Embed Size (px)
Citation preview

Research ArticleAir Pollution by Hydrothermal Volcanism and HumanPulmonary Function
Diana Linhares12 Patriacutecia Ventura Garcia13 Faacutetima Viveiros24
Teresa Ferreira24 and Armindo dos Santos Rodrigues12
1Department of Biology University of the Azores Ponta Delgada 9501-801 Azores Portugal2CVARG Center for Volcanology and Geological Risks Assessment (CVARG) University of the Azores Ponta Delgada9501-801 Azores Portugal3CE3C Centre for Ecology Evolution and Environmental Changes (CE3C) and Azorean Biodiversity GroupUniversity of the Azores 9501-801 Ponta Delgada Portugal4Department of Geosciences University of the Azores Ponta Delgada 9501-801 Azores Portugal
Correspondence should be addressed to Diana Linhares dlinharesuacpt
Received 21 November 2014 Accepted 13 March 2015
Academic Editor Petros Gikas
Copyright copy 2015 Diana Linhares et alThis is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
The aim of this study was to assess whether chronic exposure to volcanogenic air pollution by hydrothermal soil diffuse degassingis associated with respiratory defects in humans This study was carried in the archipelago of the Azores an area with activevolcanism located in the Atlantic Ocean where Eurasian African and American lithospheric plates meet A cross-sectional studywas performed on a study group of 146 individuals inhabiting an area where volcanic activity is marked by active fumarolicfields and soil degassing (hydrothermal area) and a reference group of 359 individuals inhabiting an area without these secondarymanifestations of volcanism (nonhydrothermal area) Odds ratio (OR) and 95 confidence intervals (CIs) were adjusted for agegender fatigue asthma and smoking The OR for restrictive defects and for exacerbation of obstructive defects (COPD) in thehydrothermal area was 44 (95 CI 178ndash1069) and 32 (95 CI 182ndash558) respectively Increased prevalence of restrictions and allCOPD severity ranks (mild moderate and severe) was observed in the population from the hydrothermal areaThese findingsmayassist health officials in advising and keeping up with these populations to prevent and minimize the risk of respiratory diseases
1 Introduction
About 10 of the worldwide population inhabits or lives inthe vicinity of some active or historically active volcano [1]Despite the hazards associated with volcanic activities therichness of soils in nutrients attracts people to live in theseareas Several studies have established an association betweenacute [2ndash4] and long-term [5 6] exposure to anthropogenicair pollutants and lung function while only fewhave analyzedthe respiratory effects from volcanogenic air pollution [7ndash9]
The Azores archipelago (Portugal) comprises nine vol-canic inhabited islands located between 36∘451015840ndash39∘451015840N and24∘451015840ndash31∘171015840W (Figure 1(a)) where the Eurasian Africanand American lithospheric plates meet [10] On account ofthis complex tectonic setting seismic and volcanic activitiesare frequent in the archipelago [11] Sao Miguel Island
the largest of the archipelago is formed by three majoractive central volcanoes (Sete Cidades Fogo and Furnas)linked by rift zones [12] (Figure 1(b)) Furnas Volcano islocated in the eastern part of the island where present-dayvolcanic activity is marked by several hydrothermal man-ifestations consisting of active fumarolic fields thermal andcoldCO
2-rich springs and soil diffuse degassing areas [11 13]
Gases released in these diffuse degassing areas are essen-tially carbon dioxide (CO
2) and radon (222Rn) this last one
a radioactive gas Carbon dioxide is one of the most abun-dant volcanic gases and is amongst the most importantdiffused gases released by soil degassing in Furnas Volcano(hydrothermal soil CO
2emissions in Furnas Volcano are
estimated to be approximately 968 td) [14] this gas if presentat high concentrations can become particularly dangerousfor public health since it works as asphyxiant preventing
Hindawi Publishing CorporationBioMed Research InternationalArticle ID 326794
2 BioMed Research International
(a)
(b)
60∘W 50
∘W 40∘W 30
∘W 20∘W 10
∘W 0∘
10∘E
40∘N
40∘N 30
∘N
20∘N
38∘N
32∘W 30
∘W 28∘W 26
∘W 24∘W
Sete CidadesVolcano
Ponta Delgadacity
FogoVolcano
Ribeira Quentevillage
FurnasVolcano
Figure 1 (a) Location map of the Azores archipelago and (b) Sao Miguel Island The places represented on the map correspond to the twostudied areas (Ponta Delgada and Ribeira Quente)
oxygen respiration [15] Previous studies [13] showed thatCO2is released permanently to the atmosphere from soils
in volcanic areas not only during eruptive periods but alsoduring quiescent periods of activity Considering that CO
2
released by soils may enter the buildings through pipescracks in the floor andor the contact betweenfloor andwallsit is considered important to assess the CO
2flux in buildings
Carbon dioxide level is usually greater inside a building thanoutside and it can act as an indicator of ventilation efficiencyshowing whether the supply of outside air is sufficient todilute indoor air contaminants [16] According toWHO [17]indoor air pollution is responsible for 27 of the diseases
worldwide such effects of indoor air pollution are par-ticularly highlighted in studies regarding the occupationalexposure as it was shown in the reviewmade by Balmes et al[18] that estimated that 15 of COPD was attributable to theair quality at the workplace
Furnas and Ribeira Quente are two villages locatedrespectively inside the caldera and in the south flank ofFurnas active volcano where the ground gas emissions thatcharacterize the diffuse degassing areas occur permanentlyand thus inhabitants of such areas are often exposed toelevated concentrations of CO
2from volcanic origin [14]
Previous studies evidenced that Furnas inhabitants have
BioMed Research International 3
Table 1 Description of the study populations (study and reference groups) (mean plusmn SE for continuous variables or n () for categoricalvariables)
Reference group(Ponta Delgada 119899 = 359)
Study group(Ribeira Quente 119899 = 146) P valuea
General characteristicsAge (years) 413 plusmn 127 398 plusmn 112 451 plusmn 153 0001
Age gt41b 234 (463) 152 (423) 82 (561) 0005Gender male 207 (409) 155 (431) 52 (356) 0117BMI (kgm2) 261 plusmn 44 257 plusmn 39 271 plusmn 54 0006
BMI gt26c 213 (422) 141 (393) 72 (493) 0041Smoking status
Smoker 163 (322) 135 (376) 28 (191) lt0001Previous smoker 91 (18) 69 (192) 22 (15) 0271
Easy fatigue yes 116 (23) 40 (111) 76 (52) lt0001Asthma yes 43 (85) 29 (8) 14 (96) 0581Occupation
White collar 135 (267) 122 (34) 13 (89) lt0001Blue collar 256 (507) 233 (65) 23 (158) lt0001Other 114 (226) 4 (1) 110 (753) lt0001
StudyFEV1 predicted
d 885 plusmn 204 925 plusmn 166 786 plusmn 252 0001FVC predicted 966 plusmn 192 988 plusmn 15 911 plusmn 262 lt0001FEV1FVC predicted 918 plusmn 142 938 plusmn 117 87 plusmn 181 lt0001Lung function
Restriction yes 26 (51) 11 (3) 15 (102) 0001COPD yes 92 (182) 43 (119) 49 (336) lt0001
CO2 flux gm2de 1536 508 lt0001
aP value comparing reference and study groups by Mann-Whitney for continuous variables and by 1205942 for categorical variablesbCut-off defined according to the mean value (ie 413 years) of the observed age distribution in the whole populationcCut-off defined according to the mean value (ie 261 BMI) of the observed BMI distribution in the whole populationdPredicted values from the National Health and Nutrition Examination Survey CohorteCO2 flux is expressed in mean
a high incidence of chronic bronchitis and of some cancertypes (eg lip oral cavity and pharynx) [19 20] and a higherrisk of DNA damage in human buccal epithelial cells [21]Moreover a very recent study by Camarinho et al [22]showed that chronic exposure to volcanogenic air pollutantscauses lung injury in wild mice However to our knowledgeup to date no study was carried out to assess the associationbetween volcanogenic air pollution by soil diffuse degassing(DDS) and the risk of development of respiratory defectsTherefore the present study was carried out to evaluatewhether chronic exposure to permanent volcanogenic airpollution is a risk factor for human restrictive and obstructive(COPD) respiratory defects
2 Methods
21 Study Population To perform this study two areas wereselected an area with no secondary manifestations of vol-canism therefore a nonhydrothermal area (Ponta Delgada)and an area where volcanic activity is marked by active fum-arolic fields and degassing soils (hydrothermal area) (Ribeira
Quente) A diagnosis campaign was established for eval-uation of pulmonary function by spirometry tests for theinhabitants of both areas Spirometry tests were carried outin either the participantsrsquo workplaces or their homes Astandard questionnaire was applied to each individual thatvolunteered to participate Medical history data for respira-tory symptoms were taken using a standard questionnairemodified from a standardized respiratory symptomquestion-naire fromAmericanThoracic Society (ATS) [23] and BritishMedical Research Councilrsquos Committee [24] Each personwas interviewed about their age height weight educationoccupation smoking habits (smoking of cigarettes andoruse of smokeless tobacco) amount of cigarettes smokeddayfatigue and general respiratory health status where asthmawas defined by a positive response to ldquoDid any doctordiagnose you with asthmardquo
The study group consisted of 146 participants (94 womenand 52 men) residents in Ribeira Quente village (Table 1)Ribeira Quente village has 767 inhabitants [25] 148 childrenand 619 adults (298 women and 321 men) therefore the par-ticipation rate was 263 This village is located on the south
4 BioMed Research International
flank of Furnas Volcano (Sao Miguel Island) (Figure 1(b))in an important diffuse degassing structure (DDS) about 98of buildings in this village are placed above anomalous soilCO2degassing with volcanic-hydrothermal origin [14 26]
In addition several fumaroles may be found along RibeiraQuente stream and dispersed in the village [13]Thus RibeiraQuente inhabitants are chronically exposed to gases ofvolcanic origin particularly from soil diffuse degassing Evenif no indoormeasurements were performed concomitantly tothe diagnosis tests previous works showed that in the diffusedegassing structures indoor CO
2is anomalously high and
can reach lethal values during extreme weather events [13]Permanent release of gases from the soils increases the indoorCO2concentrations independently of the anthropogenic
contributionThe reference group comprised 359 individuals (204
women and 155men)working in downtown of PontaDelgadacity (Table 1) Ponta Delgadarsquos downtown has 7818 adultworkers [25] therefore the participation rate was 45Ponta Delgada is located in the south side of Sao MiguelIsland (Azores Portugal Figure 1(b)) in the Regiao dos PicosVolcanic Complex a basaltic rift zone located between SeteCidades and Fogo Volcanoes where no manifestations ofvolcanism have been identified [11]
The Ethics Board of Divino Espirito Santo Hospital(Ponta Delgada Azores Portugal) approved the study Allindividuals signed a written informed consent in compliancewith the Helsinki Declaration and Oviedo Convention toparticipate in this study Table 1 summarizes the demographiccharacteristics and main lifestyle habits of the studied popu-lations Only individuals resident for more than five years ineach locality were considered in this study
22 Spirometry Tests The forced expiratory volume in onesecond (FEV
1) and the forced vital capacity (FVC) values
were obtained by spirometry in all participants Spirometrytests were conducted with the participants in an up positionwearing a nose clip and a disposable mouth piece usingthe EasyOne automated portable spirometer (ndd ZurichSwitzerland) which meets ATSERS spirometry standards[27] and is equipped with software that checks for unac-ceptable maneuvers and compares the measured values withreference tables Standardized operating procedures wereimplemented and controlled Participants performed three tofive attempts to provide at least three technically acceptablemaneuvers following the criteria recommended by the ATS[28] and the guidelines of the European Respiratory Society[27] Postbronchodilator tests were not applied
Spirometry datawere classified categorically as being con-sistent with either a normal pulmonary function a restrictivedefect or an obstructive defect Spirometric detection ofrestriction was considered in all subjects with normal FEV
1
FVC with FVC lt 80 predicted and FEV1FVC lt 70 was
used as a fixed cut-point for obstruction (COPD) accordingto the third United States National Health and NutritionExamination Survey (NHANES III) for adult CaucasiansAccording to the GOLD guidelines COPD was furtherclassified in the following ranks given by the spirometer
output mild (FEV1ge 80) moderate (FEV
150ndash79) and
severe (FEV130ndash49)
23 Exposure Assessment to Volcanogenic Air Pollution byDDS Carbon dioxide degassing maps may be useful for vol-canicseismic monitoring purposes as they represent a refer-ence for future variations on the state of activity of the volcano[14]
Measurements of soil CO2released by soil degassing in
Ribeira Quente village were carried out recently by Viveiroset al [14 26] The surveys were made using portable instru-ments that perform measurements based on the accumula-tion chamber method [29] Almost all buildings (about 98)in Ribeira Quente village are placed in an anomalous highCO2degassing zone (DDS) with soil CO
2fluxes that can
reach values higher than 25000 gm2d [14] Considering thatCO2released by soils may enter the buildings (eg through
pipes cracks in the floor andor the contact between floorandwalls) CO
2degassingmaps produced for Ribeira Quente
village [14 26] were used to attribute a CO2flux value to each
building Even if no indoor measurements were performedthe CO
2released from soils is positively correlated with the
indoor CO2concentrations [13] so measurements applied
outside the buildings are indirectly representative of the CO2
concentrations that can be found indoors [13] Sporadic soilCO2flux measurements were performed at Ponta Delgada in
the areas surrounding the buildings occupied by individualsfrom the reference group The 68 measurements performedshowed that CO
2flux values were lower than 25 gm2d and
thus representative of biogenic origin andwithout hydrother-mal contribution
24 Statistical Analysis Pearson Chi-Square test was used tocompare restrictions and COPD prevalence between individ-uals inhabiting the environment with volcanic degassing andindividuals from the reference group To estimate the asso-ciation between chronic exposure to an environment withvolcanic air pollution and restrictive and obstructive defects(no versus yes) odds ratio (OR) and 95 confidence intervals(95 CIs) were calculated using a binary logistic regressionmodel adjusting for age gender (male versus female) fatigue(yes versus no) and smoking status (yes versus no)
To estimate the association between chronic exposure toan environment with volcanic air pollution and the increasein the severity COPD odds ratio (OR) and 95 confidenceintervals (95 CIs) were calculated using an ordinal logisticregression model adjusting for age fatigue (yes versus no)asthma (yes versus no) and smoking status (yes versus no)The occurrence of obstructions was graded on scales accord-ing to their occurrence and severity 1 without obstructionand 2 to 4 with obstruction from the least severe (2) to themost severe (4)
Mann-Whitney 119880 test was used to compare soil CO2
fluxes released by diffuse degassing between the reference andthe study group
All statistical analysis was performed using IBM SPSSStatistics 200 for Windows [30] and the level of statisticalsignificance was set at 119875 le 005
BioMed Research International 5
Table 2 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing (DDS) andrestrictive lung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 1097Prob gt chi2 = 005
Parameter 119899 () OR (95 CI)a P valueAge 099 (096ndash102) 0933Gender
Male 207 (41) 116 (050ndash269) 0729Female 298 (59) 100
Easy fatigueYes 116 (23) 062 (023ndash167) 0349No 389 (77) 100
Smoking statusSmoker 163 (323) 094 (036ndash242) 0892Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 437 (178ndash1069) 0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
3 Results
The general characteristics of the study populations arepresented in Table 1The study group has an older populationand a higher BMI than the reference one (561 versus 423of individuals with more than 41 years and 271 kgm2 versus257 kgm2 resp) On the other hand the reference group hasa higher percentage of smokers than the study group (376versus 191)
Soil CO2flux was significantly different (119875 lt 0001)
between the studied areas (Table 1) According to criteriafor diffuse degassing susceptibility areas defined by Viveiroset al [14] all the analyzed buildings in Ponta Delgada arelocated in low susceptibility areas (CO
2flux lt 25 gm2d)
while in Ribeira Quente 19 of the buildings were locatedin moderate susceptibility areas (soil CO
2flux between
25 gm2d and 50 gm2d) and the remaining 981 were ina high susceptibility area (soil CO
2flux ge 50 gm2d) (Sup-
plementary Material 1 in Supplementary Material availableonline at httpdxdoiorg1011552015326794)
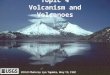
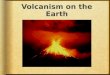
31 Prevalence of Restrictive and Obstructive RespiratoryDefects The prevalence of restrictions in the study groupwas significantly higher than in the reference group (102versus 30 resp 119875 = 0001) Similarly the prevalence ofCOPD was significantly higher in the study group than inthe reference one (336 versus 119 resp 119875 lt 0001)(Figure 2) The prevalence of more severe obstructions wasalso higher in the study group compared to the reference one(mild 157 versus 44 moderate 68 versus 22 and severe47 versus 0 resp)
32 Restrictive or Obstructive Respiratory Defects and Expo-sure to Volcanogenic Air Pollution by DDS Exposure to
0102030405060708090
Normal Restriction COPD
Prev
alen
ce (
)
Reference groupStudy group
lowastlowast lowast
lowast
Figure 2 Proportion () of individuals with obstructive andrestrictive airway diseases in study (Ribeira Quente) and reference(Ponta Delgada) groups lowastsignificantly different at 119875 lt 005
volcanogenic air pollution by DDSwas a significant predictorof the prevalence of respiratory restrictions and of COPDexacerbation in the multivariate analysis After adjustmentfor age gender fatigue and smoking status a higher preva-lence of respiratory restrictions was found associated withexposure to volcanogenic air pollution by DDS (OR = 4495 CI 178ndash1069 119875 = 0001) (Table 2) Also after theadjustment for the same factors a higher prevalence ofrespiratory obstructions was found associated with exposureto the volcanic environment (OR = 28 95 CI 160ndash499)(Table 3) Exacerbation in COPD severity was also foundsignificantly associated with exposure to volcanogenic airpollution by DDS (OR = 32 95 CI 182ndash558 119875 lt 0001)(Table 4)
The analyzed confounding factors did not show anysignificant association with respiratory restrictions (Table 2)but respiratory obstructions were significantly associated
6 BioMed Research International
Table 3 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and obstructivelung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 6080Prob gt chi2 = lt0001
Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (105ndash328) 0033No 389 (77) 100
GenderMale 207 (41) 066 (039ndash111) 0123Female 298 (59) 100
Smoking statusSmoker 163 (323) 234 (135ndash406) 0002Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 283 (160ndash499) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
Table 4 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and COPDexacerbation
Ordinal logistic regressionNumber of obs 505LR chi2(5) = 7019
Prob gt chi2 = lt0001Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (100ndash324) 0046No 389 (77) 100
AsthmaYes 43 (85) 225 (105ndash482) 0037No 462 (915) 100
Smoking statusSmoker 163 (323) 211 (125ndash356) 0005Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 319 (182ndash558) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
with age fatigue and smoking status (Table 3) The increasein COPD severity was significantly associated with asthmaand the abovementioned factors (Table 4)
4 Discussion
The association between exposure to air pollution andadverse respiratory effects has been widely demonstrated[31 32] Such association is usually related to anthropogenicair pollution while for volcanogenic pollution there are
much fewer studies Volcanoes and volcanic manifestationssuch as fumaroles and hot and cold CO
2-rich springs as
well as degassing soils release into the environment metalshazardous aerosols and gases that daily affect the quality ofthe environment and the health of human populations [33]
The measurements of CO2flux revealed that the study
group (from the hydrothermal area) is chronically exposed toelevated volcanogenic air pollution by soil diffuse degassingcompared to the reference group (average values are 508 gm2d (asymp3573 ppms) versus 1536 gm2d (asymp108 ppms)
BioMed Research International 7
resp) Carbon dioxide levels are described to be usuallygreater inside a building than outside [34 35] therefore thesepopulations are much probably subjected to higher levels ofindoor CO
2than the presented values Also independently
of the biological CO2contribution the hydrothermal CO
2
emission is permanent and thus the level of CO2in the
Ribeira Quente buildings must be always higher than theldquonormalrdquo values and sporadically reach anomalous highvalues as recognized in previous works only due to meteo-rological changes [13] The threshold limit value for 8 h timeweighted-average exposures to CO
2is 5000 ppm (WHO)
and possibly the average CO2concentrations encountered
in the buildings are below this limit and are not expectedto cause health symptoms such as headaches fatigue andeye and throat irritation However the consequences ofthe permanent presence of indoor CO
2in concentrations
higher than the outdoor environment are still far from beingunderstood and may eventually lead to some stress effect inthe organisms that needs to be better studied In additionthe CO
2emission may be also associated with other volcanic
emissions as it is the case of the radioactive gas radon Themeasurements performed showed that the study group ischronically exposed to elevated volcanogenic air pollutionnamely high CO
2soil diffuse degassing high concentrations
of CO2can cause headaches due to hypercapnia and the
decrease of O2in the bloodstream [36] When these two
events combine the body responds by increasing blood flowto the brain by dilating the blood vessels resulting in pain[36] A significant association was found between restrictiverespiratory defects and the exposure to volcanogenic airpollution by DDS measured as 44 times higher in theinhabitants of Ribeira Quente (study group) when comparedto the reference one A significant association was also foundbetween obstructive respiratory defects and exposure tovolcanogenic air pollution by DDS measured as 28 timeshigher in the study group None of the analyzed confoundingfactors (age gender fatigue and smoking status) was signifi-cantly associated with respiratory restriction but apart fromgender all confounding factors were positively associatedwith respiratory obstructions
Results also showed significant associations between theincrease in the severity of COPD and the exposure to soildiffuse degassing in the study group when compared to thereference one given as 32 times higher in Ribeira Quenteinhabitants (study group) Age asthma fatigue and smokingstatus were also significantly associated with the increase inCOPD severity
Age and smoking habits are well associated with COPDprevalence [37 38] According to our results the classificationof subjects who are at risk is relevant in middle-aged andelderly persons (ie gt 41 years old) individuals with asthmaand smokers Aging affects the structure function andcontrol of the respiratory system according to Stanojevic etal [39] both FEV
1and FVC decrease with age and thus
the observed increase in COPD associated with age wasexpected (since older individuals will have a reduced FVCand a reduced FEV
1FVC ratio) Also recently results from
Eurostat [40] demonstrated that respiratory diseases such asbronchitis and asthma affect mainly older people as almost
90 of EU-28 deaths from these diseases occur among thoseaged 65 and aboveMoreover this report presents a standard-ized death rate from diseases of the respiratory system of atleast 150 deaths per 100 000 inhabitants the highest deathrates were observed in two Portuguese regions the volcanicislands ofMadeira (2946 deaths per 100 000 inhabitants) andAzores (1958 deaths per 100 000 inhabitants) the rest of thePortuguese territory (mainland) presented a death rate below150 deaths per 100 000 inhabitants therefore the observedresults are in accordance with this general overview
Regarding asthma there might be a significant overlapwith COPD since both are characterized by an underlyingairway inflammation although the structural and patho-physiologic findings in both diseases can be usually differ-entiated [41] According to the Global Initiative for ChronicObstructive Lung Diseases [42] in individuals with chronicrespiratory symptoms and fixed airflow limitation it isdifficult to differentiate asthma from COPD However thereis epidemiological evidence that long-standing asthma canlead to fixed airflow limitation [43] which increases thefrequency of asthma attacks [44]
Fatigue is considered the secondmost common symptomof COPD after breathlessness [45] The increased level offatigue found in patients with COPD is associated with anincrease in the severity of lung impairment and a reductionin exercise tolerance Symptoms of fatigue can be physicaland mental such as lack of energy or poor concentrationBaghai-Ravary et al [46] and Breslin et al [47] found arelationship between fatigue and COPD which persists atCOPD exacerbations Since COPD was observed mainlyin elderly people that have diminished lung function andtherefore a reduction in health status fatigue was expectedto be associated with COPD
It is well established that tobacco is the most importantcausative factor for COPDwith individual susceptibility con-tinuously interacting synergistically with other risk factors[48] such as age According to Lundback et al [49] lifelongsmoking increases the chance of developing COPD andthus about 50 of the smokers eventually develop COPDduring their lifetime However according to GOLD [42]other risk factors of COPD include exposure to air pollutionsecondhand smoke and occupational dusts and chemicalsheredity a history of childhood respiratory infections andsocioeconomic status In the present study air pollution byhydrothermal volcanism was proven to be a risk factor inCOPD exacerbation
It is well known that air pollution can perpetuate achronic inflammatory process that potentially leads to lungdiseases [31] However the majority of studies regard airpollutants of anthropogenic origin such as PM
10 NO2 SO2
and O3[50 51] while only few studies were developed
in areas with volcanic activity and associate volcanogenicpollutants with human airway diseases [7 52] Longo andYang [52] and Iwasawa et al [8] reported a higher risk of acutebronchitis across the lifespan in humans exposed to sulfurousvolcanic air pollution Furthermore in 2013 Camarinhoet al [22] showed that noneruptive active volcanism isassociated with increased lung injury in mice Thus it is notunexpected to observe an increase in the exacerbation of
8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

2 BioMed Research International
(a)
(b)
60∘W 50
∘W 40∘W 30
∘W 20∘W 10
∘W 0∘
10∘E
40∘N
40∘N 30
∘N
20∘N
38∘N
32∘W 30
∘W 28∘W 26
∘W 24∘W
Sete CidadesVolcano
Ponta Delgadacity
FogoVolcano
Ribeira Quentevillage
FurnasVolcano
Figure 1 (a) Location map of the Azores archipelago and (b) Sao Miguel Island The places represented on the map correspond to the twostudied areas (Ponta Delgada and Ribeira Quente)
oxygen respiration [15] Previous studies [13] showed thatCO2is released permanently to the atmosphere from soils
in volcanic areas not only during eruptive periods but alsoduring quiescent periods of activity Considering that CO
2
released by soils may enter the buildings through pipescracks in the floor andor the contact betweenfloor andwallsit is considered important to assess the CO
2flux in buildings
Carbon dioxide level is usually greater inside a building thanoutside and it can act as an indicator of ventilation efficiencyshowing whether the supply of outside air is sufficient todilute indoor air contaminants [16] According toWHO [17]indoor air pollution is responsible for 27 of the diseases
worldwide such effects of indoor air pollution are par-ticularly highlighted in studies regarding the occupationalexposure as it was shown in the reviewmade by Balmes et al[18] that estimated that 15 of COPD was attributable to theair quality at the workplace
Furnas and Ribeira Quente are two villages locatedrespectively inside the caldera and in the south flank ofFurnas active volcano where the ground gas emissions thatcharacterize the diffuse degassing areas occur permanentlyand thus inhabitants of such areas are often exposed toelevated concentrations of CO
2from volcanic origin [14]
Previous studies evidenced that Furnas inhabitants have
BioMed Research International 3
Table 1 Description of the study populations (study and reference groups) (mean plusmn SE for continuous variables or n () for categoricalvariables)
Reference group(Ponta Delgada 119899 = 359)
Study group(Ribeira Quente 119899 = 146) P valuea
General characteristicsAge (years) 413 plusmn 127 398 plusmn 112 451 plusmn 153 0001
Age gt41b 234 (463) 152 (423) 82 (561) 0005Gender male 207 (409) 155 (431) 52 (356) 0117BMI (kgm2) 261 plusmn 44 257 plusmn 39 271 plusmn 54 0006
BMI gt26c 213 (422) 141 (393) 72 (493) 0041Smoking status
Smoker 163 (322) 135 (376) 28 (191) lt0001Previous smoker 91 (18) 69 (192) 22 (15) 0271
Easy fatigue yes 116 (23) 40 (111) 76 (52) lt0001Asthma yes 43 (85) 29 (8) 14 (96) 0581Occupation
White collar 135 (267) 122 (34) 13 (89) lt0001Blue collar 256 (507) 233 (65) 23 (158) lt0001Other 114 (226) 4 (1) 110 (753) lt0001
StudyFEV1 predicted
d 885 plusmn 204 925 plusmn 166 786 plusmn 252 0001FVC predicted 966 plusmn 192 988 plusmn 15 911 plusmn 262 lt0001FEV1FVC predicted 918 plusmn 142 938 plusmn 117 87 plusmn 181 lt0001Lung function
Restriction yes 26 (51) 11 (3) 15 (102) 0001COPD yes 92 (182) 43 (119) 49 (336) lt0001
CO2 flux gm2de 1536 508 lt0001
aP value comparing reference and study groups by Mann-Whitney for continuous variables and by 1205942 for categorical variablesbCut-off defined according to the mean value (ie 413 years) of the observed age distribution in the whole populationcCut-off defined according to the mean value (ie 261 BMI) of the observed BMI distribution in the whole populationdPredicted values from the National Health and Nutrition Examination Survey CohorteCO2 flux is expressed in mean
a high incidence of chronic bronchitis and of some cancertypes (eg lip oral cavity and pharynx) [19 20] and a higherrisk of DNA damage in human buccal epithelial cells [21]Moreover a very recent study by Camarinho et al [22]showed that chronic exposure to volcanogenic air pollutantscauses lung injury in wild mice However to our knowledgeup to date no study was carried out to assess the associationbetween volcanogenic air pollution by soil diffuse degassing(DDS) and the risk of development of respiratory defectsTherefore the present study was carried out to evaluatewhether chronic exposure to permanent volcanogenic airpollution is a risk factor for human restrictive and obstructive(COPD) respiratory defects
2 Methods
21 Study Population To perform this study two areas wereselected an area with no secondary manifestations of vol-canism therefore a nonhydrothermal area (Ponta Delgada)and an area where volcanic activity is marked by active fum-arolic fields and degassing soils (hydrothermal area) (Ribeira
Quente) A diagnosis campaign was established for eval-uation of pulmonary function by spirometry tests for theinhabitants of both areas Spirometry tests were carried outin either the participantsrsquo workplaces or their homes Astandard questionnaire was applied to each individual thatvolunteered to participate Medical history data for respira-tory symptoms were taken using a standard questionnairemodified from a standardized respiratory symptomquestion-naire fromAmericanThoracic Society (ATS) [23] and BritishMedical Research Councilrsquos Committee [24] Each personwas interviewed about their age height weight educationoccupation smoking habits (smoking of cigarettes andoruse of smokeless tobacco) amount of cigarettes smokeddayfatigue and general respiratory health status where asthmawas defined by a positive response to ldquoDid any doctordiagnose you with asthmardquo
The study group consisted of 146 participants (94 womenand 52 men) residents in Ribeira Quente village (Table 1)Ribeira Quente village has 767 inhabitants [25] 148 childrenand 619 adults (298 women and 321 men) therefore the par-ticipation rate was 263 This village is located on the south
4 BioMed Research International
flank of Furnas Volcano (Sao Miguel Island) (Figure 1(b))in an important diffuse degassing structure (DDS) about 98of buildings in this village are placed above anomalous soilCO2degassing with volcanic-hydrothermal origin [14 26]
In addition several fumaroles may be found along RibeiraQuente stream and dispersed in the village [13]Thus RibeiraQuente inhabitants are chronically exposed to gases ofvolcanic origin particularly from soil diffuse degassing Evenif no indoormeasurements were performed concomitantly tothe diagnosis tests previous works showed that in the diffusedegassing structures indoor CO
2is anomalously high and
can reach lethal values during extreme weather events [13]Permanent release of gases from the soils increases the indoorCO2concentrations independently of the anthropogenic
contributionThe reference group comprised 359 individuals (204
women and 155men)working in downtown of PontaDelgadacity (Table 1) Ponta Delgadarsquos downtown has 7818 adultworkers [25] therefore the participation rate was 45Ponta Delgada is located in the south side of Sao MiguelIsland (Azores Portugal Figure 1(b)) in the Regiao dos PicosVolcanic Complex a basaltic rift zone located between SeteCidades and Fogo Volcanoes where no manifestations ofvolcanism have been identified [11]
The Ethics Board of Divino Espirito Santo Hospital(Ponta Delgada Azores Portugal) approved the study Allindividuals signed a written informed consent in compliancewith the Helsinki Declaration and Oviedo Convention toparticipate in this study Table 1 summarizes the demographiccharacteristics and main lifestyle habits of the studied popu-lations Only individuals resident for more than five years ineach locality were considered in this study
22 Spirometry Tests The forced expiratory volume in onesecond (FEV
1) and the forced vital capacity (FVC) values
were obtained by spirometry in all participants Spirometrytests were conducted with the participants in an up positionwearing a nose clip and a disposable mouth piece usingthe EasyOne automated portable spirometer (ndd ZurichSwitzerland) which meets ATSERS spirometry standards[27] and is equipped with software that checks for unac-ceptable maneuvers and compares the measured values withreference tables Standardized operating procedures wereimplemented and controlled Participants performed three tofive attempts to provide at least three technically acceptablemaneuvers following the criteria recommended by the ATS[28] and the guidelines of the European Respiratory Society[27] Postbronchodilator tests were not applied
Spirometry datawere classified categorically as being con-sistent with either a normal pulmonary function a restrictivedefect or an obstructive defect Spirometric detection ofrestriction was considered in all subjects with normal FEV
1
FVC with FVC lt 80 predicted and FEV1FVC lt 70 was
used as a fixed cut-point for obstruction (COPD) accordingto the third United States National Health and NutritionExamination Survey (NHANES III) for adult CaucasiansAccording to the GOLD guidelines COPD was furtherclassified in the following ranks given by the spirometer
output mild (FEV1ge 80) moderate (FEV
150ndash79) and
severe (FEV130ndash49)
23 Exposure Assessment to Volcanogenic Air Pollution byDDS Carbon dioxide degassing maps may be useful for vol-canicseismic monitoring purposes as they represent a refer-ence for future variations on the state of activity of the volcano[14]
Measurements of soil CO2released by soil degassing in
Ribeira Quente village were carried out recently by Viveiroset al [14 26] The surveys were made using portable instru-ments that perform measurements based on the accumula-tion chamber method [29] Almost all buildings (about 98)in Ribeira Quente village are placed in an anomalous highCO2degassing zone (DDS) with soil CO
2fluxes that can
reach values higher than 25000 gm2d [14] Considering thatCO2released by soils may enter the buildings (eg through
pipes cracks in the floor andor the contact between floorandwalls) CO
2degassingmaps produced for Ribeira Quente
village [14 26] were used to attribute a CO2flux value to each
building Even if no indoor measurements were performedthe CO
2released from soils is positively correlated with the
indoor CO2concentrations [13] so measurements applied
outside the buildings are indirectly representative of the CO2
concentrations that can be found indoors [13] Sporadic soilCO2flux measurements were performed at Ponta Delgada in
the areas surrounding the buildings occupied by individualsfrom the reference group The 68 measurements performedshowed that CO
2flux values were lower than 25 gm2d and
thus representative of biogenic origin andwithout hydrother-mal contribution
24 Statistical Analysis Pearson Chi-Square test was used tocompare restrictions and COPD prevalence between individ-uals inhabiting the environment with volcanic degassing andindividuals from the reference group To estimate the asso-ciation between chronic exposure to an environment withvolcanic air pollution and restrictive and obstructive defects(no versus yes) odds ratio (OR) and 95 confidence intervals(95 CIs) were calculated using a binary logistic regressionmodel adjusting for age gender (male versus female) fatigue(yes versus no) and smoking status (yes versus no)
To estimate the association between chronic exposure toan environment with volcanic air pollution and the increasein the severity COPD odds ratio (OR) and 95 confidenceintervals (95 CIs) were calculated using an ordinal logisticregression model adjusting for age fatigue (yes versus no)asthma (yes versus no) and smoking status (yes versus no)The occurrence of obstructions was graded on scales accord-ing to their occurrence and severity 1 without obstructionand 2 to 4 with obstruction from the least severe (2) to themost severe (4)
Mann-Whitney 119880 test was used to compare soil CO2
fluxes released by diffuse degassing between the reference andthe study group
All statistical analysis was performed using IBM SPSSStatistics 200 for Windows [30] and the level of statisticalsignificance was set at 119875 le 005
BioMed Research International 5
Table 2 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing (DDS) andrestrictive lung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 1097Prob gt chi2 = 005
Parameter 119899 () OR (95 CI)a P valueAge 099 (096ndash102) 0933Gender
Male 207 (41) 116 (050ndash269) 0729Female 298 (59) 100
Easy fatigueYes 116 (23) 062 (023ndash167) 0349No 389 (77) 100
Smoking statusSmoker 163 (323) 094 (036ndash242) 0892Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 437 (178ndash1069) 0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
3 Results
The general characteristics of the study populations arepresented in Table 1The study group has an older populationand a higher BMI than the reference one (561 versus 423of individuals with more than 41 years and 271 kgm2 versus257 kgm2 resp) On the other hand the reference group hasa higher percentage of smokers than the study group (376versus 191)
Soil CO2flux was significantly different (119875 lt 0001)
between the studied areas (Table 1) According to criteriafor diffuse degassing susceptibility areas defined by Viveiroset al [14] all the analyzed buildings in Ponta Delgada arelocated in low susceptibility areas (CO
2flux lt 25 gm2d)
while in Ribeira Quente 19 of the buildings were locatedin moderate susceptibility areas (soil CO
2flux between
25 gm2d and 50 gm2d) and the remaining 981 were ina high susceptibility area (soil CO
2flux ge 50 gm2d) (Sup-
plementary Material 1 in Supplementary Material availableonline at httpdxdoiorg1011552015326794)
31 Prevalence of Restrictive and Obstructive RespiratoryDefects The prevalence of restrictions in the study groupwas significantly higher than in the reference group (102versus 30 resp 119875 = 0001) Similarly the prevalence ofCOPD was significantly higher in the study group than inthe reference one (336 versus 119 resp 119875 lt 0001)(Figure 2) The prevalence of more severe obstructions wasalso higher in the study group compared to the reference one(mild 157 versus 44 moderate 68 versus 22 and severe47 versus 0 resp)
32 Restrictive or Obstructive Respiratory Defects and Expo-sure to Volcanogenic Air Pollution by DDS Exposure to
0102030405060708090
Normal Restriction COPD
Prev
alen
ce (
)
Reference groupStudy group
lowastlowast lowast
lowast
Figure 2 Proportion () of individuals with obstructive andrestrictive airway diseases in study (Ribeira Quente) and reference(Ponta Delgada) groups lowastsignificantly different at 119875 lt 005
volcanogenic air pollution by DDSwas a significant predictorof the prevalence of respiratory restrictions and of COPDexacerbation in the multivariate analysis After adjustmentfor age gender fatigue and smoking status a higher preva-lence of respiratory restrictions was found associated withexposure to volcanogenic air pollution by DDS (OR = 4495 CI 178ndash1069 119875 = 0001) (Table 2) Also after theadjustment for the same factors a higher prevalence ofrespiratory obstructions was found associated with exposureto the volcanic environment (OR = 28 95 CI 160ndash499)(Table 3) Exacerbation in COPD severity was also foundsignificantly associated with exposure to volcanogenic airpollution by DDS (OR = 32 95 CI 182ndash558 119875 lt 0001)(Table 4)
The analyzed confounding factors did not show anysignificant association with respiratory restrictions (Table 2)but respiratory obstructions were significantly associated
6 BioMed Research International
Table 3 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and obstructivelung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 6080Prob gt chi2 = lt0001
Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (105ndash328) 0033No 389 (77) 100
GenderMale 207 (41) 066 (039ndash111) 0123Female 298 (59) 100
Smoking statusSmoker 163 (323) 234 (135ndash406) 0002Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 283 (160ndash499) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
Table 4 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and COPDexacerbation
Ordinal logistic regressionNumber of obs 505LR chi2(5) = 7019
Prob gt chi2 = lt0001Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (100ndash324) 0046No 389 (77) 100
AsthmaYes 43 (85) 225 (105ndash482) 0037No 462 (915) 100
Smoking statusSmoker 163 (323) 211 (125ndash356) 0005Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 319 (182ndash558) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
with age fatigue and smoking status (Table 3) The increasein COPD severity was significantly associated with asthmaand the abovementioned factors (Table 4)
4 Discussion
The association between exposure to air pollution andadverse respiratory effects has been widely demonstrated[31 32] Such association is usually related to anthropogenicair pollution while for volcanogenic pollution there are
much fewer studies Volcanoes and volcanic manifestationssuch as fumaroles and hot and cold CO
2-rich springs as
well as degassing soils release into the environment metalshazardous aerosols and gases that daily affect the quality ofthe environment and the health of human populations [33]
The measurements of CO2flux revealed that the study
group (from the hydrothermal area) is chronically exposed toelevated volcanogenic air pollution by soil diffuse degassingcompared to the reference group (average values are 508 gm2d (asymp3573 ppms) versus 1536 gm2d (asymp108 ppms)
BioMed Research International 7
resp) Carbon dioxide levels are described to be usuallygreater inside a building than outside [34 35] therefore thesepopulations are much probably subjected to higher levels ofindoor CO
2than the presented values Also independently
of the biological CO2contribution the hydrothermal CO
2
emission is permanent and thus the level of CO2in the
Ribeira Quente buildings must be always higher than theldquonormalrdquo values and sporadically reach anomalous highvalues as recognized in previous works only due to meteo-rological changes [13] The threshold limit value for 8 h timeweighted-average exposures to CO
2is 5000 ppm (WHO)
and possibly the average CO2concentrations encountered
in the buildings are below this limit and are not expectedto cause health symptoms such as headaches fatigue andeye and throat irritation However the consequences ofthe permanent presence of indoor CO
2in concentrations
higher than the outdoor environment are still far from beingunderstood and may eventually lead to some stress effect inthe organisms that needs to be better studied In additionthe CO
2emission may be also associated with other volcanic
emissions as it is the case of the radioactive gas radon Themeasurements performed showed that the study group ischronically exposed to elevated volcanogenic air pollutionnamely high CO
2soil diffuse degassing high concentrations
of CO2can cause headaches due to hypercapnia and the
decrease of O2in the bloodstream [36] When these two
events combine the body responds by increasing blood flowto the brain by dilating the blood vessels resulting in pain[36] A significant association was found between restrictiverespiratory defects and the exposure to volcanogenic airpollution by DDS measured as 44 times higher in theinhabitants of Ribeira Quente (study group) when comparedto the reference one A significant association was also foundbetween obstructive respiratory defects and exposure tovolcanogenic air pollution by DDS measured as 28 timeshigher in the study group None of the analyzed confoundingfactors (age gender fatigue and smoking status) was signifi-cantly associated with respiratory restriction but apart fromgender all confounding factors were positively associatedwith respiratory obstructions
Results also showed significant associations between theincrease in the severity of COPD and the exposure to soildiffuse degassing in the study group when compared to thereference one given as 32 times higher in Ribeira Quenteinhabitants (study group) Age asthma fatigue and smokingstatus were also significantly associated with the increase inCOPD severity
Age and smoking habits are well associated with COPDprevalence [37 38] According to our results the classificationof subjects who are at risk is relevant in middle-aged andelderly persons (ie gt 41 years old) individuals with asthmaand smokers Aging affects the structure function andcontrol of the respiratory system according to Stanojevic etal [39] both FEV
1and FVC decrease with age and thus
the observed increase in COPD associated with age wasexpected (since older individuals will have a reduced FVCand a reduced FEV
1FVC ratio) Also recently results from
Eurostat [40] demonstrated that respiratory diseases such asbronchitis and asthma affect mainly older people as almost
90 of EU-28 deaths from these diseases occur among thoseaged 65 and aboveMoreover this report presents a standard-ized death rate from diseases of the respiratory system of atleast 150 deaths per 100 000 inhabitants the highest deathrates were observed in two Portuguese regions the volcanicislands ofMadeira (2946 deaths per 100 000 inhabitants) andAzores (1958 deaths per 100 000 inhabitants) the rest of thePortuguese territory (mainland) presented a death rate below150 deaths per 100 000 inhabitants therefore the observedresults are in accordance with this general overview
Regarding asthma there might be a significant overlapwith COPD since both are characterized by an underlyingairway inflammation although the structural and patho-physiologic findings in both diseases can be usually differ-entiated [41] According to the Global Initiative for ChronicObstructive Lung Diseases [42] in individuals with chronicrespiratory symptoms and fixed airflow limitation it isdifficult to differentiate asthma from COPD However thereis epidemiological evidence that long-standing asthma canlead to fixed airflow limitation [43] which increases thefrequency of asthma attacks [44]
Fatigue is considered the secondmost common symptomof COPD after breathlessness [45] The increased level offatigue found in patients with COPD is associated with anincrease in the severity of lung impairment and a reductionin exercise tolerance Symptoms of fatigue can be physicaland mental such as lack of energy or poor concentrationBaghai-Ravary et al [46] and Breslin et al [47] found arelationship between fatigue and COPD which persists atCOPD exacerbations Since COPD was observed mainlyin elderly people that have diminished lung function andtherefore a reduction in health status fatigue was expectedto be associated with COPD
It is well established that tobacco is the most importantcausative factor for COPDwith individual susceptibility con-tinuously interacting synergistically with other risk factors[48] such as age According to Lundback et al [49] lifelongsmoking increases the chance of developing COPD andthus about 50 of the smokers eventually develop COPDduring their lifetime However according to GOLD [42]other risk factors of COPD include exposure to air pollutionsecondhand smoke and occupational dusts and chemicalsheredity a history of childhood respiratory infections andsocioeconomic status In the present study air pollution byhydrothermal volcanism was proven to be a risk factor inCOPD exacerbation
It is well known that air pollution can perpetuate achronic inflammatory process that potentially leads to lungdiseases [31] However the majority of studies regard airpollutants of anthropogenic origin such as PM
10 NO2 SO2
and O3[50 51] while only few studies were developed
in areas with volcanic activity and associate volcanogenicpollutants with human airway diseases [7 52] Longo andYang [52] and Iwasawa et al [8] reported a higher risk of acutebronchitis across the lifespan in humans exposed to sulfurousvolcanic air pollution Furthermore in 2013 Camarinhoet al [22] showed that noneruptive active volcanism isassociated with increased lung injury in mice Thus it is notunexpected to observe an increase in the exacerbation of
8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 3
Table 1 Description of the study populations (study and reference groups) (mean plusmn SE for continuous variables or n () for categoricalvariables)
Reference group(Ponta Delgada 119899 = 359)
Study group(Ribeira Quente 119899 = 146) P valuea
General characteristicsAge (years) 413 plusmn 127 398 plusmn 112 451 plusmn 153 0001
Age gt41b 234 (463) 152 (423) 82 (561) 0005Gender male 207 (409) 155 (431) 52 (356) 0117BMI (kgm2) 261 plusmn 44 257 plusmn 39 271 plusmn 54 0006
BMI gt26c 213 (422) 141 (393) 72 (493) 0041Smoking status
Smoker 163 (322) 135 (376) 28 (191) lt0001Previous smoker 91 (18) 69 (192) 22 (15) 0271
Easy fatigue yes 116 (23) 40 (111) 76 (52) lt0001Asthma yes 43 (85) 29 (8) 14 (96) 0581Occupation
White collar 135 (267) 122 (34) 13 (89) lt0001Blue collar 256 (507) 233 (65) 23 (158) lt0001Other 114 (226) 4 (1) 110 (753) lt0001
StudyFEV1 predicted
d 885 plusmn 204 925 plusmn 166 786 plusmn 252 0001FVC predicted 966 plusmn 192 988 plusmn 15 911 plusmn 262 lt0001FEV1FVC predicted 918 plusmn 142 938 plusmn 117 87 plusmn 181 lt0001Lung function
Restriction yes 26 (51) 11 (3) 15 (102) 0001COPD yes 92 (182) 43 (119) 49 (336) lt0001
CO2 flux gm2de 1536 508 lt0001
aP value comparing reference and study groups by Mann-Whitney for continuous variables and by 1205942 for categorical variablesbCut-off defined according to the mean value (ie 413 years) of the observed age distribution in the whole populationcCut-off defined according to the mean value (ie 261 BMI) of the observed BMI distribution in the whole populationdPredicted values from the National Health and Nutrition Examination Survey CohorteCO2 flux is expressed in mean
a high incidence of chronic bronchitis and of some cancertypes (eg lip oral cavity and pharynx) [19 20] and a higherrisk of DNA damage in human buccal epithelial cells [21]Moreover a very recent study by Camarinho et al [22]showed that chronic exposure to volcanogenic air pollutantscauses lung injury in wild mice However to our knowledgeup to date no study was carried out to assess the associationbetween volcanogenic air pollution by soil diffuse degassing(DDS) and the risk of development of respiratory defectsTherefore the present study was carried out to evaluatewhether chronic exposure to permanent volcanogenic airpollution is a risk factor for human restrictive and obstructive(COPD) respiratory defects
2 Methods
21 Study Population To perform this study two areas wereselected an area with no secondary manifestations of vol-canism therefore a nonhydrothermal area (Ponta Delgada)and an area where volcanic activity is marked by active fum-arolic fields and degassing soils (hydrothermal area) (Ribeira
Quente) A diagnosis campaign was established for eval-uation of pulmonary function by spirometry tests for theinhabitants of both areas Spirometry tests were carried outin either the participantsrsquo workplaces or their homes Astandard questionnaire was applied to each individual thatvolunteered to participate Medical history data for respira-tory symptoms were taken using a standard questionnairemodified from a standardized respiratory symptomquestion-naire fromAmericanThoracic Society (ATS) [23] and BritishMedical Research Councilrsquos Committee [24] Each personwas interviewed about their age height weight educationoccupation smoking habits (smoking of cigarettes andoruse of smokeless tobacco) amount of cigarettes smokeddayfatigue and general respiratory health status where asthmawas defined by a positive response to ldquoDid any doctordiagnose you with asthmardquo
The study group consisted of 146 participants (94 womenand 52 men) residents in Ribeira Quente village (Table 1)Ribeira Quente village has 767 inhabitants [25] 148 childrenand 619 adults (298 women and 321 men) therefore the par-ticipation rate was 263 This village is located on the south
4 BioMed Research International
flank of Furnas Volcano (Sao Miguel Island) (Figure 1(b))in an important diffuse degassing structure (DDS) about 98of buildings in this village are placed above anomalous soilCO2degassing with volcanic-hydrothermal origin [14 26]
In addition several fumaroles may be found along RibeiraQuente stream and dispersed in the village [13]Thus RibeiraQuente inhabitants are chronically exposed to gases ofvolcanic origin particularly from soil diffuse degassing Evenif no indoormeasurements were performed concomitantly tothe diagnosis tests previous works showed that in the diffusedegassing structures indoor CO
2is anomalously high and
can reach lethal values during extreme weather events [13]Permanent release of gases from the soils increases the indoorCO2concentrations independently of the anthropogenic
contributionThe reference group comprised 359 individuals (204
women and 155men)working in downtown of PontaDelgadacity (Table 1) Ponta Delgadarsquos downtown has 7818 adultworkers [25] therefore the participation rate was 45Ponta Delgada is located in the south side of Sao MiguelIsland (Azores Portugal Figure 1(b)) in the Regiao dos PicosVolcanic Complex a basaltic rift zone located between SeteCidades and Fogo Volcanoes where no manifestations ofvolcanism have been identified [11]
The Ethics Board of Divino Espirito Santo Hospital(Ponta Delgada Azores Portugal) approved the study Allindividuals signed a written informed consent in compliancewith the Helsinki Declaration and Oviedo Convention toparticipate in this study Table 1 summarizes the demographiccharacteristics and main lifestyle habits of the studied popu-lations Only individuals resident for more than five years ineach locality were considered in this study
22 Spirometry Tests The forced expiratory volume in onesecond (FEV
1) and the forced vital capacity (FVC) values
were obtained by spirometry in all participants Spirometrytests were conducted with the participants in an up positionwearing a nose clip and a disposable mouth piece usingthe EasyOne automated portable spirometer (ndd ZurichSwitzerland) which meets ATSERS spirometry standards[27] and is equipped with software that checks for unac-ceptable maneuvers and compares the measured values withreference tables Standardized operating procedures wereimplemented and controlled Participants performed three tofive attempts to provide at least three technically acceptablemaneuvers following the criteria recommended by the ATS[28] and the guidelines of the European Respiratory Society[27] Postbronchodilator tests were not applied
Spirometry datawere classified categorically as being con-sistent with either a normal pulmonary function a restrictivedefect or an obstructive defect Spirometric detection ofrestriction was considered in all subjects with normal FEV
1
FVC with FVC lt 80 predicted and FEV1FVC lt 70 was
used as a fixed cut-point for obstruction (COPD) accordingto the third United States National Health and NutritionExamination Survey (NHANES III) for adult CaucasiansAccording to the GOLD guidelines COPD was furtherclassified in the following ranks given by the spirometer
output mild (FEV1ge 80) moderate (FEV
150ndash79) and
severe (FEV130ndash49)
23 Exposure Assessment to Volcanogenic Air Pollution byDDS Carbon dioxide degassing maps may be useful for vol-canicseismic monitoring purposes as they represent a refer-ence for future variations on the state of activity of the volcano[14]
Measurements of soil CO2released by soil degassing in
Ribeira Quente village were carried out recently by Viveiroset al [14 26] The surveys were made using portable instru-ments that perform measurements based on the accumula-tion chamber method [29] Almost all buildings (about 98)in Ribeira Quente village are placed in an anomalous highCO2degassing zone (DDS) with soil CO
2fluxes that can
reach values higher than 25000 gm2d [14] Considering thatCO2released by soils may enter the buildings (eg through
pipes cracks in the floor andor the contact between floorandwalls) CO
2degassingmaps produced for Ribeira Quente
village [14 26] were used to attribute a CO2flux value to each
building Even if no indoor measurements were performedthe CO
2released from soils is positively correlated with the
indoor CO2concentrations [13] so measurements applied
outside the buildings are indirectly representative of the CO2
concentrations that can be found indoors [13] Sporadic soilCO2flux measurements were performed at Ponta Delgada in
the areas surrounding the buildings occupied by individualsfrom the reference group The 68 measurements performedshowed that CO
2flux values were lower than 25 gm2d and
thus representative of biogenic origin andwithout hydrother-mal contribution
24 Statistical Analysis Pearson Chi-Square test was used tocompare restrictions and COPD prevalence between individ-uals inhabiting the environment with volcanic degassing andindividuals from the reference group To estimate the asso-ciation between chronic exposure to an environment withvolcanic air pollution and restrictive and obstructive defects(no versus yes) odds ratio (OR) and 95 confidence intervals(95 CIs) were calculated using a binary logistic regressionmodel adjusting for age gender (male versus female) fatigue(yes versus no) and smoking status (yes versus no)
To estimate the association between chronic exposure toan environment with volcanic air pollution and the increasein the severity COPD odds ratio (OR) and 95 confidenceintervals (95 CIs) were calculated using an ordinal logisticregression model adjusting for age fatigue (yes versus no)asthma (yes versus no) and smoking status (yes versus no)The occurrence of obstructions was graded on scales accord-ing to their occurrence and severity 1 without obstructionand 2 to 4 with obstruction from the least severe (2) to themost severe (4)
Mann-Whitney 119880 test was used to compare soil CO2
fluxes released by diffuse degassing between the reference andthe study group
All statistical analysis was performed using IBM SPSSStatistics 200 for Windows [30] and the level of statisticalsignificance was set at 119875 le 005
BioMed Research International 5
Table 2 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing (DDS) andrestrictive lung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 1097Prob gt chi2 = 005
Parameter 119899 () OR (95 CI)a P valueAge 099 (096ndash102) 0933Gender
Male 207 (41) 116 (050ndash269) 0729Female 298 (59) 100
Easy fatigueYes 116 (23) 062 (023ndash167) 0349No 389 (77) 100
Smoking statusSmoker 163 (323) 094 (036ndash242) 0892Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 437 (178ndash1069) 0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
3 Results
The general characteristics of the study populations arepresented in Table 1The study group has an older populationand a higher BMI than the reference one (561 versus 423of individuals with more than 41 years and 271 kgm2 versus257 kgm2 resp) On the other hand the reference group hasa higher percentage of smokers than the study group (376versus 191)
Soil CO2flux was significantly different (119875 lt 0001)
between the studied areas (Table 1) According to criteriafor diffuse degassing susceptibility areas defined by Viveiroset al [14] all the analyzed buildings in Ponta Delgada arelocated in low susceptibility areas (CO
2flux lt 25 gm2d)
while in Ribeira Quente 19 of the buildings were locatedin moderate susceptibility areas (soil CO
2flux between
25 gm2d and 50 gm2d) and the remaining 981 were ina high susceptibility area (soil CO
2flux ge 50 gm2d) (Sup-
plementary Material 1 in Supplementary Material availableonline at httpdxdoiorg1011552015326794)
31 Prevalence of Restrictive and Obstructive RespiratoryDefects The prevalence of restrictions in the study groupwas significantly higher than in the reference group (102versus 30 resp 119875 = 0001) Similarly the prevalence ofCOPD was significantly higher in the study group than inthe reference one (336 versus 119 resp 119875 lt 0001)(Figure 2) The prevalence of more severe obstructions wasalso higher in the study group compared to the reference one(mild 157 versus 44 moderate 68 versus 22 and severe47 versus 0 resp)
32 Restrictive or Obstructive Respiratory Defects and Expo-sure to Volcanogenic Air Pollution by DDS Exposure to
0102030405060708090
Normal Restriction COPD
Prev
alen
ce (
)
Reference groupStudy group
lowastlowast lowast
lowast
Figure 2 Proportion () of individuals with obstructive andrestrictive airway diseases in study (Ribeira Quente) and reference(Ponta Delgada) groups lowastsignificantly different at 119875 lt 005
volcanogenic air pollution by DDSwas a significant predictorof the prevalence of respiratory restrictions and of COPDexacerbation in the multivariate analysis After adjustmentfor age gender fatigue and smoking status a higher preva-lence of respiratory restrictions was found associated withexposure to volcanogenic air pollution by DDS (OR = 4495 CI 178ndash1069 119875 = 0001) (Table 2) Also after theadjustment for the same factors a higher prevalence ofrespiratory obstructions was found associated with exposureto the volcanic environment (OR = 28 95 CI 160ndash499)(Table 3) Exacerbation in COPD severity was also foundsignificantly associated with exposure to volcanogenic airpollution by DDS (OR = 32 95 CI 182ndash558 119875 lt 0001)(Table 4)
The analyzed confounding factors did not show anysignificant association with respiratory restrictions (Table 2)but respiratory obstructions were significantly associated
6 BioMed Research International
Table 3 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and obstructivelung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 6080Prob gt chi2 = lt0001
Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (105ndash328) 0033No 389 (77) 100
GenderMale 207 (41) 066 (039ndash111) 0123Female 298 (59) 100
Smoking statusSmoker 163 (323) 234 (135ndash406) 0002Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 283 (160ndash499) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
Table 4 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and COPDexacerbation
Ordinal logistic regressionNumber of obs 505LR chi2(5) = 7019
Prob gt chi2 = lt0001Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (100ndash324) 0046No 389 (77) 100
AsthmaYes 43 (85) 225 (105ndash482) 0037No 462 (915) 100
Smoking statusSmoker 163 (323) 211 (125ndash356) 0005Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 319 (182ndash558) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
with age fatigue and smoking status (Table 3) The increasein COPD severity was significantly associated with asthmaand the abovementioned factors (Table 4)
4 Discussion
The association between exposure to air pollution andadverse respiratory effects has been widely demonstrated[31 32] Such association is usually related to anthropogenicair pollution while for volcanogenic pollution there are
much fewer studies Volcanoes and volcanic manifestationssuch as fumaroles and hot and cold CO
2-rich springs as
well as degassing soils release into the environment metalshazardous aerosols and gases that daily affect the quality ofthe environment and the health of human populations [33]
The measurements of CO2flux revealed that the study
group (from the hydrothermal area) is chronically exposed toelevated volcanogenic air pollution by soil diffuse degassingcompared to the reference group (average values are 508 gm2d (asymp3573 ppms) versus 1536 gm2d (asymp108 ppms)
BioMed Research International 7
resp) Carbon dioxide levels are described to be usuallygreater inside a building than outside [34 35] therefore thesepopulations are much probably subjected to higher levels ofindoor CO
2than the presented values Also independently
of the biological CO2contribution the hydrothermal CO
2
emission is permanent and thus the level of CO2in the
Ribeira Quente buildings must be always higher than theldquonormalrdquo values and sporadically reach anomalous highvalues as recognized in previous works only due to meteo-rological changes [13] The threshold limit value for 8 h timeweighted-average exposures to CO
2is 5000 ppm (WHO)
and possibly the average CO2concentrations encountered
in the buildings are below this limit and are not expectedto cause health symptoms such as headaches fatigue andeye and throat irritation However the consequences ofthe permanent presence of indoor CO
2in concentrations
higher than the outdoor environment are still far from beingunderstood and may eventually lead to some stress effect inthe organisms that needs to be better studied In additionthe CO
2emission may be also associated with other volcanic
emissions as it is the case of the radioactive gas radon Themeasurements performed showed that the study group ischronically exposed to elevated volcanogenic air pollutionnamely high CO
2soil diffuse degassing high concentrations
of CO2can cause headaches due to hypercapnia and the
decrease of O2in the bloodstream [36] When these two
events combine the body responds by increasing blood flowto the brain by dilating the blood vessels resulting in pain[36] A significant association was found between restrictiverespiratory defects and the exposure to volcanogenic airpollution by DDS measured as 44 times higher in theinhabitants of Ribeira Quente (study group) when comparedto the reference one A significant association was also foundbetween obstructive respiratory defects and exposure tovolcanogenic air pollution by DDS measured as 28 timeshigher in the study group None of the analyzed confoundingfactors (age gender fatigue and smoking status) was signifi-cantly associated with respiratory restriction but apart fromgender all confounding factors were positively associatedwith respiratory obstructions
Results also showed significant associations between theincrease in the severity of COPD and the exposure to soildiffuse degassing in the study group when compared to thereference one given as 32 times higher in Ribeira Quenteinhabitants (study group) Age asthma fatigue and smokingstatus were also significantly associated with the increase inCOPD severity
Age and smoking habits are well associated with COPDprevalence [37 38] According to our results the classificationof subjects who are at risk is relevant in middle-aged andelderly persons (ie gt 41 years old) individuals with asthmaand smokers Aging affects the structure function andcontrol of the respiratory system according to Stanojevic etal [39] both FEV
1and FVC decrease with age and thus
the observed increase in COPD associated with age wasexpected (since older individuals will have a reduced FVCand a reduced FEV
1FVC ratio) Also recently results from
Eurostat [40] demonstrated that respiratory diseases such asbronchitis and asthma affect mainly older people as almost
90 of EU-28 deaths from these diseases occur among thoseaged 65 and aboveMoreover this report presents a standard-ized death rate from diseases of the respiratory system of atleast 150 deaths per 100 000 inhabitants the highest deathrates were observed in two Portuguese regions the volcanicislands ofMadeira (2946 deaths per 100 000 inhabitants) andAzores (1958 deaths per 100 000 inhabitants) the rest of thePortuguese territory (mainland) presented a death rate below150 deaths per 100 000 inhabitants therefore the observedresults are in accordance with this general overview
Regarding asthma there might be a significant overlapwith COPD since both are characterized by an underlyingairway inflammation although the structural and patho-physiologic findings in both diseases can be usually differ-entiated [41] According to the Global Initiative for ChronicObstructive Lung Diseases [42] in individuals with chronicrespiratory symptoms and fixed airflow limitation it isdifficult to differentiate asthma from COPD However thereis epidemiological evidence that long-standing asthma canlead to fixed airflow limitation [43] which increases thefrequency of asthma attacks [44]
Fatigue is considered the secondmost common symptomof COPD after breathlessness [45] The increased level offatigue found in patients with COPD is associated with anincrease in the severity of lung impairment and a reductionin exercise tolerance Symptoms of fatigue can be physicaland mental such as lack of energy or poor concentrationBaghai-Ravary et al [46] and Breslin et al [47] found arelationship between fatigue and COPD which persists atCOPD exacerbations Since COPD was observed mainlyin elderly people that have diminished lung function andtherefore a reduction in health status fatigue was expectedto be associated with COPD
It is well established that tobacco is the most importantcausative factor for COPDwith individual susceptibility con-tinuously interacting synergistically with other risk factors[48] such as age According to Lundback et al [49] lifelongsmoking increases the chance of developing COPD andthus about 50 of the smokers eventually develop COPDduring their lifetime However according to GOLD [42]other risk factors of COPD include exposure to air pollutionsecondhand smoke and occupational dusts and chemicalsheredity a history of childhood respiratory infections andsocioeconomic status In the present study air pollution byhydrothermal volcanism was proven to be a risk factor inCOPD exacerbation
It is well known that air pollution can perpetuate achronic inflammatory process that potentially leads to lungdiseases [31] However the majority of studies regard airpollutants of anthropogenic origin such as PM
10 NO2 SO2
and O3[50 51] while only few studies were developed
in areas with volcanic activity and associate volcanogenicpollutants with human airway diseases [7 52] Longo andYang [52] and Iwasawa et al [8] reported a higher risk of acutebronchitis across the lifespan in humans exposed to sulfurousvolcanic air pollution Furthermore in 2013 Camarinhoet al [22] showed that noneruptive active volcanism isassociated with increased lung injury in mice Thus it is notunexpected to observe an increase in the exacerbation of
8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

4 BioMed Research International
flank of Furnas Volcano (Sao Miguel Island) (Figure 1(b))in an important diffuse degassing structure (DDS) about 98of buildings in this village are placed above anomalous soilCO2degassing with volcanic-hydrothermal origin [14 26]
In addition several fumaroles may be found along RibeiraQuente stream and dispersed in the village [13]Thus RibeiraQuente inhabitants are chronically exposed to gases ofvolcanic origin particularly from soil diffuse degassing Evenif no indoormeasurements were performed concomitantly tothe diagnosis tests previous works showed that in the diffusedegassing structures indoor CO
2is anomalously high and
can reach lethal values during extreme weather events [13]Permanent release of gases from the soils increases the indoorCO2concentrations independently of the anthropogenic
contributionThe reference group comprised 359 individuals (204
women and 155men)working in downtown of PontaDelgadacity (Table 1) Ponta Delgadarsquos downtown has 7818 adultworkers [25] therefore the participation rate was 45Ponta Delgada is located in the south side of Sao MiguelIsland (Azores Portugal Figure 1(b)) in the Regiao dos PicosVolcanic Complex a basaltic rift zone located between SeteCidades and Fogo Volcanoes where no manifestations ofvolcanism have been identified [11]
The Ethics Board of Divino Espirito Santo Hospital(Ponta Delgada Azores Portugal) approved the study Allindividuals signed a written informed consent in compliancewith the Helsinki Declaration and Oviedo Convention toparticipate in this study Table 1 summarizes the demographiccharacteristics and main lifestyle habits of the studied popu-lations Only individuals resident for more than five years ineach locality were considered in this study
22 Spirometry Tests The forced expiratory volume in onesecond (FEV
1) and the forced vital capacity (FVC) values
were obtained by spirometry in all participants Spirometrytests were conducted with the participants in an up positionwearing a nose clip and a disposable mouth piece usingthe EasyOne automated portable spirometer (ndd ZurichSwitzerland) which meets ATSERS spirometry standards[27] and is equipped with software that checks for unac-ceptable maneuvers and compares the measured values withreference tables Standardized operating procedures wereimplemented and controlled Participants performed three tofive attempts to provide at least three technically acceptablemaneuvers following the criteria recommended by the ATS[28] and the guidelines of the European Respiratory Society[27] Postbronchodilator tests were not applied
Spirometry datawere classified categorically as being con-sistent with either a normal pulmonary function a restrictivedefect or an obstructive defect Spirometric detection ofrestriction was considered in all subjects with normal FEV
1
FVC with FVC lt 80 predicted and FEV1FVC lt 70 was
used as a fixed cut-point for obstruction (COPD) accordingto the third United States National Health and NutritionExamination Survey (NHANES III) for adult CaucasiansAccording to the GOLD guidelines COPD was furtherclassified in the following ranks given by the spirometer
output mild (FEV1ge 80) moderate (FEV
150ndash79) and
severe (FEV130ndash49)
23 Exposure Assessment to Volcanogenic Air Pollution byDDS Carbon dioxide degassing maps may be useful for vol-canicseismic monitoring purposes as they represent a refer-ence for future variations on the state of activity of the volcano[14]
Measurements of soil CO2released by soil degassing in
Ribeira Quente village were carried out recently by Viveiroset al [14 26] The surveys were made using portable instru-ments that perform measurements based on the accumula-tion chamber method [29] Almost all buildings (about 98)in Ribeira Quente village are placed in an anomalous highCO2degassing zone (DDS) with soil CO
2fluxes that can
reach values higher than 25000 gm2d [14] Considering thatCO2released by soils may enter the buildings (eg through
pipes cracks in the floor andor the contact between floorandwalls) CO
2degassingmaps produced for Ribeira Quente
village [14 26] were used to attribute a CO2flux value to each
building Even if no indoor measurements were performedthe CO
2released from soils is positively correlated with the
indoor CO2concentrations [13] so measurements applied
outside the buildings are indirectly representative of the CO2
concentrations that can be found indoors [13] Sporadic soilCO2flux measurements were performed at Ponta Delgada in
the areas surrounding the buildings occupied by individualsfrom the reference group The 68 measurements performedshowed that CO
2flux values were lower than 25 gm2d and
thus representative of biogenic origin andwithout hydrother-mal contribution
24 Statistical Analysis Pearson Chi-Square test was used tocompare restrictions and COPD prevalence between individ-uals inhabiting the environment with volcanic degassing andindividuals from the reference group To estimate the asso-ciation between chronic exposure to an environment withvolcanic air pollution and restrictive and obstructive defects(no versus yes) odds ratio (OR) and 95 confidence intervals(95 CIs) were calculated using a binary logistic regressionmodel adjusting for age gender (male versus female) fatigue(yes versus no) and smoking status (yes versus no)
To estimate the association between chronic exposure toan environment with volcanic air pollution and the increasein the severity COPD odds ratio (OR) and 95 confidenceintervals (95 CIs) were calculated using an ordinal logisticregression model adjusting for age fatigue (yes versus no)asthma (yes versus no) and smoking status (yes versus no)The occurrence of obstructions was graded on scales accord-ing to their occurrence and severity 1 without obstructionand 2 to 4 with obstruction from the least severe (2) to themost severe (4)
Mann-Whitney 119880 test was used to compare soil CO2
fluxes released by diffuse degassing between the reference andthe study group
All statistical analysis was performed using IBM SPSSStatistics 200 for Windows [30] and the level of statisticalsignificance was set at 119875 le 005
BioMed Research International 5
Table 2 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing (DDS) andrestrictive lung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 1097Prob gt chi2 = 005
Parameter 119899 () OR (95 CI)a P valueAge 099 (096ndash102) 0933Gender
Male 207 (41) 116 (050ndash269) 0729Female 298 (59) 100
Easy fatigueYes 116 (23) 062 (023ndash167) 0349No 389 (77) 100
Smoking statusSmoker 163 (323) 094 (036ndash242) 0892Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 437 (178ndash1069) 0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
3 Results
The general characteristics of the study populations arepresented in Table 1The study group has an older populationand a higher BMI than the reference one (561 versus 423of individuals with more than 41 years and 271 kgm2 versus257 kgm2 resp) On the other hand the reference group hasa higher percentage of smokers than the study group (376versus 191)
Soil CO2flux was significantly different (119875 lt 0001)
between the studied areas (Table 1) According to criteriafor diffuse degassing susceptibility areas defined by Viveiroset al [14] all the analyzed buildings in Ponta Delgada arelocated in low susceptibility areas (CO
2flux lt 25 gm2d)
while in Ribeira Quente 19 of the buildings were locatedin moderate susceptibility areas (soil CO
2flux between
25 gm2d and 50 gm2d) and the remaining 981 were ina high susceptibility area (soil CO
2flux ge 50 gm2d) (Sup-
plementary Material 1 in Supplementary Material availableonline at httpdxdoiorg1011552015326794)
31 Prevalence of Restrictive and Obstructive RespiratoryDefects The prevalence of restrictions in the study groupwas significantly higher than in the reference group (102versus 30 resp 119875 = 0001) Similarly the prevalence ofCOPD was significantly higher in the study group than inthe reference one (336 versus 119 resp 119875 lt 0001)(Figure 2) The prevalence of more severe obstructions wasalso higher in the study group compared to the reference one(mild 157 versus 44 moderate 68 versus 22 and severe47 versus 0 resp)
32 Restrictive or Obstructive Respiratory Defects and Expo-sure to Volcanogenic Air Pollution by DDS Exposure to
0102030405060708090
Normal Restriction COPD
Prev
alen
ce (
)
Reference groupStudy group
lowastlowast lowast
lowast
Figure 2 Proportion () of individuals with obstructive andrestrictive airway diseases in study (Ribeira Quente) and reference(Ponta Delgada) groups lowastsignificantly different at 119875 lt 005
volcanogenic air pollution by DDSwas a significant predictorof the prevalence of respiratory restrictions and of COPDexacerbation in the multivariate analysis After adjustmentfor age gender fatigue and smoking status a higher preva-lence of respiratory restrictions was found associated withexposure to volcanogenic air pollution by DDS (OR = 4495 CI 178ndash1069 119875 = 0001) (Table 2) Also after theadjustment for the same factors a higher prevalence ofrespiratory obstructions was found associated with exposureto the volcanic environment (OR = 28 95 CI 160ndash499)(Table 3) Exacerbation in COPD severity was also foundsignificantly associated with exposure to volcanogenic airpollution by DDS (OR = 32 95 CI 182ndash558 119875 lt 0001)(Table 4)
The analyzed confounding factors did not show anysignificant association with respiratory restrictions (Table 2)but respiratory obstructions were significantly associated
6 BioMed Research International
Table 3 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and obstructivelung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 6080Prob gt chi2 = lt0001
Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (105ndash328) 0033No 389 (77) 100
GenderMale 207 (41) 066 (039ndash111) 0123Female 298 (59) 100
Smoking statusSmoker 163 (323) 234 (135ndash406) 0002Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 283 (160ndash499) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
Table 4 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and COPDexacerbation
Ordinal logistic regressionNumber of obs 505LR chi2(5) = 7019
Prob gt chi2 = lt0001Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (100ndash324) 0046No 389 (77) 100
AsthmaYes 43 (85) 225 (105ndash482) 0037No 462 (915) 100
Smoking statusSmoker 163 (323) 211 (125ndash356) 0005Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 319 (182ndash558) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
with age fatigue and smoking status (Table 3) The increasein COPD severity was significantly associated with asthmaand the abovementioned factors (Table 4)
4 Discussion
The association between exposure to air pollution andadverse respiratory effects has been widely demonstrated[31 32] Such association is usually related to anthropogenicair pollution while for volcanogenic pollution there are
much fewer studies Volcanoes and volcanic manifestationssuch as fumaroles and hot and cold CO
2-rich springs as
well as degassing soils release into the environment metalshazardous aerosols and gases that daily affect the quality ofthe environment and the health of human populations [33]
The measurements of CO2flux revealed that the study
group (from the hydrothermal area) is chronically exposed toelevated volcanogenic air pollution by soil diffuse degassingcompared to the reference group (average values are 508 gm2d (asymp3573 ppms) versus 1536 gm2d (asymp108 ppms)
BioMed Research International 7
resp) Carbon dioxide levels are described to be usuallygreater inside a building than outside [34 35] therefore thesepopulations are much probably subjected to higher levels ofindoor CO
2than the presented values Also independently
of the biological CO2contribution the hydrothermal CO
2
emission is permanent and thus the level of CO2in the
Ribeira Quente buildings must be always higher than theldquonormalrdquo values and sporadically reach anomalous highvalues as recognized in previous works only due to meteo-rological changes [13] The threshold limit value for 8 h timeweighted-average exposures to CO
2is 5000 ppm (WHO)
and possibly the average CO2concentrations encountered
in the buildings are below this limit and are not expectedto cause health symptoms such as headaches fatigue andeye and throat irritation However the consequences ofthe permanent presence of indoor CO
2in concentrations
higher than the outdoor environment are still far from beingunderstood and may eventually lead to some stress effect inthe organisms that needs to be better studied In additionthe CO
2emission may be also associated with other volcanic
emissions as it is the case of the radioactive gas radon Themeasurements performed showed that the study group ischronically exposed to elevated volcanogenic air pollutionnamely high CO
2soil diffuse degassing high concentrations
of CO2can cause headaches due to hypercapnia and the
decrease of O2in the bloodstream [36] When these two
events combine the body responds by increasing blood flowto the brain by dilating the blood vessels resulting in pain[36] A significant association was found between restrictiverespiratory defects and the exposure to volcanogenic airpollution by DDS measured as 44 times higher in theinhabitants of Ribeira Quente (study group) when comparedto the reference one A significant association was also foundbetween obstructive respiratory defects and exposure tovolcanogenic air pollution by DDS measured as 28 timeshigher in the study group None of the analyzed confoundingfactors (age gender fatigue and smoking status) was signifi-cantly associated with respiratory restriction but apart fromgender all confounding factors were positively associatedwith respiratory obstructions
Results also showed significant associations between theincrease in the severity of COPD and the exposure to soildiffuse degassing in the study group when compared to thereference one given as 32 times higher in Ribeira Quenteinhabitants (study group) Age asthma fatigue and smokingstatus were also significantly associated with the increase inCOPD severity
Age and smoking habits are well associated with COPDprevalence [37 38] According to our results the classificationof subjects who are at risk is relevant in middle-aged andelderly persons (ie gt 41 years old) individuals with asthmaand smokers Aging affects the structure function andcontrol of the respiratory system according to Stanojevic etal [39] both FEV
1and FVC decrease with age and thus
the observed increase in COPD associated with age wasexpected (since older individuals will have a reduced FVCand a reduced FEV
1FVC ratio) Also recently results from
Eurostat [40] demonstrated that respiratory diseases such asbronchitis and asthma affect mainly older people as almost
90 of EU-28 deaths from these diseases occur among thoseaged 65 and aboveMoreover this report presents a standard-ized death rate from diseases of the respiratory system of atleast 150 deaths per 100 000 inhabitants the highest deathrates were observed in two Portuguese regions the volcanicislands ofMadeira (2946 deaths per 100 000 inhabitants) andAzores (1958 deaths per 100 000 inhabitants) the rest of thePortuguese territory (mainland) presented a death rate below150 deaths per 100 000 inhabitants therefore the observedresults are in accordance with this general overview
Regarding asthma there might be a significant overlapwith COPD since both are characterized by an underlyingairway inflammation although the structural and patho-physiologic findings in both diseases can be usually differ-entiated [41] According to the Global Initiative for ChronicObstructive Lung Diseases [42] in individuals with chronicrespiratory symptoms and fixed airflow limitation it isdifficult to differentiate asthma from COPD However thereis epidemiological evidence that long-standing asthma canlead to fixed airflow limitation [43] which increases thefrequency of asthma attacks [44]
Fatigue is considered the secondmost common symptomof COPD after breathlessness [45] The increased level offatigue found in patients with COPD is associated with anincrease in the severity of lung impairment and a reductionin exercise tolerance Symptoms of fatigue can be physicaland mental such as lack of energy or poor concentrationBaghai-Ravary et al [46] and Breslin et al [47] found arelationship between fatigue and COPD which persists atCOPD exacerbations Since COPD was observed mainlyin elderly people that have diminished lung function andtherefore a reduction in health status fatigue was expectedto be associated with COPD
It is well established that tobacco is the most importantcausative factor for COPDwith individual susceptibility con-tinuously interacting synergistically with other risk factors[48] such as age According to Lundback et al [49] lifelongsmoking increases the chance of developing COPD andthus about 50 of the smokers eventually develop COPDduring their lifetime However according to GOLD [42]other risk factors of COPD include exposure to air pollutionsecondhand smoke and occupational dusts and chemicalsheredity a history of childhood respiratory infections andsocioeconomic status In the present study air pollution byhydrothermal volcanism was proven to be a risk factor inCOPD exacerbation
It is well known that air pollution can perpetuate achronic inflammatory process that potentially leads to lungdiseases [31] However the majority of studies regard airpollutants of anthropogenic origin such as PM
10 NO2 SO2
and O3[50 51] while only few studies were developed
in areas with volcanic activity and associate volcanogenicpollutants with human airway diseases [7 52] Longo andYang [52] and Iwasawa et al [8] reported a higher risk of acutebronchitis across the lifespan in humans exposed to sulfurousvolcanic air pollution Furthermore in 2013 Camarinhoet al [22] showed that noneruptive active volcanism isassociated with increased lung injury in mice Thus it is notunexpected to observe an increase in the exacerbation of
8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 5
Table 2 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing (DDS) andrestrictive lung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 1097Prob gt chi2 = 005
Parameter 119899 () OR (95 CI)a P valueAge 099 (096ndash102) 0933Gender
Male 207 (41) 116 (050ndash269) 0729Female 298 (59) 100
Easy fatigueYes 116 (23) 062 (023ndash167) 0349No 389 (77) 100
Smoking statusSmoker 163 (323) 094 (036ndash242) 0892Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 437 (178ndash1069) 0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
3 Results
The general characteristics of the study populations arepresented in Table 1The study group has an older populationand a higher BMI than the reference one (561 versus 423of individuals with more than 41 years and 271 kgm2 versus257 kgm2 resp) On the other hand the reference group hasa higher percentage of smokers than the study group (376versus 191)
Soil CO2flux was significantly different (119875 lt 0001)
between the studied areas (Table 1) According to criteriafor diffuse degassing susceptibility areas defined by Viveiroset al [14] all the analyzed buildings in Ponta Delgada arelocated in low susceptibility areas (CO
2flux lt 25 gm2d)
while in Ribeira Quente 19 of the buildings were locatedin moderate susceptibility areas (soil CO
2flux between
25 gm2d and 50 gm2d) and the remaining 981 were ina high susceptibility area (soil CO
2flux ge 50 gm2d) (Sup-
plementary Material 1 in Supplementary Material availableonline at httpdxdoiorg1011552015326794)
31 Prevalence of Restrictive and Obstructive RespiratoryDefects The prevalence of restrictions in the study groupwas significantly higher than in the reference group (102versus 30 resp 119875 = 0001) Similarly the prevalence ofCOPD was significantly higher in the study group than inthe reference one (336 versus 119 resp 119875 lt 0001)(Figure 2) The prevalence of more severe obstructions wasalso higher in the study group compared to the reference one(mild 157 versus 44 moderate 68 versus 22 and severe47 versus 0 resp)
32 Restrictive or Obstructive Respiratory Defects and Expo-sure to Volcanogenic Air Pollution by DDS Exposure to
0102030405060708090
Normal Restriction COPD
Prev
alen
ce (
)
Reference groupStudy group
lowastlowast lowast
lowast
Figure 2 Proportion () of individuals with obstructive andrestrictive airway diseases in study (Ribeira Quente) and reference(Ponta Delgada) groups lowastsignificantly different at 119875 lt 005
volcanogenic air pollution by DDSwas a significant predictorof the prevalence of respiratory restrictions and of COPDexacerbation in the multivariate analysis After adjustmentfor age gender fatigue and smoking status a higher preva-lence of respiratory restrictions was found associated withexposure to volcanogenic air pollution by DDS (OR = 4495 CI 178ndash1069 119875 = 0001) (Table 2) Also after theadjustment for the same factors a higher prevalence ofrespiratory obstructions was found associated with exposureto the volcanic environment (OR = 28 95 CI 160ndash499)(Table 3) Exacerbation in COPD severity was also foundsignificantly associated with exposure to volcanogenic airpollution by DDS (OR = 32 95 CI 182ndash558 119875 lt 0001)(Table 4)
The analyzed confounding factors did not show anysignificant association with respiratory restrictions (Table 2)but respiratory obstructions were significantly associated
6 BioMed Research International
Table 3 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and obstructivelung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 6080Prob gt chi2 = lt0001
Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (105ndash328) 0033No 389 (77) 100
GenderMale 207 (41) 066 (039ndash111) 0123Female 298 (59) 100
Smoking statusSmoker 163 (323) 234 (135ndash406) 0002Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 283 (160ndash499) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
Table 4 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and COPDexacerbation
Ordinal logistic regressionNumber of obs 505LR chi2(5) = 7019
Prob gt chi2 = lt0001Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (100ndash324) 0046No 389 (77) 100
AsthmaYes 43 (85) 225 (105ndash482) 0037No 462 (915) 100
Smoking statusSmoker 163 (323) 211 (125ndash356) 0005Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 319 (182ndash558) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
with age fatigue and smoking status (Table 3) The increasein COPD severity was significantly associated with asthmaand the abovementioned factors (Table 4)
4 Discussion
The association between exposure to air pollution andadverse respiratory effects has been widely demonstrated[31 32] Such association is usually related to anthropogenicair pollution while for volcanogenic pollution there are
much fewer studies Volcanoes and volcanic manifestationssuch as fumaroles and hot and cold CO
2-rich springs as
well as degassing soils release into the environment metalshazardous aerosols and gases that daily affect the quality ofthe environment and the health of human populations [33]
The measurements of CO2flux revealed that the study
group (from the hydrothermal area) is chronically exposed toelevated volcanogenic air pollution by soil diffuse degassingcompared to the reference group (average values are 508 gm2d (asymp3573 ppms) versus 1536 gm2d (asymp108 ppms)
BioMed Research International 7
resp) Carbon dioxide levels are described to be usuallygreater inside a building than outside [34 35] therefore thesepopulations are much probably subjected to higher levels ofindoor CO
2than the presented values Also independently
of the biological CO2contribution the hydrothermal CO
2
emission is permanent and thus the level of CO2in the
Ribeira Quente buildings must be always higher than theldquonormalrdquo values and sporadically reach anomalous highvalues as recognized in previous works only due to meteo-rological changes [13] The threshold limit value for 8 h timeweighted-average exposures to CO
2is 5000 ppm (WHO)
and possibly the average CO2concentrations encountered
in the buildings are below this limit and are not expectedto cause health symptoms such as headaches fatigue andeye and throat irritation However the consequences ofthe permanent presence of indoor CO
2in concentrations
higher than the outdoor environment are still far from beingunderstood and may eventually lead to some stress effect inthe organisms that needs to be better studied In additionthe CO
2emission may be also associated with other volcanic
emissions as it is the case of the radioactive gas radon Themeasurements performed showed that the study group ischronically exposed to elevated volcanogenic air pollutionnamely high CO
2soil diffuse degassing high concentrations
of CO2can cause headaches due to hypercapnia and the
decrease of O2in the bloodstream [36] When these two
events combine the body responds by increasing blood flowto the brain by dilating the blood vessels resulting in pain[36] A significant association was found between restrictiverespiratory defects and the exposure to volcanogenic airpollution by DDS measured as 44 times higher in theinhabitants of Ribeira Quente (study group) when comparedto the reference one A significant association was also foundbetween obstructive respiratory defects and exposure tovolcanogenic air pollution by DDS measured as 28 timeshigher in the study group None of the analyzed confoundingfactors (age gender fatigue and smoking status) was signifi-cantly associated with respiratory restriction but apart fromgender all confounding factors were positively associatedwith respiratory obstructions
Results also showed significant associations between theincrease in the severity of COPD and the exposure to soildiffuse degassing in the study group when compared to thereference one given as 32 times higher in Ribeira Quenteinhabitants (study group) Age asthma fatigue and smokingstatus were also significantly associated with the increase inCOPD severity
Age and smoking habits are well associated with COPDprevalence [37 38] According to our results the classificationof subjects who are at risk is relevant in middle-aged andelderly persons (ie gt 41 years old) individuals with asthmaand smokers Aging affects the structure function andcontrol of the respiratory system according to Stanojevic etal [39] both FEV
1and FVC decrease with age and thus
the observed increase in COPD associated with age wasexpected (since older individuals will have a reduced FVCand a reduced FEV
1FVC ratio) Also recently results from
Eurostat [40] demonstrated that respiratory diseases such asbronchitis and asthma affect mainly older people as almost
90 of EU-28 deaths from these diseases occur among thoseaged 65 and aboveMoreover this report presents a standard-ized death rate from diseases of the respiratory system of atleast 150 deaths per 100 000 inhabitants the highest deathrates were observed in two Portuguese regions the volcanicislands ofMadeira (2946 deaths per 100 000 inhabitants) andAzores (1958 deaths per 100 000 inhabitants) the rest of thePortuguese territory (mainland) presented a death rate below150 deaths per 100 000 inhabitants therefore the observedresults are in accordance with this general overview
Regarding asthma there might be a significant overlapwith COPD since both are characterized by an underlyingairway inflammation although the structural and patho-physiologic findings in both diseases can be usually differ-entiated [41] According to the Global Initiative for ChronicObstructive Lung Diseases [42] in individuals with chronicrespiratory symptoms and fixed airflow limitation it isdifficult to differentiate asthma from COPD However thereis epidemiological evidence that long-standing asthma canlead to fixed airflow limitation [43] which increases thefrequency of asthma attacks [44]
Fatigue is considered the secondmost common symptomof COPD after breathlessness [45] The increased level offatigue found in patients with COPD is associated with anincrease in the severity of lung impairment and a reductionin exercise tolerance Symptoms of fatigue can be physicaland mental such as lack of energy or poor concentrationBaghai-Ravary et al [46] and Breslin et al [47] found arelationship between fatigue and COPD which persists atCOPD exacerbations Since COPD was observed mainlyin elderly people that have diminished lung function andtherefore a reduction in health status fatigue was expectedto be associated with COPD
It is well established that tobacco is the most importantcausative factor for COPDwith individual susceptibility con-tinuously interacting synergistically with other risk factors[48] such as age According to Lundback et al [49] lifelongsmoking increases the chance of developing COPD andthus about 50 of the smokers eventually develop COPDduring their lifetime However according to GOLD [42]other risk factors of COPD include exposure to air pollutionsecondhand smoke and occupational dusts and chemicalsheredity a history of childhood respiratory infections andsocioeconomic status In the present study air pollution byhydrothermal volcanism was proven to be a risk factor inCOPD exacerbation
It is well known that air pollution can perpetuate achronic inflammatory process that potentially leads to lungdiseases [31] However the majority of studies regard airpollutants of anthropogenic origin such as PM
10 NO2 SO2
and O3[50 51] while only few studies were developed
in areas with volcanic activity and associate volcanogenicpollutants with human airway diseases [7 52] Longo andYang [52] and Iwasawa et al [8] reported a higher risk of acutebronchitis across the lifespan in humans exposed to sulfurousvolcanic air pollution Furthermore in 2013 Camarinhoet al [22] showed that noneruptive active volcanism isassociated with increased lung injury in mice Thus it is notunexpected to observe an increase in the exacerbation of
8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

6 BioMed Research International
Table 3 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and obstructivelung defects
Binomial logistic regressionNumber of obs 505LR chi2(5) = 6080Prob gt chi2 = lt0001
Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (105ndash328) 0033No 389 (77) 100
GenderMale 207 (41) 066 (039ndash111) 0123Female 298 (59) 100
Smoking statusSmoker 163 (323) 234 (135ndash406) 0002Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 283 (160ndash499) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
Table 4 Adjusted association between characteristics of study participants exposure to volcanogenic soil diffuse degassing and COPDexacerbation
Ordinal logistic regressionNumber of obs 505LR chi2(5) = 7019
Prob gt chi2 = lt0001Parameter 119899 () OR (95 CI)a P valueAge 104 (102ndash106) lt0001Easy fatigue
Yes 116 (23) 180 (100ndash324) 0046No 389 (77) 100
AsthmaYes 43 (85) 225 (105ndash482) 0037No 462 (915) 100
Smoking statusSmoker 163 (323) 211 (125ndash356) 0005Nonsmoker 342 (677) 100
Exposure to DDSYes (study group) 146 (289) 319 (182ndash558) lt0001No (reference group) 359 (711) 100
aOR odds ratio 95 CI 95 confidence interval
with age fatigue and smoking status (Table 3) The increasein COPD severity was significantly associated with asthmaand the abovementioned factors (Table 4)
4 Discussion
The association between exposure to air pollution andadverse respiratory effects has been widely demonstrated[31 32] Such association is usually related to anthropogenicair pollution while for volcanogenic pollution there are
much fewer studies Volcanoes and volcanic manifestationssuch as fumaroles and hot and cold CO
2-rich springs as
well as degassing soils release into the environment metalshazardous aerosols and gases that daily affect the quality ofthe environment and the health of human populations [33]
The measurements of CO2flux revealed that the study
group (from the hydrothermal area) is chronically exposed toelevated volcanogenic air pollution by soil diffuse degassingcompared to the reference group (average values are 508 gm2d (asymp3573 ppms) versus 1536 gm2d (asymp108 ppms)
BioMed Research International 7
resp) Carbon dioxide levels are described to be usuallygreater inside a building than outside [34 35] therefore thesepopulations are much probably subjected to higher levels ofindoor CO
2than the presented values Also independently
of the biological CO2contribution the hydrothermal CO
2
emission is permanent and thus the level of CO2in the
Ribeira Quente buildings must be always higher than theldquonormalrdquo values and sporadically reach anomalous highvalues as recognized in previous works only due to meteo-rological changes [13] The threshold limit value for 8 h timeweighted-average exposures to CO
2is 5000 ppm (WHO)
and possibly the average CO2concentrations encountered
in the buildings are below this limit and are not expectedto cause health symptoms such as headaches fatigue andeye and throat irritation However the consequences ofthe permanent presence of indoor CO
2in concentrations
higher than the outdoor environment are still far from beingunderstood and may eventually lead to some stress effect inthe organisms that needs to be better studied In additionthe CO
2emission may be also associated with other volcanic
emissions as it is the case of the radioactive gas radon Themeasurements performed showed that the study group ischronically exposed to elevated volcanogenic air pollutionnamely high CO
2soil diffuse degassing high concentrations
of CO2can cause headaches due to hypercapnia and the
decrease of O2in the bloodstream [36] When these two
events combine the body responds by increasing blood flowto the brain by dilating the blood vessels resulting in pain[36] A significant association was found between restrictiverespiratory defects and the exposure to volcanogenic airpollution by DDS measured as 44 times higher in theinhabitants of Ribeira Quente (study group) when comparedto the reference one A significant association was also foundbetween obstructive respiratory defects and exposure tovolcanogenic air pollution by DDS measured as 28 timeshigher in the study group None of the analyzed confoundingfactors (age gender fatigue and smoking status) was signifi-cantly associated with respiratory restriction but apart fromgender all confounding factors were positively associatedwith respiratory obstructions
Results also showed significant associations between theincrease in the severity of COPD and the exposure to soildiffuse degassing in the study group when compared to thereference one given as 32 times higher in Ribeira Quenteinhabitants (study group) Age asthma fatigue and smokingstatus were also significantly associated with the increase inCOPD severity
Age and smoking habits are well associated with COPDprevalence [37 38] According to our results the classificationof subjects who are at risk is relevant in middle-aged andelderly persons (ie gt 41 years old) individuals with asthmaand smokers Aging affects the structure function andcontrol of the respiratory system according to Stanojevic etal [39] both FEV
1and FVC decrease with age and thus
the observed increase in COPD associated with age wasexpected (since older individuals will have a reduced FVCand a reduced FEV
1FVC ratio) Also recently results from
Eurostat [40] demonstrated that respiratory diseases such asbronchitis and asthma affect mainly older people as almost
90 of EU-28 deaths from these diseases occur among thoseaged 65 and aboveMoreover this report presents a standard-ized death rate from diseases of the respiratory system of atleast 150 deaths per 100 000 inhabitants the highest deathrates were observed in two Portuguese regions the volcanicislands ofMadeira (2946 deaths per 100 000 inhabitants) andAzores (1958 deaths per 100 000 inhabitants) the rest of thePortuguese territory (mainland) presented a death rate below150 deaths per 100 000 inhabitants therefore the observedresults are in accordance with this general overview
Regarding asthma there might be a significant overlapwith COPD since both are characterized by an underlyingairway inflammation although the structural and patho-physiologic findings in both diseases can be usually differ-entiated [41] According to the Global Initiative for ChronicObstructive Lung Diseases [42] in individuals with chronicrespiratory symptoms and fixed airflow limitation it isdifficult to differentiate asthma from COPD However thereis epidemiological evidence that long-standing asthma canlead to fixed airflow limitation [43] which increases thefrequency of asthma attacks [44]
Fatigue is considered the secondmost common symptomof COPD after breathlessness [45] The increased level offatigue found in patients with COPD is associated with anincrease in the severity of lung impairment and a reductionin exercise tolerance Symptoms of fatigue can be physicaland mental such as lack of energy or poor concentrationBaghai-Ravary et al [46] and Breslin et al [47] found arelationship between fatigue and COPD which persists atCOPD exacerbations Since COPD was observed mainlyin elderly people that have diminished lung function andtherefore a reduction in health status fatigue was expectedto be associated with COPD
It is well established that tobacco is the most importantcausative factor for COPDwith individual susceptibility con-tinuously interacting synergistically with other risk factors[48] such as age According to Lundback et al [49] lifelongsmoking increases the chance of developing COPD andthus about 50 of the smokers eventually develop COPDduring their lifetime However according to GOLD [42]other risk factors of COPD include exposure to air pollutionsecondhand smoke and occupational dusts and chemicalsheredity a history of childhood respiratory infections andsocioeconomic status In the present study air pollution byhydrothermal volcanism was proven to be a risk factor inCOPD exacerbation
It is well known that air pollution can perpetuate achronic inflammatory process that potentially leads to lungdiseases [31] However the majority of studies regard airpollutants of anthropogenic origin such as PM
10 NO2 SO2
and O3[50 51] while only few studies were developed
in areas with volcanic activity and associate volcanogenicpollutants with human airway diseases [7 52] Longo andYang [52] and Iwasawa et al [8] reported a higher risk of acutebronchitis across the lifespan in humans exposed to sulfurousvolcanic air pollution Furthermore in 2013 Camarinhoet al [22] showed that noneruptive active volcanism isassociated with increased lung injury in mice Thus it is notunexpected to observe an increase in the exacerbation of
8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 7
resp) Carbon dioxide levels are described to be usuallygreater inside a building than outside [34 35] therefore thesepopulations are much probably subjected to higher levels ofindoor CO
2than the presented values Also independently
of the biological CO2contribution the hydrothermal CO
2
emission is permanent and thus the level of CO2in the
Ribeira Quente buildings must be always higher than theldquonormalrdquo values and sporadically reach anomalous highvalues as recognized in previous works only due to meteo-rological changes [13] The threshold limit value for 8 h timeweighted-average exposures to CO
2is 5000 ppm (WHO)
and possibly the average CO2concentrations encountered
in the buildings are below this limit and are not expectedto cause health symptoms such as headaches fatigue andeye and throat irritation However the consequences ofthe permanent presence of indoor CO
2in concentrations
higher than the outdoor environment are still far from beingunderstood and may eventually lead to some stress effect inthe organisms that needs to be better studied In additionthe CO
2emission may be also associated with other volcanic
emissions as it is the case of the radioactive gas radon Themeasurements performed showed that the study group ischronically exposed to elevated volcanogenic air pollutionnamely high CO
2soil diffuse degassing high concentrations
of CO2can cause headaches due to hypercapnia and the
decrease of O2in the bloodstream [36] When these two
events combine the body responds by increasing blood flowto the brain by dilating the blood vessels resulting in pain[36] A significant association was found between restrictiverespiratory defects and the exposure to volcanogenic airpollution by DDS measured as 44 times higher in theinhabitants of Ribeira Quente (study group) when comparedto the reference one A significant association was also foundbetween obstructive respiratory defects and exposure tovolcanogenic air pollution by DDS measured as 28 timeshigher in the study group None of the analyzed confoundingfactors (age gender fatigue and smoking status) was signifi-cantly associated with respiratory restriction but apart fromgender all confounding factors were positively associatedwith respiratory obstructions
Results also showed significant associations between theincrease in the severity of COPD and the exposure to soildiffuse degassing in the study group when compared to thereference one given as 32 times higher in Ribeira Quenteinhabitants (study group) Age asthma fatigue and smokingstatus were also significantly associated with the increase inCOPD severity
Age and smoking habits are well associated with COPDprevalence [37 38] According to our results the classificationof subjects who are at risk is relevant in middle-aged andelderly persons (ie gt 41 years old) individuals with asthmaand smokers Aging affects the structure function andcontrol of the respiratory system according to Stanojevic etal [39] both FEV
1and FVC decrease with age and thus
the observed increase in COPD associated with age wasexpected (since older individuals will have a reduced FVCand a reduced FEV
1FVC ratio) Also recently results from
Eurostat [40] demonstrated that respiratory diseases such asbronchitis and asthma affect mainly older people as almost
90 of EU-28 deaths from these diseases occur among thoseaged 65 and aboveMoreover this report presents a standard-ized death rate from diseases of the respiratory system of atleast 150 deaths per 100 000 inhabitants the highest deathrates were observed in two Portuguese regions the volcanicislands ofMadeira (2946 deaths per 100 000 inhabitants) andAzores (1958 deaths per 100 000 inhabitants) the rest of thePortuguese territory (mainland) presented a death rate below150 deaths per 100 000 inhabitants therefore the observedresults are in accordance with this general overview
Regarding asthma there might be a significant overlapwith COPD since both are characterized by an underlyingairway inflammation although the structural and patho-physiologic findings in both diseases can be usually differ-entiated [41] According to the Global Initiative for ChronicObstructive Lung Diseases [42] in individuals with chronicrespiratory symptoms and fixed airflow limitation it isdifficult to differentiate asthma from COPD However thereis epidemiological evidence that long-standing asthma canlead to fixed airflow limitation [43] which increases thefrequency of asthma attacks [44]
Fatigue is considered the secondmost common symptomof COPD after breathlessness [45] The increased level offatigue found in patients with COPD is associated with anincrease in the severity of lung impairment and a reductionin exercise tolerance Symptoms of fatigue can be physicaland mental such as lack of energy or poor concentrationBaghai-Ravary et al [46] and Breslin et al [47] found arelationship between fatigue and COPD which persists atCOPD exacerbations Since COPD was observed mainlyin elderly people that have diminished lung function andtherefore a reduction in health status fatigue was expectedto be associated with COPD
It is well established that tobacco is the most importantcausative factor for COPDwith individual susceptibility con-tinuously interacting synergistically with other risk factors[48] such as age According to Lundback et al [49] lifelongsmoking increases the chance of developing COPD andthus about 50 of the smokers eventually develop COPDduring their lifetime However according to GOLD [42]other risk factors of COPD include exposure to air pollutionsecondhand smoke and occupational dusts and chemicalsheredity a history of childhood respiratory infections andsocioeconomic status In the present study air pollution byhydrothermal volcanism was proven to be a risk factor inCOPD exacerbation
It is well known that air pollution can perpetuate achronic inflammatory process that potentially leads to lungdiseases [31] However the majority of studies regard airpollutants of anthropogenic origin such as PM
10 NO2 SO2
and O3[50 51] while only few studies were developed
in areas with volcanic activity and associate volcanogenicpollutants with human airway diseases [7 52] Longo andYang [52] and Iwasawa et al [8] reported a higher risk of acutebronchitis across the lifespan in humans exposed to sulfurousvolcanic air pollution Furthermore in 2013 Camarinhoet al [22] showed that noneruptive active volcanism isassociated with increased lung injury in mice Thus it is notunexpected to observe an increase in the exacerbation of
8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

8 BioMed Research International
COPD severity in the population living in Ribeira Quentea volcanic area with elevated soil diffuse degassing Thesefindings also corroborate the study by Amaral and Rodrigues[19] that observed higher rates of chronic bronchitis in Furnasvillage inhabitants (in comparison to a reference group) andsuggested that it could be partially associated with chronicexposure in a very humid atmosphere to environmentalfactors resulting from volcanic activity
5 Conclusions
To our knowledge this is the first study assessing long-termeffects of CO
2emissions in hydrothermal areas on the
development of respiratory defects The results of this studyshow that long-term exposure to air pollution by soil diffusedegassing increases the risk of developing restrictive defectsas well as the exacerbation of COPD in the inhabitants ofhydrothermal volcanic areas Therefore mitigation measuresshould be implemented in populations inhabiting elevateddiffuse degassing areas such as the construction of natu-ralforced ventilation systems as well as follow-up healthprograms in order to provide medical counseling whennecessary The results of the study also support the need toparticularly followup the asthmatic and the older individualssince these factors are associated with exacerbation in COPDseverity in individuals chronically exposed to volcanogenicsoil diffuse degassing
In addition considering the positive trend of the CO2in
the atmosphere areas as Ribeira Quente village can be usedas natural analogous to studying the possible effects of theseincreases on the population
Conflict of Interests
The authors declare that there is no conflict of interests
Acknowledgments
The authors thank Catarina Silva Ana Ferreira CarolinaParelho Carla Raposo and Ricardo Camarinho for theirsupport in field and laboratory work Diana Linhares andFatima Viveiros were supported respectively by PhD andpostdoc fellowships from the Fundo Regional da Ciencia(Regional Government of the Azores) (PROEMPREGOProgramme) (M312F0192011 and M317F0182011) Theauthors also thank the financial support of BioAirmdashBiom-onitoring Air Pollution Development of an Integrated Sys-tem (M212F0082011) from Fundo Regional da Ciencia(Regional Government of the Azores)
References
[1] National Research Council Active Tectonics Impact on SocietyThe National Academies Press Washington DC USA 1986
[2] K B Brunekreef D W Dockery and M Krzyzanowski ldquoEpi-demiologic studies on short-term effects of low levels of majorambient air pollution componentsrdquo Environmental Health Per-spectives vol 103 no 2 pp 3ndash13 1995
[3] J McCreanor P CullinanM J Nieuwenhuijsen et al ldquoRespira-tory effects of exposure to diesel traffic in persons with asthmardquoTheNew England Journal of Medicine vol 357 no 23 pp 2348ndash2358 2007
[4] S Weichenthal R Kulka A Dubeau C Martin D Wang andR Dales ldquoTraffic-related air pollution and acute changes inheart rate variability and respiratory function in urban cyclistsrdquoEnvironmentalHealth Perspectives vol 119 no 10 pp 1373ndash13782011
[5] R Dales L M Kauri S Cakmak et al ldquoAcute changes inlung function associated with proximity to a steel plant a ran-domized studyrdquo Environment International vol 55 pp 15ndash192013
[6] B Jacquemin J Lepeule A Boudier et al ldquoImpact of geocodingmethods on associations between long-term exposure to urbanair pollution and lung functionrdquo Environmental Health Perspec-tives vol 121 no 9 pp 1054ndash1060 2013
[7] G Gudmundsson ldquoRespiratory health effects of volcanic ashwith special reference to Iceland A reviewrdquo Clinical RespiratoryJournal vol 5 no 1 pp 2ndash9 2011
[8] S Iwasawa Y Kikuchi Y Nishiwaki et al ldquoEffects of SO2
onrespiratory system of adult miyakejima resident 2 years afterreturning to the Islandrdquo Journal of Occupational Health vol 51no 1 pp 38ndash47 2009
[9] BM LongoW Yang J B Green F L Crosby and V L CrosbyldquoAcute health effects associated with exposure to volcanic airpollution (VOG) from increased activity at kilauea volcano in2008rdquo Journal of Toxicology and Environmental Health Part ACurrent Issues vol 73 no 20 pp 1370ndash1381 2010
[10] R Searle ldquoTectonic pattern of the Azores spreading centre andtriple junctionrdquo Earth and Planetary Science Letters vol 51 no2 pp 415ndash434 1980
[11] T Ferreira J L Gaspar F Viveiros M Marcos C Faria andF Sousa ldquoMonitoring of fumarole discharge and CO
2
soildegassing in the Azores contribution to volcanic surveillanceand public health risk assessmentrdquoAnnals of Geophysics vol 48no 4-5 pp 787ndash796 2005
[12] J E Guest J L Gaspar P D Cole et al ldquoVolcanic geology ofFurnas Volcano Sao Miguel Azoresrdquo Journal of Volcanologyand Geothermal Research vol 92 no 1-2 pp 1ndash29 1999
[13] F Viveiros T Ferreira C Silva and J L Gaspar ldquoMeteorologi-cal factors controlling soil gases and indoor CO
2
concentrationa permanent risk in degassing areasrdquo Science of the Total Envi-ronment vol 407 no 4 pp 1362ndash1372 2009
[14] F Viveiros C Cardellini T Ferreira S Caliro G Chiodini andC Silva ldquoSoil CO
2
emissions at Furnas volcano Sao MiguelIsland Azores archipelago volcano monitoring perspectivesgeomorphologic studies and land use planning applicationrdquoJournal of Geophysical Research B Solid Earth vol 115 no 12Article ID B12208 2010
[15] M Durand ldquoIndoor air pollution caused by geothermal gasesrdquoBuilding and Environment vol 41 no 11 pp 1607ndash1610 2006
[16] Y Y You C Niu J Zhou et al ldquoMeasurement of air exchangerates in different indoor environments using continuous CO
2
sensorsrdquo Journal of Environmental Sciences vol 24 no 4 pp657ndash664 2012
[17] World Health Organization Programmes and Projects IndoorAir Pollution WHO 2008
[18] J Balmes M Becklake P Blanc et al ldquoAmerican ThoracicSociety Statement occupational contribution to the burden ofairway diseaserdquo American Journal of Respiratory and CriticalCare Medicine vol 167 no 5 pp 787ndash797 2003
BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 9
[19] A F S Amaral and A S Rodrigues ldquoChronic exposure tovolcanic environments and chronic bronchitis incidence in theAzores Portugalrdquo Environmental Research vol 103 no 3 pp419ndash423 2007
[20] A Amaral V Rodrigues J Oliveira et al ldquoChronic exposureto volcanic environments and cancer incidence in the AzoresPortugalrdquo Science of the Total Environment vol 367 no 1 pp123ndash128 2006
[21] A S Rodrigues M S C Arruda and P V Garcia ldquoEvidenceof DNA damage in humans inhabiting a volcanically activeenvironment a useful tool for biomonitoringrdquo EnvironmentInternational vol 49 pp 51ndash56 2012
[22] R Camarinho P V Garcia and A S Rodrigues ldquoChronicexposure to volcanogenic air pollution as cause of lung injuryrdquoEnvironmental Pollution C vol 181 pp 24ndash30 2013
[23] B G Ferris ldquoEpidemiology standardization project IIrdquo TheAmerican Review of Respiratory Disease vol 118 no 6 pp 7ndash53 1978
[24] British Medical Research Council Committee on the Aetiologyof Chronic Bronchitis ldquoStandardized questionnaire on respira-tory symptomsrdquo British Medical Journal no 2 p 1965 1960
[25] Instituto Nacional de Estatıstica Censos INE 2011 httpcen-sosinept
[26] FViveiros C Cardellini T Ferreira andC Silva ldquoContributionof CO
2
emitted to the atmosphere by diffuse degassing fromvolcanoes the furnas volcano case studyrdquo International Journalof Global Warming vol 4 no 3-4 pp 287ndash304 2012
[27] M R Miller J Hankinson V Brusasco et al ldquoStandardisationof spirometryrdquo European Respiratory Journal vol 26 no 2 pp319ndash338 2005
[28] American Thoracic Society ldquoStandardization of spirometry1994 updaterdquo American Journal of Respiratory and Critical CareMedicine vol 152 no 3 pp 1107ndash1136 1995
[29] G Chiodini R Cioni M Guidi B Raco and L Marini ldquoSoilCO2
flux measurements in volcanic and geothermal areasrdquoApplied Geochemistry vol 13 no 5 pp 543ndash552 1998
[30] IBM SPSS 200 IBM SPSS Statistics 20 Core SystemUserrsquos GuideUSA 2011
[31] T Gotschi J Heinrich J Sunyer and N Kunzli ldquoLong-termeffects of ambient air pollution on lung function a reviewrdquoEpidemiology vol 19 no 5 pp 690ndash701 2008
[32] G Weinmayr E Romeo M de Sario S K Weiland and FForastiere ldquoShort-Term effects of PM
10
and NO2
on respiratoryhealth among children with asthma or asthma-like symptomsa systematic review and Meta-Analysisrdquo Environmental HealthPerspectives vol 118 no 4 pp 449ndash457 2010
[33] A Amaral and A Rodrigues ldquoVolcanogenic contaminantschronic exposurerdquo in Encyclopedia of Environmental Health JNriagu S Kacwe T Kawamoto J A Patz and D M RennieEds vol 5 pp 645ndash653 Elsevier 2011
[34] H H Denli D Z Seker and S Kaya ldquoGIS based carbon diox-ide concentration research in ITU campus Istanbul-Turkeyrdquoin Proceedings of the FIG Congress Engaging the Challenges-Enhancing the Relevance Kuala Lumpur Malaysia June 2014
[35] D H Mudarri ldquoPotential correlation factors for interpretingCO2
measurements in buildingsrdquo ASHRAE Transactions vol103 no 2 pp 244ndash255 1997
[36] S A Rice ldquoHuman health risk assessment of CO2
survivorsof acute high-level exposure and populations sensitive toprolonged low-level exposurerdquo in Proceedings of the 3rd AnnualConference on Carbon Sequestration Rice Alexandria Va USAMay 2004
[37] P Lange ldquoChronic care for COPD patients in DenmarkrdquoPneumonologia i Alergologia Polska vol 80 no 4 pp 292ndash2952012
[38] A Lindberg B Eriksson L-G Larsson E Ronmark T Sand-strom and B Lundback ldquoSeven-year cumulative incidence ofCOPD in an age-stratified general population samplerdquo Chestvol 129 no 4 pp 879ndash885 2006
[39] S Stanojevic A Wade J Stocks et al ldquoReference ranges forspirometry across all ages a new approachrdquo The AmericanJournal of Respiratory and Critical Care Medicine vol 177 no3 pp 253ndash260 2008
[40] Eurostat Regional Yearbook General and Regional StatisticsStatistical Books Publications Office of the European UnionLuxembourg Luxembourg 2014
[41] TWelte andDAGroneberg ldquoAsthma andCOPDrdquoExperimen-tal and Toxicologic Pathology vol 57 no 2 pp 35ndash40 2006
[42] Global Initiative for Chronic Obstructive Lung Diseases(GOLD) Global Strategy for Diagnosis Management and Pre-vention of Chronic Obstructive Pulmonary Disease GOLD 2010httpwwwgoldcopcom
[43] P Lange J Parner J Vestbo P Schnohr and G Jensen ldquoA15-year follow-up study of ventilatory function in adults withasthmardquo The New England Journal of Medicine vol 339 no 17pp 1194ndash200 1998
[44] K-H Kim S A Jahan and E Kabir ldquoA review on humanhealth perspective of air pollution with respect to allergies andasthmardquo Environment International vol 59 pp 41ndash52 2013
[45] J S Paddison TW Effing S Quinn and P A Frith ldquoFatigue inCOPD association with functional status and hospitalisationsrdquoEuropean Respiratory Journal vol 41 no 3 pp 565ndash570 2013
[46] R Baghai-Ravary J K Quint J J P Goldring J R Hurst G CDonaldson and J A Wedzicha ldquoDeterminants and impact offatigue in patients with chronic obstructive pulmonary diseaserdquoRespiratory Medicine vol 103 no 2 pp 216ndash223 2009
[47] E Breslin C P van der Schans S Breukink et al ldquoPerceptionof fatigue and quality of life in patients with COPDrdquo Chest vol114 no 4 pp 958ndash964 1998
[48] S Marsh S Aldington P Shirtchiffe M Weatherall and RBeasley ldquoSmoking and COPD what really are the risksrdquo Euro-pean Respiratory Journal vol 28 no 4 pp 883ndash884 2006
[49] B Lundback A Lindberg M Lindstrom et al ldquoNot 15 but 50of smokers develop COPDmdashreport from the obstructive lungdisease in Northern Sweden studiesrdquo Respiratory Medicine vol97 no 2 pp 115ndash122 2003
[50] M Kampa and E Castanas ldquoHuman health effects of airpollutionrdquo Environmental Pollution vol 151 no 2 pp 362ndash3672008
[51] W MacNee and K Donaldson ldquoMechanism of lung injurycaused by PM10 and ultrafine particles with special reference toCOPDrdquo European Respiratory Journal vol 21 supplement 40pp 47sndash51s 2003
[52] B M Longo and W Yang ldquoAcute bronchitis and volcanic airpollution a community-based cohort study at Kilauea VolcanoHawairsquoi USArdquo Journal of Toxicology and Environmental HealthPart A Current Issues vol 71 no 24 pp 1565ndash1571 2008
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology