Embed Size (px)
Citation preview

Airway evaluation Airway evaluation andand
ManagementManagement
By :Dr. Adel ElshimyBy :Dr. Adel Elshimy

Lecture ObjectivesLecture Objectives
Students at the end of the lecture will be able to :Students at the end of the lecture will be able to : Describe the applied anatomy of the airway.Describe the applied anatomy of the airway. Conduct a preoperative airway assessment .Conduct a preoperative airway assessment . Identify a potentially difficult airway.Identify a potentially difficult airway. Learn about management of airway obstruction.Learn about management of airway obstruction. Become familiar with airway equipment.Become familiar with airway equipment. Understand issues around aspiration Understand issues around aspiration
prophylaxis.prophylaxis. Become familiar with controlled ventilation.Become familiar with controlled ventilation. Appreciate ways of monitoring of ventilation Appreciate ways of monitoring of ventilation
and oxygenation.and oxygenation.

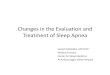
AIRWAY CONTROLAIRWAY CONTROLOpening the AirwayOpening the Airway
Jaw thrust Head tilt–chin lift

AIRWAY CONTROLAIRWAY CONTROLOropharyngeal AirwayOropharyngeal Airway

Mask VentilationMask Ventilation
Oral airwayOral airway Two-handed techniqueTwo-handed technique

AIRWAY CONTROLAIRWAY CONTROLOropharyngeal Airway (cont.)Oropharyngeal Airway (cont.)

AIRWAY CONTROLAIRWAY CONTROLNasopharyngeal Airway (cont.)Nasopharyngeal Airway (cont.)

OXYGENATION AND VENTILATIONOXYGENATION AND VENTILATIONBag-Valve-Mask (cont.)
With oxygen reservoir

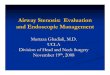
Esophageal-Tracheal CombitubeEsophageal-Tracheal Combitube
A = esophageal obturator; ventilation into trachea through side openings = B
C = tracheal tube; ventilation through open end if proximal end inserted in trachea
D = pharyngeal cuff; inflated through catheter = E
F = esophageal cuff; inflated through catheter = G
H = teeth marker; blindly insert Combitube until marker is at level of teeth
Distal End
Proximal End
B
C
D
E
F
G
H
A


UsageUsage

Indications of intubationIndications of intubation
Resuscitation (CPR)Resuscitation (CPR) Prevention of lung soilingPrevention of lung soiling Positive pressure ventilation (GA)Positive pressure ventilation (GA) Pulmonary toiletPulmonary toilet Patent airway (coma or near coma)Patent airway (coma or near coma) Respiratory failure(CO2 retention )Respiratory failure(CO2 retention )

Airway AnatomyAirway Anatomy InnervationInnervation Vagus n.Vagus n.
Superior laryngeal n.Superior laryngeal n. External branch – motor External branch – motor
to cricothyroid m.to cricothyroid m. Internal branch – Internal branch –
sensory larynx above sensory larynx above TVC’sTVC’s
Recurrent laryngeal n.Recurrent laryngeal n. Right – subclavianRight – subclavian Left – Aortic arch (board Left – Aortic arch (board
question)question) Motor to all other Motor to all other
muscles, Sensory to muscles, Sensory to TVC’s and tracheaTVC’s and trachea

Management Management
I-History:I-History: previous history of difficulty is the best previous history of difficulty is the best
predictorpredictorInquire about:-Nature of difficultyInquire about:-Nature of difficulty -No of trials-No of trials -Ability to ventilate bet trials-Ability to ventilate bet trials -Maneuver used-Maneuver used -Complications-ComplicationsII-Snoring and sleep apnea( prdictors of II-Snoring and sleep apnea( prdictors of
DMV)DMV)

LEMONLEMON
-Look for any obvious anomaly -Look for any obvious anomaly Morbid obesity(BMI)Morbid obesity(BMI) SkullSkull FaceFace JawJaw Mouth,teethMouth,teeth Neck Neck

ExaminationExamination
I-The 3 joints movementsI-The 3 joints movements A-O joint(15-20 degrees)A-O joint(15-20 degrees)
Presence of a gap bet the Presence of a gap bet the
Occiput and C1 is essentialOcciput and C1 is essential The cervical spine(range>90)The cervical spine(range>90) T.M joint:T.M joint: -subluxation (1 finger)-subluxation (1 finger)

ExamineExamine Airway Airway
The 3 – 3 – 2 ruleThe 3 – 3 – 2 rule Mouth open: 3 fingersMouth open: 3 fingers Mentum to hyoid: 3 fingersMentum to hyoid: 3 fingers Floor of mouth to thyroid Floor of mouth to thyroid
cartilage: 2 fingerscartilage: 2 fingers

ExamineExamine Airway Airway
Mouth openMouth open: 3 fingers: 3 fingersAllows insertion of tube, Allows insertion of tube,
laryngoscopelaryngoscopeMentum to hyoidMentum to hyoid: 3 fingers: 3 fingers
Predicts ability to lift tongue Predicts ability to lift tongue into mandibleinto mandible

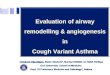
MallampattiMallampatti
Mallampatti test:Mallampatti test:
Based on the hypothesisBased on the hypothesis
That when the base of theThat when the base of the
Tongue is disproportionallyTongue is disproportionally
Large it will overshadow theLarge it will overshadow the
larynxlarynx

-Simple easy test,correlates with what is seen during -Simple easy test,correlates with what is seen during laryngoscopy or Cormack-Lehene grades ,butlaryngoscopy or Cormack-Lehene grades ,but
1-moderate sensitivity and specificity(12% false +ve)1-moderate sensitivity and specificity(12% false +ve)
2-Inter observer variation2-Inter observer variation
3-Phonation increases false negative view3-Phonation increases false negative view

II-Wilson testII-Wilson test
-Consists of 5 easily assessed factors-Consists of 5 easily assessed factors Body wight(n=0 ,>90=1,>110=2)Body wight(n=0 ,>90=1,>110=2) Head and neck movementHead and neck movement Jaw movementJaw movement Receding jawReceding jaw Buck teethBuck teeth
Each factor assigned as o ,1 ,2 max is Each factor assigned as o ,1 ,2 max is 1010

ObstructionObstruction
Apparent cause e.g. goitreApparent cause e.g. goitre OSAOSA Noisy breathing or stridorNoisy breathing or stridor Signs of upper airway obstructionSigns of upper airway obstruction Other causesOther causes

NeckNeck Mobility Mobility
Prior conditionPrior condition SurgerySurgery Rheumatoid Rheumatoid
arthritisarthritis OsteoarthritisOsteoarthritis OthersOthers

Proper EquipmentProper Equipment
-Bag and mask,oxygen source-Bag and mask,oxygen source
-Airways oro and nasopharyngeal-Airways oro and nasopharyngeal
-Laryngosopes different blades-Laryngosopes different blades
-ETT different sizes-ETT different sizes
-suction on-suction on

Airway gadgetsAirway gadgets

Mask VentilationMask Ventilation
Induction of Induction of anesthesia anesthesia produces upper produces upper airway relaxation airway relaxation and possible and possible collapsecollapse
Downward Downward displacement of displacement of mask with thumb mask with thumb and index fingerand index finger

Requirement of successful Requirement of successful intbatinintbatin
1-Normal roomy 1-Normal roomy mandiblemandible
2-Normal T-M, A-O 2-Normal T-M, A-O , and C-spine, and C-spine

Positioning for successful Positioning for successful intubationintubation
3-Alignment of 3 axes or3-Alignment of 3 axes or
Assuming sniffing positionAssuming sniffing position
-Any anomaly in these 3 joints-Any anomaly in these 3 joints
A-O, T-M or C-spine can resultA-O, T-M or C-spine can result
In difficult intubationIn difficult intubation

Endotracheal IntubationEndotracheal Intubation Look for epiglottisLook for epiglottis
If initially not found If initially not found insert laryngoscope insert laryngoscope furtherfurther
If this maneuver does If this maneuver does not work slowly pull not work slowly pull laryngoscope backlaryngoscope back
Once epiglottis visualized, Once epiglottis visualized, push laryngoscope into push laryngoscope into vallecula and apply vallecula and apply traction at 45 degree traction at 45 degree angle to “push” epiglottis angle to “push” epiglottis up and out of the wayup and out of the way

Confirm tube positionConfirm tube position
Direct visualization of ETT between Direct visualization of ETT between cordscords
Bronchoscopy ;carina seenBronchoscopy ;carina seen Continuous trace of capnographyContinuous trace of capnography 3 point auscultation3 point auscultation Esophageal detector deviceEsophageal detector device Other as bilateral chest Other as bilateral chest
movement,mist in the tube,CXRmovement,mist in the tube,CXR

Rapid sequence Rapid sequence inductioninduction
IndicationsIndications Technique: Technique:
-Preoxygenation-Preoxygenation
-IV induction with sux-IV induction with sux
-Cricoid pressure-Cricoid pressure
-Intubate, inflate the cuff ,confirm -Intubate, inflate the cuff ,confirm positionposition
-Release cricoid and fix the tube-Release cricoid and fix the tube

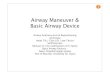
Cricoid pressureCricoid pressure
Cricoid Pressure

Complications of Complications of intubationintubation
1-Inadequate 1-Inadequate ventilationventilation
2-Esophageal 2-Esophageal intubationintubation
3-Airway obstruction3-Airway obstruction
4-Bronchospasm4-Bronchospasm
5-Aspiration5-Aspiration
6- Trauma6- Trauma
7-Stress response7-Stress response

Difficult airwayDifficult airway
CausesCauses
-Congenital-Congenital
-Acquired-Acquired


Airway gadgetsAirway gadgets

Rigid Fiberoptic ScopeRigid Fiberoptic Scope
Bullard Bullard Wu ScopeWu Scope

Rigid Fiberoptic ScopeRigid Fiberoptic Scope
Upsher Upsher GlideScopeGlideScope



Difficult airwayDifficult airway
Expected from history,examinationExpected from history,examination
Secure airway while awake under LASecure airway while awake under LA
Unexpected different optionsUnexpected different options
Priority for maintenance of patent Priority for maintenance of patent airway and oxygenationairway and oxygenation

Transtracheal Jet Transtracheal Jet VentilationVentilation

VentilationVentilation
Spontaneous ventilationSpontaneous ventilation Controlled ventilationControlled ventilation Minute volume dividerMinute volume divider
-Tidal volume 10 mls/kg-Tidal volume 10 mls/kg
-Respiratory rate to maintain -Respiratory rate to maintain normocarbianormocarbia
-I:E ratio -I:E ratio

RecommendationsRecommendations
Adequate airway assessment to pick up Adequate airway assessment to pick up expected D.A to be secured awakeexpected D.A to be secured awake
Difficult intubation cart always readyDifficult intubation cart always ready Pre oxygenation as a routinePre oxygenation as a routine
Maintenance of oxygenation not the Maintenance of oxygenation not the intubation should be your aimintubation should be your aim
Use the technique you are familiar withUse the technique you are familiar with Always have plan B,C,D in unexpected D.AAlways have plan B,C,D in unexpected D.A

ReferencesReferences
Anesthesia and resuscitationAnesthesia and resuscitation Dr. H .BradenDr. H .Braden chapters 1,2 Airway and ventilationchapters 1,2 Airway and ventilation
Lecture notes on clinical anesthesiaLecture notes on clinical anesthesia Carl Gwinnutt Carl Gwinnutt 22ndnd edition edition Chapter 2 page 18-29Chapter 2 page 18-29

DrDr. Adel Elshimy. Adel Elshimy
Date: 18/10/2011Date: 18/10/2011
TThank You hank You