing agents like polycyclic aromatichydrocarbons to metals from arsenic tozinc.

12 Air Pollution and Public Health in North Carolina
Forty to 1,000 times smaller than thewidth of a human hair, these fine particlesresult from burning fossil fuels like coal,gasoline, and diesel. For example, burninga pound of jet fuel creates 100 quadrillionparticles.13 Gasoline and diesel engines withand without catalytic converters emit par-ticles with a size of 0.1 to 1 micrometers,with the smallest particles coming fromgasoline and medium-duty diesel engines.14
Fine particles can remain suspended inthe air for weeks. They can travel throughbuilding shells and conventional heatingand air conditioning filters. When inhaled,they are able to penetrate deep into the lungwhere they deliver their toxic payload. Incontrast, larger particles such as dust orpollen travel shorter distances and are moreeffectively trapped in the upper airway.
Fine particles penetrate to the deepestpart of the lung, where they are attackedand absorbed by immune cells. In an ex-periment in England, ultra fine carbon par-ticles showed up in the immune cells ofevery child tested—even in a three-monthold infant.15 The particles were of the samesize emitted by motor vehicles, and chil-dren who lived close to busy roads had upto three times more particles in their bod-ies.
Some of the particles remain trapped inthe lung, while others travel through theblood to the rest of the body.16 Scientistshave counted particulates in the lung tis-sue of cadavers. People from highly pol-luted Mexico City had two billion particlesin every gram of lung tissue, and peoplefrom less polluted Vancouver, Canada hadabout 280 million.17
The chemicals delivered into the bodyby inhaled particulates are very dangerous.Some of them cause cancer, some cause ir-ritation to lung tissues, and some causechanges in the function of the heart.18 As aresult, particulates cause and aggravate ahost of health problems, including lungcancer and cardiovascular disease.
Particulate pollution can cause irrevers-ible damage to children, interfering withthe growth and development of the lungs.
For example, researchers at the Universityof Southern California followed the healthof over 1,000 ten-year-olds until theyreached 18. Children who lived in areaswith higher levels of particulate pollutionwere less able to breathe with normal ca-pacity.19
Particulate pollution is also deadly, kill-ing upwards of 50,000 Americans everyyear. In fact, according to the largest studyof the effects of particulates on mortality,breathing the air in major U.S. cities isabout as dangerous as living or workingwith a smoker.20
Figure 4: Soot Particles
Very small soot particles found in dieselexhaust.22 The scale bar represents 10nanometers.

Exposure to Air Pollution 13
Smog (Ground-Level Ozone)Smog can plague summer days in NorthCarolina. Smog results when a mixture ofpollutants reacts under intense sunlight toform ozone.
In the past five years, ozone levels inNorth Carolina have exceeded federalhealth standards on as few as 5 days and asmany as 51, with an average of 25.23 How-ever, ozone chronically contaminates the airat lower, but still harmful, levels from Aprilthrough October.
A natural layer of ozone exists high inthe atmosphere, absorbing ultraviolet ra-diation from the sun. However, when pol-lutants create ozone near the ground, itbecomes a threat to public health.
Ozone is a powerful chemical gas some-times used to kill bacteria in drinking wa-ter. Bubbling it through contaminatedwater destroys any infectious organisms inthe water and makes it safe to drink. Notsurprisingly, the chemical has the same ef-fect on our lungs—when inhaled, it dam-ages lung tissue and causes short-termswelling. With long-term exposure at evenlow levels, it causes permanent and irrevo-cable damage.
Scientists have known for well over adecade that ozone at levels routinely en-countered in North Carolina causes red-dening and swelling and reduces theelasticity of lung tissues over time.24 Ozonemakes lung tissues more sensitive to aller-gens and less able to ward off infections.25
It scars airway tissues. Children exposed toozone develop lungs with less flexibility andcapacity than normal. During high smogdays, otherwise healthy people who exer-cise can’t breathe normally.26
New scientific evidence continues toshow dramatic evidence of the severe andlong-term impact ozone exposure has onrespiratory health:
• College freshmen who were raised inless polluted areas have lungs that
work better than their schoolmateswho grew up in polluted cities. Forexample, University of California-Berkeley freshmen who have livedin places with less ozone pollutioncan exhale more forcefully thanstudents from more polluted areas.27
Yale freshmen who have lived forfour or more years in a countywith high ozone levels can’t breatheas well as freshmen from cleanerareas.28
• Recent studies show that the lungs ofasthmatic infant rhesus monkeys sufferirreversible structural damage whenexposed to ozone.29 Ozone exposurereduces the number of branchesformed by nerves and airway passagesin the lung and forces lung muscles toreorganize, and long recovery periodsdo not improve the damage. Theimmune system and cellular responsesto ozone are like those seen withasthma. Dr. Charles Plopper of theUniversity of California-Davis, theauthor of the studies, commented,“from a public health standpoint, it’s apretty disquieting situation.”30
Researchers believe the same damagehappens to human infants whenexposed to air pollution.
• Striking results from the SouthernCalifornia Children’s Study indicatethat exposure to ozone can causeasthma in children.31 Children whoexercise frequently in smoggy areasare more than three times as likely todevelop asthma as those in cleanerparts of the country.
Taken together, these studies paint apicture of profound and irreversible respi-ratory damage beginning with an infant’sfirst breath of ozone-tainted air, leading toimpaired lung development and chronicrespiratory disease.

14 Air Pollution and Public Health in North Carolina
The Dangers of Pollution from Traffic
Cars and trucks directly emit dangerous pollutants near roadways, in additionto contributing to soot and smog in ambient air. Fuel combustion produces
pollutants like nitrogen oxides, small particles, benzene, formaldehyde, and 1,3-butadiene. In sufficient amounts, these pollutants irritate airways and lungs,cause asthma, worsen asthma symptoms, and cause leukemia and other types ofcancers.32
Exhaust from highways and major roads poses a serious health hazard foranyone who lives, works or goes to school in or near heavy traffic. Scientificstudies have shown that automobile exhaust causes serious illnesses and increasesthe risk of death.
Children directly exposed to traffic pollution develop respiratory problems.
• Researchers in Europe found that children who live or go to school close tobusy highways and roads are more likely to suffer from cough, wheezing,and runny nose. Significantly, these children are also more likely to sufferfrom asthma.33
• Researchers in southern California found that children living closer to ahighway are more likely to have asthma, more likely to wheeze and morelikely to use asthma medication.34
• The damage begins at birth: studies have found that infants exposed totraffic-related air pollution during their first year of life are more likely tosuffer from coughs, which could later translate into chronic respiratoryproblems.35
Air pollution from traffic causes damage that increases the risk of death.
• People living near highways or highly traveled roads face an increased riskof death from stroke, lung disease and heart disease.36
Many people assume that being inside a car offers some protection fromexhaust—but pollution levels in cars are higher than in the air outdoors,especially in congested traffic.
• On congested roadways, levels of dangerous pollutants inside vehicles canbe up to 10 times higher than in general city air.37
• U.S. EPA researchers studied a group of North Carolina highway patroltroopers who regularly work on the road. After breathing elevated levels ofparticulates while on duty, the troopers’ heart rhythms and blood chemistrychanged in ways associated with increased risk of heart attack.38
In order to improve public health, state leaders must implement policies toreduce pollution directly emitted from vehicles on busy roadways.

Health Damage Caused by Air Pollution 15
Health researchers have made signifi-cant progress in mapping out theconsequences of breathing polluted
air, and the results aren’t pretty. The mostserious impacts include premature deathfrom diseases like cancer and heart disease,respiratory deaths in infants, and new casesof persistent diseases like chronic bronchi-tis and asthma.
However, these impacts are just the mostvisible indicators of widespread health dam-age that affects everyone in the state. Airpollution also causes increased emergencyroom visits, more frequent asthma attacks,and missed work days due to respiratoryillness in otherwise healthy people. At theroot of all of these problems, air pollutionirreparably damages lung tissues in wayssimilar to second-hand tobacco smoke.
In this report, we quantify the healthimpacts of air pollution in North Carolina.Our estimates stem from three basic sourcesof information:
• The exposure of people to airpollutants,
• Scientific studies documenting howthe risk of a relevant health impactchanges with increasing air pollutionlevels, and
Health Damage Caused byAir Pollution in North Carolina
• The number of deaths, hospitaladmissions, and other relevant eventsin North Carolina in 2003.
Air pollution monitors placed through-out North Carolina by the Department ofEnvironment and Natural Resources helpprovide the first piece of information. A vastbody of scientific literature in which re-searchers tracked pollution and health ef-fects provides the second piece ofinformation. And the third comes fromhealth statistics maintained by the NorthCarolina State Center for Health Statisticsand the U.S. Agency for Healthcare Re-search and Quality, estimates by the U.S.Environmental Protection Agency, andadditional information from governmentsurveys.
Using this information, we estimate thatevery year in North Carolina, thousands dieprematurely because of soot in the air, thou-sands are admitted to area hospitals withair-pollution aggravated heart and lung dis-ease, and hundreds of thousands miss workbecause of air-pollution induced respiratoryillness (see Table 1).
Additionally, during the summer smogseason, we estimate that smog causeschronic asthma in thousands of North

16 Air Pollution and Public Health in North Carolina
Carolina adults, more than one hundredthousand asthma attacks and millions ofdays of increased respiratory symptoms likeshortness of breath (see Table 2).
Premature DeathThe most serious health impact of expo-sure to air pollution is premature death.Fine particulates are tied to deaths fromrespiratory disease, heart disease, lung can-cer, and other types of diseases commonlyassociated with smoking.
The EvidenceSeveral decade-long studies have made itquite clear that long-term exposure to pol-lution shortens lives:
Table 1: Public Health Damage from Soot in North Carolina (PM10)
Health Effect Estimated Cases Range
Premature Death (Adults) 3,000 2,000 – 4,600Respiratory Hospital Admissions 2,000 1,700 – 2,600Cardiovascular Hospital Admissions 2,000 900 – 2,500New Cases of Chronic Bronchitis 2,500 260 – 4,400Asthma Attacks 200,000 100,000 – 390,000Missed Work Days 500,000 440,000 – 520,000Restricted Activity Days 5 million 4.1 million – 5.5 millionIncreased Symptom Days 15 million 7 million – 23 million
Table 2: Public Health Damage from Smog in North Carolina (Ground-levelOzone0)
Health Effect Estimated Cases Range
Adult Onset Asthma (Males, 25+) 1,500 900 –1,900Respiratory Hospital Admissions 4,000 3,000 – 5,000Asthma Attacks 200,000 100,000 – 300,000Restricted Activity Days 1 million 800,000 – 1.4 millionIncreased Symptom Days 4 million 2 million – 6 million
• In 2002, Dr. C. Arden Pope atBrigham Young University and hiscolleagues published a study trackingmore than 500,000 people in 51metropolitan areas in America forlonger than 16 years. He found thatwhen fine particulate levels increasedby 10 micrograms per cubic meter,deaths from all causes rose by 4percent; deaths from cardiopulmonaryillness by 6 percent, and deaths fromlung cancer by 8 percent.40 Dr. Popesaw no evidence for a safe level ofparticulate pollution not tied toincreased death rates. Pope estimatedthat chronic exposure to air pollutionin the most polluted cities shortens lifeexpectancy between 1.8 and 3.1years.41 He concluded that breathingpolluted air like that commonly found

Health Damage Caused by Air Pollution 17
How We Estimated the Health Effects of Air Pollution
In the 1990 amendments to the Clean Air Act, Congress required the EPA toreport on the benefits and costs of Clean Air Act regulations. In November 1999,
the EPA released a report outlining the health and economic impact of clean airefforts. In addition, scientists with the World Health Organization produced a re-port in 2000 estimating the public health impact of particulate air pollution frommotor vehicles.39
Environment North Carolina Research & Policy Center adapted the methodol-ogy developed by these experts to estimate the health effects of air pollution inNorth Carolina.
First, we gathered statistics on how many deaths, hospital admissions and otherrelevant events happened in the state in 2003. Next, we estimated how much airpollution (above natural background levels) people are exposed to by looking atdata from soot and smog monitors placed throughout the state. Finally, we ob-tained estimates of how much the risk of health problems increases with exposureto a specific amount of air pollution. Combining these three pieces of informationallowed us to estimate what fraction of deaths and other relevant health problemscould be attributed to air pollution.
We report the effects of air pollution including a range of values to emphasizethat the estimates have an inherent level of uncertainty. Reported ranges representthe 95 percent confidence interval derived by scientists for the relationship be-tween air pollution and the frequency of health outcomes, or where the estimatewould be expected to lie 95 times out of 100 observations. The range of valuespresented here is our best estimate of the public health toll of air pollution in NorthCarolina. For more specific details on how the estimates were made and a discus-sion of factors that could make the actual impacts higher or lower, see the Method-ology section.
in the Eastern U.S. causes an increasedrisk of lung cancer similar to that ofbreathing secondhand smoke.42
• Researchers with the World HealthOrganization in Europe found that airpollution caused 6 percent of all deathsin Switzerland, France and Austria(40,000 per year). Motor vehiclepollution caused about half of thesedeaths.43
Dozens of studies also link short-termexposure to pollution to acute increases inthe death rate:
• In a study of heart attack patients inBoston, Dr. Annette Peters and hercolleagues at the Harvard UniversitySchool of Public Health found that aspollution levels rose, so did the fre-quency of heart attacks a few hours toa day later.44 An increase in fineparticles of 25 micrograms per cubicmeter resulted in a 69 percent increasein the relative risk of having a heartattack over the following day.
• Dr. Jonathan Samet from JohnsHopkins University’s BloombergSchool of Public Health and his

18 Air Pollution and Public Health in North Carolina
colleagues studied health and airpollution data from 90 cities in theU.S. and found a link between dailypollution levels and daily death ratesfrom chronic heart and lung disease.The link was strongest in the North-east, the industrial Midwest, and inSouthern California.45
• Dr. Kazuhiko Ito and his colleagues atNew York University found thatincreases in ozone levels lead to ahigher risk of death. As daily 1-hourmaximum ozone concentrations inseven U.S. cities rose by 10 parts perbillion, risk of death rose by 0.4percent.46
Pollution associated with burning fossilfuels is specifically tied to increased mor-tality, as opposed to particles from dust-storms and other natural events.47 Otherstudies show that these effects are notmerely accelerating the death of elderly andinfirm adults already on the brink of death,but also kill some infants and adults whootherwise would have many years of healthremaining.48
North Carolina EstimateWe estimate that soot pollution causesabout 3,000 deaths each year, or 3 to 7 per-cent of all deaths not caused by injuries oraccidents. This estimate is comparable tothe World Health Organization study of airpollution impacts, which reported that 6percent of all mortality in Switzerland,France and Austria is linked to air pollution.49
This finding ranks air pollution as thethird leading cause of mortality in NorthCarolina, behind smoking and poor diet/physical inactivity. In 2004, researcherspublished estimates for the leading causesof death in the U.S. as a whole.50 Ac-cording to these estimates, smoking causes18 percent of all deaths, poor diet andphysical inactivity causes 15.2 percent of alldeaths and alcohol consumption leads to3.5 percent of all deaths. Air pollution in
North Carolina—causing roughly 4.5percent of all deaths—ranks just above al-cohol consumption as a risk factor inpremature mortality.
Table 3: Yearly Premature DeathsCaused by Air Pollution in NorthCarolina
Health Estimated RangeEffect Cases
PrematureDeath 3,000 2,000 – 4,600(Adults)
Hospital Stays andEmergency Room VisitsAs levels of air pollution increase, so do thenumber of people admitted into hospitalwards or emergency departments sufferingfrom severe respiratory and cardiovasculardisease.
The Evidence
• Dr. Jonathan Samet from JohnsHopkins University’s BloombergSchool of Public Health and hiscolleagues found that increases in dailypollution levels were linked to in-creased hospital admissions for cardio-vascular disease, pneumonia, andchronic obstructive pulmonary disor-der.57
• Dr. Joel Schwartz of Harvard Univer-sity and his colleagues documentedlinks between ozone and hospitaliza-tion rates for cardiovascular andrespiratory disease in Birmingham,Detroit, Minneapolis-St. Paul, andTucson.58 An increase of soot levels by100 micrograms per cubic meter andozone by 50 parts per billion increasedthe risk of hospitalization for chronic

Health Damage Caused by Air Pollution 19
respiratory disease in the range of20 percent to 100 percent.
• Dr. George Thurston at the New YorkUniversity School of Medicine and Dr.Richard Burnett at EnvironmentCanada have repeatedly linked respira-tory and cardiovascular hospitaladmissions with the levels of summer-time haze air pollution.59 According tothese studies, summertime hazepollution was responsible for 24percent of respiratory hospital admis-sions in Toronto, and up to half ofadmissions on particularly bad air days.
• Dr. Paul Lioy and his colleagues at theRutgers Environmental and Occupa-tional Health Sciences Institute andUMDNJ—Robert Wood JohnsonMedical School saw increases in thenumber of asthma emergency roomvisits in central and northern NewJersey on high-smog summer days.60
Emergency room visits occurred 28percent more frequently when the
average ozone levels were greater than60 ppb than when they were lowerthan this level. This study demon-strates health effects of ozone exposureat levels well below the EPA healthstandard of 80 ppb over an 8 hourperiod.
• Dr. Joel Schwartz from HarvardUniversity and his colleagues at theU.S. EPA found that as fine soot levelsincreased in the Seattle area, so didemergency room visits for asthma.61
An increase in fine soot levels of 30micrograms per cubic meter increasedthe relative risk of needing emergencymedical attention for asthma by 12percent. The daily fine soot levelsnever exceeded 70 percent of the EPAhealth standard at the time.
• Dr. Jennifer Peel and her colleagues atEmory University looked at airpollution levels and emergency roomvisits at 31 hospitals in Atlanta from1993 to 2000—a statistically powerful
Global Warming and Public Health
Soot and smog are not the only pollutants in North Carolina’s air. Global warm-ing pollution also has serious consequences for the health and well being of all
North Carolinians.Scientists project that global warming could raise average temperatures in North
Carolina by 1° F to 5° F over the next century.51 Coupled with a projected increasein precipitation, the heat index in the Southeast could climb by 8 to 15° F.52 Amonga host of negative impacts—from coastal flooding to ecosystem disruption—such atemperature increase would increase air pollution and harm public health.53
Scientific evidence shows that as temperatures grow hotter in the summer, sodoes the risk of death. For example, scientists tracking hospitalization of patientsfor cardiovascular diseases in Denver in the summer months of 1993 to 1997 foundthat higher temperatures increased the number of elderly people suffering fromheart attacks and congestive heart failure.54 In the summer of 2005 a severe heatwave passed through France, killing an estimated 15,000 people.55
The U.S. Environmental Protection Agency estimates that an increase of 3° F inthe average summer temperature in a city like Greensboro would cause heat-re-lated deaths to increase by nearly 70 percent.56

20 Air Pollution and Public Health in North Carolina
sample comprised of more than 4million patients. She found thatincreased levels of soot and smogpollution led to increased emergencyroom visits for upper respiratoryinfections, pneumonia and otherrespiratory conditions.62
North Carolina EstimateWe estimate that soot pollution causes2,000 respiratory and 2,000 cardiovascularhospital admissions each year, and smogcauses 4,000 respiratory hospital admissionsduring the summer smog season. This rep-resents between 5 and 8 percent of respira-tory hospital admissions in 2003, andbetween 0.5 and 1.5 percent of cardiovas-cular hospital admissions.
New Cases of ChronicDisease—Asthma andBronchitisAir pollution can cause chronic diseases inaddition to triggering short-term healthdamage. From new cases of chronic asthmain otherwise healthy children and adults to
the development of chronic bronchitis inelderly people, these are severe diseases thatcause significant distress for hundreds ofthousands of North Carolina residents.
The Evidence
• Dr. Rob McConnell at the Universityof Southern California School ofMedicine and his colleagues found thatchildren who exercise a lot developasthma at higher rates in more pol-luted areas. The researchers followedfor five years more than 3,500 childrenfrom the fourth, seventh, and tenthgrades with no history of asthma.During that time, 265 became asth-matic. Children who played three ormore sports in communities with highsmog levels developed asthma at overthree times the rate of children in low-smog communities. Children whospent relatively high amounts of timeoutdoors were 1.4 times more likely toget asthma in polluted areas comparedto cleaner ones.63 The levels of airpollution in all of the communitiesexamined were well below the U.S.EPA health standard of 80 ppb over aneight hour period.
Table 4: Annual Hospital Admissions Caused by Air Pollution in North Carolina
Health Effect Estimated Cases Range
Respiratory Hospital Admissions (Soot) 2,000 1,700 – 2,600Cardiovascular Hospital Admissions (Soot) 2,000 900 – 2,500Respiratory Hospital Admissions (Ozone) 4,000 3,000 – 5,000
Table 5: New Cases of Chronic Respiratory Disease Caused by Air Pollution inNorth Carolina Annually
Health Effect Estimated Cases Range
New Cases of Chronic Bronchitis (Soot) 2,500 260 – 4,400Adult Onset Asthma (Males, 25+) 1,500 900 – 1,900

Health Damage Caused by Air Pollution 21
• In a follow up study, Dr. McConnelland his colleagues found that childrenliving closer to a major highway weremore likely to have asthma, pointing totraffic-related pollution as a likelycause of asthma.64
• Dr. William McDonnell at the U.S.EPA National Health and Environ-mental Effects Research Laboratoryand his colleagues found a connectionbetween long-term exposure to smogand development of asthma in adults.The researchers followed more than3,000 non-smoking adults for 15 yearsin California. During this period, justover 3 percent of the men and just over4 percent of the women reported adiagnosis of asthma. Several factorsincreased the risk of developingasthma, including: history of exposureto tobacco smoke, childhood pneumo-nia or bronchitis; and exposure toozone in men.65
• In Taiwan, researchers linked develop-ment of asthma with several individualair pollutants: fine soot, sulfur dioxide,nitrogen dioxide, and carbon monox-ide. The scientists surveyed more than160,000 schoolchildren and looked atlevels of air pollutants, finding that airpollution increased asthma prevalenceby as much as 29 percent, independentof exposure to second-hand tobaccosmoke.66 Similar research in HongKong showed that children living inareas with higher air pollution hadhigher levels of asthma and lesshealthy lungs.67
• Dr. Joel Schwartz and others identifiedlinks between particulate levels andphysician diagnoses of chronic bron-chitis by looking at health records andair pollution levels in 53 U.S. metro-politan areas.68 For every 10 micro-gram per cubic meter increase intotal particulates, the relative riskfor chronic bronchitis rose about7 percent.
Asthma prevalence is increasing in theU.S. and worldwide, for unknown reasons.In the U.S., the Centers for Disease Con-trol and Prevention (CDC) estimates thatprevalence among persons up to 17 yearsold increased about 5 percent per year from1980 to 1995.69 Deaths due to asthma havedoubled, and now amount to 5,000 peryear.70 The trend in the number of chil-dren with active asthma in North Carolinaalso has been increasing over the past fewdecades, to the point where just under onein 10 children are affected.71 According toa survey carried out by the CDC in 2003,7.1 percent of North Carolina adults havebeen diagnosed with asthma.72
North Carolina EstimateWe estimate that air pollution causes 2,500new cases of chronic bronchitis and 1,500cases of adult onset asthma among NorthCarolina residents every year.73 The con-tribution of air pollution may be muchhigher when pediatric asthma is considered.74
Asthma AttacksWhen pollution levels rise, so do the fre-quency of asthma attacks suffered by asth-matic children and adults.
The Evidence
• Dr. George Thurston and his col-leagues at the New York UniversitySchool of Medicine documentedincreased asthma attacks, respiratorydifficulty, and reduced lung function inchildren on high pollution days.75 Theresearchers tracked children attendingthe American Lung Association’sConnecticut “Asthma Camp” duringsummer months. On the highestpollution days, the risk of asthmaattacks requiring medication and chesttightness climbed 40 percent higherthan usual.

22 Air Pollution and Public Health in North Carolina
• In the mid 1970s, the EnvironmentalProtection Agency collected asthmaattack diaries from Los Angelesresidents. Asthma attacks werereported more frequently when smogand soot levels were high, as well aswhen the weather was cool.76
North Carolina EstimateWe estimate that soot pollution causes200,000 asthma attacks and smog pollutioncauses another 200,000 asthma attacks amongNorth Carolina asthmatics every year.
Missed Work Daysand Sick DaysAir pollution can also affect the health ofpeople with no chronic respiratory illness.On high pollution days, the number ofpeople feeling ill with symptoms like short-ness of breath, runny or stuffy noses,coughs, burning eyes, wheezing, and chestpain increases dramatically. These symp-toms can cause people to miss work orschool, or force them to limit their usualactivity levels.
The Evidence
• Dr. Bart Ostro at the California EPAlinked high air pollution levels withmissed work days and illness daysreported in the Health InterviewSurvey collected yearly by the U.S.Centers for Disease Control andPrevention.77
• Dr. Joel Schwartz of Harvard and hiscolleagues found that elementaryschool children in six U.S. cities sufferedfrom coughs and other lower respira-tory symptoms more often on dayswhen soot and smog levels were high.78
North Carolina EstimateWe estimate that soot pollution causes500,000 missed work days, 5 million per-son-days when illness limits normal activ-ity levels, and 15 million person-days withthe presence of respiratory symptoms suchas shortness of breath, runny or stuffy noses,coughs, burning eyes, wheezing, or chestpain. In addition, we estimate that smogcauses 1 million person-days when air pol-lution limits normal activity and 4 millionperson-days with respiratory symptoms.
Table 6: Annual Asthma Attacks Triggered by Air Pollution in North Carolina
Health Effect Estimated Cases Range
Asthma Attacks (Soot) 200,000 100,000 – 390,000Asthma Attacks (Ozone) 200,000 100,000 – 300,000
Table 7: Annual Missed Work Days and Increased Respiratory Symptom DaysCaused by Air Pollution in North Carolina
Health Effect Estimated Cases Range
Missed Work Days (Soot) 500,000 440,000 – 520,000Restricted Activity Days (Soot) 5 million 4.1 million – 5.5 millionIncreased Symptom Days (Soot) 15 million 7 million – 23 millionRestricted Activity Days (Smog) 1 million 800,000 – 1.4 millionIncreased Symptom Days (Smog) 4 million 2 million – 6 million

Air Pollution and North Carolina’s Children 23
Children are especially vulnerable tothe effects of air pollution.79 First,children are developing into adults.
Their lungs are growing. Injuries sustainedduring this time can cause permanent dam-age that will have life-long effects. Second,children breathe more air per pound ofbody weight and thus inhale larger dosesof pollutants than adults.
Children in North Carolina are con-stantly exposed to air pollution, breathingit day in and day out. Recent science hasshown that this exposure causes a range oflung injuries, even among otherwisehealthy infants and children. Children ex-posed to air pollution can’t breathe as wellas children growing up in cleaner areas.Their lungs are scarred and less flexiblethan they should be, their lungs hold less
air, and they aren’t as able to breathe nor-mally. These injuries manifest themselvesin respiratory illness, missed school days,increased doctor visits, hospitalizations, andfor a small group, death.80
Environment North Carolina Research& Policy Center compiled air pollutiondata, scientific reports about how air pol-lution levels affect children’s health, andbaseline health statistics maintained by thestate Center for Health Statistics and theEPA. We used this information to estimatethe health impacts of pollution on childrenin North Carolina. (For more details, seethe Methodology section.)
We estimate that air pollution kills sev-eral dozen infants a year and causes morethan one thousand emergency room visitsfor childhood asthma, tens of thousands of
Air Pollution andNorth Carolina’s Children
Table 8: Air Pollution Damage to Children’s Health in North Carolina
Health Effect Estimated Cases Range
Infant Deaths 50 30 – 60Asthma ER Visits 1,500 200 – 3,500Acute Bronchitis 20,000 13,000 – 33,000Asthma Attacks 100,000 90,000 – 120,000Missed School Days 300,000 NA

24 Air Pollution and Public Health in North Carolina
cases of acute bronchitis, close to one hun-dred thousand asthma attacks and hundredsof thousands of missed school days. (SeeTable 8.)
Infant DeathAir pollution not only kills elderly and sickpeople. It also causes premature death ininfants and young children. Experimentshave tied particulate levels to deaths fromboth respiratory disease and sudden infantdeath syndrome.
The Evidence
• Dr. Tracey Woodruff at the U.S. EPAand her colleagues linked fine sootpollution levels and neonatal deaths in86 U.S. metropolitan areas.81 Normal-weight infants less than one year oldborn in high soot areas were 40percent more likely to die of respira-tory disease, and 26 percent morelikely to die from sudden infant deathsyndrome than infants born in lowsoot areas.
• Researchers in the Czech Republicfound that newborn deaths due torespiratory causes were linked toincreased levels of fine soot, sulfurdioxide, and oxides of nitrogen.82 Thestudy concluded, “the effects of airpollution on infant mortality arespecific for respiratory causes in [theperiod between one month and oneyear of age], are independent ofsocioeconomic factors, and are notmediated by birth weight or gesta-tional age.”
• The National Bureau of EconomicResearch found that as levels ofparticles fell during a recession in theearly 1980s, so did rates of death innewborn children younger than 28days old. Specifically in Pennsylvania,researchers found that when total fineparticulate levels dropped 25 percent,newborn death rates from cardiopul-monary and respiratory causes fell 14percent.83
North Carolina EstimateWe estimate that soot pollution causes 50infant deaths in North Carolina each year,or 4 to 7 percent of all infant deaths.
Hospitalization andEmergency Room TripsAs air pollution levels rise, children endup in the emergency room with respira-tory problems at higher rates. Some ofthem require hospitalization for longer-termcare.
The Evidence
• Dr. Michael Friedman of the U.S.Centers for Disease Control andPrevention and his colleagues foundthat reduced traffic levels and higherpublic transit use during the 1996Summer Olympics in Atlanta signifi-cantly reduced smog levels and alsoemergency room visits for childhoodasthma.84 One-hour peak ozone levelsdecreased by 27 percent, while thenumber of children visiting the
Table 9: Yearly Infant Deaths from Air Pollution in North Carolina
Health Effect Estimated Cases Range
Infant Deaths 50 30 – 60

Air Pollution and North Carolina’s Children 25
emergency room for asthma fell 41.6percent in a Medicaid database, 44.1percent in an HMO database, and11.1 percent in two major pediatricemergency departments. In otherwords, every 10 ppb decrease in smoglevels reduced the relative risk ofchildren needing emergency medical
Reducing Air Pollution Protects Children’s Health:The Case of the 1996 Olympics in Atlanta
The 1996 Summer Olympic Games in Atlanta offered researchers a unique oppor-tunity to observe the connection between lowered pollution levels and improved
health.85
Atlanta implemented a comprehensive transit plan as a part of the Olympic Games.The plan was designed to reduce congestion in the downtown area and reduce traveldelays. Atlanta launched an expanded 24-hour-a-day public transportation network,added 1,000 buses for park-and-ride service, encouraged local employers to institutealternative work hours and telecommuting, and closed the downtown area to privatevehicles.
The transit plan produced impressive results, despite the million or so additionalvisitors to the city. Weekday morning traffic trips declined by 22.7 percent and pub-lic transportation ridership increased by 217 percent.
The plan produced some unintended benefits for air quality and health that wereequally impressive. The average daily maximum ozone levels decreased by 28 per-cent, from 81 ppb before and after the Olympics to 59 ppb during the Olympics.Presumably, this effect resulted from the decreased levels of traffic-related air pollu-tion building up in the morning rush hour. Nearby cities did not experience similarreductions in ozone pollution.
At the same time, asthma-related emergency room visits for children decreasedby 41.6 percent in a Medicaid database, 44.1 percent in an HMO database, and 11.1percent in two major pediatric emergency departments. Additionally, hospitaliza-tions for asthma decreased by 19.1 percent. Unfortunately, Atlanta discontinued thetransit program at the conclusion of the Olympics, and pollution levels and emer-gency room visit rates returned to normal.
This experience powerfully demonstrates how reducing pollution levels wouldbenefit the health of children. It also highlights the role that motor vehicles play increating high levels of urban pollution and how better public transit can quicklyreduce air pollution levels.
Dr. Michael Friedman of the U.S. Centers for Disease Control and Prevention,one of the authors of the study, said that the results “provide evidence that decreas-ing automobile use can reduce the burden of asthma in our cities and that citywideefforts to reduce rush-hour automobile traffic through the use of public transporta-tion and altered work schedules is possible in America.”86
attention for asthma by roughly8 percent.
North Carolina EstimateWe estimate that air pollution causes 1,500asthma emergency room visits amongNorth Carolina children each year.

26 Air Pollution and Public Health in North Carolina
Asthma Attacks,Acute Bronchitis andMissed School DaysAir pollution triggers asthma attacks andincreases cases of acute bronchitis in chil-dren. Asthma is the leading chronic illnessin children and the number one cause ofmissed school days in the United States.87
The Centers for Disease Control and Pre-vention estimates that asthma prevalenceamong persons up to 17 years old in-creased about 5 percent per year from 1980to 1995.88 Air pollution worsens the impactof this disease, causes other acute respira-tory illnesses, and increases school absencerates.
The Evidence
• Dr. Janneane Gent at the Yale Univer-sity School of Medicine and hercolleagues recently published a studyshowing that children with asthma arevulnerable to air pollution well belowEPA health standards.89 According tothe study, every 50 ppb ozone increaseyields a 35 percent increased likelihoodof wheezing, and a 47 percent in-creased likelihood of chest tightness. Afollow-up study showed that infants,particularly those with asthmaticmothers, suffer from increased
Table 10: Yearly Pediatric Respiratory ER Visits Caused by Air Pollution inNorth Carolina
Health Effect Estimated Cases Range
Asthma ER Visits 1,500 200 – 3,500
wheezing and difficulty breathing ondays with high ozone levels.90
• Dr. Douglas Dockery at HarvardUniversity and his colleagues showedthat children living in areas with highlevels of acidic particle pollution were66 percent more likely to have had anepisode of bronchitis in the last yearthan children in low pollution areas.91
• Researchers participating in theSouthern California Children’s HealthStudy found that increased smogpollution causes more children to stayhome from school.92 When ozonelevels rose by 20 ppb, illness-relatedabsence rates went up by 63 percent,and by 174 percent for lower respira-tory illnesses with wet cough.
• Researchers in Korea found the samerelationship between air pollution andschool absences.93 When air pollutionlevels rose, so did illness-relatedabsences. When pollution levels fell,more children came in to school.
North Carolina EstimateWe estimate that air pollution causes 20,000cases of acute bronchitis and 100,000asthma attacks among North Carolina chil-dren each year. Additionally, air pollutioncauses in the range of 300,000 missedschool days each year.
Table 11: Asthma Attacks and Acute Bronchitis Caused by Air Pollution in N.C
Health Effect Estimated Cases RangeAcute Bronchitis 20,000 13,000 – 33,000Asthma Attacks 100,000 90,000 – 120,000Missed School Days 300,000 NA

Clean Air Policy Recommendations 27
Clean Air Policy Recommendations
Solutions to North Carolina’s air qual-ity problems are readily available.Strategies already in widespread use—
from modern emission controls for cars andpower plants to efficient transit systems—can cut air pollution and help people to livehealthy lives.
Aggressive action will be required onboth the state and regional level to reduceair pollution and reduce the costs societypays for the use of polluting fuels. In orderto have the greatest impact, action shouldfocus first on the largest sources of pollution.
Sources of Dirty AirIn North Carolina, mobile sources like cars,trucks, buses, and off-road equipment arethe largest source of air pollution—espe-cially in urban areas. Additional pollutantscome from power plants, industrial facili-ties, and chemical use. Pollution sources inneighboring states are also a significant partof the problem.
Within the state in 1999, almost half ofsmog-forming emissions (oxides of nitro-gen and volatile organic compounds) camefrom on-road and off-road mobile sources
like cars, trucks, and construction equip-ment. (See Table 12.) Mobile sources di-rectly released just under half of allparticulate matter under 10 micrometers indiameter. Traffic is an area of particularimportance, since pollutants are emitted atground level and in close proximity to ar-eas where people live.
In 1999, electricity generation was re-sponsible for 80 percent of the state’s re-leases of sulfur dioxide—one of theprecursors of soot particles. In 2002, NorthCarolina passed the Clean SmokestacksAct, a law that will significantly reduceemissions from coal-fired power plantswithin the state over the next decade. Ni-trogen oxide emissions from power plantswill drop 77 percent by 2009 and sulfur diox-ide emissions will drop 73 percent by 2013.94
With the passage of this law, mobilesources are now the highest priority forreducing pollution in North Carolina.
Policies Aimed at theLargest Pollution SourcesAn effective suite of policies aimed at

28 Air Pollution and Public Health in North Carolina
reducing air pollution in North Carolinawould include the following:
State Level Actions:
• Strengthen auto emission standards in linewith New York, Massachusetts, NewJersey, Connecticut, Rhode Island, Maine,Vermont, California, Oregon and Wash-ington. In these states, auto-makers arerequired to manufacture and sellvehicles that emit less pollution andincorporate advanced technologies.
• Require diesel engines to be retrofitted withparticulate filtration systems and low-sulfur fuel. Diesel engines are a signifi-cant source of fine particles. Newfederal diesel standards will be phasedin starting in 2007, reducing emissionsfrom new highway and off-roadvehicles. North Carolina can reduceemissions from older vehicles byretrofitting their emission controlsystems for lower pollution. State-owned vehicle fleets such as schoolbuses and road construction equip-ment should be included, as well asoff-road diesel vehicles like bulldozers.
• Reduce car-dependent land use practicesand sprawl. North Carolina shouldensure that future growth, develop-ment, and redevelopment focuses oncreating livable, transit-orientedcommunities to reverse the trend ofyearly increases in vehicle milestraveled that lead to greater pollution.
North Carolina should also increasethe proportion of transportationfunding for clean public transit toprovide residents with alternatives todriving.
Federal and Regional Level Actions:
• Fully enforce the Clean Smokestacks Act,pursuing all available means to reducepollution in neighboring states. TheClean Smokestacks Act instructs theNorth Carolina attorney general to useall legal means to force pollutionsources in neighboring states to cleanup. The state should continue to pushfor strong pollution controls onTennessee Valley Authority powerplants in upwind states.
• Advocate adoption of these state policiesamong neighboring and upwind states.Reducing air pollution emissions inNorth Carolina will have benefits forneighboring states. North Carolinashould encourage other states, espe-cially those upwind from the state, toadopt similar air pollution controlpolicies. Ultimately, regional coopera-tion will be required to reduce overallair pollution levels.
• Restore the New Source Review provisionof the Clean Air Act and require the oldestcoal-fired power plants and other indus-trial facilities in the country to installmodern emissions control technology. TheEPA recently enacted regulations
Table 12. Emissions of Selected Air Pollutants in 1999 by Source95
Total Mobile Area Point(Tons) Sources Sources Sources
Oxides of Nitrogen 674,848 55% 5% 40%Volatile Organic Compounds 635,687 39% 50% 11%PM10 390,632 44% 49% 7%Sulfur Dioxide 607,743 5% 5% 90%

Clean Air Policy Recommendations 29
relieving power plants and industrialfacilities grandfathered under theoriginal Clean Air Act of responsibilityto upgrade their emissions controlswhen upgrading their facilities. Thischange limits the effectiveness of theClean Air Act and effectively subsi-dizes a few industries at the expense ofpublic health. It should be reversed assoon as possible.
• Limit nationwide industrial emissions ofsulfur dioxide, nitrogen oxides, andmercury to between 10 percent and 30percent of 2000 levels. Placing a nationalcap on point-source emissions of airpollutants could dramatically reduce
the levels of pollution plaguing theeastern seaboard of the U.S., andcontribute to a regional solution to theair pollution problem.
• Strengthen national emission standards forcars, trucks, and off-road vehicles. TheEPA sets national emission standardsfor cars, trucks, and off-road vehicles.However, California has designed amore effective and ambitious mobile-source emissions control program thatincludes requirement for manufactur-ers to produce cleaner vehicles withmodern technologies. The EPA shouldupdate its standards to match orexceed the California program.

30 Air Pollution and Public Health in North Carolina
To quantify the health impacts of air pol-lution, we relied on three basic piecesof information:
• The exposure of people to airpollutants,
• How the risk of a given health impactchanges with increasing air pollutionlevels, and
• The number of deaths, hospitaladmissions, and other relevant eventsin North Carolina in 2003.
Air pollution monitors placed through-out the state by the North Carolina De-partment of Environment and NaturalResources helped provide the first piece ofinformation. A vast body of scientific lit-erature in which researchers tracked pol-lution and health effects provided thesecond piece of information. And the thirdcame primarily from health statistics main-tained by the state Department of Healthand Senior Services, plus additional infor-mation from estimates and surveys by gov-ernmental agencies and in the scientificliterature.
We compiled this information to esti-mate the health impacts of pollution in
North Carolina, adapting methodologyused by the U.S. EPA in a study on the ben-efits and costs of the Clean Air Act and theWorld Health Organization in a study onthe health impact of vehicle pollution inEurope.96 The sections below outline thesources of this information and how weused it to derive our results.
Air Pollution ExposureWe obtained annual mean levels of pollu-tion from the U.S. EPA AIRData onlinedatabase of air pollution monitoring datafor the year 2003.97 We obtained the aver-age daily one-hour peak ozone levels re-ported during the summer smog seasonfrom April through October and annualmean particulate levels for particulates lessthan 2.5 micrometers in diameter (PM2.5).
We translated PM2.5 data into PM10 data,because many of the scientific studies link-ing air pollution and health effects werecarried out in terms of PM10, and the rela-tive risk figures obtained from the WorldHealth Organization were listed in termsof PM10.
98 Because PM2.5 is a subset ofPM10, their concentrations are related. Inaccordance with assumptions made by theWorld Health Organization, we assumed
Methodology

Methodology 31
that PM2.5 levels were 60 percent of PM10levels.99
We interpolated air pollution data froma nine-state region (including South Caro-lina, Georgia, Tennessee, Kentucky, WestVirginia, Virginia, Maryland, Delaware andNorth Carolina) to estimate annual meanpollution levels across North Carolina.(ArcView 9.1 Spatial Analyst software,spline interpolation, 75 to 100 monitorpoints used in each iteration, 0.5 weight-ing factor, regularized output.) The resultsof this interpolation are graphically shownin Figures 2 and 3 on page 10.
Using the zonal statistics function ofArcView 9.1 software, we mapped air pol-lution levels to the census tract level inNorth Carolina. Coupled with populationfigures from the 2000 census, we derivedpopulation-weighted annual average expo-sure estimates for residents of each countyin the state. We used 2003 exposure levelsas representative of current conditions, anddo not take into account pollution levelsfrom earlier years or forecasts of pollutionlevels in the future.
We define the impact of air pollution asthe change in the number of various healthoutcomes if air pollution exposure werereduced to natural background levels in theabsence of anthropogenic emissions fromNorth America, but with continuing emis-sions from the rest of the world. For ozone,we used a background level of 20 ppb, inaccordance with modeling from Harvardshowing the natural background between15 and 30 ppb, with lower levels during theseason when overall ozone levels are high-est.100 For particulate matter (PM10), weestimated a background level of 7.5 micro-grams per cubic meter, in accordance withthe World Health Organization.101
Baseline Frequency of HealthProblems in North CarolinaWe obtained the baseline frequency ofhealth outcomes in North Carolina in 2003from statistics maintained by the NorthCarolina State Center for Health Statistics
and the U.S. Agency for Healthcare Re-search and Quality, or, when more specificinformation was unavailable, published es-timates for the American population as awhole from the U.S. EPA. Table 13 liststhe relevant health outcomes and datasources.
Where specific data was not available,we assumed that 50 percent of all healtheffects that could be affected by ground-level ozone happened during the Aprilthrough October ozone monitoring season,and only considered the effects of ozoneon that period of time.
We obtained North Carolina countypopulation figures by age group from theNorth Carolina State Demographics de-partment to translate the relevant rates inTable 13 to baseline population frequen-cies for the state.102
The Relationship BetweenExposure and Frequency ofHealth EffectsA vast body of scientific literature in whichresearchers tracked pollution and healtheffects provides information about how thefrequency of health effects changes withchanging exposure to air pollution. Thesestudies are known as epidemiological stud-ies. Most epidemiological studies report theexposure-response relationship for air pol-lution exposure as a relative risk (RR). Ifthe relative risk equals 1, then the pollut-ant in question does not influence thehealth outcome. If the relative risk exceedsone, then the pollutant and the health out-come are linked. Most studies report a con-siderable range in which the relative riskactually lies, because of sources of statisti-cal uncertainty. This range is called the 95percent confidence interval. We use theupper and lower bounds of these intervalsto derive the ranges for each health effectwe report.
Following assumptions made by theWorld Health Organization in calculatingthe impact of traffic-related air pollution:117

32 Air Pollution and Public Health in North Carolina
Table 13: Baseline Frequencies of Health Problems in North Carolina
Health Outcome Baseline Frequency inNorth Carolina
Mortality (Deaths per person per year),excluding violence or accidental deaths.103
Infant mortality104
Respiratory hospital admissions(ICD 390-459)105
Cardiovascular hospital admissions(ICD 460-519)106
Annual chronic bronchitis incidence per person107 0.0038
Annual chronic asthma incidence among adults27 years of age and older in ozone season.108 0.0011
Asthma prevalence among adults in NC109 7.1 percent (Range of 6.3-7.9)
Asthma attacks per asthmatic per year110 9.86
Asthma ER visits per year among allchildren 0-15 years of age111 0.01
Asthma ER visits per year among adults.112 0.0071
Number of children per year who getacute bronchitis113 4.4 percent
Yearly missed work days per worker(adults between the ages of 18 and 65)114 2.4
School absences per student per year due to illness115 6
Restricted activity days per person per year116 6.46
2003 data obtained by county of residenceand by age group from the NC State Centerfor Health Statistics.
Data obtained by county of residence fromthe North Carolina State Inpatient Database.
Data obtained by county of residence fromthe North Carolina State Inpatient Database.
• Our impact assessment includes bothshort-term and long-term impacts ofair pollution.
• Estimates for deaths and incidence ofasthma and chronic bronchitis arebased on the long-term effect of airpollution. (For example, for mortalitywe used studies that tracked largegroups of people over many years(cohort studies), comparing mortalitywith air pollution exposure. These
studies indirectly capture the effects ofchronic problems like cancer and heartdisease that would not be completelyrevealed by short-term or time-seriesstudies.)
• For hospital admissions, asthmaattacks, acute bronchitis, restrictedactivity days and respiratory symptomdays, we applied short-term effectestimates from studies that looked atdaily variations of air pollution and
2003 data obtained by county of residenceand by age group from the NC State Centerfor Health Statistics.

Methodology 33
changes in the frequency of therelevant health outcome.
• We used annual average mean levels ofair pollution to estimate exposurelevels for both short- and long-termeffects. In other words, we assume thatthe annual impact of the pollutantcorresponds to the sum of all the dailyeffects across one year.
Calculating the impact of air pollutionon a given health outcome generally fol-lows Equation 1.
All of the estimates for particulate mat-ter relevant to children and adults followedthis pattern, as described by the WorldHealth Organization.119
The remaining estimates related toozone relied on concentration-responsefunctions developed by the U.S. EPA forits study on the benefits and costs of theClean Air Act, as listed in table 14.120 Inthe table, yo represents the frequency of thehealth effect, EXP is the exponentialfunction with base e, ∆O3 represents theexposure of the relevant population to
ozone pollution above natural backgroundlevels during ozone season, β represents thecoefficient derived by EPA from epidemio-logical literature as listed in Table 16, andPop is the relevant population.
ParticulatesTable 15 lists the relative risk numbers foran increase in particulate matter pollutionof one microgram per cubic meter derivedfrom epidemiology experiments, the 95percent confidence interval, and the cita-tion for the original experiment.
OzoneTable 16 lists the relative risk for an increasein ground-level ozone pollution of 1 partper billion, derived from epidemiologystudies. It also lists confidence limits andthe citation for the original study.
For studies that used ozone measure-ments other than the daily one hour peakconcentration, we converted North Caro-lina exposure data to the appropriate
Air Pollution Attributable Portion = [yo / ( 1+ ((RR – 1) x ∆P)) ] x Pop x RR x ∆PWhere:y
o= Frequency of health effect;
RR = Relative Risk associated with increased exposure of 1 [unit];Pop = Relevant Population; and∆P = Exposure of relevant population to pollution above natural background levels.
Equation 1:118
Table 14: Concentration-Response Functions for Ozone Exposure121
Health Effect Concentration—Response Function
Adult Onset Asthma -[(yo/((1- yo)(EXP(∆O3*β)) + yo))- yo] * PopRespiratory Hospital Admissions -[ yo * (EXP(-∆O3*β) - 1)] * PopAsthma Attacks -[(yo/((1- yo)(EXP(∆O3*β)) + yo))- yo] * PopRestricted Activity Days -[ yo * (EXP(-∆O3*β) - 1)] * PopIncreased Symptom Days β * ∆ O3 * Pop

34 Air Pollution and Public Health in North Carolina
measure using the following estimated con-version factors: 12-hour ozone levels are 50percent of the daily one-hour maximum,8-hour ozone levels are 70 percent of thedaily one-hour maximum, and 5-hourozone levels are 85 percent of the daily one-hour maximum.
Children, PM10
Table 17 lists the relative risk numbers forchildren associated with an increase in par-ticulate matter pollution of 1 microgramper cubic meter or ozone of 1 part per bil-lion. The table also lists confidence limitsand the citation for the original study.
Sources of UncertaintyAs discussed in this report, scientific evi-dence clearly shows that air pollution causessignificant damage to the health of thepublic across the state and the country.However, the extent and scale of the dam-age are subject to remaining scientific un-certainties and gaps in knowledge. Possiblesources of uncertainty include, but are notlimited to:
• This report does not capture all thepossible effects of air pollution. Forexample, air pollution could haveeffects on development in the womb orearly in life that predispose adults todisease later in life. Further study
Table 15: Relative Risk Figures Derived from the Scientific Literature, PM10
Relative Lower UpperRisk of Confidence Confidence
Health Effect Population Effect Limit Limit Reference
Premature Death Age 30 + 1.0043 1.0026 1.0061 122Respiratory Hospital Admissions All Ages 1.0017 1.0013 1.0020 123Cardiovascular Hospital Admissions All Ages 1.0008 1.0004 1.0011 124Asthma Attacks Asthmatics 1.0039 1.0019 1.0059 125Chronic Bronchitis Age 25 + 1.0098 1.0009 1.0194 126Work Loss Days Age 18-65 1.0046 1.0042 1.0050 127Restricted Activity Days Age 20 + 1.0094 1.0079 1.0109 128Increased Symptom Days Age 18 + 1.17 1.08 1.26 129
Table 16: Relative Risk Figures and Coefficients Derived from the Scientific Literature, Ozone
Effect Lower UpperCoefficient Confidence Confidence
Health Effect Population (β) Limit Limit Reference
Adult Onset Asthma Males, Age 25+ 1.0277 1.0142 1.0412 130Respiratory Hospital Admissions All Ages 1.0025 1.0018 1.0032 131Asthma Attacks Asthmatics 1.0018 1.0011 1.0026 132Restricted Activity Days Age 18 + 1.0022 1.0015 1.0029 133Increased Symptom Days Age 18 + 1.00014 1.000067 1.00021 134

Methodology 35
could reveal that the impacts of airpollution on human health are moreextensive than portrayed here. Addi-tionally, chronic exposure to airpollution has effects, such as reducedlung capacity, that are not quantified inthis report.
• The nature of the statistical modelsused in scientific studies (specificallytime-series studies) could lead to asmall level of upward overestimationfor the short-term effect estimates, asdescribed by the Health EffectsInstitute.140 However, the degree towhich this bias may affect the studieswe relied upon for our estimates isunknown.
• Estimates of the overall frequency ofevents like asthma attacks are often notavailable at the state or county level.Estimates for the U.S. population as awhole, while the best informationavailable, may not fully reflect localconditions.
• We extrapolate population-wide
pollution exposures based on data froma network of pollution monitorsaround the state. This approach doesnot capture the full detail of individualexposures. The detail of exposuremeasurements and geographic differ-ences within and among the scientificstudies we rely on also affects theaccuracy of our estimates. Weattempted to make our exposureestimates and the exposure estimateswithin key scientific studies asconsistent as possible.
• There may be some degree of overlapbetween the effects of particulatematter and ground level ozone. Inother words, the estimates for theeffects of each of these pollutants maynot be 100 percent additive. However,while particulate matter levels arehighly correlated with other airpollutants like nitrogen oxides andsulfur dioxide, they are not as corre-lated with ozone levels. Thus weconsider the two pollutants separatelywithin the report.
Table 17: Relative Risk Figures and Coefficients Derived from the Scientific Literature, Children
Relative Lower UpperRisk of Confidence Confidence
Health Effect Population Effect Limit Limit Reference
Infant Death (PM) 0 – 1 Years 1.0039 1.0027 1.0051 135Asthma ER Visits (Ozone) 0 – 15 Years 1.0080 1.0010 1.0186 136Acute Bronchitis (PM) 0 – 15 Years 1.0306 1.0135 1.0502 137Asthma Attacks (PM) Asthmatics
0 – 15 Years 1.0051 1.0047 1.0056 138Missed School Days (PM) 5 – 18 Years 0.0040 NA NA 139

36 Air Pollution and Public Health in North Carolina
1. American Lung Association, State of the Air2005, North Carolina statistics available atlungaction.org, 28 April 2005.2. World Health Organization Europe, SpecialProgramme on Health and Environment, Effectsof Air Pollution on Children’s Health and Develop-ment: A Review of the Evidence, 2005; AmericanAcademy of Pediatrics, Committee on Environ-mental Health, “Policy Statement; Ambient AirPollution: Health Hazards to Children,”Pediatrics 114, 1699-1704, December 2004.3. Soot is measured in terms of two different sizefractions: particulate matter less than 10micrometers in diameter, or PM10, and particu-late matter less than 2.5 micrometers indiameter, or PM2.5. The federal standard forannual average PM2.5 levels and PM10 levels is 15micrograms per cubic meter and 50 microgramsper cubic meter, respectively. Annual averagePM10 levels in North Carolina range from 14 to25 micrograms per cubic meter. Data compiledfrom U.S. EPA, AirData: Access to Air PollutionData, 2003 monitoring results, downloaded fromwww.epa.gov/air/data/ on 20 December 2005.4. The air pollution data here represents the2003 annual average for PM2.5: U.S. EPA,AirData: Access to Air Pollution Data, downloadedfrom www.epa.gov/air/data/ on 20 December2005. See Methodology for details on how themaps were generated.5. The air pollution data here represents the2003 April – October average one hour dailypeak concentration of ozone: U.S. EPA,
AirData: Access to Air Pollution Data, downloadedfrom www.epa.gov/air/data/ on 20 December2005. See Methodology for details on how themaps were generated.6. U.S. Environmental Protection Agency, AirQuality Criteria for Particulate Matter, Volume 1,EPA/600/P-99/002aF, October 2004; A. Fiore etal., Department of Earth and Planetary Sciences,Harvard University, “Variability in SurfaceOzone Background in the United States:Implications for Air Quality Policy,” Journal ofGeophysical Research 108: 4787, doi:10.1029/2003JD003855, 2003.7. A. Fiore et al., Department of Earth andPlanetary Sciences, Harvard University,“Variability in Surface Ozone Background in theUnited States: Implications for Air QualityPolicy,” Journal of Geophysical Research 108: 4787,doi:10.1029/2003JD003855, 2003.8. Clean Air Act, § 108.9. Whitman v. American Trucking Assoc., 531U.S. 457 (2001).10. American Lung Association, State of the Air2005, 28 April 2005, 55.11. Clean Air Scientific Advisory Committee(CASAC), EPA’s Review of the National AmbientAir Quality Standards for Particulate Matter(Second Draft PM Staff Paper, January 2005): AReview by the Particulate Matter Review Panel ofthe EPA Clean Air Scientific Advisory Committee,EPA-SAB-CASAC-05-007, June 2005; EPA,Review of the National Ambient Air Quality
Notes

Notes 37
Standards for Particle Pollution: Policy Assessment ofScientific and Technical Information, EPA-452/R-05-005, June 2005.12. M. Bell and D. Davis, “Reassessment of theLethal London Fog of 1952: Novel Indicators ofAcute and Chronic Consequences of AcuteExposure to Air Pollution,” EnvironmentalHealth Perspectives 109 Supplement 3: 389-94,2001.1.3 B. Karcher et al., “A Unified Model forUltra Fine Aircraft Particle Emissions,” Journalof Geophysical Research 105: D24 29379-29386,2002.14. M. Kleeman et al., “Size and CompositionDistribution of Fine Particulate Matter EmittedFrom Motor Vehicles,” Environmental Scienceand Technology 34: 1132-1142, 2000.15. H. Bunn et al., “Ultra fine Particles inAlveolar Macrophages from Normal Children,”Thorax 56: 932-934, 2001.16. A. Seaton et al., “Particulate Air Pollutionand the Blood,” Thorax 54: 1027-1032, 1999.17. M. Brauer et al., “Air Pollution and RetainedParticles in the Lung,” Environmental HealthPerspectives 109: 1039-1043, 2001.18. J. Pekkanen et al., “Daily Variations ofParticulate Air Pollution and ST-T Depressionsin Subjects with Stable Coronary Heart Disease:The Finnish ULTRA Study,” American Journalof Respiratory Critical Care Medicine 161: A24,2000.19. W.J. Gauderman et al., “The Effect of AirPollution on Lung Development from 10 to 18Years of Age,” The New England Journal ofMedicine 351: 1057-67, 9 September 2004.20. C. Pope et al., “Lung Cancer, Cardiopulmo-nary Mortality, and Long-Term Exposure toFine Particulate Air Pollution,” Journal of theAmerican Medical Association 287: 1132-1141,2002.21. Photo by Dr. Heather Viles, OxfordUniversity.22. J. Grigg, “The Health Effects of Fossil FuelDerived Particles,” Archives of Disease inChildhood 86: 79-83, 2002.23. 8-hour ozone standard: North CarolinaDepartment of Environment and NaturalResources, Davison of Air Quality, NC Statewide1-Hour and 8-Hour Ozone Exceedence Days,downloaded from www.ncair.org on 12 January2006.24. M. Lippman, “Health Effects of Ozone: ACritical Review,” Journal of the Air Pollution
Control Association 39: 672-695, 1989; I. Mudwayand F. Kelley, “Ozone and the Lung: A SensitiveIssue,” Molecular Aspects of Medicine 21: 1-48, 2000.25. M. Gilmour et al., “Ozone-EnhancedPulmonary Infection with StreptococcusZooepidemicus in Mice: The Role of AlveolarMacrophage Function and Capsular VirulenceFactors,” American Review of Respiratory Disease147: 753-760; I. Mudway and F. Kelley, “Ozoneand the Lung: A Sensitive Issue,” MolecularAspects of Medicine 21: 1-48, 2000.26. W. McDonnell et al., “Pulmonary Effects ofOzone Exposure During Exercise: Dose-Response Characteristics,” Journal of AppliedPhysiology 5: 1345-1352, 1983.27. N. Kunzli et al., “Association BetweenLifetime Ambient Ozone Exposure andPulmonary Function in College Freshmen –Results of a Pilot Study,” Environmental Research72: 8-16, 1997; I.B. Tager et al., “ChronicExposure to Ambient Ozone and Lung Functionin Young Adults,” Epidemiology 16: 751-9,November 2005.28. A. Galizia et al., “Long-Term Residence inAreas of High Ozone: Associations withRespiratory Health in a Nationwide Sample ofNonsmoking Young Adults,” EnvironmentalHealth Perspectives 107: 675-679, 1999.29. M. Fanucchi et al., “Repeated Episodes ofExposure to Ozone Alters Postnatal Develop-ment of Distal Conducting Airways in InfantRhesus Monkeys,” American Journal of Respira-tory Critical Care Medicine 161: A615, 2000;Kendall Powell, “Ozone Exposure ThrowsMonkey Wrench Into Infant Lungs,” NatureMedicine, Volume 9, Number 5, May 2003.30. Kendall Powell, “Ozone Exposure ThrowsMonkey Wrench Into Infant Lungs,” NatureMedicine, Volume 9, Number 5, May 2003.31. R. McConnell et al., “Asthma in ExercisingChildren Exposed to Ozone: A Cohort Study,”The Lancet 359: 386-391, 2002.32. Asthma: Ralph Delfino et al., “AsthmaSymptoms in Hispanic Children and DailyAmbient Exposures to Toxic and Criteria AirPollutants,” Environmental Health Perspectives111(4), 647-656, April 2003; I.L. Bernstein, M.Chan-Yeung, J.L. Malo, and D.I. Bernstein,Asthma in the Workplace, (New York, NY: MarcelDekker), 1999; Cancer: D. Glass et al., “Leuke-mia Risk Associated with Low-Level BenzeneExposure,” Epidemiology 14: 569-577, 2003; A.Blair and N. Kazerouni, “Reactive Chemicalsand Cancer,” Cancer Causes Control 8: 473-490.

38 Air Pollution and Public Health in North Carolina
33. P. van Vliet et al., “Motor Vehicle Exhaustand Chronic Respiratory Symptoms in ChildrenLiving Near Freeways,” Environmental Research74:122-32, 1997; T. Nicolai et al., “UrbanTraffic and Pollutant Exposure Related toRespiratory Outcomes and Atopy in a LargeSample of Children,” European RespiratoryJournal 21: 956-63, June 2003.34. W.J. Gauderman et al., “Childhood Asthmaand Exposure to Traffic and Nitrogen Dioxide,”Epidemiology 16: 737-43, November 2005.35. Cough: U. Gehrinig et al., “Traffic-RelatedAir Pollution and Respiratory Health Duringthe First 2 Yrs of Life,” European RespiratoryJournal 19: 690-8, April 2002; More asthmaevidence: J.J. Kim et al., “Traffic-Related AirPollution Near Busy Roads: the East BayChildren’s Respiratory Health Study,” AmericanJournal of Respiratory Critical Care Medicine 170:520-6, September 2004.36. R. Maheswaran and P Elliott, “StrokeMortality Associated With Living Near MainRoads in England and Wales,” Stroke 34: 2776-80, December 2003; G. Hoek et al., “AssociationBetween Mortality and Indicators of Traffic-Related Air Pollution in the Netherlands: aCohort Study,” Lancet 360: 1203-9, 19 October2002.37. Bob Weinhold, “Don’t Breathe and Drive?Pollutants Lurk Inside Vehicles,” EnvironmentalHealth Perspectives 109: A422-27, September 2001.38. M. Riediker et al., “Particulate MatterExposure in Cars is Associated with Cardiovas-cular Effects in Healthy Young Men,” AmericanJournal of Respiratory Critical Care Medicine 169:934-40, 15 April 2004.39. U.S. Environmental Protection Agency,Final Report to Congress on Benefits and Costs of theClean Air Act, 1990 to 2010, Document # EPA410-R-99-001, 15 November 1999; N. Kunzli etal., Air Pollution Attributable Cases—TechnicalReport on Epidemiology; Technical Report of theHealth Costs Due to Road Traffic-Related AirPollution—An Impact Assessment Project of Austria,France, and Switzerland, World Health Organiza-tion, Bern 1999.40. See Note 20.41. C. Pope, “Epidemiology of Fine ParticulateAir Pollution and Human Health: BiologicMechanisms and Who’s at Risk?” EnvironmentalHealth Perspectives 108: 713-723, August 2000.42. American Cancer Society, “Air PollutionLinked to Deaths from Lung Cancer,”www.cancer.org, 6 March 2002.
43. N. Kunzli et al., “Public Health Impact ofOutdoor and Traffic-Related Air Pollution: AEuropean Assessment,” The Lancet 356: 795-801,2 September 2002.44. A. Peters et al., “Increased Particulate AirPollution and the Triggering of MyocardialInfarction,” Circulation 103: 2810-2815, 2001.45. J. Samet et al., The United States HealthEffects Institute, The National Morbidity,Mortality, and Air Pollution Study, Part II:Morbidity and Mortality from Air Pollution in theUnited States, Research Report Number 94, June2000.46. K. Ito, S.F. de Leon and M. Lippmann,“Associations Between Ozone and DailyMortality,” Epidemiology 16: 446-57, July 2005.47. J. Schwartz et al., “Episodes of High CoarseParticle Concentrations Are Not AssociatedWith Increased Mortality,” Environmental HealthPerspectives 107: 339-342, 1999.48. J. Schwartz, “Is There Harvesting in theAssociation of Airborne Particles with DailyDeaths and Hospital Admissions?” Epidemiology12: 55-61, 2001; M. Bobak and D.A. Leon, “TheEffect of Air Pollution on Infant MortalityAppears Specific for Respiratory Causes in thePostnatal Period,” Epidemiology 10: 666-670, 1999.49. See Note 43.50. A. Mokdad et al., “Actual Causes of Death inthe United States, 2000,” Journal of the AmericanMedical Association 291, 1238-1245, 10 March2004.51. U.S. Environmental Protection Agency,Office of Policy, Climate Change and NorthCarolina, September 1998.52. National Assessment Synthesis Team,Climate Change Impacts on the United States; ThePotential Consequences of Climate Variability andChange, report for the U.S. Global ChangeResearch Program, 2001.53. SM Bernard et al., “The Potential Impacts ofClimate Variability and Change on Air Pollu-tion-Related Health Effects in the UnitedStates,” Environmental Health Perspectives 109:199-209, May 2001; K Knowlton et al., “Assess-ing Ozone-Related Health Impacts Under aChanging Climate,” Environmental HealthPerspectives 112:1557-63, November 2004.54. PJM Koken et al., “Temperature, AirPollution, and Hospitalization for Cardiovascu-lar Diseases Among Elderly People in Denver,”Environmental Health Perspectives 111: 1312-1317, 2003.

Notes 39
55. John Tagliabue, “Scorching Heat AroundEurope Causes Deaths and Droughts,” The NewYork Times, 19 July 2005.56. U.S. Environmental Protection Agency,Climate Change and North Carolina, September1998.57. See Note 45.58. Joel Schwartz, “Air Pollution and HospitalAdmissions for the Elderly in Birmingham,Alabama,” American Journal of Epidemiology 139:589-98, 15 March 1994; Joel Schwartz, “AirPollution and Hospital Admissions for theElderly in Detroit, Michigan,” American Journalof Respiratory Critical Care Medicine 150: 648-55,1994; Joel Schwartz , “PM10, Ozone, andHospital Admissions for the Elderly in Minne-apolis-St. Paul, Minnesota,” Archives of Environ-mental Health 49: 366-374, 1994; Joel Schwartz,“Short-Term Fluctuations in Air Pollution andHospital Admissions of the Elderly for Respira-tory Disease,” Thorax 50: 531-538, 1995; J.Schwartz and R. Morris, “Air pollution andhospital admissions for cardiovascular disease inDetroit, Michigan,” American Journal ofEpidemiology 142: 23-25, 1995; Joel Schwartz,“Air Pollution and Hospital Admissions forRespiratory Disease,” Epidemiology 7: 20-28,1996; Joel Schwartz, “Air Pollution and HospitalAdmissions for Cardiovascular Disease inTucson,” Epidemiology 8: 371-377, 1997.59. George Thurston et al., “RespiratoryHospital Admissions and Summertime Haze AirPollution in Toronto, Ontario: Consideration ofthe Role of Acid Aerosols,” EnvironmentalResearch 65: 271-290, 1994; R. Burnett et al.,“The Role of Particulate Size and Chemistry inthe Association Between Summertime AmbientAir Pollution and Hospitalization for Cardio-respiratory Disease,” Environmental HealthPerspectives 105: 614-620, 1997; R. Burnett et al.,“Association Between Ozone and Hospitaliza-tion for Respiratory Diseases in 16 CanadianCities,” Environmental Research 72: 24-31, 1997.60. R. Cody et al., “The Effect of OzoneAssociated with Summertime PhotochemicalSmog on the Frequency of Asthma Visits toHospital Emergency Departments,” Environ-mental Research 58: 184-194, 1992; C. Weisel etal., “Relationship Between SummertimeAmbient Ozone Levels and Emergency Depart-ment Visits for Asthma in Central New Jersey,”Environmental Health Perspectives 103, Supple-ment 2: 97-102, 1995.61. Joel Schwartz et al., “Particulate AirPollution and Hospital Emergency Room Visits
for Asthma in Seattle,” American Review ofRespiratory Disease 147: 826-831, 1993.62. Jennifer Peel et al., “Ambient Air Pollutionand Respiratory Emergency Department Visits,”Epidemiology 6:164-174, March 2005.63. See Note 31; The causal role of ozone inasthma development may be easier to detect inchildren who exercise because breathing ratesduring exercise can be up to 17 times higherthan during rest, leading to greater exposure toair pollutants: See W.D. McArdle et al., ExercisePhysiology: Energy, Nutrition, and HumanPerformance, (Philadelphia, PA: Williams andWilkins, 1996), 228.64. See Note 34.65. W. McDonnell et al., “Long-Term AmbientOzone Concentration and the Incidence ofAsthma in Nonsmoking Adults: the AHSMOGStudy,” Environmental Research 80: 110-121,1999.66. T. Wang et al., “Association Between Indoorand Outdoor Air Pollution and AdolescentAsthma From 1995 to 1996 in Taiwan,”Environmental Research 81: 239-247, 1999.67. T. Yu et al., “Adverse Effects of Low-LevelAir Pollution on the Respiratory Health ofSchoolchildren in Hong Kong,” Journal ofOccupational Environmental Medicine 43: 310-316,2001.68. Joel Schwartz, “Particulate Air Pollution andChronic Respiratory Disease,” EnvironmentalResearch 62: 7-13, 1993; D. Abbey et al., “Long-term Ambient Concentrations of Total Sus-pended Particles, Ozone, and Sulfur Dioxideand Respiratory Symptoms in a NonsmokingPopulation,” Archives of Environmental Health 48:33-46, 1993.69. U.S. Centers for Disease Control, “Measur-ing Childhood Asthma Prevalence Before andAfter the 1997 Redesign of the National HealthInterview Survey—United States,” Mortality andMorbidity Weekly Report 49: 908-911, 13 October2000.70. National Institutes of Health, NationalHeart, Lung, and Blood Institute, Data Releasefor World Asthma Day, May 2001.71. According to the American Lung Associationof North Carolina, over 170,000 children inNorth Carolina have been diagnosed withasthma. American Lung Association of NorthCarolina, Lung Health, Answers to Your Questionsand Resources You Can Use, Web Page, Viewed atwww.lungnc.org/lunghealth.htm on 17 January2006.

40 Air Pollution and Public Health in North Carolina
72. Division of Adult and Community Health,National Center for Chronic Disease Preventionand Health Promotion, Centers for DiseaseControl and Prevention, Behavioral Risk FactorSurveillance System Online Prevalence Data, 1995-2002.73. Because ozone exposure had a statisticallysignificant link to asthma development only inmales in the McDonnell paper cited in note 65,our estimate is limited to new cases of asthmaonly in the adult male population. Actual newasthma cases caused by air pollution are likelyhigher.74. See Note 34.75. George Thurston et al., “Summertime HazeAir Pollution and Children with Asthma,”American Journal of Respiratory Critical CareMedicine 155: 654-660, February 1997.76. A. Whittemore and E. Korn, “Asthma andAir Pollution in the Los Angeles Area,” Ameri-can Journal of Public Health, 70: 687-696, 1980.77. B. Ostro and S. Rothschild, “Air Pollutionand Acute Respiratory Morbidity: an Observa-tional Study of Multiple Pollutants,” Environ-mental Research 50: 238-47, 1989.78. J. Schwartz et al., “Acute Effects of SummerAir Pollution on Respiratory Symptom Report-ing in Children,” American Journal of RespiratoryCritical Care Medicine 150: 1234-1242, 1994.79. See W.H.O., Note 2.80 Ibid.81. T. Woodruff et al., “The RelationshipBetween Selected Causes of Postneonatal InfantMortality and Particulate Air Pollution in theUnited States,” Environmental Health Perspectives105: 608-612, 1997; T. Woodruff et al., “FineParticulate Matter (PM2.5) Air Pollution andSelected Causes of Postneonatal Infant Mortal-ity in California,” Environmental Health Perspec-tives, doi:10.1289/ehp.8484 available viadx.doi.org, Online 13 January 2006.82. M. Bobak and D.A. Leon, “The Effect of AirPollution on Infant Mortality Appears Specificfor Respiratory Causes in the Postnatal Period,”Epidemiology 10: 666-670, 1999.83. K.Y. Chay and M. Greenstone, NationalBureau of Economic Research, The Impact of AirPollution on Infant Mortality: Evidence fromGeographic Variation in Pollution Shocks Induced bya Recession, Manuscript cited in “Spring 2002References,” Health and Clean Air Newsletter,www.healthandcleanair.org, 2002.84. M. Friedman et al., “Impact of Changes in
Transportation and Commuting BehaviorsDuring the 1996 Summer Olympic Games inAtlanta on Air Quality and Childhood Asthma,”Journal of the American Medical Association 285:897-905, 2001.85. Ibid.86. U.S. Center for Disease Control, CDC StudyLinks Improved Air Quality with DecreasedEmergency Room Visits for Asthma, Press Release,21 February 2001.87. American Lung Association, Asthma inChildren Fact Sheet, March 2003.88. U.S. Centers for Disease Control, “Measur-ing Childhood Asthma Prevalence Before andAfter the 1997 Redesign of the National HealthInterview Survey — United States,” Mortalityand Morbidity Weekly Report 49: 908-911, 13October 2000.89. Janneane Gent et al., “Association of low-level ozone and fine particles with respiratorysymptoms in children with asthma,” Journal ofThe American Medical Association 290, 1859-1867,8 October 2003.90. E.W. Triche et al, “Low Level OzoneExposure and Respiratory Symptoms inInfants,” Environmental Health Perspectivesdoi:10.1289/ehp.8559 (available at dx.doi.org),Online 29 December 2005.91. D. Dockery et al., “Health Effects of AcidAerosols on North American Children: Respira-tory Symptoms,” Environmental Health Perspec-tives 104: 500-505, May 1996.92. F. Gilliland et al., “The Effects of AmbientAir Pollution on School Absenteeism Due toRespiratory Illness,” Epidemiology 12: 43-54,2001.93. H. Park et al., “Association of Air Pollutionwith School Absenteeism Due to Illness,”Archives of Pediatric and Adolescent Medicine 156:1235-1239, 2002.94. North Carolina Department of Environmentand Natural Resources, Division of Air Quality,North Carolina’s Clean Smokestacks Act, down-loaded from http://daq.state.nc.us/news/leg/cleanstacks.shtml, 27 December 2005.95. Area sources include small stationaryengines, businesses that use solvents, fires, orother chemicals and other stationary sources ofpollution that emit relatively small quantities ofpollution. These are important sources ofparticulates and smog-forming volatile organiccompounds, but are much more varied in typethan either point or mobile sources. Green

Notes 41
Media Toolshed, Pollution Locator: Smog andParticulates, available at scorecard.org, viewed on27 December 2005; U.S. EnvironmentalProtection Agency, AirData Emissions by CategoryReport—Criteria Air Pollutants, 1999, down-loaded 27 December 2005.96. See Note 39.97. U.S. EPA, AirData: Access to Air PollutionData, downloaded from www.epa.gov/air/dataon 20 December 2005.98. N. Kunzli et al., Air Pollution AttributableCases—Technical Report on Epidemiology; TechnicalReport of the Health Costs Due to Road Traffic-Related Air Pollution—An Impact AssessmentProject of Austria, France, and Switzerland, WorldHealth Organization, Bern 1999.99. Ibid.100. See Note 7.101. See Note 98.102. North Carolina State Demographics,Estimated 2003 County Totals by Age, downloadedfrom demog.state.nc.us on 28 December 2005.103. North Carolina State Center for HealthStatistics: Detailed Mortality Statistics in NorthCarolina 2003, ICD-10 codes A00-R99, NorthCarolina Health Data Query System, down-loaded 29 December 2005.104. Ibid.105. U.S. Department of Health and HumanServices, Agency for Healthcare Research andQuality, Healthcare Cost and UtilizationProject, State Inpatient Database: North Carolina2003.106. Ibid.107. U.S. Environmental Protection Agency,Final Report to Congress on Benefits and Costs of theClean Air Act, 1990 to 2010, Document # EPA410-R-99-001, 15 November 1999, D-66.108. Ibid.109. Division of Adult and Community Health,National Center for Chronic Disease Preventionand Health Promotion, Centers for DiseaseControl and Prevention, Behavioral Risk FactorSurveillance System Online Prevalence Data, 2003.110. See Note 107.111. Weighted average of the 0-5 year old rateof 0.015 and 5 – adult rate of 0.0071: USDepartment of Health and Human Services,Tracking Healthy People 2010, Section 24 -Respiratory Diseases, November 2000.112. Ibid.
113. See Note 107.114. Ibid.115. Estimate based on school attendancefigures: Ken Gattis, Public Schools of NorthCarolina, Personal Correspondence, 19 January2006; and H. Park et al., “Association of AirPollution with School Absenteeism Due toIllness,” Archives of Pediatric and AdolescentMedicine 156: 1235-1239, 2002.116. See Note 107.117. See Note 98.118. Ibid.119. Ibid.120. See Note 107.121. Ibid.122. See Note 98; Estimate from 2 studies: C.Pope et al., “Lung Cancer, CardiopulmonaryMortality, and Long-Term Exposure to FineParticulate Air Pollution,” Journal of theAmerican Medical Association 287: 1132-1141,2002; and D. Dockery et al., “An AssociationBetween Air Pollution and Mortality in Six U.S.Cities,” New England Journal of Medicine 329:1753-1759, 1993.123. See Note 98; Estimate from eight U.S. andCanadian studies: George Thurston et al.,“Respiratory Hospital Admissions and Summer-time Haze Air Pollution in Toronto, Ontario:Consideration of the Role of Acid Aerosols,”Environmental Research 65: 271-290, 1994; JoelSchwartz, “Air Pollution and Hospital Admis-sions for the Elderly in Birmingham, Alabama,”American Journal of Epidemiology 139: 589-98, 15March 1994; Joel Schwartz, “Air Pollution andHospital Admissions for the Elderly in Detroit,Michigan,” American Journal of RespiratoryCritical Care Medicine 150: 648-55, 1994; JoelSchwartz , “PM10, Ozone, and Hospital Admis-sions for the Elderly in Minneapolis-St. Paul,Minnesota,” Archives of Environmental Health 49:366-374, 1994; Joel Schwartz, “Short-TermFluctuations in Air Pollution and HospitalAdmissions of the Elderly for RespiratoryDisease,” Thorax 50:531-538, 1995; J. Schwartzand R. Morris, “Air pollution and hospitaladmissions for cardiovascular disease in Detroit,Michigan,” American Journal of Epidemiology 142:23-25, 1995; Joel Schwartz, “Air Pollution andHospital Admissions for Respiratory Disease,”Epidemiology 7: 20-28, 1996; Joel Schwartz, “AirPollution and Hospital Admissions for Cardio-vascular Disease in Tucson,” Epidemiology 8: 371-377, 1997; R. Burnett et al., “The Role ofParticulate Size and Chemistry in the Association

42 Air Pollution and Public Health in North Carolina
Between Summertime Ambient Air Pollutionand Hospitalization for Cardio-respiratoryDisease,” Environmental Health Perspectives 105:614-620, 1997.124. See Note 98; Joel Schwartz, “Air Pollutionand Hospital Admissions for the Elderly inDetroit, Michigan,” American Journal ofRespiratory Critical Care Medicine 150: 648-55,1994; Joel Schwartz, “Air Pollution and HospitalAdmissions for Cardiovascular Disease inTucson,” Epidemiology 8: 371-377, 1997; R.Burnett et al., “The Role of Particulate Size andChemistry in the Association Between Summer-time Ambient Air Pollution and Hospitalizationfor Cardio-respiratory Disease,” EnvironmentalHealth Perspectives 105: 614-620, 1997.125. See Note 98; Weighted average of threeEuropean studies: A. Dusseldorp et al., “Associa-tions of PM10 and Airborne Iron with Respira-tory Health of Adults Living Near a SteelFactory,” American Journal of Respiratory CriticalCare Medicine 152: 1032-1039, 1995; T.Hiltermann et al., “Asthma Severity andSusceptibility to Air Pollution,” EuropeanRespiratory Journal 11: 686-693, 1996; F.Neukirch et al., “Short-term Effects of Low-level Winter Pollution on Respiratory Health ofAsthmatic Adults,” Archives of EnvironmentalHealth 53: 320-328, 1998.126. See Note 98; D. Abbey et al., “Long-termAmbient Concentrations of Total SuspendedParticles, Ozone, and Sulfur Dioxide andRespiratory Symptoms in a NonsmokingPopulation,” Archives of Environmental Health 48:33-46, 1993.127. B. Ostro, “Air Pollution and MorbidityRevisited: a Specification Test,” Journal ofEnvironmental Economics and Management, 14:87-98, 1987; B. Ostro and S. Rothschild, “AirPollution and Acute Respiratory Morbidity: anObservational Study of Multiple Pollutants,”Environmental Research 50: 238-47, 1989.128. B. Ostro and S. Rothschild, “Air Pollutionand Acute Respiratory Morbidity: an Observa-tional Study of Multiple Pollutants,” Environ-mental Research 50: 238-47, 1989. B. Ostro,“Associations Between Morbidity and Alterna-tive Measures of Particulate Matter,” RiskAnalysis 10: 421-427, 1990.129. A. Krupnick, W. Harrington, and B. Ostro,“Ambient Ozone and Acute Health Effects:Evidence from Daily Data.” Journal of Environ-mental Economics and Management 18: 1-18, 1990.130. See Note 107: W. McDonnell et al.,
“Long-Term Ambient Ozone Concentration andthe Incidence of Asthma in Nonsmoking Adults:the AHSMOG Study,” Environmental Research80: 110-121, 1999.131. See Note 107: R. Burnett et al., “Effects ofParticulate and Gaseous Air Pollution onCardio-Respiratory Hospitalizations,” Archives ofEnvironmental Health 54: 130-139, 1999.132. See Note 107: A. Whittemore and E. Korn,“Asthma and Air Pollution in the Los AngelesArea,” American Journal of Public Health, 70: 687-696, 1980.133. See Note 107: B. Ostro and S. Rothschild,“Air Pollution and Acute Respiratory Morbidity:an Observational Study of Multiple Pollutants,”Environmental Research 50: 238-47, 1989.134. See Note 107: A. Krupnick, W.Harrington, and B. Ostro, “Ambient Ozone andAcute Health Effects: Evidence from DailyData.” Journal of Environmental Economics andManagement 18: 1-18, 1990.135. See Note 107: T. Woodruff, “The Rela-tionship Between Selected Causes of Postneona-tal Infant Mortality and Particulate Air Pollutionin the United States,” Environmental HealthPerspectives 105: 608-612, 1997.136. See Note 84.137. See Note 98: D. Dockery et al., “Effects ofInhalable Particles on Respiratory Health ofChildren,” American Review of Respiratory Disease139: 587-594, 1989; D. Dockery et al., “HealthEffects of Acid Aerosols on North AmericanChildren: Respiratory Symptoms,” Environmen-tal Health Perspectives 104: 500-505, 1996; C.Braun-Fahrländer et al, “Respiratory Health andLong-term Exposure to Air Pollutants in SwissSchoolchildren,” American Journal of RespiratoryCritical Care Medicine 155: 1042-1049, 1997.138. See Note 98; Joint estimate from two U.S.Studies: C. Pope et al., “Respiratory Health andPM10 Pollution - A Daily Time Series Analysis,”American Review of Respiratory Disease 144: 668-674, 1991; B. Ostro et al., “Air Pollution andAsthma Exacerbations Among African-AmericanChildren in Los Angeles, Inhalation Toxicology 7:711-722, 1995.139. M.R. Ransom and C.A. Pope, «ElementarySchool Absences and PM10 Pollution in UtahValley,» Environmental Research 58: 204-219, 1992.140. Health Effects Institute (a partnershipbetween the Auto Industry and the U.S. EPA),Revised Analyses of Time-Series Studies of AirPollution and Health. May 2003.
Har
riet
Eck
stein
Gra
phic
Des
ign

Notes 43

44 Air Pollution and Public Health in North Carolina