Embed Size (px)
Citation preview
Air travel : Implications for patients with pulmonary disease
DM Seminar presented by:
Dr. Vamsi KrishnaSR, Pulmonary medicine, PGIMER
Problems associated with Air Travel
Over 1 billion people air travel each year world over.Passengers traveling by air are exposed to following risks:
• Exposure to high altitude
• Risk of DVT
• Spread of Infectious diseases
Air travel : Pressurized cabins ?
• Commercial aircraft are not pressurized to sea level, but to a relatively modest intermediate cabin altitude. (fuel efficient for jet engines and avoids much turbulence)
• Aircraft cabin altitude can thus approach 2438 m (8000 ft) while the aircraft is flying at 11582 m (38000 ft).
Cottrel JJ. Chest 1988;92:81-4
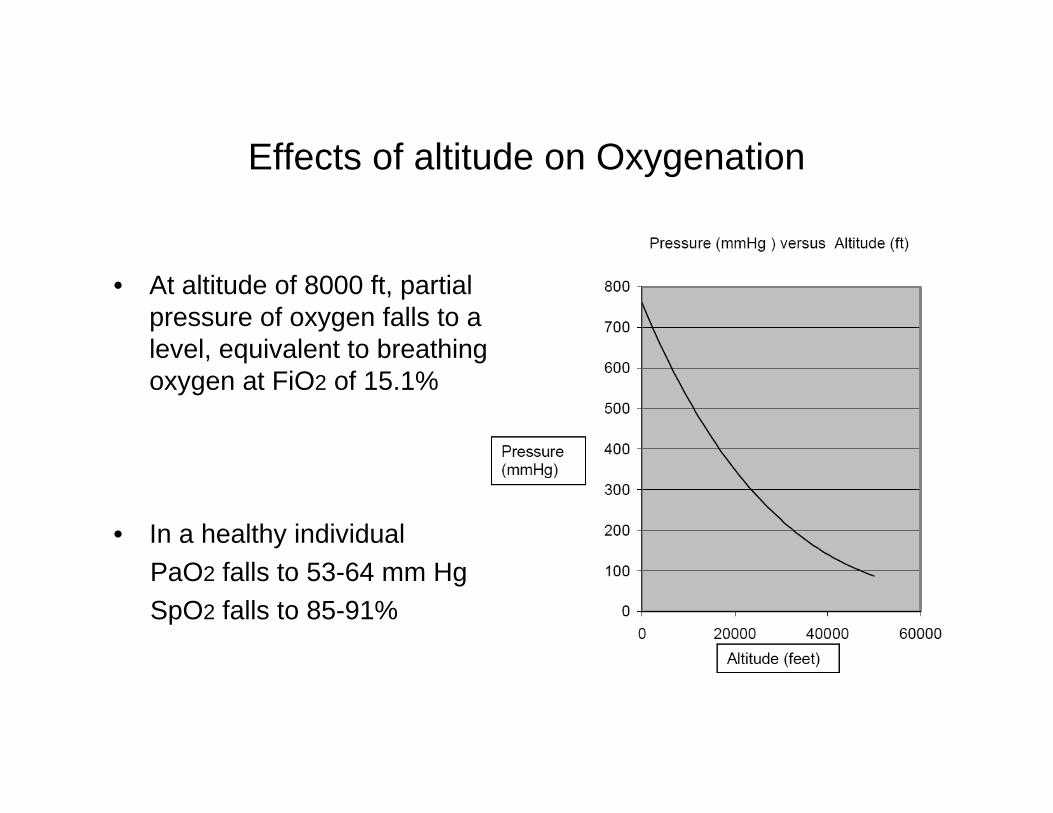
Effects of altitude on Oxygenation
• At altitude of 8000 ft, partial pressure of oxygen falls to a level, equivalent to breathing oxygen at FiO2 of 15.1%
• In a healthy individual PaO2 falls to 53-64 mm HgSpO2 falls to 85-91%
Magnitude of problem
• 5% of commercial airline passengers were ambulatory patients with some illness including chronic obstructive pulmonary disease (COPD)
Iglesias R. Aerosp Med 1974; 45: 204-206
• 10.2% of in-flight medical emergencies calls were respiratory in nature.
Cottrel J.JAMA 1989; 262(12):1653-6
• 17% of respiratory in flight emergencies resulted in diversion of air craft and was 3rd most common cause.
Sirven JI. Neurology,2002;58:1739-44
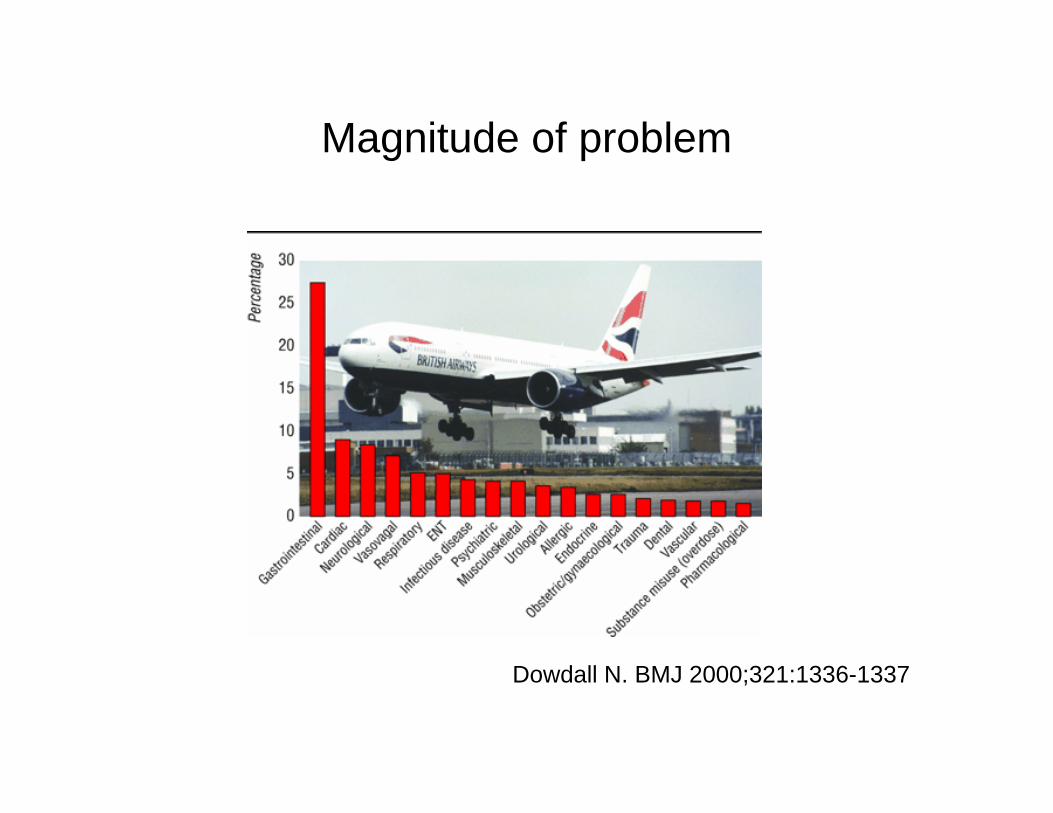
Magnitude of problem
Dowdall N. BMJ 2000;321:1336-1337
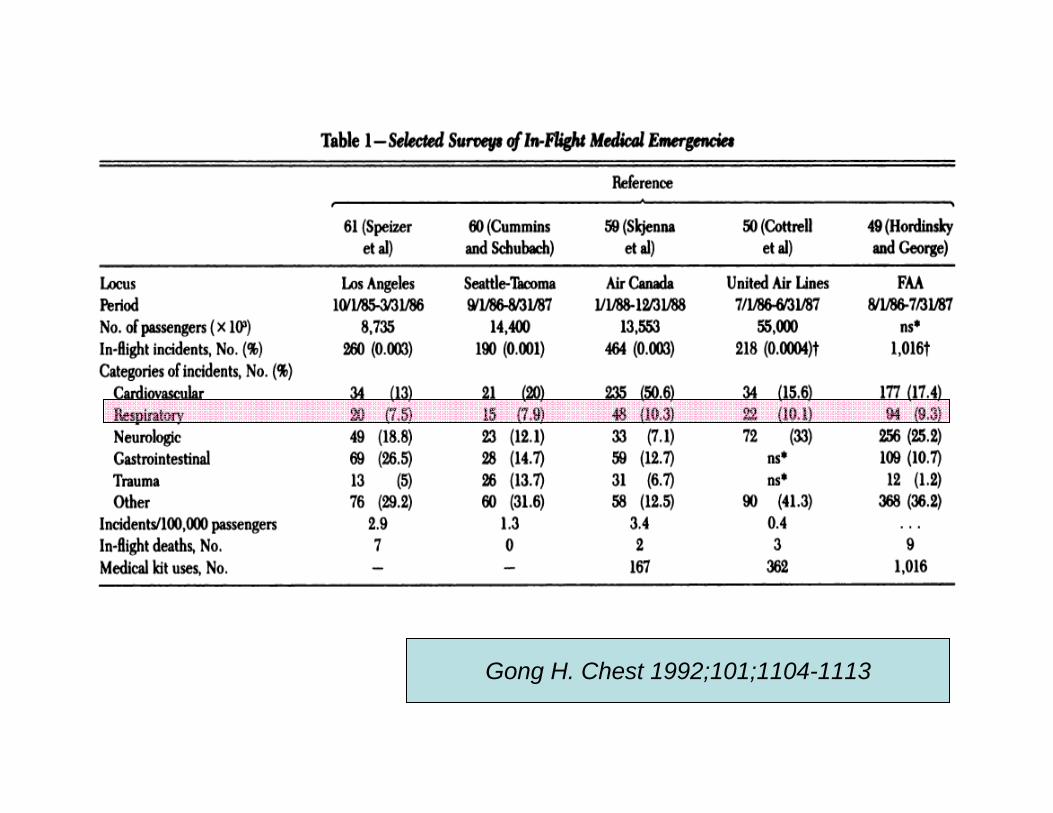
Gong H. Chest 1992;101;1104-1113
Clinical strategy
Aim :To maintain PaO2 of >50 mm Hg during travel
Target : High risk patients
Preflight assessment of in-flight PaO2
Oxygen supplementation to needy
Preflight evaluation
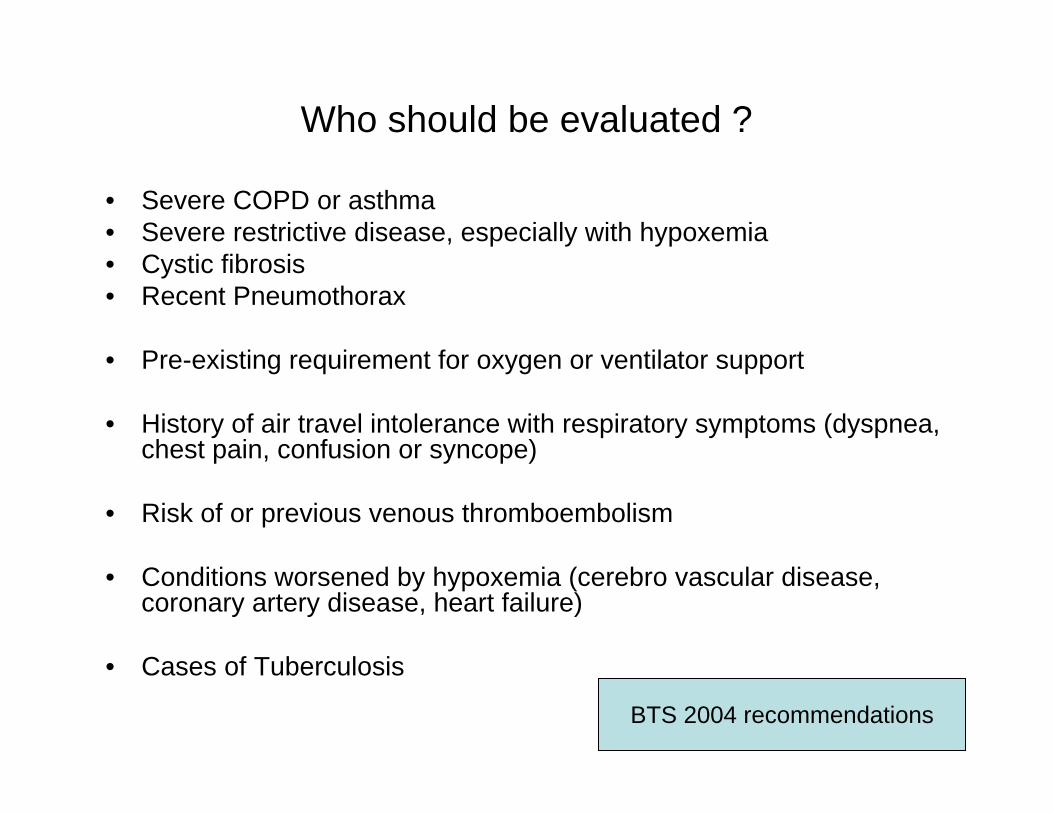
Who should be evaluated ?
• Severe COPD or asthma• Severe restrictive disease, especially with hypoxemia• Cystic fibrosis • Recent Pneumothorax
• Pre-existing requirement for oxygen or ventilator support
• History of air travel intolerance with respiratory symptoms (dyspnea, chest pain, confusion or syncope)
• Risk of or previous venous thromboembolism
• Conditions worsened by hypoxemia (cerebro vascular disease, coronary artery disease, heart failure)
• Cases of Tuberculosis
BTS 2004 recommendations
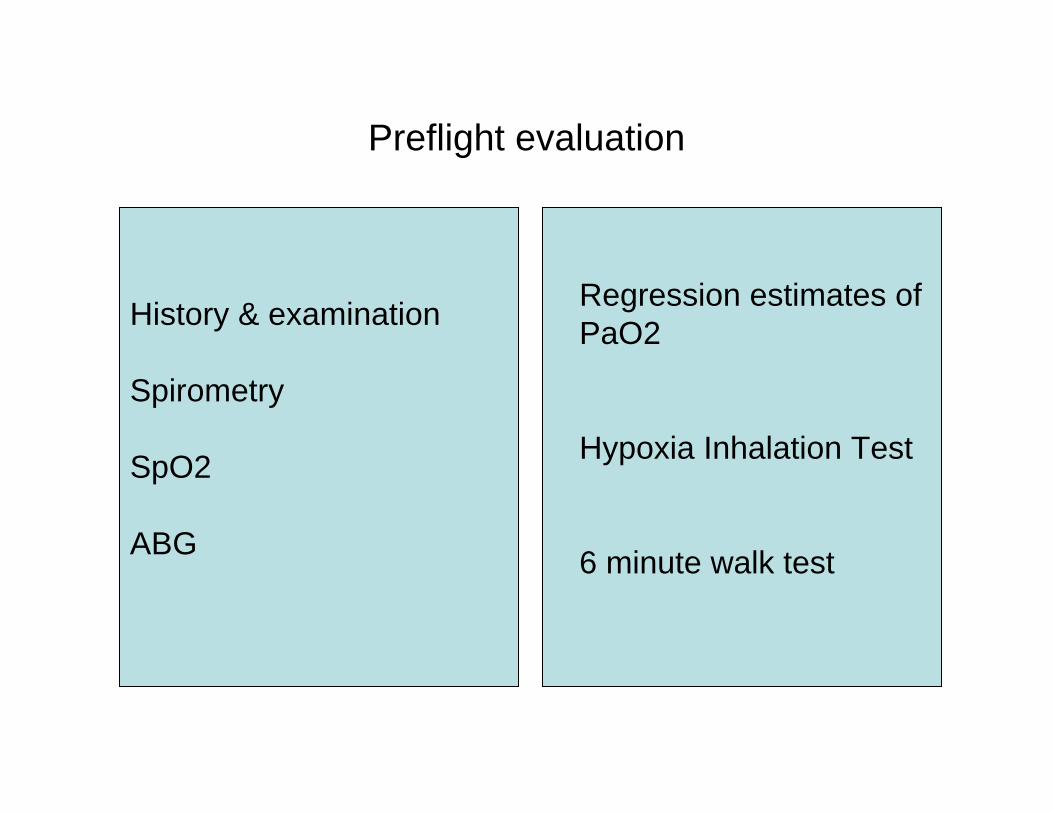
Preflight evaluation
Regression estimates of PaO2
Hypoxia Inhalation Test
6 minute walk test
History & examination
Spirometry
SpO2
ABG
Predicting PaO2
• PaO2 of 68 or 72 at ground level predicts in cabin PaO2 of 50 and 55 respectively ( making correction for FiO2, assuming constant A-a gradient
• PaO2 at sea level alone as a predictor may misclassify many patients as A-a gradient and PaO2/ FiO2 ratios do not remain same at altitudes.
Chi-Lem G. Arch. Med Res 1998;29:57-62
Regression estimates of PaO2
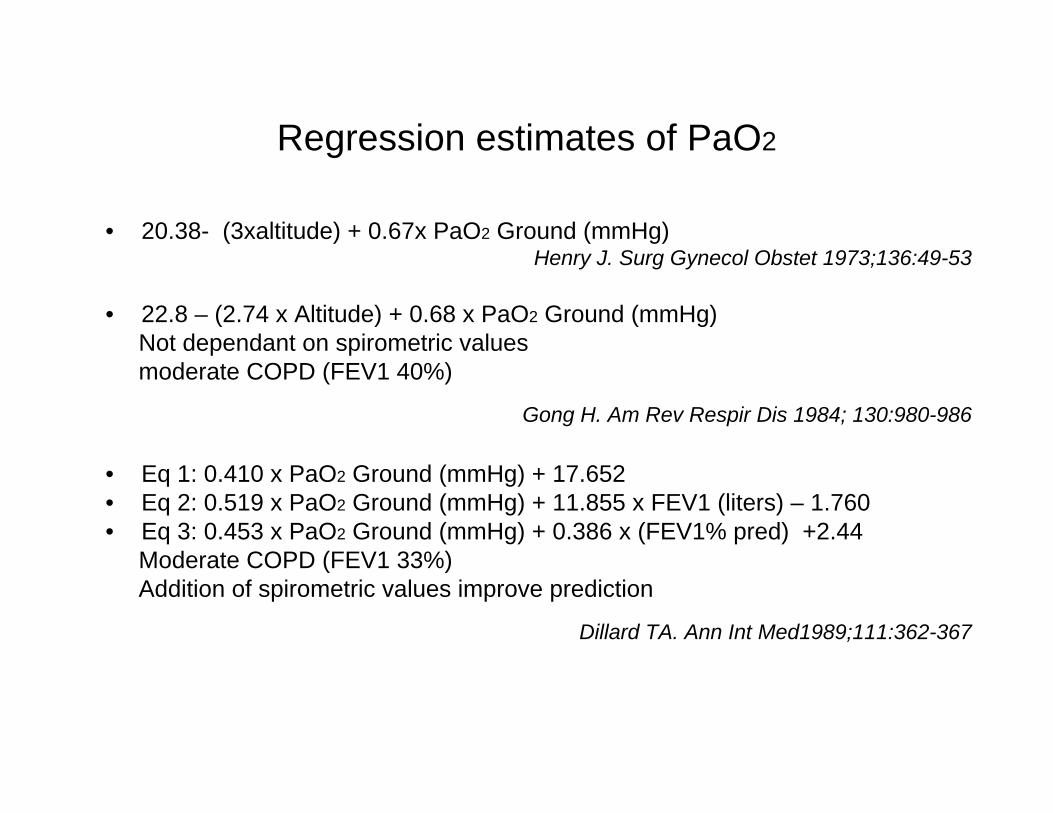
• 20.38- (3xaltitude) + 0.67x PaO2 Ground (mmHg) Henry J. Surg Gynecol Obstet 1973;136:49-53
• 22.8 – (2.74 x Altitude) + 0.68 x PaO2 Ground (mmHg)Not dependant on spirometric valuesmoderate COPD (FEV1 40%)
Gong H. Am Rev Respir Dis 1984; 130:980-986
• Eq 1: 0.410 x PaO2 Ground (mmHg) + 17.652 • Eq 2: 0.519 x PaO2 Ground (mmHg) + 11.855 x FEV1 (liters) – 1.760 • Eq 3: 0.453 x PaO2 Ground (mmHg) + 0.386 x (FEV1% pred) +2.44
Moderate COPD (FEV1 33%)Addition of spirometric values improve prediction
Dillard TA. Ann Int Med1989;111:362-367
Regression estimates of PaO2
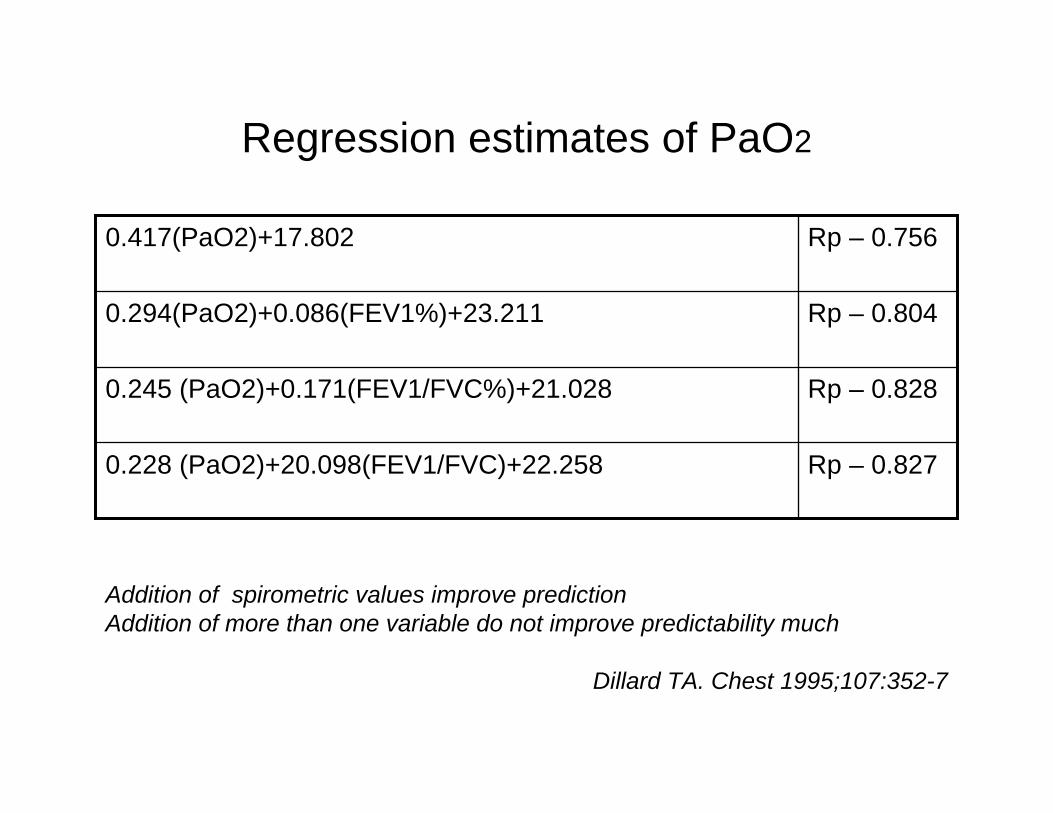
Rp – 0.8270.228 (PaO2)+20.098(FEV1/FVC)+22.258
Rp – 0.8280.245 (PaO2)+0.171(FEV1/FVC%)+21.028
Rp – 0.8040.294(PaO2)+0.086(FEV1%)+23.211
Rp – 0.7560.417(PaO2)+17.802
Addition of spirometric values improve predictionAddition of more than one variable do not improve predictability much
Dillard TA. Chest 1995;107:352-7
Regression estimates of PaO2
• No guidelines and recommendations on when and what formula to be used
• Some authors prefer use of regression estimate as first step and advice Hypoxia inhalation test, if PaO2 is (50 +/- 3) mm Hg
Hypoxia Inhalation Test
Creates FiO2 of 15%Estimate in flight PaO2
But flight duration and cabin conditions are not reproduced.
Breathing 15% O2 by face mask/mouth piece Breathing in a body box with 15% O2
Breathing Nitrogen with venturi mask ( 35-40%)
Monitor SpO2 &After 15-20 minutes measure PaO2
Hypoxia Inhalation Test (HIT)
• PaO2 levels measured by HIT correlated with PaO2 levels measured with hypobaric exposure of 8000 ft.
Dillard TA. Chest 1995;107;352-357
• Results HIT correlated well with hypobaric exposure, but full equilibration took 20 minutes
Naughton MT. Am J Respir Crit Care 1995;152:1956-60
Regression estimate Vs Hypoxia inhalation test Vs Hypobaric simulation
• Regression estimates – easy to calculate- require PaO2, FEV1 only- do not require special gases and equipment
• 15.1% HIT within 2 hrs of 8000 ft hypobaric exposure had higher accuracy than regression estimates
Naughton MT. Am J Respir Crit Care 1995;152:1956-60
• HIT performs as good as hypobaric simulation
Dillard TA. Chest 1995;107:352-7
50 meter walk test
• Inability to complete walk test or moderate to severe dyspnea (assessed by VAS) could implicate necessity for oxygen onboard.
BTS Recommendations 2002
• Equating MRC 3 or 4 at FiO2 21% to MRC 5 at FiO2 15%
• No studies to validate this test.
• Questionable utility.
Pulse Oximetry
• Preflight assessment: BTS recommendations incorporate SpO2 into preflight assessmentBut confounded by smoking and transient hyperventilation
• Use in HIT:During acute hypoxia, pulse oximetry over-estimates PaO2Currently use of pulse oximetry in HIT not recommended as it is not studied and validated
• In-flight monitoring:Studies suggest SpO2 of >90% would maintain PaO2 of >50 mm Hg
Bendrick GA. Aviat Space Environ Med 1995;66:40-44But its routine use for self monitoring by patients not recommended
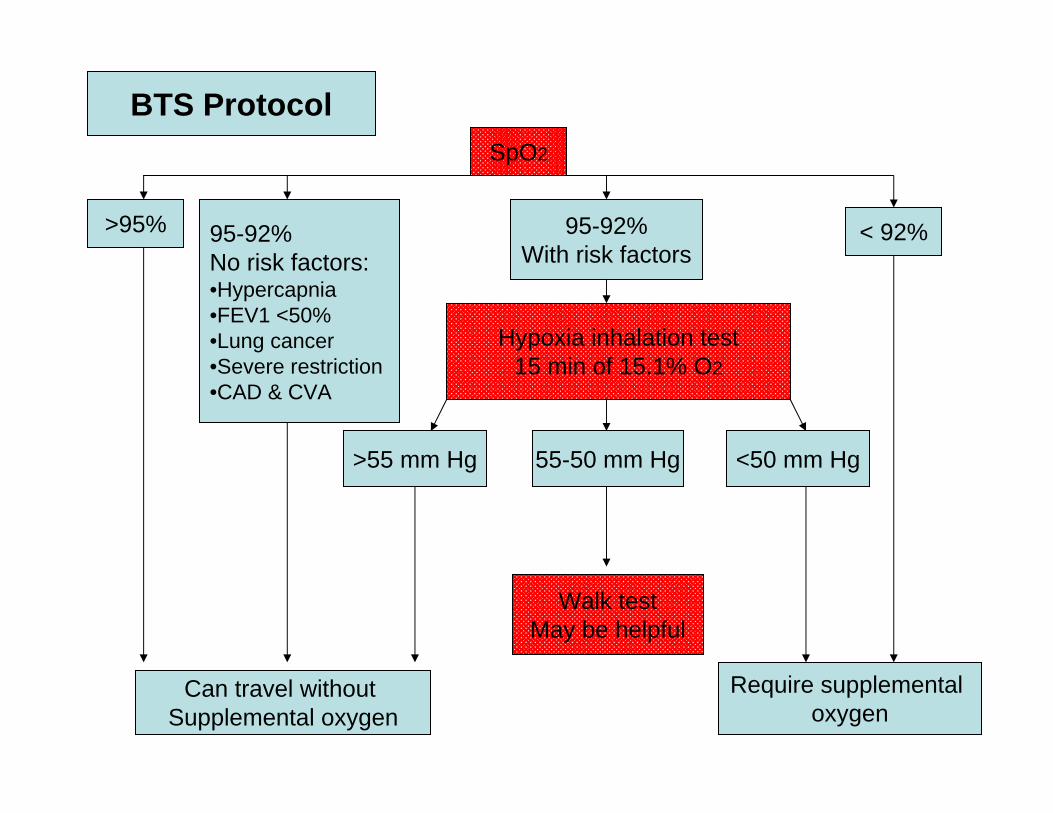
SpO2
95-92%With risk factors
>95% 95-92%No risk factors:•Hypercapnia•FEV1 <50%•Lung cancer•Severe restriction•CAD & CVA
< 92%
Hypoxia inhalation test15 min of 15.1% O2
>55 mm Hg <50 mm Hg55-50 mm Hg
Walk testMay be helpful
Can travel without Supplemental oxygen
Require supplemental oxygen
BTS Protocol
Pre flight evaluation in pediatric population
• Difficult to predict how an infant behaves in hypoxic environment.( presence of right to left shunt and fetal hemoglobin )
• Infants with respiratory disease in neonatal period and children with chronic respiratory diseases like cystic fibrosis should undergo pre flight evaluation.
• Young children and infants should undergo hypoxia inhalation test in
body box
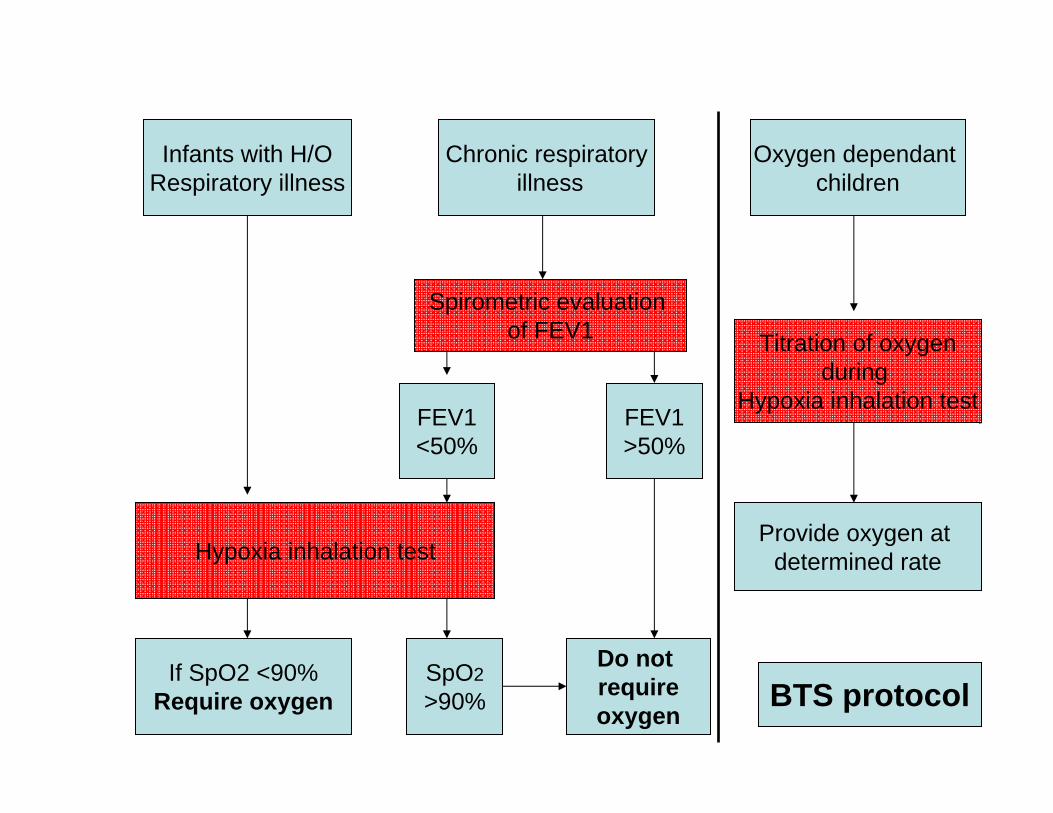
Infants with H/ORespiratory illness
Chronic respiratoryillness
Oxygen dependant children
Spirometric evaluation of FEV1
FEV1<50%
FEV1>50%
Hypoxia inhalation test
If SpO2 <90%Require oxygen
SpO2>90%
Do not requireoxygen
Titration of oxygenduring
Hypoxia inhalation test
Provide oxygen at determined rate
BTS protocol
Preflight evaluation
• 24% of physicians measuring blood gas levels recommend in-flight oxygen when PaO2 <7.3 kPa and 50% when PaO2 is 7.3-8.0 kPa.
• 65% of physicians using spirometry recommend oxygen when the FEV1 is <40%
• 50% recommend oxygen when SaO2 <90% , 33% when SaO2 is 90-94%.
• 10% physicians use predictive equations.
• More than half of specialists but fewer than 10% general physicians perform hypoxic challenge tests
Coker RK. Eur Respir J 2000; 15: 128-130
Travel advice
Supplemental oxygen
• Supplementary oxygen is usually given at a rate of 2 -4 L/min.
• Given by nasal cannulae.
• In-flight oxygen need not be switched on until the plane is at cruising altitude, and may be switched off at the start of descent.
• For patients on oxygen at sea level, the rate should only be increased while at cruising altitude.
Supplemental oxygen
• Evaluation for oxygen requirement during HIT.
2 l/min oxygen supplementation would suffice to maintain SpO2 >90% in patients with severe obstruction and moderate restriction.
Cramer D. Thorax 1996;51:202-203
• Empirical formulae:(FiO2 x SBP) at ground = (FiO2 x SBP) at altitude
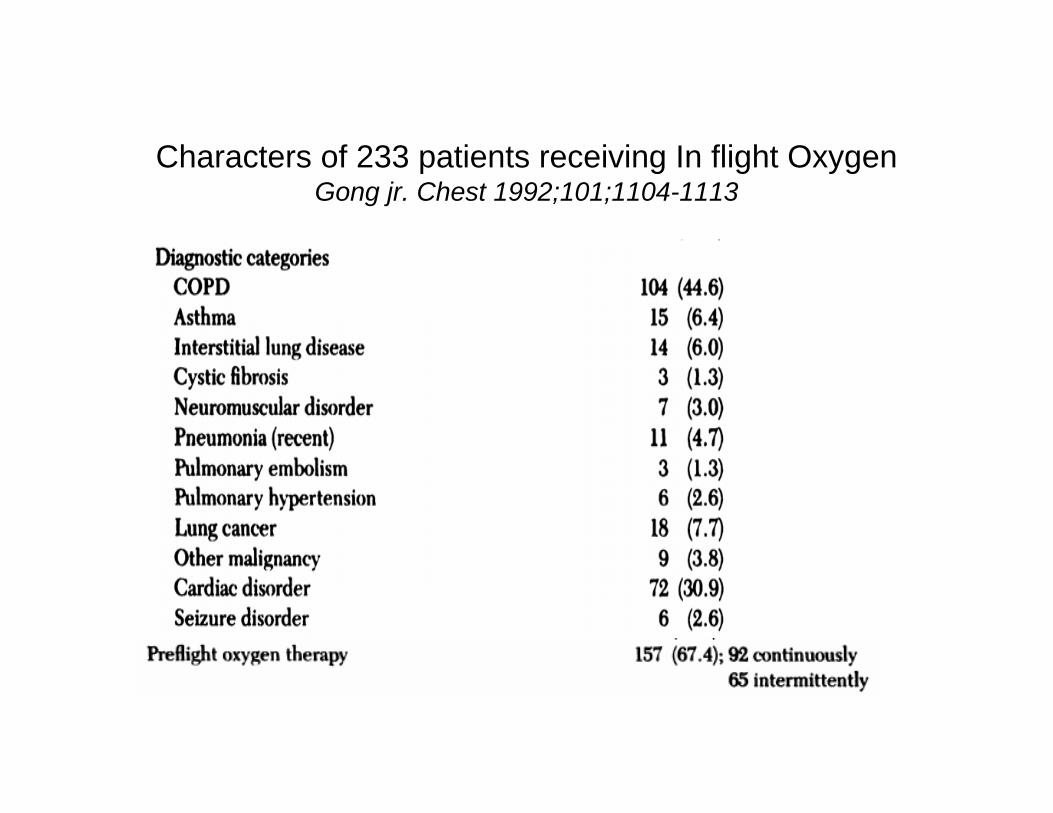
Characters of 233 patients receiving In flight OxygenGong jr. Chest 1992;101;1104-1113
General measures
• Carry well-filled reliever and preventer inhalers in their hand luggage
• Portable battery-operated nebulisers may be used at the discretion of the cabin crew.
• Spacers are as effective as nebulisers
• A full supply of all medication should be taken as hand luggage,preferably in the original packaging with pharmacy labels.
COPD
• 38% of patients with severe COPD had at least one airline trip within 2 year period.
• Only 27% of them consulted physician before trip• 18.2% of them developed symptoms or signs during travel
Dillard TA. Arch Int Med 1991;151:1793-1795
• Mean fall of SpO2 in patients with severe COPD was 11% ( 94 to 83%)Gong H. Am Rev Resp Dis 1984; 130:980-986
• Light exercise such as walking to bathroom with out supplemental oxygen could produce severe hypoxia and near syncope in patients with severe COPD.
Kramer.RA. Chest; 1995 108: 1292-96
• Risk of pneumothorax in relation to size of bulla not studied
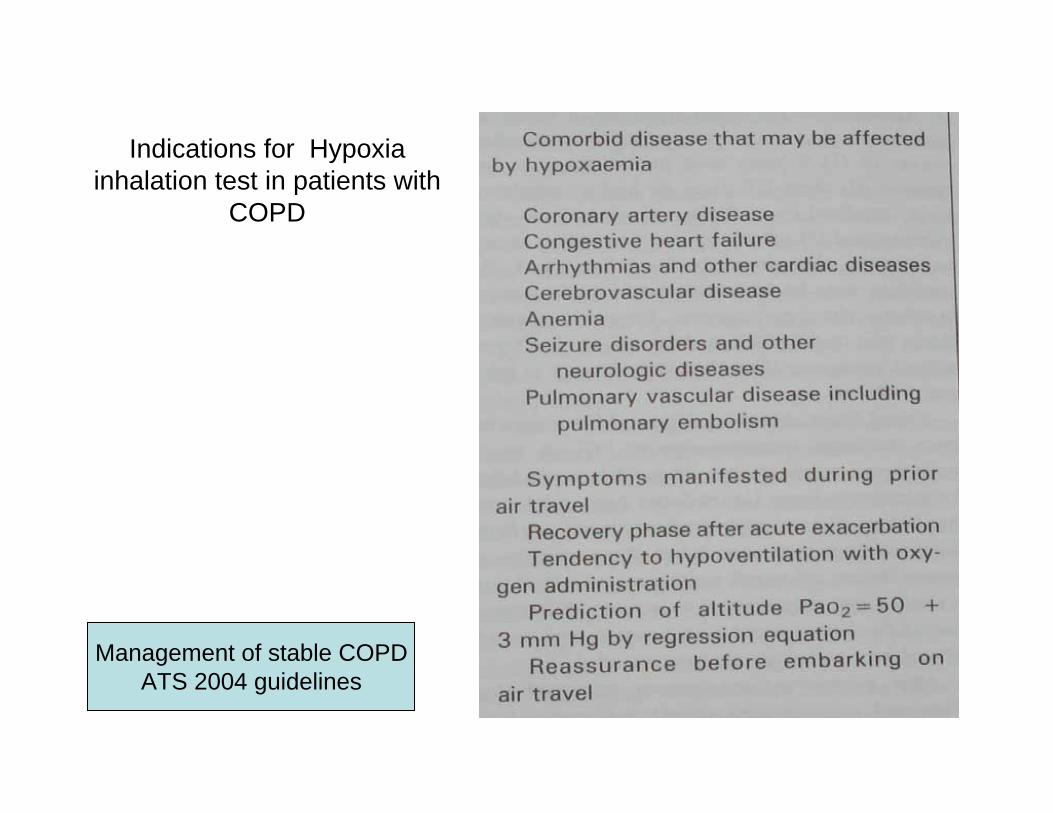
Indications for Hypoxia inhalation test in patients with
COPD
Management of stable COPDATS 2004 guidelines
Bronchial Asthma
• Around one third of in-flight respiratory emergencies are ascribed to asthma.
Cottrel JJ. JAMA 1989; 262: 1653-6
• Patients with severe asthma needs pre flight evaluation of supplemental oxygen.
• Patients are advised to carry inhalers and other regular medications in hand baggage.
• Spacers are as efficient as nebulisers in emergency
ILD
• Patients with moderate restriction (FEV1 50%), PaO2 decreased from 10.4±1.6 kPa at sea level to 6.5±1.1 kPa at 8000 ft simulated altitude, and decreased further during light exercise (5.1±0.9 kPa).
• PaO2 at this altitude correlated positively with sea-level PaO2 and transfer factor of the lung for carbon monoxide and negatively with PaCO2.
• PaO2 increased to acceptable levels with an O2 supply of 2 L/min at rest and 4 L/min during 20 W exercise.
Christensen CC. Eur Respir J 2002;20:300-305
• Patients with severe restriction especially those with hypoxia should undergo pre flight evaluation.
BTS recommendations 2004
Cystic Fibrosis
• Patients with FEV1 <50% should undergo hypoxia inhalation test
• Patients with desaturation ( SpO2< 90%), should receive supplemental oxygen.
• Low cabin humidity could increase risk of bronchospasm and retention secretions with associated risk of atlectasis
OSA
• Patients should alcoholic beverages before and during the flight.
• Should carry dry cell powered CPAP machine
• Patients with significant de-saturation should use CPAP while sleeping onboard.
Patients on LTOT
• Should increase flow of oxygen
• No studies to show how much to be increased
• Titration at Hypoxia Inhalation Test is suggested
• Arrangements for oxygen in airport and transport to be arranged before hand
Ventilator dependant patients
• Should have an escort competent enough to change the tube, perform suctioning and do manual breathing.
• Carry an additional tracheostomy tube and battery driven suction machine
• Monitor cuff pressure (a little air needs to be removed during ascent and a little air be introduced on descent)
Pneumothorax• Relative expansion of humidified gas =
(initial pressure of the gas in the cavity at sea level – 47)
(final pressure of gas in cavity – 47)
• Gas expansion with altitude is significantly greater than predicted by Boyle’s law as applied to dry gas alone.
• The volume of gas in a non-communicating bulla/cavity will thus increase by 37.6% on ascent from sea level to 2438m (8000ft).
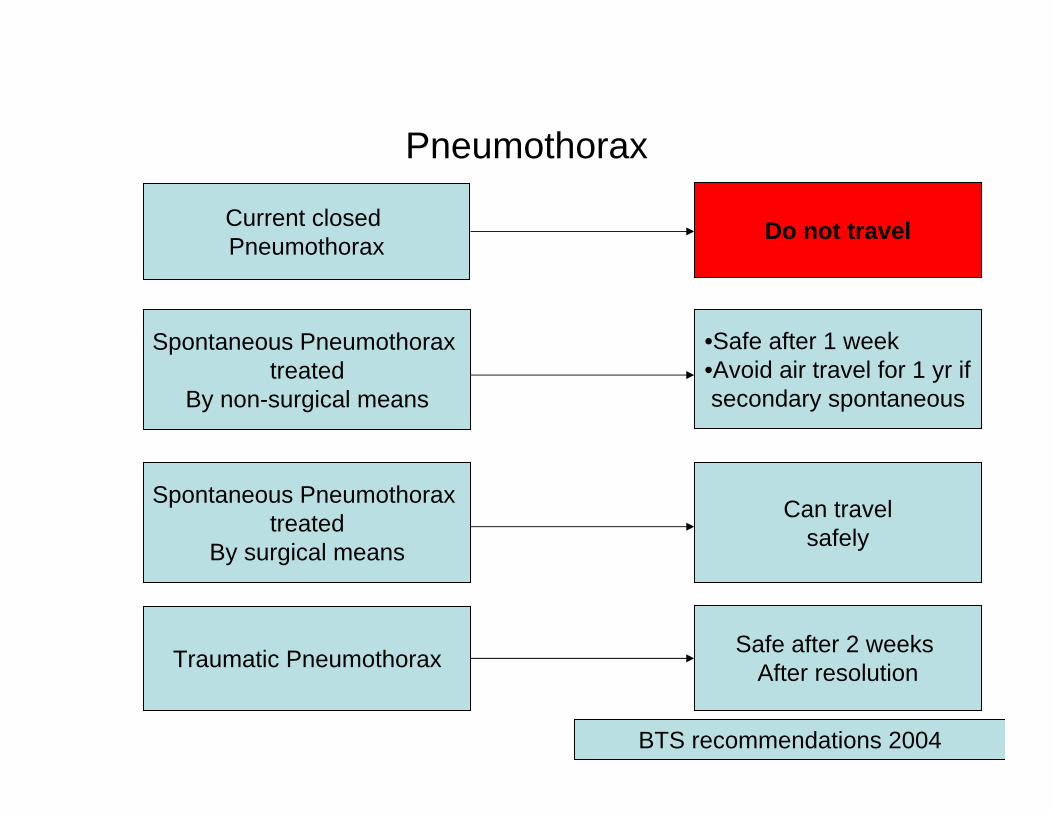
Pneumothorax
Current closed Pneumothorax
Spontaneous Pneumothorax treated
By surgical means
Spontaneous Pneumothorax treated
By non-surgical means
Traumatic Pneumothorax
Do not travel
Can travelsafely
Safe after 2 weeks After resolution
•Safe after 1 week•Avoid air travel for 1 yr ifsecondary spontaneous
BTS recommendations 2004
Deep Vein Thrombosis
DVT
• Economy class syndrome, traveler's thrombosis, flight related DVT
• Hypotheses for increased risk include restricted mobility, seated position, dehydration and alcohol ingestion
• Compression of popletial veins against seat edge
• Decreased cabin pressure and hypoxia can decrease fibrinolytic pathway
Gertler JP.J Vasc Surg 1993;18:939-946
• Hypobaric environment leads to increased activated coagulation pathway
Bendz B.Lancet 2000;356:1657-58
DVT and PTE
• 75 % of post travel DVT were idiopathic against 38% in control group, suggesting air travel as an independent risk factor
Emile F. Chest 1999;115:440–444
• Asymptomatic DVT occurs in nearly 10% of passengers Scurr JH. Lancet 2001; 357:1485-1489
• 11/61 deaths (in 3 yr duration) after arriving at Heathrow airport were due to PTE
Sarvesvaran R. Med Sci Law 1986;26:35-38
• No increase in risk of DVT due to air travel (odds ratio of 1)Rodemil A. The Lancet 2000;352:1492-92
DVT
• Frequency of DVT was 1·0% (9/878, 95% CI 0·5–1·9), which included four cases of pulmonary embolism and five of deep venous thrombosis
• Low to moderate risk populationNZATT study. Hughes RA The Lancet 2003; 362:2039-2044
• LONFLIT 1 study showed zero incidence of DVT in low risk population against 2.8% in high risk population (H/O DVT, malignancy, coagulation disorder or large varicose veins) after 12 hr air travel
Belcaro G. Angiology 2001;52:369-74
• Incidence of DVT increases with distance traveled<5000 km - 0.01 case/million>5000 km - 1.5 case/million>10,000 km - 4.8 case/million
Lapostolle F. N Engl J Med 2001;345:779-83
Prevention of DVT : Stockings
• Elastic stockings prevented DVT in healthy people traveling by air ( no one wearing stockings developed DVT, 10% of control group developed Doppler proven DVT)
Scurr JH. Lancet 2001; 357:1485-1489
• LONFLIT 2 : in high risk population (H/O DVT, malignancy, coagulation disorder or large varicose veins) showed, below kneestockings reduce incidence rate of DVT to 0.24% compared to 4.5%in controls ( flight duration 12.4 hrs)
Belcaro G. Angiology 2001;52:369-74
• LONFLIT 4 study showed reduced incidence of DVT in low and moderate risk population (0/184 Vs 6/188) in long duration flight ( 11-12 hrs) but no added advantage in short duration flights ( 7-8 hrs)
Belcaro G. Angiology 2003; 54: 143-54
Graduated compression stockings
LONFLIT 4 : • 20- 30 mm Hg at ankles
LONFLIT 5 *:• Long haul flight in high risk patients• Speicific “Scholl flight socks”• DVT incidence was 6 times greater in
control group compared to stockings users
• Pressure at ankle was 14-17 mm Hg
* Belcaro G. Clin Appl Thromb Hemost. 2003 Jul;9(3):197-201

Aspirin and LMW Heparin
5/9 patients with DVT/PTE were receiving aspirinNZATT study. Hughes RA The Lancet 2003; 362:2039-2044
LONFLIT 3 study:• 300 High risk patients defined as prior DVT, a coagulation disorder,
obesity or severely limited mobility, malignancy within the preceding 2 years, or large varicose veins
• No Tt Vs Aspirin Vs LMW heparin • 4 cases Vs 3 cases Vs none
• Supports use of LMW heparin in high risk cases ( p 0.02 when compared to controls)
Belcaro G. Angiology 2002; 53:1-6
Other modalities
LONFLIT – FLITE study:
• High risk group• Flight duration 7-8 hrs• Used profibrinolytic agent pinokinase (pine bark extract and
Nattokinase, fermented soya extract)• 0% in Tt group Vs 5.4% in placebo group
Belcaro G. Angiology 2003;54(5):531-9
BTS recommendations : Risk stratification
Slightly increased risk:•>40 yrs•Obesity•Varicose veins•Polycythemia•<72 hours from minor surgery
Moderately increased risk:•Family history of VTE•Pregnancy•Post natal state•Estrogen therapy•Recent MI•Limb paralysis•Limb surgery or trauma
High risk for DVT:•Previous VTE•Thrombophilia•Within six weeks of major surgery• History of previous stroke• Malignancy
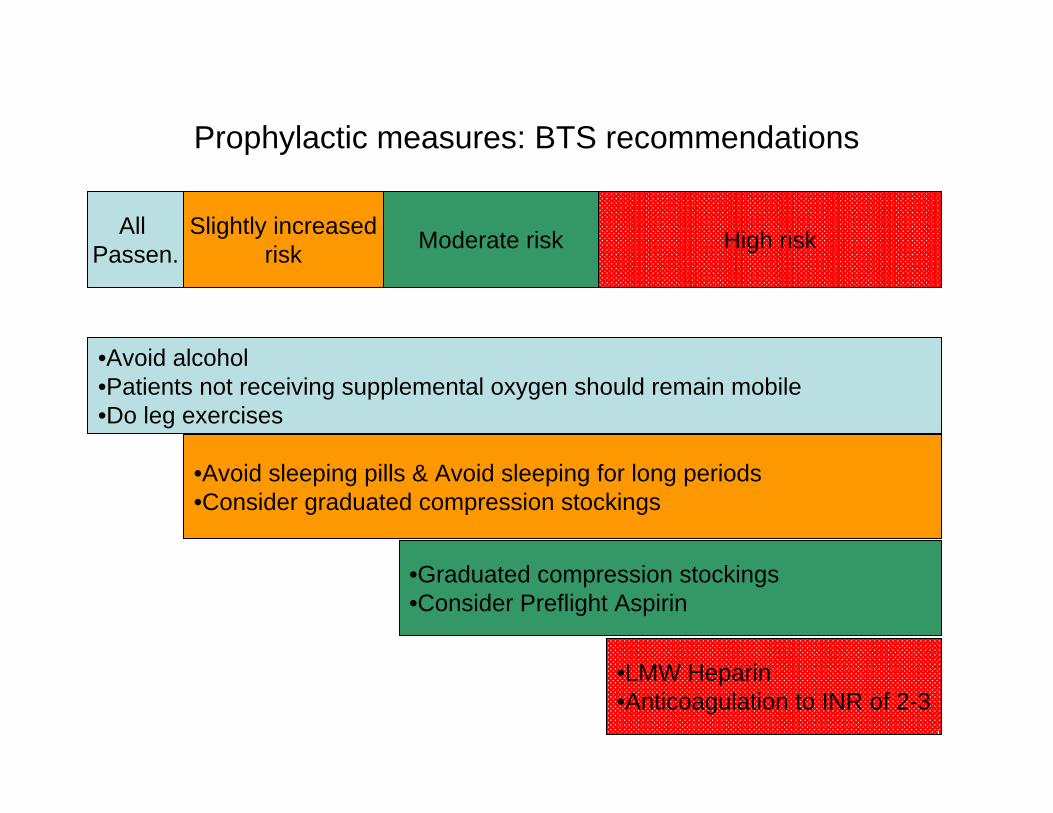
Prophylactic measures: BTS recommendations
•Avoid sleeping pills & Avoid sleeping for long periods•Consider graduated compression stockings
•Graduated compression stockings•Consider Preflight Aspirin
•LMW Heparin•Anticoagulation to INR of 2-3
Slightly increasedrisk Moderate risk High riskAll
Passen.
•Avoid alcohol•Patients not receiving supplemental oxygen should remain mobile•Do leg exercises
Spread of Infectious diseases
Tuberculosis
• Evidence of transmission was limited to crew members exposed to the index case for over 11 hours.
• Transmission was demonstrated only in a few passengers seated in close proximity to the index case, and only on a flight lasting more than eight hours.
Thomas AK. N Engl J Med 1996;334:933-938
Tuberculosis
• Transmission of M. tuberculosis may occur during long (i.e. more than eight hours) flights, from an infectious source (a passenger or crewmember) to other passengers or crew members.
• Air travel does not carry a greater risk of infection with M. tuberculosis than traveling by rail, bus or attending conferences
• To date, no case of active TB has been identified as a result of exposure while on a commercial aircraft.
WHO: Tuberculosis and air travel: Guidelines 1998
Prevention of spread of Tuberculosis
• Non infectious cases only could fly in commercial air crafts:HIV negative patients who have completed two weeks of effective anti tuberculous treatment.HIV positive patients three smear negative sputum examinations on separate days or a single negative sputum culture result are required.
• In case of ground delays >30 mins, adequate ventilation should be provided
• There is no evidence that air recirculation facilitates transmission of tuberculosis
WHO: Tuberculosis and air travel: Guidelines 1998
Other diseases
• Epidemiological studies suggest measles and influenza could spread during air travel
• No evidence that aircraft cabin air recirculation increases the risk for URI symptoms in passengers traveling aboard commercial jets.
Jessica NZ. JAMA. 2002;288:483-486

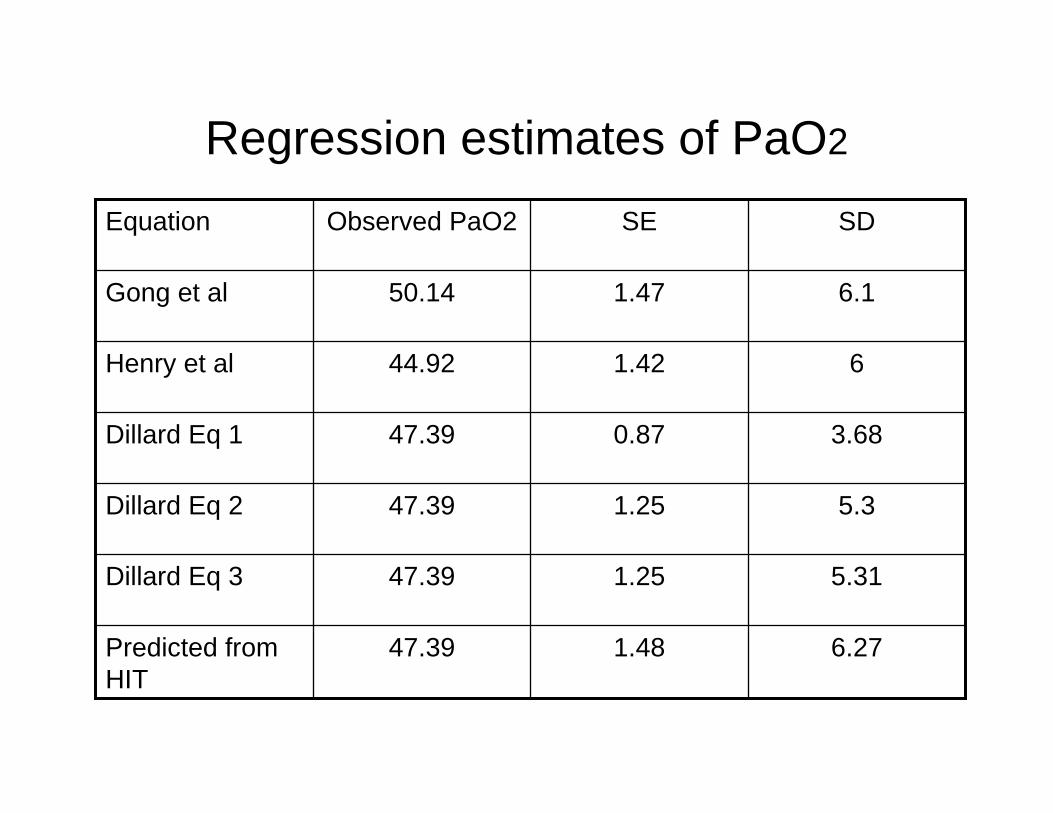
Regression estimates of PaO2
5.311.2547.39Dillard Eq 3
6.271.4847.39Predicted from HIT
5.31.2547.39Dillard Eq 2
3.680.8747.39Dillard Eq 1
61.4244.92Henry et al
6.11.4750.14Gong et al
SDSEObserved PaO2Equation
Advanced lung disease
• 21 Patients with severe diseases being transported for lung transplantation and thrombectomy
• Oxygen supplementation, pulse oximeter monitoring and medical escort
• 20 patients reached destination safely ( distance ranging from 2500 to 13,181 kms)
• Careful preparation, sufficient oxygen supply, oximetricmonitoring, and medical escort, almost any patient with severe lung disease can travel by air to any necessary destination
Kramer MR. Chest, Vol 108, 1292-1296,














![Chronic Obstructive Pulmonary Diseaseopenaccessebooks.com/chronic-obstructive-pulmonary...Chronic Obstructive Pulmonary Disease 5 a-MCI is made [32]. COPD patients without significant](https://img.pdfslide.net/doc/110x75/5f853ccf82a2412fd65b9e28/chronic-obstructive-pulmonary-dis-chronic-obstructive-pulmonary-disease-5-a-mci.jpg)